
Peripheral vascular diseases Dr Seyed Mostafa Shiryazdi Associate professor of surgery.
55
Peripheral vascular diseases Dr Seyed Mostafa Shiryazdi Associate professor of surgery
-
Upload
elaine-moore -
Category
Documents
-
view
213 -
download
0
Transcript of Peripheral vascular diseases Dr Seyed Mostafa Shiryazdi Associate professor of surgery.

Peripheral vascular diseases
Dr Seyed Mostafa Shiryazdi
Associate professor of surgery

Section 1 Introduction Pain 1 intermittent pain• (1) physical activity : intermittent
claudication, Cramping or fatigue of major muscle
groups in one or both lower extremities that is reproducible upon walking a specific distance suggests intermittent claudication, and it is relieved by several minutes of rest.

• (2) limbs position
• (3) change of tempreture
2 Continuous pain (rest pain, or pain at rest)
• (1) arterial pain at rest
• (2) venous pain at rest
• (3) inflammatory or ischemic pain at rest

Edema
• 1 venous edema
• 2 lymphedema
Paresthesias
• 1 heaviness
• 2 abnormal sensation: numbess, tingling, burning,
• 3 lose of sensation

Change of skin temperature
Changes of skin color
• 1 normal and abnormal color
• 2 changes of color with pressure
• 3 changes of color in physical activity:
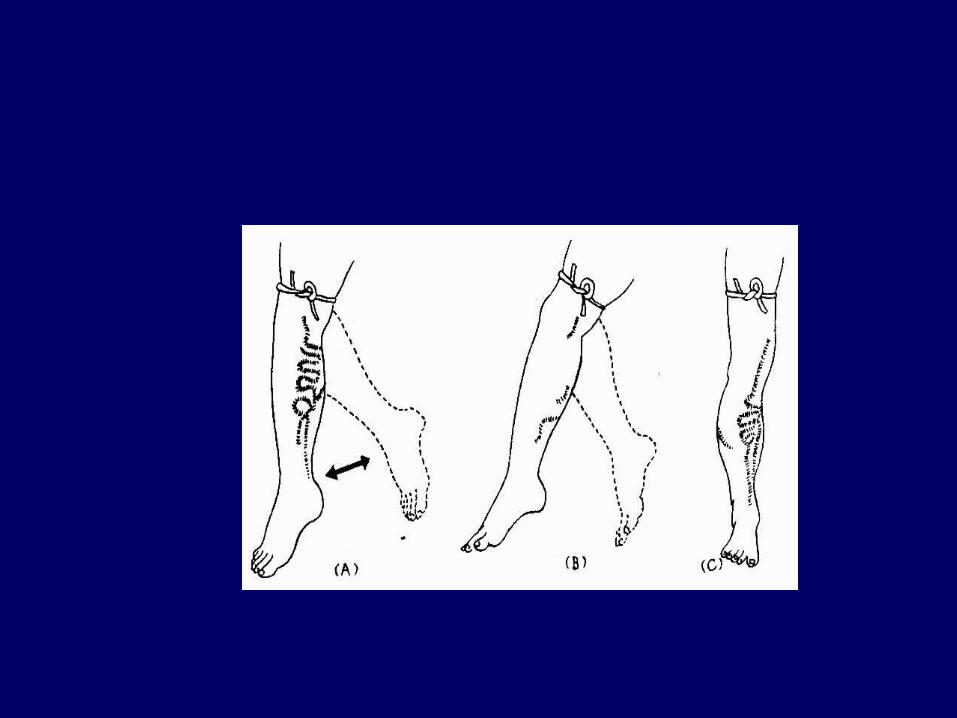
• 4 changes of color in different position : Buerger test
Changes of shape
• 1 shape changes of artery:
1) pulses decrease or disappear
2) murmur
3) form and texture
• 2 shape changes of vein

Mass
• 1 pulsatile mass
• 2 non-pulsatile mass
Skin nutritional changes
• 1 nutritional dysfunction of skin
• 2 ulceration, and gangrene
• 3 limbs grow

Section 2 Thromboangiitis Obliterans
( Buerger Disease )
• Thromboangiitis obliterans is a nonatherosclerotic, segmental, inflammatory, vasoocclusive disease that affects the small and medium-sized arteries and veins of the upper and lower extremities, cyclic upset.
• more common in males, aged 20-45 years.

etiology
unclear
• 1 external factors: tobacco, cold or humid weather, chronic trauma, infection
• 2 internal factors: immunologic dysfunction
• exposure to tobacco is essential for both initiation and progression of the disease.

Pathology
• 1 begin with artery, then vein, from distal to proximal.
• 2 segmental disease• 3 in active stage, nonsuppurtive
inflammation• 4 in end stage, intraluminal thrombosis
progressively organizes, new capillary formation, vascular fibrosis
• 5 ischemic change
Clinical findings
• 1 The hands and feet are usually cool.
• 2 skin is pale, or cyanosis.
• 3 Paresthesias.
• 4 pain in limbs, intermittent claudication
• 5 changes of nutritional dysfunction

• 6 impaired distal pulses in the presence of normal proximal pulses.
• 7 migratory superficial thrombophlebitis.
• 8 painful ulcerations and/or frank gangrene of the digits.

Clinical stage
• First stage: local ischemic stage
• Second stage: nutritional ischemic stage
• Third stage: necrotic stage


Diagnosis
1 Age younger than 45 years, current (or recent) history of tobacco use
2 Presence of distal-extremity ischemia
3 History of migratory superficial thrombophlebitis
4 Impaired distal pulses.
5 Exclusion of autoimmune diseases, hypercoagulable states, and diabetes mellitus by laboratory tests

General examination
• 1 claudication distant and claudication time
• 2 skin temperature
• 3 Buerger test
• 4 tension relief test

Special examination
• 1 Doppler examination
• 2 arteriography: formation of distinctive small-vessel collaterals around areas of occlusion known as "corkscrew collaterals"

Differential diagnosis
• 1 Atherosclerosis obliterans
• 2 Takayasu’s arteritis
• 3 Diabetes mellitus

Treatment
• 1 General treatment
• Absolute discontinuation of tobacco use is the only strategy proven to prevent the progression of Buerger disease.
• prevent trauma and thermal or chemical injury, avoidance of cold environments, drugs that lead to vasoconstriction
• Buerger exercise

• 2 Medication
• (1) Chinese traditional treatment
• (2) vasodilators, antiplatelet drugs, and anticoagulants
• (3) antibiotics to treat infected ulcers

• 3 hypertension oxygen treatment• 4 surgical treatment• to improve distal arterial flow• (1) lumber sympathectomy• (2) vascular reconstructive procedures:
bypass transfer, thrombosis • Others: Omental transfer • Arteriovenous transfer• 5 distal limb amputation for nonhealing
ulcers, gangrene

图 1 动脉旁路移植
• bypass graft

Section 3 Arteriosclerosis obliterans
• lower extremity atherosclerosis is a marker for systemic atherosclerotic disease, involving large and medium arteries, the iliac, femoral, popliteal, and/or infrapopliteal arteries
• advancing age, male sex

Etiology and pathology
• risk factors: hypertension, abnormal serum lipid levels, cigarette smoking, impaired glucose tolerance, and obesity
• Mechanism
• Pathology: atherosclerotic plaque

Clinical manifestation and diagnosis
• Early stage: intermittent claudication, Impaired distal pulses, changes of nutritional dysfunction, the limb is perfused via collateral pathways
• Late stage: rest pain• Loss of pedal pulses is characteristic of
disease of the distal popliteal artery or its trifurcation.
• the dorsalis pedis pulse, the posterior tibial pulse

• 1 general examination: ECG
• 2 noninvasive examination: Doppler
• 3 X-ray
• 4 arteriography, MRA (Magnetic resonance angiography), DSA

Differentiation of Arteriosclerosis
obliterans and thromboangiitis Obliterans Arteriosclerosis obliterans
Thromboangiitis Obliterans
age >45 <45
superficial thrombophlebitis
no common
Hypertension, coronary heart disease
common uncommon

Involving vessels large and medium arteries
the small and medium-sized arteries and veins
Change of other arteries
common no
Calcification of involving arteries
Can be found no
arteriography Extensive irregular stenosis and segmental occlusion
Segmental occlusion, others are normal

Treatment
• 1 nonoperative treatment
• 2 surgical treatment
• (1) percutaneous transluminal angioplasty
• (2) endarterectomy
• (3) vascular bypass surgery

Section 4 Arterial embolism
• acute arterial occlusion
• Etiology and pathology

Clinical Manifestation
• Pain
• Paresthesias
• Paralysis
• Pulselessness
• Pallor, coolness
• Other general symptoms

Examination and diagnosis
• 1 skin temperature
• 2 Doppler examination
• 3 arteriography

Treatment
• The usual immediate management of acute arterial occlusion is immediate heparin anticoagulation and rapid surgical thromboembolectomy.
• 1 nonoperative treatment• 2 surgical therapy: direct
thromboembolectomy, Fogarty cancal thromboembolectomy

Complication of operation
• the possibility of reperfusion complications such as compartment syndrome or myopathic-metabolic-nephrotic syndrome

Section 5 Introduction of venous diseases
• the lower extremities:
• 1 superficial veins, include the lesser and greater saphenous veins and their tributaries. These include the lateral and medial femoral cutaneous branches, the external circumflex iliac vein, the superficial epigastric vein, and the internal pudendal vein

• 2 deep veins, include the anterior tibial, posterior tibial, peroneal, popliteal, deep femoral, superficial femoral, and iliac veins.
• 3 muscular vein
• 4 perforating or communicating veins


Dynamics of blood flow
• 1 muscular pump
• 2 negative pressure in thoracic cavity
• 3 valve function

Pathophysiology
• Most varicose disease is caused by elevated superficial venous pressures, but some people have an inborn weakness of vein walls

Section 6 Simple lower extremity varicose veins
• normal veins have dilated under the influence of increased venous pressure. allow venous blood to escape from its normal flow path and flow in a retrograde direction down into an already congested leg.

Etiology and pathophysiology
• Prolonged standing leads to increased hydrostatic pressures that can cause chronic venous distention and secondary valvular incompetence anywhere within the superficial venous system.
• If proximal junctional valves become incompetent, high pressure passes from the deep veins into the superficial veins and the condition rapidly progresses to become irreversible.

Clinical manifestation and diagnosis
• Symptoms: uncomfortable, annoying, or cosmetically disfiguring, pain, soreness, burning, aching, throbbing, cramping, muscle fatigue
• Signs: dilated vessels, mild swelling. inflammatory dermatitis, recurrent or chronic cellulitis, cutaneous infarction, ulceration, and even malignant degeneration.

• 1 Trendelenburg test
• 2 Perthes test
• 3 Pratt test
• 4 others: Doppler, angiography


Differentiated diagnosis
• 1 primary lower extremity deep vein valve insufficiency
• 2 sequela of deep vein thrombosis
• 3 arteriovenous fistula

Treatment
• Treatment is indicated whenever venous reflux produces secondary skin or subcutaneous tissue changes, symptomatic varicose veins

• 1 Nonoperative treatment: compression stockings, keeping the legs elevated
• 2 Injection sclerotherapy
• 3 Operation: Vein ligation, stab evulsion technique, communicating veins ligation

complications
• 1 Superficial thrombophlebitis
• 2 ulceration
• 3 Varicose veins bleeding

Section 7 primary lower extremity deep vein valve
insufficiency
• Etiology and pathophysiology
Congenital absence of or damage to venous valves in the superficial and communicating systems
• Clinical finding and diagnosis
• Mild, moderate, severe

Examination
• 1 angiography
• 2 venous pressure
• 3 noninvasive examination

Treatment
• Reconstruction of deep venous valves

Section 8 Deep venous thrombosis
• formation of thrombi, ---chronic venous insufficiency
• Etiology and pathophysiology• Virchow triad (venous stasis,
hypercoagulability, endothelial trauma)

Clinical finding and types
• 1 upper extremity deep venous thrombosis
• 2 inferior vena cava or superior vena cava thrombosis
• 3 lower extremity deep venous thrombosis

Examination and diagnosis
• Prevention and treatment• 1 nonoperative treatment
• 2 operation
• Complications and sequela


















