Pharmacology of Chemotherapy Nurse
12
Dr. Ahmed AL-Arwali 1 د.أحمد العروليPharmacology of Chemotherapy Principles of therapy Definition of Chemotherapy: Is the term used to describe the use of drugs that are “selectively toxic” to invading micro-organisms while having minimal effects on the host. Also this term used to embraces the use of drugs that target tumor (cancer). 20 th Century definition: (Antibiotic) Use of synthetic chemicals to destroy infective agents. Kill or inhibit the growth of micro-organism or cancer. Toxic for pathogenic organism or cancer cells. Antibacterial Dugs Β- Lactams Penicillins Mechanism of Action: Bacterial Cell Wall inhibition Natural Penicillins:(Narrow spectrum). Penicillin G (Benzyl Penicillin):
-
Upload
ahmedalarwali -
Category
Documents
-
view
24 -
download
0
description
Chemotherapy
Transcript of Pharmacology of Chemotherapy Nurse
Dr. Ahmed AL-Arwali
1
د.أحمد العرولي
Pharmacology of Chemotherapy
Principles of therapy
Definition of Chemotherapy:
Is the term used to describe the use of drugs that are “selectively toxic” to invading
micro-organisms while having minimal effects on the host. Also this term used to
embraces the use of drugs that target tumor (cancer).
20th Century definition: (Antibiotic)
Use of synthetic chemicals to destroy infective agents.
Kill or inhibit the growth of micro-organism or cancer.
Toxic for pathogenic organism or cancer cells.
Antibacterial Dugs
Β- Lactams
Penicillins
Mechanism of Action:
Bacterial Cell Wall inhibition
Natural Penicillins:(Narrow spectrum).
Penicillin G (Benzyl Penicillin):
Dr. Ahmed AL-Arwali
2
د.أحمد العرولي
Activity: against Gram +ve bacteria e.g.: Niesseria, Bacillus anthracis, Treponema
palladium, collstridium prefrings, C. Tetani, Corynebacterium diphtheria…etc.
Clinical Use:
Acute RTI (respiratory tract infection), syphilis, tetanus, diphtheria and anthrax.
Dose:
1-5 million Unit per 6 hours, IV,IMor IV infusion.
Disadvantages of Natural Peicillins:
1. Short acting duration from 4 to 6 hours.
2. Acid sensitive (not effective orally).
3. Β-lactamase sensitive.(not effective against β-lactamase productive
bacteria e.g. staphylococcus strains.
4. Narrow spectrum(for Gm+ve not Gm-ve) not effective against gram –ve e.g.
E.coi, H.infl., H.pylor, shigella and salmonella.
Long acting Penicillins:
They lack No. 1 disadvantage but they have the rest(2,3,4).
They are also natural.
- Procaine penicillin: 600,000 unit per 12-24 hours.
- Fortified procaine penicillin: 100,000 unit of penicillin G + 300,000 unit
of procaine penicillin.(quick onset and longer duration).
- Benzathine Penicillin 1.2 million unit per 1-4 weeks,
o First week the drug level is therapeutic.

Dr. Ahmed AL-Arwali
3
د.أحمد العرولي
o From 2nd week till 4th week the drug level is prophylactic.
Activity:
Same as penicillin G
Clinical use:
Same as penicillin G and bacterial artheritis.
Acid Resistant Penicillins:
Oral Penicillin V ( Phenoxymethyl penicillin)
250,000, 500,000,1000,000 unit per 4-6 hours
Activity:
Same as penicillin G
Clinical Use:
Mild RTI.
Β- lactamase (Penicillinase) and acid Resistant penicillins:
Oxacillins: they lack 1,2,3 disadvatages but they still narrow spectrum.
- Oxacillin ( parenteral has S.E: hepatitis).
- Cloxacillin, dicloxacillin, flucloxacillin.(flucloxacillin used in bone
and joints infections)
- Nafcillin: parenteral (IV) use in severe staph. Infection, biliary excretion
and may cause neutropenia as side effect.
Activity:
Dr. Ahmed AL-Arwali
4
د.أحمد العرولي
Same Penicillin G + B-lactamase productive species.(staph., strepto. &
pneumococci).
Clinical Use:
RTI.
Broad spectrum Penicillins:
Still have No. 3 disadvatage.
Activity:
Same as Penicilline G and gram –ve species e.g. salmonella, shigella, H.Pylori,
HH.Influenza and E.Coli.
Clinical Use:
RTI, UTI & typhoid.
1. Ampicillin:
Incompletely absorbed orally . that is make it effective in case of
enteritis but also disturb intestinal flora which lead to diarrhea.
Affected by the presence of food.
2. Pro-Ampicillin(esters of ampicillin):
Pro-drugs so they are inactive, so no effect on intestinal flora &
better absorption than ampicillin(not useful in enteritis).
Not affected by food.
De-esterified (release ampicillin) in gut mucosa & liver.
Pivampicillin, Bacampicillin, Talampicillin, Hetacillin & Epicillin.

Dr. Ahmed AL-Arwali
5
د.أحمد العرولي
3. Amoxicillin:
Same as ampicillin esters.
B-lactmase inhibitors:
They haven’t antibacterial effect or it’s minimal.
They bind to the enzyme, cause irreversible inhibition for the enzyme(suicide
substrate).
Protect B-lactams from the bacteria enzyme of PEPSI(Proteus, E.Coli,
Pseudomonas, Staph. & H.Infleunza).
B-lactamase inhibitor Combined penicillin Route.
Clavulanic Acid Amoxicillin Oral and parenteral
Sulbactam Ampicillin Oral and parenteral
Tazobactam piperacillin Parenteral
Extend Spectrum Penicillins( Antipseudomonal):
Broad spectrum + Pseudomonas & proteus (B-lactmase sensitive so we ad B-
lactamase inhibitors – see the previous table-)
1. Ureido Penicillin:
Mezlocillin, azlocillin & Piperacillin.
We combined this group with gentamycin to give synergetic effect
and to avoid resistance.
Dr. Ahmed AL-Arwali
6
د.أحمد العرولي
They are expensive.
Used for resistant UTI..
Adverse effects of Penicillin:
1. Allergy that may cause anaphylactic shock.
2. Jarish-Herxheimer reactions:(allergy at the site of injection)
3. Diarhea (may cause super infection).
4. CNS irritation(seizures): long duration use or intra-thecal injection.
5. Pain, induration and tenderness at the site of injection(benzthine
penicillin).
6. Skin Rash(Ampicillin).
7. Bleeding(Carboxy penicillins).
CEPHALOSPORINS AND CEPHAMYCINS
Cephalosporins N and C, which are chemically related to penicillin, and
cephalosporin P, a steroidal antibiotic that resembles fusidic acid, were first
isolated from Cephalosporium fungus.
The cephamycins are β-lactam antibiotics produced by Streptomyces organisms,
and they are closely related to the cephalosporins.

Dr. Ahmed AL-Arwali
7
د.أحمد العرولي
They have the same mechanism of action as penicillins (see above).
Clinical uses of the cephalosporins Cephalosporins are used to treat infections caused by sensitive organisms. As with other
antibiotics, patterns of sensitivity vary geographically, and treatment is often started
empirically. Many different kinds of infection may be treated, including:
o - septicaemia (e.g. cefuroxime, cefotaxime)
o - pneumonia caused by susceptible organisms
o - meningitis (e.g. ceftriaxone, cefotaxime)
o - biliary tract infection
o - urinary tract infection (especially in pregnancy or in patients unresponsive to other
drugs)
o - sinusitis (e.g. cefadroxil).
Antibacterial spectrum Cephalosporins have been classified as first, second, third, and fourth generation, based largely on their bacterial susceptibility patterns and resistance to ß-lactamases [Note: Commercially available cephalo sporins are ineffective against MRSA, L. monocytogenes, Clostri dium difficile, and the enterococci.]
Clinical Uses
First-Generation Drugs
Cefazolin (parenteral) and cephalexin (oral) are examples of this subgroup. They
are active against gram-positive cocci, including staphylococci and common
streptococci. Many strains of E coli and K pneumoniae are also sensitive. Clinical
uses include treatment of infections caused by these organisms and surgical
prophylaxis in selected conditions. These drugs have minimal activity against
gram-negative cocci, enterococci, methicillin-resistant staphylococci, and most
gram-negative rods.
Second-Generation Drugs
Drugs in this subgroup usually have slightly less activity against gram-positive
organisms than the first-generation drugs but have an extended gram-negative
coverage. Marked differences in activity occur among the drugs in this subgroup.
Dr. Ahmed AL-Arwali
8
د.أحمد العرولي
Examples of clinical uses include infections caused by the anaerobe Bacteroides
fragilis ( cefotetan, cefoxitin ) and sinus, ear, and respiratory infections caused by
H influenzae or M catarrhalis (cefamandole, cefuroxime, cefaclor ).
Third-Generation Drugs
Characteristic features of third-generation drugs (eg, ceftazidime,cefoperazone,
cefotaxime ) include increased activity against gram-negative organisms resistant
to other beta-lactam drugs and ability to penetrate the blood-brain barrier (except
cefoperazone and cefixime). Most are active against Providencia,Serratia
marcescens, and beta-lactamase-producing strains of H influenzae and Neisseria;
they are less active against Enterobacter strains that produce extended-spectrum
beta-lactamases. Ceftriaxone and cefotaxime are currently the most active
cephalosporins against penicillin-resistant pneumococci (PRSP strains), but
resistance is reported. Individual drugs also have activity against
Pseudomonas(cefoperazone, ceftazidime) and B fragilis ( ceftizoxime ). Drugs in
this subclass should usually be reserved for treatment of serious infections.
Ceftriaxone (parenteral) and cefixime (oral), currently drugs of choice in
gonorrhea, are exceptions. Likewise, in acute otitis media, a single injection of
ceftriaxone is usually as effective as a 10-day course of treatment with amoxicillin.
Fourth-Generation Drugs
Cefepime is more resistant to beta-lactamases produced by gram-negative
organisms, including Enterobacter, Haemophilus, Neisseria, and some penicillin-
resistant pneumococci. Cefepime combines the gram-positive activity of first-
generation agents with the wider gram-negative spectrum of third-generation
cephalosporins.
Adverse effects : 1. Hypersensitivity reactions, very similar to those seen with penicillin, may
occur, and there may be some cross-sensitivity; about 10% of penicillin-
sensitive individuals will have allergic reactions to cephalosporins.
2. Nephrotoxicity has been reported (especially with cefradine), as has drug-
induced alcohol intolerance.
3. Diarrhoea is common and can be due to C. difficile.
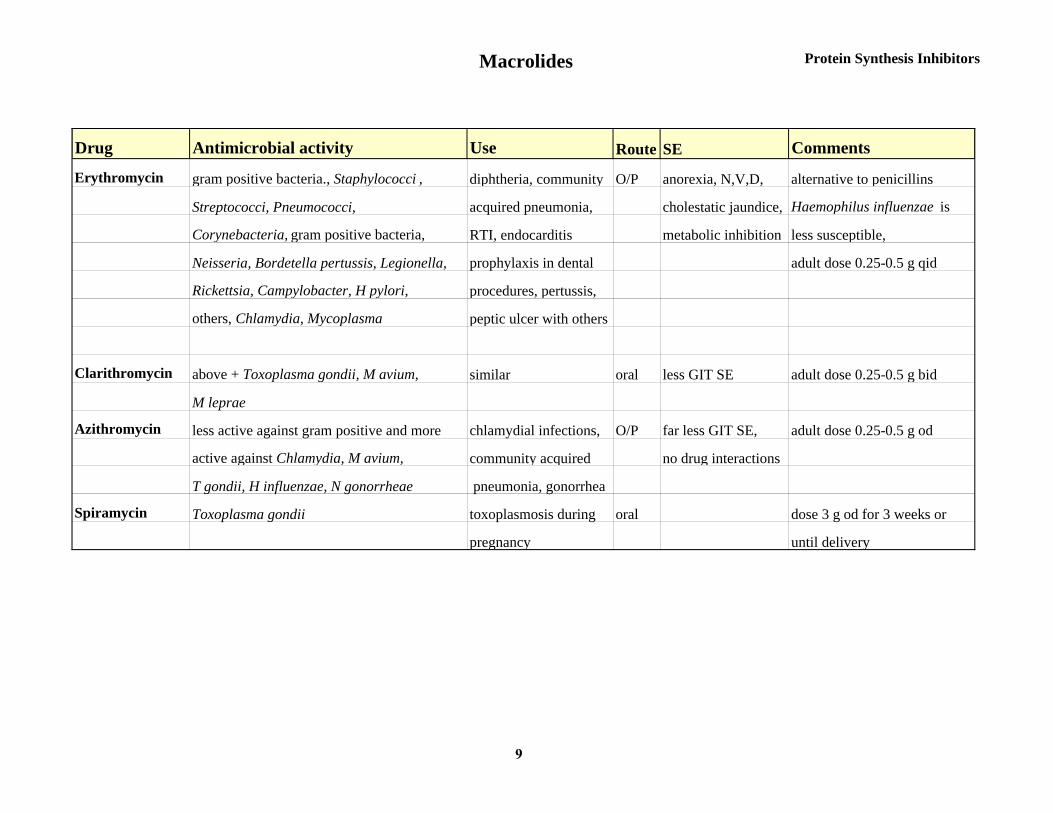
Macrolides Protein Synthesis Inhibitors
Drug Antimicrobial activity Use Route SE Comments
Erythromycin gram positive bacteria., Staphylococci , diphtheria, community O/P anorexia, N,V,D, alternative to penicillins
Streptococci, Pneumococci, acquired pneumonia, cholestatic jaundice, Haemophilus influenzae is
Corynebacteria, gram positive bacteria, RTI, endocarditis metabolic inhibition less susceptible,
Neisseria, Bordetella pertussis, Legionella, prophylaxis in dental adult dose 0.25-0.5 g qid
Rickettsia, Campylobacter, H pylori, procedures, pertussis,
others, Chlamydia, Mycoplasma peptic ulcer with others
Clarithromycin above + Toxoplasma gondii, M avium, similar oral less GIT SE adult dose 0.25-0.5 g bid
M leprae
Azithromycin less active against gram positive and more chlamydial infections, O/P far less GIT SE, adult dose 0.25-0.5 g od
active against Chlamydia, M avium, community acquired no drug interactions
T gondii, H influenzae, N gonorrheae pneumonia, gonorrhea
Spiramycin Toxoplasma gondii toxoplasmosis during oral dose 3 g od for 3 weeks or
pregnancy until delivery
9
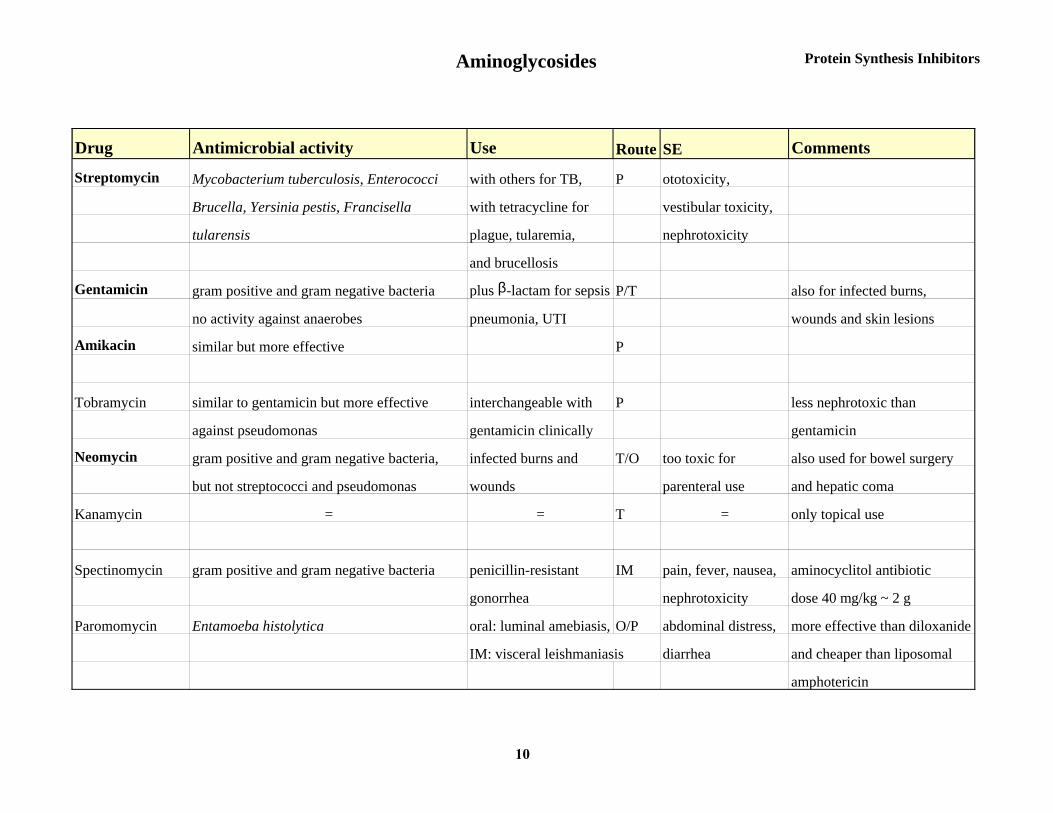
Aminoglycosides Protein Synthesis Inhibitors
Drug Antimicrobial activity Use Route SE Comments
Streptomycin Mycobacterium tuberculosis, Enterococci with others for TB, P ototoxicity,
Brucella, Yersinia pestis, Francisella with tetracycline for vestibular toxicity,
tularensis plague, tularemia, nephrotoxicity
and brucellosis
Gentamicin gram positive and gram negative bacteria plus β-lactam for sepsis P/T also for infected burns,
no activity against anaerobes pneumonia, UTI wounds and skin lesions
Amikacin similar but more effective P
Tobramycin similar to gentamicin but more effective interchangeable with P less nephrotoxic than
against pseudomonas gentamicin clinically gentamicin
Neomycin gram positive and gram negative bacteria, infected burns and T/O too toxic for also used for bowel surgery
but not streptococci and pseudomonas wounds parenteral use and hepatic coma
Kanamycin = = T = only topical use
Spectinomycin gram positive and gram negative bacteria penicillin-resistant IM pain, fever, nausea, aminocyclitol antibiotic
gonorrhea nephrotoxicity dose 40 mg/kg ~ 2 g
Paromomycin Entamoeba histolytica oral: luminal amebiasis, O/P abdominal distress, more effective than diloxanide
IM: visceral leishmaniasis diarrhea and cheaper than liposomal
amphotericin
10
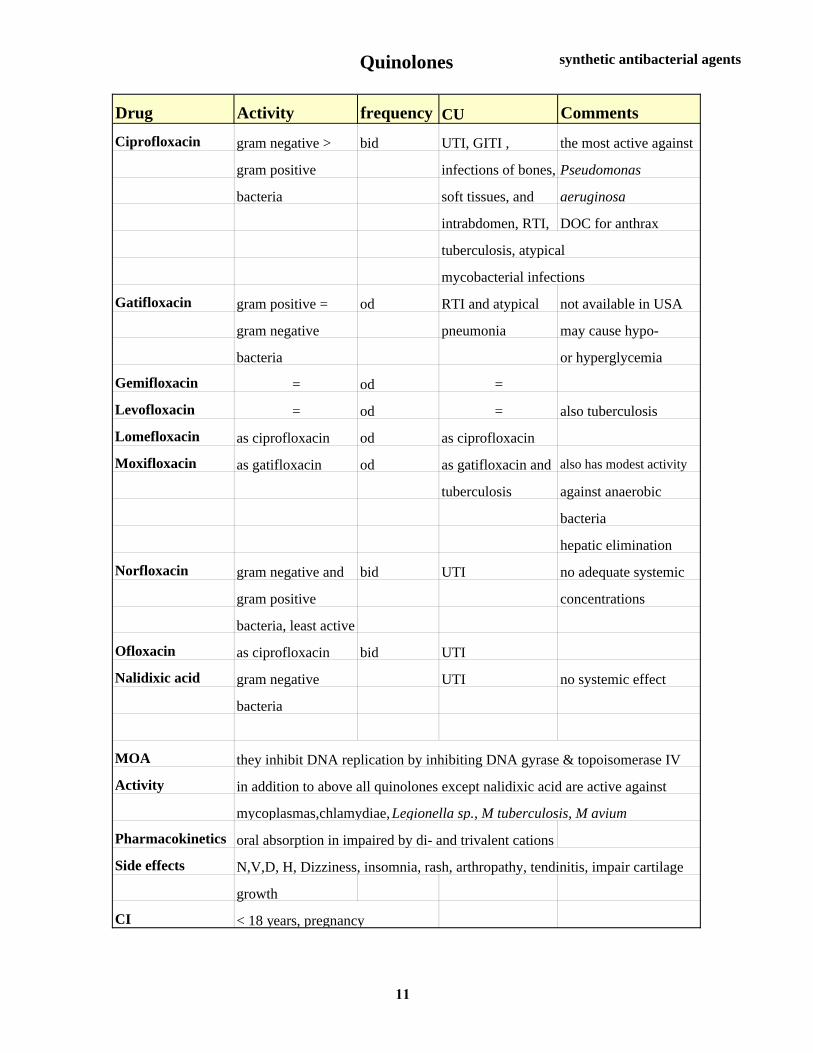
Quinolones synthetic antibacterial agents
Drug Activity frequency CU Comments
Ciprofloxacin gram negative > bid UTI, GITI , the most active against
gram positive infections of bones, Pseudomonas
bacteria soft tissues, and aeruginosa
intrabdomen, RTI, DOC for anthrax
tuberculosis, atypical
mycobacterial infections
Gatifloxacin gram positive = od RTI and atypical not available in USA
gram negative pneumonia may cause hypo-
bacteria or hyperglycemia
Gemifloxacin = od =
Levofloxacin = od = also tuberculosis
Lomefloxacin as ciprofloxacin od as ciprofloxacin
Moxifloxacin as gatifloxacin od as gatifloxacin and also has modest activity
tuberculosis against anaerobic
bacteria
hepatic elimination
Norfloxacin gram negative and bid UTI no adequate systemic
gram positive concentrations
bacteria, least active
Ofloxacin as ciprofloxacin bid UTI
Nalidixic acid gram negative UTI no systemic effect
bacteria
MOA they inhibit DNA replication by inhibiting DNA gyrase & topoisomerase IV
Activity in addition to above all quinolones except nalidixic acid are active against
mycoplasmas,chlamydiae, Legionella sp., M tuberculosis, M avium
Pharmacokinetics oral absorption in impaired by di- and trivalent cations
Side effects N,V,D, H, Dizziness, insomnia, rash, arthropathy, tendinitis, impair cartilage
growth
CI < 18 years, pregnancy
11
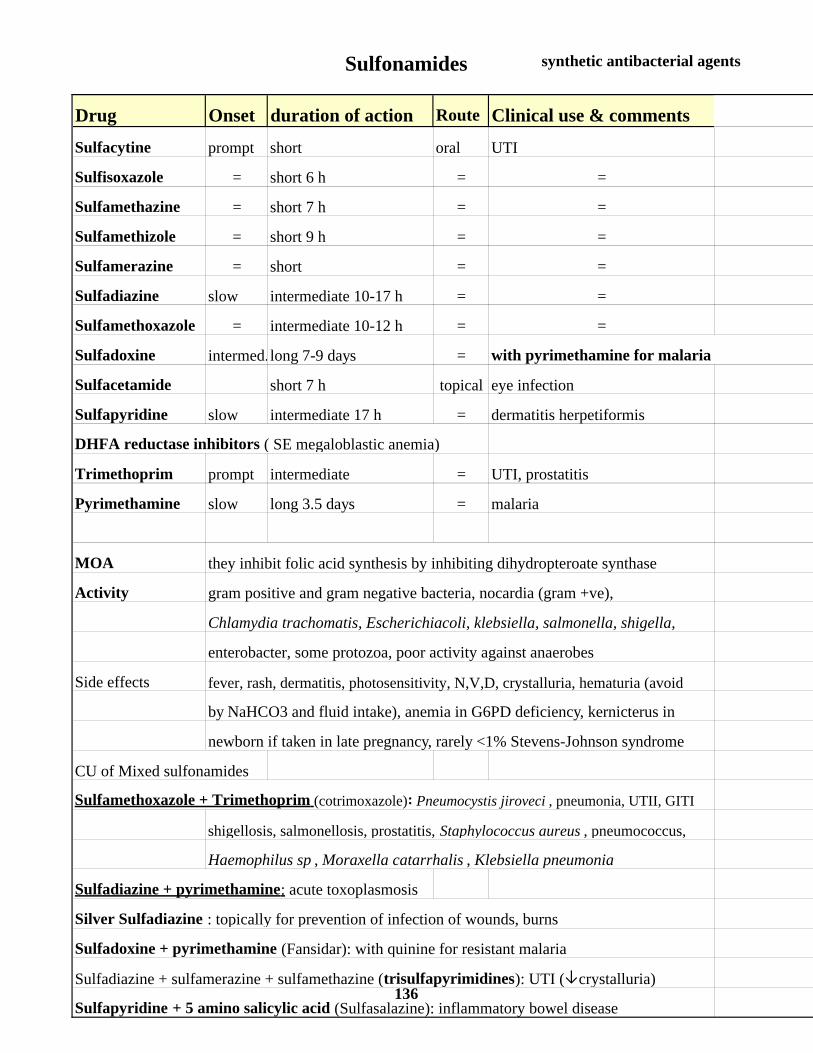
Sulfonamides synthetic antibacterial agents
Drug Onset duration of action Route Clinical use & comments
Sulfacytine prompt short oral UTI
Sulfisoxazole = short 6 h = =
Sulfamethazine = short 7 h = =
Sulfamethizole = short 9 h = =
Sulfamerazine = short = =
Sulfadiazine slow intermediate 10-17 h = =
Sulfamethoxazole = intermediate 10-12 h = =
Sulfadoxine intermed.long 7-9 days = with pyrimethamine for malaria
Sulfacetamide short 7 h topical eye infection
Sulfapyridine slow intermediate 17 h = dermatitis herpetiformis
DHFA reductase inhibitors ( SE megaloblastic anemia)
Trimethoprim prompt intermediate = UTI, prostatitis
Pyrimethamine slow long 3.5 days = malaria
MOA they inhibit folic acid synthesis by inhibiting dihydropteroate synthase
Activity gram positive and gram negative bacteria, nocardia (gram +ve),
Chlamydia trachomatis, Escherichiacoli, klebsiella, salmonella, shigella,
enterobacter, some protozoa, poor activity against anaerobes
Side effects fever, rash, dermatitis, photosensitivity, N,V,D, crystalluria, hematuria (avoid
by NaHCO3 and fluid intake), anemia in G6PD deficiency, kernicterus in
newborn if taken in late pregnancy, rarely <1% Stevens-Johnson syndrome
CU of Mixed sulfonamides
Sulfamethoxazole + Trimethoprim (cotrimoxazole): Pneumocystis jiroveci , pneumonia, UTII, GITI
shigellosis, salmonellosis, prostatitis, Staphylococcus aureus , pneumococcus,
Haemophilus sp , Moraxella catarrhalis , Klebsiella pneumonia
Sulfadiazine + pyrimethamine: acute toxoplasmosis
Silver Sulfadiazine : topically for prevention of infection of wounds, burns
Sulfadoxine + pyrimethamine (Fansidar): with quinine for resistant malaria
Sulfadiazine + sulfamerazine + sulfamethazine (trisulfapyrimidines): UTI (↓crystalluria)
Sulfapyridine + 5 amino salicylic acid (Sulfasalazine): inflammatory bowel disease136