Session FF-05 Expected Family Contribution Marianna Deeken U.S. Department of Education.
Upload
susanna-goldenCategory
view
220download
1
Pharmacogenetics and the Pharmacogenetics and the Promise of Individualized Promise of Individualized
Medical CareMedical Care
John Deeken, M.D.John Deeken, M.D.
May 18, 2009May 18, 2009

PharmacogenomicsPharmacogenomics

Non-Responders and Patients Experiencing
Severe Toxicity
All patients with same diagnosis
Responders and Patients not Experiencing
Severe Toxicity

Sources of Pharmacokinetic and Sources of Pharmacokinetic and Pharmacodynamic VariabilityPharmacodynamic Variability
Drug Specific:Dose & Schedule
Dosage formMorphometric:Body SizeBody Composition
Genetics:
Environment:Drug-drug interactions
Drug-CAM interactionsDrug-formulation interactions
Drug-food constituent interactions
Physiologic:DiseaseHepatic FunctionRenal Function
Demographic:AgeRace/EthnicitySex
VariabilityVariability

PharmacogeneticsPharmacogenetics
Implications of polymorphismson Pharmacokinetics
Implications of polymorphismson Drug Effect
• Drug Absorption• Drug Distribution • Drug Elimination• Drug Metabolism• Drug Activation
• Receptors• Target Proteins

Genetic PolymorphismsGenetic Polymorphisms
Single Nucleotide Polymorphisms Single Nucleotide Polymorphisms (SNPs)(SNPs)Non-synonymous and Non-synonymous and
synonymoussynonymous Upstream/downstream regulatory Upstream/downstream regulatory
regionsregions Copy numberCopy number

PharmacogeneticsPharmacogenetics
Implications of polymorphismson Pharmacokinetics
Implications of polymorphismson Drug Effect
• Drug Absorption• Drug Distribution • Drug Elimination• Drug Metabolism• Drug Activation
• Receptors• Target Proteins

Transporters Mediate Transporters Mediate AbsorptionAbsorption
www.solvo.com

Transporters Mediate Bile Transporters Mediate Bile EliminationElimination
www.solvo.com

Transporters Mediate Renal Transporters Mediate Renal EliminationElimination
www.solvo.com

ABCG2 (BCRP, ATP-binding cassette)ABCG2 (BCRP, ATP-binding cassette)
Involved in intrinsic or acquired multidrug Involved in intrinsic or acquired multidrug resistance (MDR) phenotype of tumor cellsresistance (MDR) phenotype of tumor cells
ABCG2 ABCG2 encodes a half transporterencodes a half transporter
Located on chromosome 4q-22Located on chromosome 4q-22
66 kb; 16 exons; 15 introns 66 kb; 16 exons; 15 introns
69 Known genetic polymorphisms including 65 69 Known genetic polymorphisms including 65 SNPs; 13 SNPs in exons; 7 SNPs cause amino acid SNPs; 13 SNPs in exons; 7 SNPs cause amino acid substitutionssubstitutions

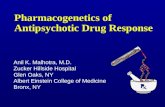
Location of ABCG2 C421A and its functional Location of ABCG2 C421A and its functional consequencesconsequences
OUT
MEMBRANE
IN
200100
300
400
500
600
ATP SITE
N Terminus
C Terminus
MXR SNPs V12M
Q141K E366E L475L D620N
E366E
V12M
L475L
Q141K
D620N
R482
Non-synonymous ABCG2 Q141K SNP: substituted amino acid residue
- The 421C to A transition at exon 5 leads to a Lys to Gln amino acid substitution at codon 141 (Q141K)
- Functional studies suggest that the C421A polymorphism has:
1. Reduced topotecan transport
2. Reduced protein expression in vitro
3. A 3-fold higher diflomotecan AUC after i.v. administration

ABCG2 pharmacogenetics: influence on imatinib ABCG2 pharmacogenetics: influence on imatinib (STI-571; Gleevec) pharmacokinetics(STI-571; Gleevec) pharmacokinetics
Parameter WT* Het** P
Cmax 11.2 36.5 0.0064
AUC 140 536 0.0063
* N = 32
** N = 4
Patients with GIST treated with imatinib at dose ranging, 100 – 1000 mg p.o.
Lepper E, et al (Figg), Pro ASCO 2005

PharmacogeneticsPharmacogenetics
Implications of polymorphismson Pharmacokinetics
Implications of polymorphismson Drug Effect
• Drug Absorption• Drug Distribution • Drug Elimination• Drug Metabolism• Drug Activation
• Receptors• Target Proteins

Drug Metabolizing Enzymes
Evans and Relling, Science 286: 487-91, 1999

PGx of Drugs Used in Medical OncologyPGx of Drugs Used in Medical Oncology
Drug Pathway Variability in CL
Amonafide N-acetyl transferase (NAT) >3-fold
Busulfan Glutathione S-transferase (GST) 10-fold
Docetaxel Cytochrome P-450 (CYP) 3A4/3A5 4 to 9-fold
5-Fluorouracil Dihydropyrimidine dehydrogenase 10-fold
6-Mercaptopurine Thiopurine methyltransferase >30-fold
Evans and Relling, Science 286: 487-91, 1999
Example of anticancer drug metabolism by polymorphic enzymes

Warfarin (Coumadin)Warfarin (Coumadin)
Name Your PoisonName Your Poison

Warfarin (Coumadin)Warfarin (Coumadin) Used for chronic Used for chronic
anticoagulationanticoagulation INR and lab testingINR and lab testing Two enantiomers (R- and Two enantiomers (R- and
S-)S-)

WarfarinWarfarin
Name Your PoisonName Your Poison Used for chronic anticoagulationUsed for chronic anticoagulation INR and lab testingINR and lab testing Two enantiomers, R and STwo enantiomers, R and S

Warfarin Metaboli
sm
Importance of CYP2C9

Warfarin Pharmacodyna
mics
Importance of
VORC1

Warfarin -PGxWarfarin -PGx
PGx: CYP2C9 and VORC1PGx: CYP2C9 and VORC1 Expert Committee Recommendation to Expert Committee Recommendation to
FDAFDA Consider PGx testing, but needs further Consider PGx testing, but needs further
studystudy Multiple studies currently ongoing, main Multiple studies currently ongoing, main
U.S. study funded by NIHU.S. study funded by NIH Medicare announced May 4 that it will not Medicare announced May 4 that it will not
pay for genetic testing at this timepay for genetic testing at this time Will pay for genetic testing in clinical trialsWill pay for genetic testing in clinical trials

PGx and Clopidogrel PGx and Clopidogrel (Plavix)(Plavix)
Thienopyridine inhibitor of platelet P2YThienopyridine inhibitor of platelet P2Y1212 ADPADP
Prodrug, requires activitation by CYP450 Prodrug, requires activitation by CYP450 enzyme(s) and also inactivated by CYP450 enzyme(s) and also inactivated by CYP450 enzyme(s) and other esterasesenzyme(s) and other esterases
Much variability between patients in Much variability between patients in terms of pK and PD (platelet aggregation)terms of pK and PD (platelet aggregation)

PGx and Clopidogrel PGx and Clopidogrel (Plavix)(Plavix)
Mega et al (NEJM Jan 22, 2009): Mega et al (NEJM Jan 22, 2009): healthy volunteers pK (n=162)healthy volunteers pK (n=162) Cardiac patients on TRITON-TIMI study (n=1477)Cardiac patients on TRITON-TIMI study (n=1477)
Pts with at least one reduced function variant Pts with at least one reduced function variant in in CYP2C19CYP2C19:: 32% reduction in active drug plasma levels32% reduction in active drug plasma levels 53% increase risk of death from CV causes, MI, or 53% increase risk of death from CV causes, MI, or
stroke (12.1% vs 8.0%, HR 1.53)stroke (12.1% vs 8.0%, HR 1.53) Three-fold increased risk of stent thrombosis Three-fold increased risk of stent thrombosis
(2.6% v. 0.8%)(2.6% v. 0.8%) Caveat: research paid for by Eli Lilly and Daiichi Caveat: research paid for by Eli Lilly and Daiichi
Sankyo since study was of prasugrel vs clopidogrelSankyo since study was of prasugrel vs clopidogrel FDA currently evaluating evidence to FDA currently evaluating evidence to
consider requiring PGx testing before consider requiring PGx testing before starting clopidogrelstarting clopidogrel

Irinotecan (CPT-11)Irinotecan (CPT-11)
Topoisomerase I inhibitorTopoisomerase I inhibitor Metabolized to active compound SN-38Metabolized to active compound SN-38 Used in colon cancerUsed in colon cancer DLT – diarrheaDLT – diarrhea SN-38 inactivated by UGT1A1 SN-38 inactivated by UGT1A1
glucoronidationglucoronidation Polymorphism in UGT1A1 (Polymorphism in UGT1A1 (UGT1A1*28UGT1A1*28) )
leads to diminished inactivation, higher leads to diminished inactivation, higher drug levels, and higher toxicitydrug levels, and higher toxicity

Mathijessen RHJ et al. Clin Cancer Res 2001:2168

Pharmacogenomics and Oncology:Pharmacogenomics and Oncology:
New label for Irinotecan, July 2005:New label for Irinotecan, July 2005:
FDA approved test in December, 2005FDA approved test in December, 2005
We still do not know what to do with doseWe still do not know what to do with dose

PharmacogeneticsPharmacogenetics
Implications of polymorphismson Pharmacokinetics
Implications of polymorphismson Drug Effect
• Drug Absorption• Drug Distribution • Drug Elimination• Drug Metabolism• Drug Activation
• Receptors• Target Proteins

TamoxifenTamoxifen
SERMSERM Used for adjuvant therapy in ER/PR+ Used for adjuvant therapy in ER/PR+
breast CAbreast CA Metabolite Endoxifen is 100x more Metabolite Endoxifen is 100x more
effective than parent compoundeffective than parent compound CYP2D6 mediates activation of CYP2D6 mediates activation of
Tamoxifen to EndoxifenTamoxifen to Endoxifen

TamoxifenTamoxifen
Importance Importance of CYP2D6of CYP2D6

PharmacogeneticsPharmacogenetics
Implications of polymorphismson Pharmacokinetics
Implications of polymorphismson Drug Effect
• Drug Absorption• Drug Metabolism• Drug Elimination• Drug Distribution• Drug Activation
• Receptors• Target Proteins

Beta Receptor and Beta Receptor and HTN/CHFHTN/CHF
Beta blockers – well namedBeta blockers – well named ADRB1 and ADRB2ADRB1 and ADRB2 In ADRB1, 2 common functional
polymorphisms (Ser49Gly and Gly389Arg). In HTN, pts treated with Metoprolol, Gly389:
WT/WT: 10.4% drop in SBP WT/Variant: 2.8% Variant/Variant: 1.1% Similar differences found in HR and SBP at rest and with
exercise
In CHF, WT patients need more medications/dosages
Liu J et al. Clin Pharmacol Ther 2003, 2006
Terra SJ, et al. Clin Pharmacol Ther 2006

Beta Receptor and ACSBeta Receptor and ACS

PharmacogeneticsPharmacogenetics
Implications of polymorphismson Pharmacokinetics
Implications of polymorphismson Drug Effect
• Drug Absorption• Drug Metabolism• Drug Elimination• Drug Distribution• Drug Activation
• Receptors• Target Proteins

Pharmacogenomics and Pharmacogenomics and FDAFDA
““Pharmacogenomics holds great promise to Pharmacogenomics holds great promise to shed scientific light on the often risky and shed scientific light on the often risky and costly process of drug development, and to costly process of drug development, and to provide greater confidence about the risks provide greater confidence about the risks and benefits of drugs in specific and benefits of drugs in specific populations. Pharmacogenomics is a new populations. Pharmacogenomics is a new field, but we intend to do all we can to use it field, but we intend to do all we can to use it to promote the development of medicines.”to promote the development of medicines.”
--Mark McClennan, M.D.Mark McClennan, M.D. FDA Commissioner Nov, FDA Commissioner Nov,
20032003

Pharmacogenomics and Pharmacogenomics and FDAFDA
2002: ‘Safe Harbor’ concept for data submissions2002: ‘Safe Harbor’ concept for data submissions 2003: Draft guidance for industry to submit genomic 2003: Draft guidance for industry to submit genomic
data data 2004: 2004:
PG identified as ‘Key opportunity’ in FDA’s PG identified as ‘Key opportunity’ in FDA’s ‘Critical Path’ for the future‘Critical Path’ for the future
Interdisciplinary PG Review Group Formed. Interdisciplinary PG Review Group Formed. First Voluntary Genomic Drug Submission (VGDS) First Voluntary Genomic Drug Submission (VGDS)
received by FDAreceived by FDA 2005 2005
Genomics Website: www.fda.gov/cder/genomicsGenomics Website: www.fda.gov/cder/genomics Final rules published on guidance for industryFinal rules published on guidance for industry

Biomarker/Genetic targets:Biomarker/Genetic targets:AbbottAbbottJohnson & JohnsonJohnson & JohnsonRoche (Swiss)Roche (Swiss)
Pharmacogenomics for individualized Rx:Pharmacogenomics for individualized Rx:PfizerPfizerBristol-Myers-SquibbBristol-Myers-SquibbGenentechGenentech
Molecular diagnostic kits/devices:Molecular diagnostic kits/devices:Roche expected sales this year: $6.5 billionRoche expected sales this year: $6.5 billion
eexpected sales by 2010: $12 billionxpected sales by 2010: $12 billion
Pharmacogenomics - IndustryPharmacogenomics - Industry

Pharmacogenomics:Pharmacogenomics:IndustryIndustry
First clinically available, FDA-approved genotype test inFirst clinically available, FDA-approved genotype test in2005 (Roche - Amplichip)2005 (Roche - Amplichip)
Chip for SNPs in all CYP450 genes, 2005 (GE)Chip for SNPs in all CYP450 genes, 2005 (GE)
Chip for p53 mutations expected mid-2006 (Roche)Chip for p53 mutations expected mid-2006 (Roche)
Affymetrix/ParAllele DMET Chip - 1,300 SNPs covering 185 Affymetrix/ParAllele DMET Chip - 1,300 SNPs covering 185 genes (enzymes and transporters) involved in druggenes (enzymes and transporters) involved in drug
metabolism Spring, 2006metabolism Spring, 2006

Pharmacogenomics and Pharmacogenomics and NIHNIH
Pharmacogenomics Research Network (PGRN)Pharmacogenomics Research Network (PGRN) Initiated based on NIH Scientific Advisory Panel Initiated based on NIH Scientific Advisory Panel
recommendation in 1999recommendation in 1999 Launched in year 2000Launched in year 2000 $140 million for first 5 years (UO1 mechanism)$140 million for first 5 years (UO1 mechanism) 12 centers funded from 2000 to 200512 centers funded from 2000 to 2005 Second 5-year period from 2005-2010, $150 Second 5-year period from 2005-2010, $150
million, again with 12 centers funded (not same as million, again with 12 centers funded (not same as original)original)
NIGMS (General Medical Science) is lead NIH NIGMS (General Medical Science) is lead NIH institute, with other institutes participating, institute, with other institutes participating, including NHLBI, NIDA, NCI, NIEHS, NHGRI, including NHLBI, NIDA, NCI, NIEHS, NHGRI, NIMH, NLM, and ORWHNIMH, NLM, and ORWH

Non-Responders and Patients Experiencing
Severe Toxicity
All patients with same diagnosis
Responders and Patients not Experiencing
Severe Toxicity
PGx – The Future of Individualized Medicine?