Diagnostic performance of CMR, SPECT, and PET imaging for ...

PET and PET and SPECT in SPECT in DementiaDementiaRodolfo Ferrando, MD, MSc
Assistant Professor of Nuclear Medicine Hospital de Clínicas, Facultad de Medicina.
Universidad de la República.Montevideo, Uruguay.

Aetiology

�� 8% of population older tan 65 years and 20% older than 75 have 8% of population older tan 65 years and 20% older than 75 have Alzheimer's Disease (AD).Alzheimer's Disease (AD).�� 15% of population have Mild Cognitive Impairment (MCI) at 15% of population have Mild Cognitive Impairment (MCI) at age 65, 60% of them will have AD.age 65, 60% of them will have AD.�� AD is the 3AD is the 3rdrd most expensive disease in the US.most expensive disease in the US.�� There are 4 million people with AD in the US.There are 4 million people with AD in the US.�� Clinical diagnosis has sensitivity 80%, specificity 70%.Clinical diagnosis has sensitivity 80%, specificity 70%.�� Late diagnosis in most casesLate diagnosis in most cases
Epidemiology and Impact

Epidemiology and Impact
NIA Alzheimer’s Disease: Unraveling the Mystery
New cases of AD estimated per year in USA (millions)

SPECT Brain Imaging in DementiaMeta Analysis
Visual Interpretation
Bilateral Posterior
89% 97%75% 84%
Devous M, Thisted R, Jagust W, et al. J Nucl Med 1995;35:107.
AD (n = 316) vs. normal (278) AD (236) vs. other dementias
(235)
Sens Spec

Voxel based analysis can improve SPECT diagnostic accuracy
Imabayashi et al. J Nucl Med 2004

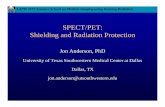
Mild AD. Bilateral posterior parietal/ temporoparietal, precuneus and posterior cingulate hypoperfusion (white arrows).
Moderate-severe AD. Progression to bilateral prefrontal cortex (white). Red arrows indicate preservation of primary sensoriomotor cortex, occipital cortex, basal ganglia, thalami and cerebellum (not shown)
Progression of AD

Okada et al. 3D-SSP FDG-PET and MRI. 31 AD vs. 551 normal controls

Evaluating early dementia with and without FDGPET: a comparison of predicted costs and benefits
Sensibility Specificity Base of Diagnosis
66 ±17% 77 ±23% Clinical evaluation,AD probable
90.5 ±5.5% 55.5 ±5.5% Clinical evaluation,AD probable + possible
91.5 ±3.5% 70 ±3% FDG-PET, AD pattern
Silverman DH, et al. J Nucl Med 2002b;43:253-266
Sensibility and specificity of PET and clinical evaluation compared to histo-pathological confirmation of AD.

Evaluating early dementia with and without FDGPET: a comparison of predicted costs and benefits
Silverman DH, et al. J Nucl Med 2002b;43:253-266
Impact of adding PET: 16% less false diagnostic results.
0.850.85
0.690.69
AccuracyAccuracy
0.940.94
0.840.84
SensibilitySensibility
0.750.75PET includedPET included
0.5250.525ConventionalConventional
SpecificitySpecificityALGORITHMALGORITHM

SPECT vs. PET�� 26 AD probable26 AD probable�� FDG vs. HMPAOFDG vs. HMPAO�� Analysis: SPMAnalysis: SPM�� r = 0.9 for posteriorr = 0.9 for posteriortemporoparietal cortex and temporoparietal cortex and posterior cingulateposterior cingulate�� FDG more intense defects FDG more intense defects (better contrast)(better contrast)
Correlation of abnormal voxelsCorrelation of abnormal voxels
SPEC
TSP
ECT
PETPET
Herholz et al J Nucl Med 2002;43:21Herholz et al J Nucl Med 2002;43:21--2626

ClinicalClinical SPECT (+)SPECT (+) SPECT (SPECT (--))
70 patients with autopsy. 70 patients with autopsy. Jagust et al. Neurology 2001;56:950Jagust et al. Neurology 2001;56:950--5656
00
2525
5050
7575
100100
AD ProbableAD Probable
AD di
agno
sis (p
atholo
gy) %
AD di
agno
sis (p
atholo
gy) % 8484
9292
7070
AD PossibleAD Possible AD absentAD absent
67678484
5252
331111
22
SPECT perfusion imaging in the diagnosis of AD

FDG-PET Mild Cognitive Impairment
00
2525
5050
7575
100100
Clinical prediction Clinical prediction progressive declineprogressive decline
Patie
nts th
at de
cline
d %Pa
tients
that
decli
ned %
ClinicalClinical PET (+)PET (+) PET (PET (--))
167 patients with MCI. Mean follow up 3 ys. 167 patients with MCI. Mean follow up 3 ys. Molec Genet Metab 2003;80:350Molec Genet Metab 2003;80:350--55
8484
Clinical prediction Clinical prediction non progressivenon progressive
9494
25253434
7474
44

SPECT MCI
76 patients with MCI. 3 years follow up.76 patients with MCI. 3 years follow up.52 converted to AD, 24 non converters.52 converted to AD, 24 non converters.
Hirao K, et al. Neuroimage 2005;28:1014Hirao K, et al. Neuroimage 2005;28:1014--2121

Differential diagnosis of Dementia

Differential diagnosis between AD & FTD by the posterior cingulate sign
4 (4 Aut)4 (4 Aut)No PCNo PC
11PCPC
19 (7 Aut)19 (7 Aut)16 (6 Aut)16 (6 Aut)No PCNo PCPCPC
20 patients with AD20 patients with AD 20 patients with FTD20 patients with FTD
Bonte FJ, et al. J Nucl Med 2004;45:771-774
FTD: frontotemporal dementia PC: posterior cingulate Aut: auFTD: frontotemporal dementia PC: posterior cingulate Aut: autopsytopsy

Vascular Dementia vs. AD�� ~10% of patients. ~10% of patients. �� Random distribution of defects. Diffuse or focal. Cortical and Random distribution of defects. Diffuse or focal. Cortical and subcortical.subcortical.�� Usually diffuse small infarcts affecting basal ganglia, thalamiUsually diffuse small infarcts affecting basal ganglia, thalami, white , white matter and hippocampus when isolated.matter and hippocampus when isolated.�� Usually focal more extent infarcts when associated with AD (Usually focal more extent infarcts when associated with AD (~~5%).5%).�� Progressive decline depends on severity of AD more than vasculaProgressive decline depends on severity of AD more than vascular r disease.disease.�� Clinical diagnosis + MRI usually overestimate vascular aetiologClinical diagnosis + MRI usually overestimate vascular aetiology and y and underestimate mixed dementia. underestimate mixed dementia.
Jellinger KA, 2002Jellinger KA, 2002

Late life depression & HypothyroidismThe two most common causes of reversible dementia in the elderlyThe two most common causes of reversible dementia in the elderly. May present with . May present with
similar pattern to AD but basal ganglia and thalami are usually similar pattern to AD but basal ganglia and thalami are usually involved.involved.

AD vs. Lewy Body DiseaseFDGFDG DATDAT
LewyLewy
Differentiation of dementia with Lewy bodies from AlzheimerDifferentiation of dementia with Lewy bodies from Alzheimer’’s s disease using a dopaminergic presynaptic ligand.disease using a dopaminergic presynaptic ligand.
Walker Z, et al. J Neurol Neurosurg Psychiatry 2002;73:136Walker Z, et al. J Neurol Neurosurg Psychiatry 2002;73:136--4040

Parkinson vs. AD vs. LBD
Recurrent andRecurrent anddetaileddetailed
CasualCasual
Less commonLess common
Visual Visual hallucinationshallucinations
YesYesWith With cognitive cognitive
impairment impairment Fluctuations Fluctuations ProgressiveProgressiveLBDLBD
YesYesBefore Before cognitive cognitive
impairmentimpairmentSlowSlow
Dementia Dementia 30%30%ParkinsonParkinson
NoNoCasualCasualLateLateProgressiveProgressiveADAD
Sensibility to Sensibility to neurolepticsneuroleptics
ExtraExtra--pyramidal pyramidal
signssignsCognitive Cognitive
impairmentimpairment

AD vs. LBDHypoperfusion/hypometabolism
++++++
++++
FrontalFrontal
++++
--
OccipitalOccipital
++
--
BGBG
++++++++++LBDLBD
++++++++++++ADAD
Mesial Mesial temporaltemporal
Posterior Posterior temporotemporo--parietalparietal

Parkinson vs. Atypical Parkinsonisms
DATDAT
D2D2
FPFP--CITCIT
IBZMIBZM
NCNC MSAMSAPDPD
EP (EP (↓))MSA (MSA (↓))
Tatsch et al. J Nucl Med 1998Tatsch et al. J Nucl Med 1998
EP (EP (N orN or ↑))MSA (MSA (↓))

Atypical Parkinsonisms
PSPPSPParkinsonParkinson
FDG PETFDG PET ECD SPECTECD SPECT
CBDCBD
ECD SPECTECD SPECT
MSAMSA--OPCAOPCA
FDG PETFDG PET

Huntington’s Disease
A. 7A. 7--year evolution with psychiatric symptoms. B. HD with year evolution with psychiatric symptoms. B. HD with dementia. dementia.
C. Cognitive impairment and family history of HD.C. Cognitive impairment and family history of HD.

Potential impact of treatment to delay AD onset
Brookmayer et al. 1998Brookmayer et al. 1998

Early markers of AD
Cerebral metabolic and cognitive decline Cerebral metabolic and cognitive decline in persons at genetic risk for AD.in persons at genetic risk for AD.Small et al. PNAS 2000;97:6037Small et al. PNAS 2000;97:6037--42.42.
APOE-4 Risk
APOE-4 Metabolic Decline (2 ys)

Imaging brain amyloid in AD using 11C-PIB PET
Klunk et al. Ann Neurol 2004Klunk et al. Ann Neurol 2004

11C-PIB for differential diagnosis of dementia
Row et al. Neurology 2007Row et al. Neurology 2007

11C-PIB as an early marker of AD
8080--90% 1090% 10--20% 40% 60% 100%20% 40% 60% 100%

Early markers of AD: the search for new treatments in preclinical stages

Alzheimer’s Association. Statement on PET. January 2004.FDG PET supported in dementia or cognitive decline of at least 6FDG PET supported in dementia or cognitive decline of at least 6 monthsmonthswhen diagnosis remains uncertain after complete clinical evaluatwhen diagnosis remains uncertain after complete clinical evaluation and ion and
PET is expected to aid in diagnosis or future treatment.PET is expected to aid in diagnosis or future treatment.
US Centres for Medicare & Medicaid Services. June 2004.FDG PET supported in dementia or cognitive decline of at least 6FDG PET supported in dementia or cognitive decline of at least 6months when criteria for both AD and FTD coexist and diagnosis months when criteria for both AD and FTD coexist and diagnosis
remains uncertain after complete clinical evaluation.remains uncertain after complete clinical evaluation.

Report of the dementia with Lewy bodies consortium 2005Low DAT uptake in SPECT or PET is a Low DAT uptake in SPECT or PET is a suggestive featuresuggestive feature for DLBfor DLBLow perfusion or metabolism in SPECT/PET with reduced occipital Low perfusion or metabolism in SPECT/PET with reduced occipital
activity is a activity is a supportive featuresupportive feature
Alzheimer’s Association & National Institute on Aging. 2010. Recommendations to update diagnostic criteria for AD.
Review and update of the NINDSReview and update of the NINDS--ADRDA criteria (1984). ADRDA criteria (1984). New proposed criteria for AD, MCI/AD and preclinical AD, includiNew proposed criteria for AD, MCI/AD and preclinical AD, including ng
PET/SPECT imaging, MRI and CSF assays as biomarkers for AD.PET/SPECT imaging, MRI and CSF assays as biomarkers for AD.

�� Early diagnosis of ADEarly diagnosis of AD�� Prediction of conversion from MCI to ADPrediction of conversion from MCI to AD�� Differential diagnosis of dementiaDifferential diagnosis of dementia�� Preclinical diagnosis of ADPreclinical diagnosis of AD�� Assessment of new therapeutic interventionsAssessment of new therapeutic interventions�� Progressive incorporation to clinical guidelinesProgressive incorporation to clinical guidelines
Summary