Pharmacological and Mechanical Management of Chronic Stable Angina
45
Pharmacological and Pharmacological and Mechanical Management of Mechanical Management of Chronic Stable Angina Chronic Stable Angina Rafat F. Padaria, M.D. Rafat F. Padaria, M.D. Cardiovascular Medicine, PC. Cardiovascular Medicine, PC.
Transcript of Pharmacological and Mechanical Management of Chronic Stable Angina

Pharmacological and Pharmacological and Mechanical Management of Mechanical Management of
Chronic Stable AnginaChronic Stable Angina
Rafat F. Padaria, M.D.Rafat F. Padaria, M.D.Cardiovascular Medicine, PC.Cardiovascular Medicine, PC.
What is Angina?What is Angina?
It is a clinical syndrome characterized by It is a clinical syndrome characterized by discomfort in the chest, jaw, shoulder, back or discomfort in the chest, jaw, shoulder, back or arm.arm.Typically aggravated by exertion or emotional Typically aggravated by exertion or emotional stressstressRelieved by nitroglycerinRelieved by nitroglycerin

Definition of AnginaDefinition of Angina
First described by William Heberden ( 1701First described by William Heberden ( 1701--1801)1801)Latin Latin ““angereangere””-- means means ““ to choke or throttleto choke or throttle””PectorisPectoris-- ““pectuspectus”” means means ““chestchest””Severe crushing chest pain with a feeling Severe crushing chest pain with a feeling beneath the sternum of pressure and beneath the sternum of pressure and suffocationsuffocation

Chest PainChest Pain-- ClassificationClassificationTypical AnginaTypical Angina
Substernal discomfort with a charactertistic quality Substernal discomfort with a charactertistic quality and durationand durationProvoked by stress/exertionProvoked by stress/exertionRelieved by restRelieved by rest
Atypical AnginaAtypical AnginaMeets 2 of the above characteristicsMeets 2 of the above characteristics
Non cardiac chest painNon cardiac chest painMeets one or none of the typical angina Meets one or none of the typical angina characteristicscharacteristics

Grading of Angina by the CCSCSGrading of Angina by the CCSCS
Class IClass IOrdinary activity does not cause anginaOrdinary activity does not cause angina-- occurs occurs with strenuous, rapid, prolonged exertionwith strenuous, rapid, prolonged exertion
Class IIClass IISlight limitation of ordinary activitySlight limitation of ordinary activity

Grading of Angina by the CCSCSGrading of Angina by the CCSCS
Class IIIClass IIIMarked limitation of ordinary physical activityMarked limitation of ordinary physical activity
Class IVClass IVInability to carry on any physical activity without Inability to carry on any physical activity without discomfortdiscomfortAngina at restAngina at rest

Stable AnginaStable Angina
Chest pain in a patient who has Chest pain in a patient who has alreadyalready been been diagnosed with ischemic heart disease that did diagnosed with ischemic heart disease that did not change its pattern in the preceding 2 not change its pattern in the preceding 2 monthsmonths

Unstable AnginaUnstable Angina
Rest AnginaRest AnginaOccurring at restOccurring at restUsually prolonged >20 min occurring within a week of Usually prolonged >20 min occurring within a week of presentationpresentation
New onset AnginaNew onset AnginaSeverity is at least CCSC III with onset within 2 months of Severity is at least CCSC III with onset within 2 months of initial presentationinitial presentation
Increasing AnginaIncreasing AnginaPreviously diagnosed angina that is distinctly more Previously diagnosed angina that is distinctly more frequent, longer in duration.frequent, longer in duration.

Treatment of Stable AnginaTreatment of Stable Angina
Two major purposesTwo major purposesIncrease Increase quantityquantity of lifeof lifeImprove Improve qualityquality of lifeof life

Treatment of Stable AnginaTreatment of Stable Angina
Pharmacological TherapyPharmacological TherapyMechanical TherapyMechanical Therapy

Pharmacological Pharmacological TreatmentTreatment

Pharmacotherapy to prevent MI and Pharmacotherapy to prevent MI and DeathDeath
Antiplatelet AgentsAntiplatelet AgentsAntithrombotic AgentsAntithrombotic AgentsLipid lowering AgentsLipid lowering AgentsACEACE--InhibitorsInhibitorsBeta BlockersBeta Blockers

Antianginal & AntiAntianginal & Anti--ischemic ischemic TherapyTherapy
Beta blockersBeta blockersNitratesNitratesCalcium Channel BlockersCalcium Channel BlockersRanolazineRanolazine
Antiplatelet AgentsAntiplatelet Agents
AspirinAspirinTiclidTiclidPlavixPlavix

AspirinAspirin
Inhibits cyclooxygenase and synthesis of Inhibits cyclooxygenase and synthesis of platelet thromboxane A2platelet thromboxane A2Stable angina trial > 3000 pts had on average a Stable angina trial > 3000 pts had on average a 33% reduction in risk of CV events33% reduction in risk of CV events

TiclidTiclid
Inhibits platelet aggregation by binding with Inhibits platelet aggregation by binding with the ADP receptorsthe ADP receptorsReduces blood viscosity by reduction in Reduces blood viscosity by reduction in plasma fibrinogen and increase in red cell plasma fibrinogen and increase in red cell deformabilitydeformabilityNot been shown to decrease adverse CV Not been shown to decrease adverse CV events in pts with stable anginaevents in pts with stable angina

PlavixPlavix
Selectively and irreversibly inhibits the Selectively and irreversibly inhibits the binding of ADP to its platelet receptors binding of ADP to its platelet receptors thereby blocking ADP mediated activation of thereby blocking ADP mediated activation of GP IIb/IIIa complexGP IIb/IIIa complexCAPRIE trial plavix did slightly better than CAPRIE trial plavix did slightly better than Aspirin in decreasing the combined risk of MI, Aspirin in decreasing the combined risk of MI, vascular death or ischemic strokevascular death or ischemic stroke

Antithrombotic TherapyAntithrombotic Therapy
LMW heparin LMW heparin ––daily s/c administrationdaily s/c administrationDecrease fibrinogen levelDecrease fibrinogen levelImprove clinical class and exercise time to 1 mm Improve clinical class and exercise time to 1 mm ST depression and peak ST depressionST depression and peak ST depression
Low intensity oral anticoagulation with Low intensity oral anticoagulation with warfarinwarfarin-- INR 1.47 INR 1.47
Decrease risk of ischemic events in pts with CAD Decrease risk of ischemic events in pts with CAD but no anginabut no angina

Lipid Lowering AgentsLipid Lowering Agents
HMGHMG--CoA reductase InhibitorCoA reductase Inhibitor--Significant reduction in non fatal and fatal MISignificant reduction in non fatal and fatal MI
Other Agents includeOther Agents includeFibric acid derivativesFibric acid derivativesBile acid sequestrantsBile acid sequestrantsNiacinNiacin
Angiotensin Converting Enzyme Angiotensin Converting Enzyme InhibitorsInhibitors
Multiple trials have shown decrease in CV Multiple trials have shown decrease in CV morbidity and mortalitymorbidity and mortalityHOPE trial HOPE trial ––Heart Outcomes Prevention Heart Outcomes Prevention Evaluation Evaluation
Reduced CV death, MI & stroke in pts who were Reduced CV death, MI & stroke in pts who were high risk for or had vascular disease in the absence high risk for or had vascular disease in the absence of heart failureof heart failure
Should be used as routine secondary Should be used as routine secondary prevention for pts with known CADprevention for pts with known CAD

Selected Developments in the Selected Developments in the History of Antianginal History of Antianginal
Treatment Treatment
Adapted from: Poole-Wilson PA, et al. Eur Heart J Suppl. 2006. Gruntzig A and Schneider HJ. Schweiz Med Wochenscher. 1977. [email protected]. Accessed April 17, 2006. Ranexa® (ranolazine extended-release tablets) PI. February 2006.
19th century
1867: Nitrates

Nitrate TherapyNitrate Therapy
Endothelin independent vasodilatorsEndothelin independent vasodilators-- reduce reduce myocardial oxygen demand and improve myocardial oxygen demand and improve perfusionperfusionAntithrombotic effects and anti platelet effect Antithrombotic effects and anti platelet effect in pts with stable anginain pts with stable anginaImprove exercise tolerance Improve exercise tolerance In combination with CCB and BB produce In combination with CCB and BB produce greater antianginal and anti ischemic effectsgreater antianginal and anti ischemic effects
20th century
Selected Developments in the Selected Developments in the History of Antianginal History of Antianginal
Treatment Treatment
Adapted from: Poole-Wilson PA, et al. Eur Heart J Suppl. 2006. Gruntzig A and Schneider HJ. Schweiz Med Wochenscher. 1977. [email protected]. Accessed April 17, 2006. Ranexa® (ranolazine extended-release tablets) PI. February 2006.
19th century
1867: Nitrates
1962: Beta-blockers
Beta BlockersBeta Blockers
They simultaneously improve symptoms and They simultaneously improve symptoms and prevent SCD and MIprevent SCD and MIDecrease myocardial oxygen demandDecrease myocardial oxygen demandVery effective with nitratesVery effective with nitratesVasospastic AnginaVasospastic Angina-- worsens with beta worsens with beta blockerblocker

20th century
Selected Developments in the Selected Developments in the History of Antianginal History of Antianginal
Treatment Treatment
Adapted from: Poole-Wilson PA, et al. Eur Heart J Suppl. 2006. Gruntzig A and Schneider HJ. Schweiz Med Wochenscher. 1977. [email protected]. Accessed April 17, 2006. Ranexa® (ranolazine extended-release tablets) PI. February 2006.
19th century
1867: Nitrates 1981: CCBs
1962: Beta-blockers1977: PCI
1967: CABG

Calcium Channel BlockersCalcium Channel Blockers
Reduce the transmembrane flux of calcium via Reduce the transmembrane flux of calcium via Ca channelsCa channelsDecrease coronary vascular resistanceDecrease coronary vascular resistanceIncrease coronary blood flowIncrease coronary blood flowDecrease SVR and arterial pressureDecrease SVR and arterial pressureVery effective in vasospastic anginaVery effective in vasospastic angina

21st century20th century
Selected Developments in the Selected Developments in the History of Antianginal History of Antianginal
Treatment Treatment
Adapted from: Poole-Wilson PA, et al. Eur Heart J Suppl. 2006. Gruntzig A and Schneider HJ. Schweiz Med Wochenscher. 1977. [email protected]. Accessed April 17, 2006. Ranexa® (ranolazine extended-release tablets) PI. February 2006.
19th century
1867: Nitrates 1981: CCBs
1962: Beta-blockers1977: PCI
1967: CABG
2006: Ranolazine
Current Hypothesis of Ischemia Current Hypothesis of Ischemia at the Cellular Levelat the Cellular Level
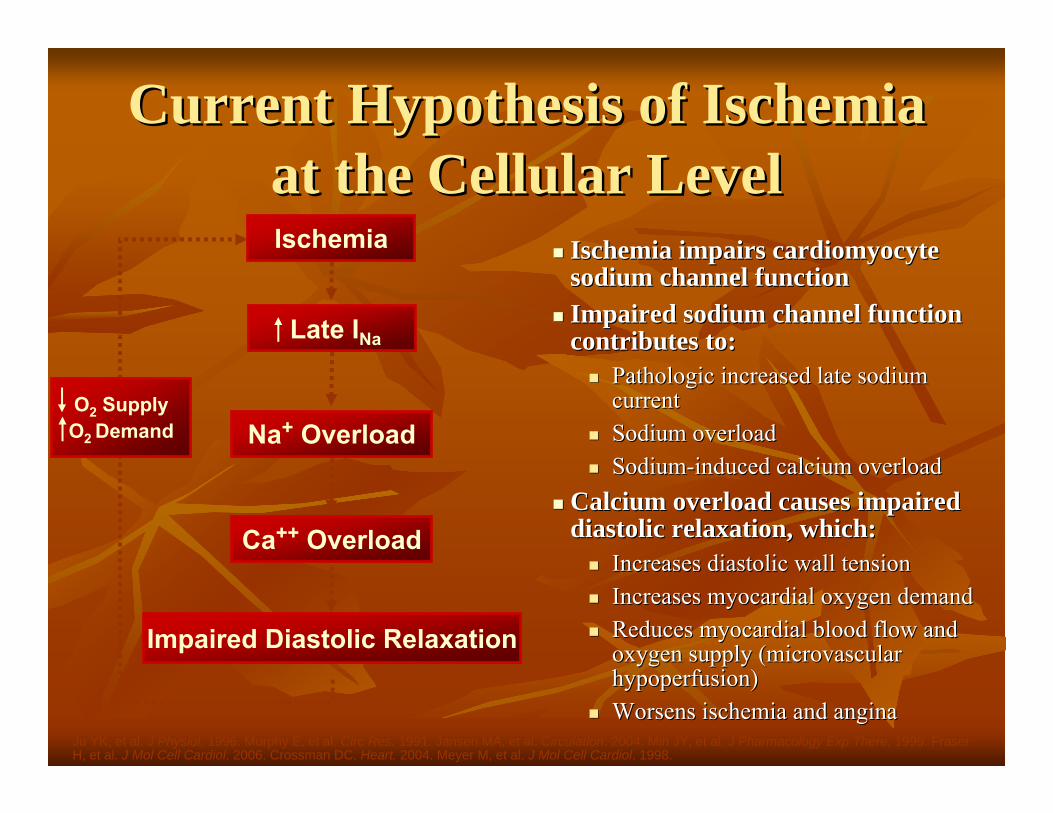
Ischemia impairs cardiomyocyte Ischemia impairs cardiomyocyte sodium channel functionsodium channel functionImpaired sodium channel function Impaired sodium channel function contributes to:contributes to:
Pathologic increased late sodium Pathologic increased late sodium currentcurrentSodium overloadSodium overloadSodiumSodium--induced calcium overloadinduced calcium overload
Calcium overload causes impaired Calcium overload causes impaired diastolic relaxation, which:diastolic relaxation, which:
Increases diastolic wall tensionIncreases diastolic wall tensionIncreases myocardial oxygen demandIncreases myocardial oxygen demandReduces myocardial blood flow and Reduces myocardial blood flow and oxygen supply (microvascular oxygen supply (microvascular hypoperfusion)hypoperfusion)Worsens ischemia and anginaWorsens ischemia and angina
Ischemia
Late INa
Na+ Overload
Impaired Diastolic Relaxation
Ca++ Overload
Ju YK, et al. J Physiol. 1996. Murphy E, et al. Circ Res. 1991. Jansen MA, et al. Circulation. 2004. Min JY, et al. J Pharmacology Exp There. 1999. Fraser H, et al. J Mol Cell Cardiol. 2006. Crossman DC. Heart. 2004. Meyer M, et al. J Mol Cell Cardiol. 1998.
O2 SupplyO2 Demand

RanolazineRanolazine
RanolazineRanolazine is a novel is a novel antianginalantianginal agent.agent.Mechanism of action is not fully elucidatedMechanism of action is not fully elucidatedThought to act by inhibiting the late sodium Thought to act by inhibiting the late sodium current current
Ranexa® (ranolazine extended-release tablets) PI. February 2006.
RanolazineRanolazine
RanolazineRanolazine has has antianginalantianginal and antiand anti--ischemic effects ischemic effects that do not depend upon reductions in HR or BPthat do not depend upon reductions in HR or BP
Does not increase the rateDoes not increase the rate--pressure product at maximal pressure product at maximal exercise exercise Minimal changes in mean HR (<2 Minimal changes in mean HR (<2 bpmbpm) and systolic BP ) and systolic BP (<3 mm Hg)(<3 mm Hg)BP increased by approximately 10 to 15 mm Hg in patients BP increased by approximately 10 to 15 mm Hg in patients with severe renal impairment; BP should be monitored with severe renal impairment; BP should be monitored regularly in such patientsregularly in such patients
Complementary to standard Complementary to standard antianginalantianginal therapytherapy
Ranexa: IndicationRanexa: IndicationRanexa (ranolazine extendedRanexa (ranolazine extended--release tablets) is release tablets) is indicated for the treatment of indicated for the treatment of chronic chronic angina angina
Because Ranexa prolongs the QT interval, it Because Ranexa prolongs the QT interval, it should be reserved for patients who have not should be reserved for patients who have not achieved an adequate response with other achieved an adequate response with other antianginal drugsantianginal drugs
Ranexa should be used in combination with Ranexa should be used in combination with amlodipine, betaamlodipine, beta--blockers, or nitrates blockers, or nitrates
The effect on angina rate or exercise tolerance The effect on angina rate or exercise tolerance appeared to be smaller in women than in menappeared to be smaller in women than in men
Ranexa® (ranolazine extended-release tablets) PI. February 2006.

RanolazineRanolazine: Adverse Effects: Adverse Effects
• The incidence of dizziness with 1000 mg b.i.d. ranolazine was 6% (vs 2% placebo), while the incidence of syncope was 0.7% (vs 0% placebo)
22 (3)22 (3)11 (2)11 (2)HeadacheHeadache
41 (5)41 (5)12 (2)12 (2)DizzinessDizziness
Nervous system disordersNervous system disorders
33 (4)33 (4)5 (1)5 (1)NauseaNausea
63 (8)63 (8)9 (2)9 (2)ConstipationConstipation
Gastrointestinal disordersGastrointestinal disordersRanolazineRanolazinen=835 (%)n=835 (%)
PlaceboPlacebon=552 (%)n=552 (%)
Doses include 500 mg b.i.d., 750 mg b.i.d., and 1000 mg b.i.d.. The 750 mg dose of ranolazine is not approved.Ranexa® (ranolazine extended-release tablets) PI. February 2006.
Safety in Older PatientsSafety in Older PatientsOf the patients with chronic angina treated with ranolazine in Of the patients with chronic angina treated with ranolazine in controlled studies, 496 (48%) were controlled studies, 496 (48%) were ≥≥65 years of age and 114 (11%) 65 years of age and 114 (11%) were were ≥≥75 years of age75 years of age
A higher incidence of placeboA higher incidence of placebo--subtracted adverse events (23%) was subtracted adverse events (23%) was observed in patients observed in patients ≥≥75 years of age on ranolazine (constipation 75 years of age on ranolazine (constipation [19%], nausea [6%], dizziness [6%])[19%], nausea [6%], dizziness [6%])
A higher incidence of placeboA higher incidence of placebo--subtracted discontinuations (11%) subtracted discontinuations (11%) due to unacceptable AEs was observed in patients due to unacceptable AEs was observed in patients ≥≥75 years of age on ranolazine75 years of age on ranolazine
Dose selection for an elderly patient should be cautiousDose selection for an elderly patient should be cautious
Ranexa® (ranolazine extended-release tablets) PI. February 2006.

Safety: DoseSafety: Dose--Related Increases in Related Increases in QT Interval Observed QT Interval Observed
QTc corrected for heart rate with Fridericia’s formula.CVT data on file RAN00253-4. Ranexa® (ranolazine extended-release tablets) PI. February 2006.
• Ranolazine prolongs the QTc interval in a dose-related manner– Linear relationship: 2.6 msec/1000 ng/mL
• A mean effect of 6 msec on QTc was observed at the highest recommended dose of ranolazine
– 5% of patients experienced QTc changes of at least 15 msec• QT changes were not related to age, weight, gender, race, heart rate,
CHF class, and diabetes • While the clinical significance of QTc prolongation in the case of
ranolazine is unknown, other drugs with this potential have beenassociated with torsades de pointes–type arrhythmias and sudden death
PlaceboPlacebo
−−2.3 2.3 (15.6)(15.6)
Mean change Mean change in QTc, msec in QTc, msec
(SD)(SD)
RanolazineRanolazine
1000 mg 1000 mg b.i.db.i.d..
5.4 5.4 (14.7)(14.7)
500 mg 500 mg b.i.db.i.d..
1.9 1.9 (20.6)(20.6)

Ranolazine:NSTEMIRanolazine:NSTEMI--ACSACS
MERLINMERLIN--TIMI 36 TrialTIMI 36 TrialNot effective in reducing major CV eventsNot effective in reducing major CV events13% relative reduction in risk of recurrent 13% relative reduction in risk of recurrent ischemiaischemiaSignificant reduction in the frequency of Significant reduction in the frequency of arrythmiasarrythmias detected by detected by HolterHolterNo excess of arrhythmias or SCD during a median No excess of arrhythmias or SCD during a median 1 yr 1 yr f/uf/uMore syncope with More syncope with ranolazineranolazine

Other TherapiesOther Therapies
Fish oil and garlicFish oil and garlic-- no current evidence to no current evidence to suggest a clinical benefitsuggest a clinical benefitAnti oxidant therapyAnti oxidant therapy-- may be of benefit , but may be of benefit , but the benefits are still unresolvedthe benefits are still unresolvedChelation therapyChelation therapy-- 4 randomized trials found 4 randomized trials found no benefit on progression of disease or clinical no benefit on progression of disease or clinical outcomeoutcome

Revascularization for Chronic Revascularization for Chronic Stable AnginaStable Angina
CABGCABGPCIPCI

Alternative TherapiesAlternative Therapies
Enhanced External Counter PulsationEnhanced External Counter PulsationSpinal cord stimulationSpinal cord stimulationSurgical Laser Surgical Laser TransmyocardialTransmyocardialRevascularizationRevascularizationExercise TrainingExercise Training-- Cardiac RehabilitationCardiac Rehabilitation
Spinal Cord StimulationSpinal Cord Stimulation
Introduced in 1987Introduced in 1987Placement of a stimulating electrode in the Placement of a stimulating electrode in the dorsal epidural space C7dorsal epidural space C7--T1 levelT1 level2 small trials2 small trialsPaucity of data on intermediate and long term Paucity of data on intermediate and long term benefitsbenefits

EECPEECP
Diastolic Augmentation of blood flowDiastolic Augmentation of blood flowPressure is applied via a series of cuffs on the Pressure is applied via a series of cuffs on the LE in a sequence synchronized with the LE in a sequence synchronized with the cardiac cyclecardiac cycleTrials have shown improvement in angina Trials have shown improvement in angina symptoms in 75symptoms in 75--80% pts80% pts

Laser TMRLaser TMR
Create a series of transmural endomyocardial Create a series of transmural endomyocardial channels to improve myocardial channels to improve myocardial revascularizationrevascularizationSurgical TMRSurgical TMRPercutaneous TMRPercutaneous TMR
Surgical TMRSurgical TMR
Use a Carbon Dioxide or YAG laserUse a Carbon Dioxide or YAG laserMechanism for improvement of symptomsMechanism for improvement of symptoms
Denervation of myocardiumDenervation of myocardiumIncreased myocardial perfusionIncreased myocardial perfusionStimulation of angiogenesisStimulation of angiogenesis
No data on long term effectsNo data on long term effects

Percutaneous TMRPercutaneous TMR
A special catheter is used A special catheter is used –– holmium: YAG holmium: YAG laserlaser2 randomized trials 2 randomized trials
Increase in ex toleranceIncrease in ex toleranceFreedom from anginaFreedom from angina
Not FDA approvedNot FDA approved

Exercise TrainingExercise TrainingCardiac RehabilitationCardiac Rehabilitation
Increases exercise toleranceIncreases exercise toleranceImprove sense of well beingImprove sense of well being
ConclusionConclusion
Goal of therapy is to improve Quantity and Goal of therapy is to improve Quantity and Quality of lifeQuality of lifeAA-- Aspirin and anti anginal therapyAspirin and anti anginal therapyBB-- betabeta--blocker and blood pressureblocker and blood pressureCC-- cigarette smoking and cholesterolcigarette smoking and cholesterolDD-- diet and diabetesdiet and diabetesEE-- education and exerciseeducation and exercise