
Persistent left superior vena cava in patients with congenital atrioventricular preexcitation...
3
Volume 101 Number 5 Brief Communications 677 Fig. 3, Top panel. (A) Recording of lead II with a paper speed of 25 mm/set in a patient with ventricular tachycardia. The precordial thump interrupts the arrhythmia (arrow). Bottom panel. (B) Recording of lead I in a patient with supraventricular tachycardia, paper speed being 25 mm/set. The arrows point to the precordial thumps. After the first thump, a ventricular reentrant mechanism was induced. ventricular and atria1 premature beats produced by pre- cordial thumps are shown in Fig. IA and B. When the thump is applied in the middle part of the sternum, the premature beats are more often atrial; when the thump is applied in the inferior part of the sternum, ventricular premature beats can be expected. This peculiar extrastimulus may interrupt a reentry mechanism at the atrial, junctional, or ventricular level, in &he same way as the electrical stimulation of the heart. In two cases we were able to interrupt the reentry in atria1 flutter, as showrn in Fig. 2,A. In five cases the reentrant supraventricular tachycardia was stopped in the same way (Fig. 2,B). In Fig. 3,A a precordial thump interrupts a ventricular tachycardia. Because of the possibility of precipitating ventricular arrhythmias, this maneuver may sometimes be dangerous.i, 7 This situation is presented in Fig. 3,B, where after the first thump a reentrant ventricular mech- anism was induced. We consider that a precordial thump may be efficient in disrupting the reentry mechanism in different cardiac arrhythmias, acting as an extrastimulus produced by a pacemaker. REFERENCES 1. 2. 3. 4. 5. 6. Baderman H, Robertson NRC: Thumping the precqrdium. Lancet 2:1293, 1965. Bornemann C, Scherf D: Paroxysmal ventricular tachycar- dia abolished by a blow to the precordium. Dis Chest 56~33, 1963. Don Michael TA, Stanford RL: Precordial percussion in cardiac asystole. Lancet 1:699, 1963. Grossman JI, Rubin IL: Cardiopulmonary resuscitation. AM HEART J 78:709, 1969. Harwood-Nash DC: Thumping of the precordium in ventric- ular fibrillation. S Afr Med J 36:280, 1962. Hodgkin JE, Foster GL, Nicolay LJ: Cardiopulmonary resuscitation. Crit Care Med 5:93, 1977. 7. Lown B, Taylor J: Thump-version. N Engl J Med 283:1223, 1970. 8. Pennington JE, Taylor J, Lown B: Chest thump for revert- ing ventricular tachycardia. N Engl J Med 283:1192, 1970. Persistent left superior vena cava in patients with congenital atrioventricular preexcitation conduction abnormalities Dwight Davis, M.D., Edward L. C. Pritchett, M.D.,* Geqrge J. Klein, M.D., D. Woodrow Benson, M.D., Ph.D., and John J. Gallagher, M.D.** Durham, N.C. In 1976 James et al.’ described two patients with sudden death, each of whom was found to have a persistent left superior vena cava at autopsy. Histologic examination of these cases demonstrated a variety of coriduction system abnormalities that were proposed as possible substrate for electrical instability and a mechanism for sudden death. From the Departments of Medicine and Pediatrics, Division of Cardiology, Duke University Medical Center. Supported in part by Grant RR-30 i?om the General Clinical Research Centers Branch, Division of Health Resources, and by Grant HL15190 from the National Institutes of Health, Bethesda, Md. Correspondence: Edward L. C. Pritchett, M.D., P.O. Box 3477, Duke University Medical Center, Durham, NC 27710. ‘Dr. Pritchett is the recipient of NHLBI Young Investigator Research Award HL21347. **This work was done during Dr. Gallagher’s tenure as an Established Investigator of the American Heart Association. 0002-8703/81/050677 + 03$00.30/O 0 1981 The C. V. Mosby Co.
-
Upload
dwight-davis -
Category
Documents
-
view
215 -
download
3
Transcript of Persistent left superior vena cava in patients with congenital atrioventricular preexcitation...
Volume 101
Number 5 Brief Communications 677
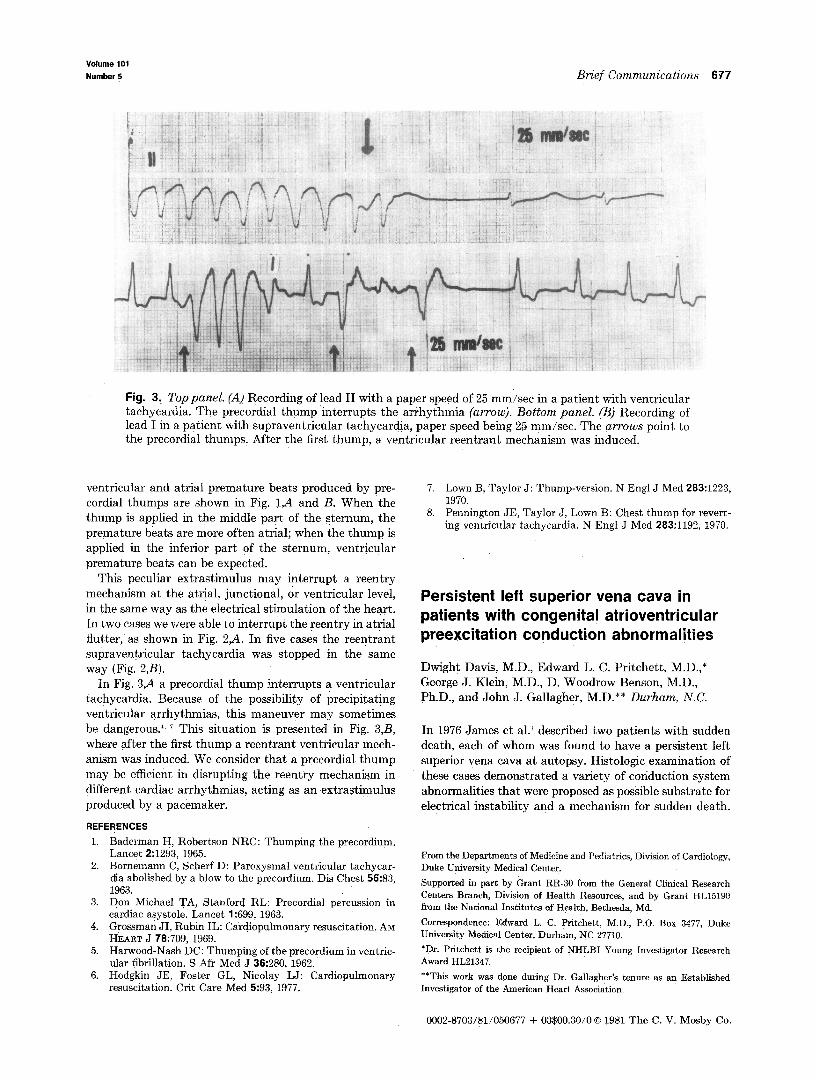
Fig. 3, Top panel. (A) Recording of lead II with a paper speed of 25 mm/set in a patient with ventricular tachycardia. The precordial thump interrupts the arrhythmia (arrow). Bottom panel. (B) Recording of lead I in a patient with supraventricular tachycardia, paper speed being 25 mm/set. The arrows point to the precordial thumps. After the first thump, a ventricular reentrant mechanism was induced.
ventricular and atria1 premature beats produced by pre- cordial thumps are shown in Fig. IA and B. When the thump is applied in the middle part of the sternum, the premature beats are more often atrial; when the thump is applied in the inferior part of the sternum, ventricular premature beats can be expected.
This peculiar extrastimulus may interrupt a reentry mechanism at the atrial, junctional, or ventricular level, in &he same way as the electrical stimulation of the heart. In two cases we were able to interrupt the reentry in atria1 flutter, as showrn in Fig. 2,A. In five cases the reentrant supraventricular tachycardia was stopped in the same way (Fig. 2,B).
In Fig. 3,A a precordial thump interrupts a ventricular tachycardia. Because of the possibility of precipitating ventricular arrhythmias, this maneuver may sometimes be dangerous.i, 7 This situation is presented in Fig. 3,B, where after the first thump a reentrant ventricular mech- anism was induced. We consider that a precordial thump may be efficient in disrupting the reentry mechanism in different cardiac arrhythmias, acting as an extrastimulus produced by a pacemaker.
REFERENCES
1.
2.
3.
4.
5.
6.
Baderman H, Robertson NRC: Thumping the precqrdium. Lancet 2:1293, 1965. Bornemann C, Scherf D: Paroxysmal ventricular tachycar- dia abolished by a blow to the precordium. Dis Chest 56~33, 1963. Don Michael TA, Stanford RL: Precordial percussion in cardiac asystole. Lancet 1:699, 1963. Grossman JI, Rubin IL: Cardiopulmonary resuscitation. AM HEART J 78:709, 1969. Harwood-Nash DC: Thumping of the precordium in ventric- ular fibrillation. S Afr Med J 36:280, 1962. Hodgkin JE, Foster GL, Nicolay LJ: Cardiopulmonary resuscitation. Crit Care Med 5:93, 1977.
7. Lown B, Taylor J: Thump-version. N Engl J Med 283:1223, 1970.
8. Pennington JE, Taylor J, Lown B: Chest thump for revert- ing ventricular tachycardia. N Engl J Med 283:1192, 1970.
Persistent left superior vena cava in patients with congenital atrioventricular preexcitation conduction abnormalities
Dwight Davis, M.D., Edward L. C. Pritchett, M.D.,* Geqrge J. Klein, M.D., D. Woodrow Benson, M.D., Ph.D., and John J. Gallagher, M.D.** Durham, N.C.
In 1976 James et al.’ described two patients with sudden death, each of whom was found to have a persistent left superior vena cava at autopsy. Histologic examination of these cases demonstrated a variety of coriduction system abnormalities that were proposed as possible substrate for electrical instability and a mechanism for sudden death.
From the Departments of Medicine and Pediatrics, Division of Cardiology, Duke University Medical Center.
Supported in part by Grant RR-30 i?om the General Clinical Research
Centers Branch, Division of Health Resources, and by Grant HL15190 from the National Institutes of Health, Bethesda, Md.
Correspondence: Edward L. C. Pritchett, M.D., P.O. Box 3477, Duke University Medical Center, Durham, NC 27710.
‘Dr. Pritchett is the recipient of NHLBI Young Investigator Research Award HL21347.
**This work was done during Dr. Gallagher’s tenure as an Established Investigator of the American Heart Association.
0002-8703/81/050677 + 03$00.30/O 0 1981 The C. V. Mosby Co.
678 Brief Communications
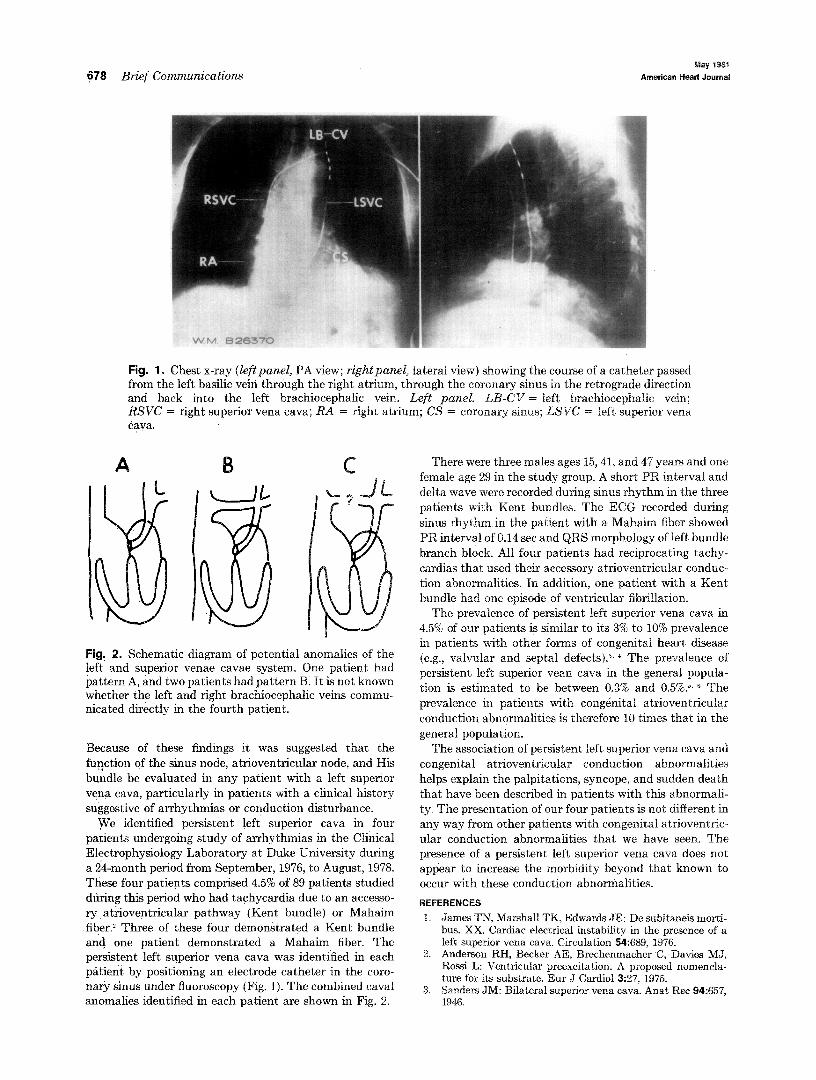
Fig. 1 s Chest x-ray (leftpanel, PA view; rightpanel> lateral view) showing the course of a catheter passed from the left basilic vein through the right atrium, through the coronary sinus in the retrograde direction and back into the left brachiocephalic vein. Left panel. LB-CV = left brachiocephalic vein; RSVC = right superior vena cava; RA = right atrium; CS = coronary sinus; LSVC = left superior vena Cava.
Fig, 2. Schematic diagram of potential anomalies of the !eft and superior venae cavae system. One patient had pattern A, and two patients had pattern B. It is not known whether the left and right brachiocephalic veins commu- nicated directly in the fourth patient.
Because of these findings it was suggested that the fuection of the sinus node, atrioventricular node, and His
bundle be evaluated in any patient with a left superior vena cava, particularly in patients with a clinical history suggestive of arrhythmias or conduction disturbance.
JVe identified persistent left superior cava in four patients undergoing study of arrhythmias in the Clinical Electrophysiology Laboratory at Duke University during a 24-month period from September, 1976, to August, 1978. These four patients comprised 4.5% of 89 patients studied dting this period who had tachycardia due to an accesso- ry at;;ioventricular pathway (Kent bundle) or Mahaim fiber.Y Three of these four demonstrated a Kent bundle and one patient demonstrated a Mahaim fiber. The persistent left superior vena cava was identified in each patient by positioning an electrode catheter in the coro- nary sinus under fluoroscopy (Fig. 1). The combined caval anomalies identified in each patient are shown in Fig. 2.
There were three males ages i&41, and 47 years and one female age 29 in the study group. A short PR interval and delta wave were recorded during sinus rhythm in the three patients with Kent bundles. The ECG recorded during sinus rhythm in the patient with a Mahaim fiber showed BR interval of 0.14 set and QRS morphology of left bundle branch block. All four patients had reciprocating tachy- cardias that used their accessory atrioventricular conduc- tion abnormalities. In addition, one patient with a Kent bundle had one episode of ventricular fibrillation.
The prevalence of persistent left superior vena cava in 4.5% of our patients is similar to its 3% to 10% prevalence in patients with other forms of congenital heart disease (e.g., valvular and septai defects).‘.’ The prevalence of persistent left superior vean cava in the general popula- tion is estimated to be between 0.3% and 0.5%.>. 6 The prevalence in patients with cong&ital atrioventricular
conduction abnormalities is therefore 10 times that in the general population.
The association of persistent left superior vena cava and congenital atrioventricular conduction abnormalities helps explain the palpitations, syncope, and sudden death that have been described in patients with this abnormali- ty. The presentation of our four patients is not different im any way from other patients withcongenital atrioventric- ular conduction abnormalities that we have seen. The presence of a persistent left superior vena cava does not appear to increase the morbidity beyond that known to occur with these conduction abnormalities.
REFERENCES
1. James TN, Marshall TK, Edwards JE: De subitaneis morti- bus. XX. Cardiac electrical instability in the presence of a left superior vena cava. Circulation 54:689, 1976.
2. Anderson RH, Becker AE, Brechenmacher 6, Davies MJ, Rossi L: Ventricular preexcitation. A proposed nomencla- ture for its substrate. Eur J Cardiol3:27, 1975.
3. Sanders JM: Bilateral superior vena cava. Anat Ret 943657, 1946.
Volume101
Number5 Brief Communications 679
4.
5.
6.
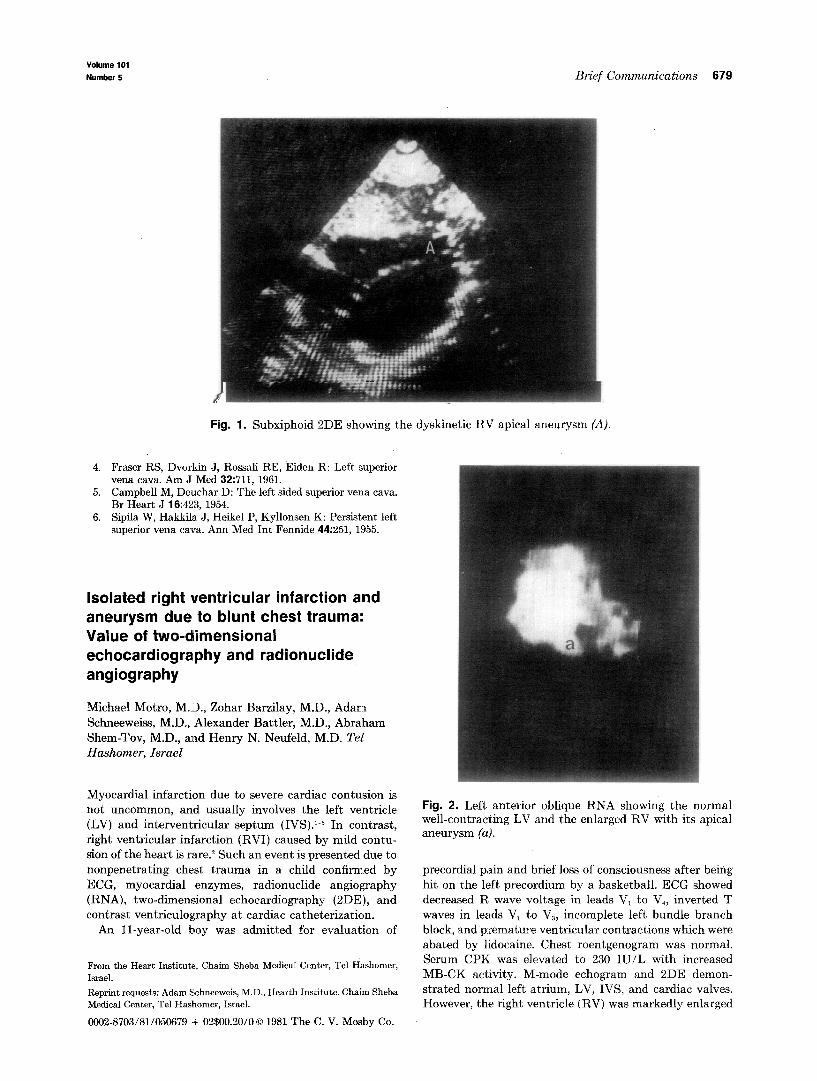
Fig. 1. Subxiphoid 2DE showing the dyskinetic RV apical aneurysm (A).
Fraser RS, Dvorkin J, Rossali RE, Eiden R: Left superior vena cava. Am J Med 32:711, 1961. Campbell M, Deuchar D: The left sided superior vena cava. Br Heart J 16:423, 1954. Sipila W, Hal&la J, Heikel P, Kyllonsen K: Persistent left superior vena cava. Ann Med Int Fennide 44:251, 1955.
Isolated right ventricular infarction and aneurysm due to blunt chest trauma:: Value of two-dimensional echocardiography and radionuclide angiography
Michael Motro, M.D., Zohar Barzilay, M.D., Adam Schneeweiss, M.D., Alexander Battler, M.D., Abraham Shem-Tov, M.D., and Henry N. Neufeld, M.D. Tel Hashomer, Israel
Myocardial infarction due to severe cardiac contusion is not uncommon, and usually involves the left ventricle (LV) and interventricular septum (IVS).1-3 In contrast, right ventricular infarction (RVI) caused by mild contu- sion of the heart is rare.? Such an event is presented due to nonpenetrating chest trauma in a child confhmed by ECG, myocardial enzymes, radionuclide angiography (RNA), two-dimensional echocardiography (2DE), and contrast ventriculography at cardiac catheterization.
An D-year-old boy was admitted for evaluation of
From the Heart Institute, Chaim Sheba Medical Center, Tel Hashomer, Israel.
Reprint requests: Adam Schneeweis, M.D., Hearth Institute, Chaim Sheba Medical Center, Tel Hashomer, Israel.
0002~8703/81/050679 + 02$00.20/O 0 1981 The C. V. Mosby Co.
Fig. 2. Left anterior oblique RNA showing the normal well-contracting LV and the enlarged RV with its apical aneurysm (a).
precordial pain and brief loss of consciousness after being hit on the left precordium by a basketball. ECG showed decreased R wave voltage in leads V, to V,, inverted T waves in leads V, to V,, incomplete left bundle branch block, and premature ventricular contractions which were abated by 1:idocaine. Chest roentgenogram was normal. Serum CPK was elevated to 230 IU/L with increased MB-CK activity. M-mode echogram and 2DE demon- strated normal left atrium, LV, IVS, and cardiac valves. However, the right ventricle (RV) was markedly enlarged


















