
Physical Activity Predicts Weight Loss Following Gastric Bypass Surgery: Findings from a Support...
8
RESEARCH ARTICLE Physical Activity Predicts Weight Loss Following Gastric Bypass Surgery: Findings from a Support Group Survey Garry Welch & Cheryl Wesolowski & Bernadette Piepul & Jay Kuhn & John Romanelli & Jane Garb Received: 13 June 2007 / Accepted: 24 July 2007 / Published online: 26 March 2008 # Springer Science + Business Media B.V. 2008 Abstract Background Patient adherence to recommended eating and physical activity behaviors is considered important to weight loss outcomes following gastric bypass surgery, but there has been little systematic research in this area to investigate behavioral predictors of weight loss. Method We developed a measure of postsurgical behaviors, the bariatric surgery self-management questionnaire (BSSQ). A survey was conducted of 200 patients attending postsurgical support groups (mean time since surgery 14 months, mean age 40 years, 85% female, presurgical weight 150 kg). Patients completed the BSSQ and measures of treatment regimen distress, perceived benefits of weight loss, and weight-related physical symptoms. Results Mean BSSQ adherence was in the 70% range, with subscale scores varying considerably. Distress levels asso- ciated with the new lifestyle were consistently low (≈20%) and perceived benefits of weight loss were high early on and maintained consistently (70–90%). A final predictive model showed premorbid weight, time since surgery, and BSSQ physical activity subscale were significant predictors of weight loss, accounting for 73% of variance. Conclusions Physical activity adherence was the sole significant behavioral predictor of weight loss, although maladaptive dietary habits and patient selection issues were identified for future research. It will be important to replicate the current study in prospective, longitudinal studies with representative patient cohorts. A challenge for researchers will be to develop novel, intensive recruiting and retention strategies to allow closer examination of these issues. Keywords RYGB . Bariatric surgery . Self management behaviors . Distress . Weight loss . Benefits Introduction Prior to the availability of bariatric surgery, medical treatment options for the morbidly obese were limited. A sizeable body of research conducted since the 1970s has shown that intensive medical weight loss interventions combining behavioral, dietary, and pharmacological strate- gies can provide mean weight losses in the 5–10% range that provide health benefits. However, these interventions have been associated with disappointing long-term (i.e., 5 year) results with high drop out rates, with most patients returning to preintervention weights [1]. Individuals with morbid obesity (who are by definition at least 45.5 kg overweight) require more aggressive and sustainable inter- ventions than traditional medical approaches can provide, and bariatric surgery has emerged as the only viable treatment option [2]. Roux-en Y gastric bypass (RYGB) and other bariatric surgery approaches are not considered to be a “magic bullet” for weight loss but adjunctive tools that can help the patient initiate and sustain new dietary and physical activity behaviors that will support weight loss OBES SURG (2008) 18:517–524 DOI 10.1007/s11695-007-9269-x G. Welch (*) Behavioral Medicine Research, Baystate Medical Center, 140 High Street, Room 2104, Springfield, MA 01199, USA e-mail: [email protected] C. Wesolowski : B. Piepul : J. Kuhn : J. Romanelli Weight Loss Surgery Program, Baystate Medical Center, Springfield, MA, USA J. Garb Department of Surgery, Baystate Medical Center, Springfield, MA, USA
-
Upload
garry-welch -
Category
Documents
-
view
212 -
download
0
Transcript of Physical Activity Predicts Weight Loss Following Gastric Bypass Surgery: Findings from a Support...

RESEARCH ARTICLE
Physical Activity Predicts Weight Loss Following GastricBypass Surgery: Findings from a Support Group Survey
Garry Welch & Cheryl Wesolowski & Bernadette Piepul &Jay Kuhn & John Romanelli & Jane Garb
Received: 13 June 2007 /Accepted: 24 July 2007 / Published online: 26 March 2008# Springer Science + Business Media B.V. 2008
AbstractBackground Patient adherence to recommended eating andphysical activity behaviors is considered important toweight loss outcomes following gastric bypass surgery,but there has been little systematic research in this area toinvestigate behavioral predictors of weight loss.Method We developed a measure of postsurgical behaviors,the bariatric surgery self-management questionnaire(BSSQ). A survey was conducted of 200 patients attendingpostsurgical support groups (mean time since surgery14 months, mean age 40 years, 85% female, presurgicalweight 150 kg). Patients completed the BSSQ and measuresof treatment regimen distress, perceived benefits of weightloss, and weight-related physical symptoms.Results Mean BSSQ adherence was in the 70% range, withsubscale scores varying considerably. Distress levels asso-ciated with the new lifestyle were consistently low (≈20%)and perceived benefits of weight loss were high early onand maintained consistently (70–90%). A final predictivemodel showed premorbid weight, time since surgery, andBSSQ physical activity subscale were significant predictorsof weight loss, accounting for 73% of variance.
Conclusions Physical activity adherence was the solesignificant behavioral predictor of weight loss, althoughmaladaptive dietary habits and patient selection issues wereidentified for future research. It will be important toreplicate the current study in prospective, longitudinalstudies with representative patient cohorts. A challengefor researchers will be to develop novel, intensive recruitingand retention strategies to allow closer examination of theseissues.
Keywords RYGB . Bariatric surgery . Self managementbehaviors . Distress .Weight loss . Benefits
Introduction
Prior to the availability of bariatric surgery, medicaltreatment options for the morbidly obese were limited. Asizeable body of research conducted since the 1970s hasshown that intensive medical weight loss interventionscombining behavioral, dietary, and pharmacological strate-gies can provide mean weight losses in the 5–10% rangethat provide health benefits. However, these interventionshave been associated with disappointing long-term (i.e.,5 year) results with high drop out rates, with most patientsreturning to preintervention weights [1]. Individuals withmorbid obesity (who are by definition at least 45.5 kgoverweight) require more aggressive and sustainable inter-ventions than traditional medical approaches can provide,and bariatric surgery has emerged as the only viabletreatment option [2]. Roux-en Y gastric bypass (RYGB)and other bariatric surgery approaches are not considered tobe a “magic bullet” for weight loss but adjunctive tools thatcan help the patient initiate and sustain new dietary andphysical activity behaviors that will support weight loss
OBES SURG (2008) 18:517–524DOI 10.1007/s11695-007-9269-x
G. Welch (*)Behavioral Medicine Research, Baystate Medical Center,140 High Street, Room 2104,Springfield, MA 01199, USAe-mail: [email protected]
C. Wesolowski : B. Piepul : J. Kuhn : J. RomanelliWeight Loss Surgery Program, Baystate Medical Center,Springfield, MA, USA
J. GarbDepartment of Surgery, Baystate Medical Center,Springfield, MA, USA

[3, 4]. Bariatric surgery procedures are not expected tooverride unhealthy lifestyle habits that might reemergefollowing surgery, such as binge eating, grazing, emotionaleating, night eating, drinking of high-calorie beverages, orreturn to a sedentary lifestyle [3, 5–7].
The aim of this study was to evaluate a new measure ofpostsurgical behaviors that we developed to assess the levelof patient adherence to the recommended postsurgicalbehaviors and to investigate related aspects of patientadjustment to the postsurgical lifestyle, such as lifestyleburden and perceived benefits of weight loss. We alsoconducted an examination of predictors of weight loss overtime that included demographic, clinical, behavioral, andpsychosocial variables using a representative sample ofpatients attending our postsurgical support groups.
Methods
We surveyed 201 consecutive RYGB patients attendingpostsurgical support group sessions conducted over a3-month period in mid-2005. All patients were seen at theBaystate Medical Center (BMC) Weight Loss Surgery(WLS) program. BMC is a large, 641-bed teaching hospitalin Western Massachusetts and the Western Campus of TuftsUniversity School of Medicine. Using the BMC surgicalprocedures database, we determined that the WLS programbegan in 1999 with 10 patients and conducted subsequent-ly the following number of surgeries: 2000, n=85; 2001,n=102; 2002, n=205; 2003, n=269; and 2004, n=348.Finally, from January 2005 to the beginning of the studysurvey period, there were n=183 surgeries, to give a total of1,202 patients eligible to attend our support groups. Wecaptured 200/201 (99.5%) of the 201 RYGB patientsattending our support groups in the 3-month survey timeframe, which represented 200/1,202 or 16.6% of all patientsoperated on.
Survey patients provided background and demographicdata by questionnaire and then completed a battery of fourstudy measures and signed an informed consent formapproved by our institutional review board committee. Arandomly selected subsample of patients (n=60) provideddata for temporal (test–retest) reliability estimates for thestudy questionnaires. These patients repeated the studyquestionnaires 2 weeks after the initial survey, returnedthem by mail, and received a small stipend for each surveybattery completed to enhance participation rates.
Table 1 shows the clinical and demographic character-istics of the survey sample, as well as a comparison sample ofconsecutive clinic patients (n=100, excluding one refusal)seen at a routine 2-week postsurgical clinic visit at theWLS clinic by the bariatric nurse in mid-2005. This samplewas obtained to provide a representative, consecutive
patient cohort to examine potential sample bias from theuse of support group patients in our survey.
Measures
Basic demographic and clinical information was obtainedfor all patients by a combination of questionnaire and chartreview. This information included age, gender, ethnicity,educational level, marital status, work status, smokingstatus, patient’s goal weight, and general health perceptions[using the general health perceptions (GHP) scale from theSF-36] [8]. Current weight was obtained by self report andconfirmed by chart review from clinic patients and selfreport only from support group patients.
We developed a new measure of postsurgical self-management behaviors, as well as measures of two othersalient constructs that were used to investigate mediators ofweight loss. These new measures assessed (1) patientperceptions of benefit from weight loss and (2) patientperceived emotional distress from the new postsurgicaltreatment regimen. We also included in our survey battery apreviously published measure of known reliability andvalidity, assessing patient-reported symptom impact fromobesity, to examine the construct validity of the newmeasures.
Description of Study Measures
Bariatric Surgery Self-management Questionnaire Sevenbehavioral domains were identified from a literature reviewand interviews by a behavioral medicine researcher (GW)of the bariatric surgery team clinicians (two bariatricsurgeons, one bariatric nurse, and one bariatric dietitian).Subscale item content was developed by a process ofconsensus among team members with the goal to createrepresentative and sufficient items for each domain (seeAppendix). The seven bariatric surgery self-managementquestionnaire (BSSQ) behavioral domains were (1) eatingbehaviors (eight EB items); (2) fluid intake (eight FI items);(3) protein intake (three PI items); (4) physical activity(three PA items); (5) dumping syndrome management (fourDSM items); (6) fruit, vegetable, and whole grains intake(three FVW items); and (7) vitamin and mineral supplementintake (four SI items). The BSSQ items were developed toassess self-management behaviors carried out over theprevious week in brief, practical, and behavioral terms thatwould be acceptable to patients. High adherence to thesebehaviors was expected to enhance the likelihood of patientsuccess after surgery in terms of excess weight loss andadequate nutritional status. BSSQ items have a Likertscale format of “never,” “sometimes,” or “always” andsubscale and total scores converted to a 0–100 range for
518 OBES SURG (2008) 18:517–524

ease of interpretation, with higher scores indicating higheradherence.
Lifestyle Distress Questionnaire This 20-item scale wasdeveloped following interviews with our bariatric surgeryclinicians regarding emotional issues reported by patients atclinic follow-up visits that reflected postsurgical treatmentregimen distress. The lifestyle distress questionnaire (LDQ)assesses a range of fears, frustrations, and concernsexperienced over the previous week; for example, “Bur-dened by the constant effort needed to maintain eating andlifestyle changes,” “Annoyed by the need to exercise to loseweight,” and “Sad that I have to give up comfort foods forthose times when I am bored, unhappy, or stressed.” LDQitems have a Likert scale format ranging from 0 (“noproblem”), 1 (“minor problem”), 2 (“moderate problem”),3 (“somewhat serious problem”), through to 4 (“severeproblem”). The LDQ total raw score was converted to a0–100 range, with higher scores indicating higher distress.
Perceived Benefits Questionnaire This 20-item scale wasdeveloped following interviews with experienced bariatricsurgery clinicians to assess a range of perceived benefitsinvolving daily functioning and self perceptions related topostsurgical weight loss; for example, “My self confidencehas improved,” “I am happier with my body shape,” and“My medications have been reduced by my doctor.”Perceived benefits questionnaire (PBQ) benefit items havea Likert scale format ranging from 1 (“not at all”), 2 (“alittle”), to 3 (“a lot”). The PBQ total raw score wasconverted to a 0–100 range, with higher scores indicatinghigher benefits.
Weight-Related Symptom Measure The weight-relatedsymptom measure (WRSM) is a 20-item scale developedfrom interviews with obese patients and overweightindividuals that measures symptoms commonly reportedwith obesity or obesity treatment. It assesses the presenceand “bothersomeness” of obesity symptoms over the
Table 1 Demographic andclinical characteristics of sup-port group survey sample andclinic patient cohort
Clinic patient cohort Support group survey
N 100 200Age (mean ± sd) 42.6±10.6 44.9±9.7Gender (% female) 87.9 84.6Minority representation 18.2 29.0Marital status (%)Married 52,6 61.3Separated 23.2 16.1Never married 24.2 18.6Education level (%)College 41.0 26.8Employment status (%)Full time/part time 76.8 78.0Disability 10.1 12.0Current smoker 2% 11%Presurgical weight (kg, mean ± sd) 137.5±29.4 150.0±39.4Current weight (kg, mean ± sd) 126.9±26.9 100.8±24.5Goal weight (kg, mean ± sd) 73.8±15.2 73.7±13.6Health perceptions (%)Excellent 17.0 26.4Very good 46.0 45.8Good 17.0 26.4Fair 46.0 45.8Poor 0 0.5Social support for weight lossPractical help with lifestyleA lot 82.0 70.6A little 13.0 22.4None 2.0 7.0Someone to listen to concernsA lot 88.9 78.6A little 9.1 16.9None 2.0 4.5
OBES SURG (2008) 18:517–524 519

previous month. Symptoms include shortness of breath,tiredness, pain in joints, and other weight-related problems.Patients endorse “yes” or “no” to each item and thenindicate the degree of “bothersomeness” of each symptomusing a 0–7-point Likert scale format ranging from 0 “not atall” to 7 “a very great deal.” Sound internal (α=0.87) andtest–retest reliability [intraclass correlation coefficient(ICC)=0.83] and evidence of construct validity has beenreported for the WRSM [9].
Statistical Analyses
Demographic, clinical, and questionnaire data were calcu-lated as means and standard deviations or percentages.Univariate comparisons involved Student’s t test for con-tinuous variables and Chi-square with Yates’ continuitycorrection for fourfold tables and Fishers exact test when anexpected cell value was less than 5. Internal consistencyand test–retest reliability of the three new measures (i.e.,BSSQ, LDQ, and PBQ) were measured using coefficientalpha α [10] and the ICC [11]. Correlations among BSSQself-management subscales, LDQ, PBQ, and WRSM scoreswere also calculated using Spearman’s rho (nonparametric)correlation index. Flesch–Kincaid reading (grade) level wascalculated for the three new measures [12] to examine easeof reading.
To explore trends in patient adherence over time forBSSQ behaviors using our cross-sectional data, we classi-fied patients into four time periods since surgery (<6, 6–12,12–18, and >18 months) and calculated seven mean BSSQsubscale scores (0–100) for these categories. Finally, step-wise multiple linear regression [13] was used to identifyvariables that predicted weight loss (presurgical weightminus current weight, WL). Variables tested includedpatient demographics (age, level of education, marital status,and ethnicity), clinical variables (presurgical weight and timesince surgery in months), and psychosocial variables (sevenBSSQ subscales, LDQ, PBQ, WRSM). All variables withp<0.1 were retained. The Statistical Package for the SocialSciences [14] was used for all analyses.
Results
Sample Characteristics
Table 1 provides the demographic and clinical character-istics of the support group sample. The mean time sincesurgery was 14.5±13.9 months (range 1.3 to 109.0 months)The sample was 85% female, mean age was 44.9 years,61% were married, 4% widowed, 17% divorced orseparated, and 19% never married. Eighty one percent werewhite, 8% black, and 10% Hispanic.
Patient mean goal weight was 73.7±13.5 kg, presurgi-cal mean weight was 150.0±39.4 kg (BMI 53.5±11.4),and current mean weight was 100.8±118.4 kg (i.e., BMI36.0±8.3), providing a mean weight loss of 108.9±68.1 kg.Mean reported weight loss (and sample sizes) for the four“time since surgery” categories created to examine trendsover time were 26.5±10.7 kg for the <6-months group(n=51), 41.5±12.4 kg for the 6–12-months group (n=57),66.9±18.1 kg for the 12–18-months group (n=41), and71.5±45.7 kg for the >18-months group (n=49). Thesetranslated into the following mean percentage excess weightloss (%EWL) values: 35.9±13.7, 50.8±15.0, 66.9±41.1, and65.7±16.6%, respectively.
The clinical comparison sample (n=100), surveyed 18.0±3.9 days following surgery was collected with a 99%response rate. The support group sample was not signifi-cantly different from this clinical comparison sample interms of proportion of females, mean age, marital status,employment status, general health perception, level ofpractical and empathic social support, and goal weight(73.8±15.2 kg). However, the support group samplediffered significantly in that education level was lower( p<0.02), prevalence of smokers was higher ( p<0.02), andmean weight prior to surgery was approximately 30 lbhigher (150.0±39.4 vs. 137.5±29.4 kg, p<0.01).
Psychometric Findings
Psychometric analysis results of the seven BSSQ subscalesand total test for internal reliability (coefficient alpha, α)were EB, α=0.83; FI, α=0.81; PI, α=0.74; PA, α=0.70;DSM, α=0.79; FVW, α=0.63; SI, α=0.79; and total score,α=0.83. Psychometric results for the LDQ were α=0.92,and those for the PBQ were α=0.78. Two-week test–retestreliabilities (ICC) for the BSSQ subscales were EB,ICC=0.72; FI, ICC=0.68; PI, ICC=0.60; PA, ICC=0.54;DSM, ICC=0.66; FVW, ICC=0.46; SI, ICC=0.66; and totalscore, ICC=0.71. Test–retest results for the LDQ wereICC=0.86, and those for the PBQ were ICC=0.64. Flesch–Kincaid reading level of all three measures was in thegrade 7th to 8th grade range.
BSSQ construct validity was examined by the patternof intercorrelations among individual BSSQ subscales, 19of 21 correlations were significant (r=0.15, p<0.05 tor=0.39, p<0.01). Results of the correlations among theBSSQ total test and the LDQ, PBQ, and WRSM ques-tionnaires and WL (weight loss) showed the total testcorrelated significantly with LDQ (r=−0.22, p<0.01), PBQ(r=0.31, p<0.01), and WRSM (r=−0.17, p<0.05) but notWL (r=−0.08, ns).
Results of the BSSQ subscale correlations with theLDQ distress measure showed that EB, DSM, and PIsubscales were significantly correlated with LDQ (r=−0.22
520 OBES SURG (2008) 18:517–524
to r=−0.26, all p<0.01) but FI, PA, SI, and FVW were not.BSSQ subscales EB (r=0.33, p<0.01) and PA (r=0.23,p<0.01) correlated significantly with PBQ benefits but notFI, DSM, SI, FVW, or PI.
Behavior Adherence Findings
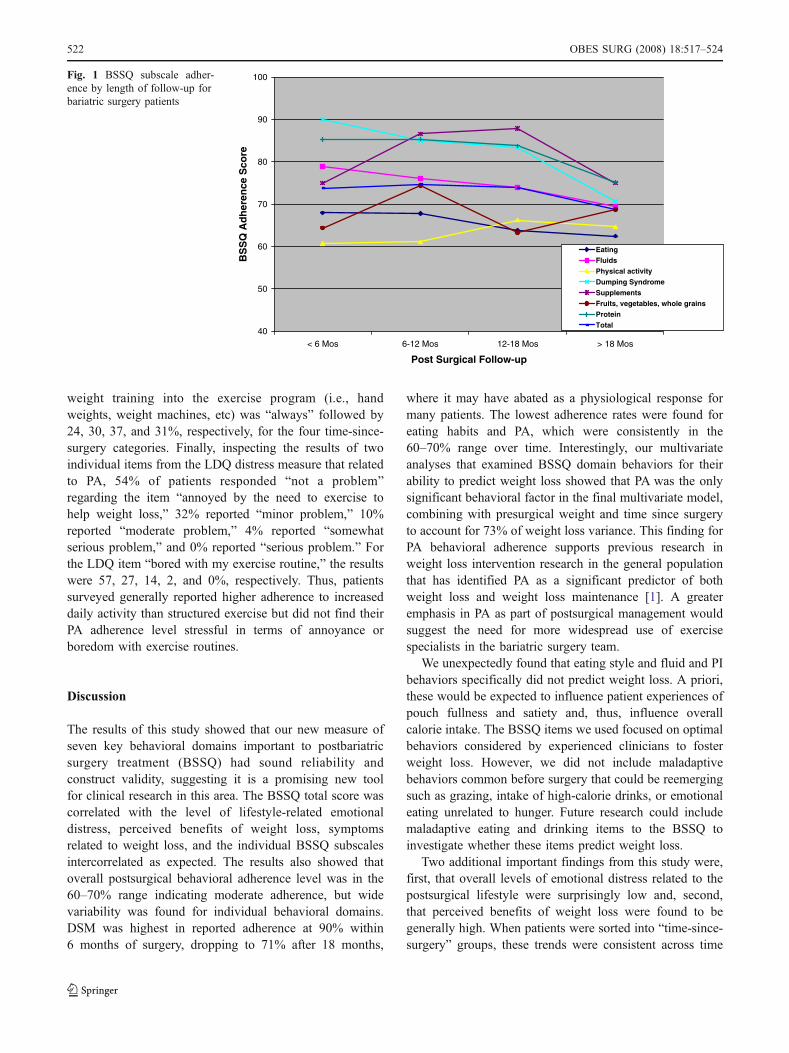
Mean BSSQ self-management behavior results showed thatthe mean total BSSQ adherence score was consistently inthe 60–70% range over time. Looking at subscale leveldata, the mean BSSQ subscale scores ranged widely from61 to 90%, with highest adherence reported for SI at 90% at<6 months dropping to 71% at >18 months, and the lowestwas for the PA subscale score, which ranged from 61 to65%.
Results for the LDQ distress measure showed that meanLDQ (0–100 range) scores for the four duration-since-surgery groups were consistently low over time sincesurgery categories, as follows: 19.5±12.1 (<6 months),20.4±13.6 (6–12 months), 20.9±12.9 (12–18 months), and25.7±19.7 (>18 months). However, inspecting individualitem scores, 39% of patients reported weight regain fears asbeing a “somewhat serious” or “serious problem,” 18%reported a similar problem with fear about pouch stretching,and 11% reported being “afraid that eating somethingwould make them nauseous or provoke pain.” Thus,whereas overall distress was consistently low, a few issueswere considered serious by a minority of patients.
Mean PBQ (benefit) scores (0–100 range) found for thetime-since-surgery category were: 72.7±19.3, 82.6±17.3,82.6±17.3, and 91.8±9.8, indicating an early strong levelof perceived benefit associated with a mean 26.2-kg loss forthe <6-months group that was increased over timecategories to a high in the 90% range at >18 months, whena mean of 71.5 kg had been lost (Table 2).
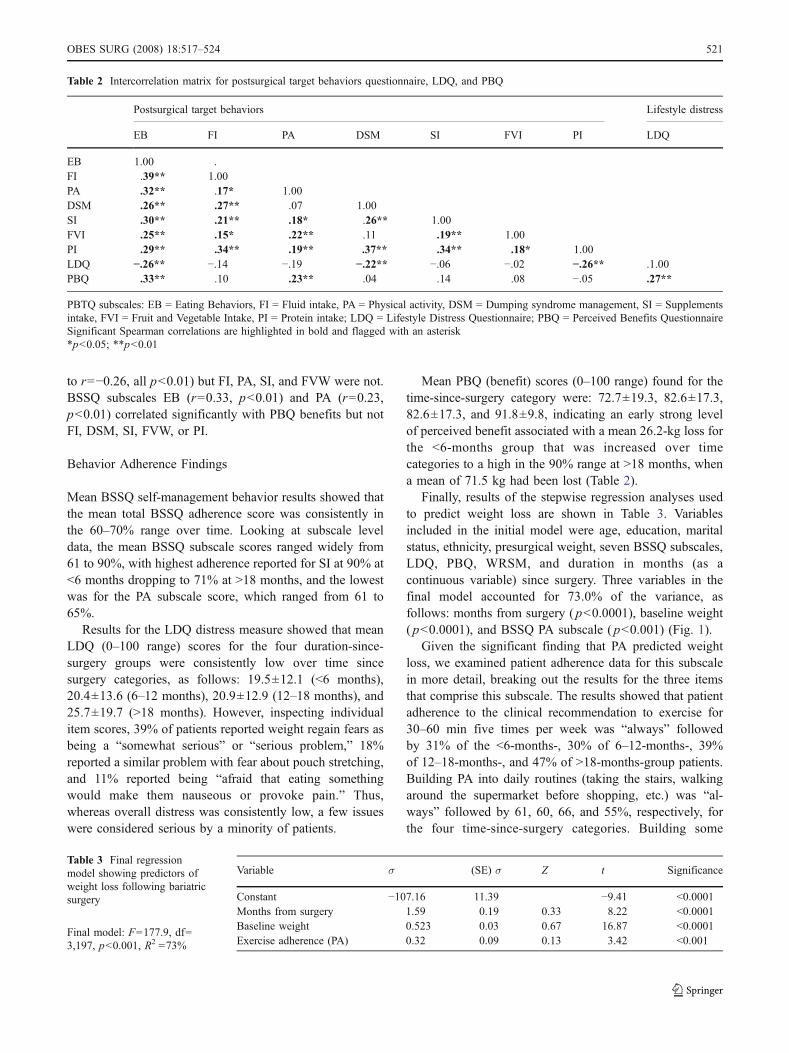
Finally, results of the stepwise regression analyses usedto predict weight loss are shown in Table 3. Variablesincluded in the initial model were age, education, maritalstatus, ethnicity, presurgical weight, seven BSSQ subscales,LDQ, PBQ, WRSM, and duration in months (as acontinuous variable) since surgery. Three variables in thefinal model accounted for 73.0% of the variance, asfollows: months from surgery ( p<0.0001), baseline weight( p<0.0001), and BSSQ PA subscale ( p<0.001) (Fig. 1).
Given the significant finding that PA predicted weightloss, we examined patient adherence data for this subscalein more detail, breaking out the results for the three itemsthat comprise this subscale. The results showed that patientadherence to the clinical recommendation to exercise for30–60 min five times per week was “always” followedby 31% of the <6-months-, 30% of 6–12-months-, 39%of 12–18-months-, and 47% of >18-months-group patients.Building PA into daily routines (taking the stairs, walkingaround the supermarket before shopping, etc.) was “al-ways” followed by 61, 60, 66, and 55%, respectively, forthe four time-since-surgery categories. Building some
Table 2 Intercorrelation matrix for postsurgical target behaviors questionnaire, LDQ, and PBQ
Postsurgical target behaviors Lifestyle distress
EB FI PA DSM SI FVI PI LDQ
EB 1.00 .FI .39** 1.00PA .32** .17* 1.00DSM .26** .27** .07 1.00SI .30** .21** .18* .26** 1.00FVI .25** .15* .22** .11 .19** 1.00PI .29** .34** .19** .37** .34** .18* 1.00LDQ −.26** −.14 −.19 −.22** −.06 −.02 −.26** .1.00PBQ .33** .10 .23** .04 .14 .08 −.05 .27**
PBTQ subscales: EB = Eating Behaviors, FI = Fluid intake, PA = Physical activity, DSM = Dumping syndrome management, SI = Supplementsintake, FVI = Fruit and Vegetable Intake, PI = Protein intake; LDQ = Lifestyle Distress Questionnaire; PBQ = Perceived Benefits QuestionnaireSignificant Spearman correlations are highlighted in bold and flagged with an asterisk*p<0.05; **p<0.01
Variable σ (SE) σ Z t Significance
Constant −107.16 11.39 −9.41 <0.0001Months from surgery 1.59 0.19 0.33 8.22 <0.0001Baseline weight 0.523 0.03 0.67 16.87 <0.0001Exercise adherence (PA) 0.32 0.09 0.13 3.42 <0.001
Table 3 Final regressionmodel showing predictors ofweight loss following bariatricsurgery
Final model: F=177.9, df=3,197, p<0.001, R2 =73%
OBES SURG (2008) 18:517–524 521
weight training into the exercise program (i.e., handweights, weight machines, etc) was “always” followed by24, 30, 37, and 31%, respectively, for the four time-since-surgery categories. Finally, inspecting the results of twoindividual items from the LDQ distress measure that relatedto PA, 54% of patients responded “not a problem”regarding the item “annoyed by the need to exercise tohelp weight loss,” 32% reported “minor problem,” 10%reported “moderate problem,” 4% reported “somewhatserious problem,” and 0% reported “serious problem.” Forthe LDQ item “bored with my exercise routine,” the resultswere 57, 27, 14, 2, and 0%, respectively. Thus, patientssurveyed generally reported higher adherence to increaseddaily activity than structured exercise but did not find theirPA adherence level stressful in terms of annoyance orboredom with exercise routines.
Discussion
The results of this study showed that our new measure ofseven key behavioral domains important to postbariatricsurgery treatment (BSSQ) had sound reliability andconstruct validity, suggesting it is a promising new toolfor clinical research in this area. The BSSQ total score wascorrelated with the level of lifestyle-related emotionaldistress, perceived benefits of weight loss, symptomsrelated to weight loss, and the individual BSSQ subscalesintercorrelated as expected. The results also showed thatoverall postsurgical behavioral adherence level was in the60–70% range indicating moderate adherence, but widevariability was found for individual behavioral domains.DSM was highest in reported adherence at 90% within6 months of surgery, dropping to 71% after 18 months,
where it may have abated as a physiological response formany patients. The lowest adherence rates were found foreating habits and PA, which were consistently in the60–70% range over time. Interestingly, our multivariateanalyses that examined BSSQ domain behaviors for theirability to predict weight loss showed that PA was the onlysignificant behavioral factor in the final multivariate model,combining with presurgical weight and time since surgeryto account for 73% of weight loss variance. This finding forPA behavioral adherence supports previous research inweight loss intervention research in the general populationthat has identified PA as a significant predictor of bothweight loss and weight loss maintenance [1]. A greateremphasis in PA as part of postsurgical management wouldsuggest the need for more widespread use of exercisespecialists in the bariatric surgery team.
We unexpectedly found that eating style and fluid and PIbehaviors specifically did not predict weight loss. A priori,these would be expected to influence patient experiences ofpouch fullness and satiety and, thus, influence overallcalorie intake. The BSSQ items we used focused on optimalbehaviors considered by experienced clinicians to fosterweight loss. However, we did not include maladaptivebehaviors common before surgery that could be reemergingsuch as grazing, intake of high-calorie drinks, or emotionaleating unrelated to hunger. Future research could includemaladaptive eating and drinking items to the BSSQ toinvestigate whether these items predict weight loss.
Two additional important findings from this study were,first, that overall levels of emotional distress related to thepostsurgical lifestyle were surprisingly low and, second,that perceived benefits of weight loss were found to begenerally high. When patients were sorted into “time-since-surgery” groups, these trends were consistent across time
40
50
60
70
80
90
100
< 6 Mos 6-12 Mos 12-18 Mos > 18 Mos
Post Surgical Follow-up
BS
SQ
Ad
her
ence
Sco
reEating
FluidsPhysical activity
Dumping Syndrome
SupplementsFruits, vegetables, whole grains
ProteinTotal
Fig. 1 BSSQ subscale adher-ence by length of follow-up forbariatric surgery patients
522 OBES SURG (2008) 18:517–524

for both distress and perceived benefits. Whether the lowdistress levels found were related to the moderate behav-ioral adherence reported by the patients or were a functionof the practical and emotional support received byattendance at the support groups should be further explored.High levels (70%) of perceived benefit from weight losswere reported within 6 months of surgery when an averageof 25.9 kg had been lost, rising to 90% perceived benefitscore at 18 months when an average of 71.3 kg had beenlost. Future studies of patients not attending support groupsor representative patient cohorts followed prospectively inlongitudinal designs would be necessary to explore thisissue further.
There were a number of limitations to the study designthat limit the generalizability of the findings and suggestcaution in interpretation. First, patient weights were self-reported by support-group patients and could be biased [15,16]. Second, whereas an almost perfect response rate wasachieved for the support group survey and comparison ofthe demographic and clinical profile with a consecutiveseries of clinic patients showed that the support group wassimilar to the clinic sample in many respects, one notablefinding was that the support-group patients were 13.6 kgheavier presurgery and had higher rates of smoking (11 vs.3%). Thus, these findings suggest some selection bias ispresent. A retrospective analysis of our hospital surgicaldatabase showed that only 16% of eligible patients who hadbeen operated on since 1999 were attending our supportgroups during the 3-month survey period, indicatingsignificant potential bias. A number of published studiespoint to the current difficulties in locating bariatric surgerypatients over time [2, 17–19], and a recent review of trendsin the area identified short-term and incomplete follow-uprates as one of the key issues facing bariatric surgeryoutcomes research [20]. We also caution that our classifi-cation of support group patients into “time-since-surgery”categories was based on a sorting of cross-sectional dataand, thus, did not reflect a true long-term trend. Futureresearch could involve replication of our findings with aprospective, longitudinal design to examine weight loss,adherence to behavioral recommendations, lifestyle dis-tress, and benefits of weight loss with a large, representa-tive patient population.
Appendix: Bariatric Surgery Self-managementBehaviors Questionnaire Items
Eating Behaviors Subscale
1. I ate a minimum of 5 mini meals or snacks during theday
2. I ate slowly, putting my utensils or food down betweenbites
3. It took about 20–30 minutes for me to eat my meals4. I chewed my food until it was a pureed consistency
like baby food5. I used a bread and butter plate or dessert plate instead
of a regular-sized plate for my meals6. I checked for feeling of fullness after every bite7. I stopped eating immediately if I had any feelings of
fullness or discomfort8. I used a baby spoon, fork, and knife instead of regular
sized ones
Fluid Intake Subscale
9. I drank 48 ounces (six 8 oz glasses) or more of fluidsduring the day
10. I only drank water, sugar-free beverages, skim milk,or 1% milk
11. I sipped drinks slowly putting my drink down betweensips
12. I avoided using a straw to drink13. I carried a suitable drink with me at all times14. I did not rely on feeling thirsty as a signal to drink15. I checked my urine through the day to make sure it
was pale yellow-to-clear in color showing good fluidintake
16. I drank 30 minutes before my meal and waited until30 minutes after my meal so that I separated my fluidsfrom my solid foods
Physical Activity Subscale
17. I got 30–60 minutes of exercise 5 days or more in thepast week (e.g., walking, exercise equipment at home,health club, class, etc.)
18. I built some exercise into my daily routines (I took thestairs, walked around the supermarket or mall beforeshopping, etc.)
19. I built some weight training into my exercise program(hand weights, climbing stairs, weight machines, etc)
Dumping Syndrome Management Subscale
20. I read nutrition fact panels on food labels to look forhigh levels of sugar in foods
21. I avoided foods and beverages with 15 grams (3 tsp)of sugar or more a serving
22. I avoided foods and beverages with sugar listed as 1of the first 3 ingredients (glucose, maltose, dextrose,
OBES SURG (2008) 18:517–524 523

fructose, honey, molasses, corn syrup, brown sugar,cane sugar, confectionary sugar)
23. I avoided sugar alcohols (mannitol, sorbitol, xylitol,lactitol) by looking at food labels as these causecramping and diarrhea
Supplement Intake Subscale
24. I took a multi-vitamin with minerals tablet every day25. I took 1,000 to 1,500 mg of calcium citrate or calcium
carbonate with vitamin D every day26. I took a B-complex vitamin supplement every day27. I took my vitamin/calcium pills 4 hours or more apart
to maximize absorption
Fruits, Vegetables, and Whole Grains Subscale
28. I ate at least 5 fruits and vegetables every day29. I mostly chose whole grain breads, cereals, and
crackers30. I mostly chose brightly colored fruits and vegetables
(yellow, green, red, orange, blue, purple)
Protein Intake Subscale
31. I ate 60–80 grams (2–3 oz) of protein every day (fish,eggs, chicken, turkey, beef, pork, ham, milk, peanutbutter, beans, soy, tofu, lentils, cheese, nuts, yogurt,skim or 1% milk, or low sugar protein bars andshakes)
32. I ate the protein on my plate first during meals andsnacks
33. I read food labels and chose the foods highest inprotein and lowest in sugar
References
1. Wing R, Marinilli Pinto A, Niemeier H. Maintenance: the ultimategoal. In: Apovian CM, Lenders CM, editors. A clinical guide for
management of overweight and obese children and adults.London: CRC Press; 2007.
2. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: asystematic review and meta-analysis. JAMA. 2004;292:1724–37.
3. Andrews G, LeMont D, Myers S. Caring for the surgical weightloss patient. Sierra Madre: Wheat Field Publishers; 2003.
4. McMahon M, Sarr M, Clark M, et al. Clinical management afterbariatric surgery: value of a multidisciplinary team. Mayo ClinProc. 2006;81:S34–45.
5. Colles S, Dixon J. Night eating syndrome: impact on bariatricsurgery. Obes Surg. 2006;16:811–20.
6. Saunders R. Grazing: a high risk behavior. Obes Surg.2004;14:98–102.
7. Elkins G, Whitfield P, Marcus J. Non-compliance with behavioralrecommendations following bariatric surgery. Obes Surg.2005;15.
8. Ware J, Kosinski M. SF-36 Physical and mental health summaryscales: a manual for users of version 1. Lincoln: Quality Metric;2001.
9. Patrick D, Bushnell D, Rothman M. Performance of two self-report measures for evaluating obesity and weight loss. Obes Res.2004;12:48–57.
10. Cronbach L. Coefficient alpha and the internal structure of tests.Psychometrika. 1951;16:297–334.
11. Streiner D, Norman G. Health measurement scales: a practicalguide to their development and use. Oxford: Oxford UniversityPress; 1989.
12. Kincaid J, Fishburne R, Rogers R. Derivation of new readabilityformulas (Automated Readability Index, Fog Count and FleschReading Ease Formula) for Navy enlisted personnel. Memphis:Naval Technical Training, U. S. Naval Air Station; 1975.
13. Snedecor G, Cochran W. Multiple linear regression. Statisticalmethods. 8th ed. Ames: Iowa State University Press; 1989.
14. SPSS. Statistical Package for the Social Sciences. 10.0 version.Chicago: SPSS; 1999.
15. Kuczmarski M, Kuczmarski R, Najjar M. Effects of age onvalidity of self-reported height, weight, and body mass index:findings from the Third National Health and Nurtition Examina-tion Survey 1988–1994. J Am Diet Assoc. 2001;101:28–34.
16. Nyholm M, Gullberg B, Merio J. The validity of obesity based onself-reported weight and height: implications for populationsstudies. Obesity. 2007;15:197–208.
17. Renquist K, Jeng G, Mason E. Calculating follow-up rates. ObesSurg. 1992;2:361–7.
18. Monteforte J, Turkelson C. Bariatric surgery for morbid obesity.Obes Surg. 2000;10:391–401.
19. Christou N, Look D, Maclean L. Weight gain after short and longterm limb gastric bypass in patients followed for longer than10 years. Ann Surg. 2006;244:734–40.
20. Courcoulas A, Flum D. Filling in the gaps in bariatric surgeryresearch. JAMA. 2005;294:1957–60.
524 OBES SURG (2008) 18:517–524


















