Angola - Country Data Profile on the Pharmaceutical Situation in the ...

Pharmaceutical Situation in Barbados
World Health Organization (WHO)
LEVEL II Health Facility and Household Surveys
Supported by:
February, 2011

PAHO HQ Library Cataloguing-in-Publication
Pan American Health Organization, Ministry of Health of Barbados
“ PHARMACEUTICAL SITUATION IN BARBADOS: World Health Organization (WHO) LEVEL II Health Facility and Household Surveys”.
Washington, D. C.: PAHO, © 2011.
ISBN 978-92-75-13158-9
I. Title
1. ECONOMICS, PHARMACEUTICAL
2. PHARMACEUTICAL SERVICES - standards
3. DRUG AND NARCOTIC CONTROL - economic
4. LEGISLATION, DRUG - organization & administration
5. HEALTH SURVEILLANCE
6. WORLD HEALTH ORGANIZATION
NLM QV 736.DB34
The Pan American Health Organization welcomes requests for permission to reproduce or
translate its publications, in part or in full. Applications and inquiries should be addressed to Editorial
Services, Area of Knowledge Management and Communications (KMC), Pan American Health Organization, Washington, D.C., U.S.A., which will be glad to provide the latest information on any
changes made to the text, plans for new editions, and reprints and translations already available.
©Pan American Health Organization, 2011
Publications of the Pan American Health Organization enjoy copyright protection in accordance
with the provisions of Protocol 2 of the Universal Copyright Convention. All rights are reserved. The designations employed and the presentation of the material in this publication do not imply
the expression of any opinion whatsoever on the part of the Secretariat of the Pan American Health Organization concerning the status of any country, territory, city or area or of its authorities, or
concerning the delimitation of its frontiers or boundaries.
The mention of specific companies or of certain manufacturers' products does not imply that they are endorsed or recommended by the Pan American Health Organization in preference to
others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.

Acknowledgements
This WHO Pharmaceutical situation assessment, Level II, was conducted with the full support of the Ministry of
Health of Barbados, including its permission from the Institutional Review Board (IRB) and endorsement to conduct
the study, with technical and financial support from Pan-American Health Organization/World Health Organization
(PAHO/WHO) through the European Union (EU)/WHO, Africa, the Caribbean and Pacific (ACP) Project
“Partnership on Pharmaceutical Policies”.
Director of the Barbados Drug Services (BDS), Ministry of Health (MOH) of Barbados coordinated the study and
took the responsibility for obtaining the necessary approval of the University of the West Indies/Ministry of Health
IRB.
The study was made possible by the support of the Chief Executive Officer (CEO) of the Queen Elisabeth Hospital
(QEH), Senior Consultant and Director of the Psychiatric Hospital, Medical Officers of Health and Sisters in charge
of the Policlinics, and heads of all health facilities visited and the householders that cooperated with this study.
The Barbados Statistical Services (BSS) collaborated with the BDS and provided assistance in the designing and the
sampling of the Household Survey. The Government Information Service (GIS) assisted with the public
announcement and press releases for the survey.
PAHO/WHO and the WHO Harvard Collaborating Center in Pharmaceutical Policy provided technical support for
the survey and their assistance is gratefully acknowledged. The support of the following individuals was invaluable
to the study:
Dennis Ross-Degnan and Catherine Vialle-Valentin, from the WHO Harvard Collaborating Center in
Pharmaceutical Policy provided methodological support for data review/analysis. Catherine Vialle-Valentin
facilitated the training of data collectors and is one of the research team members of the project. Maryam Hinds the
Director of the Barbados Drug Service, MOH Barbados, provided technical support and facilitated the conduction of
the survey as the Principal Investigator. Carol Mulder, Senior Lecturer at the University of the West Indies assisted
in the planning of the project and is one of the research team members of the project. She is also the Assistant
principal Investigator. In the absence of Carol Mulder, Jennifer Nunez took over the coordination and overall
management of the project. She coordinated the Household Survey while Cheryl Ann Yearwood coordinated the
facility Survey. Assistance was provided by the staff of BDS, generally, but especially, Pamela Payne-Wilson, Ersie
Chase, Glence Prescod, Debbie Williams, Maylene Dash-Brathwaite, Jackie Mason-Pile, Sandra Brathwaite,
Carmen Standard and Eleanor Thompson.
Data collectors were: For the Health Facility Survey: Daley Mottley, Russell Williams, June Benjamin, Joyce
Lewis, Christopher Scott, Chondelle Dash and Ibrahim Hinds. For the Household Survey: Beverley Beckles, Asha
Drakes, Carolyn Drayton, Sandra Murray, Raphael Greenidge, Carrie Reid, Hasan Patel, Mikaela Stoute, Sabrina
Drayton, Kendi Griffith, Nicole Corbin and Ria Haynes-Howard.
Adriana M. Ivama, Medicines and Biological Sub-regional Advisor, Caribbean Programme Coordination Office
(CPC) of PAHO/WHO provided technical support and reviewed the report. Nelly Marin Jaramillo, Regional
Advisor on Pharmaceutical Policy, PAHO/WHO coordinated the process in the Americas and facilitated the
technical support; Enrico Cinnella, technical officer from the Essential Medicines and Pharmaceutical Policies
Department, WHO, reviewed the report and Tassia Williams, PAHO/WHO CPC intern performed the proof reading.
Acknowledgement/Disclaimer
European Union
This document has been produced with the financial assistance of the
European Union and the technical support of the Pan American Health
Organization/World Health Organization. The views expressed herein are
those of the authors and can therefore in no way be taken to reflect the
official opinion of the European Union or the Pan-American Health
Organization/World Health Organization.
Table of Contents
LIST OF FIGURES ..................................................................................................................................................... 5
LIST OF TABLES ....................................................................................................................................................... 6
LIST OF BOXES ......................................................................................................................................................... 8
ABBREVIATIONS AND ACRONYMS ................................................................................................................... 9
CONFLICT OF INTEREST STATEMENT ........................................................................................................... 10
EXECUTIVE SUMMARY ....................................................................................................................................... 11
BACKGROUND - HEALTH AND PHARMACEUTICAL SECTOR ...................................................................................... 11
STUDY ..................................................................................................................................................................... 12
HEALTH FACILITY SURVEY ..................................................................................................................................... 12
Methods .............................................................................................................................................................. 12
Key results .......................................................................................................................................................... 12
Challenges and Constraints ................................................................................................................................ 13
HOUSEHOLD SURVEY .............................................................................................................................................. 14
Methods ............................................................................................................................................................. 14
Key results .......................................................................................................................................................... 14
Challenges and Constraints ................................................................................................................................ 16
RECOMMENDATIONS ................................................................................................................................................ 16
INTRODUCTION ..................................................................................................................................................... 17
BARBADOS BACKGROUND ................................................................................................................................. 18
HEALTH SECTOR ...................................................................................................................................................... 18
PHARMACEUTICAL SECTOR ..................................................................................................................................... 19
STUDY DESIGN AND METHODS ......................................................................................................................... 25
HEALTH FACILITY SURVEY ..................................................................................................................................... 25
HOUSEHOLD SURVEY .............................................................................................................................................. 29
RESULTS AND DISCUSSION ............................................................................................................................... 32
HEALTH FACILITY SURVEY ..................................................................................................................................... 32
Issues related to the field work ........................................................................................................................... 32
Health workers at health facilities ...................................................................................................................... 34
Access ................................................................................................................................................................ 36
Affordability ...................................................................................................................................................... 38
Quality of medicines .......................................................................................................................................... 39
Rational Use of Medicines (RUM) .................................................................................................................... 40
Challenges and constraints ................................................................................................................................. 44
HOUSEHOLD SURVEY .............................................................................................................................................. 45
Characteristics of surveyed households.............................................................................................................. 45
Geographic access and availability of medicines .............................................................................................. 56
Affordability of medicines ................................................................................................................................. 60
Medicines at home ............................................................................................................................................ 65
Use of medicines during acute illnesses ............................................................................................................. 68
Use of medicines for chronic diseases................................................................................................................ 73
Key indicators of Access and Use of Medicines ................................................................................................ 76
CONCLUSIONS AND RECOMMENDATIONS .................................................................................................. 80
REFERENCES .......................................................................................................................................................... 82
ANNEX 1. LEVEL I QUESTIONNAIRE ............................................................................................................... 83
ANNEX 2. LEVEL II SURVEY FORMS ................................................................................................................ 84
ANNEX 3. HOUSEHOLD SURVEY QUESTIONNAIRE .................................................................................... 85
ANNEX 4. ROUNDED RANGES OF HOUSEHOLD EXPENDITURES ........................................................... 86

ANNEX 5. DESCRIPTION OF INDICATORS- HEALTH FACILITY SURVEY ............................................. 87
ANNEX 6. DESCRIPTION OF INDICATORS- HOUSEHOLD SURVEY ........................................................ 89
List of Figures
FIGURE 1. GEOGRAPHIC LOCATION OF STATISTICAL SAMPLE AREAS, BARBADOS, 2010. ......... 29
FIGURE 2. STRATIFIED RANDOM SAMPLING AREA IDENTIFYING HOUSEHOLDS, BARBADOS, 2010. 30
FIGURE 3. AVAILABILITY OF KEY MEDICINES IN PUBLIC HEALTH FACILITY DISPENSARIES, AND IN
PRIVATE PHARMACIES. PHARMACEUTICAL SITUATION ASSESSMENT – HEALTH FACILITY SURVEY
LEVEL II, BARBADOS, JULY 2010. ..................................................................................................................... 37
FIGURE 4. DISTRIBUTION OF FACILITIES ACCORDING TO THE PERCENTAGE OF PRESCRIBED KEY
MEDICINES THAT WERE DISPENSED OR ADMINISTERED. PHARMACEUTICAL SITUATION
ASSESSMENT - HEALTH FACILITY SURVEY LEVEL II, BARBADOS, JULY 2010. ................................ 37
FIGURE 5. ADEQUACY OF INFRASTRUCTURE OF CONSERVATION CONDITIONS OF MEDICINES,
PHARMACEUTICAL SITUATION ASSESSMENT - HEALTH FACILITY SURVEY LEVEL II, BARBADOS,
AND JULY 2010. ....................................................................................................................................................... 39
FIGURE 6: NUMBER OF SURVEYED HOUSEHOLDS IN EACH REGION, BARBADOS, 2010.. ............. 45
FIGURE 7: AGE OF RESPONDENTS/HEALTH CARE DECISION MAKERS, BARBADOS, 2010. .......... 46
FIGURE 8. HOUSEHOLD ASSETS AND LEVELS OF MONTHLY (4 WEEKS) EXPENDITURES, BARBADOS,
2010. ........................................................................................................................................................................... 48
FIGURE 9. REPORTED SYMPTOMS OF ACUTE ILLNESS, BARBADOS, 2010. ......................................... 54
FIGURE 10. MOST FREQUENT CHRONIC DISEASES BY GENDER, BARBADOS, 2010. ........................ 55
FIGURE 11: PREVALENCE OF ILLNESSES, BARBADOS, 2010. .................................................................. 56
FIGURE 12. HOUSEHOLDS FAR AWAY FROM A PUBLIC HEALTH CARE FACILITY, BARBADOS, 2010. 57
FIGURE 13. SOURCES OF MEDICINES FOUND IN HOUSEHOLDS BARBADOS, 2010. ......................... 58
FIGURE 14. SOURCES OF MEDICINES TAKEN FOR AN ACUTE ILLNESS, BARBADOS, 2010. ........... 59
FIGURE 15. POTENTIALLY CATASTROPHIC EXPENDITURES RELATED TO MEDICINES IN MONTH
PRECEDING SURVEY, BARBADOS, 2010. ......................................................................................................... 63
FIGURE 16. MEDICINES IN HOUSEHOLDS WITH CHILDREN, BARBADOS, 2010. ................................ 65
FIGURE 17. PERCENTAGE OF HOME MEDICINES WITH ADEQUATE LABEL AND PRIMARY PACKAGE,
BY SOURCE, BARBADOS, 2010. .......................................................................................................................... 67
FIGURE 18: PRESCRIBERS OF MEDICINES IN CASE OF ACUTE ILLNESS, BARBADOS, 2010. ........ 69
FIGURE 19. ROUTE OF ADMINISTRATION OF MEDICINES PRESCRIBED FOR ACUTE ILLNESS,
BARBADOS, 2010. .................................................................................................................................................... 71
FIGURE 20. REASONS FOR NOT TAKING PRESCRIBED MEDICINES FOR ACUTE ILLNESS, BARBADOS,
2010. ............................................................................................................................................................................ 72
FIGURE 21. ACTIONS TAKEN FOR CHRONIC DISEASES, BARBADOS, 2010. ......................................... 73
FIGURE 22: REASONS FOR NOT TAKING MEDICINES PRESCRIBED FOR A CHRONIC DISEASE,
BARBADOS, 2010. .................................................................................................................................................. 75

WHO Level II Assessment - Health Facility and Household Surveys Barbados
6
List of Tables
TABLE 1. CHARACTERISTIC OF HEALTH CARE FACILITIES SURVEYED IN BARBADOS, JULY 2010. 33
TABLE 2. CHARACTERISTICS OF OUTPATIENTS INTERVIEWED IN BARBADOS, JULY 2010. ....... 34
TABLE 3. DISPENSER PROFILE AT PSA-HFS LEVEL II IN BARBADOS, JULY 2010. ............................ 35
TABLE 4. PRESCRIBER PROFILE IN THE PUBLIC SECTOR, PSA-HFS LEVEL II IN BARBADOS, JULY 2010.
..................................................................................................................................................................................... 35
TABLE 5. GENERAL INDICATORS FOR AVAILABILITY AND GEOGRAPHICAL ACCESSIBILITY,
PHARMACEUTICAL SITUATION ASSESSMENT – HEALTH FACILITY SURVEY LEVEL II, BARBADOS,
JULY 2010. ................................................................................................................................................................. 36
TABLE 6. NUMBER OF DAY’S WAGES OF THE LOWEST PAID GOVERNMENT WORKER NEEDED TO
PURCHASE STANDARD TREATMENTS. PHARMACEUTICAL SITUATION ASSESSMENT - HEALTH
FACILITY SURVEY LEVEL II, BARBADOS, JULY 2010................................................................................. 38
TABLE 7. GENERAL INDICATORS FOR QUALITY OF MEDICINES, PHARMACEUTICAL SITUATION
ASSESSMENT - HEALTH FACILITY SURVEY LEVEL II, BARBADOS, JULY 2010. ................................ 39
TABLE 8. GENERAL INDICATORS FOR RATIONAL USE, PHARMACEUTICAL SITUATION ASSESSMENT -
HEALTH FACILITY SURVEY LEVEL II, BARBADOS, JULY 2010. .............................................................. 42
TABLE 9. DISTRIBUTION OF PRIVATE PHARMACIES ACCORDING TO THEIR RESULTS ON %
PRESCRIPTION MEDICINES BOUGHT WITHOUT PRESCRIPTION, BARBADOS, JULY 2010. ........... 42
TABLE 10. ADHERENCE OF PRESCRIBERS TO RECOMMENDED TREATMENT GUIDELINES.
PHARMACEUTICAL SITUATION ASSESSMENT - HEALTH FACILITY SURVEY LEVEL II, BARBADOS,
JULY 2010. ............................................................................................................................................................... 43
TABLE 11: EDUCATION OF RESPONDENTS, BARBADOS, 2010. ................................................................ 46
TABLE 12: MONTHLY HOUSEHOLD EXPENDITURES, BARBADOS, 2010. ............................................. 49
TABLE 13. CHARACTERISTICS OF HOUSEHOLDS, BARBADOS, 2010. .................................................... 51
TABLE 14. SOURCES OF INCOME AND THE JOB OF THE MAIN EARNER IN THE HOUSEHOLD
(HOUSEHOLD HEAD), BARBADOS, 2010. ......................................................................................................... 52
TABLE 15: PREVALENCE OF ACUTE AND CHRONIC CONDITIONS, BARBADOS, 2010. .................... 53
TABLE 16: CHARACTERISTICS OF ACUTE AND CHRONIC CONDITIONS, BARBADOS, 2010. ......... 53
TABLE 17: TRAVEL TIME TO CLOSEST HEALTH CARE FACILITY, BARBADOS, 2010. .................... 57
TABLE 18: OPINIONS ABOUT GEOGRAPHIC ACCESS AND AVAILABILITY OF MEDICINE, BARBADOS,
2010. ............................................................................................................................................................................ 60
TABLE 19: COST OF MEDICINES FOR A RECENT ACUTE ILLNESS, BARBADOS, 2010. .................. 61
TABLE 20: MONTHLY COST OF MEDICINES FOR A CHRONIC DISEASE, BARBADOS, 2010. ........... 62
TABLE 21: MEDICINES INSURANCE COVERAGE, BARBADOS, 2010. ...................................................... 64
TABLE 22: OPINIONS ABOUT AFFORDABILITY OF MEDICINES, BARBADOS, 2010. .......................... 64
TABLE 23: MEDICINES FOUND AT HOME, BARBADOS, 2010. ................................................................... 66
TABLE 24. ACTIONS TAKEN FOR A RECENT ACUTE ILLNESS, BARBADOS, 2010. ............................. 68
TABLE 25 MEDICINES TAKEN FOR A RECENT ACUTE ILLNESS, BARBADOS, 2010. ......................... 69
TABLE 26 MOST FREQUENT MEDICINES PRESCRIBED FOR CHRONIC DISEASES, BARBADOS, 2010. 74
TABLE 27. OPINIONS ABOUT QUALITY OF CARE AND GENERICS, BARBADOS, 2010. ..................... 76
TABLE 28: INDICATORS OF ACCESS AND USE OF MEDICINES - ALL HOUSEHOLDS, BARBADOS, 2010.
..................................................................................................................................................................................... 77
TABLE 29: INDICATORS OF ACCESS AND USE OF MEDICINES - HOUSEHOLDS WITH AT LEAST ONE
ACUTE OR CHRONIC CONDITIONS, BARBADOS, 2010. ............................................................................... 78
WHO Level II Assessment - Health Facility and Household Surveys Barbados
7
List of boxes
BOX 1. KEY MEDICINES SELECTED FOR THE SURVEY ............................................................................. 26
BOX 2. TRACER CONDITIONS FOR COMPLIANCE OF PRESCRIBERS TO RECOMMENDED TREATMENT
PROTOCOLS/GUIDELINES. ................................................................................................................................ 26
BOX 3: TRACER CONDITIONS FOR AFFORDABILITY ................................................................................ 27
BOX 4. SUMMARY LIST OF INDICATORS AND CORRESPONDING SURVEY FORM USED TO COLLECT
THE DATA ................................................................................................................................................................ 28

WHO Level II Assessment - Health Facility and Household Surveys Barbados
8
Abbreviations and Acronyms
% ile Percentile
ARI Acute Respiratory Infection
BBD Barbados Dollar
BDS Barbados Drug Service
BNDF Barbados National Drug Formulary
CEO Chief Executive Officer
DHI Development Human Index
EML Essential Medicines List
GA Geographic Access
GBS General Bureau of Statistics
GDP Gross domestic product
HAI Health Action International
HFS Health Facility Survey
HH Household
Ind. Indicator
Inj Injection
INN International Non-Proprietary Name
IRB Institutional Review Board
M Mixed
MOH Ministry of Health
MSH Management Sciences for Health
Nb Number
NMP National Medicines Policy
OB Originator brand
PAHO Pan American Health Organization
PSF Pharmaceutical Situation Assessment
Q Quintile
QEH Queen Elizabeth Hospital
QL Quality
RUM Rational Use of Medicines
SD Standard Deviation
SES Socio-Economic Status
SF Survey Formulary
STG Standard Treatment Guidelines
UNDP United Nation Development Program
URTI Upper Respiratory Tract Infection
USD United States dollars (also US$)
WHO World Health Organization
WHO Level II Assessment - Health Facility and Household Surveys Barbados
9
Conflict of Interest Statement
None of the authors of this survey or anyone who had participated or collaborated in any phase of the planning,
field work, analysis or interpretation of the results has any competing financial or other interests.
WHO Level II Assessment - Health Facility and Household Surveys Barbados
10
Executive Summary
Background - Health and Pharmaceutical Sector
Barbados is a one of the most heavily populated Caribbean islands. It is a middle income country with a
population estimated 275,700 as of December 2009. Life expectancy at birth is 75.8 years, with 15.75%
of the population over the age of 60 years. Key contributors of morbidity and mortality are heart disease,
cerebrovascular disease, diabetes mellitus, malignant neoplasm, hypertension, and HIV/AIDS among
adults.
The Ministry of Health is responsible for assuring a functioning health care system. Health care services
are organized in three levels. The public sector works in partnership with the private sector. The Special
Benefit Service (SBS) provides medicines and related items listed in the Barbados National Drug
Formulary free of cost at point of service to the following beneficiaries in both the public and private
sectors:
(1) Persons 65 years of age and over;
(2) Children under 16 years of age;
(3) Persons who receive prescribed Formulary Drugs for the treatment of hypertension, diabetes,
cancer, asthma and/or epilepsy.
It should be noted that patients between 16 and 64 who are eligible to receive prescribed formulary
drugs for the treatment of hypertension, diabetes, cancer, asthma and epilepsy obtain the other formulary
drugs at the subsidised prices found in the ‘Prescription Pricing Guide-Purchasing Guide’. This is so
because all formulary medicines and related items enter the country free of duty and other taxes and
have an agreed mark-up attached to them. It is thus true to say that all Barbadians benefit from the
programmes of the Barbados Drug Service (BDS).
Any Barbadian Citizen or Permanent Resident seeking medical attention within the public sector can
have his/her prescription filled free of cost in one of the private participating pharmacies of the SBS or
BDS pharmacies. Prescriptions originating from private physicians can also be dispensed at the BDS
pharmacies free to beneficiaries or at a similar fixed cost + mark-up to non-beneficiaries. The public
pharmacies located at the Geriatric Hospital and the St. Philip District Hospital is set up specifically for
dispensing in-patient prescriptions only.
It should be noted that patients can obtain formulary medicines at subsidised prices because all
formulary drugs and related items enter the country free of duty and other taxes and have mark-up
attached to them.
In Barbados, a National Medicines Policy (NMP) document has existed in draft form since 2003. The
Barbados Drug Service (BDS) provides pharmaceutical regulatory services for Barbados. It also
implements a policy covering medicines‟ prices for beneficiaries that applies to both public and private
sectors. Medicines prices set up by the government are displayed in the Barbados National Drug
Formulary (BNDF), which was last updated in 2010. Medicines that do not appear in BNDF are sold by
private pharmacies according to market forces.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
11
Study
An assessment of the pharmaceutical situation was undertaken in Barbados between October, 2009 and
July, 2010 using a standardized methodology developed by the World Health Organization (WHO). The
goal of the assessment was to evaluate the pharmaceutical situation in Barbados. The specific objectives
were to provide data to measure outcomes on affordability and availability of key medicines,
geographical accessibility of dispensing facilities and rational use of medicines, as well as some
indication of the quality of medicines at health facilities and pharmacies. These data would provide
evidence on whether the pharmaceutical policy is achieving its goals.
The Pharmaceutical Situation Level II study has two components: a health facilities survey and a
household survey, both based on indicators. In the first component, data relating to pharmaceutical
policy outcomes are gathered from public and private pharmacies and warehouses that supply public
facilities. The second data comes from a questionnaire applied at the household level.
Health Facility Survey
Methods
The survey was conducted in all the public facilities of Barbados with outpatient services which are
expected to carry a full supply of essential medicines. In addition, 30 private pharmacies were included
based on random selection.
Data entry was performed using standard forms developed by WHO (Annex 2). Analysis was done
using the Excel ® software program.
Key results
Access
Overall access indicators show that the availability of key essential medicines is 100% in public health
facilities and 94% in private pharmacies. The percentage of prescribed key medicines that are dispensed
to patients is 99% in the public sector. Key medicines are those listed in Box 1.
Concerning geographical accessibility, 97% of patients interviewed at public facilities traveled less than
one hour to reach the facility.
Treating common conditions using standard regimens, the lowest paid government worker would need
between 0.02 and 0.05 of one day‟s wages to purchase the lowest priced generic medicines from the
private sector, and between 0.09 and 0.97 of one day‟s wages to purchase originator brands from the
private sector.
Data suggests that treatment for common primary health problems is generally affordable based on the
fact that the financial burden for the lowest paid public servant in terms of proportion of a working day‟s
pay is low.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
12
Quality and regulation
No expired medicines from the key medicines list were found in the public or private sector. Storage
conditions were rated at 85% with respect to adequacy in the storerooms and dispensing rooms of public
health facilities. The adequacy was slightly better in private pharmacies at 90%.
Most public dispensing facilities and private pharmacies comply with the legal requirements of the
government with regards to the presence or support of the pharmacist; these professionals were found in
most facilities. The profile of health workers dispensing medicines was adequate and followed the law,
with no untrained staff dispensing in the private or public sector. According to the findings, doctors are
the most frequent prescribers, and 78% of prescribers have been recently trained in rational use of
medicines. However, prescribing was inadequate for many of the tracer conditions cases reviewed by
surveyors.
Use of medicines
There is no Essential Medicines List (EML) in Barbados. A comprehensive National Formulary exists
however, and was found in 92% of public health facilities. There are national officially adopted
Standard Treatment Guidelines (STG) for diabetes, hypertension and asthma. However, no STG exist
for other common health conditions. The STG for diabetes, hypertension and asthma were available in
55% of surveyed health facilities. With regards to indicators of rational use, 23 % of patients with tracer
conditions were prescribed antibiotics, and 7 % were given injections. Selling of prescribed medicines
without prescription was observed in several private pharmacies. In 2 visited pharmacies, between 25
and 50% of prescription medicines were purchased without prescription. All patients interviewed at
public and at private pharmacies knew how to take their medicines.
Challenges and Constraints
Despite the presence of the pharmacist in most pharmacies, storage conditions of medicines needs to be
improved. Storage conditions were not optimal for public health facilities and private pharmacies. The
implementation of Best Practices related to distribution, storage and pharmacy practices would improve
this situation.
In Barbados, medicines are generally available based on information about current stock on hand.
However, as there were no stock cards in the polyclinics, stock-out days could not be assessed. At the
Saint Michael Psychiatric Hospital (SMPH) and Queen Elizabeth Hospital (QEH), stock-out cards are
maintained. At the former, the percentage of adequate records was 100% and the average number of
stock-out days was 0. At the QEH, the percentage of adequate records was slightly lower at 93.8%, and
the average number of stock-out days was high: 61 days. It is recommended that the computerized
system in the polyclinics be improved to facilitate retrieval of previous stock-out information.
The International Non-proprietary Name (INN) was used for only 36% of prescription medicines in
public health facilities.
Irrational use in private pharmacies is a matter of concern taking into account that 10 in 26 (38%)
private pharmacies sold at least one prescription medicine without prescription at the time of visits.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
13
There are national officially adopted Standard Treatment Guidelines (STG) for diabetes, hypertension
and asthma. The STG for diabetes, hypertension and asthma were not available in half the public
healthcare facilities. No STG exist for other common health conditions.
An important finding of the survey is the inappropriate prescription of antibiotics, which are underused
to treat pneumonia in children under 5, and overused to treat non-bacterial upper respiratory infections.
This and the fact that many children under 5 with diarrhea are not prescribed the appropriate treatment,
strongly suggest the need to intensify training of providers in key areas of primary care prescribing. It
must be noted here that the data with respect to the prescribing patterns of physicians is influenced by
the ability to extrapolate the data from the Health Management System in place at the public health
facilities.
The survey also indicates that managerial policies related to pharmaceuticals need to be improved. The
appropriate use of medicines can be improved by increasing availability and use of STG, and by
encouraging the use of INN for prescribing.
Household Survey
Methods
The survey was conducted in all parishes of Barbados. The survey was conducted using the random
stratified sampling method. A sample of 317 households was drawn out of 44 randomly-selected areas.
The questionnaire collected information about medicines kept at home, used during recent acute illness
and prescribed for chronic diseases. It also collected information on how people behaved when
confronted with acute or chronic conditions, their opinions about medicines, as well as demographic and
socio-economic data. Data entry was performed with EpiData software and analysed with Excel .
Key results
Characteristics of surveyed households
The household member most knowledgeable in health was selected as the survey respondent. The
majority of respondents was over 50 years old and had completed primary or secondary school (7 in 10).
One in four households had incurred health expenditures over the past four weeks. Over half of
households reported at least one chronic condition. The most frequently reported chronic diseases by far
were hypertension and diabetes. Few households (15%) reported at least one acute illness. The most
frequent group of symptoms of acute illness was related to cough, runny nose, sore throat, and ear ache.
The prevalence of both chronic and acute conditions was higher in the group of households with lower
socio-economic status (SES).
Geographic access and availability of medicines
Overall, indicators of geographic access to medicines suggest that the majority of surveyed households
live close to a public heath care facility. However, 11% households in the lower SES group live at more
than one hour from a public health facility. The majority of medicines, either found in households or
obtained for an acute illness, came from a private pharmacy.
WHO Level II Assessment - Health Facility and Household Surveys Barbados
14
About half of household respondents agreed that medicines are available at their public heath care
facility, while nine in ten agreed that medicines are available at private pharmacies. More respondents in
the lower SES group had a positive opinion of the availability of medicines in the public sector.
Affordability of medicines
Overall, indicators of affordability of medicines suggest that the price households pay for medicines is
not a major obstacle to accessing medicines. A larger proportion of individuals received free medicines
for chronic diseases than for acute illnesses. An average of 3% of respondents reported spending more
than 40% of their non-food expenditures on medicines over the past four weeks.
Two thirds of respondents agreed that they can usually afford medicines. This proportion was lower in
the lower SES group.
Very few people with acute or chronic conditions reported health insurance coverage for medicines. All
respondents who reported medicines insurance coverage were in the higher SES group.
Medicine use and medicines at home
About 80% of households with children stored medicines at home. The average number of medicines
found at home was 3. Most of these medicines had an appropriate label and a primary package in good
condition, especially when obtained in a public health care facility.
The two most frequent medicines found at home were paracetamol (17% of medicines) and
chlorpheniramine, an antihistaminic (5% of medicines).
Medicine use and acute illnesses
Few households reported acute illnesses. Behavior with regards to seeking care and taking medicines
depended on the perceived severity of the illness. The two most frequently used medicines were
paracetamol (26% of medicines) and chlorpheniramine (22% of medicines), which suggests a high
prevalence of treatment for allergic conditions in July. Half of the medicines for acute illness were
prescribed by a doctor or a nurse, which points to the use of non-prescription medicines for the
remaining cases of acute illness. The use of injections for treatment of acute illness was only observed
in the lower SES group: in this group, 7% of medicines were injections. The main reason for not taking
medicines was that symptoms improved.
Medicine use and chronic diseases
Over half of the households reported a chronic disease. Eight in ten individuals with a chronic disease
were told to take medicines and had medicines at home. This percentage however was halved in the
lower SES group: only four in ten individuals with a chronic disease who had been told to take
medicines had medicines at home. In addition, in this group, the percentage of people with chronic
disease not told to take medicines was much higher than in the higher SES group. This strongly suggests
that in the lower SES group, people under-use medicines for chronic diseases. Metformin was the most
frequently used antidiabetic, and indapamide the most frequently used antihypertensive. The main
reason given for not taking medicines was that symptoms improved.
Opinions about quality of care and generics

WHO Level II Assessment - Health Facility and Household Surveys Barbados
15
Overall, over half of respondents (53%) believed that the quality of medicines and services in their
public health care facility were good. More respondents (87%) agreed that the quality of services
delivered by private health care providers in their neighborhood was good. The majority of respondents
could not distinguish between brand name and generic medicines.
Challenges and Constraints
Overall, the household survey results indicate that access to medicines is of good quality in Barbados,
and that it is slightly better in households with a higher SES. They point out to an insufficient use of
medicines to treat chronic diseases in households of lower SES.
Recommendations
The survey indicates that managerial policies related to pharmaceuticals need to be improved. The
findings can be used for updating the National Pharmaceutical Policy and implementation plan.
Regarding the need for improvement of the quality of services, it is recommended to develop and
implement Good Practices in all tiers of the pharmaceutical chain from distribution to storage and
pharmacy practices, which would contribute to improve this situation. Special attention needs to be paid
to the fact that a relatively high percentage of prescription medicines are sold without a prescription.
It is recommended to develop strategies that guarantee the quality and strengthen the use of generic
medicines. These strategies would include the regulation of aspects related to quality, safety, prices and
enforcement of the prescription using the International Non-proprietary Name (INN), and generic
substitution.
Regarding aspects related to rational use of medicines, the Barbados Drug Formulary needs to be
updated using the concept of Essential Medicines, selection with evidence based criteria. Standard
Treatment Guidelines (STG) for the most common conditions should be developed, officially adopted
and widely disseminated to users. Priority can be given to chronic diseases due to their high prevalence
in Barbados, with a holistic approach considering lifestyle and treatment.
It is recommended to develop a strategy to improve knowledge and rational use of medicines by the
population. It would address medicines access, quality and safety of medicines, their management at
home (labeling, storage conditions, etc) adherence to treatment (especially for chronic conditions) and
the use of generics or INN drugs.
It is recommended to design strategies to improve equity in medicines access: tackling the higher
prevalence of chronic and acute conditions in the lower SES group, the under use of medicines in this
group. Equity in access to medicines is one aspect to be further investigated; interventions can be
designed for specifically target people of lower SES.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
16
Introduction
Between October 2009 and July 2010, the Ministry of Health (MOH) conducted a nationwide study of
the pharmaceutical situation in public health facilities and private pharmacies in Barbados. The main
goal of the study was to document the degree of success in achieving strategic pharmaceutical
objectives.
This study was conducted using the standardized methodology developed by the World Health
Organization (WHO), named Pharmaceutical Situation Assessment Level II. This is an indicator-based
approach that provides systematic data on access and rational use of quality medicines through a
facility-based survey.
The core indicators measure the most important information needed to understand the pharmaceutical
situation in a country.
The study was intended to answer the following questions:
Are medicines available and affordable in public and private dispensing facilities to treat
common conditions at primary care level?
Do people have adequate geographical access to public and private dispensing facilities?
Are there any expired medicines in public and private dispensing facilities?
Are medicines adequately stored and handled in public health facility dispensaries and
warehouses supplying the public sector?
Are medicines adequately prescribed, labeled and dispensed?
Are patients informed on how to use their medicines?
Are pharmacists present at dispensing facilities according to the law?
Are pharmacists present at dispensing facilities?
Which professionals are prescribing and dispensing?
Do prescribers comply with good prescribing practices?
How does Barbados compare to other countries with regard to access to and use of medicines?
WHO Level II Assessment - Health Facility and Household Surveys Barbados
17
Barbados background
Barbados is a small country, covering an area of 430 km2
or 166 square miles and has a population
density of 625 persons per square kilometer (1,619 persons per square mile). It is divided into 11
parishes and the total population is 275,700 (estimate at December 2009), with the majority of
population living in the southern parishes of St. Michael, Christ Church and St. Philip. It is not only one
of the most heavily populated islands in the Caribbean, but also has the highest proportion of people
over 65-years old1,2
.
Barbados is described as a middle income country, with a GDP of US $10,350.00 per capita. Of the
total labor force, approximately 10.6% of persons are unemployed, with 6.4% of these in a state of long-
term unemployment over 3 months (as of the 1st Quarter 2010).
1
Life expectancy at birth is 75.8 years, with 15.7% of the population over the age of 60 years, and 21.5%
of the population below 15 years in 2000 population census. According to the most recent national
census in 2000, the average number of people per household is 3. 1
Key contributors to morbidity and
mortality are heart disease, cerebro-vascular disease (stroke), diabetes mellitus, malignant neoplasm,
hypertension and HIV/AIDS among adults. The information from the polyclinics and out-patient clinics
indicate that in adults (20 to 65 years) the conditions commonly seen and treated are hypertension,
diabetes mellitus and disorders of the circulatory system for the older adults (45-65 years), whereas
among the younger adults there are concerns about the impact of road traffic accidents, violence and
HIV/AIDS. 2
Health sector
In 2008, when the US$1 was equivalent to Bds$2.00), government expenditure on health represented
12.9% of all government expenditures (approximately 4.4% of the GDP).1 Hospital services and primary
care accounted for the bulk of the expenditure, 52 percent and 25 percent respectively based on data
from 2003. 2
The public health sector is composed of 3 levels: primary, secondary and tertiary care.
Primary care is delivered from 8 polyclinics and 4 satellite out-patient clinics that are strategically
located and provide a wide range of preventive, curative services, and rehabilitative services. These
services include maternal and child health, immunization, oral health, general practice clinics,
hypertension and diabetes clinics, nutrition education, physiotherapy, provision of pharmaceuticals,
environmental health and a limited range of mental health services.
1 Statistics provided from Barbados Statistical Services
2 Report of the Chief Medical Officer 2002-2003

WHO Level II Assessment - Health Facility and Household Surveys Barbados
18
Secondary and tertiary care is provided by the Queen Elizabeth Hospital (QEH), Psychiatric hospital, the
St. Michael District Hospital, 3 District Hospitals, and specialized institutions that provide care for
persons with disabilities. The QEH is a 600 bed hospital that provides acute, secondary, tertiary and
emergency care on a 24-hour basis.
The Psychiatric care facility is a 627-bed hospital, and an 8-bed unit at the QEH. It provides inpatient
and outreach services with additional out-patient services offered on a limited basis at the 8 polyclinics.
The goal of the St. Michael District Hospital and 3 district institutions is to rehabilitate the elderly to
maximum functional capacity so that they can return to their respective communities.
In excess of 35% of the population is covered by private insurance. The private sector represents
approximately 50% of total health services.
The public health sector is complemented by the private sector. The program involves a partnership
with the private sector whereby specialists provide a wide range of secondary-care services, with
support from private laboratories and pharmacies. The private sector also comprises a 24-bed hospital, a
private renal dialysis provider, a halfway house providing mental health services, two substance abuse
treatment providers, as well as 45 nursing and senior citizens homes, which provide long term care for
older persons.1
Pharmaceutical sector
There are approximately 100 licensed private pharmacies outlets in Barbados and 17 public pharmacies.
Public sector pharmacies account for 27% of medicines dispensed to patients, while the private sector
accounts for the remaining 73%. The Barbados Drug Service (BDS) has responsibility for 14 of the 17
public sector pharmacies located across Barbados. The other 3 are managed by the respective
institutions namely the Queen Elizabeth Hospital, the Psychiatric Hospital, and the Ladymeade
Reference Unit. There are two parishes that do not have a Public Pharmacy, namely St. Lucy and St.
James. These parishes are serviced by the Maurice Byer and Black Rock Polyclinic pharmacies
respectively. The BDS pharmacies provide beneficiaries with drugs and related items listed in the
Barbados National Drug Formulary free of cost at point of service. Non-beneficiaries are charged a fee
for this service based on the pricing mark-up which applies to the private sector. Any Barbadian citizen
or permanent resident seeking medical attention within the public sector can have his/her prescription
filled free of cost in one of the public pharmacies. The only exception to this is the pharmacies located
at the Geriatric Hospital and the St. Philip District Hospital. These two pharmacies are set up
specifically for dispensing in-patient prescriptions with some exception given to dispensing
prescriptions for staff members. Prescriptions originating from private physicians can also be dispensed
at the BDS pharmacies at a fixed cost plus the same mark-up that applies to the private sector.
National Medicines (Drugs) Policy

WHO Level II Assessment - Health Facility and Household Surveys Barbados
19
In Barbados, a National Medicines Policy (NMP) document has existed in draft form since 2003. The
primary objective of this document is to ensure access, quality and rational use of medicines by health
care professionals and citizens. The document sets out the goal and guide for action with the expression
of the medium to long term goals set by the government of Barbados for the pharmaceutical sector. The
document provides the framework within which the activities of the pharmaceutical sector can be
coordinated. It covers both the public and private sectors. It was submitted to the Cabinet in 2004 and
was last updated in 2009. This document is an essential part of the health policy and it seeks to promote
equity and sustainability of the pharmaceutical sector. An official implementation plan that sets out
activities, responsibilities, budget and timeline is not in place.
Regulatory system
The Barbados Drug Service provides the regulatory service for Barbados on pharmaceuticals. Routine
inspections are undertaken at all pharmacies and the sole pharmaceutical manufacturing plant operating
in the country. Initial inspections are conducted in the wholesalers‟ facilities but they are not licensed.
These inspections are done primarily to ensure that the pharmacy legislation is upheld and that the
medicines manufactured and the process of manufacturing is in accordance with World Health
Organization‟s (WHO) Good Manufacturing Practice. One hundred and fifty-eight (158) pharmaceutical
samples were analyzed in 2006-07. They were found to be in compliance with Good Manufacturing
Practice techniques and were considered suitable for marketing. The products were granted certificates
of pharmaceutical product on international commerce (CPP) and are commercialized both locally and
regionally.
Registration of medicines is however not yet in place but significant progress has been made in
advancing this process. Currently, analytical testing (identity, purity and dissolution) is carried out on all
new generic medicines before they are placed on the market. No bioequivalence data is analysed. There
is a draft bill amending the Drug Service Act which is being circulated for comments. This amendment
aims to ensure that all medicines are approved and registered before being placed on the market. The
amendments also cover Pharmacovigilance and prevention and combating of counterfeit medicines.
Regulatory provisions are in place for licensing manufacturers of medicines. In accordance with Section
40 and 41 of the Financial Administration and Audit (Barbados Drug Service) Rules, 1980, the Director
of the Drug Service shall prepare and maintain a list of suppliers, approved by the Minister of Health
(MOH), of medicines and related items and may restrict invitations to tender as well as contracts for the
purchase of medicines and related items to those suppliers. Any person may apply in writing to have his
or her name included in the list of suppliers having given such information as the Director of the Drug
Service requires. The Drug Inspectorate processes new applications made by manufacturers to be listed
as approved suppliers of medicines and related items. The certificate from the Regulatory Authority in
the country in which the manufacturing plant is located and the statements which substantiate that the
manufacturer produces medicines for consumption in both the domestic and foreign market must be
properly endorsed by an accredited Notary Public.
Continuous efforts are made to ensure that medicines imported and sold in Barbados are manufactured
in accordance with the United States Pharmacopoeia and the British Pharmacopoeia standards or any
other recognized standards. In this regard, different brands of pharmaceuticals are collected and sent for
testing to the Caribbean Regional Drug Testing Laboratory (CRDTL) in Jamaica, Eurofins, England and
Experchem Laboratories Inc., Canada.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
20
In 2009, as part of the routine post market surveillance exercise, twenty six (26) results were received at
the CRDTL from Barbados with 24 Satisfactory Results and 2 Unsatisfactory Results.
Legal provisions are in place for the licensing of pharmacists and pharmacy premises through the
Pharmacy Council. There are legal provisions for licensing nurses and doctors before they can practice
through the Nursing and Medical Councils respectively. Dentists also have the Dental Council for
licensing of dentists. There is a Paramedical Council that takes the responsibility for the registration of
other allied health professionals. The Pharmacy Council with support from the Drug Inspectorate
continues to maintain vigilance over the operation and practice of pharmacy in the country. All
registered health professionals renew their licenses annually. Pharmacists as well as the premises of
private pharmacies are re-certified annually and subsequently registered in accordance with the
provisions of the Pharmacy Act. Pharmacists can only dispense medicines that are prescribed by a
medical practitioner that is registered in Barbados. Barbados does not have a generic policy or specific
regulation; however, generic substitution is performed in both the public and private pharmacies. The
private pharmacies honor the agreement signed between the Director, BDS and the Private Participating
Pharmacies in the acquisition of medicines and related items listed in the Formulary so that an adequate
supply of those medicines and related products are continuously available. Except with the express
authorization of the Director and BDS, they can purchase all such formulary medicines that the
Pharmacy requires for the purposes of the Agreement with the BDS from the designated contractors who
have concluded contracts with the Government of Barbados or the BDS in accordance with the Financial
Administration and Audit (Drug Service) Rules, 1980.
The pharmacies are also obligated to ensure that where a prescribed formulary medicine is not in stock in Barbados the BDS is immediately contacted. BDS shall then instruct the pharmacy as to which alternative medicine or related item in the same generic category to dispense to a beneficiary as the cost of this shall be borne by the Barbados Drug Service.
There are provisions in the medicines regulations covering promotion and/or advertising of medicines as
set out in the Health Service (Control of Drugs) Regulations, 1970. Nevertheless, monitoring of
medicines promotion is not performed.
Medicines supply system
Public and private sector biding is pooled at the national level from the point of view that national
tenders are awarded to local distributors with government guaranteed quantities of purchase and
estimated global quantities to be purchased (public and private sector) annually.
Individual public pharmacies are however responsible for their own medicine orders (procurement)
which are then centrally approved through the Government‟s SMART STREAM accounting system. It
is conducted under the supervision of the BDS, a department of the Ministry of Health. Public sector
medicines distribution is the responsibility of the Ministry of Health through the Barbados Drug Service.
Once the medicines are procured, they are distributed to the public health facilities by the local
wholesalers who have been awarded with contracts.
The tender processes used for public sector procurement are 100% national competitive tender. The
tender is advertised in the two local print media. The Ministry of Health is well on its way to developing
a web page that will include the BDS. Once that is completed, international tendering would be possible
WHO Level II Assessment - Health Facility and Household Surveys Barbados
21
since the Tender document will be available for downloading on the website. However, tenderers must
have local agents in Barbados. Except in emergency or exceptional situations, direct negotiations or
direct purchasing is not done. In 2009, direct procurement of Oseltamivir (Tamiflu) in response to the A
H1N1 epidemic constituted about 2% of total public expenditure on medicines, which is quite
significant. There are no regulations for national manufacturers‟ preference in public sector
procurement. Public sector procurement is not limited to medicines on Barbados Drug Formulary
(BDF).
Medicines financing
In 2007-08, the total public expenditure for medicines was US$ 23.49M. In 2009/2010 the total
expenditure for medicines was US $26.36M. The current financial year will probably be similar to
2009/2010 figures.
Barbados provides medicines and related items listed in the Barbados National Drug Formulary free of
cost at point of service, through the Barbados Drug Service, to the following beneficiaries:
(1) Persons 65 years of age and over;
(2) Children under 16 years of age; and
(3) Patients who receive prescribed Formulary Drugs for the treatment of hypertension, diabetes,
cancer, asthma and/or epilepsy.
All other items from the formulary can be obtained at the subsidized prices found in the ‘Prescription
Pricing Guide-Purchasing Guide’. This is so because all medicines from the formulary and related items
enter the country free of import duty, environmental levy and value added tax. Furthermore, they have
an agreed mark-up attached to them.
Revenues from fees or the sale of medicines from non-beneficiaries is never used to pay the salaries
directly or supplement the income of public health personnel in the same facility. Such revenue
collected in the public sector goes into the consolidated account
Prescribers in the public sector never dispense medicines; they may need to administer medicines
occasionally. In the private sector, they occasionally dispense medicines.
There is no public health insurance in Barbados. Some of the population has private health insurance,
which covers prescription medicines.
Barbados has a policy covering medicine prices under the BDS program that applies to both public and
private sectors. Local pharmaceutical distributors are fully involved in the supply process, and direct
overseas purchases are seldom made. The Local Distributors are allowed a 32% trading mark-up on
cost, insurance and freight. They are responsible for importing, warehousing, and distributing the
medicines and related items supplied under the Barbados Drug Service program. The retail private
pharmacies participating in the program use the following markup in preparing their reimbursement
claims to the BDS for payment:
Cost of Drug to Pharmacy Amount to be Charged
$0 - $2.00 Fixed Price of $5.00
WHO Level II Assessment - Health Facility and Household Surveys Barbados
22
$2.01 - $10.00 Cost plus $5.00
$10.01 - $20.00 Cost plus $7.00
$20.01 - $40.00 Cost plus $12.00
Over $40.00 Cost plus 30%
The government does not set the price or place any price controls on non-formulary medicines that are
sold according to the market forces. Similarly, there is no price control in place for the sale of formulary
medicines to non-beneficiaries in the private sector.
The Barbados National Drug Formulary (BNDF) displays the prices of medicines contained in it. As
stated earlier, prescriptions originating from private physicians written for non-beneficiaries can also be
dispensed at the BDS public pharmacies at a fixed cost plus mark-up in which applies to the private
sector. This privilege to the non-beneficiaries applies to all BDS pharmacies except those at the two
district hospitals where there is no dispensing of medicines to outpatients. Non-beneficiaries are those
who have seen a physician in the private sector for illnesses other than diabetes, hypertension, cancer,
asthma, and epilepsy, and are between the ages of 16 and 64.
Barbados does not have a national medicine price monitoring system for retail/patient prices and there
are no regulations mandating that the price information should be made publicly accessible. The draft
National Medicines Policy (NMP) and the official written guidelines on medicine donations provide
rules and regulations for donors and provide guidance to the public, private and/or NGO sectors on
accepting and handling donated medicines.
Rational use of medicines (RUM)
The Barbados National Drug Formulary is updated annually, most recently in 2010. Currently, the
BNDF is broader than an Essential Medicines List (EML). It contains approximately 1000 unique
medicine formulations. It is currently being reviewed with criteria based on evidence with the support of
PAHO/WHO and the PAHO/WHO Collaborating Centre on Rational Use of Medicines of the
University of La Plata, Argentina.
The drugs contained in the Tender document guided by selections contained in the Barbados National
Drug Formulary are being used for public and private sector procurement. There is no government price
of medicines in Barbados; the cost from the wholesalers is the same to both public and private
pharmacies. There is a Drug Formulary Committee responsible for the selection of products in the
Barbados National Drug Formulary. This Committee meets monthly.
The Drug Tender Committee is responsible for the actual award of contracts for the provision of drugs
in Barbados. This Committee makes its main adjudication during Primary Tenders and then there is a
Supplementary Tender for those drugs not tendered in the Primary document or those drugs that need
further consideration.
The health ministry produces national standard treatment guidelines (STG) for some major conditions,
namely diabetes, hypertension, asthma and HIV/AIDS. These were last updated in 2006 for diabetes and
hypertension and 2009 for asthma. As there is one specialised treatment centre for HIV/AIDS, the

WHO Level II Assessment - Health Facility and Household Surveys Barbados
23
related STG is available at this centre. The policlinics have the STG for prophylactic care for accidental
injury.
Antibiotics should not be sold over the counter without a prescription but they are occasionally sold,
while injections are seldom sold over the counter without a prescription.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
24
Study Design and Methods
The model currently proposed by WHO for monitoring country pharmaceutical situations uses a
hierarchical approach with 3 groups of indicators: Level I, Level II, and Level III. Level I indicators are
assessed with a short questionnaire measuring organizational structure and processes of the
pharmaceutical sector. WHO Level II surveys investigate outcomes of the pharmaceutical sector in
public and private health care facilities and in households. Level III assessments evaluate specific
aspects of the pharmaceutical sector.
Health Facility Survey
The survey with Level II indicators is a very important part of monitoring the pharmaceutical sector
because these indicators measure the outcomes and impact of strategic pharmaceutical programs in a
country: improved access, quality and rational use.
Access is measured in terms of availability and affordability of essential medicines. Additionally, there
is an indicator on geographical accessibility. Measuring the actual quality of medicines by testing
samples can be expensive. It is preferable to use indicators measuring the presence of expired medicines
on pharmacy shelves as well as adequate handling and conservation conditions. Finally, rational use is
measured by examining the prescribing and dispensing habits and the implementation of key strategies
such as standard treatment guidelines (STG) and essential medicines lists (EML).
Level II facility indicators are measured in public health facilities, private pharmacies, and warehouses
supplying the public sector.
The WHO level II methodology was adapted to the context of Barbados. The facility sample included
twelve public facilities, corresponding to all public health care facilities with outpatient services and
expected to carry a full supply of essential medicines in Barbados. Thirty private pharmacies out of the
100 operating in Barbados were selected randomly. No public warehouse was surveyed, as Barbados
public sector contracts out storage and distribution of medicines to private wholesalers.
In each facility surveyed, a set of Survey Forms (Annex 2) was applied. This allowed adequate
information gathering to calculate the Level II indicators.
The verification of availability, and expired medicines was based on a key medicines list developed for
the Level II survey, selected according to the first-line therapeutic choice for the most common and
important health conditions at the primary health care level (Box 1).

WHO Level II Assessment - Health Facility and Household Surveys Barbados
25
Box 1. Key medicines selected for the survey
Diseases/Symptoms Medicines (INN) dosage form
1. Analgesic/fever Aspirin tab. 81 mg
2. Analgesic/fever Paracetamol syr. 125 mg/ 5 ml
3. Inflammation Ibuprofen tab. 400mg
4. Hyperlipidemia Atorvastatin tab. 10 mg
5. Hyperlipidemia Simvastatin tab. 20 mg
6. Diabetes Glibenclamide tab. 5 mg
7. Diabetes Insulin, NPH vial
8. Diabetes Metformin tab. 500 mg
9. Gastro-intestinal disorders/ diarrhoea Oral rehydration salts granules/pre-mixed
10. Gastrointestinal disorders Ranitidine tab. 150 mg
11. Cardiovascular diseases Atenolol tab. 50 mg
12. Cardiovascular disorders Bendrofluazide tab. 2.5 mg
13.Cardiovascular disorders Enalapril tab. 20 mg
14. Respiratory disorders Beclomethasone inh. 50 mg
15. Respiratory disorders Salbutamol inh. 100 mcg
16. Infections Amoxicillin cap. 500 mg
Affordability of treatment for adults and children as well as compliance of prescribers to recommended
treatment protocols were performed considering tracer health conditions selected by the coordination
team (Box 2 and Box 3).
Box 2. Tracer conditions for compliance of prescribers to recommended treatment protocols/guidelines.
Tracer condition Medicines tracked Rationale*
Non-bacterial diarrhoea in
children under age 5
Oral Rehydration Salts
(ORS), antibiotic,
antidiarrhoeal and/or
antispasmodic
Clinical guidelines specifically refer to
correct rehydration of acute diarrhoea
cases
Mild/moderate (outpatient)
pneumonia in children
under age 5
Amoxicillin Defined as any type of lower
respiratory tract infection that authors
considered needing antibiotics.
Non-pneumonia Acute
Upper Respiratory Tract
Iinfection (UTRI) in patients
of any age
Any antibiotic Defined as any type of URTI that
authors considered not needing
antibiotics.„Common cold‟ and „sore
throat‟ cases were considered viral
URTI, i.e. not needing antibiotics.
* Medicines use in primary care in developing and transitional countries:
Fact Book summarizing results from studies reported between 1990 and 2006

WHO Level II Assessment - Health Facility and Household Surveys Barbados
26
Box 3: Tracer conditions for affordability
Tracer condition Medicine Treatment schedule
Total
amount
required
Children <2 yr: For the 1st
2 hr 240 mL; 3 x 240 mL
can be taken daily.
Children 2-5 yr For the 1st 2
hr 3 x 240 mL. Max: 6 x 240
mL daily,
Mild/moderate (outpatient)
pneumonia in children under
age 5
Amoxicillin
125mg/5ml
(millilitre )50mg/kg body mass/daily.
Every 8 hrs
1 week: 4.2 g
for a 2yo child
(weight 12kg*)
Non-pneumonia Acute Upper
Respiratory Tract Infection
(UTRI) in patients of any age
Paracetamol
500mg (cap/tab) 10mg/kg/body mass per
dose. Every 6-8 hours as
needed
5 days: 10.5 g
for an adult
(weight 70 kg)
*http://w w w .cdc.gov/grow thcharts/data/set1clinical/cj41c021.pdf
Oral
Rehydratation
Salts: When
needed for
children less
than 10%
dehydrated
Non-bacterial diarrhoea in
children under age 5
Dependent on
severity of
dehydration:
4 - 6 sachets
Data collection methods included patient and health worker interviews after oral consent, check list
guided observation and clinical and administrative documents review.
The survey was conducted after approval by the Ministry of Health. Local health managers were
contacted for specific approval and cooperation.
The field team consisted of 19 data collectors who were selected based on their qualification as data
collectors, medical students, research assistants, CAPE Students and retired Nurses, and one supervisor
who oversaw the process of data collection.
All data collectors were trained during a training course July, 14 to 17, 2010. Data collection took place
between July 19 and August 6, 2010.
Box 4 summarizes Level II indicators and lists the corresponding survey forms. Information on data
collection and calculation can be found on the respective survey forms. Only forms which applied to the
Barbados situation were used.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
27
Box 4. Summary list of indicators and corresponding survey form used to collect the data
Indicator Survey Form
Access
1 Availability of key medicines in public health facility dispensaries, private pharmacies and warehouses supplying the public sector
1, 10, 15
2 % of prescribed key medicines dispensed or administered to patients at public health facility dispensaries
6
3 Average stock-out duration in public health facility dispensaries and warehouses supplying the public sector
4, 16
4 Adequate record keeping in public health facility dispensaries and warehouses supplying the public sector
4, 16
5 Affordability of treatment for adults and children under 5 years of age at public health facility dispensaries and private pharmacies
3, 12
8 Average cost of medicines at public health facilities and private pharmacies 6, 14
9 Geographical accessibility of public health facility dispensaries and private pharmacies 6, 14
Quality
1 % medicines expired in public health facility dispensaries, private pharmacies and warehouses supplying the public sector
1, 10, 15
2 Adequacy of storage conditions and of handling of medicines in public health facility dispensaries and warehouses supplying the public sector
5, 13, 17
Rational use of medicines
1 % medicines adequately labelled at public health facility dispensaries and private pharmacies
6, 14
2 % patients informed on how to take medicines at public health facility dispensaries and private pharmacies
6, 14
3 Average number of medicines per prescription at public health facility dispensaries and public health facilities
6, 7
4 % patients prescribed antibiotics in public health facilities 7
5 % patients prescribed injections in public health facilities 7
6 % prescribed medicines on the essential medicines list at public health facilities 7
7 % medicines prescribed by generic name (INN) at public health facilities 7
8 Availability of standard treatment guidelines at public health facilities 8
9 Availability of essential medicines list at public health facilities 8
10 % tracer cases treated according to recommended treatment protocol/guide at public health facilities
9
11 % prescription medicines bought with no prescription 14
Other information
1 % of facilities that comply with the law (presence of a pharmacist) Section A, C
2 % facilities with pharmacist, nurse, pharmacy aide/ health assistant or untrained staff dispensing
Section A, C
3 % facilities with doctor, nurse, trained health worker/health aide prescribing Section B
4 % facilities with prescriber trained in Rational Medicines Use (RMU) Section B
Data collection was performed on the data forms provided in the WHO survey package. After data
collection, summaries were calculated manually on each survey form. Then, values were entered in the
automated WHO Excel spread sheet of Summary Forms which automatically calculated indicators
presented here.
In this report, results at the national level are expressed as median, followed by percentiles 25 and 75.
With regard to the analysis, the national median was only calculated if there was information from at
least four facilities in each category (public or private). Data from patient interviews were only
considered for health facilities with at least 10 interviews completed, which was the case in all facilities.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
28
Limitations of the study
The study was not intended to give a detailed analysis of the pharmaceutical sector but rather to provide
an overview of the national pharmaceutical situation in Barbados. The study represents a tool for policy
analysis and the design of appropriate interventions.
The survey has been designed to draw a picture of the national pharmaceutical situation in Barbados.
The regions and facilities selected cumulatively represent the national situation.
The sample sizes are statistically not large enough to make inter-facility comparisons with some
indicators. This survey uses all facilities in the sample areas. From the data collected, no geographic
comparisons can be made.
Household Survey
This study was conducted using an adaptation of the standardized methodology developed by the World
Health Organization (WHO), which uses health facilities included in Level II survey as nucleus to define
the clusters of the household survey.
Given the Barbados geographic context, the standard method could not be used. Instead, a multi stage
cluster sample design was applied, with cluster sizes of 7 households each. The clusters were drawn in
two stages.
The two stage cluster sample was drawn in the following way:
1. A systematic sample of census enumeration blocks within each parish, with a random start and
an appropriate sampling interval for each parish (figure 2).
2. A systematic sample of 7 households within each census enumeration block drawn in stage 1.
Households were selected through a random start and an appropriate sampling interval for each
census enumeration block. These 7 randomly selected households constitute the cluster.
The distribution of the number of clusters in Barbados is shown on Figure 1. The sample was a stratified
random sampling. The Figure 2 exemplifies one random area to show how households were identified.
Figure 1. Geographic location of statistical sample areas, Barbados, 2010.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
29
Figure 2. Stratified Random sampling area identifying households, Barbados, 2010.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
30
Interviewers were trained to use judgment in selecting respondents. Respondents were selected if they
met at least three of the following criteria:
Main health care decision maker
Household member most knowledgeable in health
Household member most knowledgeable in household health expenditures
Household member most knowledgeable in household health utilization
Designated care giver for sick household members
The survey team consisted of a survey manager and 19 data collectors. Most data collectors were
medical students of the University of the West Indies and other higher tertiary institutions, mainly
Queens and Harrison College Advanced Level Students. All survey personnel received training in the
standard survey methodology, data collection and data entry procedures at a workshop held on July 14-
16, 2010 in Bridgetown. As part of the workshop, a data collection pilot test was conducted in
households which did not form part of the survey sample.
Data collection took place between 19 July and 6 August 2010. The data collectors were divided in 6
groups for the household group and 4 groups for the facilities group. All households and facilities were
surveyed by two data collectors.
An Excel spreadsheet displaying quintiles of monthly household expenditures by number of household
members in Barbados was distributed to data collectors during the training workshop. (Annex 3, page
85) This spreadsheet was used to describe categories A, B, C, D, and E of Question 37 during interviews
with household respondents. At the end of each day of data collection all completed questionnaires were
checked by the survey manager. Upon completion of the survey, the survey manager managing the
household survey and the BDS staff managing the facilities survey conducted a quality control check of
all completed questionnaires prior to data entry.
Survey data entry was performed by the survey manager with the assistance of the data collectors.
Epidata software was used for data entry. Entry was checked by entering twice 100% of the
questionnaires using the double data entry functions of Epidata; erroneous entries and potential outliers
were verified and corrected as necessary.
Epidata records were exported into an Excel workbook containing macros and formulas that
automatically generated the tables and figures contained in this report.
WHO Level II Assessment - Health Facility and Household Surveys Barbados
31
Results and Discussion
First, results from the health facility survey are presented, followed by results from the household
survey. The results are presented in the format of groups of indicators. Key issues are highlighted in
each group.
Health Facility Survey
Issues related to the field work
The location of the facilities surveyed is presented in Table 1.
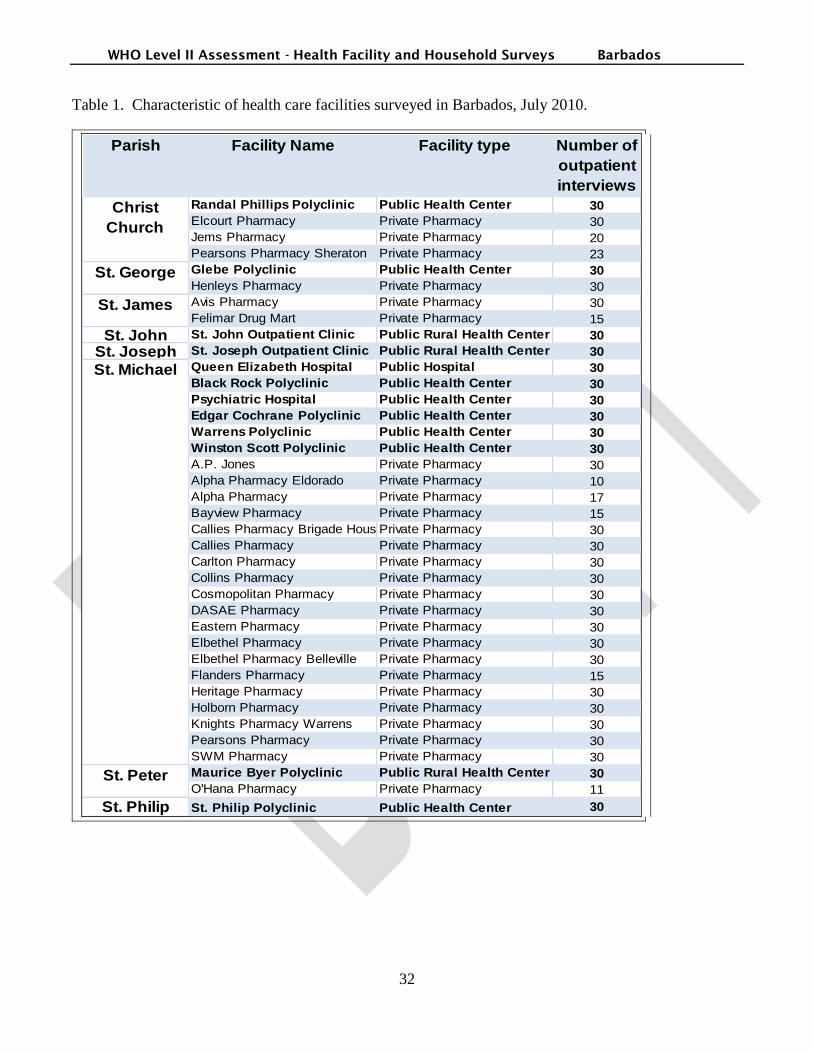
WHO Level II Assessment - Health Facility and Household Surveys Barbados
32
Table 1. Characteristic of health care facilities surveyed in Barbados, July 2010.
Parish Facility Name Facility type Number of
outpatient
interviews
Randal Phillips Polyclinic Public Health Center 30
Elcourt Pharmacy Private Pharmacy 30
Jems Pharmacy Private Pharmacy 20
Pearsons Pharmacy Sheraton Private Pharmacy 23
Glebe Polyclinic Public Health Center 30
Henleys Pharmacy Private Pharmacy 30
Avis Pharmacy Private Pharmacy 30
Felimar Drug Mart Private Pharmacy 15
St. John St. John Outpatient Clinic Public Rural Health Center 30
St. Joseph St. Joseph Outpatient Clinic Public Rural Health Center 30
Queen Elizabeth Hospital Public Hospital 30
Black Rock Polyclinic Public Health Center 30
Psychiatric Hospital Public Health Center 30
Edgar Cochrane Polyclinic Public Health Center 30
Warrens Polyclinic Public Health Center 30
Winston Scott Polyclinic Public Health Center 30
A.P. Jones Private Pharmacy 30
Alpha Pharmacy Eldorado Private Pharmacy 10
Alpha Pharmacy Private Pharmacy 17
Bayview Pharmacy Private Pharmacy 15
Callies Pharmacy Brigade HousePrivate Pharmacy 30
Callies Pharmacy Private Pharmacy 30
Carlton Pharmacy Private Pharmacy 30
Collins Pharmacy Private Pharmacy 30
Cosmopolitan Pharmacy Private Pharmacy 30
DASAE Pharmacy Private Pharmacy 30
Eastern Pharmacy Private Pharmacy 30
Elbethel Pharmacy Private Pharmacy 30
Elbethel Pharmacy Belleville Private Pharmacy 30
Flanders Pharmacy Private Pharmacy 15
Heritage Pharmacy Private Pharmacy 30
Holborn Pharmacy Private Pharmacy 30
Knights Pharmacy Warrens Private Pharmacy 30
Pearsons Pharmacy Private Pharmacy 30
SWM Pharmacy Private Pharmacy 30
Maurice Byer Polyclinic Public Rural Health Center 30
O'Hana Pharmacy Private Pharmacy 11
St. Philip St. Philip Polyclinic Public Health Center 30
Christ
Church
St. George
St. James
St. Michael
St. Peter
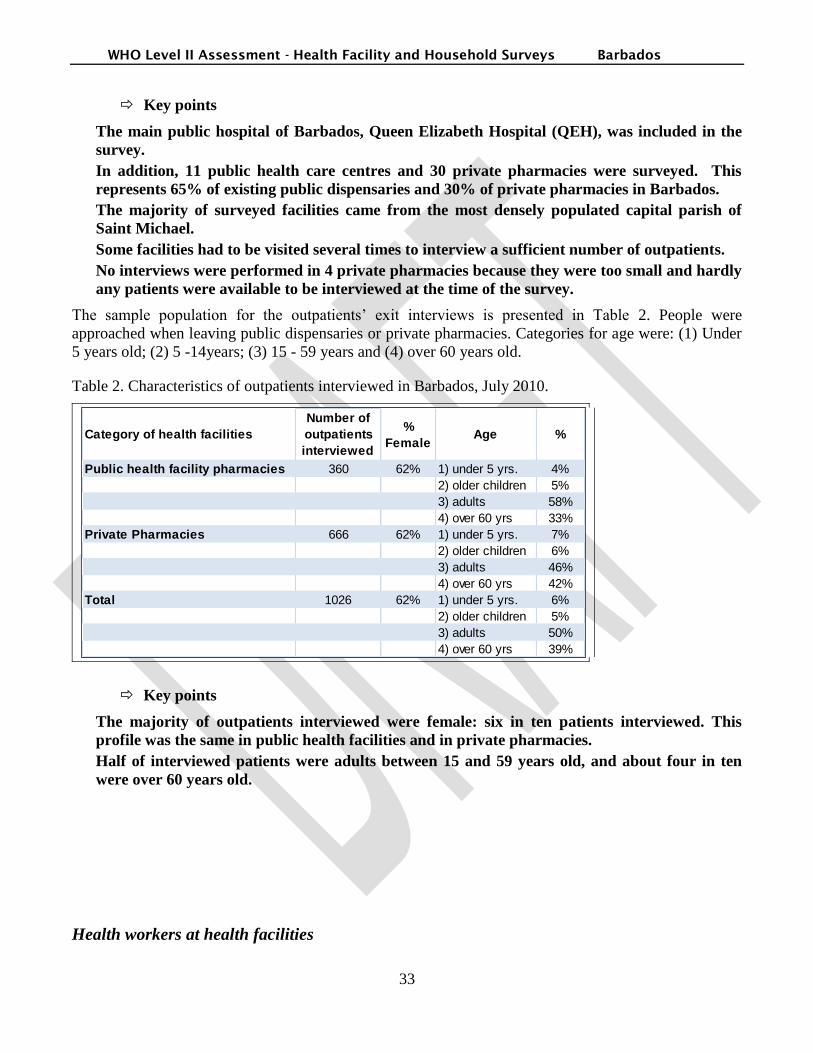
WHO Level II Assessment - Health Facility and Household Surveys Barbados
33
Key points
The main public hospital of Barbados, Queen Elizabeth Hospital (QEH), was included in the
survey.
In addition, 11 public health care centres and 30 private pharmacies were surveyed. This
represents 65% of existing public dispensaries and 30% of private pharmacies in Barbados.
The majority of surveyed facilities came from the most densely populated capital parish of
Saint Michael.
Some facilities had to be visited several times to interview a sufficient number of outpatients.
No interviews were performed in 4 private pharmacies because they were too small and hardly
any patients were available to be interviewed at the time of the survey.
The sample population for the outpatients‟ exit interviews is presented in Table 2. People were
approached when leaving public dispensaries or private pharmacies. Categories for age were: (1) Under
5 years old; (2) 5 -14years; (3) 15 - 59 years and (4) over 60 years old.
Table 2. Characteristics of outpatients interviewed in Barbados, July 2010.
Category of health facilities
Number of
outpatients
interviewed
%
FemaleAge %
Public health facility pharmacies 360 62% 1) under 5 yrs. 4%
2) older children 5%
3) adults 58%
4) over 60 yrs 33%
Private Pharmacies 666 62% 1) under 5 yrs. 7%
2) older children 6%
3) adults 46%
4) over 60 yrs 42%
Total 1026 62% 1) under 5 yrs. 6%
2) older children 5%
3) adults 50%
4) over 60 yrs 39%
Key points
The majority of outpatients interviewed were female: six in ten patients interviewed. This
profile was the same in public health facilities and in private pharmacies.
Half of interviewed patients were adults between 15 and 59 years old, and about four in ten
were over 60 years old.
Health workers at health facilities
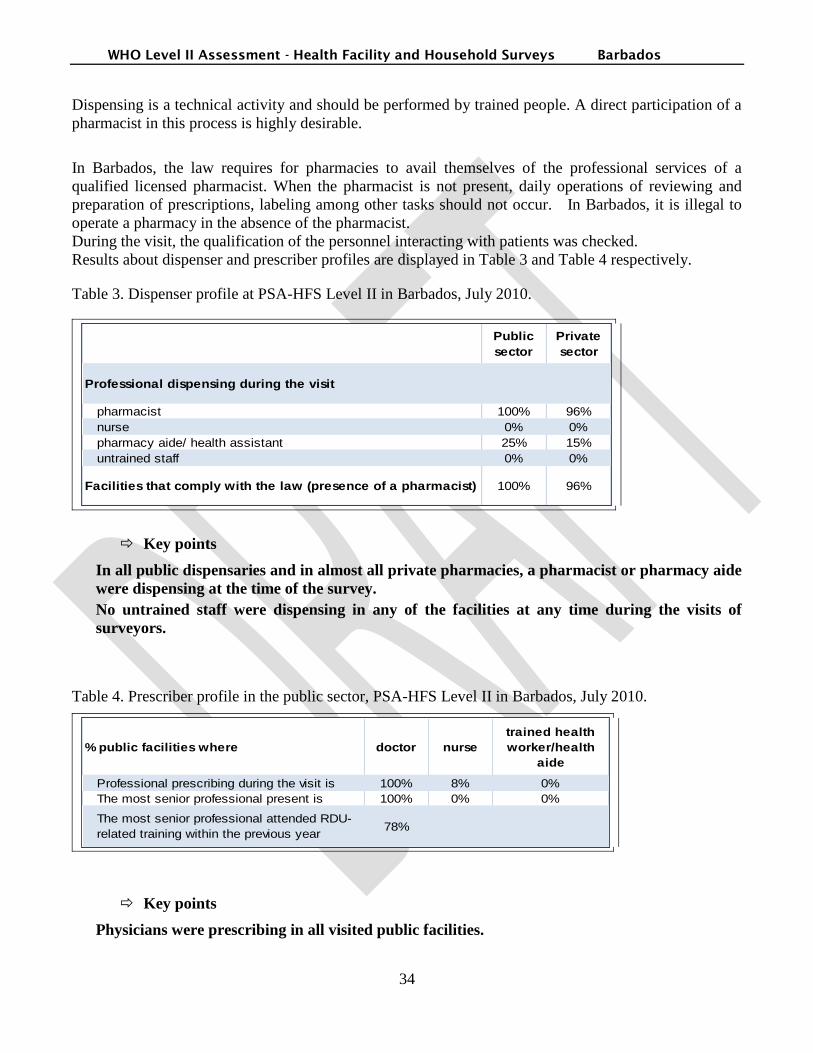
WHO Level II Assessment - Health Facility and Household Surveys Barbados
34
Dispensing is a technical activity and should be performed by trained people. A direct participation of a
pharmacist in this process is highly desirable.
In Barbados, the law requires for pharmacies to avail themselves of the professional services of a
qualified licensed pharmacist. When the pharmacist is not present, daily operations of reviewing and
preparation of prescriptions, labeling among other tasks should not occur. In Barbados, it is illegal to
operate a pharmacy in the absence of the pharmacist.
During the visit, the qualification of the personnel interacting with patients was checked.
Results about dispenser and prescriber profiles are displayed in Table 3 and Table 4 respectively.
Table 3. Dispenser profile at PSA-HFS Level II in Barbados, July 2010.
Public
sector
Private
sector
Professional dispensing during the visit
pharmacist 100% 96%
nurse 0% 0%
pharmacy aide/ health assistant 25% 15%
untrained staff 0% 0%
Facilities that comply with the law (presence of a pharmacist) 100% 96%
Key points
In all public dispensaries and in almost all private pharmacies, a pharmacist or pharmacy aide
were dispensing at the time of the survey.
No untrained staff were dispensing in any of the facilities at any time during the visits of
surveyors.
Table 4. Prescriber profile in the public sector, PSA-HFS Level II in Barbados, July 2010.
% public facilities where doctor nurse
trained health
worker/health
aide
Professional prescribing during the visit is 100% 8% 0%
The most senior professional present is 100% 0% 0%
The most senior professional attended RDU-
related training within the previous year78%
Key points
Physicians were prescribing in all visited public facilities.
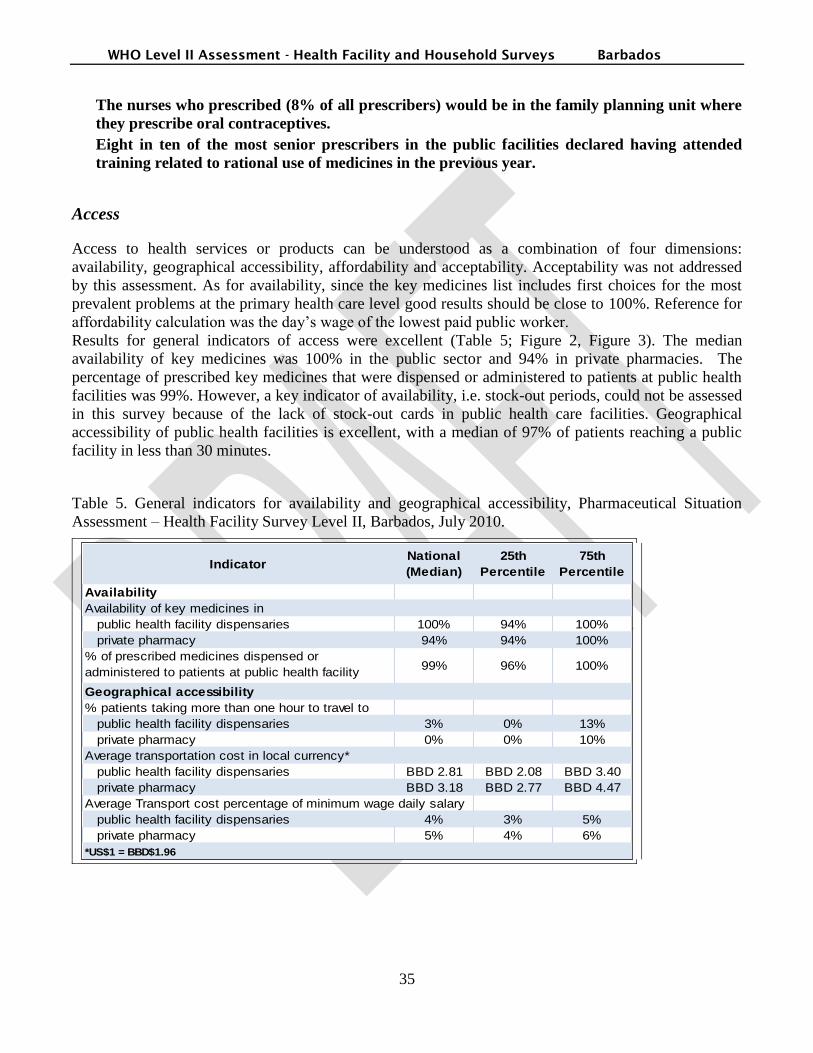
WHO Level II Assessment - Health Facility and Household Surveys Barbados
35
The nurses who prescribed (8% of all prescribers) would be in the family planning unit where
they prescribe oral contraceptives.
Eight in ten of the most senior prescribers in the public facilities declared having attended
training related to rational use of medicines in the previous year.
Access
Access to health services or products can be understood as a combination of four dimensions:
availability, geographical accessibility, affordability and acceptability. Acceptability was not addressed
by this assessment. As for availability, since the key medicines list includes first choices for the most
prevalent problems at the primary health care level good results should be close to 100%. Reference for
affordability calculation was the day‟s wage of the lowest paid public worker.
Results for general indicators of access were excellent (Table 5; Figure 2, Figure 3). The median
availability of key medicines was 100% in the public sector and 94% in private pharmacies. The
percentage of prescribed key medicines that were dispensed or administered to patients at public health
facilities was 99%. However, a key indicator of availability, i.e. stock-out periods, could not be assessed
in this survey because of the lack of stock-out cards in public health care facilities. Geographical
accessibility of public health facilities is excellent, with a median of 97% of patients reaching a public
facility in less than 30 minutes.
Table 5. General indicators for availability and geographical accessibility, Pharmaceutical Situation
Assessment – Health Facility Survey Level II, Barbados, July 2010.
IndicatorNational
(Median)
25th
Percentile
75th
Percentile
Availability
Availability of key medicines in
public health facility dispensaries 100% 94% 100%
private pharmacy 94% 94% 100%
% of prescribed medicines dispensed or
administered to patients at public health facility
dispensaries
99% 96% 100%
Geographical accessibility
% patients taking more than one hour to travel to
public health facility dispensaries 3% 0% 13%
private pharmacy 0% 0% 10%
Average transportation cost in local currency*
public health facility dispensaries BBD 2.81 BBD 2.08 BBD 3.40
private pharmacy BBD 3.18 BBD 2.77 BBD 4.47
Average Transport cost percentage of minimum wage daily salary
public health facility dispensaries 4% 3% 5%
private pharmacy 5% 4% 6%
*US$1 = BBD$1.96
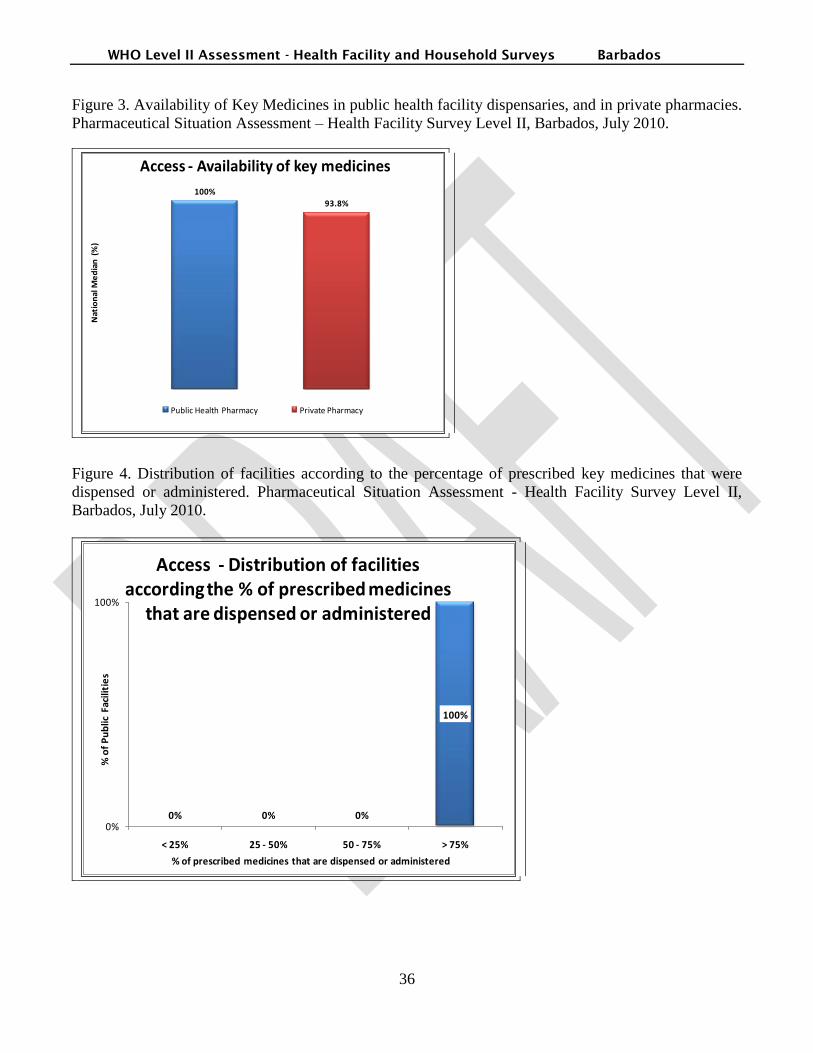
WHO Level II Assessment - Health Facility and Household Surveys Barbados
36
Figure 3. Availability of Key Medicines in public health facility dispensaries, and in private pharmacies.
Pharmaceutical Situation Assessment – Health Facility Survey Level II, Barbados, July 2010.
100%
93.8%
Nat
ion
al M
ed
ian
(%
)
Access - Availability of key medicines
Public Health Pharmacy Private Pharmacy
Figure 4. Distribution of facilities according to the percentage of prescribed key medicines that were
dispensed or administered. Pharmaceutical Situation Assessment - Health Facility Survey Level II,
Barbados, July 2010.
0% 0% 0%
100%
0%
100%
< 25% 25 - 50% 50 - 75% > 75%
% o
f P
ub
lic F
acili
tie
s
% of prescribed medicines that are dispensed or administered
Access - Distribution of facilities according the % of prescribed medicines
that are dispensed or administered
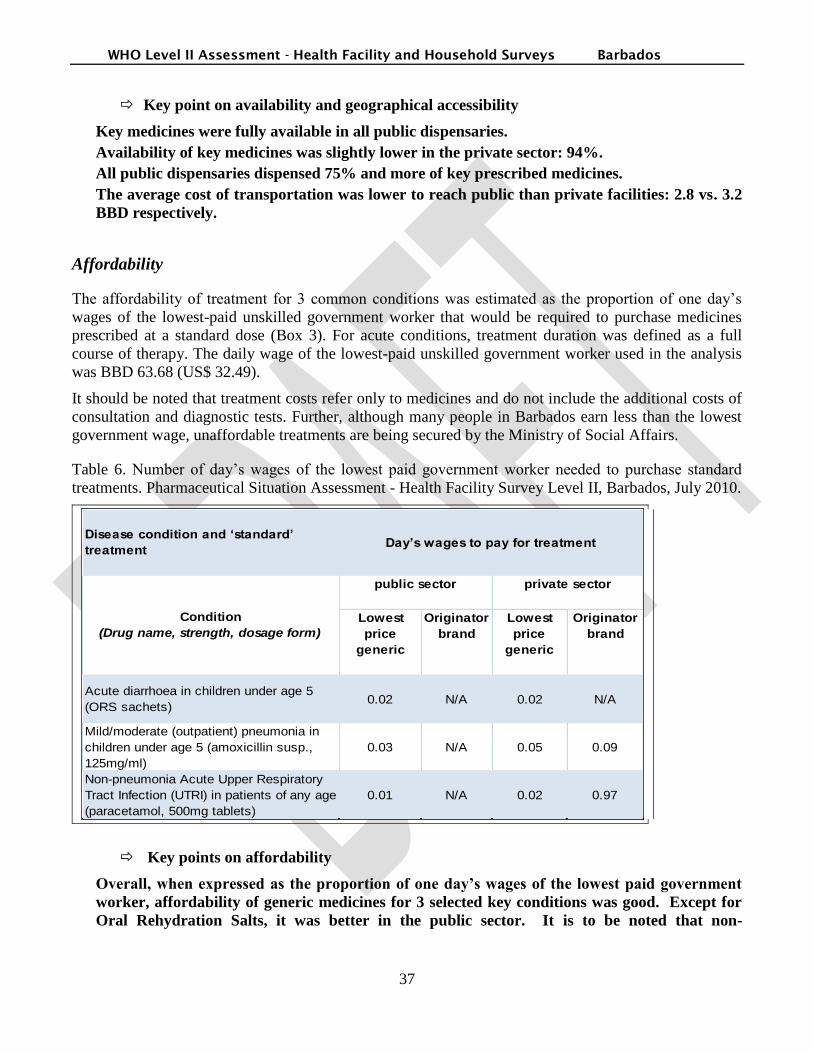
WHO Level II Assessment - Health Facility and Household Surveys Barbados
37
Key point on availability and geographical accessibility
Key medicines were fully available in all public dispensaries.
Availability of key medicines was slightly lower in the private sector: 94%.
All public dispensaries dispensed 75% and more of key prescribed medicines.
The average cost of transportation was lower to reach public than private facilities: 2.8 vs. 3.2
BBD respectively.
Affordability
The affordability of treatment for 3 common conditions was estimated as the proportion of one day‟s
wages of the lowest-paid unskilled government worker that would be required to purchase medicines
prescribed at a standard dose (Box 3). For acute conditions, treatment duration was defined as a full
course of therapy. The daily wage of the lowest-paid unskilled government worker used in the analysis
was BBD 63.68 (US$ 32.49).
It should be noted that treatment costs refer only to medicines and do not include the additional costs of
consultation and diagnostic tests. Further, although many people in Barbados earn less than the lowest
government wage, unaffordable treatments are being secured by the Ministry of Social Affairs.
Table 6. Number of day‟s wages of the lowest paid government worker needed to purchase standard
treatments. Pharmaceutical Situation Assessment - Health Facility Survey Level II, Barbados, July 2010.
Lowest
price
generic
Originator
brand
Lowest
price
generic
Originator
brand
0.02 N/A 0.02 N/A
0.03 N/A 0.05 0.09
0.01 N/A 0.02 0.97
Disease condition and ‘standard’
treatmentDay’s wages to pay for treatment
private sector
Condition
(Drug name, strength, dosage form)
public sector
Mild/moderate (outpatient) pneumonia in
children under age 5 (amoxicillin susp.,
125mg/ml)
Non-pneumonia Acute Upper Respiratory
Tract Infection (UTRI) in patients of any age
(paracetamol, 500mg tablets)
Acute diarrhoea in children under age 5
(ORS sachets)
Key points on affordability
Overall, when expressed as the proportion of one day’s wages of the lowest paid government
worker, affordability of generic medicines for 3 selected key conditions was good. Except for
Oral Rehydration Salts, it was better in the public sector. It is to be noted that non-
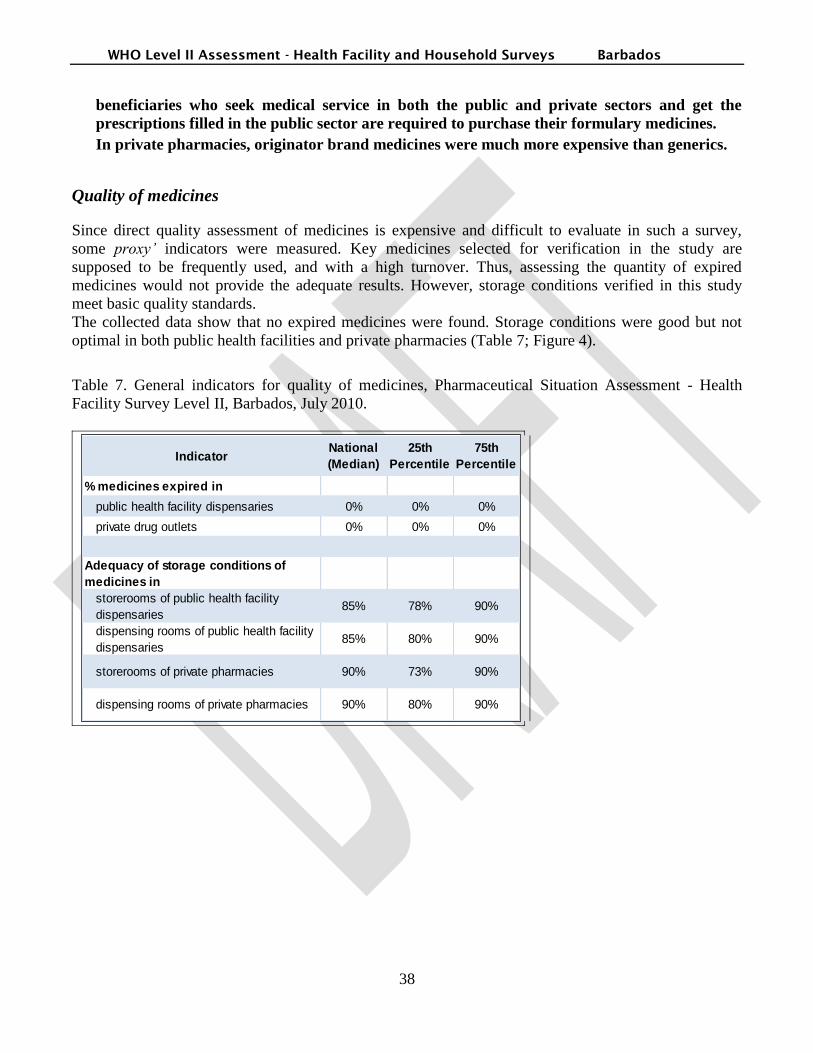
WHO Level II Assessment - Health Facility and Household Surveys Barbados
38
beneficiaries who seek medical service in both the public and private sectors and get the
prescriptions filled in the public sector are required to purchase their formulary medicines.
In private pharmacies, originator brand medicines were much more expensive than generics.
Quality of medicines
Since direct quality assessment of medicines is expensive and difficult to evaluate in such a survey,
some proxy’ indicators were measured. Key medicines selected for verification in the study are
supposed to be frequently used, and with a high turnover. Thus, assessing the quantity of expired
medicines would not provide the adequate results. However, storage conditions verified in this study
meet basic quality standards.
The collected data show that no expired medicines were found. Storage conditions were good but not
optimal in both public health facilities and private pharmacies (Table 7; Figure 4).
Table 7. General indicators for quality of medicines, Pharmaceutical Situation Assessment - Health
Facility Survey Level II, Barbados, July 2010.
IndicatorNational
(Median)
25th
Percentile
75th
Percentile
% medicines expired in
public health facility dispensaries 0% 0% 0%
private drug outlets 0% 0% 0%
Adequacy of storage conditions of
medicines in
storerooms of public health facility
dispensaries85% 78% 90%
dispensing rooms of public health facility
dispensaries 85% 80% 90%
storerooms of private pharmacies 90% 73% 90%
dispensing rooms of private pharmacies 90% 80% 90%

WHO Level II Assessment - Health Facility and Household Surveys Barbados
39
Figure 5. Adequacy of infrastructure of conservation conditions of medicines, Pharmaceutical Situation
Assessment - Health Facility Survey Level II, Barbados, and July 2010.
85%90%
85%90%
Storeroom Dispensing area
Nat
ion
al M
ed
ian
(%
)
QualityAdequacy of infrastructure of
conservation conditions of medicines
Public health pharmacy Private pharmacy
\zx\zx\\z
Key points on quality of medicines
No expired medicines were found in the public or private sectors.
Adequacy of infrastructure for conservation conditions of medicines in public health
pharmacies was 85% in both the storage and dispensing rooms.
Adequacy of infrastructure for conservation conditions of medicines in private pharmacies
was slightly better than in public pharmacies: 90% in both the storage and dispensing rooms.
Rational Use of Medicines (RUM)
According to WHO3, the target for indicators measuring the extent of adequate labeling, proportion of
prescribed medicines dispensed, adherence to treatment guidelines and availability of key medicines is
ideally 100%. However, internationally valid targets for other indicators, such as average number of
medicines per prescription, and the percentage use of antibiotics and injections, are more complex and
have not been empirically established. Targets may require modification over time and across countries.
A commonly used recommendation is to average 2 medicines per prescription, with less than 30% of
prescriptions including antibiotics and less than 20% including injections. The optimal values for these
indicators largely depend on disease patterns, policies, and treatment guidelines, and therefore may vary
3 WHO, (World Health Organization) (2006). Using indicators to measure country pharmaceutical situations: Fact Book
on WHO Level I and Level II monitoring indicators. Geneva, WHO.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
40
from country to country and over time. Average number of medicines per prescription was addressed by
two different methods: patient exit interview (cross sectional approach) and retrospective prescription
review (one year review).
The data concerning rational use of medicines (Table 8 and Table 9) show that the average number of
medicines per prescription is 3. The median percentage of patients prescribed with injections is 7%.
Although the median percentage of patients receiving antibiotics is 23%, the median percentage of
patients with tracer non-bacterial diseases treated with antibiotics is too high: 50%. Although the
majority of pharmacies did not sell prescription medicines without a prescription, surveyors found
several instances of prescription medicines sold by private pharmacies without prescription.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
41
Table 8. General indicators for rational use, Pharmaceutical Situation Assessment - Health Facility
Survey Level II, Barbados, July 2010.
IndicatorNational
(Median)
25th
Percentile
75th
Percentile
Prescribing indicators
Average number of medicines per prescription
at public health facility dispensaries and
public health facilities(SF6)
3.00 2.00 3.00
Average number of medicines per prescription
at public health facility dispensaries and
public health facilities(SF7)
3.07 2.82 4.40
% patients prescribed antibiotics in public
health facilities23% 13% 33%
% patients prescribed injections in public
health facilities7% 0% 13%
% prescribed medicines on the formulary at
public health facilities99% 97% 100%
% medicines prescribed by generic name
(INN) at public health facilities36% 25% 48%
Patient care indicators
% medicines adequately labeled at
public health facility dispensaries 100% 100% 100%
private dispensaries 100% 96% 100%
% patients know how to take medicines at
public health facility dispensaries 100% 100% 100%
private dispensaries 100% 100% 100%
% of prescription medicines bought without
prescription in private pharmacy0% 0% 7%
Facility specific factors for the rational use
of medicines
National
percentage
Availability of standard treatment guidelines at
public health facilities 55%
Availability of formulary at public health facilities 92%
Table 9. Distribution of private pharmacies according to their results on % prescription medicines
bought without prescription, Barbados, July 2010.
% prescription
medicines bought
without prescription
Number of
private
pharmacies
% of private
pharmacies
< 25% 24 92%
25 - 50% 2 8%
51 - 75% 0 0%
> 75% 0 0%
TOTAL 26 100%

WHO Level II Assessment - Health Facility and Household Surveys Barbados
42
Key points on rational use of medicines
The average number of medicines per prescription was close to 3 for both the exit interviews
and retrospective review of prescriptions.
In four out of the twelve public health facilities, over 30% of outpatient prescriptions included
an antibiotic.
In three out of twelve public health facilities, over 10% of outpatient prescriptions included an
injection.
Almost all prescribed medicines were on the national formulary.
Prescriptions using INN (generic name) are low, which does not correspond with the intended
policy.
Labeling of medicines was excellent both in the public and the private sector.
Most of the patients knew how to use their medicines.
About half of public health facilities did not have a copy of Standard Treatment Guidelines.
Ten of the 26 private pharmacies where interviews took place sold some prescription
medicines without prescription. In one pharmacy, 46% of prescription medicines were sold
without prescription.
Percentage of tracer cases treated according to recommended treatment protocol is presented in Table
10.
Table 10. Adherence of prescribers to recommended treatment guidelines. Pharmaceutical Situation
Assessment - Health Facility Survey Level II, Barbados, July 2010.
Indicator Information source Median
National
Average
Standard
Deviation
Non-bacterial diarrhoea
in children under age 5
Total number of
cases 99
% ORS 40% 35% 22%
% Antibiotics 20% 18% 14%
% Antidiarrhoeal and/or
Antispasmodic10% 25% 30%
Mild/moderate
pneumonia in children
under age 5
Total number of
cases40
% receiving any one
first line antibiotic32% 34% 37%
% receiving more than
one antibiotic17% 19% 21%
Non-pneumonia ARI in
patients of any age
Total number of
cases96
% Antibiotics 50% 54% 25%

WHO Level II Assessment - Health Facility and Household Surveys Barbados
43
Key points on rational prescription of medicines
Overall, results suggest the need for intensifying training of providers on rational prescribing.
Only four in ten children under five with diarrhea were prescribed Oral Rehydration Salts,
the recommended treatment. In addition it was not infrequent for providers to prescribe
unnecessary medicines for diarrhea: two in ten of these children received an antibiotic, and
about one in ten received an antispasmodic.
Few cases of pneumonia in children under 5 were available for review at the time of the
survey. Of the 40 cases reviewed, only a third was prescribed a first line antibiotic, which
appears far too low. However, because suspected cases of pneumonia in children under 5
years old are automatically and immediately referred from polyclinics to Queen Elizabeth
Hospital, the proportion of such cases receiving antibiotics may be higher than is reported in
this survey.
On the other hand, antibiotics were largely overused to treat non-pneumonia Acute
Respiratory Infection. Half of the patients of any age with ARI received antibiotics which is an
unusually high rate suggesting unnecessary use of antibiotics.
Challenges and constraints
Despite the presence of the pharmacist in most pharmacies, storage conditions of medicines need to be
improved as these were not optimal for public health facilities and private pharmacies. The
implementation of Good Practices related to distribution, storage and the Pharmacy Practices would
contribute to this.
In Barbados, medicines are generally available. The computerized system in place in the polyclinics is
quite remarkable and is likely responsible for the good performance in labeling. It can represent an asset
for monitoring the implementation of the proposed recommendations; Nevertheless, at policlinic
pharmacies, the previous stock-out information is not available. As there were no stock cards and only
current stock at hand can be retrieved, stock-out days could not be assessed. At Saint Michael
Psychiatric Hospital (SMPH), the percentage of adequate records was 100% and the average number of
stock out days was 0. At Queen Elizabeth Hospital (QEH), the percentage of adequate records was
slightly lower at 93.8%, and the average number of stock out days was high: 61 days. It is
recommended to improve the stock control in the computerized system to be able to retrieve previous
stock-out information.
International Non-proprietary Name (INN) drugs were used for only 36% of the prescription medicines
in public health facilities. Strategies for promoting the use of INN and incentives for prescribers can
contribute to the improvement of the use of generic medicines.
The rational use of medicines in private pharmacies is a matter of concern since ten of 26 private
pharmacies sold prescription medicines without a prescription.
There are STG for diabetes, hypertension and asthma which were available only in about half of
surveyed health facilities.
An important finding of the survey is the inappropriate prescription of antibiotics, which are underused
to treat pneumonia in children under 5, and overused to treat non-bacterial upper respiratory infections.
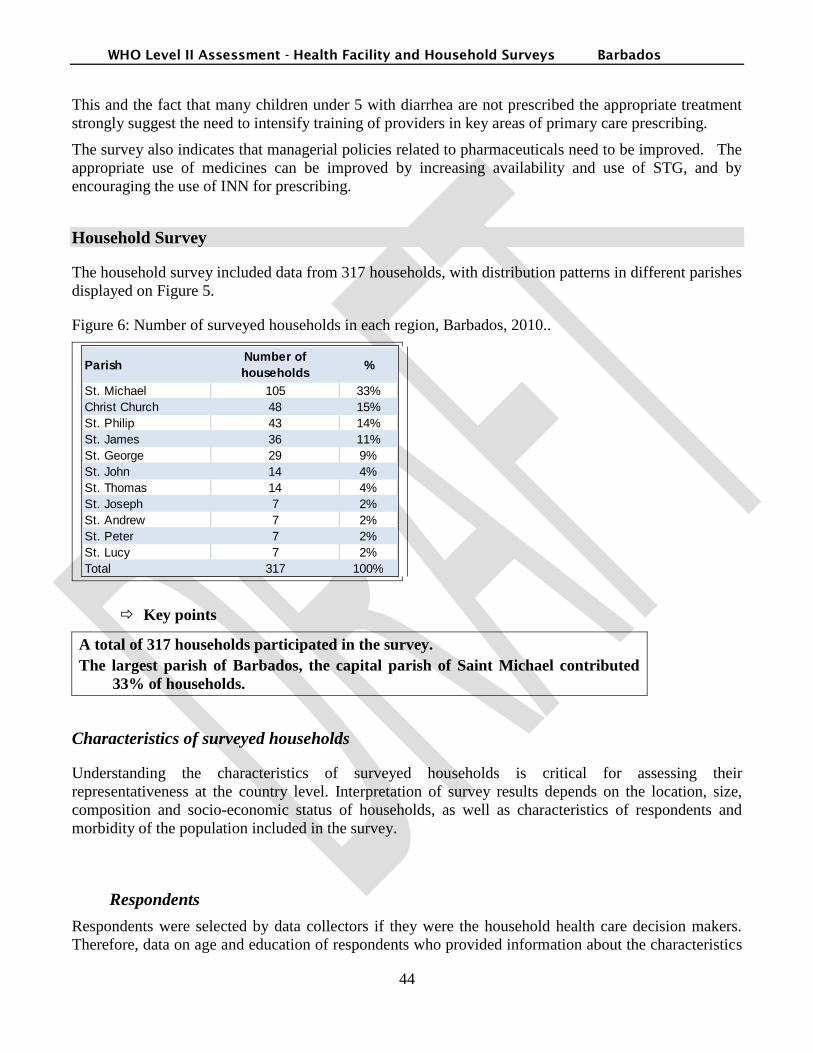
WHO Level II Assessment - Health Facility and Household Surveys Barbados
44
This and the fact that many children under 5 with diarrhea are not prescribed the appropriate treatment
strongly suggest the need to intensify training of providers in key areas of primary care prescribing.
The survey also indicates that managerial policies related to pharmaceuticals need to be improved. The
appropriate use of medicines can be improved by increasing availability and use of STG, and by
encouraging the use of INN for prescribing.
Household Survey
The household survey included data from 317 households, with distribution patterns in different parishes
displayed on Figure 5.
Figure 6: Number of surveyed households in each region, Barbados, 2010..
ParishNumber of
households%
St. Michael 105 33%
Christ Church 48 15%
St. Philip 43 14%
St. James 36 11%
St. George 29 9%
St. John 14 4%
St. Thomas 14 4%
St. Joseph 7 2%
St. Andrew 7 2%
St. Peter 7 2%
St. Lucy 7 2%
Total 317 100%
Key points
A total of 317 households participated in the survey.
The largest parish of Barbados, the capital parish of Saint Michael contributed
33% of households.
Characteristics of surveyed households
Understanding the characteristics of surveyed households is critical for assessing their
representativeness at the country level. Interpretation of survey results depends on the location, size,
composition and socio-economic status of households, as well as characteristics of respondents and
morbidity of the population included in the survey.
Respondents
Respondents were selected by data collectors if they were the household health care decision makers.
Therefore, data on age and education of respondents who provided information about the characteristics

WHO Level II Assessment - Health Facility and Household Surveys Barbados
45
of the main health care decision makers in households was collected. In addition, the profile of
respondents is important to interpret their opinions. Figure 6 presents the age of respondents, by gender.
Figure 7: Age of respondents/health care decision makers, Barbados, 2010.
1% 3%
14%
27%
19%
34%
0%
50%
100%
men women
Pe
rce
nta
ge o
f re
spo
nd
en
ts
<25 yo 25 to 50 yo >50 yo
Key points
Data collectors interviewed the person who was the most knowledgeable about matters related
to the health of household members.
Two third of respondents were women.
Over half of respondents were over 50 years old.
Table 11 presents the highest level of education reached by respondents.
Table 11: Education of respondents, Barbados, 2010.
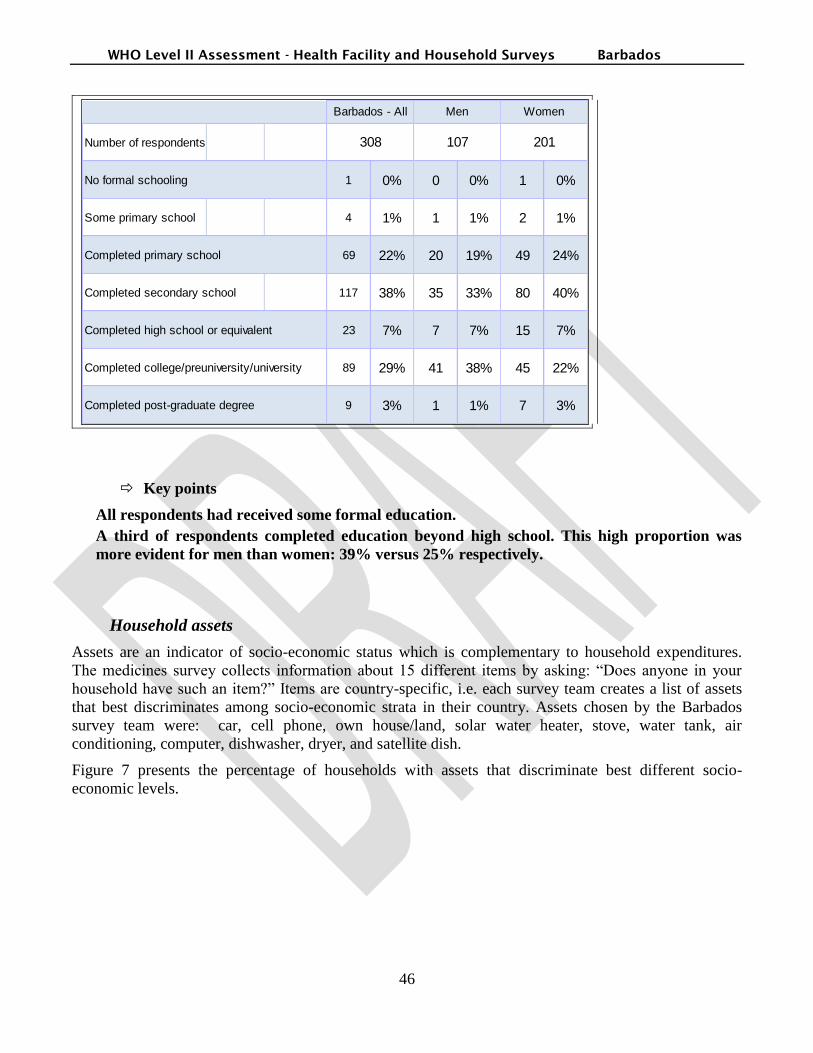
WHO Level II Assessment - Health Facility and Household Surveys Barbados
46
Number of respondents
No formal schooling 1 0% 0 0% 1 0%
Some primary school 4 1% 1 1% 2 1%
Completed primary school 69 22% 20 19% 49 24%
Completed secondary school 117 38% 35 33% 80 40%
Completed high school or equivalent 23 7% 7 7% 15 7%
Completed college/preuniversity/university 89 29% 41 38% 45 22%
Completed post-graduate degree 9 3% 1 1% 7 3%
Barbados - All Men Women
308 107 201
Key points
All respondents had received some formal education.
A third of respondents completed education beyond high school. This high proportion was
more evident for men than women: 39% versus 25% respectively.
Household assets
Assets are an indicator of socio-economic status which is complementary to household expenditures.
The medicines survey collects information about 15 different items by asking: “Does anyone in your
household have such an item?” Items are country-specific, i.e. each survey team creates a list of assets
that best discriminates among socio-economic strata in their country. Assets chosen by the Barbados
survey team were: car, cell phone, own house/land, solar water heater, stove, water tank, air
conditioning, computer, dishwasher, dryer, and satellite dish.
Figure 7 presents the percentage of households with assets that discriminate best different socio-
economic levels.
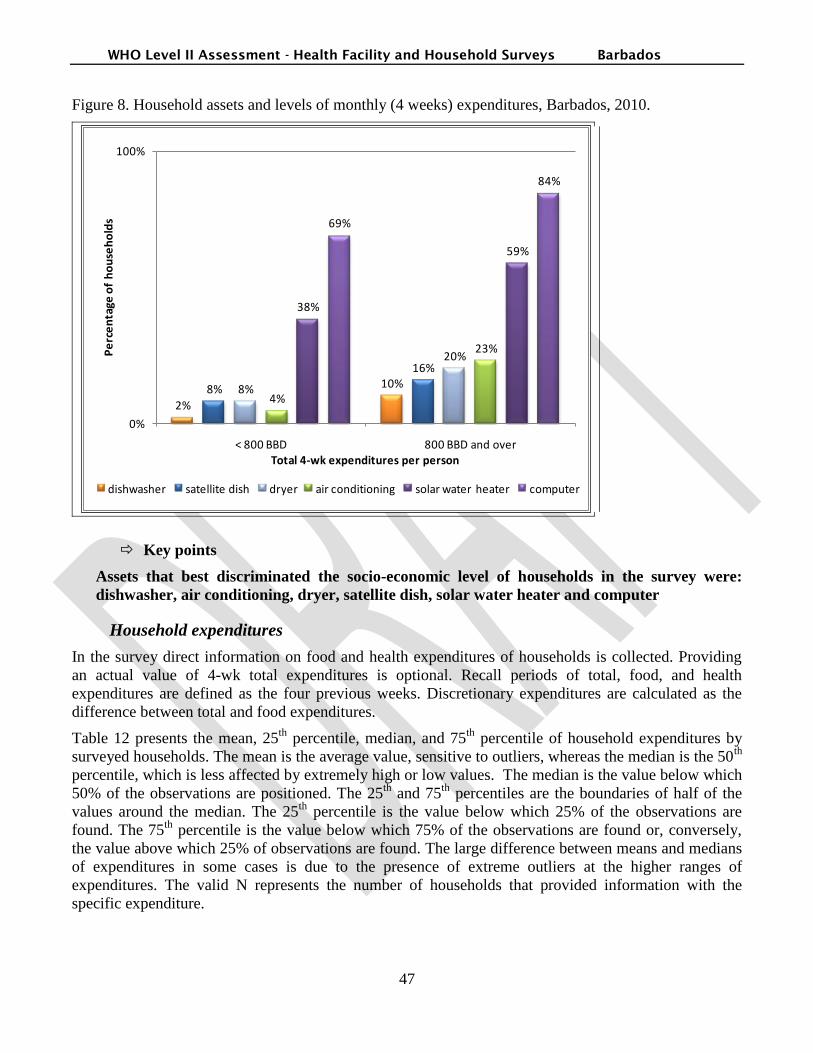
WHO Level II Assessment - Health Facility and Household Surveys Barbados
47
Figure 8. Household assets and levels of monthly (4 weeks) expenditures, Barbados, 2010.
2%
10%8%
16%
8%
20%
4%
23%
38%
59%
69%
84%
0%
100%
< 800 BBD 800 BBD and over
Pe
rce
nta
ge o
f h
ou
seh
old
s
Total 4-wk expenditures per person
dishwasher satellite dish dryer air conditioning solar water heater computer
Key points
Assets that best discriminated the socio-economic level of households in the survey were:
dishwasher, air conditioning, dryer, satellite dish, solar water heater and computer
Household expenditures
In the survey direct information on food and health expenditures of households is collected. Providing
an actual value of 4-wk total expenditures is optional. Recall periods of total, food, and health
expenditures are defined as the four previous weeks. Discretionary expenditures are calculated as the
difference between total and food expenditures.
Table 12 presents the mean, 25th
percentile, median, and 75th
percentile of household expenditures by
surveyed households. The mean is the average value, sensitive to outliers, whereas the median is the 50th
percentile, which is less affected by extremely high or low values. The median is the value below which
50% of the observations are positioned. The 25th
and 75th
percentiles are the boundaries of half of the
values around the median. The 25th
percentile is the value below which 25% of the observations are
found. The 75th
percentile is the value below which 75% of the observations are found or, conversely,
the value above which 25% of observations are found. The large difference between means and medians
of expenditures in some cases is due to the presence of extreme outliers at the higher ranges of
expenditures. The valid N represents the number of households that provided information with the
specific expenditure.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
48
Table 12: Monthly household expenditures, Barbados, 2010.
Valid N MeanPercentile
25Median
Percentile
75
4-wk hh total expenditures* 122 1,451 813 1,200 1,800
4-wk hh food expenditures* 290 693 400 600 800
4-wk discretionary expenditures
(e.g. total - food)*122 726 300 600 1,000
4-wk hh health expenditures* 82 251 71 128 250
4-wk hh hospital expenditures* 1 200 200 200 200
4-wk hh medicine expenditures* 43 102 20 52 84
4-wk hh other health expenditures* 24 229 70 103 200
4-wk hh voluntary health insurance
expenditures*40 262 90 134 260
* Barbados Dollar (BBD)
US$1=BBD$1.96
Key points
Less than half of households shared their actual total expenditures with surveyors.
One in four households (82/318) reported health expenditures over the past month. For these
households, the median spending on health was 128 BBD.
One in eight households (43/318) reported medicines expenditures over the past month. For
these households, the median spending on medicines was 52 BBD.
One in eight households (40/318) reported health insurance expenditures over the past month.
For these households, the median spending on health insurance was 134 BBD.
One household had spent 200 BBD on hospital expenditures during the previous month.
Household socio-economic status
Socio-economic status (SES) is a key attribute of households, influencing their options and decisions
about health care. In addition to collecting assets and expenditures data, socio-economic status can be
estimated by asking respondents to choose which level of expenditures best matches what their
household spends over a defined period of time.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
49
The medicines survey identifies poor households by asking respondents to match their household
expenditures with one of five pre-defined ranges (Annex 4, page 85). In Barbados, the lowest range of
expenditures was range A defined as spending less than 800 BBD per person per month. Range B
corresponded to spending between 800 and 1100 BBD per person per month, range C to spending
between 1101 and 1300 BBD per person and per month, range D to spending between 1301 and 1900
BBD per person per month. Range E was the highest possible range of expenditures, defined as
spending more than 1900 BBD per person per month. Respondents chose one of these five ranges of
expenditures that corresponded to the monthly total expenditures of their household. Very few
respondents identified their household in higher ranges.
Households were classified in two socio-economic categories: lower and higher socio-economic status
(SES) based on assets and expenditures criteria, as follows:
Group 1 called lower SES included all households that reported total expenditures below 800 BBD per
person over the past four weeks, and who did not possess any of the following assets: dishwasher, air
conditioning, dryer, satellite dish, or solar water heater. A total of 112 households belonged to this
group.
Group 2 called higher SES included all other households who reported expenditures directly or
indirectly and possessed at least one on the five most discriminating assets: dishwasher, air conditioning,
dryer, satellite dish, or solar water heater. A total of 160 households belonged to this group.
The remaining 46 households are not included in the analysis by SES presented in this report, because
they did not report their expenditures either by self-selecting a spending range or by providing an actual
total.
Figure 9 presents the distribution of the two SES groups in the survey, by parish.
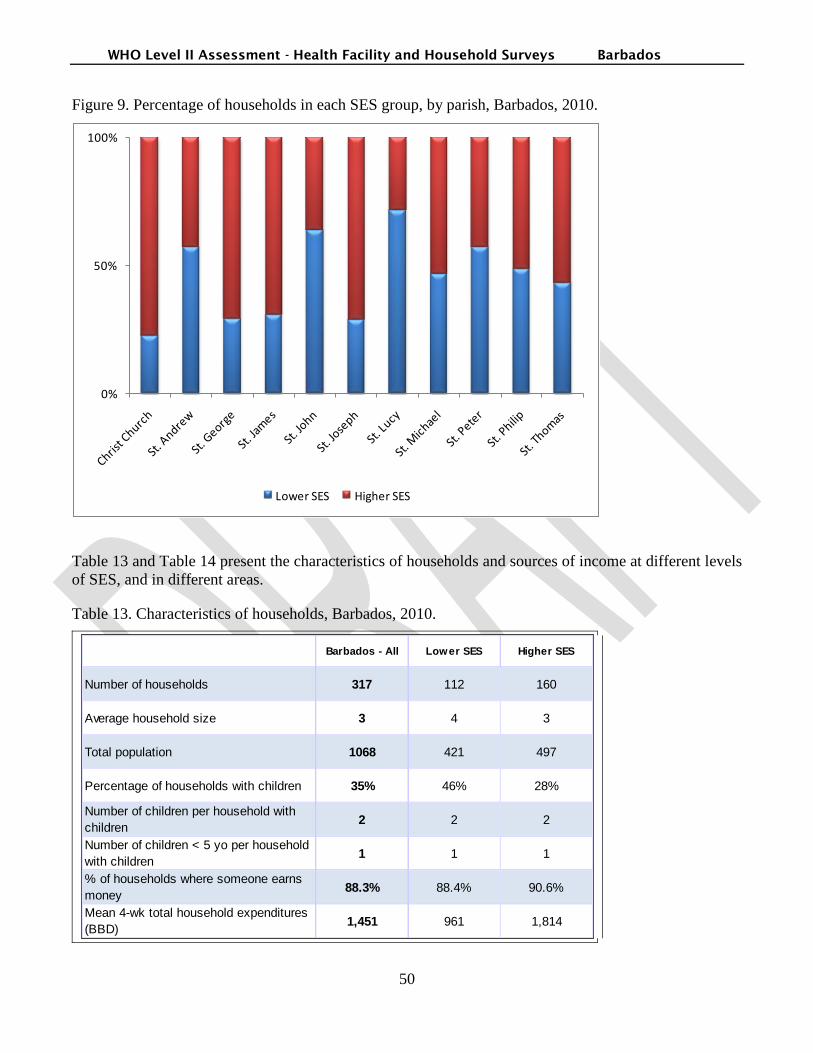
WHO Level II Assessment - Health Facility and Household Surveys Barbados
50
Figure 9. Percentage of households in each SES group, by parish, Barbados, 2010.
0%
50%
100%
Lower SES Higher SES
Table 13 and Table 14 present the characteristics of households and sources of income at different levels
of SES, and in different areas.
Table 13. Characteristics of households, Barbados, 2010.
Barbados - All Lower SES Higher SES
Number of households 317 112 160
Average household size 3 4 3
Total population 1068 421 497
Percentage of households with children 35% 46% 28%
Number of children per household with
children 2 2 2
Number of children < 5 yo per household
with children 1 1 1
% of households where someone earns
money 88.3% 88.4% 90.6%
Mean 4-wk total household expenditures
(BBD)1,451 961 1,814

WHO Level II Assessment - Health Facility and Household Surveys Barbados
51
Table 14. Sources of income and the job of the main earner in the household (household head),
Barbados, 2010.
Barbados - All Lower SES Higher SES
Unspecified 9% 10% 9%
Farmer 0% 0% 1%
Self-employed 11% 8% 14%
Civil servant 12% 16% 10%
Teacher 6% 5% 8%
Office worker 17% 16% 20%
Artisan 4% 6% 3%
Agricultural labor 1% 1% 1%
Non-agricultural labor 3% 6% 1%
Health worker 2% 2% 2%
Retired 31% 28% 30%
Key points
More households in the lower SES group had children: 46% vs. 28% in the higher SES group.
The average 4-week spending of households in the lower SES group was half that of
households in the higher SES group: 961 BBD vs. 1,814 BBD.
Overall, close to a third of the main household earners were retired.
A higher proportion of self-employed was observed in the higher SES group: 14% vs. 8% in
the lower SES group.
Household morbidity
The medicines survey collects information about household morbidity by asking respondents if a
member of the household had acute illness within two weeks preceding the survey and if a member of
the household has a chronic disease. If that is the case, data collectors collect health data on the youngest
member with a recent acute illness and on the oldest member with a chronic disease. They also ask how
many members had or have a recent acute illness or have a chronic disease.
Table 15 presents the prevalence of illnesses in surveyed households and Table 15 displays the average
number of illnesses in households with a sick member, as well as the age and gender of members whose
health information was collected.
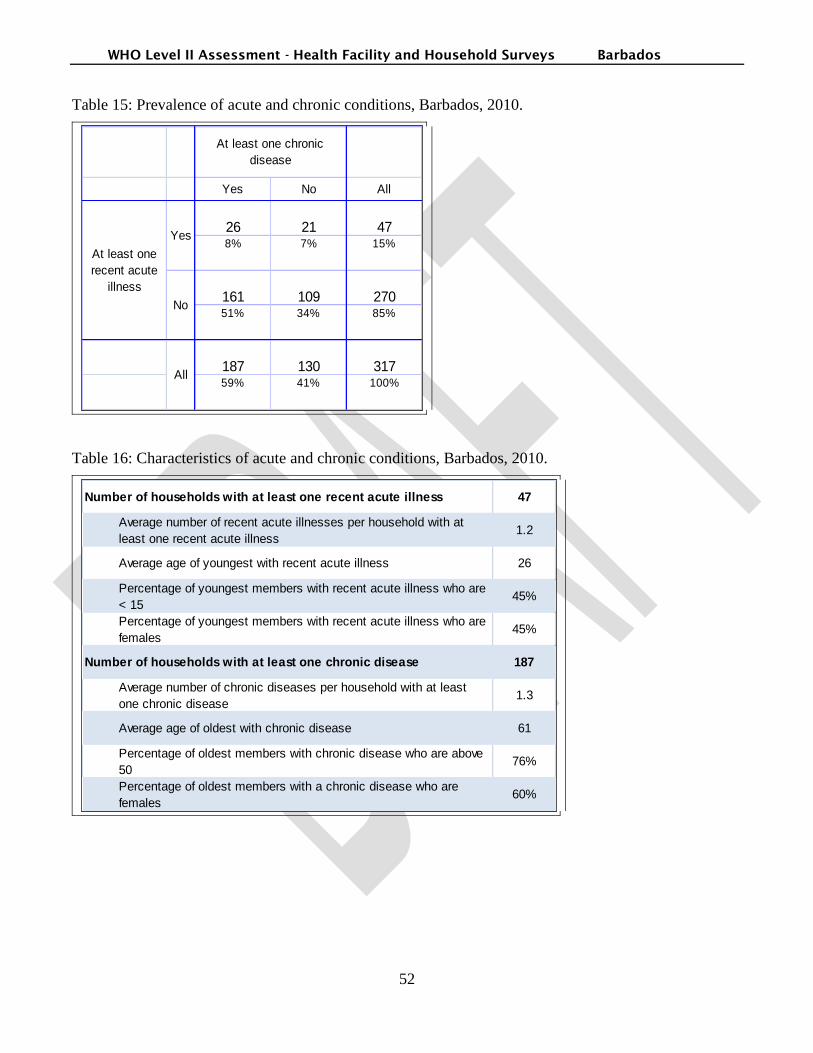
WHO Level II Assessment - Health Facility and Household Surveys Barbados
52
Table 15: Prevalence of acute and chronic conditions, Barbados, 2010.
Yes No All
26 21 478% 7% 15%
161 109 27051% 34% 85%
187 130 31759% 41% 100%
All
At least one
recent acute
illness
At least one chronic
disease
Yes
No
Table 16: Characteristics of acute and chronic conditions, Barbados, 2010.
Number of households with at least one recent acute illness 47
Average number of recent acute illnesses per household with at
least one recent acute illness1.2
Average age of youngest with recent acute illness 26
Percentage of youngest members with recent acute illness who are
< 1545%
Percentage of youngest members with recent acute illness who are
females45%
Number of households with at least one chronic disease 187
Average number of chronic diseases per household with at least
one chronic disease1.3
Average age of oldest with chronic disease 61
Percentage of oldest members with chronic disease who are above
5076%
Percentage of oldest members with a chronic disease who are
females60%
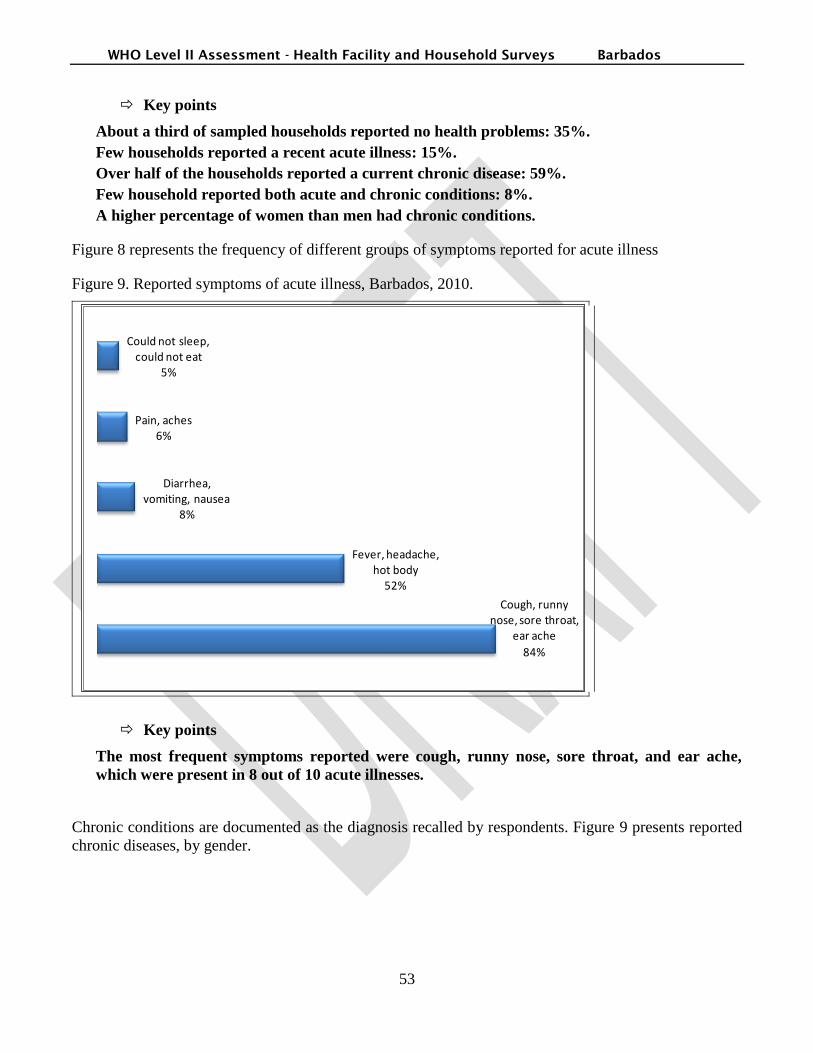
WHO Level II Assessment - Health Facility and Household Surveys Barbados
53
Key points
About a third of sampled households reported no health problems: 35%.
Few households reported a recent acute illness: 15%.
Over half of the households reported a current chronic disease: 59%.
Few household reported both acute and chronic conditions: 8%.
A higher percentage of women than men had chronic conditions.
Figure 8 represents the frequency of different groups of symptoms reported for acute illness
Figure 9. Reported symptoms of acute illness, Barbados, 2010.
Cough, runny nose, sore throat,
ear ache
84%
Fever, headache, hot body
52%
Diarrhea, vomiting, nausea
8%
Pain, aches6%
Could not sleep, could not eat
5%
Key points
The most frequent symptoms reported were cough, runny nose, sore throat, and ear ache,
which were present in 8 out of 10 acute illnesses.
Chronic conditions are documented as the diagnosis recalled by respondents. Figure 9 presents reported
chronic diseases, by gender.
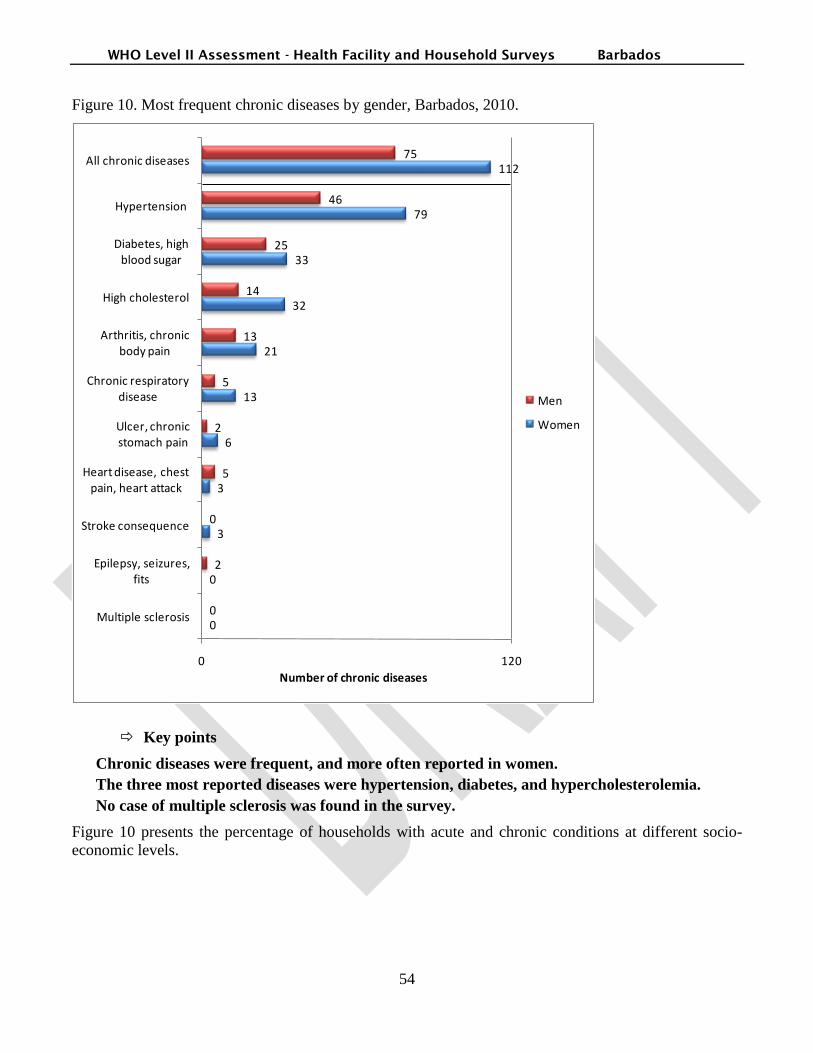
WHO Level II Assessment - Health Facility and Household Surveys Barbados
54
Figure 10. Most frequent chronic diseases by gender, Barbados, 2010.
0
0
3
3
6
13
21
32
33
79
112
0
2
0
5
2
5
13
14
25
46
75
0 120
Multiple sclerosis
Epilepsy, seizures, fits
Stroke consequence
Heart disease, chest pain, heart attack
Ulcer, chronic stomach pain
Chronic respiratory disease
Arthritis, chronic body pain
High cholesterol
Diabetes, high blood sugar
Hypertension
All chronic diseases
Number of chronic diseases
Men
Women
Key points
Chronic diseases were frequent, and more often reported in women.
The three most reported diseases were hypertension, diabetes, and hypercholesterolemia.
No case of multiple sclerosis was found in the survey.
Figure 10 presents the percentage of households with acute and chronic conditions at different socio-
economic levels.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
55
Figure 11: Prevalence of illnesses, Barbados, 2010.
15%
21%
12%
59%
67%
53%
0%
50%
100%
Barbados - All lower SES higher SES
Households with at least one recent acute illness
Households with at least one chronic disease
Key point
The prevalence of both acute and chronic conditions was higher in households of the lower
SES group.
Geographic access and availability of medicines
Geographic access to public health facilities is an important indicator to measure equity in access to
medicines.
Proximity to health care facilities
The medicines survey records the proximity of each household to different types of health care facilities,
using the time to travel as unit of distance. Facilities are classified into the following categories: public
hospital, private or NGO hospital, public health care center or dispensary, private clinic or physician,
traditional healer, or private pharmacy. For each facility, options to choose from were at less than 15
minutes, between 15 minutes and 1 hour, and over one hour of travel time.
Table 17 displays the proximity of households to any health care facility. Figure 11 presents the
proportion of households at more than 1 hour from a public health hospital or public health care center.
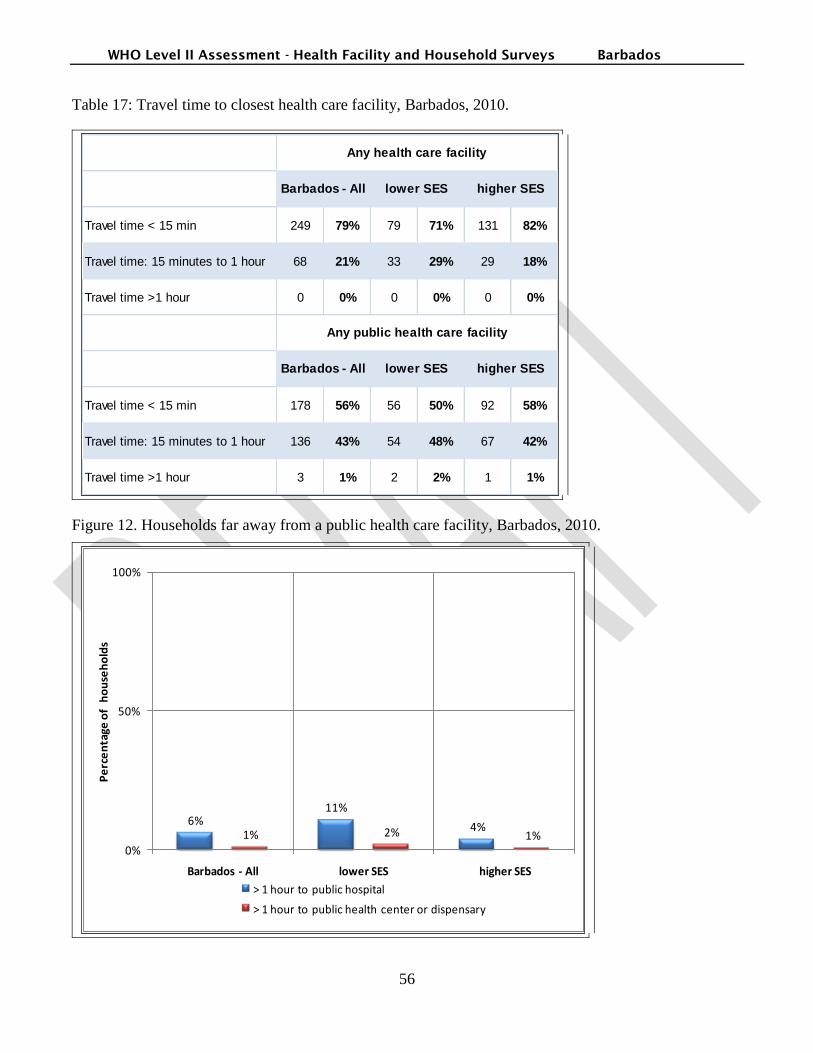
WHO Level II Assessment - Health Facility and Household Surveys Barbados
56
Table 17: Travel time to closest health care facility, Barbados, 2010.
Travel time < 15 min 249 79% 79 71% 131 82%
Travel time: 15 minutes to 1 hour 68 21% 33 29% 29 18%
Travel time >1 hour 0 0% 0 0% 0 0%
Travel time < 15 min 178 56% 56 50% 92 58%
Travel time: 15 minutes to 1 hour 136 43% 54 48% 67 42%
Travel time >1 hour 3 1% 2 2% 1 1%
Any health care facility
Any public health care facility
Barbados - All
Barbados - All lower SES higher SES
lower SES higher SES
Figure 12. Households far away from a public health care facility, Barbados, 2010.
6%11%
4%1% 2% 1%
0%
50%
100%
Barbados - All lower SES higher SES
Pe
rce
nta
ge o
f h
ou
seh
old
s
> 1 hour to public hospital
> 1 hour to public health center or dispensary

WHO Level II Assessment - Health Facility and Household Surveys Barbados
57
Key points
Overall, geographic access to health care and medicines was excellent.
All surveyed households were at less than 1 hour travel from a health care facility of any kind,
public or private.
Only 6% of households were located at more than one hour of travel time from a public
hospital. This percentage was higher in the lower SES group: 11%.
Sources of medicines found in households
Figure 12 presents the percentage of medicines found in households that were obtained in different types
of health care facilities, by SES group.
Figure 13. Sources of medicines found in households Barbados, 2010.
17%
30%
10%
74%
62%
82%
8% 7% 8%
0%
100%
Barbados - All Lower SES Higher SES
Pe
rce
nta
ge o
f m
ed
icin
es
Public health care facility Private pharmacy Other
Key points
Three in four medicines found in households came from a private pharmacy.
Less than 10% of medicines found at home were obtained from a private source other than a
pharmacy: private hospital, private provider, or herbalist.
More people in the lower SES group obtained their medicines from a public health care
facility: in this group, three in ten medicines found at home came from a public health care
facility vs. one in ten in the higher SES group.
Sources of medicines in case of acute illness

WHO Level II Assessment - Health Facility and Household Surveys Barbados
58
Figure 13 presents the sources of medicines in case of acute illness, by surveyed area.
Figure 14. Sources of medicines taken for an acute illness, Barbados, 2010.
16%19%
0%
76%
58%
74%
29%
23%26%
0%
100%
Barbados - All lower SES higher SES
Pe
rce
nta
ge o
f m
ed
icin
es
Public health care facility Private pharmacy Other
Key points
Like medicines found at home, three in four medicines obtained for acute illness came from a
private pharmacy.
Different from medicines found at home, 29% of medicines obtained for an acute illness came
from a private source other than a pharmacy: private hospital, private provider, or herbalist.
No one in the higher SES group obtained their medicines for acute illness from a public health
care facility.
Opinions about geographic access and availability of medicines
Table 18 presents the percentage of respondents who agreed with statements related to geographic
access and availability of medicines.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
59
Table 18: Opinions about geographic access and availability of medicine, Barbados, 2010.
Barbados -
All
Lower
SES
Higher
SES
Barbados
- All
Number of respondents 316 112 160 272
Agree Agree AgreeDon't
know
The public health care facility closest to my
household is easy to reach.87% 87% 88% 9%
My household would use public health care
facilities more if opening hours were convenient.49% 54% 43% 22%
The public health care facility closest to my
household usually has the medicines we need.53% 61% 48% 35%
The private pharmacy closest to my household
usually has the medicines my household needs.88% 84% 91% 9%
Key points
Close to nine in ten respondents agreed that their public health care facility is easy to reach.
Half of respondents would like facilities to have more convenient opening hours.
Overall, respondents felt that the availability of medicines is better in private pharmacies than
in public facilities. Almost nine in ten respondents agreed that their private pharmacy has the
medicines they need.
Only half of the respondents agreed that their public health care facility has the medicines they
need. This proportion was higher in the lower SES group: 61 % vs. 48% in the higher SES
group.
Affordability of medicines
Affordability of medicines is a critical indicator of equity in access to medicines. The level of medicine
insurance coverage and the actual cost of medicines for different conditions are important to consider
when assessing medicines affordability. The percentage of households experiencing potentially
catastrophic expenditures during the month preceding the survey provides a useful account of the
affordability of medicines in the surveyed population.
Cost of medicines for acute illnesses
In addition to collecting monthly household expenditures for medicines, information about the cost of
prescriptions for recent acute illnesses is collected. Table 19 presents the cost of prescriptions for acute
illnesses, by surveyed areas.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
60
Table 19: Cost of medicines for a recent acute illness, Barbados, 2010.
Barbados -
Alllower SES higher SES
Number of households with at least one acute illness 47 21 19
Number of persons with recent acute illness who took
medicines40 20 14
Number of housheolds who paid for the medicines 25 13 10
Average number of medicines by acute illness 1 1 2
Average cost of medicines when not free of charge BBD 28 BBD 25 BBD 34
Maximum cost of medicines for one acute illness BBD 170 BBD 100 BBD 170
Barbados Dollar (BBD)
US$1=BBD$1.96
Key points
Overall, a high proportion of people with acute illness took medicines.
Less people with an acute illness took medicines in the higher SES group, but when they did,
they took more medicines and paid more than people in the lower SES group.
The proportion of people with an acute condition who took medicines for this condition was
higher in the lower SES group: 20/21 than in the higher SES group: 14/19.
The average number of medicines per acute illness was 1 in the lower SES group and 2 in the
higher SES group.
For households who paid for medicines, the average cost of medicines for acute illness was 28
BBD (US$14.3). The average cost of medicines was higher for people in the higher SES group:
34 BBD vs. 25 BBD in the lower SES group.
Cost of medicines for chronic diseases
The medicines survey also collects information about the price of medicines taken for chronic diseases.
In this case, the monthly cost of each prescribed medicine is recorded.
Table 20 presents the monthly cost of medicines for chronic diseases, by surveyed areas.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
61
Table 20: Monthly cost of medicines for a chronic disease, Barbados, 2010.
Barbados
- All
lower
SES
higher
SES
Number of persons with chronic disease 187 75 85
Number of persons with chronic disease who take
medicines139 54 62
Number of persons who pay for medicines 18 1 16
Average number of medicines for a chronic disease 1 1 1
Average monthly cost of medicines for those who pay for
medicinesBBD 19 BBD 9.0 BBD 177
Maximum monthly cost of medicines for a chronic
diseaseBBD 1,500 BBD 9.0 BBD 1,500
US$1=BBD$1.96
Barbados Dollar (BBD)
Key points
Three in four persons diagnosed with a chronic disease took medicines
The average number of medicines taken for a chronic disease was 1.
Overall, 18/139 (13%) individuals with a chronic disease paid for the medicines they received.
Only one person with a chronic disease paid for medicines in the lower SES group, while 16/62
(26%) in the higher SES paid for their medicines.
The maximum monthly price of 1500 BBD was the cost an unidentified medicine taken by a
patient with cancer.
Even when excluding this outlier value, the monthly cost of medicines for patients with chronic
disease was ten times higher in the higher SES group. (data not shown)
Potentially catastrophic expenditures related to medicines
Potentially catastrophic expenditures are payments that may push people into poverty. They can be
expressed in different ways. In the survey, potentially catastrophic expenditures are calculated as
expenditures higher than 40% of discretionary expenditures.i Catastrophic expenditures could only be
calculated in the subgroup of 122 respondents who disclosed the actual amount of total expenditures by
their household during the month preceding the survey.
Figure 14 presents the percentage of households with catastrophic expenditures related to medicines
during the month preceding the survey.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
62
Figure 15. Potentially catastrophic expenditures related to medicines in month preceding survey,
Barbados, 2010.
12%10%
14%
3%2%
4%
0%
50%
Barbados - All Lower SES Higher SES
Pe
rce
nta
ge o
f h
ou
seh
old
s
Potentiallly catastrophic health expenditures
Potentiallly catastrophic medicines expenditures
Key points
In the survey, discretionary expenditures correspond to the difference between total spending
and spending on food. Expenditures are considered potentially catastrophic when they are
higher than 40% of discretionary expenditures.
Results show that 12% of households experienced potentially catastrophic health expenditures
in the month preceding the survey. A quarter of these were related to medicines expenditure.
Potentially catastrophic expenditures related to health and to medicines occurred more often
in the higher SES group than the lower SES group.
Medicines free-of-charge and insurance coverage
Table 21 presents the percentage of households with medicines insurance coverage for acute and chronic
conditions.
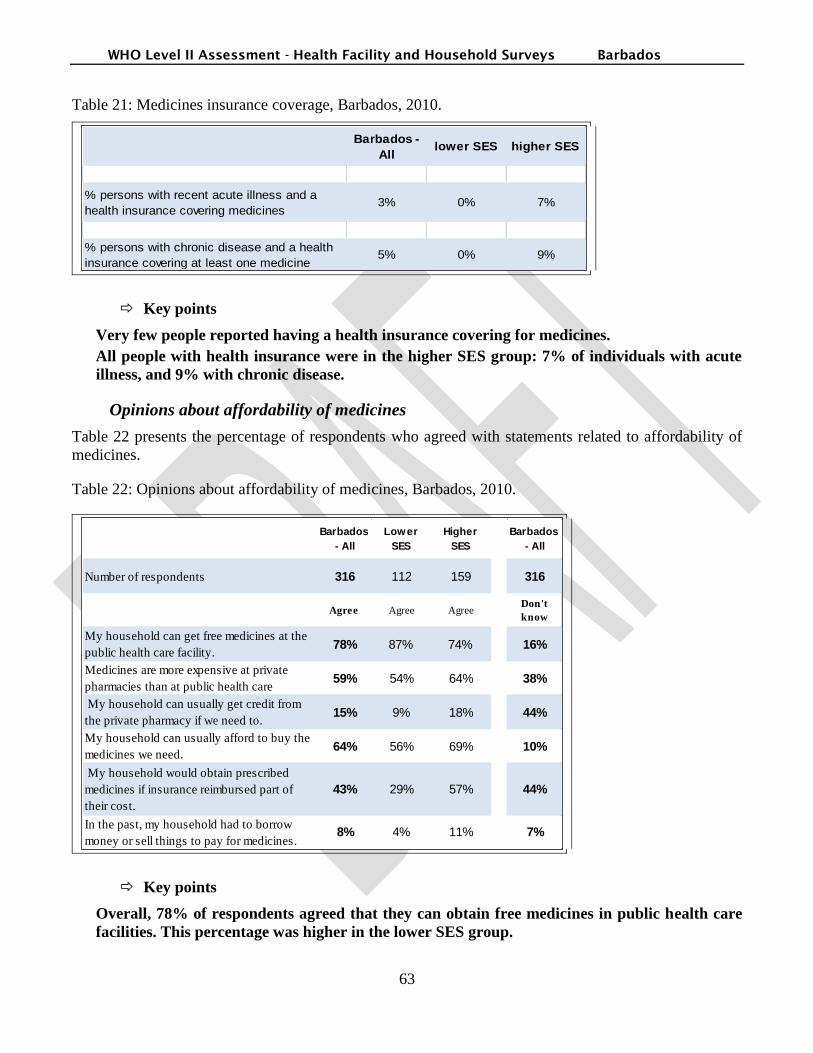
WHO Level II Assessment - Health Facility and Household Surveys Barbados
63
Table 21: Medicines insurance coverage, Barbados, 2010.
Barbados -
Alllower SES higher SES
% persons with recent acute illness and a
health insurance covering medicines3% 0% 7%
% persons with chronic disease and a health
insurance covering at least one medicine5% 0% 9%
Key points
Very few people reported having a health insurance covering for medicines.
All people with health insurance were in the higher SES group: 7% of individuals with acute
illness, and 9% with chronic disease.
Opinions about affordability of medicines
Table 22 presents the percentage of respondents who agreed with statements related to affordability of
medicines.
Table 22: Opinions about affordability of medicines, Barbados, 2010.
Barbados
- All
Lower
SES
Higher
SES
Barbados
- All
Number of respondents 316 112 159 316
Agree Agree AgreeDon't
know
My household can get free medicines at the
public health care facility. 78% 87% 74% 16%
Medicines are more expensive at private
pharmacies than at public health care
facilities.
59% 54% 64% 38%
My household can usually get credit from
the private pharmacy if we need to.15% 9% 18% 44%
My household can usually afford to buy the
medicines we need.64% 56% 69% 10%
My household would obtain prescribed
medicines if insurance reimbursed part of
their cost.
43% 29% 57% 44%
In the past, my household had to borrow
money or sell things to pay for medicines.8% 4% 11% 7%
Key points
Overall, 78% of respondents agreed that they can obtain free medicines in public health care
facilities. This percentage was higher in the lower SES group.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
64
Close to two thirds of respondents agreed that they can usually afford medicines. This
proportion fell to half of respondents in the lower SES group.
More households in the higher SES group reported having to borrow or sell items to pay for
medicines in the past: 11% vs. 4% in the lower SES group.
Medicines at home
The objective of the medicines survey is to understand which medicines people access and use, who
prescribes them, where they can be obtained, how much they cost and why people do or do not take
them. Collecting information on medicines kept at home contributes to answering these questions.
In each household, data collectors ask to see all medicines that are kept at home, and record the name,
source, reason for keeping each medicine, as well as the condition of their label and primary package.
Medicines are entered in the data base with both their originator brand actual and generic names, and a
code derived from the 16th
WHO Model List of Essential Medicines.ii
Number of households where medicines could be found
Figure 15 presents the percentage of households with children where medicines were found.
Figure 16. Medicines in households with children, Barbados, 2010.
73% 71%76%
80% 80% 82%
0%
50%
100%
Barbados - All Lower SES Higher SES
Pe
rce
nta
ge o
f h
ou
seh
old
s
all households households with children
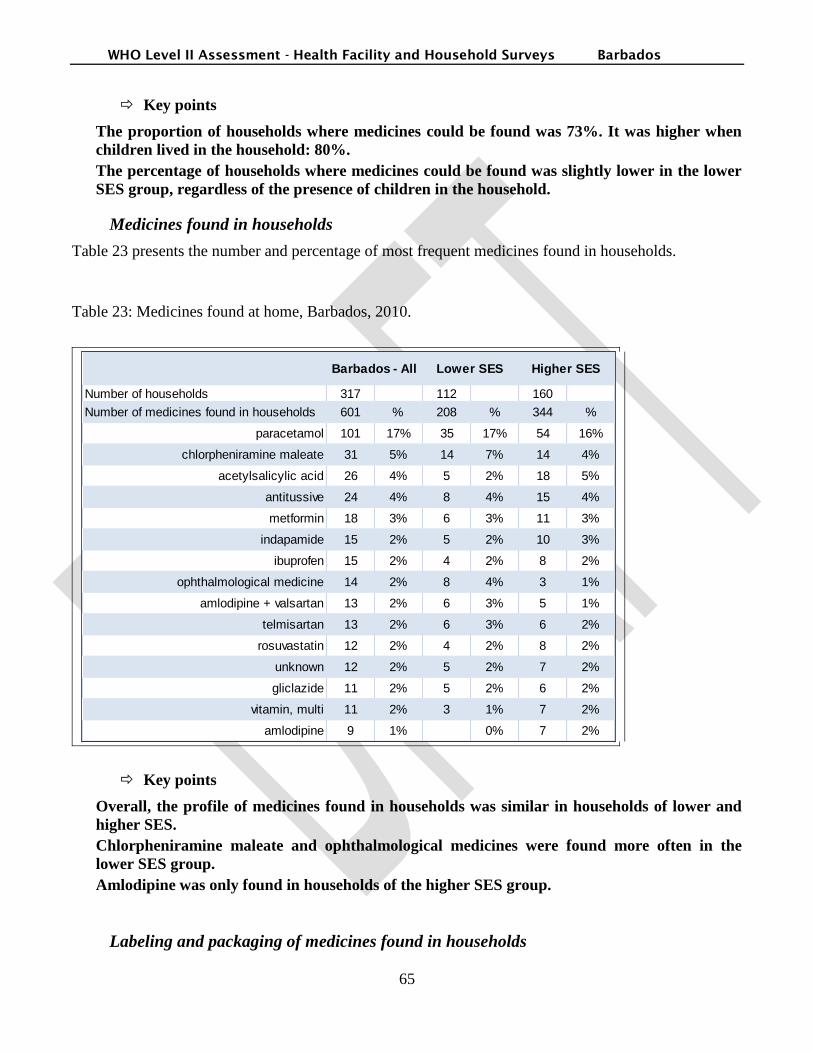
WHO Level II Assessment - Health Facility and Household Surveys Barbados
65
Key points
The proportion of households where medicines could be found was 73%. It was higher when
children lived in the household: 80%.
The percentage of households where medicines could be found was slightly lower in the lower
SES group, regardless of the presence of children in the household.
Medicines found in households
Table 23 presents the number and percentage of most frequent medicines found in households.
Table 23: Medicines found at home, Barbados, 2010.
Number of households 317 112 160
Number of medicines found in households 601 % 208 % 344 %
paracetamol 101 17% 35 17% 54 16%
chlorpheniramine maleate 31 5% 14 7% 14 4%
acetylsalicylic acid 26 4% 5 2% 18 5%
antitussive 24 4% 8 4% 15 4%
metformin 18 3% 6 3% 11 3%
indapamide 15 2% 5 2% 10 3%
ibuprofen 15 2% 4 2% 8 2%
ophthalmological medicine 14 2% 8 4% 3 1%
amlodipine + valsartan 13 2% 6 3% 5 1%
telmisartan 13 2% 6 3% 6 2%
rosuvastatin 12 2% 4 2% 8 2%
unknown 12 2% 5 2% 7 2%
gliclazide 11 2% 5 2% 6 2%
vitamin, multi 11 2% 3 1% 7 2%
amlodipine 9 1% 0% 7 2%
Barbados - All Lower SES Higher SES
Key points
Overall, the profile of medicines found in households was similar in households of lower and
higher SES.
Chlorpheniramine maleate and ophthalmological medicines were found more often in the
lower SES group.
Amlodipine was only found in households of the higher SES group.
Labeling and packaging of medicines found in households

WHO Level II Assessment - Health Facility and Household Surveys Barbados
66
Labels of medicines found in households are considered acceptable by data collectors if they include
medicine name, dose, and expiration date. Similarly, the primary package of a medicine is considered
acceptable if it is an envelope or a closable container which contains only one medicine.
Figure 16 presents the percentage of medicines that had an acceptable label, primary package and
validity, by source of medicine.
Figure 17. Percentage of home medicines with adequate label and primary package, by source,
Barbados, 2010.
82%87%
80%
94%
All medicines found at home
Obtained from a public facility
Obtained from a private pharmacy
Obtained from other source
% o
f m
ed
icin
es
wit
h a
de
qu
ate
lab
elin
g an
d p
rim
ary
pac
kage
Key points
Overall, about eight in ten medicines found in households had a label and primary package in
good condition.
Compared to medicines from private pharmacies, medicines from public health care facilities
were more likely to be appropriately labeled and to be kept in an adequate container
Use of medicines during acute illnesses

WHO Level II Assessment - Health Facility and Household Surveys Barbados
67
For each recent acute illness reported, data collectors record name, route of administration, prescriber,
and source of each medicine taken for this illness. Medicines are entered in the data base with both their
actual and generic names, and a code derived from the 16th
WHO Model List of Essential Medicines.
Actions taken when an acute illness occurs
Table 24 presents the actions taken in case of recent acute illness.
Table 24. Actions taken for a recent acute illness, Barbados, 2010.
Sick persons with an acute illness perceived as very severe 1
Went for care and took all prescribed medicines 1 100%
Went for care and took some of the prescribed medicines 0 0%
Went for care but did not take any medicines 0 0%
Did not go for care 0 0%
Sick persons with an acute illness perceived as moderately
severe14
Went for care and took all prescribed medicines 6 43%
Went for care and took some of the prescribed medicines 2 14%
Went for care but did not take any medicines 1 7%
Did not go for care 5 36%
Sick persons with an acute illness perceived as not severe 33
Went for care and took all prescribed medicines 6 18%
Went for care and took some of the prescribed medicines 0 0%
Went for care but did not take any medicines 0 0%
Did not go for care 27 82%
Key points
Overall, how an acute illness was treated depended on its perceived severity.
The person with a severe acute illness went for care and took all prescribed medicines.
Of people who had a moderately severe acute illness, 43% went for care and took all
prescribed medicines. This percentage fell to 18% when the acute illness was considered mild.
Medicines for acute illness

WHO Level II Assessment - Health Facility and Household Surveys Barbados
68
Table 25 presents the most frequent medicines taken in case of recent acute illness.
Table 25 Medicines taken for a recent acute illness, Barbados, 2010.
Generic
Count of generic
medicines for acute
illnesses
total 58
paracetamol 15 26%
chlorpheniramine maleate 13 22%
cold medicine 5 9%
loratadine 3 5%
diclophenac sodium 2 3%
Key points
The two most frequent medicines taken for an acute illness were paracetamol and
chlorpheniramine maleate.
Prescribers of medicines in case of acute illness
Figure 17 presents prescribers of medicines in case of acute illness, by different survey areas, Barbados,
2010.
Figure 18: Prescribers of medicines in case of acute illness, Barbados, 2010.
51%
44%
60%
49%
56%
40%
0%
100%
Barbados - All lower SES higher SESPe
rce
nta
ge o
f m
ed
icin
es
pre
scri
be
d f
or
acu
te i
llne
ss
Medicines prescribed by a doctor/nurse
Medicines prescribed by someone who is not a doctor or a nurse
WHO Level II Assessment - Health Facility and Household Surveys Barbados
69
Key points
Overall in the case of acute illness, half of medicines were prescribed by doctors or nurses.
This percentage was higher in the higher SES group: 60% vs 44%
Routes of administration of medicines prescribed for acute illness
Figure 18 presents the route of administration of medicines prescribed for acute illness, by different
survey areas.
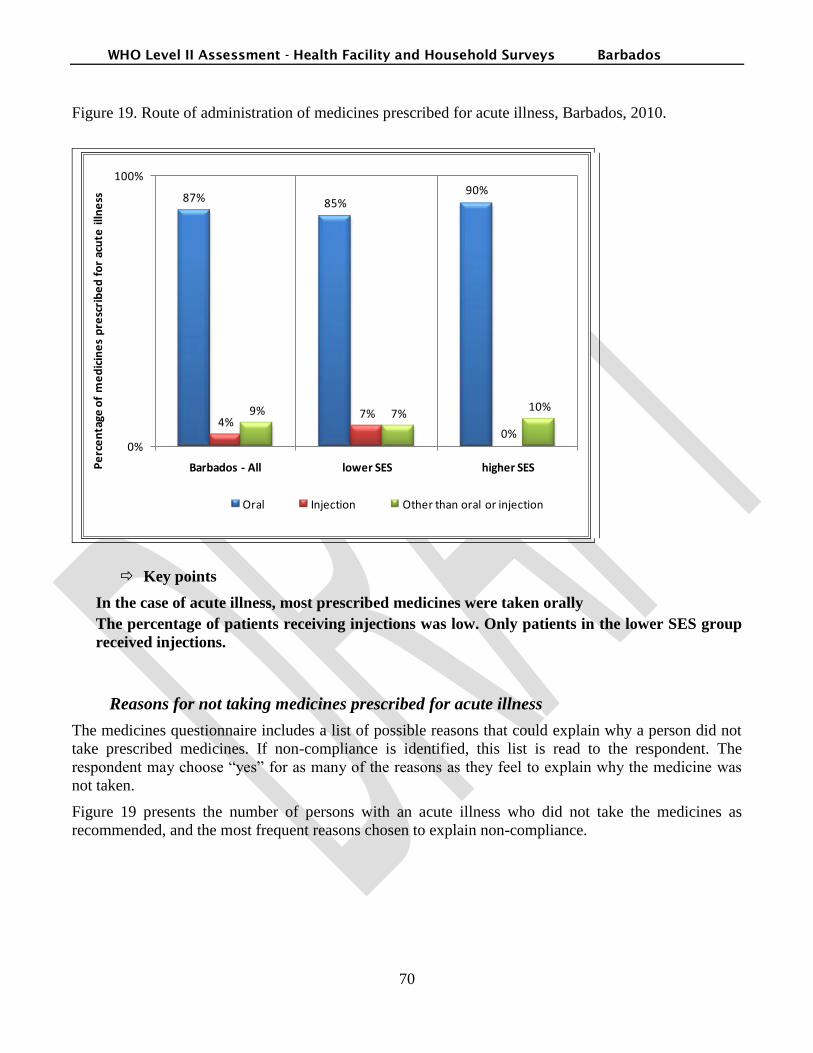
WHO Level II Assessment - Health Facility and Household Surveys Barbados
70
Figure 19. Route of administration of medicines prescribed for acute illness, Barbados, 2010.
87% 85%90%
4%7%
0%
9% 7%10%
0%
100%
Barbados - All lower SES higher SESPe
rce
nta
ge o
f m
ed
icin
es
pre
scri
be
d f
or
acu
te i
llne
ss
Oral Injection Other than oral or injection
Key points
In the case of acute illness, most prescribed medicines were taken orally
The percentage of patients receiving injections was low. Only patients in the lower SES group
received injections.
Reasons for not taking medicines prescribed for acute illness
The medicines questionnaire includes a list of possible reasons that could explain why a person did not
take prescribed medicines. If non-compliance is identified, this list is read to the respondent. The
respondent may choose “yes” for as many of the reasons as they feel to explain why the medicine was
not taken.
Figure 19 presents the number of persons with an acute illness who did not take the medicines as
recommended, and the most frequent reasons chosen to explain non-compliance.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
71
Figure 20. Reasons for not taking prescribed medicines for acute illness, Barbados, 2010.
18
6
12
14
3
8
1 10
0
20
Barbados - All lower SES higher SESNu
mb
er
of
pe
rso
ns
wit
h a
cute
illn
ess
wh
o d
id n
ot
take
m
ed
icin
es
as p
resc
rib
ed
Did not follow their prescription Symptoms had improved
Could not afford medicines
Key points
Of the 47 individuals with acute illness, 18 did not follow their prescription.
The most frequent reason (cited by 78% of people who did not follow their prescription) for
not taking medicines as prescribed was that symptoms had improved.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
72
One respondent in the lower SES group identified affordability of medicines as a reason for
non-compliance.
Use of medicines for chronic diseases
Over half of households (59%) reported at least one chronic disease. In households with a person
diagnosed with a chronic disease, data collectors recorded the name of each medicine prescribed to the
person with a chronic disease, the condition for which it was recommended, the number of days of
supply usually obtained, the usual cost for one month, and insurance coverage for every person with a
chronic disease.
Actions taken when a chronic disease has been diagnosed
Figure 20 presents actions taken in case of chronic disease.
Figure 21. Actions taken for chronic diseases, Barbados, 2010.
72%68%
71%
19% 17%23%
10%15%
6%
82%
69%
83%
Barbados - All lower SES higher SESWas told to take medicines and takes them as directed
Was told to take medicines and does not take them as directed
Was not told to take medicines
Was told to take medicines and medicines are found at home
Key points
Overall, three in four individuals with a chronic disease were told to take medicines and took
them as directed.
Large differences were observed between individuals in the lower and higher SES groups.
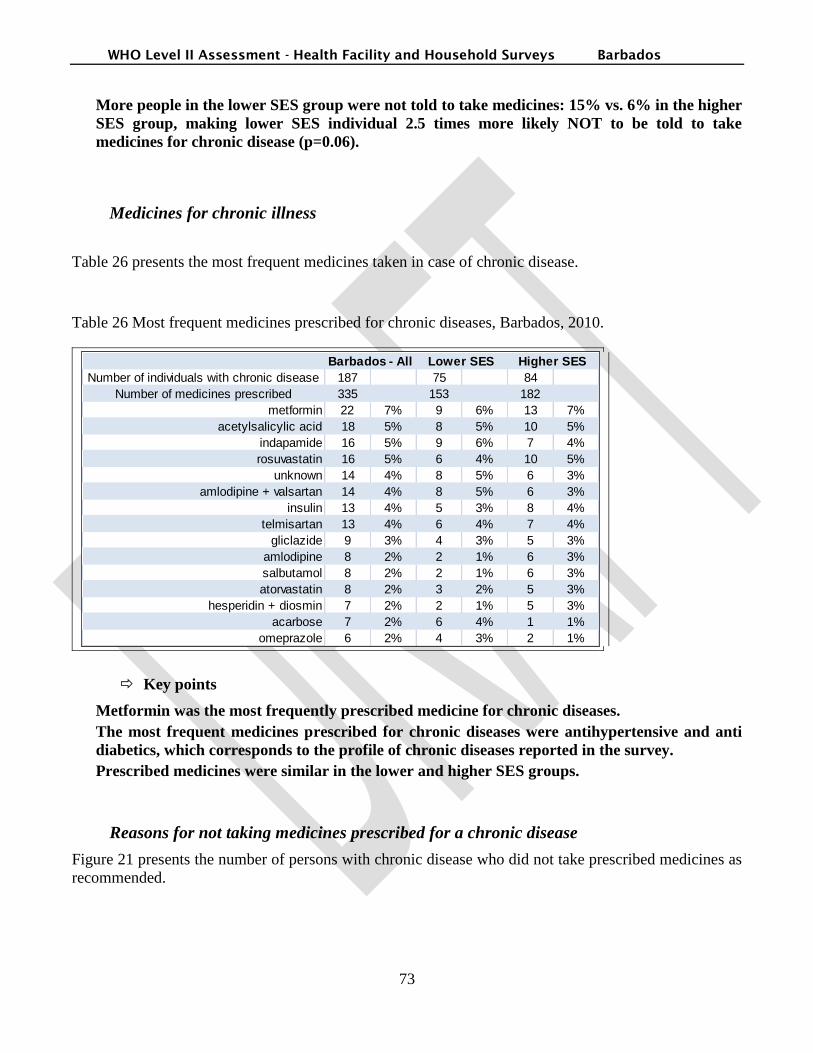
WHO Level II Assessment - Health Facility and Household Surveys Barbados
73
More people in the lower SES group were not told to take medicines: 15% vs. 6% in the higher
SES group, making lower SES individual 2.5 times more likely NOT to be told to take
medicines for chronic disease (p=0.06).
Medicines for chronic illness
Table 26 presents the most frequent medicines taken in case of chronic disease.
Table 26 Most frequent medicines prescribed for chronic diseases, Barbados, 2010.
Number of individuals with chronic disease 187 75 84
Number of medicines prescribed 335 153 182
metformin 22 7% 9 6% 13 7%
acetylsalicylic acid 18 5% 8 5% 10 5%
indapamide 16 5% 9 6% 7 4%
rosuvastatin 16 5% 6 4% 10 5%
unknown 14 4% 8 5% 6 3%
amlodipine + valsartan 14 4% 8 5% 6 3%
insulin 13 4% 5 3% 8 4%
telmisartan 13 4% 6 4% 7 4%
gliclazide 9 3% 4 3% 5 3%
amlodipine 8 2% 2 1% 6 3%
salbutamol 8 2% 2 1% 6 3%
atorvastatin 8 2% 3 2% 5 3%
hesperidin + diosmin 7 2% 2 1% 5 3%
acarbose 7 2% 6 4% 1 1%
omeprazole 6 2% 4 3% 2 1%
Barbados - All Lower SES Higher SES
Key points
Metformin was the most frequently prescribed medicine for chronic diseases.
The most frequent medicines prescribed for chronic diseases were antihypertensive and anti
diabetics, which corresponds to the profile of chronic diseases reported in the survey.
Prescribed medicines were similar in the lower and higher SES groups.
Reasons for not taking medicines prescribed for a chronic disease
Figure 21 presents the number of persons with chronic disease who did not take prescribed medicines as
recommended.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
74
Figure 22: Reasons for not taking medicines prescribed for a chronic disease, Barbados, 2010.
32
13
19
9
6
31 0 1
Barbados - All lower SES higher SES
Nu
mb
er
of
ind
ivid
ual
s w
ith
ch
ron
ic d
ise
ase
Did not follow their prescription Symptoms have improved
Can not afford medicines
Key points
Of the 187 surveyed individuals with a chronic disease, 32 (17.1%) did not take the prescribed
medicines.
The reason given most often for non adherence was the improvement of symptoms.
One person in the higher SES group identified affordability as a reason for non-adherence.
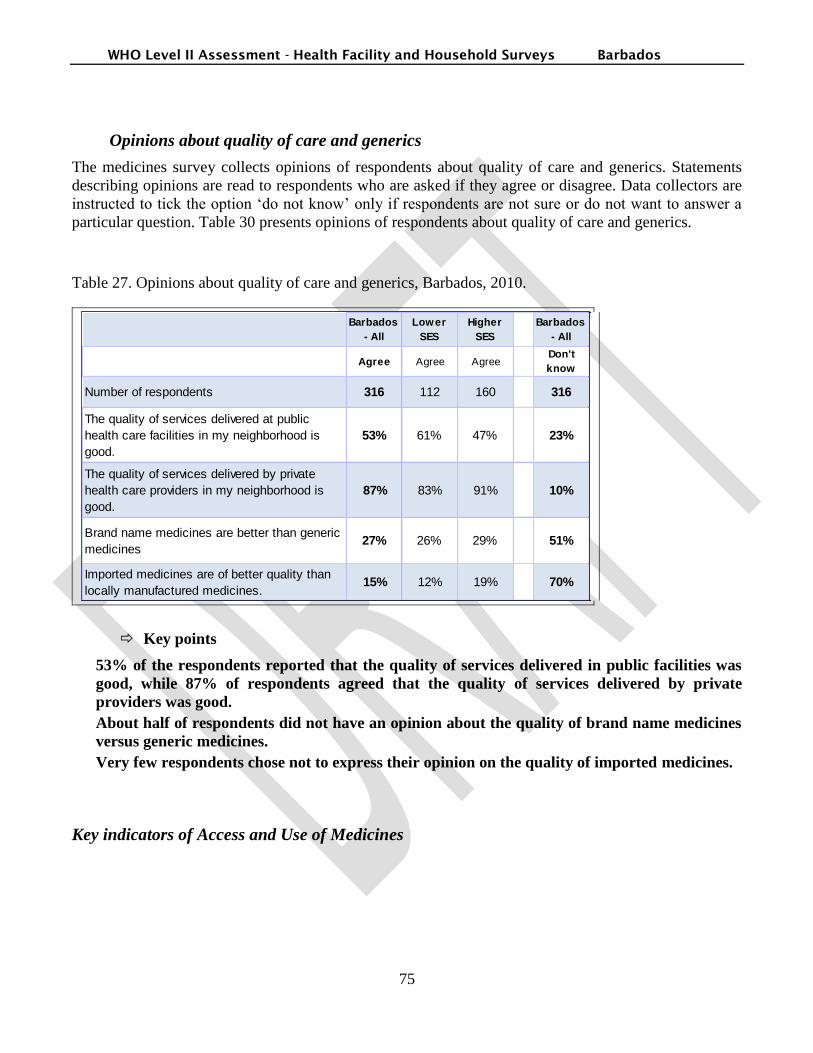
WHO Level II Assessment - Health Facility and Household Surveys Barbados
75
Opinions about quality of care and generics
The medicines survey collects opinions of respondents about quality of care and generics. Statements
describing opinions are read to respondents who are asked if they agree or disagree. Data collectors are
instructed to tick the option „do not know‟ only if respondents are not sure or do not want to answer a
particular question. Table 30 presents opinions of respondents about quality of care and generics.
Table 27. Opinions about quality of care and generics, Barbados, 2010.
Barbados
- All
Lower
SES
Higher
SES
Barbados
- All
Agree Agree AgreeDon't
know
Number of respondents 316 112 160 316
The quality of services delivered at public
health care facilities in my neighborhood is
good.
53% 61% 47% 23%
The quality of services delivered by private
health care providers in my neighborhood is
good.
87% 83% 91% 10%
Brand name medicines are better than generic
medicines27% 26% 29% 51%
Imported medicines are of better quality than
locally manufactured medicines.15% 12% 19% 70%
Key points
53% of the respondents reported that the quality of services delivered in public facilities was
good, while 87% of respondents agreed that the quality of services delivered by private
providers was good.
About half of respondents did not have an opinion about the quality of brand name medicines
versus generic medicines.
Very few respondents chose not to express their opinion on the quality of imported medicines.
Key indicators of Access and Use of Medicines

WHO Level II Assessment - Health Facility and Household Surveys Barbados
76
Table 28: Indicators of Access and Use of Medicines - All households, Barbados, 2010.
Geographic access of medicinesBarbados -
AllLower SES
Higher
SES
% households who have to travel > one hour to reach the
closest public health care facility1% 2% 1%
% respondents who agree that the location of public health
care facilities is convenient87% 87% 88%
% respondents who agree that they would use public health
care facilities more if opening hours were convenient49% 54% 43%
Availability of medicines
% respondents who agree that medicines are usually
available at their public health care facility53% 61% 48%
% respondents who agree that medicines are usually
available at their private pharmacy88% 84% 91%
Affordability of medicines
% households whose monthly medicines expenditures
represent > 40% of discretionary spending3% 2% 5%
% respondents who agree that they can get free medicines at
their public health care facility78% 87% 74%
% respondents who agree that medicines are more
expensive at private pharmacies than at public health care
facilities
59% 54% 64%
% respondents who agree that they can get credit from the
private pharmacy if need be15% 9% 18%
% respondents who agree that they can usually afford to buy
the medicines they need64% 56% 69%
% respondents who agree that they would obtain prescribed
medicines if insurance reimbursed part of their cost43% 29% 57%
% respondents who agree that they had to borrow money or
sell things in the past to pay for medicines8% 4% 11%
Access to medicines - Mixed indicators
% households with medicines at home 73% 71% 76%
% households with children and medicines at home 80% 80% 82%
Average number of medicines kept at home 3 3 4
% medicines found at home and obtained from a public
health care facility17% 30% 10%
% home medicines obtained from a public health care facility
and with an adequate label and primary package87% - -
% respondents who agree that the quality of services
delivered in public health care facilities is good53% 61% 47%
% respondents who agree that the quality of services
delivered by private health care providers is good87% 83% 91%
% respondents who do not know if brand name medicines
are better than generic medicines51% 58% 48%
% respondents who agree that brand name medicines are
better than generic medicines27% 26% 29%
% respondents who agree that imported medicines are of
better quality than locally manufactured medicines15% 12% 19%

WHO Level II Assessment - Health Facility and Household Surveys Barbados
77
Table 29: Indicators of Access and Use of Medicines - Households with at least one acute or chronic
conditions, Barbados, 2010.
Geographic access to medicinesBarbados -
Alllower SES higher SES
% respondents who say that distance from source of
medicines is a reason for not taking medicines prescribed
for a recent acute illness
0% 0% 0%
% respondents who say that distance from source of
medicines is a reason for not taking medicines prescribed
for a chronic disease
0% 0% 0%
Availability of medicines
% respondents who say that availability of medicines in
their public health care facility is a reason for not taking
medicines prescribed for a recent acute illness
0% 0% 0%
% respondents who say that availabity of medicines in
their public health care facility is a reason for not taking
medicines prescribed for a chronic disease
0% 0% 0%
Affordability of medicines
% households where someone with a recent acute illness
obtained medicines free-of-charge38% 35% 29%
Average cost of a prescription for acute illness for those
who did not obtain medicines free-of-chargeBBD 28 BBD 25 BBD 34
Maximum cost of a prescription for acute illness for those
who did not obtain medicines free-of-chargeBBD 170 BBD 100 BBD 170
% households where someone with a recent acute illness
had medicines completely covered by a health insurance3% 0% 7%
% households with a chronic disease who obtain
medicines for this disease free-of-charge87% 98% 74%
Average monthly cost of medicines for a chronic diseases
when not obtained free-of chargeBBD 19 BBD 9 BBD 177
Maximum monthly cost of medicines for a chronic
diseases when not obtained free-of chargeBBD 1,500 BBD 9 BBD 1,500
% households with someone with a chronic disease who
has at least one medicine covered by a health insurance5% 0% 9%
Access to medicines - Mixed indicators
% households reporting a member with a recent serious
illness who sought care outside home and took all
prescribed medicines
100% - -
% households where someone with a chronic disease was
told to take medicines and takes them as directed73% 69% 96%
% households where someone with a chronic disease was
told to take medicines and where medicines are found81% 38% 89%
WHO Level II Assessment - Health Facility and Household Surveys Barbados
78
Overall, the household survey results indicate that access to medicines is of good quality in Barbados,
and that it is slightly better in households with a higher SES. Geographical access and availability of
medicines do not seem to represent a barrier for access to medicines.
Nevertheless, they point out to an insufficient use of medicines to treat chronic diseases, mainly in
households of lower SES. Treatment management, especially non-adherence is also an issue to be
addressed. This is especially true in the group of surveyed individuals with a chronic disease. The
reason given most often for non adherence in this group was the improvement of symptoms. For
chronic conditions, this is neither a valid nor safe reason for suspending treatment.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
79
Conclusions and recommendations
The data from this survey provide a baseline for future interventions and the same indicators can be used
for monitoring the progress as well as to establish benchmarks, once they are standardized, it allows
comparing the national situation with results obtained in countries from Caribbean and other parts of the
globe.
In Barbados, medicines are generally available. Nevertheless there are several areas to be addressed to
improve the overall pharmaceutical situation. Despite of the existence of a draft national pharmaceutical
policy, the document was not implemented. The review of this draft and the development of an
implementation plan based on the outcomes of the survey and the proposal of the Caribbean
Pharmaceutical Policy is strongly recommended.
The survey also indicates that managerial policies related to pharmaceuticals need to be improved. The
appropriate use of medicines can be improved by the review of the National Drug Formulary, with
selection criteria based on evidence, together with the development, availability and use of STG. It is
also recommended to establish a strategy for strengthening the use of generics, and by enforcing the
current regulations and encouraging the use of INN for prescribing and increasing generic substitution.
An important finding of the survey is the inappropriate prescription of antibiotics, which are underused
to treat pneumonia in children under 5, and overused to treat non-bacterial upper respiratory infections.
This and the fact that many children under 5 with diarrhea are not prescribed the appropriate treatment,
strongly suggest the need to intensify training of providers in key areas of primary care prescribing.
It is recommended to increase the regulation of medicines and pharmaceutical services, including the
economic regulation as prices of the treatments in the private pharmacies were much higher than in the
public pharmacies. Despite the presence of a pharmacist in most pharmacies, storage conditions were
not optimal for public health facilities and private pharmacies and dispensing of prescription medicines
without prescription was also found. The development of national guidelines of Good Practices related
to distribution, storage and pharmacy practices as well as the strengthening of the pharmaceutical
services based on the renewal of primary health care, according to the PAHO/WHO recommendations
and guidelines are recommended as part of the strategies for improving the situation.
A strategy related to improving the knowledge and the rational use of medicines for the population can
be developed. Among the aspects to be included are medicines access and management at home
(labeling, storage conditions, etc), quality and safety issues and generic medicines and the importance of
adherence to treatment, especially in the management of chronic conditions.
It is recommended to design strategies to improve the situation related to the lower SES Group, tackling
the barriers for access, such as geographical barriers (11% households in the lower SES group live at
more than one hour from a public health facility) and the higher prevalence of both chronic and acute
conditions. The data suggests there is an under-use of medicines in this group, with individuals in lower
SES households 2.5 more likely NOT to be told to take medicines for chronic conditions.
Considering the high prevalence of chronic diseases in the country, it is recommended to strengthen the
holistic approach to tackling them, considering as a priority the promotion of healthy life style and other

WHO Level II Assessment - Health Facility and Household Surveys Barbados
80
non-pharmacological aspects. Treatment management, especially to strengthen adherence is an
important aspect to be highlighted. Specific interventions can be designed.
WHO Level II Assessment - Health Facility and Household Surveys Barbados
81
References
1. Pharmaceutical Assessment Level II of Barbados, June 2009
2. WHO Operational package for assessing, monitoring and evaluating country pharmaceutical
situations; Guide for coordinators and data collectors, December 2007
3. Xu, K. et al., 2003. Household catastrophic health expenditure: a multi country analysis. Lancet,
362(9378), 111-117. 4. WHO Model Lists of Essential Medicines. Available at:
http://www.who.int/medicines/publications/essentialmedicines/Updated_sixteenth_adult_list_en.pdf [Accessed August 26, 2010].

WHO Level II Assessment - Health Facility and Household Surveys Barbados
82
Annex 1. Level I Questionnaire
This filled out Level I questionnaire has to be adjusted and improved.
i Xu, K. et al., 2003. Household catastrophic health expenditure: a multi country analysis. Lancet,
362(9378), 111-117.
ii WHO | WHO Model Lists of Essential Medicines. Available at:
http://www.who.int/medicines/publications/essentialmedicines/en/ [Accessed August 18, 2009].

WHO Level II Assessment - Health Facility and Household Surveys Barbados
83
Annex 2. Level II Survey Forms

WHO Level II Assessment - Health Facility and Household Surveys Barbados
84
Annex 3. Household Survey Questionnaire
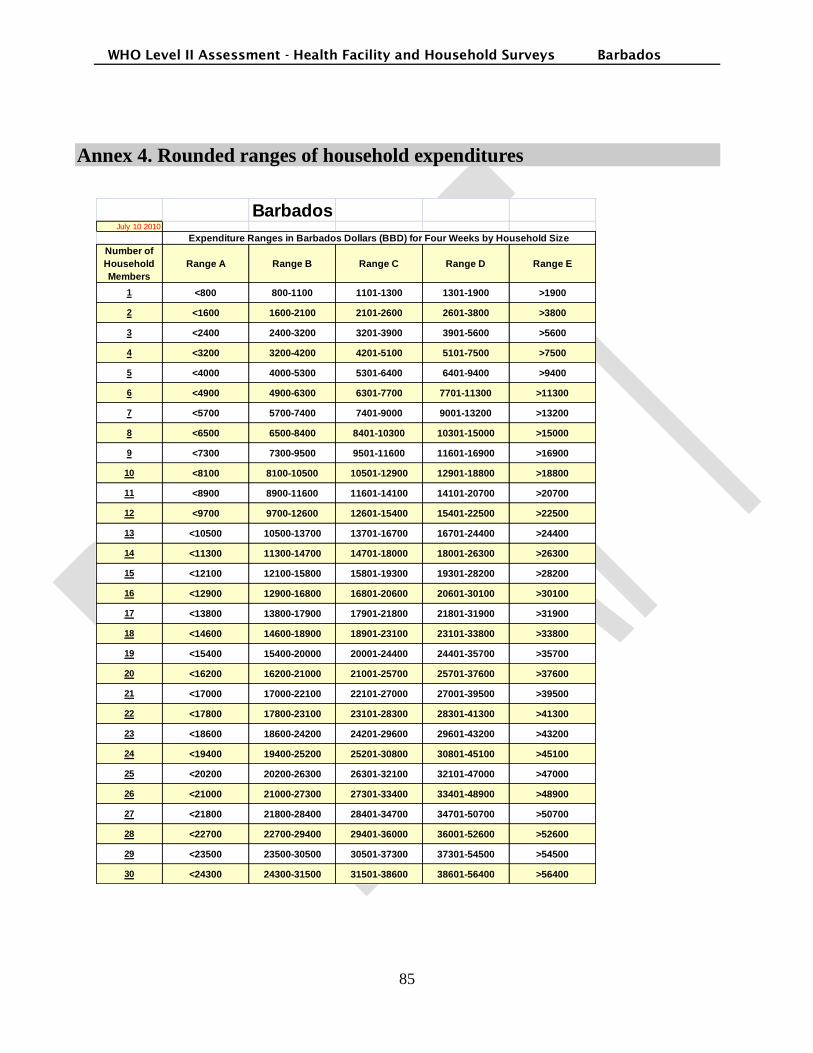
WHO Level II Assessment - Health Facility and Household Surveys Barbados
85
Annex 4. Rounded ranges of household expenditures
BarbadosJuly 10 2010
Expenditure Ranges in Barbados Dollars (BBD) for Four Weeks by Household Size
Number of
Household
Members
Range A Range B Range C Range D Range E
1 <800 800-1100 1101-1300 1301-1900 >1900
2 <1600 1600-2100 2101-2600 2601-3800 >3800
3 <2400 2400-3200 3201-3900 3901-5600 >5600
4 <3200 3200-4200 4201-5100 5101-7500 >7500
5 <4000 4000-5300 5301-6400 6401-9400 >9400
6 <4900 4900-6300 6301-7700 7701-11300 >11300
7 <5700 5700-7400 7401-9000 9001-13200 >13200
8 <6500 6500-8400 8401-10300 10301-15000 >15000
9 <7300 7300-9500 9501-11600 11601-16900 >16900
10 <8100 8100-10500 10501-12900 12901-18800 >18800
11 <8900 8900-11600 11601-14100 14101-20700 >20700
12 <9700 9700-12600 12601-15400 15401-22500 >22500
13 <10500 10500-13700 13701-16700 16701-24400 >24400
14 <11300 11300-14700 14701-18000 18001-26300 >26300
15 <12100 12100-15800 15801-19300 19301-28200 >28200
16 <12900 12900-16800 16801-20600 20601-30100 >30100
17 <13800 13800-17900 17901-21800 21801-31900 >31900
18 <14600 14600-18900 18901-23100 23101-33800 >33800
19 <15400 15400-20000 20001-24400 24401-35700 >35700
20 <16200 16200-21000 21001-25700 25701-37600 >37600
21 <17000 17000-22100 22101-27000 27001-39500 >39500
22 <17800 17800-23100 23101-28300 28301-41300 >41300
23 <18600 18600-24200 24201-29600 29601-43200 >43200
24 <19400 19400-25200 25201-30800 30801-45100 >45100
25 <20200 20200-26300 26301-32100 32101-47000 >47000
26 <21000 21000-27300 27301-33400 33401-48900 >48900
27 <21800 21800-28400 28401-34700 34701-50700 >50700
28 <22700 22700-29400 29401-36000 36001-52600 >52600
29 <23500 23500-30500 30501-37300 37301-54500 >54500
30 <24300 24300-31500 31501-38600 38601-56400 >56400

WHO Level II Assessment - Health Facility and Household Surveys Barbados
86
Annex 5. Description of indicators- Health facility survey
Indicator Purpose/ Rationale
Availability of key medicines in public
health facility dispensaries, private
pharmacies and warehouses supplying
the public sector
To measure current availability of key medicines to treat common
health problems in public health facility dispensaries, private
pharmacies and warehouses. Essential medicines to treat common
diseases should be available in all these facilities, especially in public
sector facilities providing health services for the poor. Physical
availability is a basic measure of access to essential medicines. See
pages 29–30 for guidance on selecting key medicines for this study.
% of prescribed key medicines
dispensed or administered to patients at
public health facility dispensaries
To measure the degree to which facilities are able to provide needed
medicines
Stock out duration at public health
facility dispensaries and warehouses
supplying the public sector
To measure availability over the past 12 months of key medicines to
treat common health problems. An adequate logistic system ensures
that essential medicines remain in stock at all times.
% Adequate record keeping at public
health facility dispensaries and
warehouses supplying the public sector
To determine the extent to which stock records are maintained. The
presence of adequately maintained and accurate stock records
contributes to proper management, estimation of needs and the
reorder of medicines.
Affordability of treatment for adults and
children under 5 years of age at public
health facility dispensaries and private
pharmacies
To measure affordability of basic pharmaceutical treatment as an
indicator of access to essential medicines. In most developing
countries, a majority of the population pays for treatment out-of-
pocket. Affordability is expressed as the ratio of the cost of treating
moderate pneumonia another condition to a standard unit of measure.
For this survey, the lowest daily government salary is used. Countries
may also identify an optional second unit of measure (e.g. poverty
line, basket of food, etc.).
Average selling cost of medicines
public health facilities and private
pharmacies
To measure average cost paid by patient for medicines at public
health facilities and private pharmacies as an indicator of access to
essential medicines. In most developing countries, a majority of the
population pays for treatment out-of-pocket.
% patients taking more than one hour to
travel to the facility
To assess geographic accessibility in terms of how long does it take
the patients to get to the pharmacy they get their medicines
Average transportation cost to the
facility
To assess geographic accessibility in terms of how much does it cost
to the patients to get to the pharmacy they get their medicines
Presence of expired medicines in public
health facility dispensaries, private
pharmacies and warehouses supplying
the public sector
To determine if expired medicines are being distributed or sold. In
some countries, expired medicines are distributed or medicines are
allowed to go out of date on pharmacy shelves. See page 29–30 for
guidance on selecting key medicines for this study.
Adequacy of conservation conditions
and handling of medicines in public
health facility pharmacies/dispensaries,
private pharmacies and
central/regional/district warehouses
supplying the public sector
To determine status of conservation conditions and handling of
medicines in public sector facilities, both of which are factors that
affect quality of medicines
% medicines adequately labeled at
public health facility dispensaries
To assess quality of dispensing practice. If medicines are to be used
properly, they should be labeled appropriately by the person
dispensing them.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
87
Indicator Purpose/ Rationale
% patients know how to take medicines
at public health facility dispensaries
To assess if patients have adequate knowledge of how to take their
medicines.
Average number of medicines
prescribed in public health facilities
To determine prevalence of polypharmacy, which is one measure of
unnecessary prescribing
% patients prescribed antibiotics in
public health facilities (Survey Form 7)
To determine prevalence of antibiotic prescribing, since over-
prescribing of antibiotics is one common type of inappropriate
medicine use
% patients prescribed injections in
public health facilities
To determine prevalence of injection use, since over-prescribing of
injections is one common type of inappropriate medicine use
% prescribed medicines on the essential
medicines list at public health facilities
To measure the degree to which prescribing practice conforms to the
national essential medicines list (EML). The essential medicines
concept is one of the main strategies being promoted in medicines
policy. More and more countries are formulating national EMLs. For
most, this should be the basis for all public medicines procurement
and prescribing.
% medicines prescribed by generic
name (INN) at public health facilities
To measure the degree to which prescribing practice conforms to the
principles of generic prescribing.
Availability of standard treatment
guidelines at public health facilities
To determine if prescribers have available to them the key source of
therapeutic information they need in daily practice.
Availability of EML at public health
facilities
To determine if prescribers and/or dispensers have available to them
the key source of pharmaceutical information that should be the basis
for all medicine prescribing and dispensing.
% tracer cases treated according to
recommended treatment protocol/guide
To measure quality of care for common conditions with clear
recommended treatment protocols. Adherence to recommended
protocols can be measured by checking if tracer diseases are treated
appropriately. Such recommendations might include use of ORS for
watery diarrhea in children, use of the recommended antibiotic for
mild pneumonia or non-use of antibiotics for simple ARI. The survey
form has space for countries to track additional conditions, if desired.
% of prescription medicines bought
without prescription
To determine if costumers are purchasing and dispensers are selling
prescription medicines without prescription. The existence of a
prescription (and therefore a medical encounter) as the source of
(prescription) medicine seeking behavior should be the basis for all
medicine dispensing as a way to promote rational use of medicines.
% of facilities that comply with the law
(presence of a pharmacist)
To determine if facilities comply with the law (presence of a
pharmacist where the law requires).
% facilities with pharmacist, nurse,
pharmacy aide/ health assistant or
untrained staff dispensing
To determine the profile of the health professionals that dispense
medicines in health facilities and private pharmacies.
% facilities with doctor, nurse, trained
health worker/health aide prescribing
To determine the profile of the health professionals prescribing in
health facilities.
% facilities with prescriber trained in
RDU
To determine if the most senior health professionals prescribing in
health facilities were trained in RDU.
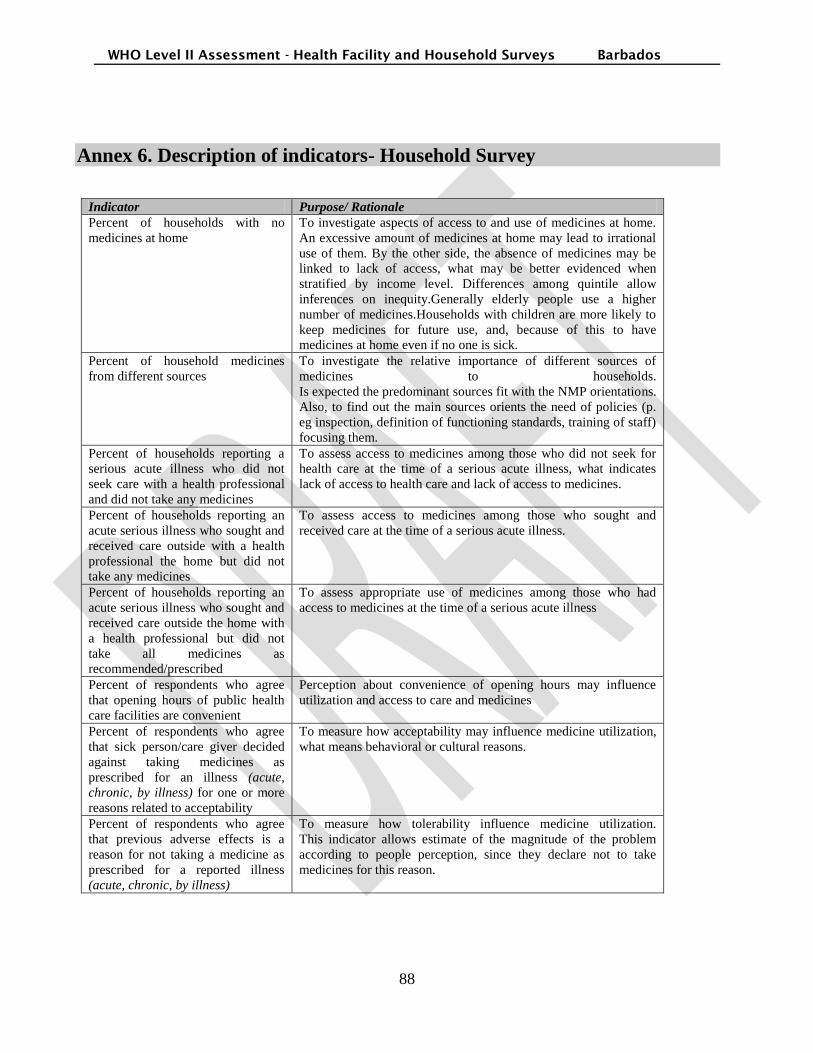
WHO Level II Assessment - Health Facility and Household Surveys Barbados
88
Annex 6. Description of indicators- Household Survey
Indicator Purpose/ Rationale
Percent of households with no
medicines at home
To investigate aspects of access to and use of medicines at home.
An excessive amount of medicines at home may lead to irrational
use of them. By the other side, the absence of medicines may be
linked to lack of access, what may be better evidenced when
stratified by income level. Differences among quintile allow
inferences on inequity.Generally elderly people use a higher
number of medicines.Households with children are more likely to
keep medicines for future use, and, because of this to have
medicines at home even if no one is sick.
Percent of household medicines
from different sources
To investigate the relative importance of different sources of
medicines to households.
Is expected the predominant sources fit with the NMP orientations.
Also, to find out the main sources orients the need of policies (p.
eg inspection, definition of functioning standards, training of staff)
focusing them.
Percent of households reporting a
serious acute illness who did not
seek care with a health professional
and did not take any medicines
To assess access to medicines among those who did not seek for
health care at the time of a serious acute illness, what indicates
lack of access to health care and lack of access to medicines.
Percent of households reporting an
acute serious illness who sought and
received care outside with a health
professional the home but did not
take any medicines
To assess access to medicines among those who sought and
received care at the time of a serious acute illness.
Percent of households reporting an
acute serious illness who sought and
received care outside the home with
a health professional but did not
take all medicines as
recommended/prescribed
To assess appropriate use of medicines among those who had
access to medicines at the time of a serious acute illness
Percent of respondents who agree
that opening hours of public health
care facilities are convenient
Perception about convenience of opening hours may influence
utilization and access to care and medicines
Percent of respondents who agree
that sick person/care giver decided
against taking medicines as
prescribed for an illness (acute,
chronic, by illness) for one or more
reasons related to acceptability
To measure how acceptability may influence medicine utilization,
what means behavioral or cultural reasons.
Percent of respondents who agree
that previous adverse effects is a
reason for not taking a medicine as
prescribed for a reported illness
(acute, chronic, by illness)
To measure how tolerability influence medicine utilization.
This indicator allows estimate of the magnitude of the problem
according to people perception, since they declare not to take
medicines for this reason.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
89
Indicator Purpose/ Rationale
Percent of persons with reported
illnesses (acute by illness) who are
treated with injections
To evaluate one aspect of rational use of medicines. The injectable
administration via is always more dangerous then others and
should only be used when really indicated.Since current standard
as 20% proposed by WHO refers to primary health care and here
any level of care may be addressed interpretation should be done
with caution. Indeed, in this moment it is very important to
calculate this indicator at household level in order to create
evidence to establish adequate standard concerning this approach.
Percent of respondents who agree
that quality of medicines purchased
at medicine retailers (private
pharmacy, medicine seller) is better
than at public health care facilities
Perceptions about quality of medicines may influence utilization.
In many middle and low countries medicines provided by the
public system are perceived of low quality by general people, what
may influence medicines use and medicines seeking behavior.
Percent of respondents who agree
that locally made medicines are of
lesser quality
Perceptions about quality of medicines may influence utilization.
In many middle and low countries medicines locally made are
perceived of low quality by general people, what may influence
medicines use and medicines seeking behavior.
Average number of medicines at
home
To investigate aspects of access to and use of medicines at home.
An excessive amount of medicines at home may lead to irrational
use of them. By the other side, the absence of medicines may be
linked to lack of access, what may be better evidenced when
stratified by income level. Differences among quintile allows
inferences on inequity.
Generally elderly people use a higher number of medicines.
Households with children are more likely to keep medicines for
future use, and, because of this to have medicines at home even if
no one is sick.
Percent of household medicines by
category of person who prescribed
or recommended them
To investigate who prescribed or recommended medicines
available at home.
Data allows identifying origin of prescription/recommendation
according to sectors (public/private) and authorized
professionals/lay people. Importance of specific informal
prescribers that constitutes problems in some countries, e.g.,
private pharmacies may also be identified.
Stratification allows assessing differential behavior among these
prescribers in relation to OTC and medicines from the EML (e.g.
are authorized prescribers more adherent to EML? are lay people
prescribing prescription medicines?). Severe acute and chronic
health problems are more likely to require professional care and
less likely to be solved with OTC medicines.
Percent of antibiotics kept for future
use
To investigate aspects of rational use of medicines available at
home.Systemic use antibiotics are always prescription medicines
and the incorrect use is linked to emergence of resistance and
treatment failure.
Percent of antimalarials kept for
future use
To investigate aspects of rational use of medicines available at
home.
National epidemic level for malaria and national guidance on
treatment should be considered to interpret the indicator.
Depending on the epidemic level it is advisable that people keep
first line treatment at home.
Percent of household medicines
with adequate label
To investigate on aspect of rational use of medicines and quality of
care.
Items verified are the minimum to assure medicines identification
and validity.

WHO Level II Assessment - Health Facility and Household Surveys Barbados
90
Indicator Purpose/ Rationale
Percent of household medicines
with adequate primary packaging
To investigate one aspect of rational use of medicines and quality
of care.
Despite other conditions are also important, primary package is
fundamental to preserve medicines specifications and
identification
Percent of households with a
chronically ill person who was never
told to take medicines (overall, by
illness)
To investigate overall access to care and medicines for chronic
illnesses.
As chronic ill people are only consider in this approach if they
have already been told by a doctor to have the illness, a high
percentage of people never been told to take medicines indicates
lack of access or quality of health care.
Percent of households with a
chronically ill person prescribed
medicines who does not take
recommended medicines regularly
(overall, by illness)
To investigate regular access to and use of medicines in chronic
illnesses.
Not to take medicines regularly may be linked to access or
adherence.
Percent of medicines taken for a
reported illness (acute, chronic, by
illness) that were recommended by a
doctor or other qualified healthcare
provider
To investigate rational use of medicines in various conditions. The
performance of this indicator may be linked to access to health
care and prescription behavior.
Percentage of people referring the
use of herbal for a reported illness
(acute, chronic disease)
This indicator allows to estimate the importance and acceptance of
herbal medicines by the population
Average household medicine
expenditures as percent of total
expenditures
To determine the overall financial burden of medicines on
households, in relation to total expenditures. The indicator allows
assessing the magnitude of total household expenditures
committed with medicines.
Average household medicine
expenditures as percent of non-food
expenditures
To determine the financial burden of medicines as a proportion of
non-food (discretionary) expenditures in households.
This indicators allows to calculated catastrophic expenditure on
medicines
Average household medicine
expenditures as percent of total
health expenditures
To determine the financial burden of medicines as a proportion of
health expenditures in households.
Differences among quintiles express inequity level. Different
policies targeting different groups of population should be
considered t the interpretation.
Average annualized health
expenditures per person
To determine the annual level of health expenditures per person.
Differences among quintiles indicate inequity.
Average annualized medicine
expenditures per person
To determine the annual level of medicine expenditures per
person.
Differences among quintiles indicates inequity
Average household medicine
expenditures for a reported illness
(acute, chronic, by illness) as
percent of total expenditures in a
4-week period
To determine financial burden of expenditures on medicines for a
reported illness
Percent of households with
insurance coverage for any of the
medicines prescribed for a reported
illness (acute, chronic, by illness)
To determine the extent of insurance coverage of medicines in
households

WHO Level II Assessment - Health Facility and Household Surveys Barbados
91
Indicator Purpose/ Rationale
Percent of respondents who agree
that price is a reason for not taking
medicines prescribed for a reported
illness (acute, chronic, by illness)
To measure cost as a barrier to medicines access.
Percent of households who can get
free medicines at public health care
facilities
Free medicines may increase access. Differences among quintiles
allows to assess if goals established in the NMP are being met.
Percent of households who agree
that medicines are more affordable
at public health care facilities than at
private pharmacies
Perception about affordability may influence utilization
Percent of households who can get
credit for medicines at medicine
retailers (private pharmacies,
medicine sellers)
Possibility of getting credit to buy medicines may influence
patterns of utilization and access
Percent of households who had to
borrow money or sell assets in the
past to pay for medicines
To assess how the cost of medicines affects household economic
status and poverty risk
Percent of respondents who agree
that lack of availability of medicines
at point of distribution (public
health care facility, private
pharmacy or medicine seller) is a
reason for not taking medicines as
prescribed for a reported illness
(acute, chronic, by illness)
To measure perception about availability of medicines.
This indicator intend to assess if availability is perceived by
people as problem not to take medicine and if the problem has
different magnitude concerning to acute or chronic conditions.
Percent of respondents who agree
that medicines are available at point
of distribution (public health care
facility, private pharmacy, medicine
seller)
Perceived availability of medicines in health care facilities may be
a barrier to utilization and access
Percent of households located > 1h
5km from the closest provider of
medicines
To measure the distance to public health care facilities. Living
more than 1 hour walking distance from a public health care
facility may impact access to medicines.
Catherine, do you have any evidence on this distance? Why 1h. In
Brazil we found people start be concerned to distance over 30
minutes travel
Percent of households located > 1h
from the point of distribution of
medicines prescribed for a reported
illness (acute, chronic, by illness)
To measure distance from the actual source of medicines. Having
to travel more than 1 hour walking distance to obtain medicines
may impact access to medicines.
Percent of respondents who declare
that distance from source of
medicines is a reason for not taking
a medicine as prescribed for a
reported illness (acute, chronic, by
illness)
To measure geographic access as a perceived barrier to not access
all needed medicines.Results according to kind of illness (acute,
chronic, specific illness) have different potential hazard. In serious
acute illness people probably were in need to access medicines
quickly, may be in life threatening situations. In chronic
conditions people generally requires the same medicines
continuously and any barrier to access declared is probably faced
frequently.
Percent of respondents who agree
that location of public health care
facilities is convenient
Perception about convenience of health care facilities may
influence utilization and access to medicines
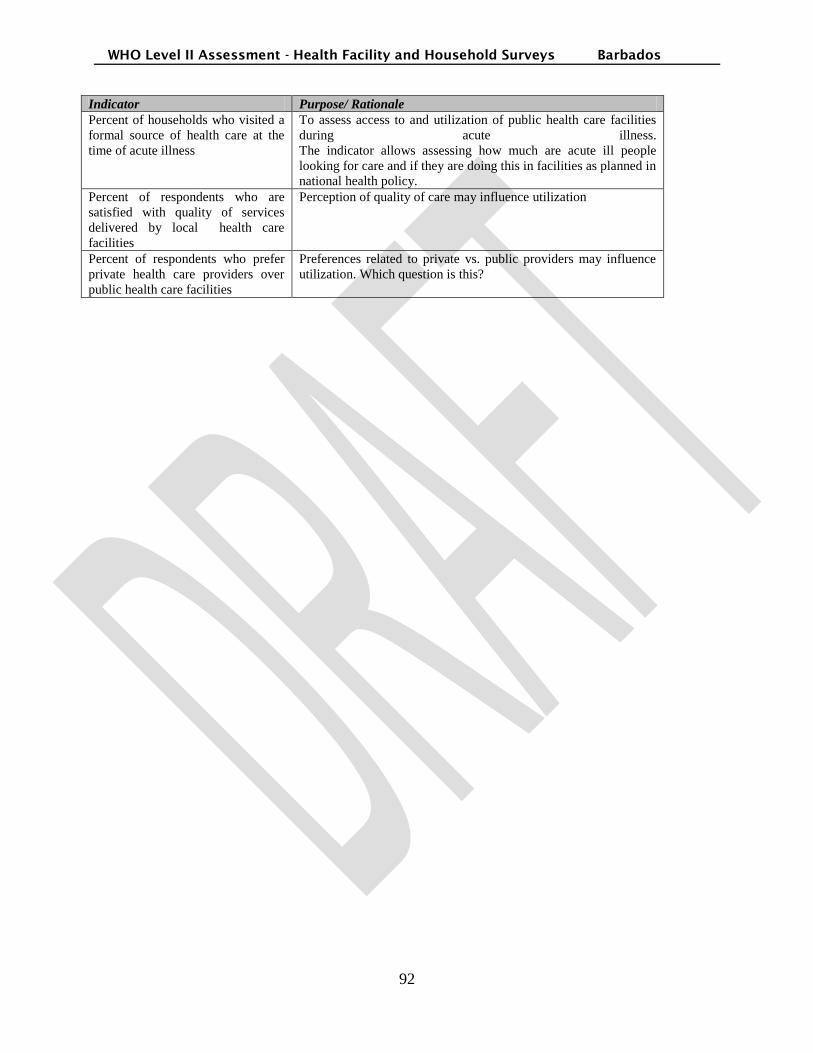
WHO Level II Assessment - Health Facility and Household Surveys Barbados
92
Indicator Purpose/ Rationale
Percent of households who visited a
formal source of health care at the
time of acute illness
To assess access to and utilization of public health care facilities
during acute illness.
The indicator allows assessing how much are acute ill people
looking for care and if they are doing this in facilities as planned in
national health policy.
Percent of respondents who are
satisfied with quality of services
delivered by local health care
facilities
Perception of quality of care may influence utilization
Percent of respondents who prefer
private health care providers over
public health care facilities
Preferences related to private vs. public providers may influence
utilization. Which question is this?






![IB - Barbados International Finance & Business Magazine 2010 [Barbados]](https://static.fdocuments.in/doc/165x107/5553d3efb4c905c4048b4c4b/ib-barbados-international-finance-business-magazine-2010-barbados.jpg)











