Phenotype-Genotype Correlations and Estimated …jasn.asnjournals.org/content/26/10/2559.full.pdffor...
12
CLINICAL RESEARCH www.jasn.org Phenotype-Genotype Correlations and Estimated Carrier Frequencies of Primary Hyperoxaluria Katharina Hopp,* Andrea G. Cogal,* Eric J. Bergstralh, † Barbara M. Seide,* Julie B. Olson,* Alicia M. Meek,* John C. Lieske,* Dawn S. Milliner,* ‡ and Peter C. Harris,* § on behalf of the Rare Kidney Stone Consortium *Division of Nephrology and Hypertension, † Division of Biomedical Statistics and Informatics, § Department of Biochemistry and Molecular Biology, and ‡ Division of Pediatric Nephrology, Mayo Clinic, Rochester, Minnesota ABSTRACT Primary hyperoxaluria (PH) is a rare autosomal recessive disease characterized by oxalate accumulation in the kidneys and other organs. Three loci have been identified: AGXT (PH1), GRHPR (PH2), and HOGA1 (PH3). Here, we compared genotype to phenotype in 355 patients in the Rare Kidney Stone Consortium PH registry and calculated prevalence using publicly available whole-exome data. PH1 (68.4% of families) was the most severe PH type, whereas PH3 (11.0% of families) showed the slowest decline in renal function but the earliest symp- toms. A group of patients with disease progression similar to that of PH3, but for whom no mutation was detected (11.3% of families), suggested further genetic heterogeneity. We confirmed that the AGXT p.G170R mistargeting allele resulted in a milder PH1 phenotype; however, other potential AGXT mistargeting alleles caused more severe (fully penetrant) disease. We identified the first PH3 patient with ESRD; a homozygote for two linked, novel missense mutations. Population analysis suggested that PH is an order of magnitude more common than determined from clinical cohorts (prevalence, approximately 1:58,000; carrier frequency, approx- imately 1:70). We estimated PH to be approximately three times less prevalent among African Americans than among European Americans because of a limited number of common European origin alleles. PH3 was pre- dicted to be as prevalent as PH1 and twice as common as PH2, indicating that PH3 (and PH2) cases are under- diagnosed and/or incompletely penetrant. These results highlight a role for molecular analyses in PH diagnostics and prognostics and suggest that wider analysis of the idiopathic stone-forming population may be beneficial. J Am Soc Nephrol 26: 2559–2570, 2015. doi: 10.1681/ASN.2014070698 The primary hyperoxalurias (PHs) are rare autosomal recessive inborn errors of hepatic glyoxylate metabo- lism characterized by oxalate overproduction and elevated excretion. 1–3 Calcium oxalate oversaturation leads to recurrent urolithiasis and/or nephrocalci- nosis, with reduced renal elimination due to renal damage resulting in oxalate deposition in all tissues (systemic oxalosis). 1,2,4,5 The estimated PH prevalence is ,3:1,000,000, but in approximately 20%–50% of cases severe renal in- sufficiency, or recurrent disease after transplantation, occurs before diagnosis. 3,6–8 Underdiagnosis proba- bly occurs because of the phenotypic heterogeneity of PH, ranging from infantile nephrocalcinosis with kidney failure to only occasional stone formation (similar to idiopathic stone disease), and unfamiliarity with this rare monogenic disorder. 3,9 Three genetic forms of PH have been defined: PH1–3, associated with mutations to AGXT , GRHPR, and HOGA1, respectively. 10–12 PH1, caused by deficiency of the liver-specific peroxisomal enzyme alanine-glyoxylate aminotrans- ferase (AGT), is the most severe PH form, accounting Received July 22, 2014. Accepted December 13, 2014. K.H. and A.G.C. contributed equally to this work. Published online ahead of print. Publication date available at www.jasn.org. Correspondence: Dr. Peter C. Harris, Division of Nephrology and Hypertension, Mayo Clinic, 200 First Street SW, Rochester, MN 55905. Email: [email protected] Copyright © 2015 by the American Society of Nephrology J Am Soc Nephrol 26: 2559–2570, 2015 ISSN : 1046-6673/2610-2559 2559
-
Upload
nguyentuyen -
Category
Documents
-
view
219 -
download
1
Transcript of Phenotype-Genotype Correlations and Estimated …jasn.asnjournals.org/content/26/10/2559.full.pdffor...

CLINICAL RESEARCH www.jasn.org
Phenotype-Genotype Correlations and EstimatedCarrier Frequencies of Primary Hyperoxaluria
Katharina Hopp,* Andrea G. Cogal,* Eric J. Bergstralh,† Barbara M. Seide,*Julie B. Olson,* Alicia M. Meek,* John C. Lieske,* Dawn S. Milliner,*‡ andPeter C. Harris,*§ on behalf of the Rare Kidney Stone Consortium
*Division of Nephrology and Hypertension, †Division of Biomedical Statistics and Informatics, §Department ofBiochemistry and Molecular Biology, and ‡Division of Pediatric Nephrology, Mayo Clinic, Rochester, Minnesota
ABSTRACTPrimary hyperoxaluria (PH) is a rare autosomal recessive disease characterized by oxalate accumulation in thekidneys andother organs. Three loci havebeen identified:AGXT (PH1),GRHPR (PH2), andHOGA1 (PH3).Here,we compared genotype to phenotype in 355 patients in the Rare Kidney Stone Consortium PH registry andcalculated prevalence using publicly available whole-exome data. PH1 (68.4% of families) was the most severePH type, whereas PH3 (11.0% of families) showed the slowest decline in renal function but the earliest symp-toms. A group of patients with disease progression similar to that of PH3, but for whom no mutation wasdetected (11.3% of families), suggested further genetic heterogeneity. We confirmed that the AGXT p.G170Rmistargeting allele resulted in a milder PH1 phenotype; however, other potential AGXT mistargeting allelescaused more severe (fully penetrant) disease. We identified the first PH3 patient with ESRD; a homozygote fortwo linked, novel missense mutations. Population analysis suggested that PH is an order of magnitude morecommon thandetermined fromclinical cohorts (prevalence, approximately 1:58,000; carrier frequency, approx-imately 1:70). We estimated PH to be approximately three times less prevalent among African Americans thanamong European Americans because of a limited number of common European origin alleles. PH3 was pre-dicted to be as prevalent as PH1 and twice as common as PH2, indicating that PH3 (and PH2) cases are under-diagnosed and/or incompletely penetrant. These results highlight a role for molecular analyses in PH diagnosticsand prognostics and suggest that wider analysis of the idiopathic stone-forming population may be beneficial.
J Am Soc Nephrol 26: 2559–2570, 2015. doi: 10.1681/ASN.2014070698
The primary hyperoxalurias (PHs) are rare autosomalrecessive inborn errors of hepatic glyoxylate metabo-lism characterized by oxalate overproduction andelevated excretion.1–3 Calcium oxalate oversaturationleads to recurrent urolithiasis and/or nephrocalci-nosis, with reduced renal elimination due to renaldamage resulting in oxalate deposition in all tissues(systemic oxalosis).1,2,4,5
The estimated PHprevalence is,3:1,000,000, butin approximately 20%–50% of cases severe renal in-sufficiency, or recurrent disease after transplantation,occurs before diagnosis.3,6–8 Underdiagnosis proba-bly occurs because of the phenotypic heterogeneityof PH, ranging from infantile nephrocalcinosis withkidney failure to only occasional stone formation(similar to idiopathic stone disease), andunfamiliaritywith this rare monogenic disorder.3,9 Three genetic
forms of PH have been defined: PH1–3, associatedwith mutations to AGXT, GRHPR, and HOGA1,respectively.10–12
PH1, caused by deficiency of the liver-specificperoxisomal enzyme alanine-glyoxylate aminotrans-ferase (AGT), is themost severe PH form, accounting
Received July 22, 2014. Accepted December 13, 2014.
K.H. and A.G.C. contributed equally to this work.
Published online ahead of print. Publication date available atwww.jasn.org.
Correspondence: Dr. Peter C. Harris, Division of Nephrologyand Hypertension, Mayo Clinic, 200 First Street SW, Rochester,MN 55905. Email: [email protected]
Copyright © 2015 by the American Society of Nephrology
J Am Soc Nephrol 26: 2559–2570, 2015 ISSN : 1046-6673/2610-2559 2559

for about 80% of genetically characterized patients.1,3,13 It canmanifest as infantile oxalosis, resulting in early death,14,15 but amore typical course is recurrent urolithiasis with progressivenephrocalcinosis and ESRD by 20–30 years of age.5,16–18 A totalof 178 AGXT mutations have been described; the three mostcommon, p.G170R, c.33dupC, and p.I244T, account for approx-imately 30%, 11%, and 6%ofAGXTmutant alleles, respectively;p.I244T is common in Spanish/North African populations.19–24
AGXT p.G170R is associated with mistargeting of the AGThomodimer to mitochondria and the associated unmaskingof the p.P11L mitochondrial targeting sequence (MTS) of the“minor” p.P11L/p.I340Mhaplotype.25–29 Patients with p.G170Rhavemilder renal disease and respond to pyridoxine treatment, acofactor that reduces enzyme mistargeting.25,27,28,30–32 The mu-tations p.G41R, p.F152I and p.I244T also unmask the MTS ifpresent on the minor allele, and anecdotal evidence suggests thatpatientswith p.F152I benefit frompyridoxine treatment.29,30,32,33
Detecting genotype-phenotype correlations beyond the minorallele requiring (MiR) variants is complicated by the allelic het-erogeneity andmarked phenotypic variability, both intrafamilialand amongunrelated patients with the same allelic combination,suggesting environmental and modifier gene roles.5,25
PH2 is generally less severe than PH1 but with a similar ageat first symptoms.1,2,4 It is caused by deficiency of glyoxylatereductase/hydroxypyruvate reductase (GR/HPR), and accountsfor about 10% of genetically characterized PH cases.1,34,35 Todate, 28 different mutations have been described, withc.103delG and c.403_404+2delAAGT accounting for 37% and18% of mutant alleles, respectively; c.403_404+2delAAGT ispredominantly a mutation found in Asians.4,22,35
PH3 is the least severe form, with good preservation ofkidney function in most patients. The typical presentation isrecurrent urolithiasis and marked hypercalciuria in the firstdecade, but less active stone formation later.1,2,36,37 HOGA1encodes the liver-specific mitochondrial enzyme 4-hydroxy-2-oxogluterate aldolase (HOGA), and mutations causehydroxy-2-oxogluterate aldolase build-up, inhibiting GR/HPRfunction.11,38 PH3 accounts for approximately 10%of geneticallycharacterized cases, with some carriers found to be idiopathicstone formers, suggesting sensitivity to haploinsufficiency.1,39
There are 19 described mutations with c.700+5G.Taccountingfor about 50% of allHOGA1 alleles; p.E315del is found predom-inantly in Ashkenazi Jews.22,36,37,39 No allelic correlations havebeen established for PH2 or PH3.
Here, we evaluated genotype-phenotype correlations at thegenic and allelic level using a large collection of PH patientsfrom theRareKidney StoneConsortiumPrimaryHyperoxaluriaregistry (RKSC PH registry). In addition, we used publicly avail-able whole-exome sequencing data to provide population-basedestimates of PH prevalence. Overall, these studies provide newinsight into PH phenotypes and the significance of particularalleles. In addition, they indicate a carrier rate far higher thanestimated from clinical populations, suggesting a significantlevel of underdiagnosis and/or incomplete penetrance/variableexpressivity.
RESULTS
Genic and Allelic Analysis of the RKSC PH RegistryPopulationWe mutation-screened the three known PH loci in 301 PHfamilies (355 patients) using Sanger sequencing. Of these, 68.4%(206 pedigrees, 247 patients) were PH1, 9.3% (28 pedigrees,35 patients) were PH2, and 11.0% (33 pedigrees, 38 patients)were PH3. Two mutant alleles were detected in each case. Theremaining 11.3% (34 pedigrees, 35 patients) had a clinicalphenotype consistentwithPHaccording to theRKSCPHregistryentry criteria (Concise Methods), yet no mutation was detected(NMD) in the known genes.
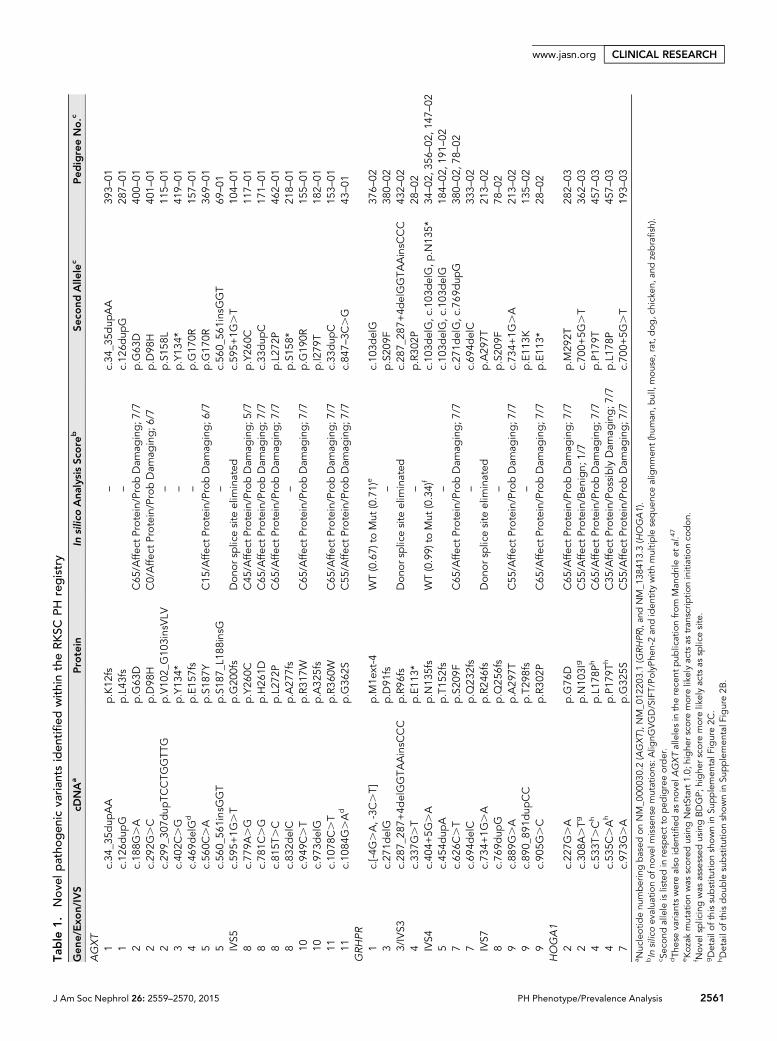
In total, we identified 121 different mutations within thiscohort (83AGXT, 21GRHPR, and 17HOGA1), of which 36 havenot been previously described in the Human Gene MutationDatabase (HGMD 2013.3 Professional) or the PHMutation Da-tabase22 (PHMD; 18 AGXT, 13 GRHPR, and 5 HOGA1) (Sup-plemental Figure 1, Table 1). One of the novel mutations, GRHPRc.[-4G.A, -3C.T], is upstream of the transcription start codongenerating a frameshifted novel start site with a stronger Kozakconsensus (Supplemental Figure 2A).
The genotypic and allelic breakdown varied considerablybetween the different genes (Figure 1). For instance, 50.0% ofPH2 pedigrees contained two truncating mutations, an alleliccombination that accounted for only the minority of PH1genotypes (14.1%) and was absent in PH3 (Figure 1A).GRHPR was more prone to frameshifting InDels (insertion,duplication, deletion, or insertion+deletion), accounting for44.6% of all mutant alleles, whereas most AGXT mutationswere missense (67.0%) (Figure 1B). These enrichments weredriven by common mutations; the AGXTmistargeting changep.G170R was found in 50.5% of PH1 families and GRHPRc.103delG in 35.7% of PH2 families. HOGA1 showed consid-erably less allelic heterogeneity with the two most commonalleles (c.700+5G.Tand p.E315del), accounting for 74.2% ofthe total (Figure 1B).
Genotype-Phenotype Comparisons between PH TypesWithin our cohort, themedian (25th, 75thpercentiles) age at PHsymptomonsetwas5.2 years (1.7, 15years) andageat last contactwas 21 years (9, 43 years). To date, 22 of 355 patients have died,and 139 developed ESRD. Renal survival analysis showed thatPH1 patients were more likely to reach ESRD and at an earlierage, followed by PH2 and then PH3 (Figure 2A).1,2 No NMDpatient experienced ESRD by age 60 years (Figure 2A), althoughtwo had later renal failure. Patients with PH1 had a higher in-cidence of nephrocalcinosis and higher urine oxalate, lower cal-cium, and lower citrate levels (Table 2). Patients with PH3 hadearlier onset of symptoms than did those with PH1 or PH2, buthad lower urine oxalate excretion and, in general, more slowlyprogressive disease. The NMD patients were the latest to showsymptoms and had oxalate levels similar to those in patients withPH3. Elevated glycolate or L-glycerate levels indicated PH1 orPH2, respectively (Table 2).4,5
2560 Journal of the American Society of Nephrology J Am Soc Nephrol 26: 2559–2570, 2015
CLINICAL RESEARCH www.jasn.org
Table
1.Nov
elpatho
gen
icva
rian
tsiden
tified
withintheRKSC
PHregistry
Gen
e/Exo
n/IVS
cDNAa
Protein
Insilico
Ana
lysisSc
ore
bSe
cond
Alle
lec
Ped
igreeNo.c
AGXT
1c.34
_35d
upAA
p.K12
fs–
c.34
_35d
upAA
393–
011
c.12
6dup
Gp.L43
fs–
c.12
6dup
G28
7–01
2c.18
8G.A
p.G
63D
C65
/Affe
ctProtein/ProbDam
aging;7
/7p.G
63D
400–
012
c.29
2G.C
p.D
98H
C0/Affe
ctProtein/ProbDam
aging;6
/7p.D
98H
401–
012
c.29
9_30
7dup
TCCTG
GTT
Gp.V10
2_G10
3insVLV
–p.S15
8L11
5–01
3c.40
2C.G
p.Y13
4*–
p.Y13
4*41
9–01
4c.46
9delG
dp.E15
7fs
–p.G
170R
157–
015
c.56
0C.A
p.S18
7YC15
/Affe
ctProtein/ProbDam
aging;6
/7p.G
170R
369–
015
c.56
0_56
1insGGT
p.S18
7_L1
88insG
–c.56
0_56
1insGGT
69–01
IVS5
c.59
5+1G
.T
p.G
200fs
Don
ors
plicesite
elim
inated
c.59
5+1G
.T
104–
018
c.77
9A.G
p.Y26
0CC45
/Affe
ctProtein/ProbDam
aging;5
/7p.Y26
0C11
7–01
8c.78
1C.G
p.H26
1DC65
/Affe
ctProtein/ProbDam
aging;7
/7c.33
dup
C17
1–01
8c.81
5T.C
p.L27
2PC65
/Affe
ctProtein/ProbDam
aging;7
/7p.L27
2P46
2–01
8c.83
2delC
p.A27
7fs
–p.S15
8*21
8–01
10c.94
9C.T
p.R31
7WC65
/Affe
ctProtein/ProbDam
aging;7
/7p.G
190R
155–
0110
c.97
3delG
p.A32
5fs
p.I2
79T
182–
0111
c.10
78C.T
p.R36
0WC65
/Affe
ctProtein/ProbDam
aging;7
/7c.33
dup
C15
3–01
11c.10
84G.Ad
p.G
362S
C55
/Affe
ctProtein/ProbDam
aging;7
/7c.84
7–3C
.G
43–01
GRHPR
1c.[-4
G.A,-3C
.T]
p.M
1ext-4
WT(0.67)
toMut
(0.71)
ec.10
3delG
376–
023
c.27
1delG
p.D
91fs
–p.S20
9F38
0–02
3/IVS3
c.28
7_28
7+4d
elGGTA
AinsC
CC
p.R96
fsDon
ors
plicesite
elim
inated
c.28
7_28
7+4d
elGGTA
AinsC
CC
432–
024
c.33
7G.T
p.E11
3*–
p.R30
2P28
–02
IVS4
c.40
4+5G
.A
p.N
135fs
WT(0.99)
toMut
(0.34)
fc.10
3delG,c
.103
delG,p
.N13
5*34
–02
,356
–02
,147
–02
5c.45
4dup
Ap.T15
2fs
–c.10
3delG,c
.103
delG
184–
02,1
91–02
7c.62
6C.T
p.S20
9FC65
/Affe
ctProtein/ProbDam
aging;7
/7c.27
1delG,c
.769
dup
G38
0–02
,78–
027
c.69
4delC
p.Q
232fs
–c.69
4delC
333–
02IVS7
c.73
4+1G
.A
p.R24
6fs
Don
ors
plicesite
elim
inated
p.A29
7T21
3–02
8c.76
9dup
Gp.Q
256fs
–p.S20
9F78
–02
9c.88
9G.A
p.A29
7TC55
/Affe
ctProtein/ProbDam
aging;7
/7c.73
4+1G
.A
213–
029
c.89
0_89
1dup
CC
p.T29
8fs
–p.E11
3K13
5–02
9c.90
5G.C
p.R30
2PC65
/Affe
ctProtein/ProbDam
aging;7
/7p.E11
3*28
–02
HOGA1
2c.22
7G.A
p.G
76D
C65
/Affe
ctProtein/ProbDam
aging;7
/7p.M
292T
282–
032
c.30
8A.Tg
p.N
103I
gC55
/Affe
ctProtein/Ben
ign;
1/7
c.70
0+5G
.T
362–
034
c.53
3T.Ch
p.L17
8Ph
C65
/Affe
ctProtein/ProbDam
aging;7
/7p.P17
9T45
7–03
4c.53
5C.Ah
p.P17
9Th
C35
/Affe
ctProtein/PossiblyDam
aging;7
/7p.L17
8P45
7–03
7c.97
3G.A
p.G
325S
C55
/Affe
ctProtein/ProbDam
aging;7
/7c.70
0+5G
.T
193–
03a N
ucleotid
enu
mberingbased
onNM_0
0003
0.2(AGXT),NM_0
1220
3.1(G
RHPR),an
dNM_1
3841
3.3(HOGA1).
bIn
silicoev
alua
tionof
nove
lmissensemutations:A
lignG
VGD/SIFT/PolyP
hen-2an
diden
titywith
multip
leseque
ncealignm
ent(hum
an,b
ull,mouse,
rat,dog
,chicken
,and
zebrafish).
c Sec
ondallele
islistedin
resp
ectto
ped
igreeorder.
dTh
eseva
riantswerealso
iden
tified
asno
velA
GXTallelesin
therece
ntpub
licationfrom
Man
drileetal.47
eKoz
akmutationwas
scoredusingNetStart1.0;
highe
rsco
remorelikelyac
tsas
tran
scrip
tioninitiationco
don.
f Nov
elsp
licingwas
assessed
usingBDGP;
highe
rsco
remorelikelyac
tsas
splicesite.
gDetailo
fthissubstitu
tionshownin
Supplemen
talF
igure2C
.hDetailo
fthisdou
ble
substitu
tionshownin
Supplemen
talF
igure2B
.
www.jasn.org CLINICAL RESEARCH
J Am Soc Nephrol 26: 2559–2570, 2015 PH Phenotype/Prevalence Analysis 2561

Allelic Associations with Phenotype in PH1To compare AGXT genotype with PH1 phenotype, we charac-terized patients by their combination of mutation types, definedas truncating, nontruncating, or MiR (p.G41R, p.F152I,p.G170R, p.I244T), with the hypothesis that nontruncating/MiR mutations might still have some residual function. Patientswith two MiR mutations had later onset of symptoms, progres-sed more slowly to ESRD, and had lower oxalate and glycolatelevels than patients with any other genotypes (Figure 2B, Sup-plemental Table 1, Table 3). These results are consistent withprevious findings for p.G170R25 and highlight the incompletepenetrance/variable expressivity of these alleles. No significantdifference in phenotype was noted between patients with twotruncating or two nontruncating mutations when MiR muta-tions were excluded (Supplemental Figure 3, SupplementalTable 2), suggesting that non-MiR, nontruncating alleles areusually fully inactivating. However, we did notice a renal survivalbenefit among those heterozygous for a MiR allele compared
with those having no MiR allele, as previ-ously reported for p.G170R (Figure 2B).25
This milder phenotype was also evident bylower urine glycolate levels but not by otherurine chemistries, the age at disease onset,or the incidence of nephrocalcinosis (Table3). To evaluate whether all MiR alleles be-haved similarly with regard to phenotype,we separated p.G170R from the other MiRalleles (p.G41R, p.F152I, p.I244T). Kaplan-Meier renal survival curves revealed thatonly p.G170R homozygotes hadmilder dis-ease, not patients homozygous for theother MiR alleles (Figure 3). The survivaladvantage for p.G170R persisted, althoughsignificance decreased, even after adjust-ment for treatment with pyridoxine beforerenal failure (Figure 3); this occurred in53% of p.G170R homozygotes, 26% ofother MiR homozygotes, and 38% of pa-tients without a MiR allele. The proportionof patients treated did not significantly dif-fer between the groups (P=0.14). There-fore, although all MiR alleles unmask thefunctional MTS, their penetrance signifi-cantly differs.29
Allelic Associations with Phenotype inPH2 and PH3To evaluate genotype-phenotype correlationsin our PH2 cohort, patients were groupedaccording to mutation type (two truncating,two nontruncating, or a truncating plus anontruncating allele). However, no signifi-cant associations were observed with age atsymptoms or ESRD, nephrocalcinosis, andurine chemistry (Supplemental Table 3).
Patients with PH3 were grouped by the common mutations(homozygous for c.700+5G.Tor p.E315del; heterozygous, com-pound heterozygous for c.700+5G.T/p.E315del, or lackingthesemutations). As for PH2, no significant genotype-phenotypeassociations in our relatively small PH3 cohort were apparent(Supplemental Table 4). Interestingly, one PH3patient developedESRDat 8 years. This patientwas homozygous for a pair of closelylinked, nonconservative missense variants predicted to be highlypathogenic, rather than the common HOGA1 alleles (Supple-mental Figure 2B, Table 1). This patient was symptomatic atage 18 months, with multiple calcium oxalate stones that weresurgically removed; CKD was first noted at age 6 years, at leastpartly attributed to obstructive uropathy.
Disease Variability among Patients with the SameGenotype and within FamiliesIntrafamilial variable disease expression and phenotypic hetero-geneity among patients with the same allelic combinations have
Figure 1. Genotypic and allelic breakdown varies considerably between the different PHtypes in themutation resolved 267pedigrees. (A) Genotypic breakdownby PH type showingpatients with two truncating alleles (nonsense, splice, and frameshifting InDels [insertion,duplication, deletion, or insertion+deletion]), two nontruncating alleles (missense and in-frame InDels), or a truncating plus a nontruncating allele. Number in parentheses representsnumber of families with that genotype. (B) Allelic analysis by PH type of different mutationtypes. Common alleles of each PH type plus their frequencies are also highlighted. AGXTp.G170R was found homozygously (hom) in 29 families and heterozygously (het) in75 families, GRHPR c.103delG (hom, 5 families; het, 5 families), HOGA1 c.700+5G.T(hom, 8 families; het, 12 families), HOGA1 p.E315del (hom, 7 families; het, 7 families).
2562 Journal of the American Society of Nephrology J Am Soc Nephrol 26: 2559–2570, 2015
CLINICAL RESEARCH www.jasn.org

been observed in PH1.5,25 In the current cohort, five PH1families had differences of .20 years between siblings re-garding the timing of ESRD onset, and considerable pheno-typic variability was present between patients homozygousfor specific AGXT alleles (Supplemental Table 5A). Withinthe PH2 and PH3 cohorts, homozygotes for common muta-tions also displayed considerable variability of disease ex-pression (Supplemental Table 5A). Within one PH2 familyhomozygous for GRHPR c.103delG, one of three affectedsiblings reached ESRD at age 21 years, whereas the othertwo manifested with only occasional stone disease, witheGFRs of 40 and 85 ml/min per 1.73 m2 at 56 and 53 years,respectively.
Estimation of PH Prevalence Using Public Whole-Exome Sequencing DataFrom the National Heart, Lung, and Blood Institute (NHLBI)Exome Sequencing Project (ESP) data, we extracted alleliccounts of 22 known PH mutations (12 AGXT, 5 GRHPR, and5 HOGA1) found within the population of 4300 EuropeanAmericans (EA) and 2203 African Americans (AA) (Supple-mental Figure 1, Supplemental Table 6).40 Further, we in-cluded all frameshifting or nonsense changes and scored allrare, nonsynonymous variants not previously identified as PHmutations using in silico tools, and thus identified 20 addi-tional likely pathogenic variants (4 AGXT, 6 GRHPR, and10 HOGA1) (Supplemental Figure 1, Supplemental Table 7).
With use of the Hardy-Weinberg equation, an overall PHcarrier frequency (CF) of 1:71 with a predicted prevalence of1:58,243 was calculated from the 22 known mutant alleles(Supplemental Table 6, Table 4). Including the predicted path-ogenic alleles increased the CF and prevalence to 1:58 and1:38,630, respectively (Supplemental Tables 7 and 8). PH waspredicted to be approximately 60% less prevalent in AAs than inEAs (EA: CF, 1:61, prevalence, 1:40,276; AA: CF, 1:104, preva-lence, 1:100,380) (Table 4). This difference was largely driven bythe commonEAalleleHOGA1 c.700+5G.T (CF, 1:165; AA: CF,1:1102) (Figure 4, Supplemental Table 6). The prevalence ofPH1 was similar in EAs and AAs, even though AGXT p.G170R(EA: CF, 1:429) was unique to the EA population, but was bal-anced by AGXT p.R289H, the most prevalent AA allele, whichaccounted for approximately 33% of all AA mutant alleles (CF,1:289; EA: CF, 1:1956) (Figure 4, Supplemental Table 6). Inter-estingly, theAGXT “minor” allele variants p.P11L/p.I340Mwere15 times less prevalent in AAs than EAs (EA: CF, 1:3, prevalence,1:15; AA: CF, 1:8, prevalence, 1:236) (Supplemental Table 6). Aswith PH1, PH2 prevalence was also similar in EAs versus AAs asGRHPR c.103delG was relatively common in both populations(EA: CF, 1:375; AA: CF, 1:426) (Figure 4, Supplemental Table 6).
When separated by PH type, PH1 and PH3 had a similar CF(1:195versus 1:185) andprevalence (1:151,887 versus 1:135,866)(Table 4), whereas in our patient screen PH1 was six timesmorecommon (68.4% of families versus 11.0%). These data suggest adistinct underdiagnosis and/or lack of penetrance of PH3.The frequency of PH3 was predominantly driven by HOGA1c.700+5G.T, which had an approximately 2.8 times greaterCF (1 in 232) than AGXT p.G170R (1 in 649) in the ESP data,yet they accounted for 5.2% and 24.9% of all PH alleles, respec-tively, within our patient cohort. On the basis of these calcula-tions, PH2 was predicted to be about 2.2 times less prevalentthan PH1 or PH3 (CF, 1:279; prevalence, 1:310,055) (Table 4),but in our disease cohort its prevalence was similar to that ofPH3 and approximately seven times rarer than PH1.
DISCUSSION
Herewepresent genotype-phenotype correlations inoneof thelargest fully genotyped PH cohorts to date and for the first time
Figure 2. Renal Survival plots showing (A) poorer renal survivalfor PH1 patients followed by PH2, and (B) better renal surviv-al for PH1 patients with two MiR alleles. (A) Kaplan-Meier re-nal survival plot of the PH1, PH2, PH3, and NMD cohorts. (B)Kaplan-Meier renal survival plot of PH1 patients categorizedas having two MiR alleles (homozygous, or compound het-erozygous; AGXT p.G41R, p.F152I, p.G170R, p.I244T, 89patients), one MiR allele in combination with a non-MiR allele(97 patients), or two alleles of which neither was a MiR allele(no MiR, 81 patients). Tables below Kaplan-Meier plotsshow survival estimates with number of patients at risk inparentheses.
J Am Soc Nephrol 26: 2559–2570, 2015 PH Phenotype/Prevalence Analysis 2563
www.jasn.org CLINICAL RESEARCH

calculate PH prevalence based on large population data. Be-cause of the population size, we have significantly increasedthe number of unique PH mutations (AGXT by 10.1%,GRHPR by 46.4%, and HOGA1 by 26.3%) (SupplementalFigure 1). This analysis highlights the allelic heterogeneity ofthese disorders, although the population importance of a fewcommon alleles is also reinforced (Figure 1). While elevatedurinary glycolate,5 L-glycerate,4 or HOGA38 levels can often pro-vide strong evidence regarding the PH gene involved (Table 2),there is significant overlap between PH types and normal indi-viduals. Thus, we emphasize here the value ofmolecular analysesas a gold standard method to diagnose PH. As sequencing costsfall and new methods are adopted, it is increasingly practical toimplement a protocol that fully screens the coding regions of allgenes, not just commonly inherited variants,5 and thoroughlyevaluates all detected variants.
Our genic prevalence in mutation resolved families—77.1%PH1, 10.5% PH2, 12.4% PH3—coincides with previous esti-mates (PH1, 80%; PH2, 10%; PH3, 10%) and highlights PH1 asthe most common form, while PH3 is now at least as commonas PH2.1–3 Interestingly, 11.3% of our clinically defined cohort(34 pedigrees) had no mutation detected in the known PH
genes. Given the phenotype in these families (see below) andthe reliability of molecular diagnostics (with no single PHmuta-tions detected in our NMD group), further genetic heterogeneityin PH seems likely. Although our NMD cases met the RKSC PHregistry criteria (ConciseMethods), first symptoms occurred 4–9years later than for genetically definedPH (Table 2), urine oxalateexcretionwas lower than PH1 and PH2 (but similar to PH3), andESRD was rare, although there was considerable interfamilialvariability (Supplemental Table 5B). These data indicate thatrigorous clinical/molecular assessment is required to identify apopulation suitable for further gene discovery efforts in PH.
Our PH1 cohort displayed many characteristics reported insmaller cohorts; twoAGXT variants accounted for 47.8%of PH1mutant alleles (p.G170R [32.3%] and c.33dupC [15.5%]), andmost mutations were missense, even after exclusion of com-mon alleles (Figure 1).6,25,41–43 PH1 was the most severe PH type(Figure 2, Table 2), with amedian age of first symptoms (5.2 years)and a cumulative renal survival (76%, 43%, and 12% at 20 years,40 years, and 60 years, respectively) similar to that reported inthe literature.1,2,5,18,25 Further, although elevated urinary excre-tion of glycolate suggested PH1, the range (6.0–1183.0 mg/gcreatinine) overlapped with other PH types and NMD patients
Table 2. Clinical presentation of RKSC PH patients based on PH type
Variable PH1 (n=247) PH2 (n=35) PH3 (n=38) NMD (n=35) P Value, Adjusted
Age at symptoms 0.01Median (y) 5.2 7.4 2.6 11.5Q1, Q3 (y) (2.0, 14.0) (1.7, 15.8) (0.9, 5.5) (3.9, 24.1)Minimum, maximum (y) (0.1, 53.0) (0.6, 42.0) (0.3, 31.0) (0.1, 69.7)Patients (n) 213 31 33 29
Nephrocalcinosis, n (%) ,0.0001Yes 49 (30.6) 5 (16.7) 1 (2.7) 5 (16.7)No 111 (69.4) 25 (83.3) 36 (97.3) 25 (83.3)
Urine chemistryOx24 (mmol/1.73 m2) (normal , 0.46)a ,0.0001Median 1.8 1.7 1.1 1.2Q1, Q3 (1.2, 2.7) (1.1, 2.2) (0.9, 1.4) (1.0, 1.5)Patients (n) 121 23 34 23
Ca24 (mg/1.73m2) (normal 100–300)a ,0.0001Median 56.8 91.5 91.4 135.9Q1, Q3 (34.1, 91.2) (55.8, 134.2) (63.5, 153.0) (79.9, 236.8)Patients (n) 82 19 26 20
Cit24 (mg/1.73 m2) (normal 320–1240)a ,0.0001Median 278.5 722.9 676.9 371.0Q1, Q3 (108.2, 488.3) (245.2, 1285.0) (416.3, 812.9) (289.3, 954.5)Patients (n) 74 15 27 20
Glycolate (mg/g creatinine) (normal 0–78)b ,0.0001Median 102.2 28.0 18.0 33.0Q1, Q3 (46.5, 218.0) (22.0, 41.0) (8.0, 42.0) (14.0, 54.0)Patients (n) 96 22 23 22
L-glycerate (mg/g creatinine) (normal 0–8)b ,0.0001Median 3.0 785.0 1.0 7.0Q1, Q3 (2.0, 9.0) (271.0, 1467.0) (0.0, 6.0) (2.0, 11.0)Patients (n) 91 19 21 21
Q1, Q3, first and third quartiles; Ox24, 24-hour oxalate; Ca24, 24-hour calcium; Cit24, 24-hour citrate.aNormal values are for adult patients. Values in table have been adjusted for body surface area to permit comparison of adult and pediatric patients.52,53bNormal values may be higher in children from birth to 5 years of age.
2564 Journal of the American Society of Nephrology J Am Soc Nephrol 26: 2559–2570, 2015
CLINICAL RESEARCH www.jasn.org

(minimum,maximumurine glycolatemg/g creatinine: PH2, 0.0,105.0; PH3, 0.0, 116.0; NMD, 1.0, 168.0) (Table 2), indicatingthat glycolate analysis alone cannot unequivocally identify thisPH form.5 Patients homozygous for one of the fourMiR alleles29
had milder PH1 (Figure 2, Table 3), as suggested for p.G170R,25
but separating p.G170R from the other MiR alleles highlightedthat later onset of ESRD was associated only with p.G170R (Fig-ure 3); renal survival of the otherMiR patients was similar to thatof patients with truncating or non-MiR nontruncating alleles.These results emphasize the incompletely penetrant nature/variable expressivity of p.G170R and suggest a different patho-mechanism for other MiR alleles, such as monomer aggregationor active site disruption, as indicated for p.G41R.29,44 This isimportant in considering pyridoxine therapy for patients withother MiR alleles because this cofactor is thought to stabilizethe monomer/dimer. Nevertheless, anecdotal evidence suggestspyridoxine response in a variety of AGXTmutation patients(including p.F152I or two truncating alleles), indicating thatalternative therapeutic benefits of pyridoxine may exist (e.g., in-fluence on gene expression and/or enzyme activity).30,32,45–47
We found no difference in phenotype between patients withtwo non-MiR nontruncating versus two truncating alleles,suggesting that all these AGXT alleles are fully inactivating(Supplemental Figure 3, Supplemental Table 2). This contrastswith a recent publication that reported better renal survival of
patients with two non-p.G170R nontruncating variants versustwo truncating variants (16.9 years versus 9.9 years).47 Althoughit is possible we did not observe this correlation because of oursmaller cohort size (247 patients in the RKSC PH registry versus410patients in theOxalEuropeConsortium), and the significanceof pairwise comparisons was not provided.47 The OxalEuropeinvestigators also analyzed allelic effects between specificmissensevariants,47 but given the observed intrafamilial/intragenotypephenotypic heterogeneity (Supplemental Table 5A)5,25,47 due togenetic/environmental modifier effects, caution is required withinterpretation in these small populations. More detailed allelicanalysis of PH1 will be possible as population sizes increase andthrough pooled analysis of available cohorts.
In our cohort, PH2was similar to PH1 in terms of age at symp-toms and oxalate levels; however, progression to ESRD wassignificantly slower (Figure 2, Table 2).2,4 Elevated urinaryL-glycerate levels separated PH2 cases from PH1 and PH3 cases,but some overlap with the genetically unresolved group was seen(minimum, maximum urine L-glycerate mg/g creatinine: PH1,0.0, 129.0; PH2, 151.0, 4355.0; PH3, 0.0, 40.0; NMD, 0.0, 152.0).4
Similarly, dramatic intrafamilial/intragenotype phenotypicheterogeneity was observed (Supplemental Table 5A), suggestingsignificant genetic/environmental modifier effects in PH2. Nosignificant associations of phenotype with mutation type weredetected in patients with PH2 (Supplemental Table 3), although
Table 3. Evaluation of PH1 severity based on number of MiR variants per genotype
Variable Hom MiR (n=69) Het MiR (n=97) No MiR (n=81) P Value, Adjusted
Age at symptoms 0.006Median (y) 10.6 4.7 4.3Q1, Q3 (y) (2.4, 22.0) (1.7, 12.4) (0.7, 8.4)Minimum, maximum (y) (0.5, 49.8) (0.1, 53.0) (0.1, 41.5)Patients (n) 59 86 68
Nephrocalcinosis, n (%) 0.08Yes 7 (18.4) 21 (30.4) 21 (39.6)No 31 (81.6) 48 (69.6) 32 (60.4)
Urine chemistryOx24 (mmol/1.73 m2) (normal , 0.46)a ,0.001Median 1.1 2.0 2.3Q1, Q3 (0.7, 1.7) (1.3, 2.6) (1.7, 2.9)Patients (n) 26 63 32
Ca24 (mg/1.73m2) (normal 100–300)a 0.10Median 79.5 54.1 54.9Q1, Q3 (29.0, 157.5) (35.8, 78.6) (32.7, 69.2)Patients (n) 19 42 21
Cit24 (mg/1.73 m2) (normal 320–1240)a 0.71Median 402.5 275.7 281.7Q1, Q3 (125.4, 584.7) (112.7, 436.2) (87.9, 471.6)Patients (n) 16 36 22
Glycolate (mg/g creatinine) (normal 0–78)b 0.002Median 45.0 96.0 182.0Q1, Q3 (19.0, 143.0) (48.0, 182.0) (89.0, 310.0)Patients (n) 23 47 26
Hom, homozygous; Het, heterozygous; Q1, Q3, first and third quartiles; Ox24, 24-hour oxalate; Ca24, 24-hour calcium; Cit24, 24-hour citrate.aNormal values are for adult patients. Values in table have been adjusted for body surface area to permit comparison of adult and pediatric patients.52,53bNormal values may be higher in children from birth to 5 years of age.
J Am Soc Nephrol 26: 2559–2570, 2015 PH Phenotype/Prevalence Analysis 2565
www.jasn.org CLINICAL RESEARCH

our cohortwas probably too small to identify subtle differences indisease severity. Interestingly, most GRHPR mutant alleles wereframeshifting, largely driven by the common c.103delG variant.
In our cohort, no PH3 family had two truncating alleles(Figure 1), with only one such patient described.36 Phenotypicanalysis of patients with varying or no detected HOGA levelswill prove interesting and provide insight into whether mostHOGA1 alleles are incompletely or fully penetrant, consistentwith structural analyses.48 Interestingly, some HOGA1 carrierspresent with mild hyperoxaluria or idiopathic urinary stone dis-ease39 (unlike other forms of PH), and the first reported patientwith PH3 to reach ESRD was homozygous for two novel, linkedmissense variants (Supplemental Figure 2); suggesting thatmorepenetrant mutations may have a stronger phenotypic effect.However, the ESRD in this single patient with PH3 may have,at least in part, been aggravated by renal injury from recurrentstone removal surgeries. Paradoxically, patients with PH3 pres-ent with symptoms at the earliest age but subsequently haverelatively mild disease (Figure 2, Table 2), suggesting decreasedsensitivity to HOGA levels with aging. The lack of a detectedgenotype-phenotype correlationbetween the twomost commonHOGA1 alleles (c.700+5G.Tand p.E315del) may again be dueto the small populations and other genetic/environmental mod-ifier effects (Supplemental Figure 5A).
Themost importantfinding from this study is that the overallcarrier frequency (approximately 1:70) and the inferred preva-lence (approximately 1:58,000) calculated from population dataare close to an order of magnitude greater than estimates fromclinical studies.Because thesenewestimates come fromcountingknown mutant alleles and are largely driven by a few commonalleles, this study isunlikely tooverestimate the carrier frequency.The estimates of PH1 prevalence are about twice the previousestimates, but the difference is much more notable for PH3,which has an observed population carrier frequency higher than
PH1 but is 6-fold less common in currentlyidentified clinical populations. PH2 has apopulation carrier frequencyhalf that ofPH1but is more than 7-fold less common inclinical populations. It is notable that PH isdetermined to be about 2.5-fold less preva-lent in AAs than EAs, a difference mainlydriven by the HOGA1 c.700+5G.T mu-tation (Figure 4). Interestingly, AGXTp.G170R is exclusively found in EAs, andthe AGXT MTS variants (p.P11L, p.I340M,minor haplotype) aremuch rarer inAAs thanEAs (Figure 4, Supplemental Table 6).49
This finding suggests that mutations predic-ted to mistarget AGTmight generally remainasymptomatic in AAs because presence ofthe minor haplotype is required for theMTS to be active.29 Interestingly, PH1 prev-alence is nonetheless similar between EAsand AAs because of the most common AAmutation, AGXT p.R289H (reported in thePHMD22). This variant is significantlymore common than any PH allele (exclud-ing EA: HOGA1 c.700+5G.T) (Figure 4)
Figure 3. Renal survival plots showing that only homozygousp.G170R patients but not homozygotes of other MiR genotypeshad a renal survival advantage. Kaplan-Meier renal survival plot plussurvival estimate table for PH1 patients homozygous for p.G170R(34 patients), homozygous or compound heterozygous for anotherMiR allele (p.G41R, p.F152I, p.I244T, 19 patients), or having no MiRallele (81 patients). Pairwise comparisons show greater renal survival inpatients homozygous forAGXT p.G170R but not the other MiR allelescompared with patients without a MiR allele (Hom p.G170R versus noMiR; P,0.0001 [P,0.001], Hom other MiR versus no MiR P=0.27[P=0.35], Hom p.G170R versus Hom other MiR P=0.04 [P=0.05]).P values in square brackets are adjusted for the effect of pyridoxinetreatment, reducing the overall significance but upholding the sur-vival advantage of AGXT p.G170R homozygotes.
Table 4. Carrier frequency and prevalence based on PH mutant alleles found in theNHLBI ESP
Variable EA Patients AA Patients All Patients (EA + AA)
PH1+PH2+PH3Allele count (Alt/Ref) 70/8495 21/4361 91/12,856Mutant allele frequency (%) 0.824 0.482 0.708Prevalence (1 in)a 40,276 100,380 58,243CF (1 in)a 61 104 71
PH1 (AGXT )Allele count (Alt/Ref) 22/8502 11/4359 33/12,861Mutant allele frequency (%) 0.259 0.252 0.257Prevalence (1 in) 149,347 157,032 151,887CF (1 in) 194 199 195
PH2 (GRHPR)Allele count (Alt/Ref) 15/8459 8/4348 23/12,807Mutant allele frequency (%) 0.177 0.184 0.180Prevalence (1 in) 318,021 295,392 310,055CF (1 in) 282 272 279
PH3 (HOGA1)Allele count (Alt/Ref) 33/8524 2/4377 35/12,901Mutant allele frequency (%) 0.387 0.046 0.271Prevalence (1 in) 66,720 4,789,532 135,866CF (1 in) 130 1095 185
aPrevalence was determined by combining the individual prevalence of all PH types with bigenic PHcases counting as carriers.
2566 Journal of the American Society of Nephrology J Am Soc Nephrol 26: 2559–2570, 2015
CLINICAL RESEARCH www.jasn.org

and scores poorly,40 calling into question its true pathogenicnature. Removal of this allele would decrease PH1 prevalenceby 48% (CF, 1:270; prevalence, 1:291,256) and overall PH prev-alence by 18% (CF, 1:79; prevalence, 1:71,333, SupplementalTable 9). Further, PH1 prevalence in AAs would decrease by87% (CF, 1:549; prevalence, 1:1,203,908) and PH prevalenceoverall within the AApopulation by 56% (CF, 1:156; prevalence,1:225,971). Consequently, PH would be about 82% less preva-lent in AAs than EAs.
Thedifference between the expected andobservedprevalence,especially for PH3 and to a lesser extent for PH2, is likely dueto underdiagnosis of these diseases, which have overall milderphenotypes and are much less likely than PH1 to result in ESRD.In addition, relatively mild disease in a subset of PH1 patients(especially p.G170Rhomozygotes) and awide variability in age atfirst symptoms (Table 2), may account for the 2-fold underdiag-nosis of PH1. Further, misdiagnosis of PH for other renal dis-eases, as illustrated by homozygosity for an AGXTmutation in apatient with nephronophthisis,50 may also play a role in under-estimation of PH prevalence. Therefore, PH genotype analysis ofidiopathic stone disease populations and other patients with PHphenocopies but no known mutations are likely to be informa-tive for undiagnosed PH cases. Indeed, within a stone clinicsetting the diagnosis of PH should be carefully considered amongpatients with unexplained hyperoxaluria and/or CKD, accordingto the published diagnostic algorithm.51 This consists of an initialcomprehensive analysis of urine oxalate and chemistries plusplasma oxalate, followed by molecular testing of the PH genesin suspected cases.
CONCISE METHODS
RKSC PH RegistryThe relevant institutional review boards and ethics committees
approved the study, and all participants gave informed consent. The
RKSCPHregistry is a secureweb-based registry
that enables international contributions.3 Pa-
tients within the registry met at least one of the
following criteria: (1) Liver biopsy confirmed
specific enzyme deficiency of AGT, GR/HPR,
or HOGA, (2) molecular diagnostic testing of
AGXT, GRHPR, and HOGA1 identified two
mutant alleles in one of the genes, (3) urinary
oxalate excretion was .0.8 mmol/1.73 m2 per
day in the absence of an identifiable secondary
cause of hyperoxaluria, and/or (4) ESRD had
developed, along with (a) predialysis plasma
oxalate.60 mmol/L and renal biopsy confirm-
ing extensive oxalate deposition or (b) sys-
temic oxalosis (retinal oxalate deposits; oxalate
deposits in bone marrow, skin, or other tissue;
nephrocalcinosis; or calcium oxalate nephroli-
thiasis). As of June 2014, 422 patients from
37 countries had been enrolled in the RKSC PH
registry, of whom 355 were screened for mutations in the known PH
genes.
DNA Collection and Sanger Mutation ScreeningPatients enrolled in the RKSC PH registry who consented to molecular
testing had blood drawn for DNA isolation. Sanger sequencing was
performed of all coding exons620 bp (AGXT, NM_000030.2; GRHPR,
NM_012203.1; HOGA1, NM_138413.3) using M13-tailed primers
(Beckman Coulter). Primer sequences can be obtained by request. All
Sanger chromatograms were analyzed usingMutation Surveyor, version
4.06 (Softgenetics), and identified variantswere categorized as nonsense,
missense, frameshifting, or inframe InDels; typical splice (62 bp from
exon boundary); or atypical splice (.62 bp from exon boundary). A
total of 115 families (approximately 38%) were screened for the cod-
ing regions of all three genes simultaneously, while the remainder
were screened sequentially until two pathogenic alleles were identi-
fied (first AGXT, second GRHPR, third HOGA1). None of the NMD
cases had a single pathogenic allele in any of the three genes, and none
of the patients with PH1, 2, or 3 had a third pathogenic allele in the
same or another PH gene.
Evaluation of Novel PH AllelesAminoacid substitutionsnotpreviously reported inHGMDorPHMD22
were evaluated using the in silico prediction programs AlignGVGD
(http://agvgd.iarc.fr/index.php), PolyPhen-2 (http://genetics.bwh.harvard.
edu/pph2/), and SIFT (http://sift.jcvi.org). The novel GRHPR atypical
splice site mutation (c.404+5G.A) was evaluated using the Berkeley
Drosophila Genome Project (http://www.fruitfly.org) with the DNA
sequence of the altered 62 exons as input. The novel GRHPR Kozak
sequencemutation (c.[24G.A,23C.T]) was assessed usingNetStart
1.0 (http://www.cbs.dtu.dk/services/NetStart/) with the full mRNA+59
untranslated region as input. Additionally, for amino acid substitutions,
multiple sequence alignments usingAGT,GR/HPR, andHOGAprotein
orthologs of bull (Bos taurus), mouse (Mus musculus), rat (Rattus
norvegicus), dog (Canis lupus), chicken (Gallus gallus), and zebrafish
(Danio rerio) were used to evaluate evolutionary conservation. Amino
Figure 4. Carrier frequencies of common PH alleles found in the NHLBI ESP accountfor significant racial differences. Depiction of the most common PH alleles separated byEA and AA CF. AGXT p.G170R (CF in EAs, 0.23%) and p.R289H (CF in AAs, 0.35%)account for 45.1% and 68.8% of the total PH1 CF, respectively. Similarly, GRHPRc.103delG accounts for 75.3% and 63.4% of the total EA or AA PH2 CF, respectively,and HOGA1 c.700+5G.T accounts for 78.4% and 100% of the total EA or AA PH3 CF,respectively.
J Am Soc Nephrol 26: 2559–2570, 2015 PH Phenotype/Prevalence Analysis 2567
www.jasn.org CLINICAL RESEARCH

acid substitutions were scored as pathogenic if two of three in silico tools
predicted them as damaging, the change was evolutionarily conserved,
and/or the variant segregated appropriately.
Statistical AnalysesPhenotype analyses used the first available 24-hour urine (oxalate,
calcium, citrate, glycolate, L-glycerate) and first renal imaging (nephro-
calcinosis).More than 80%of these tests were done from1 year before to
3 years after PH diagnosis. Comparisons of genotypic groups with con-
tinuous and nominal phenotypic factors at disease presentation were
done using the Kruskal–Wallis rank test and chi-squared tests, respec-
tively. Mixed-effects models (urine chemistry ranks) and generalized
estimating equations (nephrocalcinosis) were also used to test genotypic
effects while adjusting for possible pedigree effects. Time from birth to
development of renal failure was estimated using Kaplan–Meier curves,
with comparisons based on the log-rank test and censoring subjects
without renal failure at last follow-up. The Cox model with robust var-
iance estimator was used to test associations of phenotype with time to
ESRD, with adjustment for potential within-pedigree correlations. The
adjustment for the effect of pyridoxine treatment was performed using a
time-dependent covariate in the Coxmodel. All statistical tests were two
sided, with ana level of 0.05; only P values adjusted for potential within-
pedigree effects as described above were reported.
Prevalence CalculationsThe data of the NHLBI ESP40 were downloaded from http://evs.gs.
washington.edu/EVS/ in VCF file format and analyzed using SNP &
Variation Suit, version 7 (GoldenHelix). Variants withinAGXT, GRHPR,
andHOGA1 that were known as PHmutations (HGMD, PHMD, RKSC
PH registry) were annotated (Supplemental Figure 1, Supplemental
Table 6). All other variants with an MAF,0.01% were scored for po-
tential pathogenicity using the criteria described above (Supplemental
Figure 1, Supplemental Table 7). The only PH mutation reported as
homozygous in ESP was GRHPR c.103delG. However, the variant is
located in a poly-G stretch, which often results in misalignment; hence,
genotype and allele counts were adjusted to represent this homozygous
call as heterozygous. Using alternate and total allele counts, prevalence
(1/p2) and CFs [1/(12p22q2)=1/(2pq)] were calculated according to
Hardy-Weinberg equilibrium for each PH type using the sum of all alter-
nate PH1, 2, or 3 alleles (p, known [Table 4] or known+
scored as pathogenic [Supplemental Table 8]) and all WT alleles
(12p=q). Calculations for PHoverall were done by adding the p2 values
of each PH type, with bigenic PH individuals counted as carriers.
ACKNOWLEDGMENTS
We thank all of the patients and families who have participated in the
RKSC PH registry as well as the many physicians who collected the
detailed clinical records (see below and Supplemental Material for
the list of RKSC coordinators and participation/contribution sites,
respectively). Further, we thank the study coordinators who collected
clinical data and biological samples, as well as Ramila A. Mehta for
her statistical advice.
The RKSC is a part of the National Institutes of Health Rare Diseases
Clinical Research Network. Funding and/or programmatic support for
this project has been provided by U54-DK083908 from the National
Institute of Diabetes andDigestive and Kidney Diseases, National Center
for Advancing Translational Sciences, Mayo Hyperoxaluria Center, and
Mayo Foundation. This work was further supported by the Oxalosis and
Hyperoxaluria Foundation and the American Society of Nephrology
Ben J. Lipps Research Fellowship (K.H.).
This work was partially presented as two abstracts at the Annual
Meeting of the American Society of Nephrology, 2013 (Atlanta, GA),
and the 11th International Primary Hyperoxaluria Workshop, 2014
(Chicago, IL).
RKSC Coordinators and Coordination Sites: Craig Langman
(Children’s Memorial Hospital, Chicago), Lawrence Copelvitch
(Children’s Hospital of Philadelphia), Yaacov Frishberg (Shaare Zedek
Medical Center, Jerusalem, Israel), Vidar Edvardsson (Landspitali Uni-
versity Hospital, Reykjavik, Iceland), David Goldfarb (New York Uni-
versity), DeanAssimos (University of Alabama, Birmingham), andTodd
Lowther (Wake Forest University School of Medicine, Winston-Salem).
DISCLOSURESNone.
REFERENCES
1. Hoppe B: An update on primary hyperoxaluria. Nat Rev Nephrol8: 467–475, 2012
2. Cochat P, Rumsby G: Primary hyperoxaluria. N Engl J Med 369: 649–658, 2013
3. Lieske JC,Monico CG, HolmesWS, Bergstralh EJ, Slezak JM, RohlingerAL, Olson JB, Milliner DS: International registry for primary hyper-oxaluria. Am J Nephrol 25: 290–296, 2005
4. Rumsby G: Primary hyperoxaluria type 2. In: GeneReviews(R), edited byPagon RA, AdamMP, Bird TD, Dolan CR, Fong CT, Smith RJH, StephensK, Seattle, WA, University of Washington, 1993, Updated 2011
5. Coulter-Mackie MB, White CT, Hurley RM, Chew BH, Lange D: Primaryhyperoxaluria type 1. In: GeneReviews(R), edited by Pagon RA, AdamMP, Bird TD, Dolan CR, Fong CT, Smith RJH, Stephens K, Seattle, WA,University of Washington, 1993, Updated 2011
6. Pirulli D, Marangella M, Amoroso A: Primary hyperoxaluria: Genotype-phenotype correlation. J Nephrol 16: 297–309, 2003
7. Harambat J, van Stralen KJ, Espinosa L, Groothoff JW, Hulton SA,Cerkauskiene R, Schaefer F, Verrina E, Jager KJ, Cochat P; EuropeanSociety for Pediatric Nephrology/European Renal Association-EuropeanDialysis and Transplant Association (ESPN/ERA-EDTA) Registry: Charac-teristics and outcomes of children with primary oxalosis requiring renalreplacement therapy. Clin J Am Soc Nephrol 7: 458–465, 2012
8. van der Hoeven SM, van Woerden CS, Groothoff JW: Primary hyper-oxaluria type 1, a too often missed diagnosis and potentially treatablecause of end-stage renal disease in adults: Results of the Dutch cohort.Nephrol Dial Transplant 27: 3855–3862, 2012
9. Danpure CJ, Jennings PR, Fryer P, Purdue PE, Allsop J: Primary hy-peroxaluria type 1: Genotypic and phenotypic heterogeneity. J InheritMetab Dis 17: 487–499, 1994
10. Cramer SD, Ferree PM, Lin K, Milliner DS, Holmes RP: The gene en-coding hydroxypyruvate reductase (GRHPR) is mutated in patientswith primary hyperoxaluria type II. Hum Mol Genet 8: 2063–2069,1999
2568 Journal of the American Society of Nephrology J Am Soc Nephrol 26: 2559–2570, 2015
CLINICAL RESEARCH www.jasn.org

11. Belostotsky R, Seboun E, Idelson GH, Milliner DS, Becker-Cohen R,Rinat C, Monico CG, Feinstein S, Ben-Shalom E, Magen D,Weissman I,Charon C, Frishberg Y: Mutations in DHDPSL are responsible for pri-mary hyperoxaluria type III. Am J Hum Genet 87: 392–399, 2010
12. Purdue PE, Lumb MJ, Fox M, Griffo G, Hamon-Benais C, Povey S,DanpureCJ: Characterization and chromosomalmapping of a genomicclone encoding human alanine:glyoxylate aminotransferase. Genomics10: 34–42, 1991
13. Danpure CJ, Jennings PR: Peroxisomal alanine:glyoxylate amino-transferase deficiency in primary hyperoxaluria type I. FEBS Lett 201:20–24, 1986
14. Millan MT, Berquist WE, So SK, Sarwal MM, Wayman KI, Cox KL, FillerG, Salvatierra O Jr, Esquivel CO: One hundred percent patient andkidney allograft survival with simultaneous liver and kidney trans-plantation in infants with primary hyperoxaluria: A single-center expe-rience. Transplantation 76: 1458–1463, 2003
15. Cochat P: Primary hyperoxaluria type 1. Kidney Int 55: 2533–2547,1999
16. Hoppe B: Evidence of true genotype-phenotype correlation in primaryhyperoxaluria type 1. Kidney Int 77: 383–385, 2010
17. Cochat P, Liutkus A, Fargue S, Basmaison O, Ranchin B, Rolland MO:Primary hyperoxaluria type 1: Still challenging! Pediatr Nephrol 21:1075–1081, 2006
18. Hoppe B, Beck BB, Milliner DS: The primary hyperoxalurias. Kidney Int75: 1264–1271, 2009
19. Danpure CJ: Molecular aetiology of primary hyperoxaluria type 1.Nephron, Exp Nephrol 98: e39–e44, 2004
20. Danpure CJ, Lumb MJ, Birdsey GM, Zhang X: Alanine:glyoxylateaminotransferase peroxisome-to-mitochondrion mistargeting inhuman hereditary kidney stone disease. Biochim Biophys Acta 1647:70–75, 2003
21. Williams EL, Acquaviva C, Amoroso A, Chevalier F, Coulter-Mackie M,Monico CG, Giachino D, Owen T, Robbiano A, Salido E, Waterham H,Rumsby G: Primary hyperoxaluria type 1: Update and additional mu-tation analysis of the AGXT gene. Hum Mutat 30: 910–917, 2009
22. Rumsby G: Primary Hyperoxaluria Mutation Database. 2013. https://www.uclh.nhs.uk/OurServices/ServiceA-Z/PATH/PATHBIOMED/CBIO/Pages/Phmdatabase.aspx. Accessed October 12, 2014
23. BenhajMbarek I, Abroug S,Omezzine A, ZellamaD, Achour A, Harbi A,Bouslama A: Selected AGXT gene mutations analysis provides a ge-netic diagnosis in 28% of Tunisian patients with primary hyperoxaluria.BMC Nephrol 12: 25, 2011
24. Santana A, Salido E, Torres A, Shapiro LJ: Primary hyperoxaluria type 1in the Canary Islands: A conformational disease due to I244T mutationin the P11L-containing alanine:glyoxylate aminotransferase. Proc NatlAcad Sci U S A 100: 7277–7282, 2003
25. Harambat J, Fargue S, Acquaviva C, GagnadouxMF, Janssen F, LiutkusA, Mourani C, Macher MA, Abramowicz D, Legendre C, Durrbach A,Tsimaratos M, Nivet H, Girardin E, Schott AM, Rolland MO, Cochat P:Genotype-phenotype correlation in primary hyperoxaluria type 1: Thep.Gly170Arg AGXT mutation is associated with a better outcome.Kidney Int 77: 443–449, 2010
26. Danpure CJ, Cooper PJ, Wise PJ, Jennings PR: An enzyme traffickingdefect in two patients with primary hyperoxaluria type 1: Peroxisomalalanine/glyoxylate aminotransferase rerouted to mitochondria. J CellBiol 108: 1345–1352, 1989
27. Cellini B, Lorenzetto A, Montioli R, Oppici E, Voltattorni CB: Humanliver peroxisomal alanine:glyoxylate aminotransferase: Different sta-bility under chemical stress of the major allele, the minor allele, and itspathogenic G170R variant. Biochimie 92: 1801–1811, 2010
28. Pey AL, Salido E, Sanchez-Ruiz JM: Role of low native state kineticstability and interaction of partially unfolded states with molecularchaperones in the mitochondrial protein mistargeting associated withprimary hyperoxaluria. Amino Acids 41: 1233–1245, 2011
29. Fargue S, Lewin J, Rumsby G, Danpure CJ: Four of the most com-mon mutations in primary hyperoxaluria type 1 unmask the cryptic
mitochondrial targeting sequence of alanine:glyoxylate aminotrans-ferase encoded by the polymorphic minor allele. J Biol Chem 288:2475–2484, 2013
30. Monico CG, Olson JB, Milliner DS: Implications of genotype and en-zyme phenotype in pyridoxine response of patients with type I primaryhyperoxaluria. Am J Nephrol 25: 183–188, 2005
31. Monico CG, Rossetti S, Olson JB,Milliner DS: Pyridoxine effect in type Iprimary hyperoxaluria is associated with the most common mutant al-lele. Kidney Int 67: 1704–1709, 2005
32. van Woerden CS, Groothoff JW, Wijburg FA, Annink C, Wanders RJ,Waterham HR: Clinical implications of mutation analysis in primaryhyperoxaluria type 1. Kidney Int 66: 746–752, 2004
33. Cellini B, Montioli R, Paiardini A, Lorenzetto A, Voltattorni CB: Molec-ular insight into the synergism between the minor allele of human liverperoxisomal alanine:glyoxylate aminotransferase and the F152I muta-tion. J Biol Chem 284: 8349–8358, 2009
34. Giafi CF, Rumsby G: Kinetic analysis and tissue distribution of humanD-glycerate dehydrogenase/glyoxylate reductase and its relevance tothe diagnosis of primary hyperoxaluria type 2. Ann Clin Biochem 35:104–109, 1998
35. Cregeen DP, Williams EL, Hulton S, Rumsby G: Molecular analysis ofthe glyoxylate reductase (GRHPR) gene and description of mutationsunderlying primary hyperoxaluria type 2. Hum Mutat 22: 497, 2003
36. Williams EL, Bockenhauer D, van’t Hoff WG, Johri N, Laing C, Sinha MD,Unwin R, Viljoen A, Rumsby G: The enzyme 4-hydroxy-2-oxoglutaratealdolase is deficient in primary hyperoxaluria type 3. Nephrol DialTransplant 27: 3191–3195, 2012
37. Beck BB, Baasner A, Buescher A, Habbig S, Reintjes N, Kemper MJ,Sikora P,MacheC, PohlM, StahlM, Toenshoff B, Pape L, FehrenbachH,JacobDE, Grohe B,WolfMT, NürnbergG, Yigit G, Salido EC, HoppeB:Novel findings in patients with primary hyperoxaluria type III and im-plications for advanced molecular testing strategies. Eur J Hum Genet21: 162–172, 2013
38. Riedel TJ, Knight J, Murray MS, Milliner DS, Holmes RP, Lowther WT:4-Hydroxy-2-oxoglutarate aldolase inactivity in primary hyperoxaluriatype 3 and glyoxylate reductase inhibition.BiochimBiophys Acta 1822:1544–1552, 2012
39. MonicoCG, Rossetti S, Belostotsky R, Cogal AG,Herges RM, Seide BM,Olson JB, Bergstrahl EJ, Williams HJ, Haley WE, Frishberg Y, MillinerDS: Primary hyperoxaluria type III gene HOGA1 (formerly DHDPSL) as apossible risk factor for idiopathic calcium oxalate urolithiasis. Clin J AmSoc Nephrol 6: 2289–2295, 2011
40. Exome Variant Server: NHLBI GO Exome Sequencing Project (ESP).http://evs.gs.washington.edu/EVS/. Accessed October 20, 2014
41. AmorosoA, Pirulli D, Florian F, PuzzerD, BoniottoM,Crovella S, ZezlinaS, Spanò A, Mazzola G, Savoldi S, Ferrettini C, Berutti S, Petrarulo M,Marangella M: AGXT gene mutations and their influence on clinicalheterogeneity of type 1 primary hyperoxaluria. J Am Soc Nephrol 12:2072–2079, 2001
42. Takayama T, Nagata M, Ichiyama A, Ozono S: Primary hyperoxaluriatype 1 in Japan. Am J Nephrol 25: 297–302, 2005
43. Coulter-Mackie MB, Rumsby G: Genetic heterogeneity in primary hy-peroxaluria type 1: Impact on diagnosis. Mol Genet Metab 83: 38–46,2004
44. Cellini B, Montioli R, Paiardini A, Lorenzetto A, Maset F, Bellini T,Oppici E, Voltattorni CB: Molecular defects of the glycine 41 variants ofalanine glyoxylate aminotransferase associated with primary hyper-oxaluria type I. Proc Natl Acad Sci U S A 107: 2896–2901, 2010
45. Fargue S, Rumsby G, Danpure CJ: Multiple mechanisms of action ofpyridoxine in primary hyperoxaluria type 1. Biochim Biophys Acta1832: 1776–1783, 2013
46. Hoyer-Kuhn H, Kohbrok S, Volland R, Franklin J, Hero B, Beck BB,Hoppe B: Vitamin B6 in primary hyperoxaluria I: First prospective trialafter 40 years of practice. Clin J Am Soc Nephrol 9: 468–477, 2014
47. Mandrile G, van Woerden CS, Berchialla P, Beck BB, AcquavivaBourdain C, Hulton SA, Rumsby G: Data from a large European study
J Am Soc Nephrol 26: 2559–2570, 2015 PH Phenotype/Prevalence Analysis 2569
www.jasn.org CLINICAL RESEARCH

indicate that the outcome of primary hyperoxaluria type 1 correlateswith the AGXT mutation type. Kidney Int 86: 1197–1204, 2014
48. Riedel TJ, Johnson LC, Knight J, Hantgan RR, Holmes RP, Lowther WT:Structural and biochemical studies of human 4-hydroxy-2-oxoglutaratealdolase: Implications for hydroxyproline metabolism in primary hy-peroxaluria. PLoS ONE 6: e26021, 2011
49. Caldwell EF, Mayor LR, Thomas MG, Danpure CJ: Diet and the fre-quency of the alanine:glyoxylate aminotransferase Pro11Leu poly-morphism in different human populations. Hum Genet 115: 504–509,2004
50. GeeHY,Otto EA, Hurd TW, Ashraf S, ChakiM, Cluckey A, Vega-WarnerV, Saisawat P, Diaz KA, Fang H, Kohl S, Allen SJ, Airik R, Zhou W,Ramaswami G, Janssen S, Fu C, Innis JL, Weber S, Vester U, Davis EE,Katsanis N, Fathy HM, Jeck N, Klaus G, Nayir A, Rahim KA, Al Attrach I,Al Hassoun I, Ozturk S, Drozdz D, Helmchen U, O’Toole JF, AttanasioM, Lewis RA, NürnbergG, Nürnberg P,Washburn J,MacDonald J, Innis
JW, Levy S, Hildebrandt F: Whole-exome resequencing distinguishescystic kidney diseases from phenocopies in renal ciliopathies. KidneyInt 85: 880–887, 2014
51. Edvardsson VO, Goldfarb DS, Lieske JC, Beara-Lasic L, Anglani F,Milliner DS, Palsson R: Hereditary causes of kidney stones and chronickidney disease. Pediatr Nephrol 28: 1923–1942, 2013
52. Gibbs DA, Watts RW: The variation of urinary oxalate excretion withage. J Lab Clin Med 73: 901–908, 1969
53. Stapenhorst L, SassenR,BeckB, LaubeN,HesseA,HoppeB:Hypocitraturiaas a risk factor for nephrocalcinosis after kidney transplantation. PediatrNephrol 20: 652–656, 2005
This article contains supplemental material online at http://jasn.asnjournals.org/lookup/suppl/doi:10.1681/ASN.2014070698/-/DCSupplemental.
2570 Journal of the American Society of Nephrology J Am Soc Nephrol 26: 2559–2570, 2015
CLINICAL RESEARCH www.jasn.org