
Pharmacogenetic and Genomic Applications for Safety and ... · PDF file2e-NADPH+H+ NADP ++2H+...
45
Pharmacogenetic and Genomic Applications for Safety and Therapeutic Efficacy Assessment in Drug Development Programs [email protected]
-
Upload
nguyendung -
Category
Documents
-
view
220 -
download
1
Transcript of Pharmacogenetic and Genomic Applications for Safety and ... · PDF file2e-NADPH+H+ NADP ++2H+...

Pharmacogenetic and Genomic Applications for Safety and
Therapeutic Efficacy Assessment in Drug Development Programs

- Topics of my presentation –
Centre for Pharmacology and Toxicology
• Translational genomics(HUGO, disease diagnostics, clinical trialsand patient stratification)
• How SNPs affect drug safety andtherapeutic efficacy (PK, ADME genes,treatment „responder“, clinical outcome..)
• Genetic factors linked to DILI
Human Genome Project• At the DNA sequence level all humans are >99% identical
(initial draft 2001; the 1000 Genomes Project in 2010)
• Mice and chimpanzee genomes are very similar to humans; even protein coding regions are ~ 90% identical
• “Housekeeping” genes are highly conserved (human versus yeast 26% or fruit fly ~ 44%)
• Individual genomes carry ∼3 million SNPs but most do not impact protein function.
• SNPs in non-coding regions affect gene splicing, transcription factor binding, messenger RNA degradation, or the sequence of non-coding RNAs.
• Each person carries ~ 250 to 300 loss-of-function and 50 to 100 variant genes previously implicated in inherited disorders
Centre for Pharmacology and Toxicology

.
Centre for Pharmacology and Toxicology

N=149 pharmacogenomic studies listedin EU Clinical Trials Register (03.2017)
Centre for Pharmacology and Toxicology
149
60
21 2011 9 6
22
0
20
40
60
80
100
120
140
160

Pharmacogenetics of metoprolol drug disposition
2 4 6 8 12 24Time (h)
200
400
600
Deficient metabolism of drugs is referred to as POOR METABOLIZERas these individuals exert a dramatic change in pharmacokinetic parameters.
METABOLIC RATIO EM
METABOLIC RATIO EM PM
3.5 billion years
today
Cytochrome P450
• There is no life without CYP monooxygenases; all livingsystems (plants, bacteria, fungi, animals) carry CYP genes.
• In animals original functions lie within chlosterolmetabolism/ membrane biology and host defense againstplant „secondary synthesis products“ such as alkaloids
Centre for Pharmacology and Toxicology
Humans have 57 CYP genes and ~ 59 pseudogenes.CYP genes are divided among 18 families & 43 subfamilies.Mice have ~ 100 CYP genes

Examples of CYP monoxygenase functions
P450 family FunctionCYP1-CYP3 xenobiotic/steroid metabolismCYP4 fatty acid hydroxylation, foreign compound metabolismCYP5 thromboxane synthesisCYP7 cholesterol 7-hydroxylaseCYP11 cholesterol side chain cleavage
steroid 11 hydroxylaseCYP17 steroid 17 hydroxylaseCYP19 steroid aromataseCYP21 steroid 21-hydroxylaseCYP24 vitamin D metabolismCYP27 cholesterol 27-hydroxylase
Centre for Pharmacology and Toxicology

Centre for Pharmacology and Toxicology
OOH
N
O NO
N
N
O
NS
O ON
O
O
N
O
PROPANOLOL
BUFURALOL
TIMOLOL
METOPROLOL
O
O
ON
N N
NN
N
HH
HH
N
O
NO
O
ONH
N H 2
N H
NH
N
O
NO
H
N
O H
NO H
H
P R O P A F E N O N
D E B R IS O Q U IN E
E N C A IN ID E
G U A N O X A N
S P A R T E IN E
P E R H E X IL IN E
N -P R O P Y L A JM A L IN E
ß-adrenergic blocking agents and antiarrhythmics are substrates for polymorphic CYP monooxygenase genes

Centre for Pharmacology and Toxicology
Reaction cycle of cytochrome P450
HP-Fe3+
HP-Fe3+
RH
RH
HP-Fe2+
RH
1e-
HP-Fe2+ -O2
RHHP-Fe3+ -O2
-
RH
HP-Fe3+ -O22-
RH
HP-Fe3+
RH
O21e-
O
H2O
2H+
ROH
Flavoprotein2e-
NADPH+H+ NADP++2H+

Centre for Pharmacology and Toxicology
Most drug metabolising enzymes exhibit clinically relevant genetic polymorphism
CYP1A1/2CYP1B1
CYP2A6CYP2B6
CYP2C8
CYP2C9CYP2C19
CYP2D6
CYP2E1
CYP3A4/5/7
ALDH
ADH
DPD
NQO1
esterases
epoxidehydrolase
others NAT1NAT2
GST-M
GST-T
GST-P
GST-A
STs
HMT
COMT
TPMT
UGTs
others
Phase 1 Phase 2

Centre for Pharmacology and Toxicology
Discovery of the first genetic polymorphism of human cytochrome P450 (CYP2D6)
Melatonin (MT), N-acetyl-5-methoxytryptamine, is a major hormone of the pineal gland, is a multitasking molecule and exerts anti-excitatory and sedating effects. MT is an anticonvulsant and functions through two MT-receptor (GPCR).
13α helices5ß-sheets
Ma et al. 2005;DMD 33(4):489-94.
(A) Melatonin 6-hydroxylation (A) and (B) O-demethylation.

Examples of variant CYP2D6 alleles but NOT all of them affect activity
Allele1Trivialname
Nucleotide differencesfrom wild-type CYP2D6
Enzymeactivity
CYP2D6*1 Wild-type none normalCYP2D6*2A CYP2D6L1 G1749C; C2938T; G4268C normal
CYP2D6N G4268C normalCYP2D6L2 G1749C; C2938T; G4268C increased
CYP2D6L2 x 2 G1749C; C2938T; G4268C increasedCYP2D6L2 x 12 G1749C; C2938T; G4268C increased
CYP2D6*3 CYP2D6A A2367 deletion inactiveCYP2D6*4 CYP2D6B C188T; C1062A; A1072G;C1085G;
G1749C; G1934A; G4268Cinactive
CYP2D6*5 CYP2D6D CYP2D6 deleted inactiveCYP2D6*6 CYP2D6T T1795 deleted; G2064A inactive
Centre for Pharmacology and Toxicology

Centre for Pharmacology and Toxicology
There are about 100 known SNPs within the CYP2D6 gene. However, only four of them, i.e. CYP2D6*3, *4, *5
and *6 account for 93% to 97% of PMs
(Source:http://www.genome.utah.edu/genesnps/genes/CYP2D6/)
flanking, 620,G/A
flanking, 660,G/C
flanking, 780,A/T
flanking, 801,C/G
flanking, 880,C/T
flanking, 883,A/G
flanking, 942,G/A
flanking, 1032,G/A
flanking, 1255,G/A
flanking, 1444,G/A
nonsyn, 1650,G/A
nonsyn, 1696,G/A
nonsyn, 1719,T/C
nonsyn, 1719,C/T
intronic, 1833,G/C
intronic, 1840,C/A
intronic, 1842,C/G
intronic, 1846,T/C
intronic, 1851,GA/CC
intronic, 1864,A/G
nonsyn, 4194,C/A
nonsyn 4469,T/C
nonsyn, 4482,C/G
nonsyn 4484,G/A
nonsyn, 4515,C/T
nonsyn, 4884,G/A
nonsyn, 4910,A/G
intronic, 5003,A/C
intronic, 5201,A/G
nonsyn, 5472,G/A
3'UTR, 5862,C/T
flanking, 7895,G/A
intronic, 1889,C/T
intronic, 1929,G/T
intronic 2348,C/A
intronic 2365,C/G
intronic, 2462,T/G
synon, 2658,C/T
intronic, 2789,G/A
nonsyn, 3280,C/G
nonsyn, 4085,T/C
synon, 4089,T/C

Centre for Pharmacology and Toxicology
CYP2D6 metabolizes about 20–25% of clinically used drugs; the enzyme also catalyzes oxidation of hydroxytryptamines
4378 bp
CYP2D6
i1 i2 i3 i4 i5 i6 i7 i8
i3 intron 4
1846 1934 2005 27052528Exon 4 Exon 5
Ex1 Ex2 Ex3 Ex4 Ex5 Ex6 Ex7 Ex8 Ex9
1934 : G to A substitution*4 Allel
2637 : A deletion*3 Allel
Allan Gough et al., Nature 347, 773 – 776; Kagimoto M et al., J Biol Chem. 1990 Oct 5;265(28):17209-14

The case of tramadol and the challenge: Analysis of the most common SNPs within 60 minutes of blood with-drawl.
Genotyping in clinical trials
wildtype
hetero-zygote
homo-zygote
CYP2D6*3
CYP2D6*4 wildtype
heterozygote
homo-zygote
Centre for Pharmacology and Toxicology

Pharmacokinetics of tramadol and M1
Centre for Pharmacology and Toxicology
Results Standard deviations
Phenotype PM EM PM EM
Cmax(tramadol) [ng/ml] 303,75 340,23 90,76 48,40
Cmax(M1) [ng/ml] 34,43 87,00 23,24 20,03
AUC(tramadol) [ng/ml*h] 3482,57 2283,54 1534,79 572,19
AUC(M1) [ng/ml*h] 431,00 829,62 215,72 166,43

Tramadol
CYP2D6
M1
-opioidreceptor
NMDA, 5HT, nAChR, mAChRs, SRI, NRI...
CYP2D6
CYP2D6
CYP2D6
Tramadol receptors
Centre for Pharmacology and Toxicology
The metabolite (+)-M1 showsthe highest affinity (Ki=3.4 nM)to the human mu-opioid receptor

Qiang Ma, and Anthony Y. H. Lu Pharmacol Rev 2011;63:437-459
(S)-warfarin blocks Vitamin K epoxide Reductase Complex VKORC1 activity resulting in the depletion of reduced vitamin K.This results in decreased γ-carboxylation of coagulation factors II, VII, IX, and X by gamma-glutamylcarboxylase GGCX and prolonged blood coagulation. CYP2C9 catalyzes the 7-hydroxylation of (S)-warfarin to inactivate the drug, whereas, calumenin modulates GGCX function to affect blood clotting. Variant CYP2C9 and VKORC1 genotypes require dose adjustment
Centre for Pharmacologyand Toxicology

Thiopurine methyltransferase (TPMT) and Dehydro-pyrimidine dehydrogenase (DPD) polymorphism –- implications for drug therapy -
Typical substrates for TPMT and DPD are mercaptopurine, ACE inhibitors such as captopril, D-penicilamine given to Morbus Wilson and arthritis patients, antidiuretic spironolactone, 5-flurouracil…
Centre for Pharmacology and Toxicology
TPMT9ß-sheets6 α-helices
DPDHomodimer of2 x 111kDa prot.

Centre for Pharmacology and Toxicology
Thiopurine methyltransferase
N NH
NN
SH
N NH
NN
SCH3
Ado-Met Ado-Hcy
6-Methylmercaptopurine
45 112 184 93 133 53 75 86 45 2075TPMT*1(wild type)
ATG
TPMT*2( activity)
ATG G238CAla Pro
TPMT*3(no activity)
ATG G460CAla Pro
A719GTyr Cys

• TPMT*3 is of great importance in cancer therapy. Drugs such as mercaptopurine, azathiopurine and thioguanine are prodrugs and must be converted to thiopurine nucleotides.
• TPMT competes with HPRT (hypoxanthine phosphoribosyl transferase) and inactivates drugs by S-methylation.
• TPMT deficient patients require dose adjustment because they experience severe toxicity to drug treatment due to increased levels of thioguanine nucleotides (TGN).
Thiopurine methyltransferase
Centre for Pharmacology and Toxicology
N
NH2
O NH
NH
O NH
O
NH
O NH
O
N
NH2
O N
F
NH3H2O
NADPH + H
NADP+
H2O
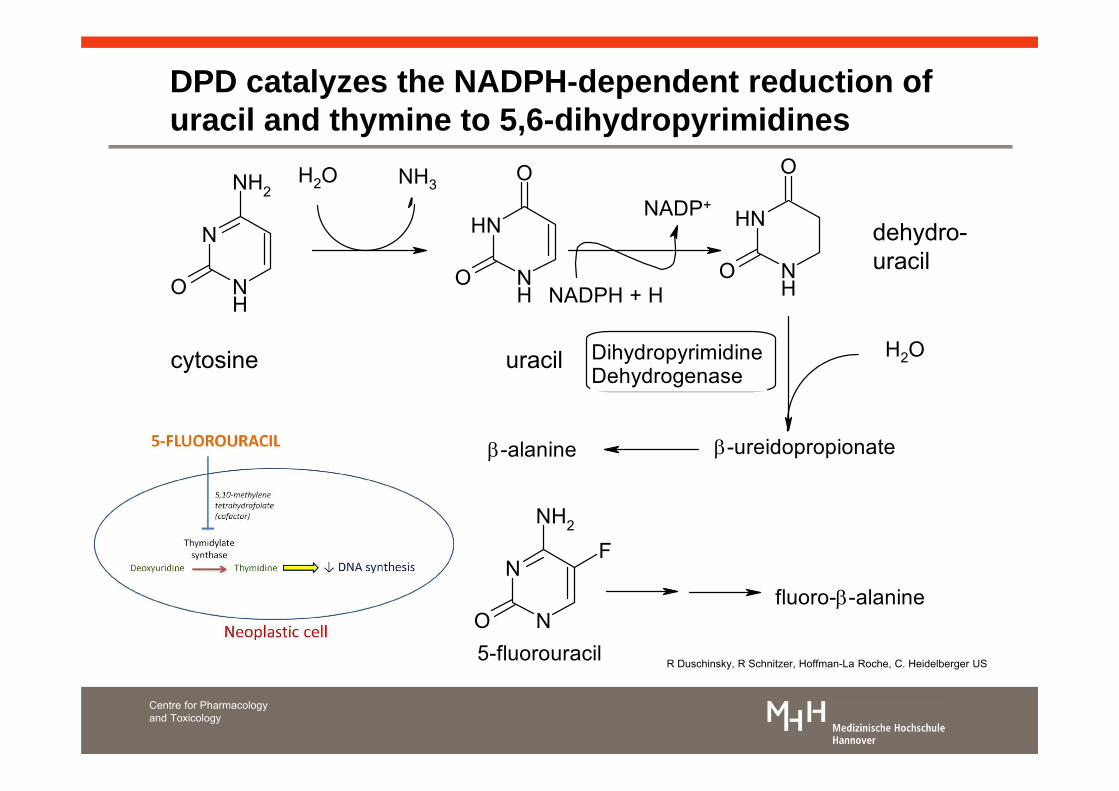
-ureidopropionate-alanine
DihydropyrimidineDehydrogenase
fluoro--alanine
5-fluorouracil
DPD catalyzes the NADPH-dependent reduction of uracil and thymine to 5,6-dihydropyrimidines
cytosine uracil
dehydro-uracil
Centre for Pharmacology and Toxicology
R Duschinsky, R Schnitzer, Hoffman-La Roche, C. Heidelberger US

Expression of DPD activity in human leucocytes
subjects
Patient number 8 is a cancer patient that experienced high toxicity when administered 5-FU.
Centre for Pharmacology and Toxicology
Centre for Pharmacology and Toxicology
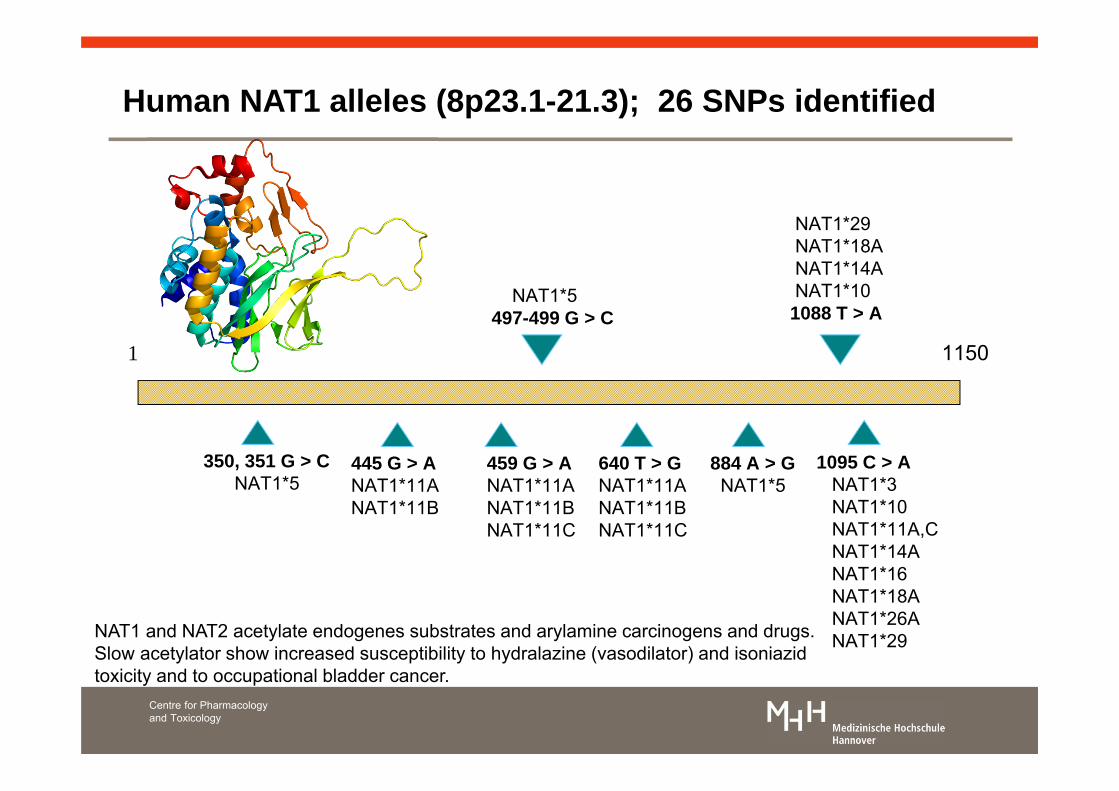
Human NAT1 alleles (8p23.1-21.3); 26 SNPs identified
1 1150
1095 C > ANAT1*3NAT1*10NAT1*11A,CNAT1*14ANAT1*16NAT1*18ANAT1*26ANAT1*29
350, 351 G > CNAT1*5
NAT1*5497-499 G > C
884 A > GNAT1*5
NAT1*29NAT1*18ANAT1*14ANAT1*10
1088 T > A
445 G > ANAT1*11ANAT1*11B
459 G > ANAT1*11ANAT1*11BNAT1*11C
640 T > GNAT1*11ANAT1*11BNAT1*11C
NAT1 and NAT2 acetylate endogenes substrates and arylamine carcinogens and drugs.Slow acetylator show increased susceptibility to hydralazine (vasodilator) and isoniazidtoxicity and to occupational bladder cancer.

Centre for Pharmacology and Toxicology
Schematic representation of the NAT2 RFLP multiplex PCR
KapI digest DdeI digest
BamHI digest TaqI digest
A
547
433
114
B
345
137
114
65
C
547490
57
D
392
222170155
Kk kk KK Dd dd DD
Bb bb BB Tt tt TT
Constant
Constant
Constant
Centre for Pharmacology and Toxicology
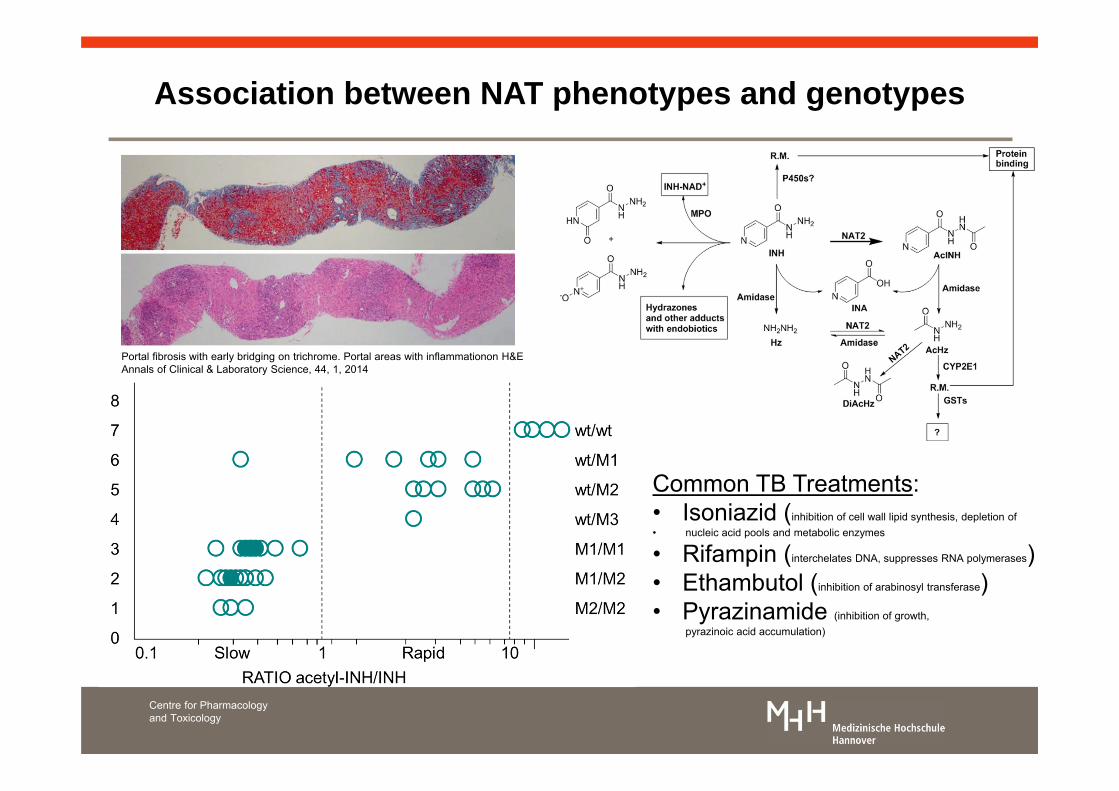
Association between NAT phenotypes and genotypes
Common TB Treatments:• Isoniazid (inhibition of cell wall lipid synthesis, depletion of• nucleic acid pools and metabolic enzymes
• Rifampin (interchelates DNA, suppresses RNA polymerases)• Ethambutol (inhibition of arabinosyl transferase)• Pyrazinamide (inhibition of growth,
pyrazinoic acid accumulation)
Portal fibrosis with early bridging on trichrome. Portal areas with inflammationon H&EAnnals of Clinical & Laboratory Science, 44, 1, 2014

Centre for Pharmacology and Toxicology
• Significant differences in the allelic frequencies of the pNAT and CYP2D6 genes among epileptic patients (role of melatonin…)
• Actylation of melatonin is extremely important and protects 5HT against MAO degradation and thus permanent loss of function
• Melatonin increases in epileptic seizures• There was a significant increase of PMs
amongst epileptic patients (2=4.01, p<0.05), i.e. 9.1 vs 4.3%
• There was a significant increase of slow acetylators among epileptic patients and many anticonvulsive drugs require N-acetylation for metabolic clearance
Critical Care Clinics 1997;13[4]:763-83

Centre for Pharmacology and Toxicology
Clinically relevant human UGT gene polymorphism
Human UGT Gene Family
UGT1*2P
UGT1*3
UGT1*5
UGT1*4
UGT1*1
UGT1*6
UGT1*02
UGT2B11
UGT2B4
UGT2B9
UGT2B7
UGT2B15
UGT2B10
UGT2B8
HugBr2 / HP2
HugBr1 / HP2
HP1
HP4
Hlug25 / UDPGTh-1
Hlug6
UDPGTh-2
Hlug7
Hlug4 / UDPGTh-3
human olfactory UGT
UGT1
UGT2
UGT2B
Percentage protein similarity 100%30%

Exon 1 2 3 4 5
A C
(TA)6 TAA
39 53
D B98-100 bp
253-255 bp
3’5’
Centre for Pharmacology and Toxicology
Structure of UGT1*1 gene highlighting promotor region
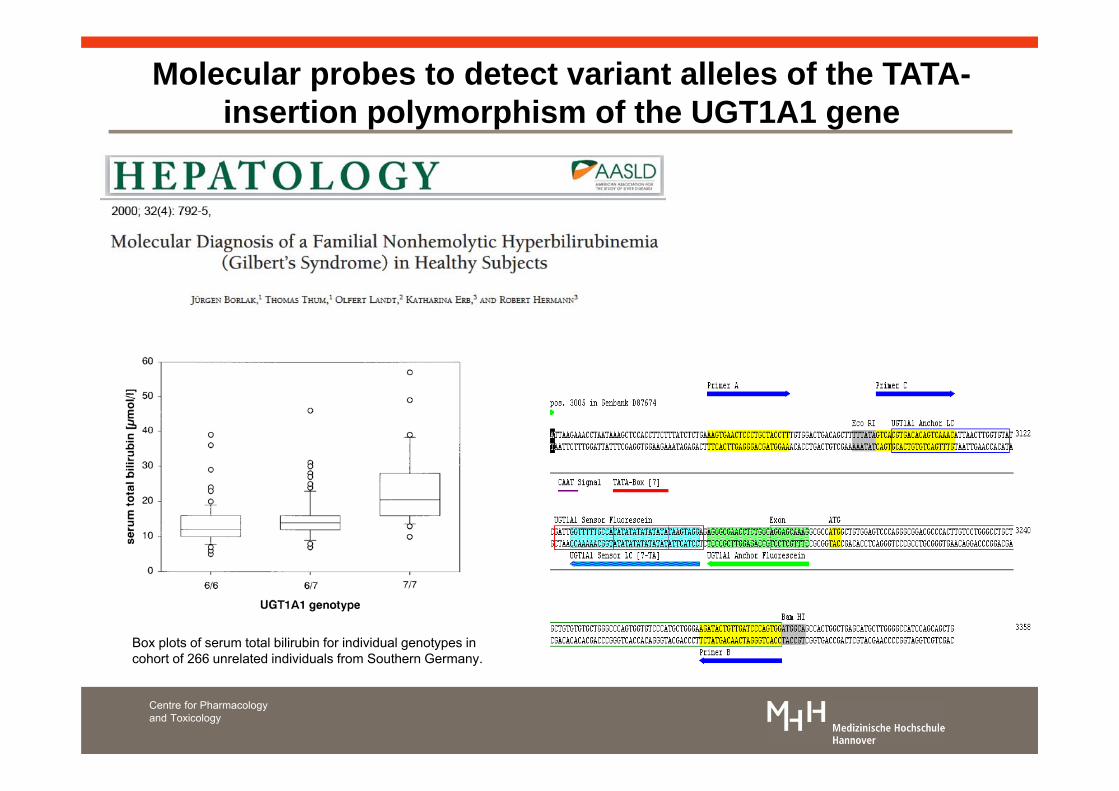
Molecular probes to detect variant alleles of the TATA-insertion polymorphism of the UGT1A1 gene
http://onlinelibrary.wiley.com/doi/10.1053/jhep.2000.18193/abstrac
Centre for Pharmacology and Toxicology
Box plots of serum total bilirubin for individual genotypes incohort of 266 unrelated individuals from Southern Germany.

Centre for Pharmacology and Toxicology
Molecular diagnosis of a familial nonhaemolytic hyperbilirubinemia
clonedcontrols
individual genotypes
negative control (water)wild type (homozygote)mutation (heterozygote)mutation (homozygote)
(TA)6TAA (TA)7TAA
(TA)6TAA (TA)7TAA
SF2

Folie 32
SF2 Histologic image from the liver biopsy of a 54-year-old patient with drug-related hepatitis and Gilbert’s syndrome. (A) Presence of a significant granulocyte population in the portal tracts with a lymphocytic spill-over and morphology alterations to small and medium bile canaliculi (hematoxylin and eosin stain, original magnification ×10). (B) Hepatocellular intracytoplasmatic edema with few microthrombi inside canalicular bile ducts (hematoxylin and eosin stain, original magnification ×10)Schoppmeier, Frauke; 15.03.2017
Centre for Pharmacology and Toxicology
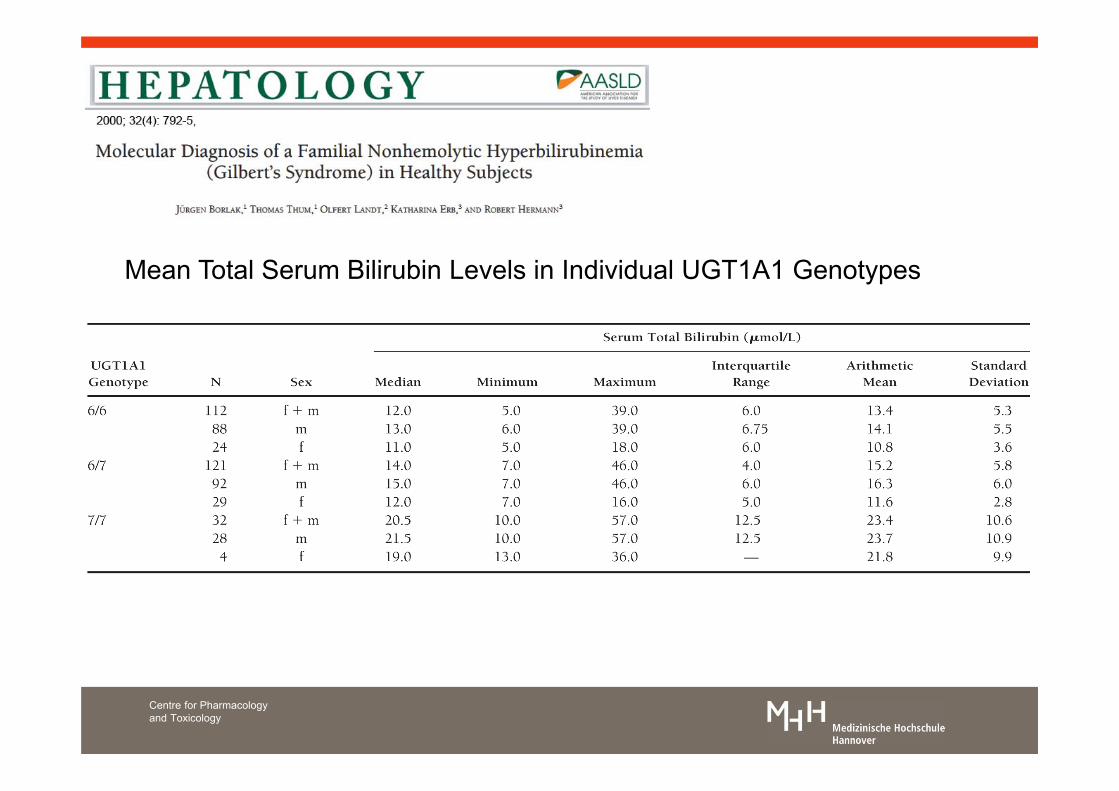
Mean Total Serum Bilirubin Levels in Individual UGT1A1 Genotypes

Metabolism of irinotecan to APC
Centre for Pharmacology and Toxicology

Centre for Pharmacologyand Toxicology
Pharmacokinetic parameter estimates of AWD21-360 after multiple oral doses of 200mg retigabine b.i.d.

Polymorphisms in other phase II enzymes(GSTs, COMT, esterases, aldehyd (ALDH) /
alcohol (ADH) dehydrogenases andsulfotransferases)
Centre for Pharmacology and Toxicology
SAM, 3,5-Dinitrocatechol

Centre for Pharmacology and Toxicology
GSTs are of vital importance in maintaining cellular defenceagainst ROS. SNPs contribute to risk for carcinogenesis andindividual variation in drug response
position, allele
9363, A/G9425, A/T9616, C/T9685, C/T9920, A/G
implication
intronic, intron 7nonsyn, exon 83‘UTR3‘UTRflanking
function
unknownunknownunknownunknownunknown
submitter population ID: NIHPDRCollins et al (1998), Genome Research 8:1229-1231160 to 190 probes analysed
Source: http://www.genome.utah.edu/genesnps/genes/GSTM1
implication
exon 7whole gene
position, allele
534 G/Cnull allele
function
unchangedno activity
Brockmoller et al (1993), Cancer Research 53:1004-1011272 probes analysed
nomenclature
GSTM1*AGSTM1*BGSTM1*0
Human cytosolic GSTs involve alpha, zeta, theta, mu, pi, sigma, and omega classes

• Catechol-O-methyl-transferase playsan essential role in the metabolism ofneurotransmitter such as dopamine, epinephrine, norepinephrine, catecholestrogens, and drugs
• Polymorphism may be related to neuropsychiatricconditions involving catecholamine neurotransmission.
• COMT*2 encodes for a missense val 158 Met thatcauses lower activity and protein instability. The allelicfrequecies is about 0.46.
COMT polymorphisms
Centre for Pharmacology and Toxicology

Centre for Pharmacology and Toxicology
AIMS: A 23-year-old Caucasian woman, with cystic fibrosis, bilateral lung-transplantation and immunosuppressive therapy with prednisolone, tacrolimus and sirolimus, presented with clinical symptoms of a chronic transplant rejection.METHODS: Since constant sufficient blood level of tacrolimus and sirolimus had never been achieved, a genetic analysis was carried out to clarify drug metabolism.RESULTS: The genetic analysis for polymorphisms of cytochrome P450 (CYP) 3A4,5,7 revealed no sequence alterations in the CYP 3A4,5,7 gene. Thus, drug intake was scrutinized in detail, disclosing a missing interval between the intake of both immunosuppressiveagents. After a correct drug intake the woman's condition ameliorated and the blood levels reached normal range.CONCLUSIONS: This case report highlights the crucial importance of basic medical skills like an accurate and dainty drug anamnesis before high tech approaches were applied.

.
Centre for Pharmacology andToxicology
Fig. 1 - Current mechanistic understanding in the initiation and progression events relevant to idiosyncratic drug-induced liver injury.

Lazarou et al., 1998 estimate 6.7% ADR‘s [95%CI, 5.2 - 8.2%] for the US alone with 0.32% [95% CI, 0.23 – 0. 41%] fatal outcome ( > 100.000,00 patient die of ADRs, i.e. third leading cause of death!)
Centre for Pharmacology and Toxicology

Centre for Pharmacology and Toxicology
• HLA-B*5701 allele was associated with an 80-fold increased risk of developing DILI (Dale et al., 2009 Nature Genetics; DILIGEN & Serious Adverse Event consortium)
• This HLA allele is also associated with abacavir-hypersensitivity in HIV patients. • The HLA-B*5701 in the general population (6 to 8%) and the low incidence of DILI in
treated patients (1 in 10,000) leads to a low positive predictive value (0.12%).• Testing for HLA-B*5701 may help diagnose flucloxacillin cholestasis in patients that
develop jaundice but use of the drug should not be withheld in HLA-B*5701 positive individuals.
Fontana Gastroenterology. 2014 April ; 146(4): 914–928.
Genetic studies of Flucloxacillin hepatotoxicity

Centre for Pharmacology and Toxicology
Genetic studies in pooled idiosyncratic DILI patients
• DILI susceptibility may be shared across multiple drugs but a GWA study in 783 Caucasian individuals who experienced DILI from over 200 different drugs did not reveal significant associations.
• Stratification of cases according to injury pattern, latency, severity, drug class and clinical phenotypes/medical history did not reveal any association
• Susceptibility to Amoxicillin-Clavulanate-induced liver injury is influenced by multiple HLA class I and II alleles
• Pharmacogenetic polymorphisms influence the metabolism and therefore PK of drugs.
• This can impact safety, particularly with drugs of narrow therapeutic index.
• Pharmacogenetics permits “personalized” dose selection to ensure safety and therapeutic efficacy.
• The pharmacogenetics of drug targets (receptors, ion channels etc.) will be key for defining “drug responders” and a sine qua non for precision medicine
• Pharmacogentics and translational genomics will bea major breakthrough in precision medicine
Summary
Centre for Pharmacology and Toxicology


















![This leaflet format has been determined by the Ministry of ... · of CYP2D6 metabolism [see Clinical Pharmacology 12.3]. The potential for a pharmacokinetic interaction exists with](https://static.fdocuments.in/doc/165x107/5d52c28088c993383f8b74ff/this-leaflet-format-has-been-determined-by-the-ministry-of-of-cyp2d6-metabolism.jpg)