Plant-Derived Compounds with Potential Sedative and Anxiolytic ...
Upload
shanthi-priyaCategory
view
492download
2
04/11/23 1
Pharmacology of Anxiolytic/ Sedative-Hypnotics
Philip G. Janicak, MDProfessor of Psychiatry and Pharmacology
University of Illinois at Chicago

04/11/23 2
Abstract
Recent anxiolytic and sedative-hypnotic agents offer comparable efficacy, fewer serious adverse effects, and less risk of a fatal consequence due to accidental or intentional overdose in comparison to alcohol, barbiturates and other non-barbiturate agents (e.g., meprobamate). Unfortunately, they have not entirely eliminated the hazards of tolerance, dependency, and withdrawal syndromes, although they have a lower abuse potential than their predecessors.
For these reasons, it is important to become knowledgeable about the basic pharmacology of these drugs, in addition to their appropriate clinical indications, dosages, and duration of usage. Most importantly, their limitations must receive as much attention as their assets.
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 3
pharmacology of anxiolytic/sedative-hypnotics
Objectives
Review diagnostic indications for anxiolytic/ sedative-hypnotics
Review different classes of antianxiety and sedative-hypnotic agents in terms of their pharmacodynamics; pharmacokinetics; adverse effects; and potential for drug interactions.
Review treatment strategies for anxiety and sleep disorders.

04/11/23 4
pharmacology of anxiolytic/sedative-hypnotics
Anxiety
Natural human experience
Subjective qualities of fear or related emotions
Ensures survival and adaptation
In excess, can cripple and destroy

04/11/23 5
pharmacology of anxiolytic/sedative-hypnotics
Anxiety Symptoms
Anxiety symptoms are associated with numerous medical conditions: Cardiovascular disease Endocrine disease Gastrointestinal disease Neurologic disease Drug-induced

04/11/23 6
pharmacology of anxiolytic/sedative-hypnotics
Indications for Antianxiety/Sedative-Hypnotics
Generalized anxiety disorder (GAD) Phobic disorders Psychological factors affecting medical condition
Panic disorder Obsessive-compulsive disorder Posttraumatic stress disorder
Sleep disorders (dyssomnias; parasomnias)

04/11/23 7
pharmacology of anxiolytic/sedative-hypnotics
GAD
Represents up to 50% of anxious patients seen by physicians
Increased annual medical expenses
Often unnecessary medical consultations
55 million prescriptions for BZDs in 1989
Anxiolytic agents fourth most prescribed class of medication

04/11/23 8
Phobic Disorders
Disabling anxiety (at times associated with panic attacks) and avoidance
Agoraphobia
Social phobia (Social Anxiety Disorder)
Specific phobia
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 9
Psychological FactorsAffecting Medical Condition
Psychologically meaningful environmental stimuli
Temporally related to the initiation or exacerbation of a physical condition
Demonstrable organic pathology (e.g., rheumatoid arthritis)
Known physiological process (e.g., migraine)
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 10
pharmacology of anxiolytic/sedative-hypnotics
Panic Disorder
Sudden, spontaneous, unexpected feelings of terror and anxiety
The autonomic equivalence of anxiety The desire to flee the situation and return to
a safe place A phobic avoidance of the places where
such attacks occur

04/11/23 11
Symptomatology of Panic Attacks
Shortness of breath /smothering sensations
Dizziness, unsteady feelings, or faintness
Palpitations/tachycardia Trembling/shaking Sweating Choking
Nausea/abdominal distress Depresonalization/
derealization Paresthesias Flushes/chills Chest pain or discomfort Fear of dying Fear of going crazy or doing
something uncontrolled
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 12
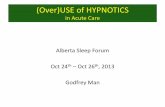
Course of Illness
Panic
GAD
Normal
anxiety level
time
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 13
pharmacology of anxiolytic/sedative-hypnotics
Obsessive-Compulsive Disorder (OCD)
Recurrent obsessions and/or compulsions:Cause marked distress, are time-consuming, or
interfere with functioningAre recognized as excessive or unreasonableAre not due to the effect of a substance or general
medical condition

04/11/23 14
pharmacology of anxiolytic/sedative-hypnotics
Obsessions in OCD
Contamination Pathological doubt Aggressive impulses Somatic concerns Need for symmetry Sexual impulses

04/11/23 15
pharmacology of anxiolytic/sedative-hypnotics
Compulsive Behaviors in OCD
Cleaning Washing Checking Excessive ordering/arranging Counting Repeating Collecting

04/11/23 16
Posttraumatic Stress Disorder (PTSD)
Due to an unusual experience that would be very stressful for almost anyone (e.g., combat, rape, sudden unexpected death of a loved one)
Symptoms include: Intrusive recollections; frightening dreams; sense of event recurring Intensive physiological stress; hyperarousal Emotional numbing Persistent avoidance of stimuli associated with the trauma
High comorbidity with other psychiatric disorders Increase suicide attempt risk Female-to-male lifetime prevalence ratio of 2:1
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 17
Sleep Disorders
Dyssomnias (difficulty initiating or maintaining sleep or not feeling rested) Primary Insomnia Primary Hypersomnia Circadian Rhythm Disorder
Parasomnias (abnormal event) Nightmare Disorder Sleep Terror Disorder Sleepwalking Disorder
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 18
pharmacology of anxiolytic/sedative-hypnotics
Pharmacodynamics
BenzodiazepinesSpecific binding site associated with GABAA receptor-
chloride ion channelPotentiate GABA Serotonergic effects (e.g., clonazepam)
Azapirone (e.g., buspirone)5-HT1A agonist: acutely, firing, in dorsal raphe nuclei;
chronically, receptor desensitization activity Beta-blockers
receptors central and peripheral, post synaptic Clonidine
Agonist at 2 receptors, central, pre-synaptic Antidepressants

04/11/23 19
pharmacology of anxiolytic/sedative-hypnotics
GABA Function and Distribution
Inhibitory neurotransmitter
Widely distributed throughout CNS
Local inhibitory action, therefore rapidly alters neuronal output
Desensitization to inhibitory effects with chronic stimulation of GABA

20 04/11/23
GABAA-BZD Supramolecular Complex

04/11/23 21S.M. Paul, 1995
GABAA Receptor Structure
BenzodiazepinesAgonists
Antagonists-Inverse Agonists
DBI Peptides
ConvulsantsPicrotoxinTBPS
Cl-
GABA AgonistsMuscimol
GABA AntagonistsBicuculline
Barbiturates
Neuroactive Steroids
Alcohols
Anesthetics

04/11/23 22
GABAA receptorCytoplasm
Benzodiazepine-binding domain
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 23
BZD Receptors Type I
Predominates in cerebellum Anxiolytic properties Less sedative properties
Type II Located in cortex, hippocampus, spinal cord No anxiolytic properties Sedative properties
Type III Located in peripheral tissue No anxiolytic properties ? other properties
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 24
BZD Receptor Activity
Full AgonistPartialAgonist Antagonist
Partial InverseAgonist
Full InverseAgonist
AnxiolyticSed-HypnoticMyorelaxantAnticonvulsantAmnesticDependency
Anxiolytic No clinicaleffect
PromnesticAnxiogenicPro-convulsant
PromnesticAnxiolyticConvulsant
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 25
Non-Benzodiazepine Agents
Imidazopyridines (e.g., zolpidem, alpidem)
Pyrazolopyrimidine (e.g., zaleplon)
Cyclopyrralone (e.g., zopiclone)
Sedating antidepressants (e.g., trazodone)
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 26
Non-Benzodiazepine Agents (con’t)
Antihistamines (e.g., diphenhydramine)
Natural Remedies (e.g., melatonin, valerian)
B-carbolines (e.g., abecarnil)
BZD structural derivatives (e.g., biretazanil)
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 27
pharmacology of anxiolytic/sedative-hypnotics
Serotonin Model
Majority of 5-HT pathways originate in the dorsal raphe (DR)
DR innervates cortex, hypothalamus, thalamus, and limbic system
5-HT mediates behavioral effects in animal models and humans

04/11/23 28
Serotonin Receptors
5-HT1A -Anxiety, alcoholism, sexual function
5-HT1C -Anxiety, migraine pain
5-HT1D -Migraine pain
5-HT2 -Anxiety, depression, schizophrenia negative symptoms, sexual function
5-HT3 -Migraine pain, emesis, schizophrenia (e.g., ondansetron)
5-HT4 -Anxiety, schizophrenia?
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 29
Serotonin Agents: Indications forAnxiety-Related Disorders
SSRI
Sertraline - OCD; PD; PTSD
Paroxetine - OCD; PD; SAD; GAD
Fluoxetine - OCD; BN; PMDD
Fluvoxamine - OCD Venlafaxine - GAD Buspirone - GAD
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 30
Noradrenergic Model
Hypersensitivity to autonomic nervous system
Locus coeruleus (LC)
Stimuli norepinephrine release stimulation of the sympathetic nervous system
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 31
Norepinephrine Receptors
Locus coeruleus Alpha -2 adrenergic receptors
somatodendritic autoreceptors terminal autoreceptors negative feedback system antagonists are anxiogenic agonists may be anxiolytic and decrease withdrawal
symptoms (e.g., clonidine)
Beta adrenergic receptors Beta-blockers (e.g., propranolol)
Social phobiaPerformance anxiety
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 32
Pharmacokinetics: Benzodiazepines
Absorption: rapid absorption, except clorazepate Onset of action: increase lipid solubility faster onset Duration of action: single dose with increased lipid
solubility faster redistribution to fat tissues shorter duration of action.
Chronic use: in equilibrium with fat tissues Half life: In part, determines duration of action Metabolism: lorazepam, oxazepam, temazepam
not metabolized by liver
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 33
Drug Interactions: Benzodiazepines
Additive pharmacodynamic effects (e.g., alcohol)
BZD withdrawal when other drugs that increase seizure risk are also taken
Inhibit BZD metabolism (e.g., nefazodone via P450 3A 3/4 inhibits metabolism of triazolam)
Diazepam may increase levels of digoxin and phenytoin
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 34
Adverse Effects: Benzodiazepines
Sedation and impairment of performancePsychomotor skills: driving; engaging in dangerous physical activities; using hazardous machinery, especially during initial phase of treatment
Memory impairmentAnterograde amnesia (desired before surgery, other procedures).
Dose-related, and tolerance may not develop.
Most likely with triazolam
DisinhibitionPossible risk factors: history of aggression, impulsivity, borderline or antisocial personality
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 35
Abuse, Dependence, Withdrawal, and Rebound Anxiety: Benzodiazepines
Abuse potential decreased when properly prescribed and supervised.
Dependence may occur at usual doses taken beyond several weeks.
Withdrawal may occur even when discontinuation is not abrupt (e.g., by 10% every 3 days). Symptoms include: tachycardia, increased blood pressure, muscle cramps, anxiety, insomnia, panic attacks, impairment of memory and concentration, perceptual disturbances, derealization, hallucinations, hyperpyrexia, seizures. May continue for months.
Rebound anxiety: return of target symptoms, with increase intensity.
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 36
Pharmacokinetics/Pharmacodynamics: Buspirone
Onset of action (i.e., weeks versus days)
No sedation or impairment of performance No cross-tolerance with BZDs No tolerance or withdrawal No abuse potential
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 37
Adverse Effects: Buspirone
Nausea
Headache
Insomnia, nervousness
Restlessness
Dizziness, lightheadedness
pharmacology of anxiolytic/sedative-hypnotics

04/11/23 38
CLINICAL PRESENTATION TREATMENT STRATEGY
PSYCHOTHERAPY: Supportive, Cognitive-Behavioral or Insight-Oriented
Acute anxiety (mild)
Acute anxiety (more severe) (start) Benzodiazepine (BZD) plus Psychotherapy
(may start)
(insufficient response)
Treatment Strategy for GAD
(may add)
(insufficient response)
(may try)

04/11/23 39
CLINICAL PRESENTATION TREATMENT STRATEGY
Buspirone (up to 90 mg/day for up to 6 weeks) plus CBT
Chronic anxiety(no prior BZD therapy)
Venlafaxine
(may start)
(insufficient response)
Treatment Strategy for GAD
(insufficient response)

04/11/23 40
CLINICAL PRESENTATION TREATMENT STRATEGY
Buspirone or Venlafaxine plus BZD initially, then taper BZD
plus CBT
Chronic anxiety,prior BZD therapy
Chronic anxiety with panic or depressive symptoms
(may start)
Buspirone or Venlafaxine plus BZD for longer period
plus CBT
(may start)
(insufficient response)
Treatment Strategy for GAD
Other Antidepressants (TCA, SSRI, MAOI) w/wo a BZD or Buspirone
(insufficient response)

04/11/23 41
CLINICAL PRESENTATION TREATMENT STRATEGY
Cognitive Behavioral TherapySocial Phobia, Generalized (Social Anxiety Disorder)
(may start)
(insufficient response)
Treatment Strategyfor PHOBIC Disorders
(or)
Selective Serotonin Reuptake Inhibitor (e.g., Paroxetine)
(insufficient response)

04/11/23 42
CLINICAL PRESENTATION TREATMENT STRATEGY
BEHAVIORAL THERAPY PLUS SSRI
MAOI (must wait at least 2 weeks after discontinuation of SSRI [longer for fluoxetine] before starting MAOI)
(insufficient response)
Treatment Strategyfor PHOBIC Disorders
orAlprazolam
orClonidine

04/11/23 43
CLINICAL PRESENTATION TREATMENT STRATEGY
Cognitive Behavioral TherapySystematic desensitization
Specific Phobia
B-blocker (e.g., performance anxiety)
(start)
(insufficient response)
Treatment Strategyfor PHOBIC Disorders
MAOI (e.g., phenelzine)
(insufficient response)

04/11/23 44
CLINICAL PRESENTATION TREATMENT STRATEGY
Behavioral Therapy only
(may require several months)CognitiveIn-vivo exposureRelaxationSystematic desensitization
Panic attacks (mild) w/wo agoraphobia
(start)
(insufficient response)
Treatment Strategy for PANIC Disorder with or without Agoraphobia
(may add)From Janicak PG, Davis JM, Preskorn SH, Ayd FJ Jr. Principles and Practice of Psychopharmacotherapy. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.

04/11/23 45
CLINICAL PRESENTATION TREATMENT STRATEGY
SSRI plus Behavioral TherapyPanic attacks (moderate) w/wo agoraphobia
(may start)
(insufficient response)
(or)
Other Antidepressant (e.g., Venlafaxine, TCA) plus Behavioral Therapy
(insufficient response)
Treatment Strategy for PANIC Disorder with or without Agoraphobia
From Janicak PG, Davis JM, Preskorn SH, Ayd FJ Jr. Principles and Practice of Psychopharmacotherapy. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.

04/11/23 46
CLINICAL PRESENTATION TREATMENT STRATEGY
ALPRAZOLAM/CLONAZEPAM
plus Behavioral Therapy
(insufficient response)
Treatment Strategy for PANIC Disorder with or without Agoraphobia
From Janicak PG, Davis JM, Preskorn SH, Ayd FJ Jr. Principles and Practice of Psychopharmacotherapy. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.

04/11/23 47
CLINICAL PRESENTATION TREATMENT STRATEGY
TCA/SSRI and Behavioral TherapyPanic attacks (severe) w/wo agoraphobia
Alprazolam/Clonazepamfor first month
(start)
(plus)
(insufficient response)
Treatment Strategy for PANIC Disorder with or without Agoraphobia
From Janicak PG, Davis JM, Preskorn SH, Ayd FJ Jr. Principles and Practice of Psychopharmacotherapy. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.

04/11/23 48
Alprazolam/Clonazepamindefinitely
CLINICAL PRESENTATION TREATMENT STRATEGY
TCA/SSRI and Behavioral Therapy
Treatment Strategy for PANIC Disorder with or without Agoraphobia
(plus)
(insufficient response)
From Janicak PG, Davis JM, Preskorn SH, Ayd FJ Jr. Principles and Practice of Psychopharmacotherapy. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.

04/11/23 49
CLINICAL PRESENTATION TREATMENT STRATEGY
MONOAMINE OXIDASE INHIBITOR (N.B. SSRI) must be stopped prior to beginning MAOI:Fluoxetine, at least 5 weeksOther SSRIs, at least 2 weeks
Valproate w/wo BZD
(insufficient response)
(may try)
Treatment Strategy for PANIC Disorder with or without Agoraphobia
From Janicak PG, Davis JM, Preskorn SH, Ayd FJ Jr. Principles and Practice of Psychopharmacotherapy. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.

04/11/23 50
CLINICAL PRESENTATION TREATMENT STRATEGY
Behavioral Therapy
(e.g., exposure and response prevention)
Mild symptoms (may start)
(insufficient response)
Treatment Strategy for OBSESSIVE-COMPULSIVE and Related Disorders
(may add)
From Janicak PG, Davis JM, Preskorn SH, Ayd FJ Jr. Principles and Practice of Psychopharmacotherapy. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.

04/11/23 51
CLINICAL PRESENTATION TREATMENT STRATEGY
SSRIFluvoxamineSertralineParoxetineCitalopramFluoxetine
Moderate to severe symptoms
(start)
(insufficient response)
Clomipramine
From Janicak PG, Davis JM, Preskorn SH, Ayd FJ Jr. Principles and Practice of Psychopharmacotherapy. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.
Behavioral Therapy(plus)
(or)
Treatment Strategy for OBSESSIVE-COMPULSIVE and Related Disorders

04/11/23 52
CLINICAL PRESENTATION TREATMENT STRATEGY
Alternate SRI
(insufficient response)
From Janicak PG, Davis JM, Preskorn SH, Ayd FJ Jr. Principles and Practice of Psychopharmacotherapy. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.
Treatment Strategy for OBSESSIVE-COMPULSIVE and Related Disorders
(insufficient response)
Clonazepam/Buspirone plus SRI

04/11/23 53
CLINICAL PRESENTATION TREATMENT STRATEGY
Pimozide/Haloperidol/Risperidone or Lithium w/wo SRI
TrichotillomaniaTics (e.g., Tourette’s)Delusional symptoms
MAOI (SRI must be completely cleared first)
(may start)
(insufficient response)
(insufficient response)
From Janicak PG, Davis JM, Preskorn SH, Ayd FJ Jr. Principles and Practice of Psychopharmacotherapy. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.
Treatment Strategy for OBSESSIVE-COMPULSIVE and Related Disorders
(may consider)

04/11/23 54
CLINICAL PRESENTATION TREATMENT STRATEGY
Somatic TherapyECTNeurosurgeryTMS (?)
Severe, unremitting course (e.g., 5 years; failed trials with SSRI, CMI, MAOI; severe dysfunction)
(consider)
From Janicak PG, Davis JM, Preskorn SH, Ayd FJ Jr. Principles and Practice of Psychopharmacotherapy. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.
Treatment Strategy for OBSESSIVE-COMPULSIVE and Related Disorders

04/11/23 55
CLINICAL PRESENTATION TREATMENT STRATEGY
Clarify diagnosistreat any medical or psychiatric disordercheck for non-prescribed drugs
Transient or short-term insomnia
(first)
(insufficient response or no other disorder discovered)
Treatment Strategy for SLEEP Disorders
Adapted from Janicak PG, Davis JM, Preskorn SH, Ayd FJ Jr. Principles and Practice of Psychopharmacotherapy. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.

04/11/23 56
CLINICAL PRESENTATION TREATMENT STRATEGY
Nonpharmacological therapiesStimulus controlSleep restrictionRelaxation techniquesParadoxical intentionSleep hygiene techniques
Treatment Strategy for SLEEP Disorders
(insufficient response)
Adapted from Janicak PG, Davis JM, Preskorn SH, Ayd FJ Jr. Principles and Practice of Psychopharmacotherapy. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.

04/11/23 57
CLINICAL PRESENTATION TREATMENT STRATEGY
Short- to intermediate-acting BZD Sedative-Hypnotic (e.g., estazolam 0.5-1 mg QHS)
(insufficient response)
Zolpidem or Zaleplon (5-20 mg QHS)
(or)
Treatment Strategy for SLEEP Disorders
Adapted from Janicak PG, Davis JM, Preskorn SH, Ayd FJ Jr. Principles and Practice of Psychopharmacotherapy. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.

04/11/23 58
CLINICAL PRESENTATION TREATMENT STRATEGY
Non-pharmacological therapies w/wo sedating antidepressant
Chronic insomnia (7-12 weeks)
(start)
e.g., trazodone (25-50 mg QHS)
Treatment Strategy for SLEEP Disorders
COMBINED TREATMENT non-pharmacological and intermittent, sedative-hypnotic when necessary
(insufficient response)
Adapted from Janicak PG, Davis JM, Preskorn SH, Ayd FJ Jr. Principles and Practice of Psychopharmacotherapy. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.

04/11/23 59
Generic Names Trade Names Daily Dosage (mg/day)
BENZODIAZEPINESChlordiazepoxide Librium, others 10-100Diazepam Valium, others 2-40Oxazepam Serax, others 30-120Chlorazepate Tranxene, others 15-60Lorazepam Ativan 1-10Prazepam Centrax 20-60Halazepam Paxipam 60-160Alprazolam Xanax 0.75-4
AZAPIRONESBuspirone Buspar 15-60
ANTIDEPRESSANTSSSRI Sertraline, others 25-250Venlafaxine Effexor 75-375
ANTIANXIETY AGENTS

04/11/23 60
Generic Names Trade Names Daily Dosage (mg /day)BENZODIAZEPINESLong-actingFlurazepam Dalmane 15-45Quazepam Doral 7.5-15Intermediate-actingEstazolam Prosom 0.5-2Temazepam Restoril 15-45Short-actingTriazolam Halcion 0.125-0.25
NONBENZODIAZEPINE Zolpidem Ambien 5-20Zaleplon Sonata 5-20
SEDATING ANTIDEPRESSANTSTrazodone Dyserel 25-100
BARBITURATE-LIKEChloral Hydrate Notec 500-1500
OTHERMelatonin 0.3-2
SEDATIVE-HYPNOTICS

04/11/23 61
References
Ayd FJ Jr, Janicak PG, Davis JM, Preskorn SH. Advances in the pharmacotherapy of anxiety-related disorders. In: Janicak PG, ed. Principles and Practice of Psychopharmacotherapy Update. Baltimore, MD: Williams & Wilkins; 1996. Vol 1.
Janicak PG, Ayd FJ Jr. Sedatives and hypnotics in the elderly patient. In: Nelson JC, ed. Geriatric Psychopharmacology. New York, NY: Marcel-Dekker; 1998:347-366.
Janicak PG, Davis JM, Preskorn SH, Ayd FJ Jr. Principles and Practice of Psychopharmacotherapy. 3rd Ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001:463-558.
Israni TH, Janicak PG, Davis JM. Obsessive compulsive disorder. In: Flaherty JA, Davis JM, Janicak PG, eds. Psychiatry: diagnosis and therapy. 2nd ed. Norwalk, CN: Appleton & Lange; 1993:145-155.
pharmacology of anxiolytic/sedative-hypnotics