
Pharmacology of the endocrine pancreas -...
48
Pharmacology of the endocrine pancreas 1 Tri Widyawati – Datten Bangun Pharmacology and Therapeutic Department School of Medicine Universitas Sumatera Utara 2008
Transcript of Pharmacology of the endocrine pancreas -...
Pharmacology of the endocrine pancreas
1
Tri Widyawati – Datten BangunPharmacology and Therapeutic Department School of Medicine
Universitas Sumatera Utara
2008
2

An illustration…….
At her annual check up, 55-years old Mrs Sweetie complains of fatique
and frequent urination (polyuria), even at night. She also reports drinking
large volumes of fluids (polydipsia) to quench her thirst. Although these symptoms have been ‘going on for a while’ and are getting worse, Mrs.
Sweetie has difficulty pinpointing their exact onset. She denies other
urinary symptoms such as pain on urination, blood in her urine, dribbling, and incontinence. Her past medical history is remarkable for
3
and incontinence. Her past medical history is remarkable for hyperlipidemia of 10 years duration. Both of her parents died of coronary
heart disease in their early 60s.
On physical examination, Mrs Sweetie is moderately obese but otherwise appears normal. Glucose is detected in her urine, but proteins and
ketones are not. Mrs. Sweetie’s blood tests are significant for elevated
glucose (240 mg/dl), elevated total cholesterol (340 mg/dl), and elevated HbA1c ( a measure of glucose colavently bound to hemoglobin) (9,2%).
The physician discusses with Mrs Sweetie the importance of decreasing her caloric intake and increasing her exercise to improve her metabolic state. The physician also prescribes metformin ( a biguanide) for Mrs. Sweetie’s diabetes.

Apollonius (250 SM, Memphis) :
• Diabetes = “untuk menggunakan” atau “mengeringkan”
• (harfiah) = “siphon” atau mengalirkan ⇒⇒⇒⇒ volume urin besar
• Mellitus = bahasa latin dari madu = sweet ⇒⇒⇒⇒ ada glukosa dalam urin
4
Diabetes Mellitus : a group of diseases characterized by high levels of blood glucoseresulting from defects in insulin production, insulin action, or both

5

Physiologic and Pharmacologic Regulation of Glucose Homeostasis
GITDietary complex carbohydrates
Glucose
αααα-glucosidase
inhibitors β β β β cell
Other tissues
Metabolism
Glucosidases
Glucose
(from GIT
& liver)
To tissues To tissues
Endogenous insulin
(from ββββ cell) or
Exogenous insulin
Glucose Metabolism
Insulin
secretionATP
DiazoxideSulfonylureas,
meglitinides
Blood
6
Glucose Glycogen
InsulinInsulinLiver cell
Insulin
Adipose cell
glucose Triglyceride
PPARγγγγThiazolidinediones
GlucoseGlycogen
GlucoseGlucagon
Gluconeogenesis
Biguanides
Muscle
cell
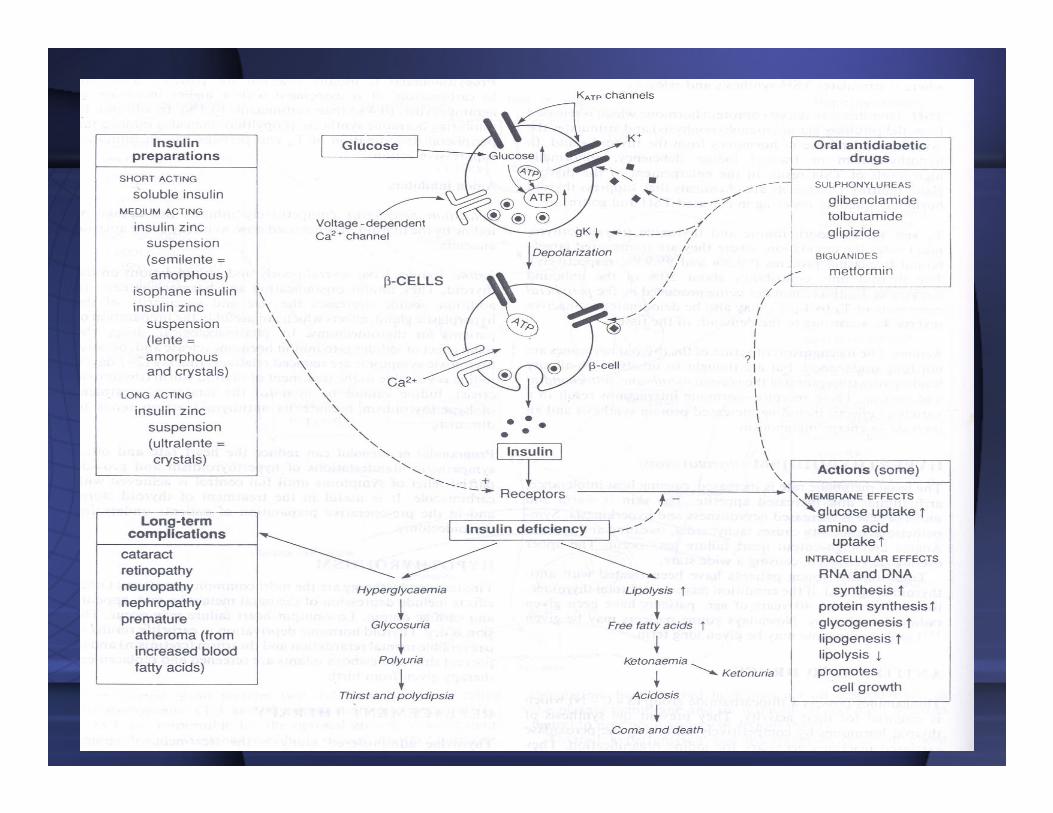
Dietary complex CH are broken down to simple sugars in the GIT by the action of glucosidases; simple sugar then absorbed by GI epithelial cells and
transported into the bloodstream. Glucose in the blood is taken up by all metabolically active tissues in the body. In pancreatic β cells, glucose metabolism ↑levels of cytosolic ATP, which stimulates insulin secretion. Insulin then acts on plasma membrane insulin receptors in target tissues (muscle, adipose, liver)
to ↑ glucose uptake and storage as glycogen or TG. Glucose is also taken up by other cells and tissues to fuel metab. In muscle cells, ins. Promotes
glucose storage as glycogen. In adipose cells, ins. Promotes glucose conversion to TG. Peroxisme proliferator-activated rec’r γ (PPARγ) also promotes the
conversion of glucose to TG in adipose cells. In liver cells, insulin promotes glucose storage as glycogen. Glucagon promotes both the conversion of
glycogen back to glucose and gluconeogenesis; glucose generated from glycogen or by gluconeogenesis is transported out of the liver cell into the
bloodstream. Pharmacologic interventions that ↓ blood gluc. Levels include : inhibiting intestinal α-glucosidase; administering exogenous ins; using
sulfonylurea or meglitinides to augment secretion of insulin by β cells; and using biguanides or thiazolidinediones to enhance the action of insulin in liver or
adipose cells, respectively. Diazoxide inhibits insulin scretion from pancreatic β cells.

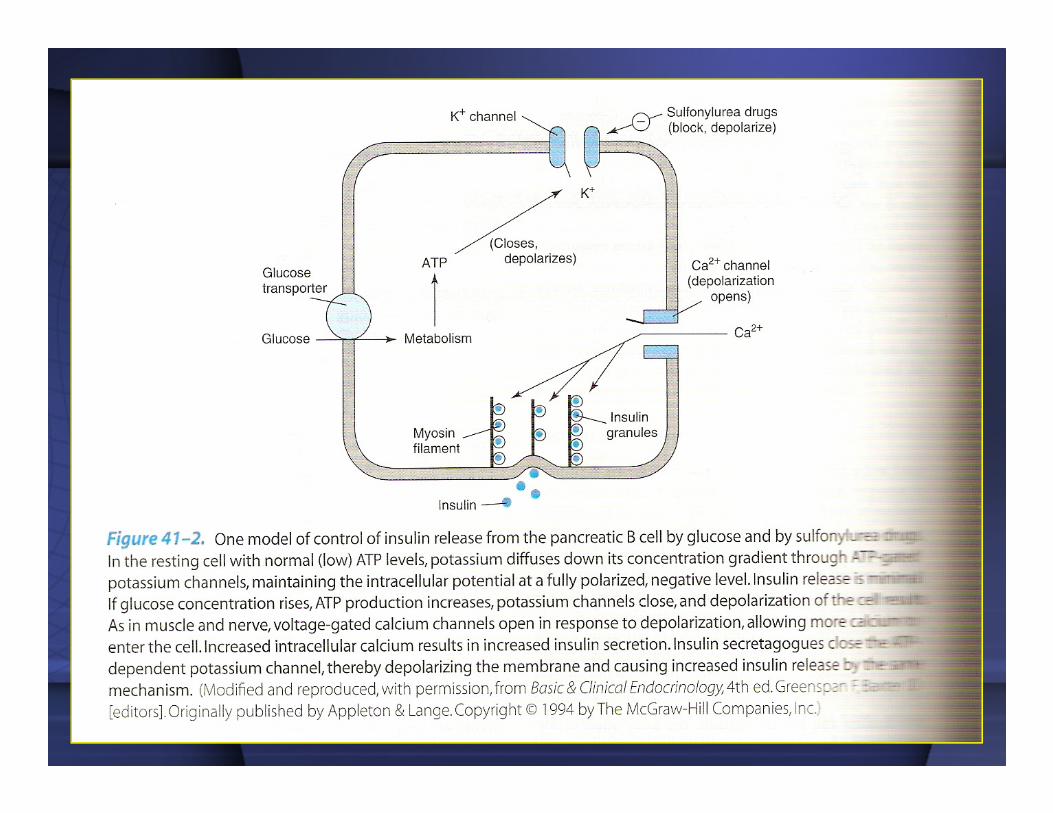
Mekanisme intrasel sekresi insulin oleh βcellsINSULIN
1) Glukosa masuk ke βcells dengan bantuan glucose transporters
(GLUT2).
2) Di dalam βcells glukosa difosforilasi ⇒
glucose-6 phosphate yang
dimetabolisme menghasilkan ATP
7
dimetabolisme menghasilkan ATP (glycolysis, mitochondria).
3) ↑ rasio ATP/ADP ratio ⇒ tertutupnya
ATP sensitive K+ channels,membrane
depolarization dan membuka voltage-
dependent Ca2+ channels.
4) ↑Ca2+intrasellular ⇒ exositosis dari insulinsecretory granules.
8
9

10
� Diet : medical nutrition therapy
� Aktivitas Fisik/OR
� Farmakoterapi
� Kontrol BB
� Self-monitoring of blood glucose (SMBG)
Penatalaksanaan
11
� Self-monitoring of blood glucose (SMBG)
� Patient self-management education
KEBERHASILAN MANAJEMEN
ASPEK METABOLIK DARI DM

Insulin Replacement Therapy
Farmakoterapi
1. Insulin dependent group (type 1) :
- virtually no insulin secretion
- depends on administration of exogenous insulin
12
- depends on administration of exogenous insulin
2. Type 2 :
- most type 2 diabetics do not require exogenous insulin
for survival, but many need exogenous supplementation
of their endogenous secretion to achieve optimum
health
- 20% ⇒ taking insulin
Characteristics of Available Insulin Preparations
1. Rapid acting :
- very fast onset & short duration
- duration of action : 3-5 hours
4 principal types of insulins :
13
- duration of action : 3-5 hours
2. Short acting: rapid onset of action :
- onset of action : within 30 minutes
- duration of action : 5-8 hours
3. Intermediate acting
4. Long acting : slow onset of action
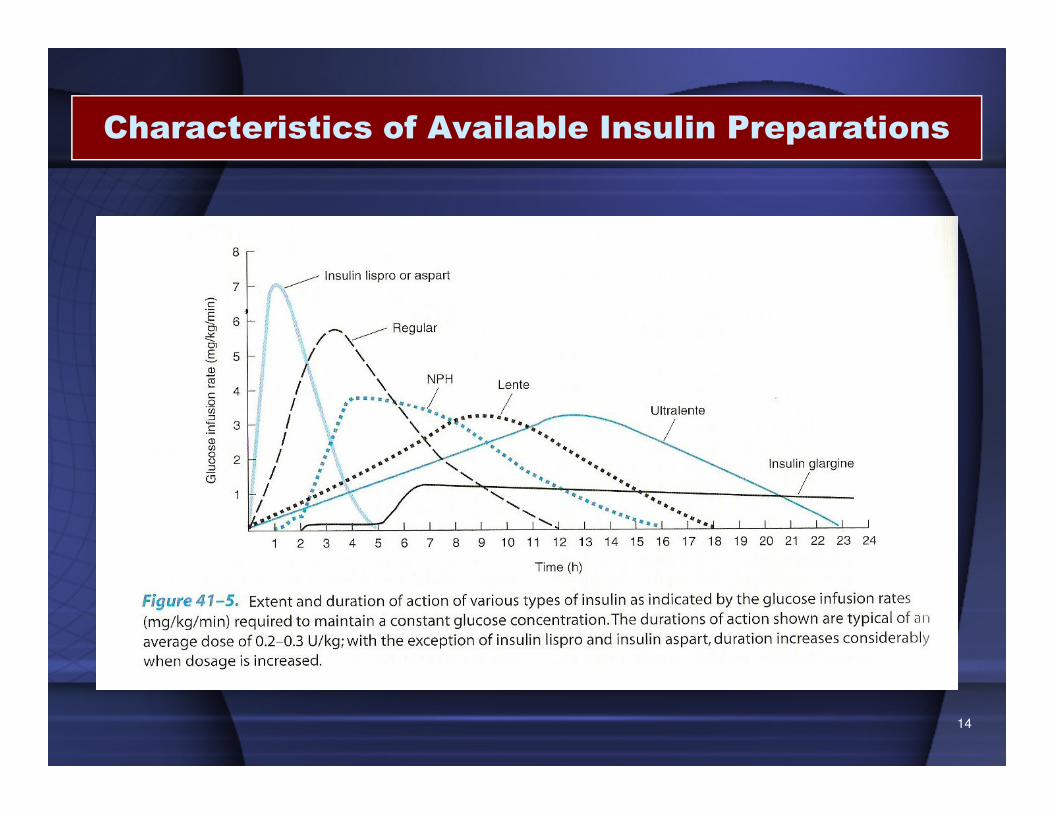
Characteristics of Available Insulin Preparations
14
15
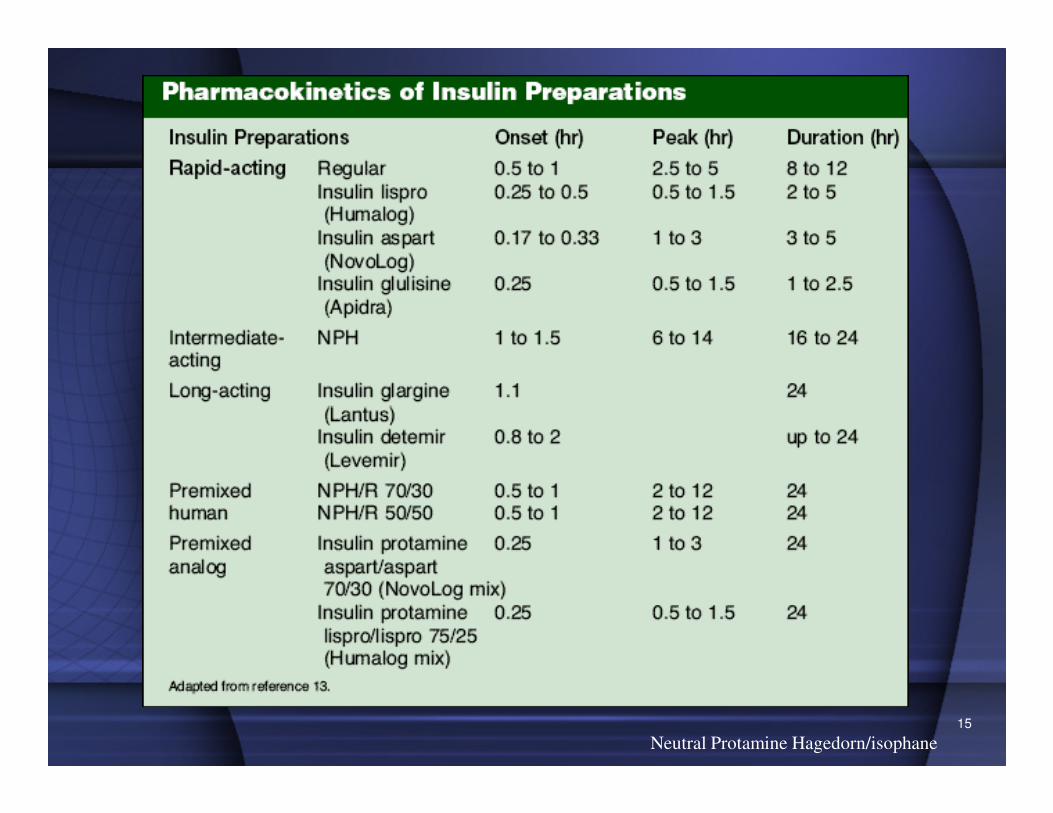
Neutral Protamine Hagedorn/isophane
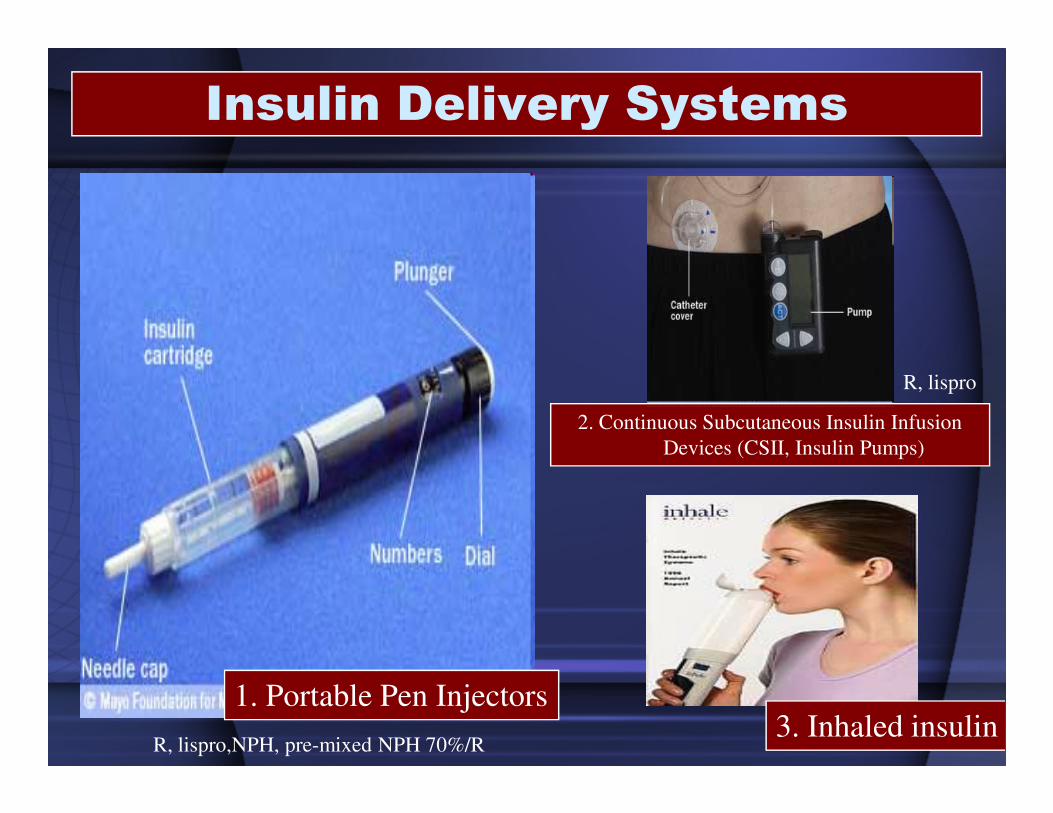
Insulin Delivery Systems
R, lispro
16
1. Portable Pen Injectors
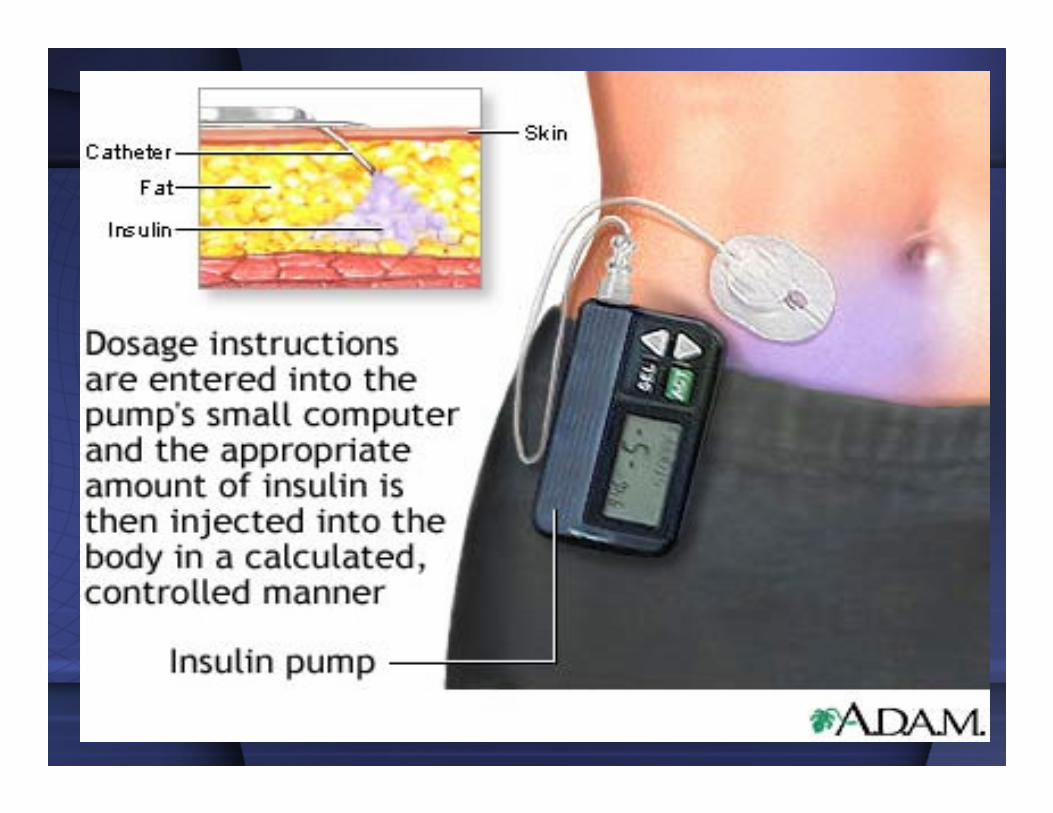
2. Continuous Subcutaneous Insulin Infusion
Devices (CSII, Insulin Pumps)
3. Inhaled insulinR, lispro,NPH, pre-mixed NPH 70%/R
17
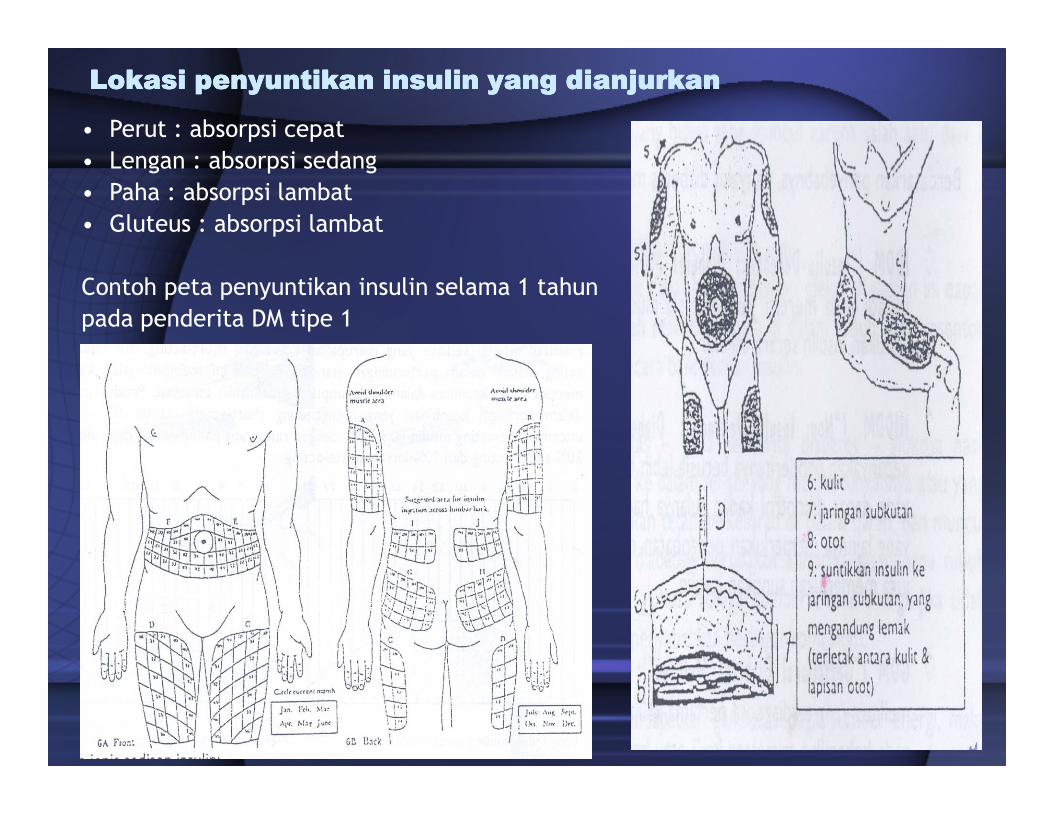
• Perut : absorpsi cepat
• Lengan : absorpsi sedang
• Paha : absorpsi lambat
• Gluteus : absorpsi lambat
Contoh peta penyuntikan insulin selama 1 tahun
pada penderita DM tipe 1
Lokasi penyuntikan insulin yang dianjurkanLokasi penyuntikan insulin yang dianjurkanLokasi penyuntikan insulin yang dianjurkanLokasi penyuntikan insulin yang dianjurkan
18
Complications of Insulin Therapy
1. Hypoglycemia
2. Immunopathology of Insulin Therapy
19
2. Immunopathology of Insulin Therapy
3. Lipodystrophy at injection sites

Complications of Insulin Therapy
1. Hypoglycemia
- Delay in taking a meal
- Inadequate carbohydrate consumed
- Physical over exertion
causes
20
- Dose of insulin ⇒ too large for immediate needs
- Autonomic hyperactivity :
• Sympathetic : tachycardia, palpitations, sweating, tremulousness
• Parasympathetic : nausea, hunger
- Convulsions
- Coma
signs

Complications of Insulin Therapy
1. Hypoglycemia
treatment
21
- Glucose administration :
• Simple sugar/glucose
• Liquid form

Complications of Insulin Therapy
1. Hypoglycemia
- Mild hypoglycemia : conscious and able to swallow :
• Orange juice
• Glucose gel
• Any sugar containing beverage/food
treatment
22
• Any sugar containing beverage/food
- Severe hypoglycemia : unconsciousness/stupor :
• 20-50 ml of 50% glucose solution (IV infusion over 2-3 minutes)
• 1 mg glucagon : IM/SC
• small amounts of honey or syrup : buccal pouch
Contraindication : oral feeding

Complications of Insulin Therapy
- Insulin allergy :
• Rare condition
• Urticaria
• Anaphylaxis
• Highly purified and human insulins : ↓ insulin allergy
treatment
2. Immunopathology of Insulin Therapy
23
• Highly purified and human insulins : ↓ insulin allergy
- Immune insulin resistance :
• A low titer of circulating IgG anti-insulin antibodies that neutralize
the action of insulin to a negligable extent develops in most insulin-
treated patients.
• Rarely, the titer of insulin antibodies will lead to insulin resistance
and may be associated with other systemic autoimmune processes
such as lupus erythematosus

Complications of Insulin Therapy
3. Lipodystrophy at injection sites
- Atrophy
- Hyperthrophy
24
- Hyperthrophy
Corrected by :
- avoidance of that spesific injection
- liposuction

Oral Antidiabetic Agents
25

Major Classes of Medications
1. Drugs that stimulate the pancreas to make more insulin (Insulin secretagogues)
2. Drugs that sensitize the body to insulin
SulfonylureasMeglitinides
26
2. Drugs that sensitize the body to insulin and/or control hepatic glucose production (Insulin sensitizers)
3. Drugs that slow the absorption of starches
ThiazolidinedionesBiguanides
Alpha-glucosidase inhibitors
Oral Antidiabetic Agents
Insulin secretagogues : sulfonylureas
• Mechanism of Action :
- To increase the insulin release from pancreatic cells
- Reduction of serum glucagon concentrations
27
- Reduction of serum glucagon concentrations
- Potassium channel closure in extrapancreatic
tissues

Sulfonylureas
♦ 1st generation
- tolbutamide
- tolazamide
- chlorpropamide∴∴∴∴ may become dislodged ���� delayed activity
28
♦ 2nd generation
– Glipizide
– glyburide
- glimepiride
Re
l. P
ote
ncy
Oral Antidiabetic Agents
Insulin secretagogues : sulfonylureas
1. Tolbutamide :
- well absorbed but rapidly metabolized in the liver
- duration of effect : short
1st generation
29
- duration of effect : short
- t1/2 : 4-5 hours
- safest for elderly diabetics
- dicumarol, phenylbutazone, some sulfonamide
⇒ inhibit the metabolism tolbutamide
⇒ hypoglycemia

Oral Antidiabetic Agents
Insulin secretagogues : sulfonylureas
2. Chlorpropamide :
1st generation
- slowly metabolized
- t1/2 : 32 hours
- 20-30% excreted unchanged in the urine
30
- 20-30% excreted unchanged in the urine
- drug int. : dicumarol, phenylbutazone, some sulfonamide
- contraindicated : hepatic /renal insufficiency, elderly patients
- dosages > 500 mg daily increase the risk of jaundice
- side effects : hypoglicemia, hyperemic flush, hematologic
toxicity ( transient leukopenia, thrombocytopenia)
~ 1%

Oral Antidiabetic Agents
Insulin secretagogues : sulfonylureas
2. Tolazamide :
1st generation
31
- more slowly absorbed than the other sulfonylurea
- t1/2 : 7 hours
- metabolized to several compounds that retain hypoglycemia
- dosages > 500 mg daily ~ divided twice daily

Oral Antidiabetic Agents
Insulin secretagogues : sulfonylureas
1. Glyburide /glybenclamide :
2 nd generation• fewer side effects
• fewer drug interaction
32
1. Glyburide /glybenclamide :
- metabolized in the liver into products with very low hypoglycemic
activity
- usual starting dosage : 2,5 mg/d or less
- average maintenance dosage : 5-10 mg/d single morning dose
- maintenace dosages higher than 20 mg/d are not recommended
- adverse effects : hypoglycemia, flushing
- contraindication : hepatic impairment, renal insufficiency

Oral Antidiabetic Agents
Insulin secretagogues : sulfonylureas
2. Glipizide (Glucotrol ®)
2 nd generation
- shortest half life : 2-4 hours
- 30 minutes before breakfast
33
- 30 minutes before breakfast
- 90% metabolized in the liver to inactive products
- 10% excreted unchanged in the urine
-starting dosage : 5 mg/d up to 15 mg/d as a single dose
max. 40 mg/d
- lower hypoglycemia compared long acting glyburide
- contraindicated : hepatic impairment, renal insufficiency

Oral Antidiabetic Agents
Insulin secretagogues : sulfonylureas
3. Glimepiride
- t1/2 : 5 hours
- long duration of effect
34
- long duration of effect
- once daily use as monotherapy or in combination
with insulin ~ compliance
- lowets dose of anysulfonylurea compound : 1 mg
single daily dose, maximal 8 mg.

Oral Antidiabetic AgentsInsulin secretagogues : meglitinides
• Meglitinides stimulate insulin secretion (rapidly and for a short duration) in the presence of glucose.
• “quick-on, quick-off” (awal kerja cepat, masa kerja pendek) � kontrol postprandial yang lebih baik dan menurunkan insiden hipoglikemia postprandial.
• Efficacy
– Decreases peak postprandial glucose
– Decreases plasma glucose 60-70 mg/dl (3.3-3.9 mmol/L)
35
– Decreases plasma glucose 60-70 mg/dl (3.3-3.9 mmol/L)
• Other Effects
– Hypoglycemia (although may be less than with sulfonylureas if patient has a variable eating schedule)
– Weight gain
• Ex: repaglinide (Prandin), nateglinide (Starlix)
can be taken safely by people with impaired kidney function or sulfa allergies.

Oral Antidiabetic Agents
Insulin secretagogues : D- phenylalanine derivative
Nateglinide
• the latest insulin secretagogue to become clinically available
• stimulate release of insulin very rapidly and transiently from
B cells through closure of the ATP-sensitivie K+ channel
36
• ingested just prior to meal
• absorbed within 20 minutes after oral administration
• t1/2 1,5 hours
• metabolized by CYP2C9 and CYP3A4
• hypoglycemia : lowest
• safe in : very reduced renal function

Oral Antidiabetic Agents
37Insulin secretagogues

Oral Antidiabetic Agents
Biguanides
Mechanisms of Action
1. Direct stimulation of glycolisis in tissues
2. Reduced hepatic & renal gluconeogenesis
3. Slowing of glucose absorption from GIT
38
Metabolism & Excretion
4. Reduction of plasma glucagon levels
Metformin :
- t1/2 : 1,5-3 hours
- Is not bound to plasma protein
- Is not metabolized
- Is excreted by the kidney as the active compound

Oral Antidiabetic Agents
Biguanides
Clinical Use
• Insulin resistance syndrome
• Dosage : 500 mg to max 2,55 gr daily
39
Toxicities
• anorexia, nausea, vomiting, abdominal discomfort, diarrhea
• lactic acidosis
Contraindication
• renal disease, alcoholism, hepatic disease, conditions
predisposing to tissue anoxia (eg. Chronic cardioplumonary
dysfunction)
Oral Antidiabetic Agents
Thiazolidinediones
• Pioglitazone (Actos), rosiglitazone (Avandia),
• [troglitazone (Rezulin) - (muncul 1997, ditarik tahun 2000 karena dicurigai menyebabkan idiosinkratik hepatoselular)
• Decrease : insulin resistance
40
Oral Antidiabetic Agents
Alpha Glucosidase Inhibitors
• Alpha-glucosidase inhibitors block the enzymes that digest starches in the small intestine � slowing the rise in B.G.L.
• Efficacy
– Decrease peak postprandial glucose 40-50 mg/dl (2.2-2.8 mmol/L)
– Decrease fasting plasma glucose 20-30 mg/dl (1.4-1.7 mmol/L)
• Other Effects
– Flatulence or abdominal discomfort
41
– Flatulence or abdominal discomfort
– No specific effect on lipids or blood pressure
– No weight gain
– Contraindicated in patients with inflammatory bowel disease or cirrhosis
• Examples:
– acarbose (Glucobay),
– miglitol (Glyset) → absorpsi oral yang lebih baik daripada acarbose

GLUCAGON
42
GLUCAGON
Pharmacologic Effects
• metabolic effects : glucagon – rec’r liver cells-Gs protein-linked
increase I adenyly cyclase activity-cAMP> ~ catabolism of stored
glycogen and increases gluconeogenesis and ketogenesis
• release of insulin from normal pancreatic B cells, cathecolamines
43
• release of insulin from normal pancreatic B cells, cathecolamines
from pheochromocytoma, calcitonin from medullary carcinoma cells
• cardiac effects : inotropic (+)ve and chronothropic (+)ve
• smooth muscle : profound relaxation of intestine

GLUCAGON
Clinical Use
• severe hypoglicemia
• endocrine diagnosis
• beta-blocker poisoning
44
Adverse Reactions
• beta-blocker poisoning
• radiology of the bowel
• transient nausea and occasional vomiting

ISLET AMYLOID POLYPEPTIDE
(IAPP, AMYLIN)
45

ISLET AMYLOID POLYPEPTIDE
(IAPP, AMYLIN)
• 37-amino-acid peptide
• derived from amyliod deposits in pancreas material from patients
with longstanding type 2 diabetes or insulinomas
46
• inhibit the action of insulin to promote muscle uptake of glucose
• pramlintide (analog IAPP) : adjunct to insulin therapy in type 1
diabetic patients with recurrent episodes of severe insulin-induced
hypoglycemia. ⇒ still in clinical trial

Glucose meter
47

48
KEBANGGAAN INDONESIA UNTUK DUNIA










![BODY TEMP. KBK.ppt [Read-Only] - ocw.usu.ac.idocw.usu.ac.id/course/download/1110000095-metabolism-system/mbs127...Fakultas Kedokteran USU. Homeostasis Poikilotherms : body temperature](https://static.fdocuments.in/doc/165x107/5c8b529409d3f2a66a8b51e7/body-temp-kbkppt-read-only-ocwusuacidocwusuacidcoursedownload1110000095-metabolism-systemmbs127fakultas.jpg)







