
Pharmacokinetics and dynamics
41
Pharmacokinetics and Pharmacodynamics Moderator: Dr Shruthi
-
Upload
dranest87 -
Category
Health & Medicine
-
view
176 -
download
1
Transcript of Pharmacokinetics and dynamics

Pharmacokinetics
and
Pharmacodynamics
Moderator: Dr Shruthi

Definitions
Pharmacokinetics
Relationship between
drug dose and drug
concentration in in
plasma.
Absorption distribution
and clearance.
Pharmacodynamics
Relationship between
plasma drug concentration
and pharmacologic effect.
Potency efficacy and
therapeutic window

Pharmacokinetics

Volume of
distribution:volume = amount (dose)/conc.
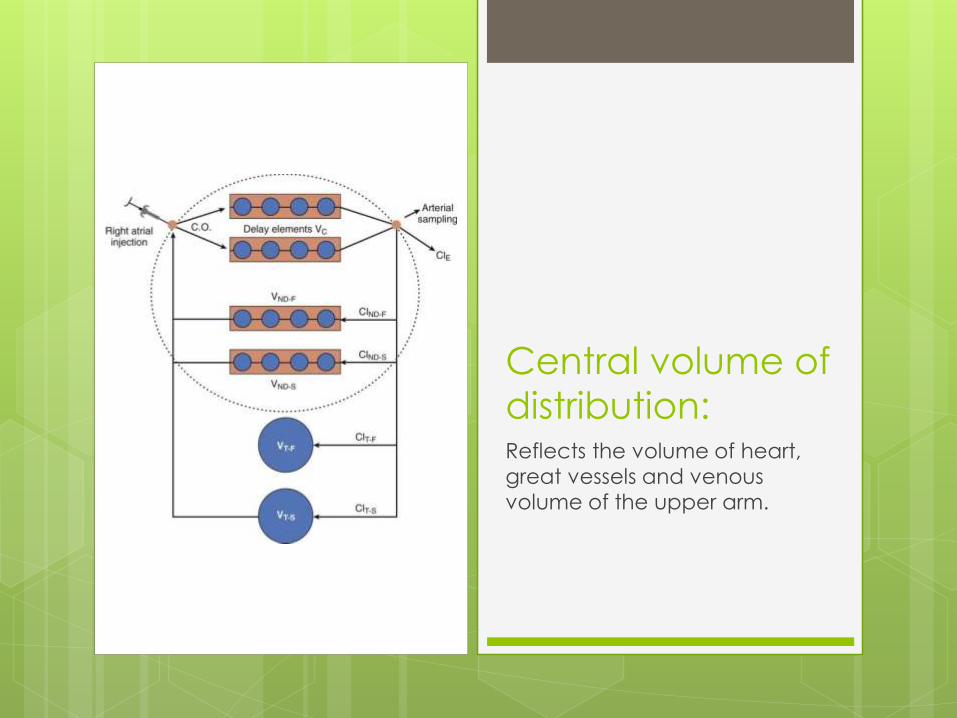
Central volume of
distribution:Reflects the volume of heart,
great vessels and venous
volume of the upper arm.

Peripheral volume of
distribution:
Inter compartmental clearance.
Mammillary model
Vdss: Volume of distribution at steady
state.
Vdss= central volume+ peripheral volume

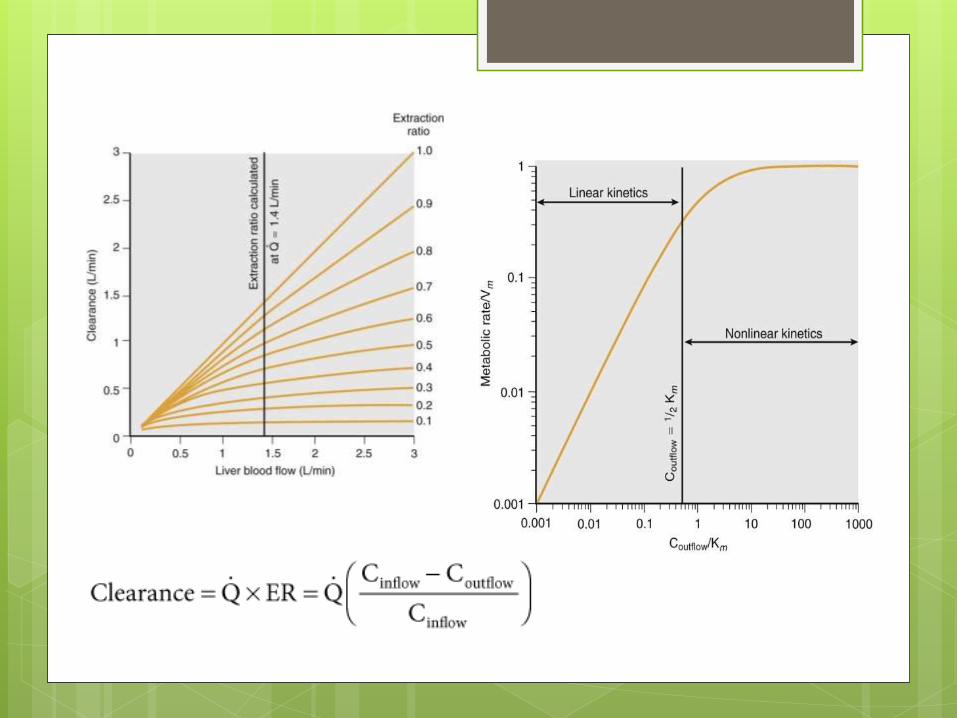
ClearanceThe volume completely
cleared of drug per unit time.
Actual rate is, clearance times
the concentration.

Hepatic Clearance

Renal Clearance
Tissue Clearance
Distribution Clearance
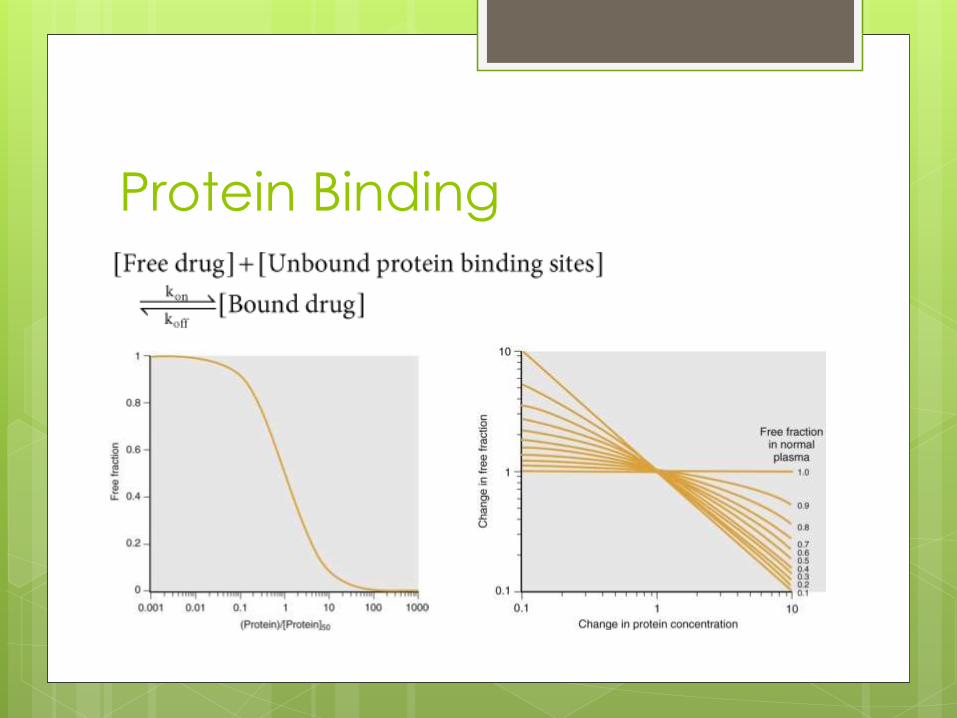
Protein Binding

First and zero order processes:
Zero order: processes continuing at a constant rate.
First order: rate proportional to the amount

Compartmental
pharmacokinetic models:

Increased volume of distribution
Increased clearance

Multi-compartment models

Pharmacodynamics

Classic receptor theory:
Receptor: component of cell that interacts selectively
with extracellular compound to initiate a cascade of
biochemical events.
The amount of drug at the receptor is a function of dose,
time and pharmacokinetic properties of the drug.

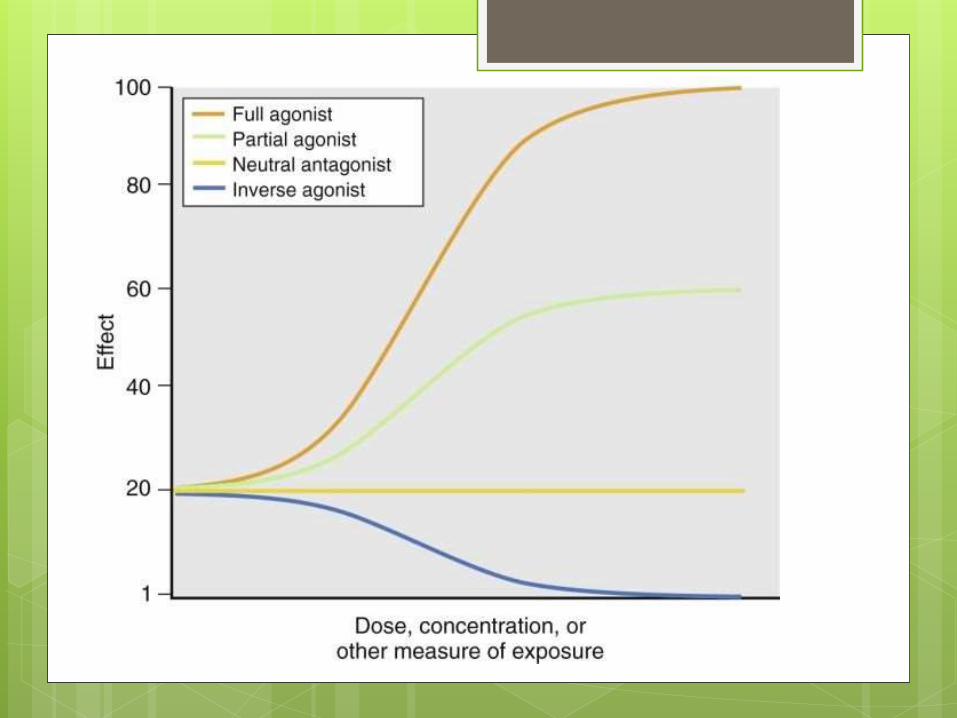
Agonists and antagonists:
Agonists Mimic endogenous
hormones when bound
to receptor.
Full agonists- completely
activate receptor
Partial agonists-only
partially activate
receptor
Antagonists
Competitive antagonists
Non competitive
antagonists
Inverse agonists
Neutral antagonists
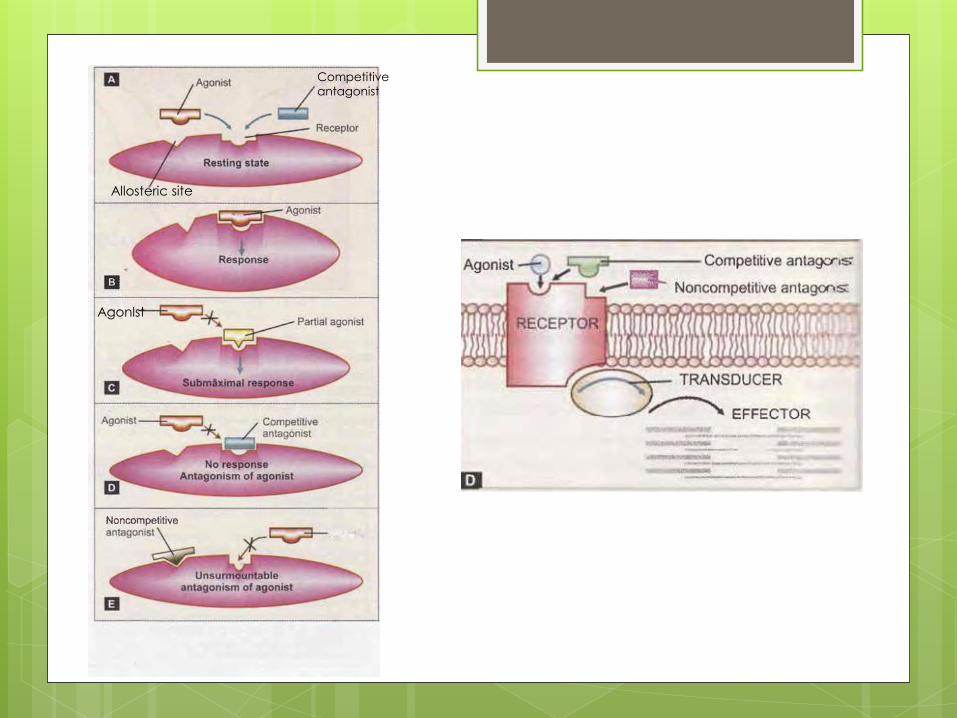
Competitive
antagonist
Allosteric site
Agonlst

AntagonistsCompetitive Antagonist
Antagonist binds with the same receptor as the agonist
Antagonist resembles chemically with the agonist
Parallel rightward shift of agonist DRC The same maximal response can be
attained by increasing dose of agonist (surmountable antagonism) The antagonist appears to have
inactivated a certain number of agonist molecules
Intensity of response depends on the concentration of both agonist and antagonist
Examples: ACh-Atropine,Morphine-Naloxone, Vecuronium -ACh
Non competitveAntagonist
Binds to another site of receptor
Does not resemble the agonist
Flattening of agonist DRC
Maximal response is suppressed(unsurmountableantagonism)
The antagonist appears to have inactivated a certain number of receptors
Maximal response depends only on the concentration
of antagonist
Diazepam-Bicuculline

Receptor States:
Spontaneous
conversion of
receptors from an
inactive to active
stateG- guanine nucleotide
E-

Equilibrium between inactive
receptors and active receptors
is tissue specific and depends
on the type of ligand
administered.
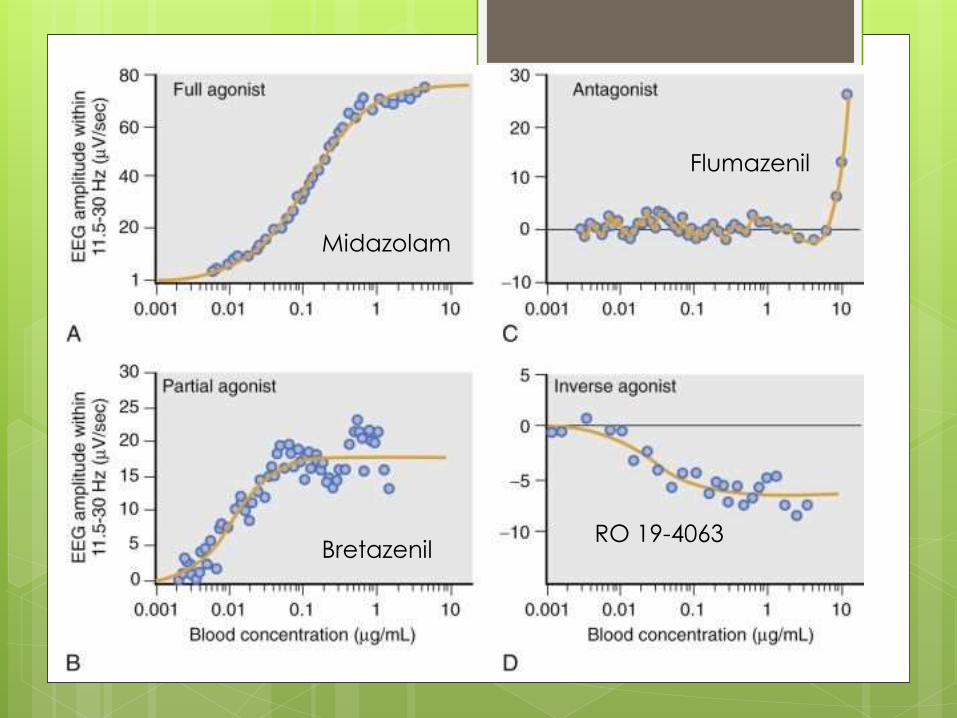
Midazolam
Bretazenil
Flumazenil
RO 19-4063

Receptor structure:

G-protein coupled receptor:
Most abundant
type of receptor
in the body.

Ion channels:Most hypnotics act through
the potentiation of GABA
and GABAa ligand gated
ion channels.
They permit certain drugs to
directly alter membrane
potential.
ION PUMPS:
e.g sodium posassium
ATPase pump.

Second messengers:
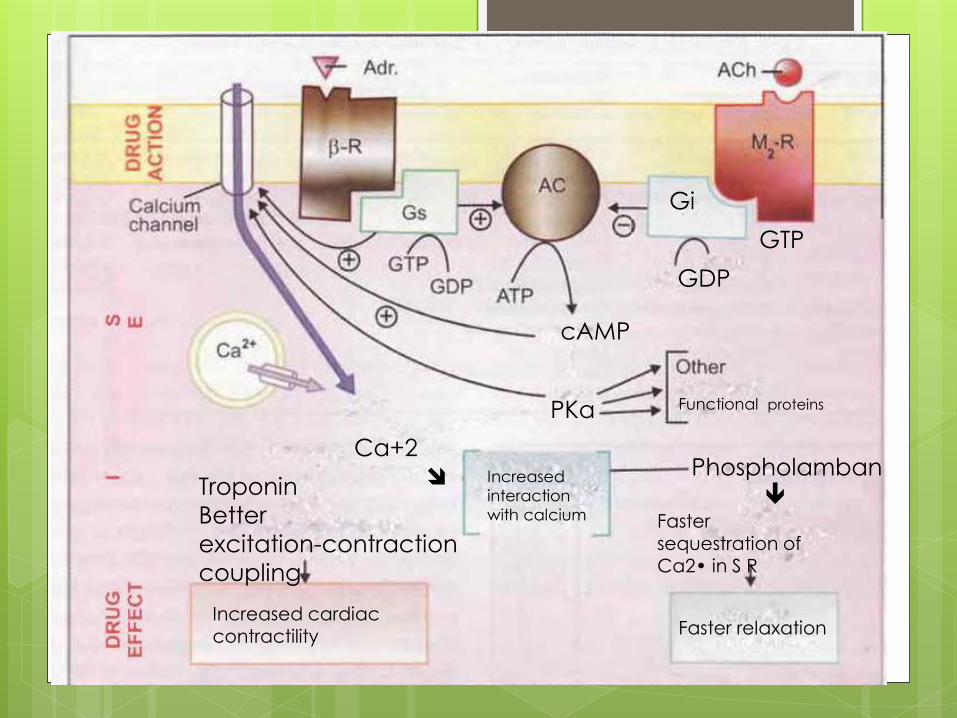
cAMP
PKa Functional proteins
Gi
GDP
GTP
Increased
interaction
with calcium
Troponin
Better
excitation-contraction
coupling
Ca+2
Increased cardiac contractility Faster relaxation
Faster
sequestration ofCa2• in S R
Phospholamban
Clinical evaluation of
drug effects:

Potency and Efficacy
Potency
The effect of a given dose of a drug.
Quantity of drug that must be administered to produce a specific effect.
Efficacy
Intrinsic ability of a
drug to produce a
given physiologic
or clinical effect.

The concentration-response curve is shifted to the right (B➙C) in the presence of a competitive antagonist after desensitization.
Curve C might also represent an agonist with lower receptor affinity (Ka) or potency than curve B (or both).
Curve A represents an agonist with higher receptor affinity or potency than curve B.

Effective Dose and Lethal
DoseEffective Dose
ED50
The dose of a drug
required to
produce a specific
effect in 50% of
individuals to
whom it is
administered.
Lethal dose LD50
The dose of a drug
required to
produce death in
50% of patients.


Variability in drug
response

Pharmacogenetics
Genetic polymorphisms
Genetic variability in pharmacokinetics
Genetic variability in pharmacodynamics

Patient physiology:Age:1.Total body water
2.Lean body mass
3.Liver volume and liver blood flow
4.Cardiac output
5.Albumin levels decreased
6.Alpha1 glycoprotein increased
Disease states

Drug Interactions Desensitization:Waning of physiologic responsiveness to a drug over time.
TACHYPHYLAXIS- rapid development of tolerance when doses of a drug given in quick succession result in marked reduction in response.
E.g. Ephedrine, Tyramine, Nicotine
TOLERANCE- Requirement of higher doses of a drug to produce a given response.
E.g. tolerance to analgesic and euphoric action of morphine.
Cross tolerance: Development of tolerance to pharmacologically related drugs
E.g. Alcoholics are relatively tolerant to barbiturates

Increased receptor sensitivity:
Long term exposure to a drug leads to compensatory
responses by the receptor system.
Drug resistance:
Tolerance of micro-organisms to inhibitory effect of anti
microbials.

References
Millers 7th edition
Clinical Anesthesiology- Millers
Stoeltings handbook of pharmacology
and physiology in anesthetic practice
Essentials of medical pharmacology, K D
Tripathi

Thank You


















