Peritoneal Dialysis Kidney A&P. I. Kidneys A. Location - back of the abdominal cavity. The right...
47
Peritoneal Dialysis Kidney A&P
-
Upload
aubrey-casey -
Category
Documents
-
view
215 -
download
0
Transcript of Peritoneal Dialysis Kidney A&P. I. Kidneys A. Location - back of the abdominal cavity. The right...

Peritoneal Dialysis
Kidney A&P

I. Kidneys
A. Location - back of the abdominal cavity. The right kidney is lower than the left due to the liver
B. Size approx. same size
as your fist
4" long (12cm) 1-1/2" thick (3cm) 2-1/2“ wide (6 cm) weighs:1/3 lb (150 gm)
C. Layers
1. Cortex- outermost layer (85% nephrons)
shorter cortical nephrons (excretory/regulatory)
2. Medulla- middle layer (15% nephrons) longer juxtamedullary
nephrons (concentration and dilution of urine)
3. Pelvis- inner layer (collecting system- urine)
D. Blood flow through the Kidneys
Heart pumps approx.1.2 liter blood/min to the kidneys via the renal artery. Blood then travels through a series of smallerarteries and then enters the glomeruli. Some of thefluid is filtered out of each glomerulus and thenmoves into Bowman's capsule. The filtrate thenmoves through the tubules where most ofThe sugar, water, and minerals are reabsorbed back into the blood vessels. The filtrate then goes into the renal pelvis.
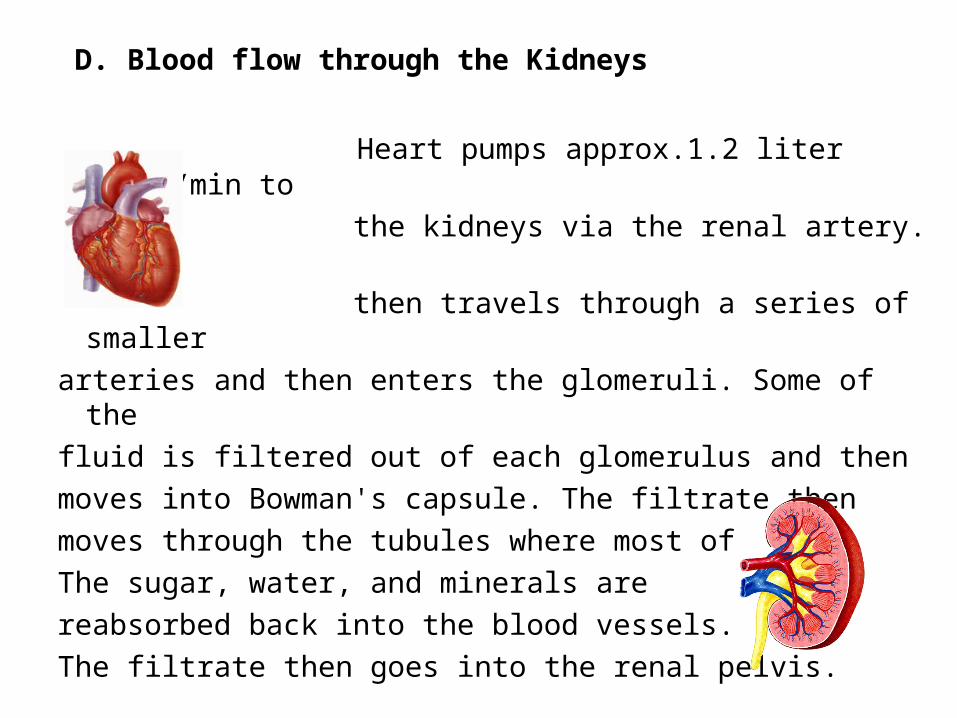
E. Nephrons Functional units of the kidney. Approximately one million in the cortex and medulla of each kidney
CorticalNephron
JuxtamedularyNephron

1. Glomerulus filters blood approx.1200 ml/min (1/4 cardiac output)
2. Bowman's Capsule surrounds the glomerulus and collects the filtrate
distal convoluted tubule
efferent arteriole- blood out
afferent arteriole- blood in

3. Juxtaglomerular Apparatus
macula densa and
juxtaglomerular cells
(1) systemic BP and volume control via therenin-angiotensin system
(2) local control of the (GFR) by nitric oxide production
(3) the production of erythropoietin in response to decrease in O2.

4. Tubules
Proximal Convoluted- where 60%-70% filtrate containing water, glucose, nutrients, amino acids & ions from the glomerulus is re-absorbed into the capillaries.

Loop of Henley- concentration of urine occurs (descending) water excreted
(ascending) Na+, K+, Cl- excreted

Distal Convoluted Tubulesregulation electrolytes, H2O and pH(aldosterone- Na+) (ADH- water)
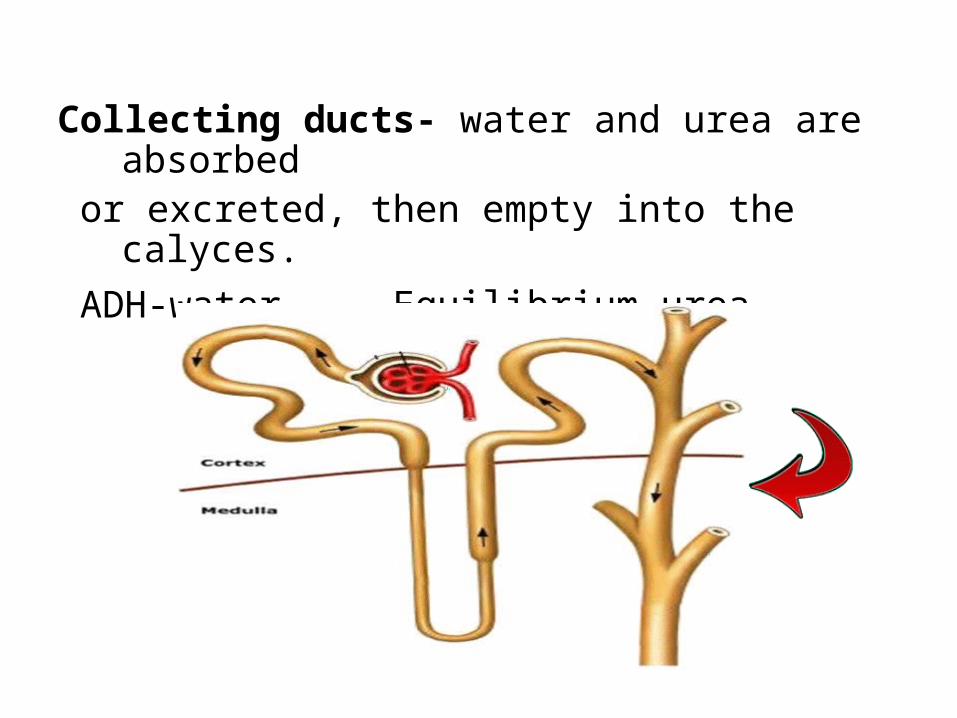
Collecting ducts- water and urea are absorbed or excreted, then empty into the calyces. ADH-water Equilibrium-urea
F. Major Functions
1. Remove water, urea, creatinine, and uric acid (components of urine)
2. Maintain electrolyte balance
3. Maintain acid/base balance by removing or retaining H+ / HCO3 ions
4. Regulate blood pressure by initiating renin / angiotensin response
5. Release erythropoietin to help maintain RBC production
6. Detoxification & elimination of toxins, drugs, and their metabolites

Peritoneal Dialysis
Renal Failure
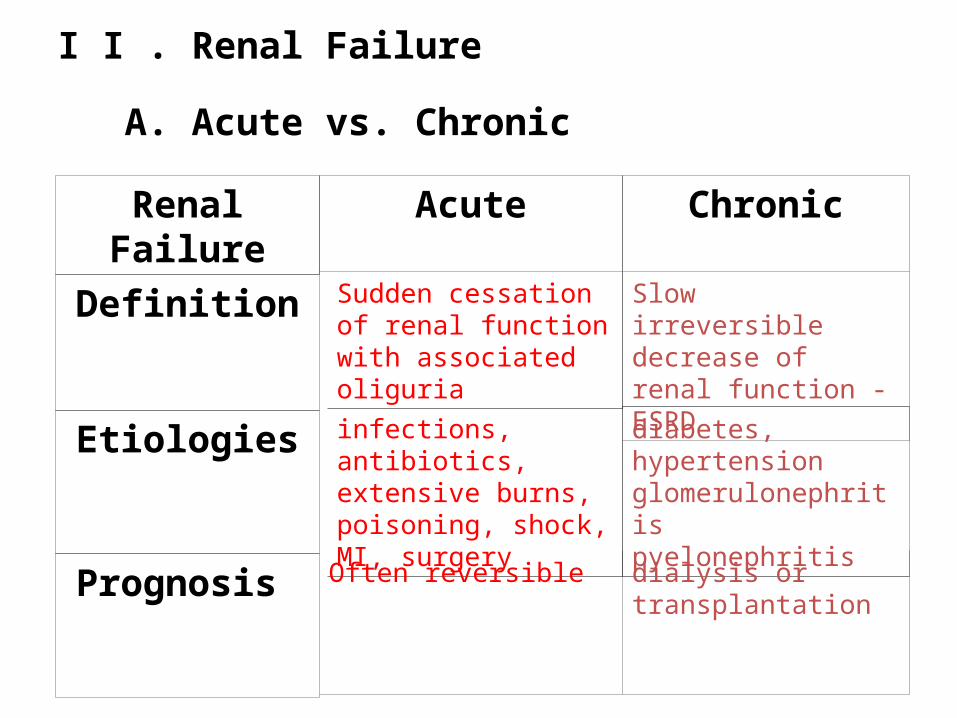
I I . Renal Failure
A. Acute vs. Chronic
Renal Failure
Definition
Etiologies
Prognosis
Acute Chronic
Sudden cessation of renal function with associated oliguria
infections, antibiotics, extensive burns, poisoning, shock, MI, surgery
Often reversible
Slow irreversible decrease of renal function - ESRD
diabetes, hypertension
glomerulonephritis pyelonephritis
dialysis or transplantation

B. Types
1. Pre-Renal
a) Definition Any condition that impairs renal blood flow. Nephrons remain intact but decreased blood supply causes a drop in the glomerular filtration rate which results in decreased urine output
b) Causes
cardiac disorders- arrhythmias, chf, cardiac tamponade, MI
vasodilatation- sepsis, anaphylaxis, medications, OD
hypovolemia- hemorrhage, third spacing, shock, diuretics diabetes insipidus, burns, dehydration, vomiting, diarrhea, cirrhosis
vascular- thrombus, stenosis, surgical clamping (AAA repair)

2. Renal (Intra-Renal)
a) Definition direct damage to the kidneys
b) Causes
Pyelonephritis - infection of the kidneys from UTI (E.coli)
Glomerulonephritis - antigen/antibody complexes (strep throat)
Systemic lupus - connective tissue disorder
Hereditary lesions - polycystic kidneys
Acute Tubular Necrosis - anesthesia, radiographic dyes, lasix, vancomycin, corticosteroids, Amphotericin-B, ibuprophen, rhabdomyolysis, prolonged pre-renal causes
3. Post-Renal
a) Definition obstruction of the
urinary system
b) Causes prostatic hypertrophy, renal calculi, tumors, blood clots, pregnancy
C. Stages of Chronic Renal Failure (normal GFR is 125 mL/min/1.73 m2)
• STAGE 1 Kidney damage with normal GFR ( ≥90)
• STAGE 2 Mild decrease in GFR (60-89)
• STAGE 3 Moderate decrease in GFR (30-59)
• STAGE 4 Severe decrease in GFR (15-29)
• STAGE 5 Kidney failure (GFR <15)

Glomerular Filtration Rate
Serum Creatinine (mg/dl)
Age
Male/Female
African American
GFR (mL/min/1.73 m2) = 186 x (Scr)-1.154 x (Age)-0.203 x (0.742 if female) x (1.212 if African-
American)

D. Symptoms
1. weakness, fatigue 2. drowsiness, confusion 3. restless legs 4. itching 5. dry flaky skin 6. loss of appetite 7. metallic taste 8. nausea/vomiting
9. edema, puffiness around eyes 10. shortness of breath 11. high blood pressure 12. muscle cramping13. decreased sexual interest 14. decreased urinary frequency 15. amenorrhea16. testicular atrophy
Symptoms (continued)

E. Complications As renal function declines, the end products of protein
metabolism accumulate in the blood and adversely affect every system in the body.
1. Hyperkalemia 2. Metabolic Acidosis 3. Pericarditis (effusion / tamponade) 4. Pulmonary Edema 5. Hypertension 6. Anemia 7. Bone disease 8. Vascular calcifications


1. Transplantation
F. Treatment Options
2. Dialysis a) hemodialysis b) CRRT (ICU) c) Peritoneal
3. No Treatment
ComplicationsTransplantation
Pain/Discomfort of Surgery
Risk of Rejection
Frequent Medical Needs
Weakened Immune System
Side Effects of Medications
Cancer (skin)
Stress
Cost
Hemodialysis
Bleeding (anticoagulation)
Clotting in dialyzer
Disequilibrium syndrome
Muscle cramping
Hypotension
Air emboli
Fever / Infection
Arrhythmias
Angina
Complications Peritoneal Dialysis
Abdominal pain / cramps Anorexia Nausea Reflux Hernias
Weight gain Peritonitis Exit site infection Dyspnea (fluid retention)
Peritoneal Dialysis
C A P D
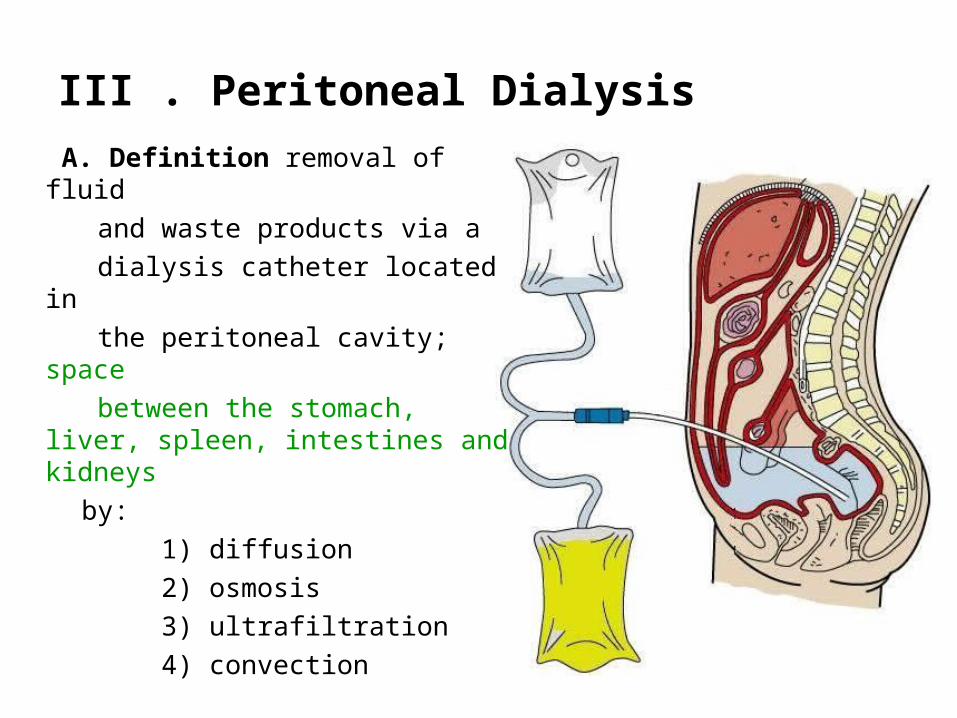
III . Peritoneal Dialysis
A. Definition removal of fluid and waste products via a dialysis catheter located in the peritoneal cavity; space between the stomach, liver,
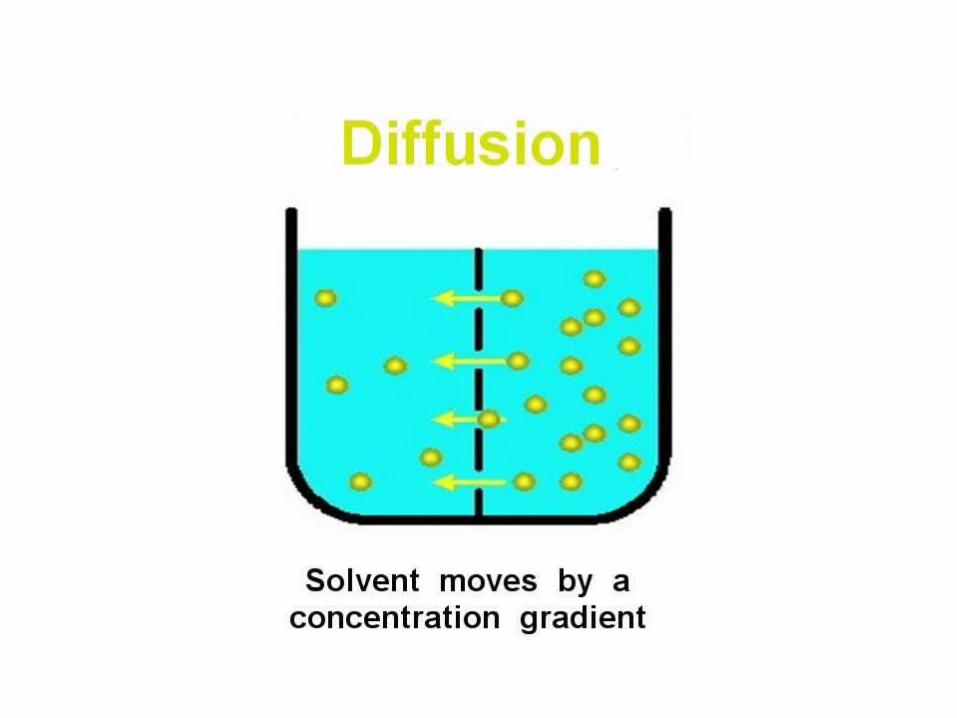
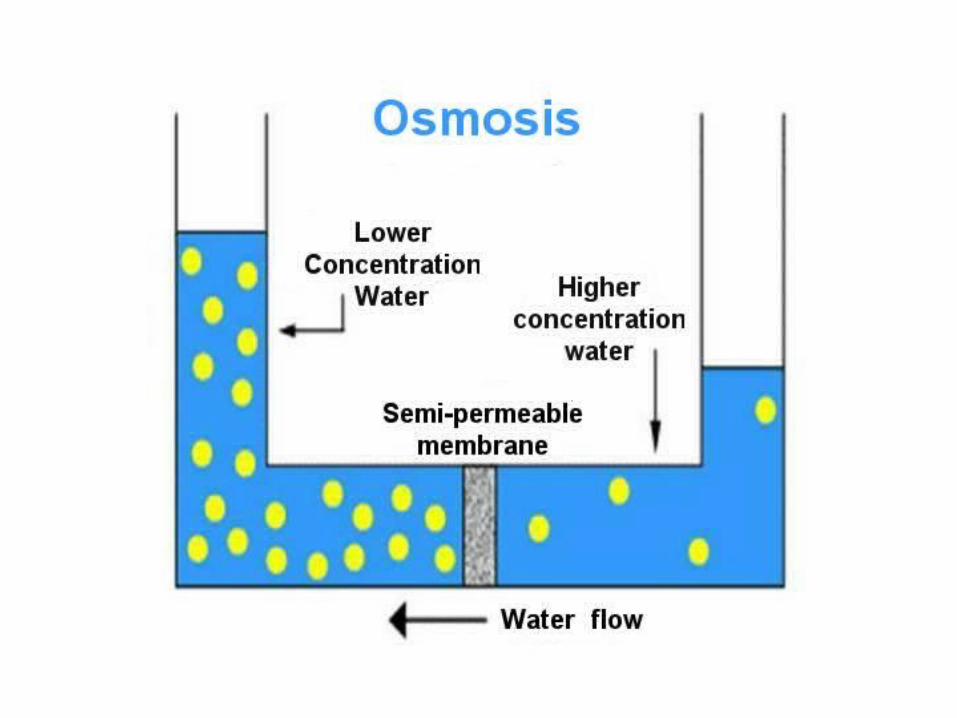
spleen, intestines and kidneys by: 1) diffusion 2) osmosis 3) ultrafiltration 4) convection

Ultrafiltration Occurs because of a
pressure gradient
Convection Occurs as solvent
drag. Solvent brings the solute with it.

B. Process
3. Drain - After a specified dwell time the
fluid containing the waste and excess fluid
is drained out.
1. Infusion- 1 to 3 liters of sterile dialysate solution is infused through the dialysis catheter into the abdominal cavity which comes into contact with the peritoneal membrane.
2. Dwell - The membrane is semi-permeable and acts as a filter which allows waste products and excess fluid to pass from the blood stream, across the membrane and into the dialysis solution.
(however!!!)
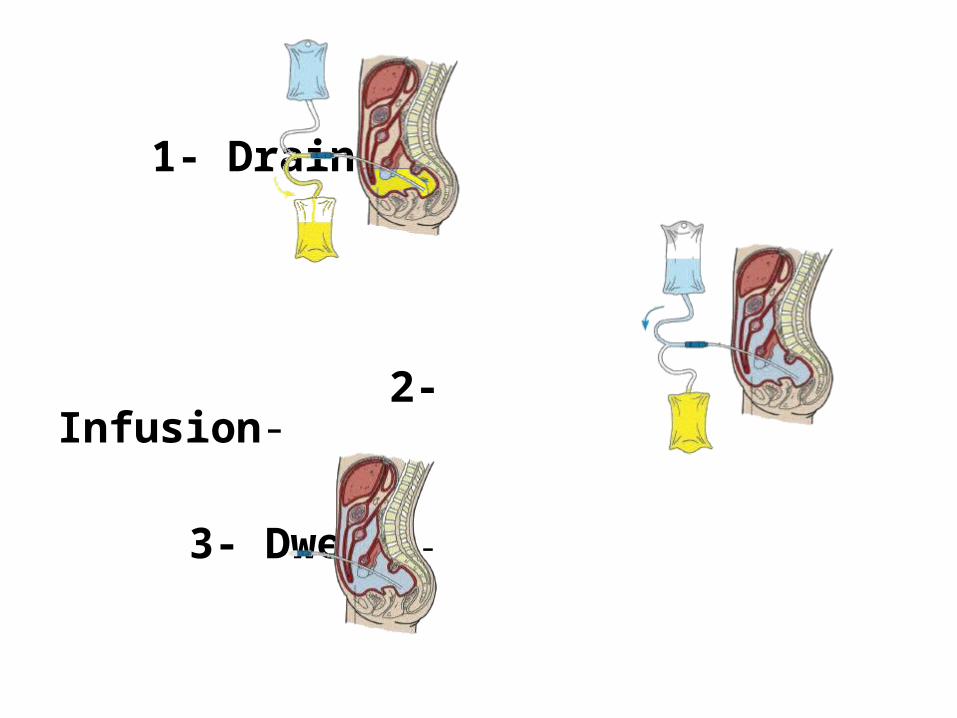
1- Drain -
2- Infusion-
3- Dwell -

C. Types
1. CCPD - Continuous Cycler Peritoneal Dialysis (or APD - Automated PD). Cycler is used during the night to perform up to 8 exchanges. Long dwell during the day
2. CAPD - Continuous Ambulatory Peritoneal Dialysis 4 or 5 exchanges per day
D. Dialysate 1. Definition: Fluid containing dextrose and
electrolytes
2. Concentrations: Higher concentrations of glucose pull more fluid a) 1.5%
b) 2.5% c) 4.25%

ƒ
Recent findings have shown that it improvesthe long-dwell ultrafiltration and clearance of creatinine and urea compared to 4.25% dextrose.
EXTRANEAL is a glucose-free polymer that is indicated for a single daily exchange for the long 8-16 hour dwell during CAPD or APD.



3. Possible Additives
a) heparin b) insulin (added by pharmacy)
c) antibiotics (added by pharmacy)
d) potassium (added by pharmacy)

Advantages
1. flexible schedule
2. less expensive than Hemodialysis
3. fairly easy to learn
4. fewer dietary restrictions
5. no needles required
6. dialysis can be done at home, on vacation or wherever you are
7. no blood loss
8. continue daily activities
Disadvantages
1. burn out, no days off
2. procedure must be followed exactly to prevent peritonitis
3. altered body image
4. risk of infection
5. permanent catheter access
6. larger clothing size because of fluid in the peritoneal cavity
7. some protein loss
8. storage space (supplies)

Peritoneal Dialysis
Nursing Responsibilities
IV Nursing responsibilities
A. room environment - during bag connection, tubing change, adding meds, exit-site care for recent post ops
1. prefer a private room (roommate approved by MD) 2. air vent covered 3. door closed (sign on door) Procedure in Progress Do Not Enter 4. curtain pulled 5. mask on patient, roommate, staff

B. accurate I&O
C. daily weights abdomen must be empty,
weigh after first AM drain
D. exit site care (daily)
immediately post-op - do not disturb
recent post-op - ExSept
long standing - soap & water

E. phosphate binders must be given immediately before or after meals, otherwise they are calcium supplements Examples:. PhosLo, Renagel, Ca+ carbonate (Tums)
F. sorbitol standing order. No fleets enema or MOM.
(Mg+ not removed by dialysis)
G. tubing clamps soak in hibiclens / betasept (in open position)
rinse off prior to use change solution every 24hrs.
H. IV rates watch, especially pre-op and post-op patients. Use IV Pump!
I. insulin is stable 2 hrs. in the warmer 24 hrs. out of the warmer
J. potassium is stable 1 hr after added (adheres to bag)

K. heparin should be added to the bag prior to the infusion during the current exchange. Does not cross the peritoneal membrane so does not cause systemic anticoagulation
L. Specimens C & S – aerobic & anaerobic culture bottles, 30ml extra in sterile specimen cup
Cell Count – lavender top tube
(must hand deliver specimens to the lab!)
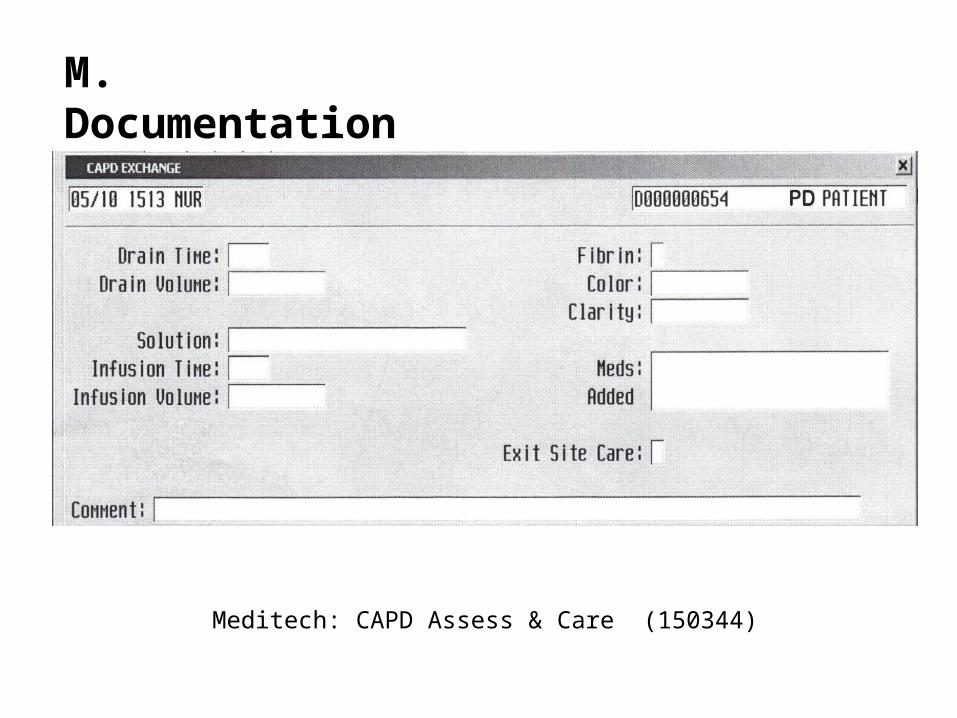
M. Documentation
Meditech: CAPD Assess & Care (150344)