Physical Examination of the Skin, Hair, and Nails.
55
Physical Examination of the Skin, Hair, and Nails
-
Upload
ethan-richards -
Category
Documents
-
view
269 -
download
5
Transcript of Physical Examination of the Skin, Hair, and Nails.
Physical Examination of the
Skin, Hair, and Nails

Skin Function
Protective barrier
Mechanical barrier
Temperature regulator
Sensor
Vitamin D producer
Repairer
Excreter
Expresser

Skin Anatomy

Skin Appendages

Hair

Nails
Signs & Symptoms
Hair Loss
Lesiones
moles

Skin CA
Basal cell carcinoma(BCC)
Squamous cell carcinoma(SCC)
Melanom

معاینه خال از لحاظ بدخیمی
Asymmetry
Irregular borders
Cheng in color
Diameter > 6mm

History
Past Medical History
previous problems
systemic disease
Family History
skin CA, psoriasis, allergy, infestations and infections
Psychosocial
personal habits
exposures

Examination
Ruler
Lighting
Penlight
Gloves
Magnifying glass
Woods lamp

Examination (exposure!)
Inspection Color Uniformity Thickness Hygiene Lesions
Palpation Moisture Temperature Texture Turgor Mobility

color
تغییرات پیگمانتاسیون:
لکه شیر قهوه
تینه آورسیکالر
لک و پیس
سیانوز
زردی
کاروتنمی
اریتم
هلیوتروپ

)اکسی هموگلوبین و رنگ پریدگیpale(: در الیه شاخی اپیدرم (ناخن های انگشتان، دستها، لبها و غشاهای محیطی)
سیانوز مرکزی: لب ها، مخاط دهان ، زبان
سیانوز مرکزی: ناخن ها، دست و پا
،یرقان (ایکتر): در صلبیه، ملتحمه پلکی، لب ها، کام سختسطح زیرین زبان، پرده صماخ
کاروتنمی: کف دست و پا و صورت

turgor
کاهش تحرک: ادم و اسکلرودرمی
کاهش توگور: هیدراتاسیون

الگوها و اشکال
خطی
جغرافیایی
خوشه ایی
پیچ و خم دار
حلقوی و قوسی شکل

Terminology
:ضایعات پوستی اولیه
:ماکول – وصلهضایعات تخت غیر قابل لمس
:(توده های توپر)پالک – پاپول – برجستگی های قابل لمسندول – کیست – ویل
:وزیکول – برجستگی های قابل لمس با حفرات پر از مایعتاول - پوستول

ضایعات پوستی ثانویه: ضایعات فرو رفته
)ساییدگیerosion :( ازدست رفتن اپیدرم بدون جوشگاه وسطح مرطوب بدون خونریزی
)خراشیدگیexcoriation :(ضایعات ناشی از خراشیدن
)شقاقfissure :( شکاف خطی در پوست ناشی از خشکیبیش از حد
)زخمulcer :(از دست رفتن عمیق اپیدرم و درم

ضایعات پوستی ثانویه ناشی از(درمان بیش از حد،خراشیدن بیش
از حد وعفونت ضایعات اولیه)پوسته: اپیدرم مرده ریزش یافته
دلمه: باقی مانده خشک شده سرم، چرک و خون
لینفیکاسیون(چرمی شدن): ضخیم شدگی اپیدرم با خطوططبیعی
اسکار: بافت همبند بر اثر جراحت
کلویید: هیپرتروفی اسکار

I. Primary lesions = lesions which have not been altered by external forces or time
A. Flat, non-palpable lesions (demarcated only by color change from the surrounding skin; cannot be distinguished by touch)
1. Macule – smaller than 2 cm. In diameter
2. Patch – larger than 2 cm.
B. Solid, palpable lesions
1. Papule – smaller than 1 cm., elevated above the skin surface.
2. Plaque – larger than 1 cm., flat-topped and elevated above the skin surface. Plaques may be very large, covering extensive areas. Smaller plaques may be composed of grouped, confluent papules.
3. Nodule – Usually spherical, a nodule may be palpated deeper than a papule or plaque and may be below the skin surface.
4. Wheal – A papule or plaque which is formed by edema in the skin, and which typically disappears after a short time.

II. Fluid-filled lesions
1. Vesicle – smaller than 1 cm and raised above the skin surface; a
vesicle usually contains a clear serous fluid, but may also contain
blood. Vesicles are commonly called blisters.
2. Bulla – Larger than 1 cm with the same contents as a vesicle.
3. Cyst – A firm-walled lesion usually containing a semisolid material. A
cyst may be distinguished from a nodule by its softer, more rubbery
feel.
4. Pustule – Small lesion raised above the skin which contains purulent
(opaque) material (pus). Lesions which contain pus and that are larger
and extend deeper are called in order of the increasing size, furuncles,
carbuncles (made up of multiple furuncles) and abscesses.
III. Depressed lesions
1. Erosion – An area of skin loss, usually with a moist, erythematous
base. An erosion is fairly superficial and does not extend below the epidermis.
2. Ulcer – An area of skin loss extending into the dermis or deeper.
3. Fissure – A linear erosion or ulcer.
IV. Secondary lesions – These occur as the result of change in primary lesions over time, or from exogenous manipulation of the skin.
1. Scale – White flakes from the top of the epidermal layer
(stratum
corneum) which are retained on the skin surface.
2. Crust (scab or eschar) – A solid, brownish covering over a lesion
which is composed of old dried serum, blood or exudate.
3. Erosion – As described above. An erosion may be secondary if it
results from the rupture of a vesicle or bulla. An excoriation is
erosion created by scratching and is usually linear or angular.
4. Lichenification – Thickening of the skin with accentuation of skin
lines. Lichenification results from repeated rubbing and scratching.

اختالالت ناخن:
پارونشیا یا عقربک: عفونت سطحی چین های پروگزیمال ومعموال ناشی از استافیلوکوک طالیی
)شل شدن ناخنonycholysis جدایی بدون درد صفحه : (ناخن ناشی از آرایش بیش از حد ناخن،عفونت ناخن،واکنش
آلرژیک، دیابت، کم خونی، پرکاری تیرویید
ناخن های تری: سفیدی صفحه ناخن با نوار دیستال قهوه ایی ومحو ماهک ناخن
چماقی شدن: افزایش زاویه بین ناخن و چین پروگزیمال بیش درجه بیماریهای مادرزادی قلبی،سزطان، التهابی روده، 180از
هیپوکسی

)لکه های سفیدleukonychia لکه های غیر هم شکل سفید :(که همراه با ناخن رشد می کنند در آرایش مفرط ناخن
خطوط عرضی سفید یا میز: خطوط عرضی منحنی سفید بهموازات ماهک در مسمومیت با آرسنیک، نارسایی قلبی
خطوط بیو: فرورفتگی های عرضی ناخن در در بیماریهایشدید، مواجهه با سرما و ضربها
پیتینگ یا چالدار شدن: فرورفتگی نقطه نقطه صفحه ناخن دردرماتیت آتوپیک، آلوپسی آره آتا

ریزش مو
آلوپسی آره تا: تکه های گرد با حدود مشخص از ریزشمو(معموال درنوجوانان و جوانان)
تریکوتیلومانی: ریزش مو با کشیدن یا پیچاندن مو(شایعتردرکودکان) تحت تنش روانی
)کچلی سرringworm ناشی از عفونت قارچی شبیه :(درماتیت سبورییک به صورت تکه های پوسته ریز مدورناشی از
ریزش مو

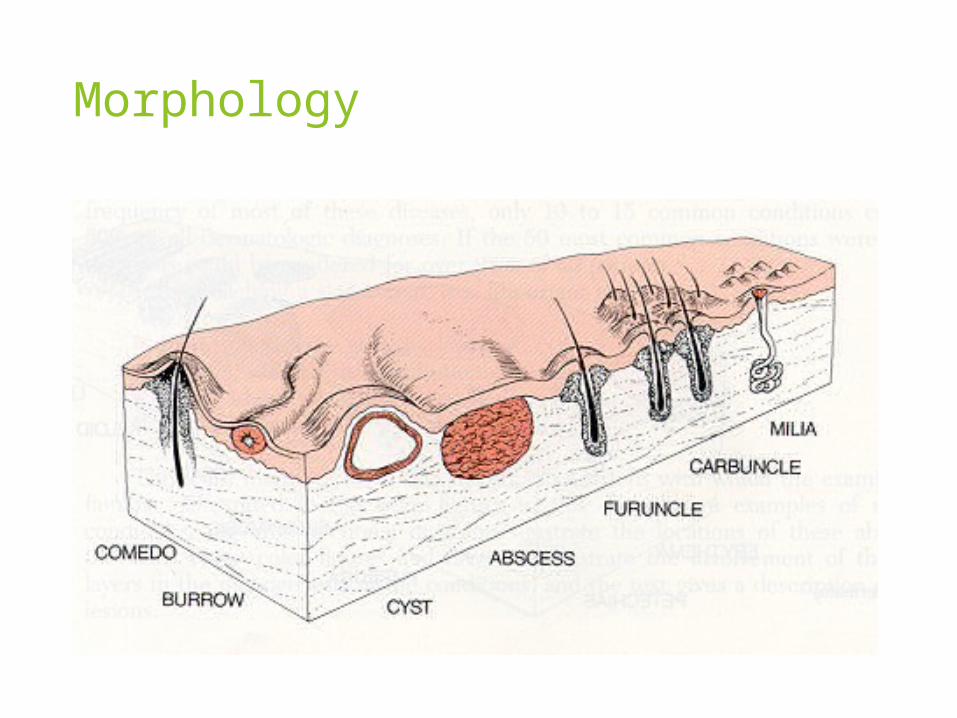
Morphology

MACULE PATCH

Morphology

PLAQUE WHEAL

NODULES

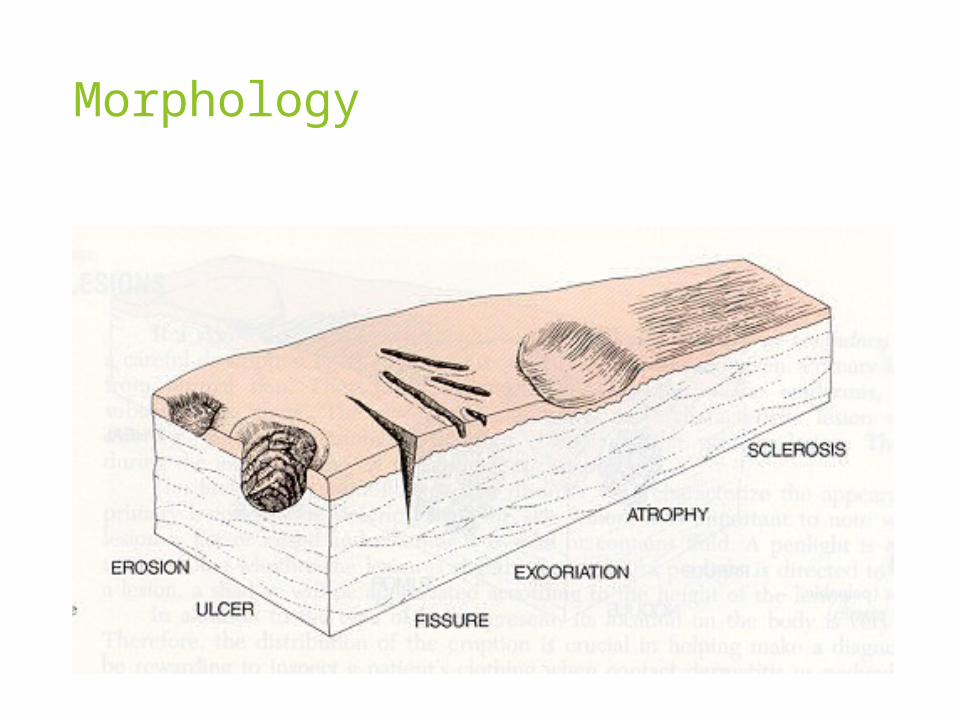
Morphology
Morphology

VESICLE BULLA

PUSTULE CYST

Morphology

CRUSTINGSCALING
Morphology

EXCORIATION EROSION

FISSURE ULCER

ATROPHY LICHENIFICATION

HYPERTROPHIC SCAR KELOID

Configuration

Distribution

EXAMINATIONNAILS

EXAMINATIONNAILS
Spooning - kiolonychia

EXAMINATIONNAILS

Example Documentation
No abnormalities - General Statement about overall skin assessment:
Skin is warm, smooth and well hydrated. Full hair distribution on scalp, axilla, and genitalia. Nails are neatly trimmed and without deformity. No discrete lesions noted.

Example write-up
A wide variety of lesions are seen on the face, shoulders, and back. Pustules on an inflammatory base are most predominant. Inflammatory pustules are seen on the forehead, lower cheeks, and chin. Large abscesses and cysts are seen on the shoulders and upperback. Numerous scars are present.

Example write-up
There are multiple large oval plaques with well defined borders and silvery scale symmetrically present on the elbows, knees and scalp. Examination of the nails reveals pitting. The hair is of normal texture.

Example write-up
A diffuse erythematous maculopapular patch is present on the trunk. Few excoriations are present on the shoulders and chest. The hair and nails are unremarkable.

Example write-up
There is a bright red 6 cm linear eruption of edematous papules and bulae along the lateral aspect of the left leg. There are no lesions on the palms or soles or in the mouth.

ضایعات عروقی
تالنژکتازی ها یا رگهای کوچک گشاد که قرمز یا مایل به آبی
2cmآنژیوم عنکبوتی: در صورت ،گردن و بازوها و تقریبا در پایین کمر وجود ندارد در بیماری کبدی، آبستنی، کمبود ویتامینB ،بدنه مرکزی گاه برامده و احاطه شده توسط اریتم و پاهای افشان
ورید عنکبوتی:مایل به آبیشبیه عنکبوتافزایش فشار در ورید مرکزیواریس
میلی متر1-3آنژیوم عنکبوتی: قرمز روشن و یاقوتی، گرد، تخت یا گاه برامدهتنه همچنین دست ها و پاهااهمیت ندارد، با باال رفتن سن

ضایعات عروقی
پتشی یا پورپورا:قرمز تیره که با گذشت زمان محو
:میلی متر؛ پورپورا: بزرگتر1-3پتشی
مدور، فشار تاثیری بر جای نمی گذارد
توزیع: متغیر
اهمیت: خون خارج شده از رگها نشانگر یک اختالل خونریزیدهنده
در مورد پتشی آمبولی به پوست
پورپورا: واسکولیت

ضایعات عروقی
:اکیموز
بنبفش با بنفش مایل به آبی
>3اندازه متغیر و بزرگتر از پتشیmm
مدور، بیضی یا نامنظم ممکن است در مرکز یک ندول زیرپوستی
فشار تاثیری بر جای نمی گذارد
توزیع متغیر
ثانویه به کوفتگی یا ضربه و اختالالت خونریزی دهنده