Pharmacy Quality Commitment Pharmacy Quality Commitment A Way to Improve Patient Safety Confidential...
56
Pharmacy Quality Pharmacy Quality Commitment Commitment A Way to Improve Patient Safety Confidential Training
-
Upload
nancy-lane -
Category
Documents
-
view
228 -
download
4
Transcript of Pharmacy Quality Commitment Pharmacy Quality Commitment A Way to Improve Patient Safety Confidential...

Pharmacy Quality Pharmacy Quality CommitmentCommitment
A Way to Improve Patient Safety
Confidential Training

AgendaOverview of 2005 Patient Safety Act
Discussion of Patient Safety Organizations
Pharmacy Quality Commitment
Quality SupervisorQuality Related Event (QRE)
Quality Assurance (QA)Continuous Quality Improvement (CQI)
Patient Safety Work Product (PSWP)

“We must accept human error as inevitable – and design around that fact.”
-Dr. Donald M. BerwickFormer Administrator, Centers for Medicare and Medicaid Services (CMS)

Institute of Medicine Reports – there is a problem!
• To Err is Human: Building a Safer Health System (1999)o 7,000 deaths from medication errors
• Crossing the Quality Chasm: A New Health System for the 21st Century (2001)o Patient Safety: Achieving a New Standard for Care (2003)
Need for an information infrastructure
o Preventing Medication Errors: Quality Chasm Series (2006)
At least 1.5 million ADEs occur each year
The Focus on Quality

• Provided for the creation of Patient Safety Organizations (PSOs) and establishes Network Patient Safety Databases (NPSD).
• Patient Safety Act GOALS:1. Encourage
1. Promote
3. Share
Patient Safety and Quality Improvement Act of 2005

PSOs are federally listed non-governmental organizations that collect QA data from members
Operate independently, without a relationship to regulatory and/or accrediting bodies
Benefits only extend to member pharmacies
Duties to maintain confidentiality and security
Duties to analyze data and provide feedback
Patient Safety Organizations: protect your
QA data

Includes protections from:
Discovery or Subpoena or FOI request or Evidence Federal, State, or local civil, criminal, or administrative
subpoena or order, including disciplinary proceeding
Limited disclosures allowed for certain criminal proceedings.
If you are uncertain, an attorney should be consulted to help protect your privileges and rights.
PSO Protections
PSO privileges do not protect:
• Patient's medical record• Billing and discharge information• Any other original patient or provider record• Prescription vials, labels, dispensing documents• Information collected, maintained, or
developed separately, or exists separately, from a patient safety evaluation system
What data is “discoverable”

Good business sense = protect patients AND business
State CQI laws (13 states)
CMS Requirement – 3rd Party Contracts
Accreditation and Credentialing programs have CQI requirements
Pharmacies need to have a program in place

The National Coordinating Council for Medication Error Reporting and Prevention (NCCMERP) Entire dispensing process
Agency for Health Research and Quality (AHRQ) Incident = reaches patient Near miss Unsafe Condition
Institute for Safe Medication Practices (ISMP) Error, Near miss and close call (error happened/not
reached patient)
Alliance for Patient Medication Safety (APMS) Quality-related event (incident, near miss and unsafe
condition)
What is a Medication Error?

Near miss capture = successful ability to avoid disaster
What you do not measure, you cannot manage
“No news” is NOT
“good news”

= mistake/errormistake/error
Workflow Employees
Equipment
Technology
Swiss Cheese Effect
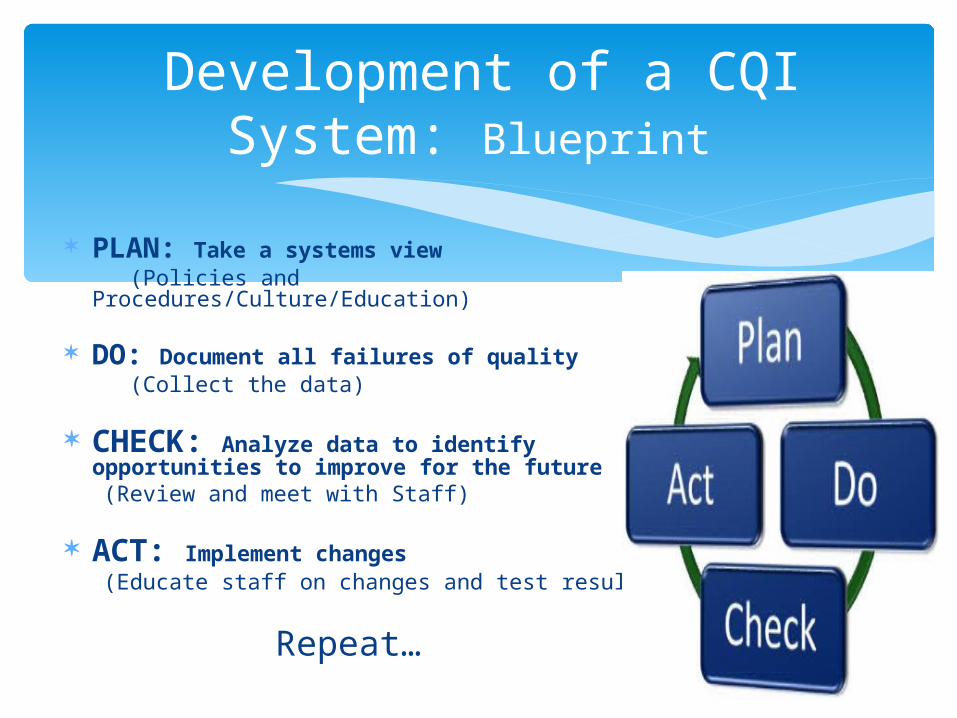
Development of a CQI System: Blueprint
PLAN: Take a systems view (Policies and Procedures/Culture/Education)
DO: Document all failures of quality (Collect the data)
CHECK: Analyze data to identify opportunities to improve for the future
(Review and meet with Staff)
ACT: Implement changes (Educate staff on changes and test results)
Repeat…

Pharmacy Quality Commitment®
~ PQC In store program pharmacies use in order to:
o Establish a quality conscious workflow o Identify, collect, and report Quality Related Events
(QREs)o Analyze QREs to identify process improvement
opportunities to improve workflow and decrease QREs
The APMS PSO provides :o Immediate access to the pharmacy’s reported patient
safety data in chart and graph formo Recommendations on best practices and workflow
processes to help reduce medication errors, improve medication use, and enhance patient safety and health outcomes

PQC helps you…..
Establish written CQI Policies and Procedures.
Ensure that staff CQI training and/or education is provided to all pharmacy personel
Ensure that QREs are documented, reported, and analyzed
Maintain security of patient safety data

CQI Verified Certificate

A. Commitment to program (already have!)
B. Create culture of safety
C. Develop Policy & Procedures/Standardization
D. Institute process for collection, analysis and improvement cycle
How to Start?

B. Create a Culture
of Safety
Culture of Safety

Negative
Dwells on the past
Threatening, insulting, punitive
Focuses on WHO made an error
Concludes erring individual has character flaws they need to correct
Individuals won’t willingly participate
Positive
Looks to the future
Open, blame-free, non-punitive
Focuses on HOW or WHAT in the system allowed error to occur
Realizes error is a reality and recognizes the opportunities to improve for the future
Creates blame-free, shame-free environment
Discussing Errors

ISMP Medication Safety Self Assessment Tool www.ismp.org
AHRQ Pharmacy Survey on Patient Safety Culture htpp://www.ahrq.gov/qual/patientsafetyculture/pharmsurvindex.htm
Semi-quantitative measures of the “current state” in each pharmacy.
Self Assessment Resources

C. Develop Policies
and Procedures/
Standardization

Policy: Pharmacy will actively participate in Continuous Quality Improvement
Designate an individual or individuals responsible for monitoring CQI Program compliance
Identify and document QREs Minimize impact of QREs on patients Analyze data collected in response to QREs to assess causes and any
contributing factors Use the findings of the analysis to formulate an appropriate response and
develop pharmacy systems and workflow processes designed to prevent QREs Provide ongoing education
Procedures:Employee Training Identification and Documentation of Quality Related Events
Root Cause Analysis (Investigative Analysis)
Process Improvements Records
QA Policies and Procedures(in Resource Area)
Basically….Review and sign. Educate Staff – Powerpoint in Resource Area
WHEN: When and how patient safety data enters the PSES space
WHERE: Where it is protected – “where the dome covers”
WHO: Who works with the data
WHAT: What data needs to be reported and what applies to it
HOW: How you report and handle the data
(Mark it all CONFIDENTIAL Patient Safety Work Product)
Patient Safety Evaluation System(PSES)
(in Resource Area)

• Organized workflow• Use a systematic approach
• reduce the likelihood that a quality related event will be made• “Now where was I?”• Less likely to miss a step that could lead to an incident that
reaches the patient
• Quality does not happen by chance, it is a result of quality habits
• Redundancy is positive• Process ingrained
You Can Fix the System
13
No longer asking yourself this !

D. Institute process for
collection, analysis and
improvement cycle

Quality Related Events (QREs) Incidents that reach the patient whether they caused
harm or not Near Misses Unsafe Conditions
Both are important to track and analyze
Type, Who, What, Where, How, When and whether it reached the patient
Collect!
RECORD
:

#s and letters for easy recording

Fictional data for illustration purposes only
Completed Form
Example
Record QREs, THEN transfer to
the internet to pharmacy’s PQC
site
1.Go to www.pqc.net
2.Enter Username
3.Enter Password







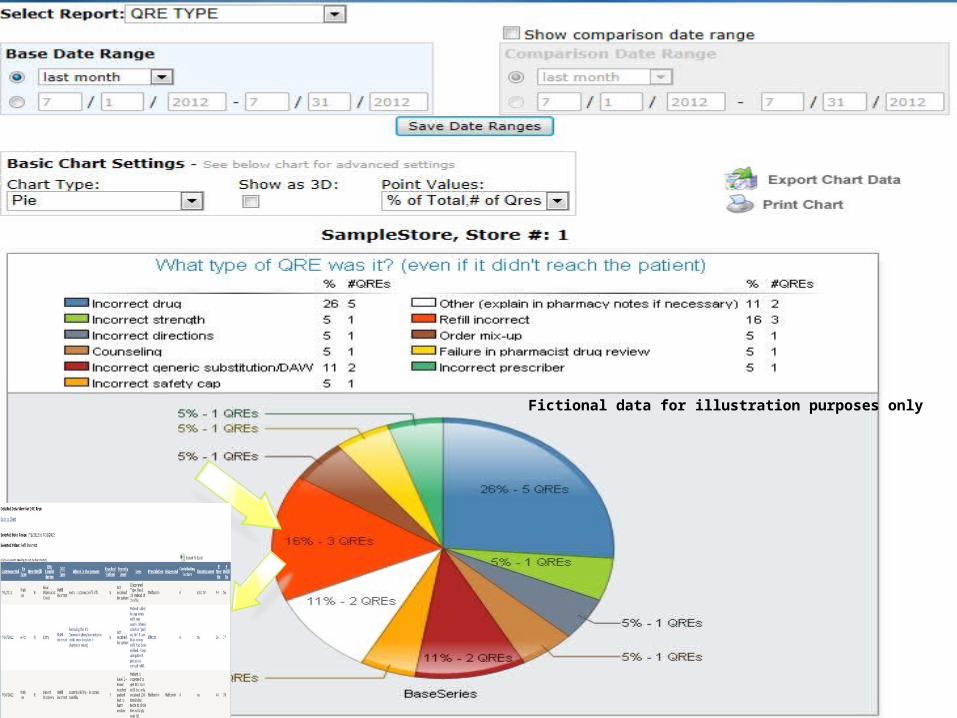
Fictional data for illustration purposes only

1. Login
2. Enter report on correct day
3. Close your pharmacy each day (# of fills and refills)
Review – to Report

QRE’s

Communication?
Training provided?
Had procedures been reviewed?
Staffing?
Work area?
Policy & Procedure followed?
How to analyze – questions to consider

Intensive Investigation vs Root Cause Analysis
Peer Review – “Intensive Investigation”
1.What happened?
a. What happened on that
particular day?
2.Why did it happen?
a.What made that
particular day different?
b. What usually happens?
c. What should have happened
according to policy and
procedure?


1. Gather Quality Related Event (QRE). 2. Describe the QRE3. WHAT happened? WHY? HOW?
4. Identify possible failures in the systems.5. Identify possible contributing factors 6. Where in workflow the QRE occurred 7. Classify and record the causal factors and system failures. 8. Identify improvement plans. What would prevent this error in
the future? What will be monitored to assure that the corrective action is working?
Peer Review


Process Improvement form
Date _______________Results of Peer Review ProcessProcess/Issue Identified Root Cause IdentifiedAction Planned Date to be implemented Follow up analysis scheduled Results found at follow-up
Patient Safety Work Product
Privileged and Confidential
Inadmissible as evidence and not subject to Discovery
* MARK all process improvement notes as PSWP and Secure this information in safe place in pharmacy or report directly to PSO

• Ideally will prevent the same event or minimize its occurrence
• PhysicalPhysical rather than proceduralInstall speed bumps instead of relying on speed limit sign
• PermanentPermanent rather than temporaryReplace equipment known to malfunction in the hands of “float” staff, instead of taping warnings or additional instructions on machine
Proposed actions should not burden people’s memory (i.e., “pay more attention next time”)
Actions and Changes


1. Positive Safety Culture2. Patient Safety Evaluation System3. Policies and Procedures4. Collect Data5. Analyze Data6. Implement New Process with Training
ReviewReview

Select Quality Supervisor
Review the training
Log in
Main Page > CQI Compliance Program Certification Enrollment
Complete Steps
Continue to report/Analyze
Implementation





www.medicationsafety.org APMS Web sitewww.pqc.net PQC Web site
Tara Modisett Executive Director APMS For assistance or questions email us at
[email protected] or [email protected] Toll free (866) 365-7472
Contact