Pharmacoepidemiological study protocol ER11-9411
27
Pharmacoepidemiological study protocol ER-9542 EPID Research CONFIDENTIAL Pharmacoepidemiological study protocol ER-9542 An Observational Cohort Study on Multiple Myeloma Patients in Finland Authors: Jenna Anderson, Juha Mehtälä, Ilona Iso-Mustajärvi, Saara Hetemäki, Alisa Kopilow, Carina von Schantz-Fant, Saku Torvinen, Tatu Miettinen, Juha Lievonen, Pasi Korhonen Protocol ID: ER-9542 Sponsor: Takeda Finland Protocol version: 2.0 Protocol date: 13 June 2019 Pharmacoepidemiological study protocol ER-9542 as??? so u'a' "G _ U esearch ' an IQVIA company Pharmacoepidemiological study protocol ER-9542 An Observational Cohort Study on Multiple Myeloma Authors: Protocol ID: Sponsor: Protocol version: Protocol date: EPID Research Patients in Finland Jenna Anderson, Juha Meht'ala, Ilona Iso-Mustaj‘cirvi, Saara Hetemaki, Alisa Kopilow, Carina von Schantz-Fant, Saku Torvinen, Tatu Miettinen, Juha Lievonen, Pasi Korhonen ER-9542 Takeda Finland 2.0 13 June 2019 CONFIDENTIAL
Transcript of Pharmacoepidemiological study protocol ER11-9411

Pharmacoepidemiological study protocol ER-9542
EPID Research CONFIDENTIAL
Pharmacoepidemiological study protocol ER-9542
An Observational Cohort Study on Multiple Myeloma Patients in Finland
Authors: Jenna Anderson, Juha Mehtälä, Ilona Iso-Mustajärvi, Saara Hetemäki, Alisa Kopilow, Carina von Schantz-Fant, Saku Torvinen, Tatu Miettinen, Juha Lievonen, Pasi Korhonen
Protocol ID: ER-9542
Sponsor: Takeda Finland
Protocol version: 2.0
Protocol date: 13 June 2019
Pharmacoepidemiological study protocol ER-9542
as??
?
so u'a' "G _ U
esearch' an IQVIA company
Pharmacoepidemiological study protocolER-9542
An Observational Cohort Study on Multiple Myeloma
Authors:
Protocol ID:
Sponsor:
Protocol version:
Protocol date:
EPID Research
Patients in Finland
Jenna Anderson, Juha Meht'ala, Ilona Iso-Mustaj‘cirvi, Saara Hetemaki, AlisaKopilow, Carina von Schantz-Fant, Saku Torvinen, Tatu Miettinen, JuhaLievonen, Pasi Korhonen
ER-9542
Takeda Finland
2.0
13 June 2019
CONFIDENTIAL

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 2 of 27
Study Information
Title An Observational Cohort Study on Multiple Myeloma Patients in Finland
Protocol ID ER-9542
Protocol version 2.0
Protocol date 13 June 2019
EU PAS register number
EUPAS19582
Sponsor Takeda Finland
Sponsor contact person Tatu Miettinen
Active substance NA
Medicinal product NA
Country(-ies) of study Finland
Authors of the protocol Jenna Anderson, Juha Mehtälä, Ilona Iso-Mustajärvi, Saara Hetemäki, Alisa Kopilow, Carina von Schantz-Fant, Saku Torvinen, Tatu Miettinen, Juha Lievonen, Pasi Korhonen
Main author of the protocol
Jenna Anderson
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
Study Information
Title An Observational Cohort Study on Multiple Myeloma Patients in Finland
Protocol ID ER-9542
Protocol version 2.0
Protocol date 13 June 2019
EU PAS register EUPAS19582number
Sponsor Takeda Finland
Sponsor contact person Tatu Miettinen
Active substance NA
Medicinal product NA
Country(—ies) of study Finland
Authors ofthe protocol Jenna Anderson, Juha Mehtala, ||ona lso-Mustajarvi, Saara Hetem'aki, AlisaKopilow, Carina von Schantz-Fant, Saku Torvinen, Tatu Miettinen, JuhaLievonen, Pasi Korhonen
Main author of the Jenna Andersonprotocol
EPID Research Page 2 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 3 of 27
Table of contents
1 Abstract .................................................................................................................................... 4
2 List of abbreviations ................................................................................................................. 5
3 Approvals ................................................................................................................................. 7
4 Amendments and updates ....................................................................................................... 9
5 Milestones ................................................................................................................................ 9
6 Rationale and background ..................................................................................................... 11
7 Research questions and objectives ........................................................................................ 12
7.1 Primary objectives .................................................................................................................. 12
7.2 Secondary objectives ............................................................................................................. 12
8 Research methods .................................................................................................................. 13
8.1 Study design ........................................................................................................................... 13
8.2 Population and setting ........................................................................................................... 13
8.3 Variables ................................................................................................................................. 15
8.4 Other definitions .................................................................................................................... 18
8.5 Data sources ........................................................................................................................... 18
8.6 Study size ............................................................................................................................... 18
8.7 Data management.................................................................................................................. 19
8.8 Data analysis .......................................................................................................................... 19
8.9 Quality control ....................................................................................................................... 21
8.10 Limitations of the research methods ..................................................................................... 21
9 Informed consent ................................................................................................................... 22
10 Protection of human subjects ................................................................................................ 22
11 Management and reporting of adverse events/adverse reactions ....................................... 23
12 Plans for disseminating and communicating study results .................................................... 23
13 References.............................................................................................................................. 24
Annex 1. List of stand alone documents ............................................................................................... 25
Annex 2. ISS and R-ISS ........................................................................................................................... 25
Annex 3. Finnish national guidelines for MM treatment ...................................................................... 26
Annex 4. Definitions of patient populations ......................................................................................... 26
Annex 5. Definitions of disease status ................................................................................................... 27
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 lune 2019
Table of contents
1 Abstract .................................................................................................................................... 4
2 List of abbreviations ................................................................................................................. 5
3 Approvals ................................................................................................................................. 7
4 Amendments and updates ....................................................................................................... 9
5 Milestones ................................................................................................................................ 9
6 Rationale and background ..................................................................................................... 11
7 Research questions and objectives ........................................................................................ 12
7.1 Primary objectives .................................................................................................................. 12
7.2 Secondary objectives ............................................................................................................. 12
8 Research methods .................................................................................................................. 13
8.1 Study design ........................................................................................................................... 13
8.2 Population and setting ........................................................................................................... 13
8.3 Variables ................................................................................................................................. 15
8.4 Other definitions .................................................................................................................... 18
8.5 Data sources ........................................................................................................................... 18
8.6 Study size ............................................................................................................................... 18
8.7 Data management.................................................................................................................. 19
8.8 Data analysis .......................................................................................................................... 19
8.9 Quality control ....................................................................................................................... 21
8.10 Limitations of the research methods ..................................................................................... 21
9 Informed consent ................................................................................................................... 22
10 Protection of human subjects ................................................................................................ 22
11 Management and reporting of adverse events/adverse reactions ....................................... 23
12 Plans for disseminating and communicating study results .................................................... 23
13 References.............................................................................................................................. 24
Annex 1. List of stand alone documents ............................................................................................... 25
Annex 2. ISS and R-ISS ........................................................................................................................... 25
Annex 3. Finnish national guidelines for MM treatment ...................................................................... 26
Annex 4. Definitions of patient populations ......................................................................................... 26
Annex 5. Definitions of disease status ................................................................................................... 27
EPID Research Page 3 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 4 of 27
1 Abstract
Rationale and background: Multiple myeloma (MM) is a progressive clonal haematologic malignancy of plasma cells. In Finland, there are approximately 350-400 new MM cases diagnosed each year, primarily amongst the elderly. The average survival time following diagnosis is 5-6 years, but prognosis varies greatly and the recent introduction of novel therapies has improved overall survival. However, the treatment and subsequent outcomes of MM in Finland are not completely understood.
Research question and objectives: The primary objective of this study is to describe the Finnish MM patient population, treatment patterns, and treatment outcomes with different types and stages of the disease, and to stratify by known patient-related prognostic factors. The secondary objective is to identify and describe characteristics of specific subpopulations, including those who received a specific treatment selection, who have short treatment durations, as well as risk-stratified subpopulations. Where possible, the effect of transplant, duplet/triplet therapies, treatment duration, and risk-stratification on overall survival (OS) and time to next treatment (TTNT) outcomes will also be determined.
Study design: Descriptive retrospective study using nationwide data from the Finnish Hematology Register (FHR). The study will collect retrospective data including but not limited to information such as age, gender, co-morbidities, date of MM diagnosis, clinical status of MM, and received treatment.
Population and setting: The whole study cohort will include patients diagnosed for MM during the FHR data availability period 01 January 2010 – 31 December 2015 aged 18 years or older at the time of diagnosis. The actual study cohort will include patients diagnosed with MM during the period 01 January 2010 – 31 December 2015 and treated for MM during the period 01 January 2010 – 31 December 2016, who have at least one year of potential follow-up time following start of treatment (to 31 December 2017). Characteristics of all MM patients recorded in the FHR will be described on an overall level.
Data sources: The whole cohort will be identified from the FHR. Patient data will be collected from the FHR retrospectively starting from diagnosis.
Study size: Baseline data will be collected from all new MM patients for descriptive analyses. The study size for the actual cohort will be at least 300-400 Finnish MM patients. There are approximately 1600 MM patients all together recorded at FHR.
Data analysis: Descriptive statistics of subject baseline characteristics, diagnosis, gender, age, treatment selection, and laboratory values will be provided. Continuous variables will be described by mean, standard deviation, median, 25th and 75th percentiles, minimum and maximum. Categorical variables and continuous variables that are also categorized will be described by proportion and frequency in each category. 95% confidence intervals (CI) will be presented when appropriate. Time to event analyses will be estimated using Kaplan-Meier curves and multivariate Cox proportional hazard models where appropriate.
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 june 2019
1 Abstract
Rationale and background: Multiple myeloma (MM) is a progressive clonal haematologic malignancy ofplasma cells. In Finland, there are approximately 350-400 new MM cases diagnosed each year, primarilyamongst the elderly. The average survival time following diagnosis is 5-6 years, but prognosis varies greatlyand the recent introduction of novel therapies has improved overall survival. However, the treatment andsubsequent outcomes of MM in Finland are not completely understood.
Research question and objectives: The primary objective of this study is to describe the Finnish MM patientpopulation, treatment patterns, and treatment outcomes with different types and stages of the disease, andto stratify by known patient-related prognostic factors. The secondary objective is to identify and describecharacteristics of specific subpopulations, including those who received a specific treatment selection, whohave short treatment durations, as well as risk-stratified subpopulations. Where possible, the effect oftransplant, duplet/triplet therapies, treatment duration, and risk-stratification on overall survival (OS) andtime to next treatment (TTNT) outcomes will also be determined.
Study design: Descriptive retrospective study using nationwide data from the Finnish Hematology Register(FHR). The study will collect retrospective data including but not limited to information such as age, gender,co-morbidities, date of MM diagnosis, clinical status of MM, and received treatment.
Population and setting: The whole study cohort will include patients diagnosed for MM during the FHR dataavailability period 01 January 2010 — 31 December 2015 aged 18 years or older at the time of diagnosis. Theactual study cohort will include patients diagnosed with MM during the period 01 January 2010 — 31December 2015 and treated for MM during the period 01 January 2010 — 31 December 2016, who have atleast one year of potential follow-up time following start oftreatment (to 31 December 2017). Characteristicsof all MM patients recorded in the FHR will be described on an overall level.
Data sources: The whole cohort will be identified from the FHR. Patient data will be collected from the FHRretrospectively starting from diagnosis.
Study size: Baseline data will be collected from all new MM patients for descriptive analyses. The study sizefor the actual cohort will be at least 300-400 Finnish MM patients. There are approximately 1600 MMpatients all together recorded at FHR.
Data analysis: Descriptive statistics of subject baseline characteristics, diagnosis, gender, age, treatmentselection, and laboratory values will be provided. Continuous variables will be described by mean, standarddeviation, median, 25th and 75th percentiles, minimum and maximum. Categorical variables and continuousvariables that are also categorized will be described by proportion and frequency in each category. 95%confidence intervals (Cl) will be presented when appropriate. Time to event analyses will be estimated usingKaplan-Meier curves and multivariate Cox proportional hazard models where appropriate.
EPID Research Page 4 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 5 of 27
2 List of abbreviations
ANC Absolute neutrophil count
ASCT Autologous stem cell transplant
BUN Blood urea nitrogen
CA Chromosomal abnormality
CKD-EPI Chronic Kidney Disease Epidemiology Collaboration
CI Confidence interval
CP Cyclophosphamide + prednisone treatment
CR Complete response
CRAB C = calcium (elevated), R = renal failure, A = anaemia, B = bone lesions
Dg Diagnosis
DSS Durie-Salmon clinical staging system
eGFR Estimated glomerular filtration rate
EMA European Medicines Agency
ENCePP European Network of Centres for Pharmacoepidemiology and Pharmacovigilance
EU European Union
EU PAS European register of non-interventional post-authorisation studies
FHR Finnish Hematology Register
FSH Finnish Society of Hematology
FIMM The Institute of Molecular Medicine Finland
FISH Fluorescence in situ hybridization
FRCBS Finnish Red Cross Blood Service
GPP Good Pharmacoepidemiology Practice
IC Informed consent
ICMJE International Committee of Medical Journal Editors
iFISH Interphase fluorescence in situ hybridization
IMWG International Myeloma Working Group
ISPE International Society for Pharmaceutical Engineering
ISS International staging system
LDH Lactate dehydrogenase
LenDex Lenalomide + dexamethasone treatment
MGUS Monoclonal gammopathy of unknown significance
MM Multiple myeloma
MP Melphalan + prednisone treatment
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
2 List of abbreviations
ANC Absolute neutrophil count
ASCT Autologous stem cell transplant
BUN Blood urea nitrogen
CA Chromosomal abnormality
CKD-EPI Chronic Kidney Disease Epidemiology Collaboration
CI Confidence interval
CP Cyclophosphamide + prednisone treatment
CR Complete response
CRAB C = calcium (elevated), R = renal failure, A = anaemia, B = bone lesions
Dg Diagnosis
DSS Durie-Salmon clinical staging system
eGFR Estimated glomerular filtration rate
EMA European Medicines Agency
ENCePP European Network of Centres for Pharmacoepidemiology and Pharmacovigilance
EU European Union
EU PAS European register of non-interventional post-authorisation studies
FHR Finnish Hematology Register
FSH Finnish Society of Hematology
FIMM The Institute of Molecular Medicine Finland
FISH Fluorescence in situ hybridization
FRCBS Finnish Red Cross Blood Service
GPP Good Pharmacoepidemiology Practice
IC Informed consent
ICMJE International Committee of Medical Journal Editors
iFISH Interphase fluorescence in situ hybridization
IMWG International Myeloma Working Group
ISPE International Society for Pharmaceutical Engineering
ISS International staging system
LDH Lactate dehydrogenase
LenDex Lenalomide + dexamethasone treatment
MGUS Monoclonal gammopathy of unknown significance
MM Multiple myeloma
MP Melphalan + prednisone treatment
EPID Research Page 5 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 6 of 27
MR Minimal response
MRD Minimal residual disease
MRI Magnetic resonance imaging
NDMM Newly diagnosed multiple myeloma
ORR Overall response rate
OS Overall survival
PAS Post-authorization study
PD Progressive disease
PFS Progression-free survival
PR Partial response
RCT Randomized-controlled trial
RD Lenalomide + dexamethasone treatment
R-ISS Revised international staging system
RRMM Relapsed/refractory multiple myeloma
SAP Statistical analysis plan
sCR Stringent complete response
SID Study Identification Number
SD Stable disease
TTNT Time to next treatment
VCD Bortezomib + cyclophosphamide + dexamethasone treatment
VD Bortezomib + dexamethasone treatment
VGPR Very good partial response
VMD Bortezomib + melphalan + dexamethasone treatment
VRD Bortezomib + lenalomide + dexamethasone treatment
VTD Bortezomib + thalidomide + dexamethasone treatment
VTD-PACE Bortezomib + thalidomide + dexamethasone + cisplatin + doxorubicin + cyclophosphamide + etoposide treatment
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
MR Minimal response
MRD Minimal residual disease
MRI Magnetic resonance imaging
NDMM Newly diagnosed multiple myeloma
ORR Overall response rate
OS Overall survival
PAS Post-authorization study
PD Progressive disease
PFS Progression-free survival
PR Partial response
RCT Randomized-controlled trial
RD Lenalomide + dexamethasone treatment
R-ISS Revised international staging system
RRMM Relapsed/refractory multiple myeloma
SAP Statistical analysis plan
sCR Stringent complete response
SID Study Identification Number
SD Stable disease
TTNT Time to next treatment
VCD Bortezomib + cyclophosphamide + dexamethasone treatment
VD Bortezomib + dexamethasone treatment
VGPR Very good partial response
VMD Bortezomib + melphalan + dexamethasone treatment
VRD Bortezomib + lenalomide + dexamethasone treatment
VTD Bortezomib + thalidomide + dexamethasone treatment
VTD-PACE Bortezomib + thalidomide + dexamethasone + cisplatin + doxorubicin +cyclophosphamide + etoposide treatment
EPID Research Page 6 of 27

Phafinacoepidemiological study protocol FIR-9542 Version 2.0 13 June 2019
3 ApprovalsWe have reviewed this study protocol (ER-9542 Version 2.0, dated 13 June 2013) and agree to its terms bysigning it.
//‘
Sign ure Date
F si Korhonen, Adjunct professor of biostatisties, PhD, Senior PrincipalMetsénneidonkuja 12, 02130 Espoo, Finland
6’ Ave 20/?
Co-iM‘fitors:
g): Vfge .20efrw - “(/9
signature , 7 DateJohn Lievonen, M'D//’//Dept. of Hematology, Helsinki University Hospital Comprehensive Cancer Center and University of HelsinkiHaartmaninkatu 4, rakennus 3, HelsinkiPL 372, 00029 HUS, Finland
Signature . V DateTatu Miettinen, MD
Takeda 0y, Paciuksenicatu 21, PO Box 1406, 00101 Helsinki, Finland
lEPDmr " A 7 Page7oi’
Phafinacoepidemiological study protocol FIR-9542 Version 2.0 13 June 2019
3 ApprovalsWe have reviewed this study protocol (ER-9542 Version 2.0, dated 13 June 2013) and agree to its terms bysigning it.
//‘
Sign ure Date
F si Korhonen, Adjunct professor of biostatisties, PhD, Senior PrincipalMetsénneidonkuja 12, 02130 Espoo, Finland
6’ Ave 20/?
Co-iM‘fitors:
g): Vfge .20efrw - “(/9
signature , 7 DateJohn Lievonen, M'D//’//Dept. of Hematology, Helsinki University Hospital Comprehensive Cancer Center and University of HelsinkiHaartmaninkatu 4, rakennus 3, HelsinkiPL 372, 00029 HUS, Finland
Signature . V DateTatu Miettinen, MD
Takeda 0y, Paciuksenicatu 21, PO Box 1406, 00101 Helsinki, Finland
lEPDmr " A 7 Page7oi’
Pharinacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
3 ApprovalsWe have reviewed this study pretocol (ER-9542 Version 2.0, dated 13 June 2019)- and agree to. its terms bysigning it.
(5’ Ave. 20 I?Sign ure Date
F si Korhonen, Adjunct professor of biostatistics, PhD, Senior PrincipalMetsfinneidonkuja '12, 02130 Espoo, Finland
(Jo-investigators:
“l
- “Jr-‘- ‘ '"fl-Fh) ' - 4’ _ 1___,,.:' "W’ ' h“(F-ff“. *3 { .‘t'f. \d" L“ , . L. 1-3
“‘5 DateSignature _. __ _Julia Lievonen, DDept. of Hematology, Helsinki University Hospital Comprehensive Cancer Center and University ef HelsinkiHaartmaninkatu 4, rakennus 3, HelsinkiPL 372, 00029 HUS, Finland
Signature - ' Date
Tatu Miettinen, MD
Takeda 0y, Paciuksenkatu- 21', PO Box 1406, 00101 Helsinki, Finland
--u _~. mm...— _.
Mr %' w " ' ' L ‘ ' ' Page? 072
Pharinacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
3 ApprovalsWe have reviewed this study pretocol (ER-9542 Version 2.0, dated 13 June 2019)- and agree to. its terms bysigning it.
(5’ Ave. 20 I?Sign ure Date
F si Korhonen, Adjunct professor of biostatistics, PhD, Senior PrincipalMetsfinneidonkuja '12, 02130 Espoo, Finland
(Jo-investigators:
“l
- “Jr-‘- ‘ '"fl-Fh) ' - 4’ _ 1___,,.:' "W’ ' h“(F-ff“. *3 { .‘t'f. \d" L“ , . L. 1-3
“‘5 DateSignature _. __ _Julia Lievonen, DDept. of Hematology, Helsinki University Hospital Comprehensive Cancer Center and University ef HelsinkiHaartmaninkatu 4, rakennus 3, HelsinkiPL 372, 00029 HUS, Finland
Signature - ' Date
Tatu Miettinen, MD
Takeda 0y, Paciuksenkatu- 21', PO Box 1406, 00101 Helsinki, Finland
--u _~. mm...— _.
Mr %' w " ' ' L ‘ ' ' Page? 072
Pharrnacoepidemioiogical study protocol FIR-9542 Version 2.0 13 June 2019
3 ApprovalsWe have reviewed this study protocol {ER-9542 Version 2.0, dated 13 June 2019) and agree to its terms bysigning it.
6’ Ave. 201‘?Sign ure Date
F si Korhonen, Adjunct professor of biostatistics, PhD, Senior Principal
Metsanneidonkuja 12, 02130 Espoo, Finland
Co-invest'fitors:
Datesignature , .0 rJilin Lievonen, M'D/I/Dept. of Hematology, Helsinki University Hospital Comprehensive Cancer Center and University of HelsinkiHaartmanlnkatu 4, rakennus 3, HelsinkiPL 372, 00029 HUS, Finland
Signature - ' Date
Tatu Miettinen, MD
Takeda 0y, Pacluksenkatu 21, PO Box 1406, 00101 Helsinki, Finland
Page7or27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 8 of 27
Responsible parties
Sponsor: Takeda Finland
Study conduct: EPID Research (an IQVIA company), Metsänneidonkuja 12, FI-02130 Espoo, Finland
Principal investigator: Pasi Korhonen
Co-investigators: Juha Mehtälä, Jenna Anderson, Ilona Iso-Mustajärvi, Saara Hetemäki and Alisa Kopilow from EPID Research, Carina von Schantz-Fant, Saku Torvinen and Tatu Miettinen from Takeda Finland, Juha Lievonen from HUS
Sponsor project lead: Tatu Miettinen
Steering committee: Principal investigator Pasi Korhonen (PhD), EPID Research
Medical expert Juha Lievonen (MD), Helsinki University Central Hospital
Representative of the sponsor Tatu Miettinen (MD), Takeda Finland
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
Responsible parties
Sponsor: Takeda Finland
Study conduct: EPID Research (an IQVIA company), Metsanneidonkuja 12, F|-0213O Espoo, Finland
Principal investigator: Pasi Korhonen
Co-investigators: Juha Mehtala, Jenna Anderson, Ilona Iso-Mustajarvi, Saara Hetemaki and AlisaKopilow from EPID Research, Carina von Schantz-Fant, Saku Torvinen and TatuMiettinen from Takeda Finland, Juha Lievonen from HUS
Sponsor project lead: Tatu Miettinen
Steering committee: Principal investigator Pasi Korhonen (PhD), EPID Research
Medical expert Juha Lievonen (MD), Helsinki University Central Hospital
Representative of the sponsor Tatu Miettinen (MD), Takeda Finland
EPID Research Page 8 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 9 of 27
4 Amendments and updates
5 Milestones
Milestone Actual/Planned date
Registration in the EU PAS register 01 September 2017
Start of data permit process 12 September 2017
End of data permit process 20 April 2018
Start of data collection 18 June 2018
End of data collection 13 November 2017
Start of data analysis 21 September 2018
End of data analysis August 2019
Start of data permit process for extended study period
May 2019
End of data permit process for extended study period July 2019
Start of data collection for extended study period July 2019
End of data collection extended study period August 2019
No. Date Section of study protocol
Amendment or update Reason
1 13 June 2019 - Abstract - 5 Milestones - 7.2 Secondary objectives - 8.1 Study design - 8.2.3 Follow-up - 8.3.4 Treatment patterns - 8.3.5.3 Treatment selection - 8.10.1 Data source - 10 Protection of human subjects
- The actual study cohort changed to include patients diagnosed with MM during the period 01 January 2010 – 31 December 2015 and treated for MM during the period 01 January 2010 – 31 December 2016. - The end of the follow-up period changed from 31 December 2015 to 31 December 2017. - "No treatment" removed from treatment selection. - References to applicable legislation updated.
Extension of the follow-up period until the end of 2017. Treatment selection redefined for accuracy. Outdated references to applicable legislation.
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
4 Amendments and updates
No. Date Section of Amendment or update Reasonstudy protocol
1 13 June 2019 - Abstract - The actual study cohort changed to Extension of the follow-up- 5 Milestones- 7.2Secondaryobjectives- 8.1 Studydesign- 8.2.3 Follow-
UP- 8.3.4Treatmentpatterns- 8.3.5.3Treatmentselection- 8.10.1 Datasource- 10 Protectionof humansubjects
include patients diagnosed with MMduring the period 01 January 2010 —31 December 2015 and treated forMM during the period 01 January2010 — 31 December 2016.- The end of the follow-up periodchanged from 31 December 2015 to31 December 2017.- "No treatment" removed fromtreatment selection.- References to applicable legislationupdated.
period until the end of2017. Treatment selectionredefined for accuracy.Outdated references toapplicable legislation.
5 Milestones
Milestone Actual/Planned date
Registration in the EU PAS register 01 September 2017
Start of data permit process 12 September 2017
End of data permit process 20 April 2018
Start of data collection 18 June 2018
End of data collection 13 November 2017
Start of data analysis 21 September 2018
End of data analysis August 2019
pefiodStart of data permit process for extended study May 2019
End of data permit process for extended study period July 2019
Start of data collection for extended study period July 2019
End of data collection extended study period August 2019
EPID Research Page 9 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 10 of 27
Start of data analysis extended study period August 2019
End of data analysis extended study period September 2019
Start of study reporting process September 2019
Final report of study results December 2019
Start of scientific reporting process January 2020
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
Start of data analysis extended study period August 2019
End of data analysis extended study period September 2019
Start of study reporting process September 2019
Final report of study results December 2019
Start of scientific reporting process January 2020
EPID Research Page 10 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 11 of 27
6 Rationale and background
Multiple myeloma (MM) is a clonal haematologic malignancy of plasma cells that is characterized by accumulation of these malignant plasma cells in the bone marrow. The development of MM results from early genetic aberrations that lead to monoclonal gammopathy of unknown significance (MGUS), and further genetic changes that may lead to smouldering myeloma and potentially to the progression to active myeloma [1]. However, factors that cause MM are not fully known. MM symptoms including bone pain, bleeding, anaemia, fatigue, hypercalcaemia, renal insufficiency, and frequent infections occur as the disease advances. Treatment is usually required only after the disease has advanced. It constitutes approximately 1% of all reported cancers and it is the second most common haematologic malignancy worldwide [2]. In Finland, approximately 350 – 400 new MM cases are diagnosed each year. The median age at diagnosis is close to 70 years of age and the average survival with the disease is estimated to be 5-6 years, but it varies greatly depending on the patient’s risk status. As MM patients are generally elderly patients, they have potentially multiple co-morbidities. Therefore, and due to factors related to the disease itself and myeloma-specific and supportive treatments, patients require frequent monitoring and hospital visits.
The overall survival (OS) in MM has improved significantly during the last decades, mainly due to developments in autologous stem cell transplants and novel drug treatments. However, despite improved treatment options, MM remains practically incurable with current therapy and it is characterized by multiple relapses. It typically recurs with a more aggressive disease course after each remission, resulting in shorter duration of response with each successive line of therapy and eventually treatment-refractory disease [3]. Patients may have several phenotypic characteristics, such as tumour burden, co-morbidities, age, or other general conditions that influence treatment decisions. In addition, there are genotypic factors that affect prognosis and treatment responses. These high-risk biomarkers include cytogenetic abnormalities (defined as deletion 17p [del(17p)], translocation [t(4;14)], and/or translocation [t(14;16)]) [4].
Standardized staging systems for MM help predict outcome and help physicians in some cases select appropriate therapy for patients [5]. The International Staging System (ISS), which has recently been updated to the revised (R)-ISS by the International Myeloma Working Group (IMWG), is commonly used for staging of MM [6]. The systems are based on key measures that describe the disease burden and assess patients’ characteristics. These risk assessment scores (described in Annex 2) include parameters like serum β2-microglobulin, albumin and lactate dehydrogenase, and the presence or absence of high-risk cytogenetic changes. The Finnish nationwide characterization of myeloma patients regarding phenotypic and genotypic features, and their effect on survival, has not been studied.
There are general treatment guidelines for myeloma [7]. The treatment guidelines are different for patients older than 65 (-70) years and younger than that. Stem cell transplant is considered the front-line treatment in younger and fit enough patients and is most often autologous (called ASCT) but may be allogenic. ASCT treatment consists of induction therapy of 3-4 cycles with a doublet or triplet therapy (primarily bortezomib + cyclophosphamide + dexamethasone OR bortezomib + dexamethasone) followed by collection of stem cells, high-dose chemotherapy, and stem cell transplantation. In some cases, a second ASCT (called a tandem transplant) may be recommended within 6 to 12 months, or upon relapse. Elderly and/or frail patients are not considered eligible for ASCT and their primary treatment options include bortezomib + melphalan + prednisone for 8-9 nine cycles (or 12 months) OR lenalidomide + dexamethasone for 18 months or until progression OR bortezomib + dexamethasone for 8-9 nine cycles (or 12 months). The complete guidance is presented in Annex 3.
It is thought that already at the time of diagnosis, there are heterogeneous populations of tumour cells present, known as sub-clones [8]. It is not known how myeloma treatments and different treatment combinations and their sequences modify the drug-sensitivity and/or the resistance of myeloma cell clones. Therefore, it is interesting to study whether initial or early line therapies have a significant effect on later treatment responses and survival.
Evidence of new treatments is usually based on phase III randomized-controlled trials (RCTs). Despite being the gold standard for providing evidence on treatments’ causal effects on patient outcomes, RCTs may have
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
6 Rationale and background
Multiple myeloma (MM) is a clonal haematologic malignancy of plasma cells that is characterized byaccumulation of these malignant plasma cells in the bone marrow. The development of MM results fromearly genetic aberrations that lead to monoclonal gammopathy of unknown significance (MG US), and furthergenetic changes that may lead to smouldering myeloma and potentially to the progression to active myeloma[1]. However, factors that cause MM are not fully known. MM symptoms including bone pain, bleeding,anaemia, fatigue, hypercalcaemia, renal insufficiency, and frequent infections occur as the disease advances.Treatment is usually required only after the disease has advanced. It constitutes approximately 1% of allreported cancers and it is the second most common haematologic malignancy worldwide [2]. In Finland,approximately 350 — 400 new MM cases are diagnosed each year. The median age at diagnosis is close to 70years of age and the average survival with the disease is estimated to be 5-6 years, but it varies greatlydepending on the patient’s risk status. As MM patients are generally elderly patients, they have potentiallymultiple co-morbidities. Therefore, and due to factors related to the disease itself and myeloma-specific andsupportive treatments, patients require frequent monitoring and hospital visits.
The overall survival (OS) in MM has improved significantly during the last decades, mainly due todevelopments in autologous stem cell transplants and novel drug treatments. However, despite improvedtreatment options, MM remains practically incurable with current therapy and it is characterized by multiplerelapses. It typically recurs with a more aggressive disease course after each remission, resulting in shorterduration of response with each successive line of therapy and eventually treatment-refractory disease [3].Patients may have several phenotypic characteristics, such as tumour burden, co-morbidities, age, or othergeneral conditions that influence treatment decisions. In addition, there are genotypic factors that affectprognosis and treatment responses. These high-risk biomarkers include cytogenetic abnormalities (definedas deletion 17p [del(17p)], translocation [t(4;14)], and/or translocation [t(14;16)]) [4].
Standardized staging systems for MM help predict outcome and help physicians in some cases selectappropriate therapy for patients [5]. The International Staging System (ISS), which has recently been updatedto the revised (R)-ISS by the International Myeloma Working Group (IMWG), is commonly used for staging ofMM [6]. The systems are based on key measures that describe the disease burden and assess patients’characteristics. These risk assessment scores (described in Annex 2) include parameters like serum [32-microglobulin, albumin and lactate dehydrogenase, and the presence or absence of high-risk cytogeneticchanges. The Finnish nationwide characterization of myeloma patients regarding phenotypic and genotypicfeatures, and their effect on survival, has not been studied.
There are general treatment guidelines for myeloma [7]. The treatment guidelines are different for patientsolder than 65 (-70) years and younger than that. Stem cell transplant is considered the front-line treatmentin younger and fit enough patients and is most often autologous (called ASCT) but may be allogenic. ASCTtreatment consists of induction therapy of 3-4 cycles with a doublet or triplet therapy (primarily bortezomib+ cyclophosphamide + dexamethasone OR bortezomib + dexamethasone) followed by collection of stemcells, high-dose chemotherapy, and stem cell transplantation. In some cases, a second ASCT (called a tandemtransplant) may be recommended within 6 to 12 months, or upon relapse. Elderly and/or frail patients arenot considered eligible for ASCT and their primary treatment options include bortezomib + melphalan +prednisone for 8-9 nine cycles (or 12 months) OR lenalidomide + dexamethasone for 18 months or untilprogression OR bortezomib + dexamethasone for 8-9 nine cycles (or 12 months). The complete guidance ispresented in Annex 3.
It is thought that already at the time of diagnosis, there are heterogeneous populations of tumour cellspresent, known as sub-clones [8]. It is not known how myeloma treatments and different treatmentcombinations and their sequences modify the drug-sensitivity and/or the resistance of myeloma cell clones.Therefore, it is interesting to study whether initial or early line therapies have a significant effect on latertreatment responses and survival.
Evidence of new treatments is usually based on phase III randomized-controlled trials (RCTs). Despite beingthe gold standard for providing evidence on treatments’ causal effects on patient outcomes, RCTs may have
EPID Research Page 11 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 12 of 27
several practical limitations. Real-life clinical practice may differ greatly from the RCTs’ highly selected patient population, who are randomised to obtain pre-selected study treatments. Therefore, the risks and benefits may manifest differently in real-life clinical practice as compared to that in an RCT. In addition, RCTs are often based on a relatively small population with a short follow-up time. Observational studies based on secondary data collected in routine clinical practice may provide the opportunity to investigate large-scale populations with long-term follow-up.
In Finland, it is not completely known how MM patients are treated in real-life clinical settings. In addition, the prevalence of various risk factors, and the effect of a patient’s risk status on treatment, e.g. on type, duration, and outcomes such as overall survival (OS) and time to next treatment (TTNT), have not been sufficiently reported in Finland. In order to evaluate the effectiveness of new MM treatments in real-life clinical practice it may not be possible to find suitable comparators shortly after the new treatment has entered the market. Historical comparators may then serve as alternative references. Moreover, the need for real-world evidence for new improved treatment options might be highlighted in certain MM patient subgroups. For example, there might be subgroups who have not been able to receive certain conventional therapies due to their condition or who have had the need to discontinue or modify the dose of therapy due to (unsuitable) nature of the therapy. To be able to evaluate how such subgroups could benefit from new treatment options, it is important to identify these subgroups and to evaluate the outcomes under current and past treatment options.
7 Research questions and objectives
There is a lack of information on real-life clinical practice, treatment patterns, and treatment outcomes in Finnish MM patients with different types and stages of the disease. The aim of this study is to provide a representative description of MM patients’ characteristics, treatment patterns, and treatment outcomes in Finland. The results of this study can be used as a historical reference when evaluating the changing MM treatment landscape. This is a descriptive study without specific a-priori hypotheses to be tested.
7.1 Primary objectives
The primary objective is to characterise the Finnish MM population and to describe the overall survival and time to next treatment on the overall level, and stratified by known patient-related prognostic factors.
Primary objective 1 is to describe the characteristics and patient journey of Finnish MM patients, including
• Demographics
• Disease characteristics
• Treatment patterns
Primary objective 2 is to evaluate OS and TTNT among MM patients, stratified by
• Patients’ demographics
• Disease characteristics
• Types of treatment (major treatment regimens in the 1st, 2nd, 3rd, 4th, >4th line)
• Lines of treatment, including first-line treatment in newly diagnosed (ND) MM patients as well as later treatment lines (relapsed/refractory (RR) MM patients)
7.2 Secondary objectives
Secondary objective 1 is to identify patient, disease, and treatment-related factors that are associated with
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 june 2019
several practical limitations. Real-life clinical practice may differ greatly from the RCTs’ highly selected patientpopulation, who are randomised to obtain pre-selected study treatments. Therefore, the risks and benefitsmay manifest differently in real-life clinical practice as compared to that in an RCT. In addition, RCTs are oftenbased on a relatively small population with a short follow-up time. Observational studies based on secondarydata collected in routine clinical practice may provide the opportunity to investigate large-scale populationswith long-term follow-up.
In Finland, it is not completely known how MM patients are treated in real-life clinical settings. In addition,the prevalence of various risk factors, and the effect of a patient’s risk status on treatment, e.g. on type,duration, and outcomes such as overall survival (OS) and time to next treatment (TTNT), have not beensufficiently reported in Finland. In order to evaluate the effectiveness of new MM treatments in real-lifeclinical practice it may not be possible to find suitable comparators shortly after the new treatment hasentered the market. Historical comparators may then serve as alternative references. Moreover, the needfor real-world evidence for new improved treatment options might be highlighted in certain MM patientsubgroups. For example, there might be subgroups who have not been able to receive certain conventionaltherapies due to their condition or who have had the need to discontinue or modify the dose of therapy dueto (unsuitable) nature of the therapy. To be able to evaluate how such subgroups could benefit from newtreatment options, it is important to identify these subgroups and to evaluate the outcomes under currentand past treatment options.
7 Research questions and objectives
There is a lack of information on real-life clinical practice, treatment patterns, and treatment outcomes inFinnish MM patients with different types and stages of the disease. The aim of this study is to provide arepresentative description of MM patients’ characteristics, treatment patterns, and treatment outcomes inFinland. The results of this study can be used as a historical reference when evaluating the changing MMtreatment landscape. This is a descriptive study without specific a-priori hypotheses to be tested.
7.1 Primary objectives
The primary objective is to characterise the Finnish MM population and to describe the overall survival andtime to next treatment on the overall level, and stratified by known patient-related prognostic factors.
Primary objective 1 is to describe the characteristics and patient journey of Finnish MM patients, including
0 Demographics
0 Disease characteristics
0 Treatment patterns
Primary objective 2 is to evaluate OS and TTNT among MM patients, stratified by
Patients’ demographics
0 Disease characteristics
0 Types of treatment (major treatment regimens in the 1“, 2nd, 3rd, 4th, >4th line)
0 Lines of treatment, including first-line treatment in newly diagnosed (ND) MM patients as well aslater treatment lines (relapsed/refractory (RR) MM patients)
7.2 Secondary objectives
Secondary objective 1 is to identify patient, disease, and treatment-related factors that are associated with
EPID Research Page 12 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 13 of 27
• Treatment selection
• OS
• Duration of each treatment line
• TTNT
Secondary objective 2 is to characterise MM patient subpopulations, including those categorised as high-, standard- or low-risk according to R-ISS. Additionally, the following MM patient subpopulations will be identified and characterised:
• Patients who did not receive the following pre-specified treatments:
o Transplant, duplet vs. triplet therapy, other
• Patients who had short durations of each treatment line
The definition of short treatment duration will be described in more detail in the statistical analysis plan (SAP). Characterisation of each of these subpopulations includes similar description as in Primary objective 1. In addition, OS and TTNT will be described in these subgroups.
8 Research methods
8.1 Study design
This is a retrospective observational cohort study using the Finnish Hematology Register (FHR) as the data source. The study will include:
1) Patients diagnosed with MM during the period 01 January 2010 – 31 December 2015 and aged 18 years or older at diagnosis (i.e. the whole study cohort).
2) Patients diagnosed with MM during the period 01 January 2010 – 31 December 2015 and treated for MM during the period 01 January 2010 – 31 December 2016 and aged 18 years or older at diagnosis. This actual study cohort will include only patients for whom at least one treatment initiation date can be identified and who have a minimum of one year of potential follow-up time (to 31 December 2017).
Parameters such as age, gender, co-morbidities, date of MM diagnosis, disease status, received treatments, start of treatments and lines of treatment will be collected.
8.2 Population and setting
8.2.1 Subject selection
The FHR includes approximately 1600 MM patients, but it is estimated that data are comprehensively recorded for at least 300-400 patients. Main analyses are conducted on the actual cohort with complete records and at least one year of potential follow-up time. Descriptive and sensitivity analyses will be performed on the whole MM cohort.
8.2.1.1 Inclusion criteria
• MM diagnosis recorded in the FHR
• Age 18 years or older at the time of MM diagnosis
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 lune 2019
0 Treatment selection
0 OS
0 Duration of each treatment line
0 TTNT
Secondary objective 2 is to characterise MM patient subpopulations, including those categorised as high-,standard- or low-risk according to R-ISS. Additionally, the following MM patient subpopulations will beidentified and characterised:
0 Patients who did not receive the following pre-specified treatments:
0 Transplant, duplet vs. triplet therapy, other
0 Patients who had short durations of each treatment line
The definition of short treatment duration will be described in more detail in the statistical analysis plan(SAP). Characterisation of each of these subpopulations includes similar description as in Primary objective1. In addition, OS and TTNT will be described in these subgroups.
8 Research methods
8.1 Study design
This is a retrospective observational cohort study using the Finnish Hematology Register (FHR) as the datasource. The study will include:
1) Patients diagnosed with MM during the period 01 January 2010 — 31 December 2015 and aged 18 yearsor older at diagnosis (i.e. the whole study cohort).
2) Patients diagnosed with MM during the period 01 January 2010 — 31 December 2015 and treated for MMduring the period 01 January 2010 — 31 December 2016 and aged 18 years or older at diagnosis. This actualstudy cohort will include only patients for whom at least one treatment initiation date can be identified andwho have a minimum of one year of potential follow-up time (to 31 December 2017).
Parameters such as age, gender, co-morbidities, date of MM diagnosis, disease status, received treatments,start of treatments and lines of treatment will be collected.
8.2 Population and setting
8.2.1 Subject selection
The FHR includes approximately 1600 MM patients, but it is estimated that data are comprehensivelyrecorded for at least 300-400 patients. Main analyses are conducted on the actual cohort with completerecords and at least one year of potential follow-up time. Descriptive and sensitivity analyses will beperformed on the whole MM cohort.
8.2.1.1 Inclusion criteria
0 MM diagnosis recorded in the FHR
0 Age 18 years or older at the time of MM diagnosis
EPID Research Page 13 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 14 of 27
8.2.1.2 Exclusion criteria
• Multiple haematological diagnoses in the FHR for which the treatments cannot be differentiated
All individuals meeting the above inclusion criteria and none of the exclusion criteria will be included for descriptive analyses (e.g. whole study cohort). Data recordings related to treatment are required for some analyses and therefore only individuals for which such records are available in the register (i.e. actual study cohort) will be included in those analyses. The analyses will be described in more detail in the SAP. It is expected that data recordings in the FHR are not selective and that the study population represents the general MM patient population in Finland.
8.2.2 Cohort entry date
For each patient, the whole study cohort entry date is defined as date of MM diagnosis. The actual study cohort entry date is defined as the first MM treatment initiation in the FHR.
8.2.3 Follow-up
Patients in the actual study cohort will be followed-up starting from the first treatment initiation date recorded in the FHR during the study period. Follow-up will continue until the first of the following events occur: death, loss to follow-up, or end of the study or follow-up period (31 December 2017).
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
8.2.1.2 Exclusion criteria
0 Multiple haematological diagnoses in the FHR for which the treatments cannot be differentiated
All individuals meeting the above inclusion criteria and none of the exclusion criteria will be included fordescriptive analyses (e.g. whole study cohort). Data recordings related to treatment are required for someanalyses and therefore only individuals for which such records are available in the register (i.e. actual studycohort) will be included in those analyses. The analyses will be described in more detail in the SAP. It isexpected that data recordings in the FHR are not selective and that the study population represents thegeneral MM patient population in Finland.
8.2.2 Cohort entry date
For each patient, the whole study cohort entry date is defined as date of MM diagnosis. The actual studycohort entry date is defined as the first MM treatment initiation in the FHR.
8.2.3 Follow-upPatients in the actual study cohort will be followed-up starting from the first treatment initiation daterecorded in the FHR during the study period. Follow-up will continue until the first of the following eventsoccur: death, loss to follow-up, or end of the study or follow-up period (31 December 2017).
EPID Research Page 14 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 15 of 27
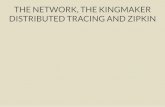
8.2.4 Schematic presentation of a study patient
Figure 1. Schematic presentation of the study for a single MM patient. The figure shows several patient and treatment-related characteristics as a function of time, starting from the date of MM diagnosis until death. Specifically, the M-component amount (g/L) is shown with the light brown curve, start of symptoms with a vertical dashed brown line and time of death with a vertical dashed black line. Depending on the patient, date of diagnosis can occur at any time over an interval and is indicated with a black horizontal arrow. At the top of the figure, type of myeloma is presented as being asymptomatic vs. symptomatic, and more specifically as being either MGUS, active MM, relapsed, or relapsed refractory. Dates of different disease statuses are indicated with blue horizontal arrows (status start/end). Treatment line start (1st, 2nd, 3rd) is shown with a vertical arrow and the duration of each treatment line with a horizontal blue line. The cohort entry date is indicated by a black dot at the start of the first line of treatment. Outcomes (OS, TTNT) are illustrated at the bottom of the figure with black arrows.
8.3 Variables
The following data will be collected from the FHR, from diagnosis (Dg), from the start of treatment, and/or from the time of follow-up as indicated when available for the actual cohort.
8.3.1 Patients’ demographics
Variables concerning patient demographics are available only at diagnosis.
• Year of birth • Gender • Date of MM diagnosis • Age at diagnosis • Known co-morbidities
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
8.2.4 Schematic presentation of a study patient
Figure 1. Schematic presentation of the study for a single MM patient. The figure shows several patient and treatment-relatedcharacteristics as a function of time, starting from the date of MM diagnosis until death. Specifically, the M-component amount(g/L) is shown with the light brown curve, start of symptoms with a vertical dashed brown line and time of death with a verticaldashed black line. Depending on the patient, date of diagnosis can occur at any time over an interval and is indicated with a blackhorizontal arrow. At the top of the figure, type of myeloma is presented as being asymptomatic vs. symptomatic, and morespecifically as being either MGUS, active MM, relapsed, or relapsed refractory. Dates of different disease statuses are indicatedwith blue horizontal arrows (status start/end). Treatment line start (1“, 2nd, 3“) is shown with a vertical arrow and the durationof each treatment line with a horizontal blue line. The cohort entry date is indicated by a black dot at the start of the first line oftreatment. Outcomes (OS, TTNT) are illustrated at the bottom of the figure with black arrows.
A Death
Asymptomatic : Symptomatic :I IMEUE or Rela pseclI peed I
Smolderlng I Active MM fidelapmd “1:; refractoryr |myeloma I sease ase disease I
I II FTUEI'ESEIVE Relapse Relapse Progresstve II dISEHSE H 53' disease :-* a :: . Iii—H
Complete Partial response I I |response I
II
I 3'“ lin:e treatment ‘{durationl'
-..IIIIIII
15" lineltreatment
M-co
mpo
nent
{gill}
I Diagnosis | I
-—
_—
——
——
1—
—
||||I
|Etreatrnent .4 TTHTLI TTI'ITldi fine to flrsl: Tim;
I I T 1 os1I £ | U52I ; U53I. 05
8.3 Variables
The following data will be collected from the FHR, from diagnosis (Dg), from the start of treatment, and/orfrom the time of follow-up as indicated when available for the actual cohort.
8.3.1 Patients’ demographics
Variables concerning patient demographics are available only at diagnosis.
Year of birthGenderDate of MM diagnosisAge at diagnosisKnown co-morbidities
EPID Research Page 15 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 16 of 27
8.3.2 Disease characteristics
8.3.2.1 Available only at diagnosis
• Calcium (elevated), Renal failure, Anaemia, Bone lesions (CRAB) o Hypercalcaemia o Renal dysfunction o Anaemia o Lytic bone lesions
• Fluorescence in situ hybridization (FISH), including (and/or)
o High risk cytogenics, e.g.
▪ Deletion 17p [del(17p)]
▪ Translocation [t(4;14)]
▪ Translocation [t(14;16)]
o Non-high risk cytogenics, e.g.
▪ Translocation [t(14;20)]
▪ Gain 1q [gain(1q21)]
▪ Deletion 1p32 [del(1p32)]
8.3.2.2 Available at diagnosis and/or for each treatment line
• Myeloma type (e.g. smouldering, MGUS, or active MM)
• Disease stage (ISS/R-ISS)
• Risk classification, according to the R-ISS in Annex 2 (high-, standard-, or low-risk)
• Disease status (Diagnosis (Dg), stringent complete response (sCR), complete response (CR), very good partial response (VGPR), partial response (PR), minimal response (MR), stable disease (SD), progressive disease (PD), clinical relapse, relapse from CR, relapse from minimal residual disease (MRD) negative, exitus)
• M-component, including:
o Concentration and type (serum and urine): g/L and IgA/IgG/IgD/IgM
o Concentration and type of light chain (serum): K, L
• Clinical haematology, including:
o Absolute neutrophil count (ANC)
o Haemoglobin
o Platelet count
o Creatinine (eGFR to be calculated by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula)
o Lactate dehydrogenase (LDH)
• Bone lesions
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
8.3.2 Disease characteristics
8.3.2.1 Available only at diagnosis
0 Calcium (elevated), Renal failure, Anaemia, Bone lesions (CRAB)o Hypercalcaemia0 Renal dysfunction0 Anaemiao Lytic bone lesions
0 Fluorescence in situ hybridization (FISH), including (and/or)
0 High risk cytogenics, e.g.
I Deletion 17p [del(17p)]
I Translocation[t(4;14)]
I Translocation[t(14;16)]
o Non-high risk cytogenics, e.g.
I Translocation[t(14;20)]
I Gain 1q [gain(1q21)]
I Deletion 1p32 [del(1p32)]
8.3.2.2 Available at diagnosis and/or for each treatment line
0 Myeloma type (e.g. smouldering, MGUS, or active MM)
0 Disease stage (lSS/R-ISS)
0 Risk classification, according to the R-ISS in Annex 2 (high-, standard-, or low-risk)
0 Disease status (Diagnosis (Dg), stringent complete response (sCR), complete response (CR), very goodpartial response (VGPR), partial response (PR), minimal response (MR), stable disease (SD),progressive disease (PD), clinical relapse, relapse from CR, relapse from minimal residual disease(MRD) negative, exitus)
o M-component, including:
0 Concentration and type (serum and urine): g/L and IgA/IgG/IgD/IgM
0 Concentration and type of light chain (serum): K, L
0 Clinical haematology, including:
0 Absolute neutrophil count (ANC)
o Haemoglobin
o Platelet count
0 Creatinine (eGFR to be calculated by the Chronic Kidney Disease Epidemiology Collaboration(CKD-EPI) formula)
0 Lactate dehydrogenase (LDH)
0 Bone lesions
EPID Research Page 16 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 17 of 27
• Bone marrow aspirate and/or biopsy results, including (and/or):
o Percentage of plasma cells in bone marrow aspirates
o Percentage of plasma cells in bone marrow trephine biopsies
o Percentage of MM cells of total cells and of plasma cells (flow cytometry)
8.3.3 Follow-up variables
• Date of last follow-up
• Patient status at the date of last follow-up or end of the data collection period
• Date of death (where available)
8.3.4 Treatment patterns
Variables concerning treatment patterns as may be available during follow-up for the actual cohort:
• Line of treatment (1st, 2nd, 3rd, 4th, >4 lines of treatment)
• Treatment, such as:
o Transplant (single/tandem) vs. no transplant
o Duplet vs triplet therapy
o Other
• Number of cycles per treatment line
• Date of start of each treatment
• Date of end of each treatment
• Time to discontinuation of each treatment, where applicable
8.3.5 Outcomes
8.3.5.1 OS
OS is defined as time from actual cohort entry until death. In addition, OS among those who have received treatment lines 1, 2, 3, 4, >4, will be defined as time from first having the treatment in question (1st, 2nd, 3rd, 4th, >4 lines of treatment) until death.
8.3.5.2 TTNT
The time to next treatment (TTNT1, TTNT2, and further) is defined as the length of time between the start of a treatment line to the start of the next treatment line. Specifically, TTNT1 is defined as the length of time between the start of the first treatment line (following diagnosis) to the start of the second treatment line, TTNT2 is the length of time between the start of the second treatment line to the start of the third treatment line, and so on.
8.3.5.3 Treatment selection
Treatment selection is defined as single transplant, tandem transplant, duplet therapy, triplet therapy, or other. All available treatments will be described and later categorised into selected treatment groups in the SAP.
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
0 Bone marrow aspirate and/or biopsy results, including (and/or):
0 Percentage of plasma cells in bone marrow aspirates
0 Percentage of plasma cells in bone marrow trephine biopsies
0 Percentage of MM cells of total cells and of plasma cells (flow cytometry)
8.3.3 Follow-up variables
0 Date of last follow-up
0 Patient status at the date of last follow-up or end of the data collection period
0 Date of death (where available)
8.3.4 Treatment patterns
Variables concerning treatment patterns as may be available during follow-up for the actual cohort:
- Line of treatment (1“, 2nd, 3rd, 4th, >4 lines of treatment)
0 Treatment, such as:
o Transplant (single/tandem) vs. no transplant
0 Duplet vs triplet therapy
0 Other
0 Number of cycles per treatment line
0 Date of start of each treatment
0 Date of end of each treatment
0 Time to discontinuation of each treatment, where applicable
8.3.5 Outcomes
8.3.5.1 OS
OS is defined as time from actual cohort entry until death. In addition, OS among those who have receivedtreatment lines 1, 2, 3, 4, >4, will be defined as time from first having the treatment in question (1“, 2nd, 3rd,4th, >4 lines of treatment) until death.
8.3.5.2 TTNT
The time to next treatment (TTNT1, TTNT2, and further) is defined as the length of time between the start ofa treatment line to the start of the next treatment line. Specifically, TTNT1 is defined as the length of timebetween the start of the first treatment line (following diagnosis) to the start of the second treatment line,TTNT2 is the length oftime between the start ofthe second treatment line to the start ofthe third treatmentline, and so on.
8.3.5.3 Treatment selection
Treatment selection is defined as single transplant, tandem transplant, duplet therapy, triplet therapy, orother. All available treatments will be described and later categorised into selected treatment groups in theSAP.
EPID Research Page 17 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 18 of 27
8.3.5.4 Treatment duration
The duration of treatment is defined as the length of time (month) from the start of a treatment line to the end of that treatment line. In cases where treatment has been discontinued, the time from the initiation to discontinuation of the treatment will be calculated.
8.3.5.5 Overall response rate
The overall response rate (ORR) is defined as the proportion of patients in the actual cohort who have at least a partial response to treatment, and will be calculated per treatment regimen within a line of treatment.
8.4 Other definitions
• Newly diagnosed multiple myeloma (NDMM) is defined as those patients who have active, measurable MM and have initiated no more than the first line of treatment. Definitions of other patient populations according to the IMWG, including RRMM, can be found in Annex 4.
• CRAB components are defined below according to the IMWG [4]: o Hypercalcaemia is defined as corrected serum calcium > 11.5 mg/dL or 2.5 mmol/L. o Renal dysfunction is defined as having a creatinine clearance of < 40 mL per minute, or serum
creatinine > 2 mg/dL (177 µmol/L). o Anaemia is defined as a haemoglobin value < 100 g/L, or > 20 g/L below the lowest limit of
normal o Bone lesions including one or more osteolytic lesions found on skeletal radiography, CT,
Magnetic Resonance Imaging (MRI), or PET-CT • Overall response to treatment is defined as any of the following disease statuses as recorded in the FHR:
PR, VGPR, CR, or sCR. In the case of missing data, partial or complete response to treatment will be defined as not having SD nor disease progression.
• Disease progression is defined as any of the following disease statuses as recorded in the FHR: PD or clinical relapse. In the case of missing data, disease progression is defined according to the IMWG criteria as indicated in Annex 5.
• Relapse is defined as any of the following disease statuses as recorded in the FHR: Relapse from CR, or relapse from MRD negative.
• Line of treatment is defined as one or more cycles of a treatment program. Treatment lines are numbered successively, starting with first treatment line, second treatment line, and further. Where available, they are defined numerically using the line of treatment variable recorded in the register. If not available in this way, each new treatment line is defined as a drug regimen that starts following disease progression. In the case of transplantation, tandem transplantation is defined as two transplantations within 6 months, whereas multiple single transplants are defined as two transplantations separated by at least a 12-months interval.
8.5 Data sources
Data from FHR on MM patients with recordings will be used. The FHR is owned by the Finnish Society of Hematology (FSH). The FHR is a national, population-based register founded in January 2010. Information concerning the treatment and treatment responses of patients with haematological disorders are included in this register, starting from the time of diagnosis and during follow-up. Patients must provide informed consent (IC) for their data to be recorded into the register and to be available for research purposes. The FHR includes approximately 1600 MM patients, but it is estimated that currently data including treatment are recorded for at least 300-400 patients.
8.6 Study size
The population size for the whole study cohort is approximately 1600 MM patients, while the population size for the actual study cohort is approximately 300-400 patients. As this is primarily a descriptive study, this
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
8.3.5.4 Treatment duration
The duration of treatment is defined as the length of time (month) from the start of a treatment line to theend of that treatment line. In cases where treatment has been discontinued, the time from the initiation todiscontinuation of the treatment will be calculated.
8.3.5.5 Overall response rate
The overall response rate (ORR) is defined as the proportion of patients in the actual cohort who have atleast a partial response to treatment, and will be calculated per treatment regimen within a line oftreatment.
8.4 Other definitions
0 Newly diagnosed multiple myeloma (NDMM) is defined as those patients who have active, measurableMM and have initiated no more than the first line of treatment. Definitions of other patient populationsaccording to the IMWG, including RRMM, can be found in Annex 4.
- CRAB components are defined below according to the IMWG [4]:o Hypercalcaemia is defined as corrected serum calcium > 11.5 mg/dL or 2.5 mmol/L.0 Renal dysfunction is defined as having a creatinine clearance of < 40 mL per minute, or serum
creatinine > 2 mg/dL (177 umol/L).o Anaemia is defined as a haemoglobin value < 100 g/L, or > 20 g/L below the lowest limit of
normal0 Bone lesions including one or more osteolytic lesions found on skeletal radiography, CT,
Magnetic Resonance Imaging (MRI), or PET-CT- Overall response to treatment is defined as any of the following disease statuses as recorded in the FHR:
PR, VGPR, CR, or sCR. In the case of missing data, partial or complete response to treatment will bedefined as not having SD nor disease progression.
0 Disease progression is defined as any of the following disease statuses as recorded in the FHR: PD orclinical relapse. In the case of missing data, disease progression is defined according to the IMWG criteriaas indicated in Annex 5.
- Relapse is defined as any of the following disease statuses as recorded in the FHR: Relapse from CR, orrelapse from MRD negative.
0 Line oftreatment is defined as one or more cycles of a treatment program. Treatment lines are numberedsuccessively, starting with first treatment line, second treatment line, and further. Where available, theyare defined numerically using the line of treatment variable recorded in the register. If not available inthis way, each new treatment line is defined as a drug regimen that starts following disease progression.In the case of transplantation, tandem transplantation is defined as two transplantations within 6months, whereas multiple single transplants are defined as two transplantations separated by at least a12-months interval.
8.5 Data sources
Data from FHR on MM patients with recordings will be used. The FHR is owned by the Finnish Society ofHematology (FSH). The FHR is a national, population-based register founded in January 2010. Informationconcerning the treatment and treatment responses of patients with haematological disorders are includedin this register, starting from the time of diagnosis and during follow-up. Patients must provide informedconsent (IC) for their data to be recorded into the register and to be available for research purposes. The FHRincludes approximately 1600 MM patients, but it is estimated that currently data including treatment arerecorded for at least 300-400 patients.
8.6 Study size
The population size for the whole study cohort is approximately 1600 MM patients, while the population sizefor the actual study cohort is approximately 300-400 patients. As this is primarily a descriptive study, this
EPID Research Page 18 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 19 of 27
population size is considered sufficient. The MM population in FHR is also considered to be a representative sample of the complete MM population in Finland.
8.7 Data management
The FHR data have been collected from the electronic medical records and are managed by an ICT services company Granitics Ltd. The FHR is responsible for collecting data from the electronic medical records into the database maintained by Granitics.
Contract research organization EPID Research Oy will receive the study data from Granitics and is responsible for data processing and analyses. EPID Research will also perform quality assurance for the received data. Database lock will occur when EPID Research has performed the quality assurance procedures and resolved all potential issues with either Granitics, FHR, or both. The final statistical analyses will start after the database lock.
EPID Research will use R language [9] in data processing, creating the analysis database, and in statistical analyses. All study data, source code of data management, and data analyses are kept for inspection for five years after the end of the study.
The study may be inspected by the sponsor’s independent representatives, steering committee, or by competent authorities.
Access to the study data cannot be given to any third parties, nor may the study data be used for other purposes than prescribed in this protocol. All requests to use the study data for other purposes than those mentioned in this study protocol must be subjected to appropriate data permit processes.
8.8 Data analysis
The principles of the statistical analysis are outlined below. A more detailed SAP will be written separately before any data is being transferred to EPID Research. In the descriptive analyses, continuous variables will be described by mean, standard deviation, median, 25th and 75th percentiles, minimum and maximum. Categorical variables and continuous variables that are also categorised will be described by proportion and frequency in each category. 95% confidence intervals (CIs) will be presented when appropriate.
Potential confounders and effect modifiers
In the analysis of OS and TTNT outcome variables the potential confounding variables include but are not limited to:
• Age, gender, CRAB, ISS-/R-ISS-stage, FISH-test results, type of MM, early progression
8.8.1 Primary objective 1
Patient demographics and disease characteristics will be described separately by the relevant summary statistics at diagnosis, for the whole study cohort and for the actual study cohort.
Treatment patterns and where relevant, disease characteristics, will be described at cohort entry for the actual study cohort and during follow-up. During follow-up, variables will be described at the start and end of each treatment line as relevant and available from the data source.
For the general description, the follow-up variables will be described at the end of follow-up.
8.8.2 Primary objective 2
OS and TTNT (including TTNT1, TTNT2, and further) will be described with the Kaplan-Meier estimator in the actual study cohort population and stratified by patients’ demographic factors, disease characteristics, and
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 lune 2019
population size is considered sufficient. The MM population in FHR is also considered to be a representativesample of the complete MM population in Finland.
8.7 Data management
The FHR data have been collected from the electronic medical records and are managed by an ICT servicescompany Granitics Ltd. The FHR is responsible for collecting data from the electronic medical records intothe database maintained by Granitics.
Contract research organization EPID Research Oy will receive the study data from Granitics and is responsiblefor data processing and analyses. EPID Research will also perform quality assurance for the received data.Database lock will occur when EPID Research has performed the quality assurance procedures and resolvedall potential issues with either Granitics, FHR, or both. The final statistical analyses will start after thedatabase lock.
EPID Research will use R language [9] in data processing, creating the analysis database, and in statisticalanalyses. All study data, source code of data management, and data analyses are kept for inspection for fiveyears after the end of the study.
The study may be inspected by the sponsor’s independent representatives, steering committee, or bycompetent authorities.
Access to the study data cannot be given to any third parties, nor may the study data be used for otherpurposes than prescribed in this protocol. All requests to use the study data for other purposes than thosementioned in this study protocol must be subjected to appropriate data permit processes.
8.8 Data analysis
The principles of the statistical analysis are outlined below. A more detailed SAP will be written separatelybefore any data is being transferred to EPID Research. In the descriptive analyses, continuous variables willbe described by mean, standard deviation, median, 25th and 75th percentiles, minimum and maximum.Categorical variables and continuous variables that are also categorised will be described by proportion andfrequency in each category. 95% confidence intervals (Cls) will be presented when appropriate.
Potential confounders and effect modifiers
In the analysis of OS and TTNT outcome variables the potential confounding variables include but are notlimited to:
0 Age, gender, CRAB, |SS-/R-|SS-stage, FISH-test results, type of MM, early progression
8.8.1 Primary objective 1
Patient demographics and disease characteristics will be described separately by the relevant summarystatistics at diagnosis, for the whole study cohort and for the actual study cohort.
Treatment patterns and where relevant, disease characteristics, will be described at cohort entry for theactual study cohort and during follow-up. During follow-up, variables will be described at the start and endof each treatment line as relevant and available from the data source.
For the general description, the follow-up variables will be described at the end of follow-up.
8.8.2 Primary objective 2
OS and TTNT (including TTNT1, TTNT2, and further) will be described with the Kaplan-Meier estimator in theactual study cohort population and stratified by patients’ demographic factors, disease characteristics, and
EPID Research Page 19 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 20 of 27
types and lines of treatment. These time-to-event outcomes will also be summarized by the relevant statistics among uncensored events. In addition, the proportion of censoring will be reported.
In the analyses of time-to-event outcomes there might be potential immortal time bias in case IC was requested after the start of follow-up. Hence, for each patient the time periods prior to the request of IC will not be considered as a risk-time and will be left-censored. The same will apply in the analyses of the secondary objectives as well.
8.8.3 Secondary objective 1
Factors associated with treatment duration (TTNT) and OS will be identified using a multivariate Cox regression model. The previously defined potential confounders and effect modifiers will be included in all models. In addition, additional demographic variables, disease characteristics, and treatment patterns will be added into the models using a variable selection procedure. The detailed variable selection procedure will be defined in the SAP.
In the treatment selection analyses, a specified treatment type will be defined as a binary outcome variable that indicates if a patient received the specified treatment at the start of the treatment line or not (1 meaning that the patient received the treatment and 0 that the patient did not receive the specified treatment). Thereafter, factors associated with treatment selection will be identified using a multivariate logistic model in a similar manner as described for TTNT and OS / Cox model above.
8.8.4 Secondary objective 2
Patients at low-, standard-, and high-risk will be identified at diagnosis and divided into groups based on the ISS/R-ISS categorisation (shown in Annex 2). Patients who did not receive the pre-specified treatments (e.g. transplant, duplet or triplet therapies) as the 1st, 2nd, 3rd, 4th, >4th line treatment will be identified and followed-up at the start of each treatment line (1st, 2nd, 3rd, 4th, >4th line). Patients with short treatment duration will be defined at the end of a treatment line (short duration of 1st line treatment, short duration of 2nd line treatment and so on) and followed-up after the end of the treatment line with short duration.
After identifying the above subpopulations, they will be described similarly as described in Primary objective 1. OS, TTNT (including TTNT1, TTNT2, and further) will be described with the Kaplan-Meier estimator in these subpopulations.
8.8.5 Sensitivity analyses
The representativeness of the actual study cohort in the FHR will be investigated by presenting baseline summary statistics of the whole study cohort. These baseline statistics will be compared with the actual study cohort. Comparisons will concentrate on demographic variables and disease characteristics as available in the whole study cohort.
As described in Section 8.4, PD is recorded in the FHR and missing data will be completed according to the IMWG criteria. The number of original PD events recorded in the FHR and the number of PD events found only using the IMWG criteria will be reported.
As described in Section 8.4, for patients whose treatment line is not recorded in the FHR, the start of each treatment line will be defined as a drug regimen following disease progression. In a sensitivity analysis, treatment line will be defined in the latter way for all patients and compared to the original treatment line recorded in the FHR.
Sensitivity analyses will be performed by excluding variables with a high proportion of missingness from statistical models, as described in Section 8.8.7.
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
types and lines oftreatment. These time-to-event outcomes will also be summarized by the relevant statisticsamong uncensored events. In addition, the proportion of censoring will be reported.
In the analyses of time-to-event outcomes there might be potential immortal time bias in case IC wasrequested after the start of follow-up. Hence, for each patient the time periods prior to the request of IC willnot be considered as a risk-time and will be left-censored. The same will apply in the analyses of thesecondary objectives as well.
8.8.3 Secondary objective 1
Factors associated with treatment duration (TTNT) and OS will be identified using a multivariate Coxregression model. The previously defined potential confounders and effect modifiers will be included in allmodels. In addition, additional demographic variables, disease characteristics, and treatment patterns willbe added into the models using a variable selection procedure. The detailed variable selection procedure willbe defined in the SAP.
In the treatment selection analyses, a specified treatment type will be defined as a binary outcome variablethat indicates if a patient received the specified treatment at the start of the treatment line or not (1 meaningthat the patient received the treatment and 0 that the patient did not receive the specified treatment).Thereafter, factors associated with treatment selection will be identified using a multivariate logistic modelin a similar manner as described for TTNT and OS / Cox model above.
8.8.4 Secondary objective 2
Patients at low-, standard-, and high-risk will be identified at diagnosis and divided into groups based on theISS/R-ISS categorisation (shown in Annex 2). Patients who did not receive the pre-specified treatments (e.g.transplant, duplet or triplet therapies) as the 1“, 2nd, 3rd, 4th, >4th line treatment will be identified andfollowed-up at the start of each treatment line (1“, 2nd, 3rd, 4th, >4th line). Patients with short treatmentduration will be defined at the end of a treatment line (short duration of 1St line treatment, short duration of2"“l line treatment and so on) and followed-up after the end of the treatment line with short duration.
After identifying the above subpopulations, they will be described similarly as described in Primary objective1. OS, TTNT (including TTNT1, TTNT2, and further) will be described with the Kaplan-Meier estimator in thesesubpopulations.
8.8.5 Sensitivity analyses
The representativeness of the actual study cohort in the FHR will be investigated by presenting baselinesummary statistics ofthe whole study cohort. These baseline statistics will be compared with the actual studycohort. Comparisons will concentrate on demographic variables and disease characteristics as available inthe whole study cohort.
As described in Section 8.4, PD is recorded in the FHR and missing data will be completed according to theIMWG criteria. The number of original PD events recorded in the FHR and the number of PD events foundonly using the IMWG criteria will be reported.
As described in Section 8.4, for patients whose treatment line is not recorded in the FHR, the start of eachtreatment line will be defined as a drug regimen following disease progression. In a sensitivity analysis,treatment line will be defined in the latter way for all patients and compared to the original treatment linerecorded in the FHR.
Sensitivity analyses will be performed by excluding variables with a high proportion of missingness fromstatistical models, as described in Section 8.8.7.
EPID Research Page 20 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 21 of 27
8.8.6 Statistical analysis plan
EPID Research will produce a separate SAP including detailed description of statistical analyses and the corresponding outputs before undertaking the analyses.
8.8.7 Missing data
If a given variable is totally or systematically missing from a database, it is excluded from the analyses. If a variable is missing for only some of the patients or arbitrarily missing, a missing data category will be added and used in the analyses. However, in case a variable with a high proportion of missingness is included in an analysis, a sensitivity analysis will be conducted without having that variable in the model. If a variable is missing from the database but equivalent information can be inferred using available variables, this will be specified and performed.
8.9 Quality control
The study will be conducted as specified in this protocol. All revisions to the protocol must be approved by the principal investigator, sponsor, and co-authors of the study. All changes to the protocol shall be properly documented as protocol amendments and when necessary such protocol amendments are delivered to FHR.
The study protocol has been written by following the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (ENCePP) Code of Conduct [10] and the Guideline for Good Pharmacoepidemiology Practices (GPP) [11] by the International Society for Pharmacoepidemiology (ISPE). The study protocol and as well as results will be published in EU PAS register maintained by EMA.
All study data, source code of data management, and data analyses will be retained for five years after the end of the study and then destroyed. As the register holder of the study register EPID Research is responsible of archiving and destroying the data. Secure archives will be maintained for the orderly storage and retrieval of all study related material on the EPID Research server. An index shall be prepared to identify the archived contents and their locations. Access to the archives will be controlled and limited to authorised personnel only.
Due to the study type (register study using administrative databases) on-site monitoring will not be performed.
8.10 Limitations of the research methods
8.10.1 Data source
This study is based on data collected from the FHR, which covers the whole of Finland and has an accuracy considered appropriate for scientific research. It is expected that the majority of all MM diagnoses have been recorded but that comprehensive coverage is available for approximately 25% of the recorded MM diagnoses and may differ based on region. However, it must be considered that data is recorded by different individuals and therefore there may be variability within variables for which there is no clear clinical definition. In some cases, some data may be missing from individual patients but this may be verified based on other existing variables.
Data which would be relevant for the objectives of this study but are completely missing overall from the FHR include:
• Treating hospital district (for determining distance between place of residence and treating hospital) • History data (prior to date of diagnosis) • Reason for loss to follow-up • Reason for treatment discontinuation
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
8.8.6 Statistical analysis plan
EPID Research will produce a separate SAP including detailed description of statistical analyses and thecorresponding outputs before undertaking the analyses.
8.8.7 Missing data
If a given variable is totally or systematically missing from a database, it is excluded from the analyses. If avariable is missing for only some of the patients or arbitrarily missing, a missing data category will be addedand used in the analyses. However, in case a variable with a high proportion of missingness is included in ananalysis, a sensitivity analysis will be conducted without having that variable in the model. If a variable ismissing from the database but equivalent information can be inferred using available variables, this will bespecified and performed.
8.9 Quality control
The study will be conducted as specified in this protocol. A” revisions to the protocol must be approved bythe principal investigator, sponsor, and co-authors of the study. All changes to the protocol shall be properlydocumented as protocol amendments and when necessary such protocol amendments are delivered to FHR.
The study protocol has been written by following the European Network of Centres forPharmacoepidemiology and Pharmacovigilance (ENCePP) Code of Conduct [10] and the Guideline for GoodPharmacoepidemiology Practices (GPP) [11] by the International Society for Pharmacoepidemiology (ISPE).The study protocol and as well as results will be published in EU PAS register maintained by EMA.
A” study data, source code of data management, and data analyses will be retained for five years after theend of the study and then destroyed. As the register holder of the study register EPID Research is responsibleof archiving and destroying the data. Secure archives will be maintained for the orderly storage and retrievalof all study related material on the EPID Research server. An index shall be prepared to identify the archivedcontents and their locations. Access to the archives will be controlled and limited to authorised personnelonly.
Due to the study type (register study using administrative databases) on-site monitoring will not beperformed.
8.10 Limitations of the research methods
8.10.1 Data source
This study is based on data collected from the FHR, which covers the whole of Finland and has an accuracyconsidered appropriate for scientific research. It is expected that the majority of all MM diagnoses have beenrecorded but that comprehensive coverage is available for approximately 25% of the recorded MM diagnosesand may differ based on region. However, it must be considered that data is recorded by different individualsand therefore there may be variability within variables for which there is no clear clinical definition. In somecases, some data may be missing from individual patients but this may be verified based on other existingvariables.
Data which would be relevant for the objectives of this study but are completely missing overall from theFHR include:
Treating hospital district (for determining distance between place of residence and treating hospital)History data (prior to date of diagnosis)Reason for loss to follow-upReason for treatment discontinuation
EPID Research Page 21 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 22 of 27
Data relevant to the objectives of this study that may be incompletely recorded in the FHR include:
• Line of treatment • Date of end of treatment • LDH
For the incompletely recorded data, other variables may be used to supplement the missing information.
Since as date of end of treatment and clear denotation of progression is likely missing from the register, progression-free survival (PFS) cannot be calculated. In this case, TTNT will be used instead.
As the study period ends in 31 December 2017 the reporting delay of the FHR will not affect study outcomes.
8.10.2 Selection bias and study power
This study will also characterize treatment selection. Treatment selection may be based on age or existing medical factors and therefore co-morbidities will be analysed. Similarly, due to confounding by indication it may not be possible to compare the efficacy of different treatments.
This is a small retrospective study with expected data recorded for at least 300-400 MM patients in the actual study cohort. This is sufficient for descriptive analyses but may in some cases result in limited study power when comparing different groups.
Risk-stratification using the R-ISS is based in part on FISH results. FISH results from before 2011-2012 are not fully comparable with those after 2012. Therefore, it may not be possible to compare risk-stratified groups of patients from before and after 2012.
8.10.3 Immortal time bias
In case the IC was requested after diagnosis, the time period from diagnosis to the date of IC is the immortal time. The immortal time is handled in survival analyses as left-censoring.
9 Informed consent
Since this is a retrospective analysis on data obtained from the FHR, using epidemiological methods for analysis based on data selected from the abovementioned sources, the patients will not be asked for their IC for this specific study. However, the FHR asks patients for their IC before any patient data is entered into the FHR. This IC indicates that data from the register may be used for collaborative research projects with national study groups and commercial organisations.
10 Protection of human subjects
This is a fully register-based study. The study does not affect the treatment of the patients, and the patients will not be contacted in any phase of the study. The study is conducted by following the ENCePP code of conduct [10] as well as the Guidelines for GPP [11].
EPID Research will receive pseudonymised data including study identification numbers (SIDs) only. EPID Research employees have undertaken professional secrecy and are aware of their concern with the local legislation: Act on the Openness of Government Activities 621/1999 (based on which the data can be received from the original register holders). The study register is formed on the basis of the Data Protection Act (1050/2018). The implications of the General Data Protection Regulation (EU) 2016/679 on the national legislations, during the course of the study, will be considered.
The sponsor will not have access to the patient level data at any time of the study. Sponsor’s representation in the steering committee does not repeal this principle.
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
Data relevant to the objectives of this study that may be incompletely recorded in the FHR include:
0 Line of treatment0 Date of end of treatment0 LDH
For the incompletely recorded data, other variables may be used to supplement the missing information.
Since as date of end of treatment and clear denotation of progression is likely missing from the register,progression-free survival (PFS) cannot be calculated. In this case, TTNT will be used instead.
As the study period ends in 31 December 2017 the reporting delay of the FHR will not affect study outcomes.
8.10.2 Selection bias and study power
This study will also characterize treatment selection. Treatment selection may be based on age or existingmedical factors and therefore co-morbidities will be analysed. Similarly, due to confounding by indication itmay not be possible to compare the efficacy of different treatments.
This is a small retrospective study with expected data recorded for at least 300-400 MM patients in the actualstudy cohort. This is sufficient for descriptive analyses but may in some cases result in limited study powerwhen comparing different groups.
Risk-stratification using the R-ISS is based in part on FISH results. FISH results from before 2011-2012 are notfully comparable with those after 2012. Therefore, it may not be possible to compare risk-stratified groupsof patients from before and after 2012.
8.10.3 Immortal time bias
In case the IC was requested after diagnosis, the time period from diagnosis to the date of IC is the immortaltime. The immortal time is handled in survival analyses as left-censoring.
9 Informed consent
Since this is a retrospective analysis on data obtained from the FHR, using epidemiological methods foranalysis based on data selected from the abovementioned sources, the patients will not be asked for their ICfor this specific study. However, the FHR asks patients for their IC before any patient data is entered into theFHR. This IC indicates that data from the register may be used for collaborative research projects withnational study groups and commercial organisations.
10 Protection of human subjects
This is a fully register-based study. The study does not affect the treatment of the patients, and the patientswill not be contacted in any phase of the study. The study is conducted by following the ENCePP code ofconduct [10] as well as the Guidelines for GPP [11].
EPID Research will receive pseudonymised data including study identification numbers (SIDs) only. EPIDResearch employees have undertaken professional secrecy and are aware of their concern with the locallegislation: Act on the Openness of Government Activities 621/1999 (based on which the data can be receivedfrom the original register holders). The study register is formed on the basis of the Data Protection Act(1050/2018). The implications of the General Data Protection Regulation (EU) 2016/679 on the nationallegislations, during the course of the study, will be considered.
The sponsor will not have access to the patient level data at any time of the study. Sponsor’s representationin the steering committee does not repeal this principle.
EPID Research Page 22 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 23 of 27
The protocol will be subjected to the Ethics Committee of the Hospital District of Helsinki and Uusimaa for review and approval. Register notification of the forming study register will be sent to the Office of the Data Protection Ombudsman.
11 Management and reporting of adverse events/adverse reactions
The nature of this non-interventional study does not meet the criteria for adverse event reporting [12].
12 Plans for disseminating and communicating study results
The principal investigator together with the co-investigators will write a study report. This report will be delivered to the sponsor and members of the steering committee.
Within three months following the final study report, at minimum an abstract of the study findings will be provided through the EU PAS register. According to the ENCePP Code of Conduct, the principal investigator is responsible for publication of the results. The main results of the study will be published, whether positive or negative. In no way shall the interpretation and presentation of the results be aimed towards any commercial, financial or personal interests.
Based on the study report, the principal investigator and co-investigators with co-authors (members of the steering committee and possible other contributors approved by the steering committee) will prepare (a) scientific manuscript(s) for academic publication. The steering committee decides the publication forums.
The sponsor is entitled to view the final results prior to submission for publication. The sponsor also has the right to comment the results and interpretations thereof. This must be done without unjustifiably delaying the publication. In this particular study the commenting time for the sponsor during the review rounds is agreed to be maximum of one month. Possible changes in the presentations must be based on scientific reasons only. The steering committee is free not to take the comments of the sponsor into account.
The principal investigator and the sponsor are committed to ensuring that authorship for all publications should comply with the criteria defined by the International Committee of Medical Journal Editors, ICMJE. There it is stated that each author should have participated sufficiently in the work to take public responsibility for the content [13]. These conditions apply equally to external investigators and to employees of the sponsor.
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
The protocol will be subjected to the Ethics Committee of the Hospital District of Helsinki and Uusimaa forreview and approval. Register notification of the forming study register will be sent to the Office of the DataProtection Ombudsman.
11 Management and reporting of adverse events/adverse reactions
The nature of this non-interventional study does not meet the criteria for adverse event reporting [12].
12 Plans for disseminating and communicating study results
The principal investigator together with the co-investigators will write a study report. This report will bedelivered to the sponsor and members of the steering committee.
Within three months following the final study report, at minimum an abstract of the study findings will beprovided through the EU PAS register. According to the ENCePP Code of Conduct, the principal investigatoris responsible for publication of the results. The main results of the study will be published, whether positiveor negative. In no way shall the interpretation and presentation of the results be aimed towards anycommercial, financial or personal interests.
Based on the study report, the principal investigator and co-investigators with co-authors (members of thesteering committee and possible other contributors approved by the steering committee) will prepare (a)scientific manuscript(s) for academic publication. The steering committee decides the publication forums.
The sponsor is entitled to view the final results prior to submission for publication. The sponsor also has theright to comment the results and interpretations thereof. This must be done without unjustifiably delayingthe publication. In this particular study the commenting time for the sponsor during the review rounds isagreed to be maximum of one month. Possible changes in the presentations must be based on scientificreasons only. The steering committee is free not to take the comments of the sponsor into account.
The principal investigator and the sponsor are committed to ensuring that authorship for all publicationsshould comply with the criteria defined by the International Committee of Medical Journal Editors, ICMJE.There it is stated that each author should have participated sufficiently in the work to take publicresponsibility for the content [13]. These conditions apply equally to external investigators and to employeesof the sponsor.
EPID Research Page 23 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 24 of 27
13 References
1 Palumbo A, Anderson K. Multiple Myeloma. New England Journal of Medicine 2011;364:1046–60. doi:10.1056/NEJMra1011442
2 Bergin K, McQuilten Z, Moore E, et al. Myeloma in the Real World: What Is Really Happening? Clinical Lymphoma, Myeloma and Leukemia 2017;17:133–144.e1. doi:10.1016/j.clml.2016.12.002
3 Dimopoulos MA, Richardson PG, Moreau P, et al. Current treatment landscape for relapsed and/or refractory multiple myeloma. Nat Rev Clin Oncol 2015;12:42–54. doi:10.1038/nrclinonc.2014.200
4 Rajkumar SV. Updated Diagnostic Criteria and Staging System for Multiple Myeloma. Am Soc Clin Oncol Educ Book 2016;35:e418-423. doi:10.14694/EDBK_159009
5 Roy V, Greipp PR. Staging of Multiple Myeloma. In: Gertz MA, Rajkumar SV, eds. Multiple Myeloma. Springer New York 2014. 47–53. doi:10.1007/978-1-4614-8520-9_5
6 Palumbo A, Avet-Loiseau H, Oliva S, et al. Revised International Staging System for Multiple Myeloma: A Report From International Myeloma Working Group. J Clin Oncol 2015;33:2863–9. doi:10.1200/JCO.2015.61.2267
7 Hoito | SHY. Multiple Myeloma: Care. http://www.hematology.fi/fi/hoito-ohjeet/veritaudit/plasmasolutaudit/myelooma/hoito (accessed 25 Apr 2017).
8 Morgan GJ, Walker BA, Davies FE. The genetic architecture of multiple myeloma. Nat Rev Cancer 2012;12:335–48. doi:10.1038/nrc3257
9 R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL http://www.R-project.org/
10 European Medicines Agency. The ENCePP Code of Conduct, Revision 3 editorial amendment. 2016. http://www.encepp.eu/code_of_conduct/documents/ENCePPCodeofConduct_Rev3amend.pdf.
11 Public Policy Committee IS of P. Guidelines for good pharmacoepidemiology practice (GPP). Pharmacoepidemiol Drug Saf 2016;25:2–10. doi:10.1002/pds.3891
12 European Medicines Agency, Heads of Medicines Agencies. Guideline on good pharmacovigilance practices (GVP) Module VI – Management and reporting of adverse reactions to medicinal products (Rev 1). http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2014/09/WC500172402.pdf (accessed 14 Oct 2016).
13 ICMJE Recommendations. Defining the Role of Authors and Contributors. http://www.icmje.org/recommendations/browse/roles-and-responsibilities/defining-the-role-of-authors-and-contributors.html (accessed 5 Oct 2016).
14 Greipp PR, Miguel JS, Durie BGM, et al. International Staging System for Multiple Myeloma. JCO 2005;23:3412–20. doi:10.1200/JCO.2005.04.242
15 Durie BGM, Salmon SE. A clinical staging system for multiple myeloma correlation of measured myeloma cell mass with presenting clinical features, response to treatment, and survival. Cancer 1975;36:842–54. doi:10.1002/1097-0142(197509)36:3<842::AID-CNCR2820360303>3.0.CO;2-U
16 Rajkumar SV, Harousseau J-L, Durie B, et al. Consensus recommendations for the uniform reporting of clinical trials: report of the International Myeloma Workshop Consensus Panel 1. Blood 2011;117:4691–5. doi:10.1182/blood-2010-10-299487
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
13 References
1
9
10
11
12
13
14
15
16
Palumbo A, Anderson K. Multiple Myeloma. New England Journal of Medicine 2011;364:1046—60.doi:10.1056/NEJMra1011442
Bergin K, McQuilten Z, Moore E, et al. Myeloma in the Real World: What Is Really Happening? ClinicalLymphoma, Myeloma and Leukemia 2017;17:133—144.e1. doi:10.1016/j.clml.2016.12.002
Dimopoulos MA, Richardson PG, Moreau P, et al. Current treatment landscape for relapsed and/orrefractory multiple myeloma. Nat Rev Clin Oncol 2015;12:42—54. doi:10.1038/nrclinonc.2014.200
Rajkumar SV. Updated Diagnostic Criteria and Staging System for Multiple Myeloma. Am Soc Clin OncolEduc Book 2016;352e418-423. doi:10.14694/EDBK_159009
Roy V, Greipp PR. Staging of Multiple Myeloma. In: Gertz MA, Rajkumar SV, eds. Multiple Myeloma.Springer New York 2014. 47—53. doi:10.1007/978-1-4614-8520-9_5
Palumbo A, Avet-Loiseau H, Oliva S, et al. Revised International Staging System for Multiple Myeloma: AReport From International Myeloma Working Group. J Clin Oncol 2015;33:2863—9.doi:10.1200/JCO.2015.61.2267
Hoito | SHY. Multiple Myeloma: Care. http://www.hematology.fi/fi/hoito-ohjeet/veritaudit/plasmasolutaudit/myelooma/hoito (accessed 25 Apr 2017).
Morgan GJ, Walker BA, Davies FE. The genetic architecture of multiple myeloma. Nat Rev Cancer2012;12:335—48. doi:10.1038/nrc3257
R Core Team. R: A language and environment for statistical computing. R Foundation for StatisticalComputing, Vienna, Austria. URL http://www.R-project.org/
European Medicines Agency. The ENCePP Code of Conduct, Revision 3 editorial amendment. 2016.http://www.encepp.eu/code_of_conduct/documents/ENCePPCodeofConduct_Rev3amend.pdf.
Public Policy Committee IS of P. Guidelines for good pharmacoepidemiology practice (GPP).Pharmacoepidemiol Drug Saf 2016;25:2—10. doi:10.1002/pds.3891
European Medicines Agency, Heads of Medicines Agencies. Guideline on good pharmacovigilancepractices (GVP) Module VI — Management and reporting of adverse reactions to medicinal products (Rev1).http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2014/09/WC500172402.pdf (accessed 14 Oct 2016).
ICMJE Recommendations. Defining the Role of Authors and Contributors.http://www.icmje.org/recommendations/browse/roles-and-responsibilities/defining-the-roIe-of-authors-and-contributors.htm| (accessed 5 Oct 2016).
Greipp PR, Miguel JS, Durie BGM, et al. International Staging System for Multiple Myeloma. JCO2005;23:3412—20. doi:10.1200/JCO.2005.04.242
Durie BGM, Salmon SE. A clinical staging system for multiple myeloma correlation of measured myelomacell mass with presenting clinical features, response to treatment, and survival. Cancer 1975;36:842—54.doi:10.1002/1097-0142(197509)36:3<842::AID-CNCR2820360303>3.0.CO;2-U
Rajkumar SV, Harousseau J-L, Durie B, et al. Consensus recommendations for the uniform reporting ofclinical trials: report of the International Myeloma Workshop Consensus Panel 1. Blood 2011;117:4691—5. doi:10.1182/blood-2010-10-299487
EPID Research Page 24 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 25 of 27
Annex 1. List of stand alone documents
• ENCePP checklist for study protocols.
Annex 2. ISS and R-ISS
ISS for MM
Stage Criteria Median survival, months
I • Serum β2-microglobulin <3.5 mg/L
• Serum albumin ≥3.5 g/dL 62
II Not fitting stage I or III 44
III • Serum β2-microglobulin ≥5.5 mg/L 29
There are two categories of stage II: serum β2-microglobulin <3.5 mg/L but serum albumin <3.5 g/dL; or serum β2microglobulin 3.5 to <5.5 mg/L irrespective of the serum albumin level. Source: [14]
Revised-ISS for MM
Stage Criteria 5-year PFS
rate, %
5-year OS
rate, %
Median OS,
months
I • Original ISS stage I; and
• Standard-risk* CAs by iFISH; and
• Normal LDH
55% 82% Not reached
II Not fitting stage I or III 36% 62% 83
III • Original ISS stage III; and
• High-risk* CAs by iFISH; and/or
• High LDH
24% 40% 43
*High-risk chromosomal abnormalities (CAs) include the presence of deletion [del(17p)] and/or translocation [t(4;14)] and/or translocation [t(14;16)], whereas all other CAs are considered standard-risk. Source: [6]
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
Annex 1. List of stand alone documents
0 ENCePP checklist for study protocols.
Annex 2. ISS and R-ISS
ISS for MM
Stage Criteria Median survival, months| 0 Serum Bz-microglobulin <3.5 mg/L 52
0 Serum albumin 23.5 g/dL
l| Not fitting stage I or III 44
m 0 Serum Bz-microglobulin 25.5 mg/L 29
There are two categories of stage II: serum Bz-microglobulin <3.5 mg/L but serum albumin <3.5 g/dL; or serumBz-microglobulin 3.5 to <5.5 mg/L irrespective of the serum albumin level.Source: [14]
Revised-ISS for MM
| 0 Original ISS stage I; and 55% 82% Not reached0 Standard-risk* CAs by iFISH; and0 Normal LDH
ll NOt fitting stage I or III 36% 62% 83
Ill 0 Original ISS stage III; and 24% 40% 43o High-risk* CAs by iFISH; and/or. High LDH
*High-risk chromosomal abnormalities (CAs) include the presence of deletion [de|(17p)] and/or translocation [t(4;14)] and/ortranslocation [t(14;16)], whereas all other CAs are considered standard-risk.Source: [6]
EPID Research Page 25 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 26 of 27
Annex 3. Finnish national guidelines for MM treatment
Figure 2. Finnish national guidelines for MM treatment, divided along the type by patient age and along the side by line of treatment.
The following abbreviations are used above: VCD, bortezomib + cyclophosphamide + dexamethasone; VD, bortezomib + dexamethasone; VTD, bortezomib + thalidomide + dexamethasone; LenDex, lenalidomide + dexamethasone; VTD-PACE, bortezomib + lenalidomide + dexamethasone + cisplatin + doxorubicin + cyclophosphamide + etoposide; VMP, bortezomib + melphalan + prednisone; MP, melphalan + prednisone; CP, cyclophosphamide + prednisone; V, bortezomib; D, dexamethasone.
Source: [7]
Annex 4. Definitions of patient populations
IMWG definitions of MM patient populations.
Category Definition
Primary refractory multiple myeloma Non-responsive patients who have never achieved MR or better
with no significant change in M-component concentration and no
evidence of clinical progression
Refractory multiple myeloma Non-responsive while on primary or salvage* therapy or progress
within 60 days of last therapy
Relapsed multiple myeloma Previously-treated myeloma that progresses and requires the
initation of salvage* therapy but does not meet criteria for either
primary refractory MM or RRMM
Relapsed and refractory multiple myeloma
(RRMM)
Non-responsive while on salvage* therapy, or progress within 60
days of last therapy in patients who have achieved MR or better
at some point previously before, then progress in their disease
course
Where possible, additional qualifiers that describe the specific population, for example “relapsed and refractory to
immunomodulatory therapy”, should be included.
*Salvage, or rescue, therapy is a form of treatment provided to patients who have relapse following ASCT, with primary
progressive disease following ASCT, or who are ineligible for ASCT following initial induction therapy.
Source: [16]
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
Annex 3. Finnish national guidelines for MM treatmentFigure 2. Finnish national guidelines for MM treatment, divided along the type by patient age and along the side byline of treatment.
Age 1 :r 65-?!) years :- 65-70 yearsCencliticin " 55'?” “a” healthy frail
— ycn n VMPE' 34 Eggs [s9 cycles nr 12 months, as daysfcycle) MPAutolugcius E {21 dawcycl-El [+5 weeks uftreatment cycles}
First stem cell 6) = LenDex Q)transplant E VTD/LenDex! 18—day cycle, 13 mnnths or until pros resslnn
MEET) D VTD-PACE CFi VD (C: Hweek; P: every other day]
if _ 3-9 cycles or 12 menths, 35 claysfcycle
E | WP15.g | use {low dose)E Later Repeat transplantation I V +f- doxorubicin {low dose)
3 I Len+D {low dose)
| CF
I L Try new cembinatien treatments, consider health status
I‘ VI Repeat firsttreatment
The following abbreviations are used above: VCD, bortezomib + cyclophosphamide + dexamethasone; VD, bortezomib +dexamethasone; VTD, bortezomib + thalidomide + dexamethasone; LenDex, lenalidomide + dexamethasone,- VTD-PACE,bortezomib + lenalidomide + dexamethasone + cisplatin + doxorubicin + cyclophosphamide + etoposide; VMP, bortezomib +melphalan + prednisone; MP, melphalan + prednisone; CP, cyclophosphamide + prednisone; V, bortezomib; D,dexamethasone.Source: [7]
Annex 4. Definitions of patient populations
IMWG definitions of MM patient populations.Category
v
ary refractory multiple myelomaDefinition
Non-responsive patients who have never achieved MR orwith no significant change in M-component concentration aevidence of clinical progression
Refractory multiple myeloma Non-responsive while on primary or salvage* therapy or progresswithin 60 days of last therapy
sed multiple myeloma Previously-treated myeloma that progresses and requireinitation of salvage* therapy but does not meet criteria forprimary refractory MM or RRMM
Relapsed and refractory multiple myeloma(RRMM)
Non-responsive while on salvage* therapy, or progress within 60days of last therapy in patients who have achieved MR or betterat some point previously before, then progress in their diseasecourse
Where possible, additional qualifiers that describeimmunomodulatory therapy”, should be included.
the specific population, for example ”relapsed and refractory to
*Salvage, or rescue, therapy is a form of treatment provided to patients who have relapse following ASCT, with primaryprogressive disease following ASCT, or who are ineligible for ASCT following initial induction therapy.Source: [16]
EPID Research Page 26 of 27

Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
EPID Research Page 27 of 27
Annex 5. Definitions of disease status
IMWG definitions of disease status.
Disease status Definition
CR* • Negative immunofixation of serum and urine, and
• Disappearance of any soft tissue plasmacytomas, and
• < 5% plasma cells in bone marrow
sCR • CR as defined, and
• Normal free light chain ratio, and
• Absence of clonal plasma cells by immunohistochemistry or 2- to 4-color flow cytometry
VGPR* • Serum and urine M-component detectable by immunofixation but not on electroporesis,
or
• 90% reduction in serum M-component and urine M-component < 100 mg/24 h
PR • 50% reduction of serum M-component and 90% reduction in 24-h urine M-component
or to < 200 mg/24 h
• Where M-component and serum free light assay not measurable, 50% reduction in bone
marrow plasma cells (provided baseline percentage 30%)
• If present at baseline, also 50% reduction in the size of soft tissue plasmacytomas
SD Not meeting criteria for CR, VGPR, PR, or PD
PD** • Increase of 25% from baseline in serum M-component (absolute increase 0.5 g/dL)
• Increase of 25% from baseline in urine M-component (absolute increase 200 mg/24 h)
• For those with measurable serum and urine M-protein levels, the difference between
involved and uninvolved free light chain levels must have absolute increase > 10 mg/dL
• Absolute bone marrow plasma cell percentage 10%
• Definite development of new bone lesions, soft tissue plasmacytomas, or increase in size
of existing bone lesions, soft tissue plasmacytomas
• Development of hypercalcaemia attributed solely to multiple myeloma
MR† • 25% but 49% reduction of serum M-component, and
• Reduction in 24-h urine M-component by 50-89%, and
• If present at baseline, 25-49% reduction in the size of soft tissue plasmacytomas, and
• No increase in size or number of lytic bone lesions
Clinical relapse • Development of new soft tissue plasmacytomas or bone lesions on skeletal survey, MRI, or
other imaging, and/or
• Definite increase in the size of existing plasmacytomas or bone lesions, as defined as a 50%
and at least 1 cm increase as measured serially by the sum of products of the cross-
diameters of the measurable lesion, and/or
• Hypercalcaemia (> 11.5 mg/dL; > 2.875 mM/L)
• Decrease in haemoglobin of more than 2 g/dL (1.25 mM) or to less than 10 g/dL, and/or
• Rise in serum creatinine by 2 mg/dL ( 177 mM/L)
• Hyperviscosity
*For CR and VGPR in patients for whom the only measurable disease is by serum free light chain levels, CR indicates a normal
free light chain ration (0.26 to 1.65) in addition to other critera. VGPR requires a > 90% decrease in the difference between
involved and uninvolved free light chain levels.
**For PD, bone marrow criteria are only to be used for those patients without measurable disease by M-component and free
light chain levels. Baseline is considered to be the lowest response value and does not need to be a confirmed value.
†For patients with RRMM
Source: [16]
Pharmacoepidemiological study protocol ER-9542 Version 2.0 13 June 2019
Annex 5. Definitions of disease status
IMWG definitions of disease status.
DefinitionDisease status
sCR
PR
PD**
Clinical relapse
Negative immunofixation of serum and urine, andDisappearance of any soft tissue plasmacytomas, a< 5% plasma cells in bone marrowCR as defined, andNormal free light chain ratio, andAbsence of clonal plasma cells by immunohistochemistry or 2- to 4-color flow cytometrySerum and urine M-component detectable by immunofixation but not on electroor2 90% reduction in serum M-component and urine M-component < 100 mg/24 h2 50% reduction of serum M-component and 2 90% reduction in 24-h urine M-componentor to < 200 mg/24 hWhere M-component and serum free light assay not measurable, 2 50% reduction in bonemarrow plasma cells (provided baseline percentage 2 30%)If present at baseline, also 2 50% reduction in the size of soft tissue plasmacytomas
Increase of 2 25% from baseline in serum M-component (absolute increase 2 0.5 g/dL)Increase of 2 25% from baseline in urine M-component (absolute increase 2 200 mg/24 h)For those with measurable serum and urine M-protein levels, the difference betweeninvolved and uninvolved free light chain levels must have absolute increase > 10 mg/dLAbsolute bone marrow plasma cell percentage 2 10%Definite development of new bone lesions, soft tissue plasmacytomas, or increase in sizeof existing bone lesions, soft tissue plasmacytomasDevelopment of hypercalcaemia attributed solely to multiple myeloma2 25% but S 49% reduction of serum M-component, andReduction in 24-h urine M-component by 50-89%, andIf present at baseline, 25-49% reduction in the size of soft tissue plasmacytomas, andNo increase in size or number of lytic bone lesionsDevelopment of new soft tissue plasmacytomas or bone lesions on skeletal survey, MRI, orother imaging, and/orDefinite increase in the size of existing plasmacytomas or bone lesions, as defined as a 50%and at least 1 cm increase as measured serially by the sum of products of the cross-diameters of the measurable lesion, and/orHypercalcaemia (> 11.5 mg/dL; > 2.875 mM/L)Decrease in haemoglobin of more than 2 g/dL (1.25 mM) or to less than 10 g/dL, and/orRise in serum creatinine by 2 2 mg/dL (2 177 mM/L)Hyperviscosity
*For CR and VGPR in patients for whom the only measurable disease is by serum free light chain levels, CR indicates a normalfree light chain ration (0.26 to 1.65) in addition to other critera. VGPR requires a > 90% decrease in the difference betweeninvolved and uninvolved free light chain levels.**For PD, bone marrow criteria are only to be used for those patients without measurable disease by M-component and freelight chain levels. Baseline is considered to be the lowest response value and does not need to be a confirmed value.fFor patients with RRMMSource: [16]
EPID Research Page 27 of 27