


Pharmacotherapy of TUBERCULOSIS
107
PHARMACOTHERAPY OF TUBERCULOSIS By – Mr. Rahul P Kshirsagar M.Pharm (Ph.D) Assistant Professor Dept. of Pharmacology School of Pharmacy, Anurag Group of Institutions
-
Upload
rahulkshirsagar85 -
Category
Education
-
view
844 -
download
3
Transcript of Pharmacotherapy of TUBERCULOSIS

PHARMACOTHERAPY
OF
TUBERCULOSIS
By – Mr. Rahul P Kshirsagar M.Pharm (Ph.D)
Assistant Professor
Dept. of Pharmacology
School of Pharmacy, Anurag Group of Institutions

WHAT IS TB?
TB is a disease caused by
infection with a bacteria called
Mycobacterium tuberculosis.

HOW CAN YOU CATCH TB?
TB is spread through tiny drops
sprayed into the air when an infected
person coughs, sneezes, or speaks,
or another person breathes the air
into their lungs containing the TB
bacteria.

TUBERCULOSIS – THE FACTS
• 7. position of leading causes of deaths
• 1/3 of the world's population could be
infected
• > 80% can be cured
• prevention can be > 90% effective
Global tuberculosis control: WHO report 2011

TUBERCULOSIS – THE FACTS
• 1.45 million people died in 2010 due to TB
• equally to 3800 deaths per day
• 8.8 million new cases of TB in 2010
• Global incidence rate of 128/100 000
• Most cases occurred in
• Asia (59%) and
• Africa (26%)
WHO report 2011

ESTIMATED TB INCIDENCE RATES 2010
WHO report 2011

THE GLOBAL BURDEN OF TB IN 2010
IN RELATION TO HIV CO-INFECTION
Estimated number
of cases
Estimated number of
deaths
All forms of TB 8.8 Mio
(8.5–9.2 Mio)
1.45 Mio
(1.2–1.5 Mio)
HIV-associated TB 1.1 Mio (13%)*
(1.0–1.3 Mio)
0.35 Mio
(0.32–0.39 Mio)
WHO report 2011
*82% of TB cases among people livingwith HIV originate from the African region

ESTIMATED HIV PREVALENCE
IN NEW TB CASES 2010
WHO report 2011

TRENDS IN TB INCIDENCE RATES
Lawn and Zumla (2011) Lancet 378: 57

• M. tuberculosis causes most TB cases in U.S.
• Mycobacteria that cause TB:
• M. tuberculosis
• M. bovis
• M. africanum
• M. microti
• M. canetti
• Mycobacteria that do not cause TB
• e.g., M. avium complex
M. tuberculosis
ETIOLOGY - TYPES OF MYCOBACTERIA

CHARACTERISTICS OF M. TUBERCULOSIS
• Slightly curved, rod shaped
bacilli
• 0.2 - 0.5 microns in
diameter; 2 - 4 microns in
length
• Acid fast - resists
decolorization with
acid/alcohol
• Multiplies slowly (every 18
- 24 hrs)
• Thick lipid cell wall
• Can remain dormant
for decades
• Aerobic
• Non-motile

HOW IS TB TRANSMITTED?
• Person-to-person through
the air by a person with
TB disease of the lungs
Less frequently transmitted by:
• Ingestion of Mycobacterium bovis found in unpasteurized milk products
• Laboratory accident

TRANSMISSION OF M. TUBERCULOSIS
• One cough can
release 3,000 droplet
nuclei
• One sneeze can
release tens of
thousands of droplet
nuclei
• Millions of tubercle bacilli in lungs
(mainly in cavities)
• Coughing projects droplet nuclei
into the air that contain tubercle
bacilli

FATE OF M. TB AEROSOLS
• Large droplets settle to
the ground quickly
• Smaller droplets form
“droplet nuclei” of 1–5
µ in diameter
• Droplet nuclei can
remain airborne

PATHOGENESIS

TB PATHOGENESIS• Bacterial entry
• T Lymphocytes.
• Macrophages.
• Epitheloid cells.
• Proliferation.
• Central Necrosis.
• Giant cell formation.
• Fibrosis.

MORPHOLOGY OF GRANULOMA
1. Rounded tight collection of chronic inflammatory cells.
2. Central Caseous necrosis.
3. Active macrophages - epithelioid cells.
4. Outer layer of lymphocytes & fibroblasts.
5. Langhans giant cells – joined epithelioid cells.

TUBERCULOUS GRANULOMA

TB TRANSMISSION AND
PATHOGENESIS
Not everyone who is exposed to TB will become infected
No infection (70%)
Adequate Immunity
Non-specific immunity
Inadequate Immunity
Infection (30%)
EXPOSURE

THE CHANCE OF INFECTION INCREASES…
• When the concentration of TB bacteria circulating in the air
is greater
• Coughing; smear +;
• Exposure occurs indoors
–Poor air circulation and ventilation; small, enclosed
space
–Poor or no access to sunlight (UV light)

THE CHANCE OF INFECTION INCREASES…(2)
• The greater the time spent with the infectious person or
breathing in air with infectious particles

TB GERMS CANNOT BE SPREAD BY:• Sharing dishes and utensils
• Using towels and linens
• Handling food
• Sharing cell phones
• Touching computer keyboard

SPREAD OF TB TO OTHER PARTS OF THE
BODY1. Lungs (85% all cases)
2. Pleura
3. Central nervous system(e.g., brain, meninges)
4. Lymph nodes
5. Genitourinary system
6. Bones and joints
7. Disseminated (e.g., miliary)
© ITECH, 2006

TB CAN AFFECT ANY PART OF YOUR BODY: EXTRA PULMONARY TB
Pleura
Lymph Node
Brain
Spine

CELL-MEDIATED IMMUNE RESPONSE
Special immune cells
form a hard shell (in
this example, bacilli are
in the lungs)
Source: CDC, 2001

Latent TB Infection (LTBI)
Person:
• Not ill
• Not contagious
• Normal chest x-ray
• Usually the tuberculin skin test is
positive
Germs:
• Sleeping but still alive
• Surrounded (walled off) by body’s
immune system

TB TRANSMISSION AND PATHOGENESIS
(2)
Immunologic defenses
No infection (70%)
Adequate Immunity
Non-specific immunity
Inadequate Immunity
Infection (30%)
Inadequate Defenses
Early Progression
(5%)
Adequate Defenses
Containment(95%)
EXPOSURE

REACTIVATION
Hard shell breaks down
and tubercle bacilli
escape and multiply
(in this example, TB
disease develops in the
lungs)
Source: CDC, 2001

ACTIVE TB DISEASE
Granuloma breaks down and tubercle escape and multiply
TBGerms:
• Awake and multiplying
• Cause damage to the lungs
Person:
• Most often feels sick
• Contagious (before TB treatment started)
• Usually have a positive tuberculin skin
test
• Chest X-ray is often abnormal (with
pulmonary TB)

TB TRANSMISSION AND PATHOGENESIS (3)
Immunologic defenses
Continued
containment
(90%)
Adequate Defenses
Immunologic defenses
No infection (70%)
Adequate Immunity
Non-specific immunity
Inadequate Immunity
Infection (30%)
Inadequate Defenses
Early Progression
(5%)
Adequate Defenses
Containment(95%)
EXPOSURE
Inadequate Defenses
Late progression (5%)

TB INFECTION & DISEASETHERE ARE 2 CATEGORIES OF TB: LATENT & ACTIVE
TB infection of the lungs can fall into 2 categories of disease: Latent TB or Active TB.
Latent TB means a person is infected by TB bacteria, but cannot infect others, and is not coughing or appearing sick.
Latent TB means the body’s immune system has contained the infection.

TB - INFECTION & DISEASE CATEGORIES OF TB - LATENT
Persons with latent TB are
identified by a positive skin test
(PPD).
Persons who are not infected
with Mycobacterium
tuberculosis have a negative
skin test (PPD).

TB - INFECTION & DISEASECATEGORIES OF TB - LATENT
• When a person with a previously negative PPD, converts to a
positive PPD, the conversion indicates recent infection with
M. tuberculosis.

TB - INFECTION & DISEASECATEGORIES OF TB - ACTIVE
Active pulmonary and laryngeal TB means a person infected
with the TB bacteria is sick and can infect others unless they
are taking medicine prescribed by their physician to treat TB.

TB - INFECTION & DISEASECATEGORIES OF TB - ACTIVE
Persons with active TB disease
usually have some of the following
symptoms: cough ( 3 weeks or
more), feel weak, have a fever, lose
weight, experience night sweats,
cough up blood, or have chest pain
when coughing.

TB - INFECTION & DISEASE CATEGORIES OF TB - ACTIVE
Persons with active TB need to take their
medications as prescribed in order to treat
the disease and prevent the spread to
others.

DIAGNOSIS OF TB
• Clinical features are not confirmatory.
• Zeil Nielson Stain
• Adenosine deaminase test
• Culture most sensitive and specific test.
• Conventional Lowenstein Jensen media 3-6 wks.
• Automated techniques within 9-16 days
• PCR is available, but should only be performed by
experienced laboratories
• Mantoux test

AFB - ZEIL-NIELSON STAIN


COLONY MORPHOLOGY – LJ SLANT

MANTOUX TEST
• Infection with mycobacterium tuberculosis leads delayed
hypersensitivity reaction which can be detected by Mantoux
test
• About 2 to 4 weeks after infection, intracutaneous injection of
purified protein derivative (PPD) of M.tuberculosis induces a
visible and palpable induration that peaks in 48 to 72 hours

PPD TUBERCULIN TESTING
• Sub cutaneous
• Weal formation
• Itching – no scratch.
• Read after 72 hours.
• Induration size.
• 5-10-15mm
• (i) Induration less than 5 mm – no exposure to tubercular
bacilli.
• (ii) Induration between 5-9 mm – this can be due to atypical
mycobacteria or BCG vaccination. It may suggest infection in
immunocompromised children such as HIV infection or other
immunosupression;
• (iii) Induation 10 mm or more – an induration of 10 mm or
more at 48-72 hours in a child with symptoms of tuberculosis
should be interpreted as tubercular disease

PPD RESULT AFTER – 72 HOURS.

TREATMENT FOR LATENT TBWHY DO YOU NEED TREATMENT FOR LATENT TB IF YOU DO NOT HAVE
THE DISEASE?
Medication is given to prevent
the Latent TB from becoming
Active TB disease.
Preventive treatment reduces
the risk of getting active TB by
more then 90%.

TREATMENT OF T.B.
• Divided into chemoprophylaxis and treatment of active
disease.
• Careful diagnostic studies must always precede therapy.

CHEMOPROPHYLAXIS
• To prevent clinically active disease in people already
infected.
• Given only to those who will derive the greatest benefit
and the least risk.

CHEMOPROPHYLAXIS
• 300 mg Isoniazid once daily for 6-12 months.

TREATMENT OF ACTIVE T.B.
• First line drugs (used in the initial treatment of
T.B.) : Isoniazid, Rifampin, Streptomycin,
Ethambutol And Pyrazinamide.

TREATMENT OF ACTIVE T.B.
• Secondary agents: PAS, Ethionamide, Amikacin,
Kanamycin, Capreomycin, Cycloserine,
Ciprofloxacin, Levofloxacin And Clofazimine.

MECHANISM OF ACTION OF
ANTITUBERCULOSIS AGENTS
• Drugs which interfere with mycolic acid synthesis
• Drugs which inhibit nucleic acid synthesis
• Drugs inhibiting protein synthesis
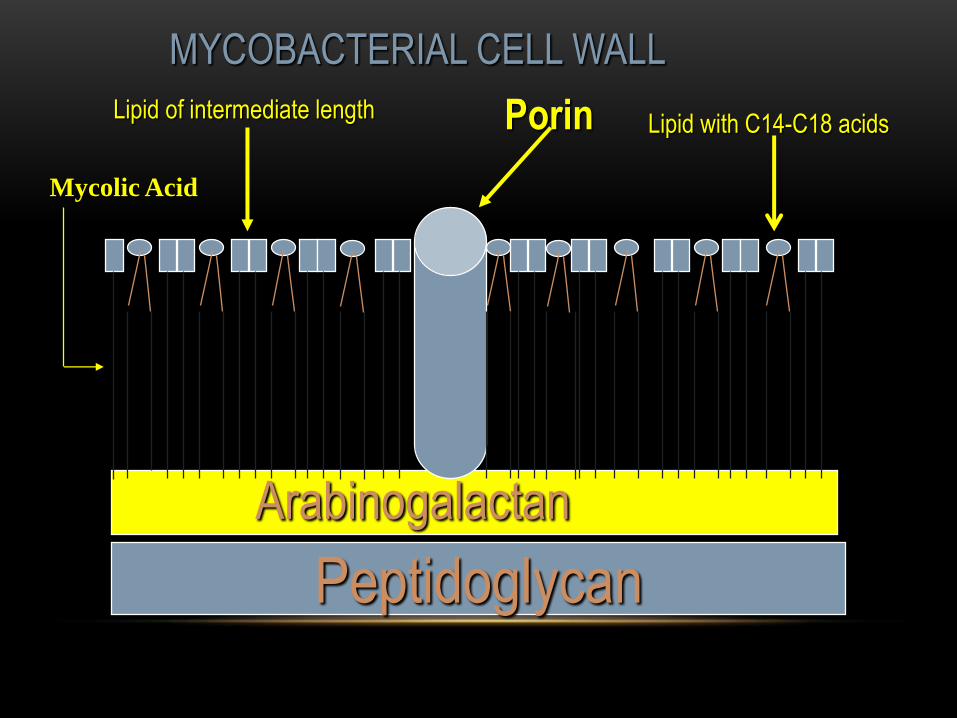
Peptidoglycan
Porin
Arabinogalactan
Mycolic Acid
Lipid of intermediate lengthLipid with C14-C18 acids
MYCOBACTERIAL CELL WALL

ISONIAZID-MECHANISM OF ACTION
• Interferes with biosynthesis of cell wall mycolic acids.
• Mycolate depleted cell walls are structurally weak.

Isoniazid
(Prodrug)
Active
Form
Catalase/Peroxidase
katG

INH MECHANISM OF ACTION
• InhA gene encodes an enoyl-ACP reductase of fatty acidsynthase II which converts 2 -unsaturated to saturated fattyacids on the pathway to mycolic acid biosynthesis.
• Activated INH inhibits this enzyme.

Peptidoglycan
Porin
Arabinogalactan
Mycolic Acid
Lipid of intermediate lengthLipid with C14-C18 acids
Mycobacterial Cell Wall
INH

RESISTANCE
• Mutations in the katG gene can lead to loss of catalase-
peroxidase activity.
• Resistance also maps to mutations in four other genes
including inhA

RESISTANCE
• Overall incidence of resistance is higher in certain ethnic
groups such as African Americans, Mexican Americans
and Indochinese refugees.

ETHAMBUTOL-MECHANISM OF
ACTION
• It is not bactericidal.
• Inhibits synthesis of the mycobacterial cell wall.

MECHANISM OF ACTION
• It is an inhibitor of mycobacterial arabinosyl transferases
(encoded by the embAB genes).
• Arabinoglycan an essential component of the cell wall.

Peptidoglycan
Porin
Arabinogalactan
Mycolic Acid
Lipid of intermediate lengthLipid with C14-C18 acids
MYCOBACTERIAL CELL WALL
Ethambutol

RESISTANCE
• Mutations in the emb genes.

PYRAZINAMIDE-MECHANISM OF
ACTION
• PZA POA (pyrazinoic acid)pyrazinamidase
Occurs mostly in the liver.

MECHANISM OF ACTION
• Inhibits fatty acid synthetase I of Mycobacterium
tuberculosis.

Short chain fatty acid precursors
Pyrazinamide

RESISTANCE
• Mutations in the pncA gene which results in impairment in
the conversion of PZA to its active form.

DRUGS INHIBITING NUCLEIC ACID
SYNTHESIS
• Rifampin

RESISTANCE
• Results from an alteration in the polymerase enzyme (mutation
in the rpoB gene).

STREPTOMYCIN-ANTI TB ACTIVITY
• Most strains of M.Tuberculosis are sensitive.
• Bactericidal only against the extracellular tuberculosis
bacilli.
• Overall only suppressive.

RESISTANCE
• Major problem with streptomycin use in T.B.
• Combination therapy will delay or prevent resistance.

THERAPEUTIC USES IN T.B.
• It is used in drug resistant disease.
• More serious forms of T.B. (disseminated T.B. or
meningitis).


ANTITUBERCULAR ACTIVITY
• Bactericidal vs actively growing tubercle bacilli .
• Also bactericidal vs intracellular bacteria.
• Poor activity against atypical organisms.

TREATMENT OF ACTIVE T.B.
• Therapy requires at least two effective drugs
concurrently.

TREATMENT OF ACTIVE T.B.
• If the treatment is appropriate improvement is usually
seen within 2 weeks.
• Continue treatment for at least 3-6 months after the
sputum becomes negative.

TREATMENT OF ACTIVE T.B.
• Never use 1 drug and never add a single drug to
a failing regimen.

TREATMENT OF ACTIVE T.B.
• Minimum length of therapy is 6-9 months.

TREATMENT OF ACTIVE T.B.
• Initiation phase of 2 months.
• Continuation phase of 4-7 months.

TREATMENT OF ACTIVE T.B.
• Initial therapy is a 4 drug regimen of INH, rifampin,
pyrazinamide and ethambutol.
• For patients with drug-susceptible disease the
pyrazinamide can be discontinued after 2 months.
• Ethambutol can also be discontinued.

TREATMENT OF ACTIVE T.B.
• Combining daily therapy with intermittent therapy.

INTERMITTENT THERAPY
• Daily therapy for 2 weeks (INH, rifampin, pyrazinamide
and streptomycin) followed by therapy 2 times a week for
six weeks. Then INH + Rifampin 2x weekly for 16 weeks.

DOT

Directly Observed Therapy (“DOT”) –
DOT is especially critical for patients with drug-
resistant TB, HIV-infected patients, and those on intermittent
treatment regimens (i.e., 2 or 3 times weekly).
What is DOT?
DOT means that a trained health care worker or other
designated individual (excluding a family member) provides
the prescribed TB drugs and watches the patient swallow
every dose.

Why use DOT?
• We cannot predict who will take medications as directed, and
who will not. People from all social classes, educational
backgrounds, ages, genders, and ethnicities can have
problems taking medications correctly.
• Studies show that 86-90% of patients receiving DOT complete
therapy, compared to 61% for those on self-administered
therapy.
• DOT helps patients to finish TB therapy as quickly as possible,
without unnecessary gaps.
• DOT helps to prevent TB from spreading to others.
• DOT decreases the risk of drug-resistance resulting from
erratic or incomplete treatment.
• DOT decreases the chances of treatment failure and relapse.

HIV COUNSELING
All persons with suspected and confirmed TB disease
should be offered HIV counseling and blood testing, in
addition to treatment.
This is because TB is more likely to occur among HIV
positive individuals.

HIV COUNSELING
Treatment recommendations may differ for HIV infected
persons.
It is best to offer HIV counseling and testing in the health care
facility.
Follow up testing and counseling is essential.

FUNDAMENTALS OF TB
INFECTION CONTROL PRACTICES
Identify persons with active TB early.
Initiate effective and appropriate isolation of known or suspected TB cases.
Initiate effective anti-TB treatment promptly.

FUNDAMENTALS OF TB
INFECTION CONTROL PRACTICES
Employees should use N95 respirators for any contact with
patients suspected of having TB.
Screen persons at high risk for TB and provide preventative
therapy if infected.

FUNDAMENTALS OF TB
INFECTION CONTROL PRACTICES
Identify and evaluate persons and
health care workers exposed to
infectious TB.
Screen health care workers for
skin test conversions.
Conduct surveillance for TB
cases among patients and
healthcare workers.

INITIATE
AIRBORNE PRECAUTIONS WHEN:
A patient is suspected of having TB.
A patient has a rule-out diagnosis of TB.
A patient has a positive AFB smear.
A patient has a significant skin test reaction.
A patient is at high risk for TB, and has pneumonia, a cough
or bloody sputum.

ISOLATION ROOMS
Isolation rooms are necessary to prevent the spread of TB.
Isolation rooms should have at least 6 total air exchanges per
hour.
Isolation rooms must have air that flows from the hallway into
the isolation room (negative pressure).

ISOLATION ROOMS
Doors to isolation rooms must remain closed at all times to
maintain the negative pressure.
The number of healthcare workers entering an isolation room
should be limited.

ISOLATION ROOMS
When isolation rooms are in use, the air flow must be
checked daily.
P1
P2

WHAT FACTORS CONTRIBUTE TO TB OUTBREAKS IN
HEALTHCARE FACILITIES?
Lack of compliance with infection
control practices to control the
transmission of TB.
Healthcare facilities which are
providing services to increased
numbers of people with TB and HIV
infection.

WHAT FACTORS CONTRIBUTE TO TB OUTBREAKS IN
HEALTHCARE FACILITIES?
Multi-drug resistant TB cases are on the rise.
Lack of using a respirator mask when taking care of patients
with active TB.
Lack of suspicion that some patients are at risk for TB.

AS A HEALTHCARE WORKER, HOW CAN I PROTECT
MYSELF FROM BEING EXPOSED?
Have your skin test performed at least once a year to determine your TB status.
Always wear personal protective equipment (N95) when taking care of patients with active or suspected TB. Personal protective equipment includes a respirator (N95) and may include a gown and gloves.

AS A HEALTHCARE WORKER, HOW CAN I PROTECT
MYSELF FROM BEING EXPOSED?
Instruct your patients to cover their mouth when coughing and
do not transport patients with TB throughout the hospital
unless they are wearing a mask.

AS A HEALTHCARE WORKER, HOW CAN I PROTECT
MYSELF FROM BEING EXPOSED?
Protect yourself in the community by being more aware
of the disease and its transmission.
Patients with active TB or suspected of having TB should
be placed in an isolation room until it is determined that
this is no longer necessary.

OCCUPATIONAL HEALTH & SAFETY
PROTOCOLS FOR MONITORING TB
All applicants are screened for TB.
All employees are screened annually for TB, or more
frequently if necessary.
Employees exposed to patients with active TB will be
identified and followed through Employee Health.

FIT TESTING FOR N95 RESPIRATORSWHAT IS FIT TESTING AND WHY MUST IT BE DONE?
Fit testing determines whether a healthcare worker can
achieve an adequate facial seal with a particular respirator.
(N95)
An appropriately fitted respirator (mask) will prevent the
transmission of TB to the healthcare worker.

FIT TESTINGWHAT IS FIT TESTING AND WHY MUST IT BE DONE?
Fit testing must be done prior to the initial use of a respirator
mask.
Each time a respirator is worn the healthcare worker should
ensure it fits tightly over the nose and mouth.

PATIENT EDUCATION
Patient education is an essential component to prevent the
spread of TB.
TB patients should be taught to use tissues to cover coughs
and sneezes.
Tissues should be disposed appropriately and not left on
counter tops.

PATIENT EDUCATION
A surgical mask must be worn by a TB patient
whenever they leave the isolation room.
Visitors of a TB patient must wear a respirator
but are not required to be tested.

EVEN IF A SKIN TEST IS NEGATIVE…..
Chiclls
FFeverTHINK TB !
Chills
Fatigue
Difficulty
in
Breathing
Anorexia
Loss
of Appetite
Night sweats
Coughing
up Blood


















![Pharmacotherapy III - جامعة نزوى · peritonitis or diabetic foot infection. ... [TB] Mycobacterium tuberculosis Mycobacterium avium Acid-Fast Stain (AFB) Fungi Aspergillusfumigatus,](https://static.fdocuments.in/doc/165x107/5c80852109d3f2a2228cfcb9/pharmacotherapy-iii-peritonitis-or-diabetic-foot-infection.jpg)