Peripheral nerve blocks 1 by dr.mushtaq
67
1
-
Upload
mushtaq-ahmed -
Category
Documents
-
view
198 -
download
2
description
Transcript of Peripheral nerve blocks 1 by dr.mushtaq

1

PERIPHERAL NERVE BLOCKS
DR.MU
SHTAQ
AHMA
D
2

INTRODUCTION
Local anesthetic induced blockade of peripheral nerve impulses from a targeted body part with preserved level of consciousnessInjecting local anesthetic near the course of a named nerve •Surgical procedures in the distribution of the blocked nerve
3

STRUCTURE OF NERVE4

CLASSIFICATION
Regional anaesthesiaCentral neuraxial blocks
Subarachnoid
epidural
Peripheral blocksTruncal
Plexus
Distal
Field & topical
IV regional anaesthesia
5

ADVANTAGES
Avoids general anaesthesia complications
• Safer than GA especially when anaesthetist is inexperienced
Pt remains awake .....pt will & helpfull for suegeon----feedback
Postops analgesia----continue / catheter
Less PONV-----less opiods need
Less post ops sedation------less confision(cognitive functions) in elderly
6

Faster return to street fitness & early discharge
Cheep & relatively safe in remote location
hemodynamic stability than neuraxial & GA
Sole anesthetic technique , supplemented with monitored anesthesia care (moderate sedation) or with a "light" general anesthetic
Premptive analgesia
7

Less immunosuppressive than GA
• Hemodynamically compromised• Too ill to tolerate GA• MH• PONV is risk
Excellent alternative to GA
• Modern equipments—USG,Nerve stimulator ect
Growing populalarity of RA & PNB
8

DISADVANTAGES
TIME DELAY
• 15-30 MIN –Procedure & onset
PATIENT FACTORS
• Discomfort due to procedure & positioning & awake during surgery• Distress due to paralysis & numbness---postops• Managed easily—benzodizepine & opiods
SURGEON FACTORS
• Irritated by awake & conversation with surgeon
ANAESTHETIST FACTORS
• Skill,knowledge & proper equipments
BLOCK FAILURE
9

10

NERVE DEMAGE
• Chronic paresthesias• Permanent N demage
FAILURE RATE-----10%
• If No catheter----GA
SURGERY OUTLASTS THE BLOCK
• Respiratory failure-phrenic N Block• Seizures ---intraarterial injecton
LOCAL ANAESTHETIC TOXICITY
SPECIFIC COMLPICATIONS RELATED TO NERVE BEING BLOCKED
11

CONTRAINDICATIONS OF PNB
CI
ABSOLUTE RELATIVE
12

ABSOLUTE COTRAINDICATI
ONS Patient refusal• Hemophilia• DIC• Anticoagulant drugs
Inexperienced ,incompetent anaesthetist
Major coagulation disorders & drugs
Infection at site
13

Related to specific N Block
• Interscalene block• with contralateral phrenic N paralysis• Severe pulmonary disease
Increased risk fo LA toxicity
• Bilateral axillary Block• Multiple intercostal blocks
LA Allergy
• Penile block,toes,fingers etc
Ring block at site---endarteries---LA containing Adrenaline
14

RELATIVE COTRAINDICATI
ONSDemented , combative & uncooperative patients
Pediatric patients
Placing block under GA
Surgeons who feel uncomfortable
Uncertain duration of surgery
Bloodstream infection
Preexisting peripheral neuropathy
15

COMPLICATIONS
Local anaesthetic toxicity
Nerve damage
Vasoconstrictor problems
Infection
16

Haematoma• Bleeding diorder• Anticoagulant drugs
Wrong drug• supra &infra clavicular• inter costal block
Pneumothorax• Vasovagal –mistaken as LA toxicity• Anxious pt--sedate
Psychological reaction
17

1.LA TOXICITY
Immediate or delayed-----signs & symptoms (CNS & CVS)
• Maintain IV line before• Have resuscitation equipments & drugs• Always aspirate before injecting• Inject slowly & aspirate after every 3-5 ml• Stablize needle ……short fine bone plasting tubing b/w needle & synge (isolated needle technique)• Observe pulse,ECG & sign of IV injection
Prevention ---always
18

UNIPOLAR INSULATED
NEEDLE19

2.NERVE DEMAGE
Direct by needle or by injection of LA
• Withdraw 1-2 mm after eliciting paraesthesia-before injection
Eliciting paraesthesia technique -----can demage
• 1 in 1000 blocks• Most dysaesthesiasis & paresis resolve—few months• 1 in 10000 blocks=permanent demage
Incidence---experienced anaesthetist
20

RECOMMENDATIONS TO REDUCE RISK OF
NERVE DEMAGE
Use short bevel needle
• STOP –undo resistance & severe pain-----withdraw & then reinject
Use nerve stimulator & insulated short bevel needle
Avoid rapid,forceful injection
Avoid block under GA
21

4.VASOCONSTRICTOR PROBLEM
General rule—epinephrine should not be used in concentration > 1:200000 (5ug/ml) in PNB
• Skin ----- 1:300000 or 1:400000 sufficient• Dentist –1:80000 but in small vol
Never use----areas of endarteries
Careful-----ischemic areas---varicose leg ulcer
22

H/O IHD-----avoid/reduce dose---- can cause palpatation,angina,HTN• Adding sodium bicarbonate• Felypressin in stead of epinephrine• Warming the sol to body tempPregnancy-----epinephrine in significant quntity -----avoid /reduce dose
Max recommended dose of epinephrine--- 4 ug/kg
Epinephrine sol-----lower Ph--pain on injection-----can be reduced by
23

INFECTION
Aseptic technique
• 1% chlorhexidine in 75% alcohol—allergic to iodine
No needle prick through infected skin except abscess
Use atiseptic Alcoholic Betadine(povidone/ iodine in ethanol)
24

PREPARATION
FEW GOLDEN RULES
• Designed procedure room—block room• Insert an intravenous lin e before • Monitor (pulse oximetry,EG G , BP • Practice proper aseptic technique .• Resuscitation equipments at hand • Patients informed consent• Adequate knowledge of the correct
tehnique an d know how to handle complications
25

PREMEDICATION
Anxiolysis with Benzodiazipines and/or opiods
Light sedation----elicitation of paresthesia technique
Deep sedation----nerve stimulator
O2 supplementation----heavy sedation
26

EQUIPMENTS
Nerve stimulator—ECG Electrode• different lengths ( 25- 150 mm)and (20 to 25G).• tip may angled at 15 or 30 degrees.• catheters
Unipolar inculated B-Bevel needles
Ultransound machine
Syringes
Local anaesthetic
27

BLOCK ROOM28

EQUIPMENTS FOR PNB
29

30 Screnecurrent & frequency
CurrentDuration
frequency
DIAL
ANODE
CATHODE

NERVE STIMULATOR
31
Cathode-connectected with needle
Anode to patientThrough ECG
electrode

NERVE STIMULATOR
Current range from 0.1-6.0 mA
• Linear & constant• Low output
Pulse Frequency
• 1 Hz -Mixed nerve• 2 Hz - Sensory nerve
32

WHAT IS HZ ?
33
Cycles/second

STIMULATION AND INJECTION
TECNIQUEInitial current
2-3 mAFrequency
1-2 Hz
Threshold current 0.3- 0.5 mA
Aspirate– inj LA 1-2 ml----no pain &
resistance
Aspiration test 5- 10 ml LA injected
slowly
Increase the current to initial
level
No stimulatory response -inject the remaining
drug
Recurring response - May
indicate intraneural needle
position
34

USING NERVE STIMULATOR
35

UNIPOLAR B-BEVEL NEEDLES
less-experienced practitioners, the shortest recommended needle is generally safest
longer needle (up to 5 cm) may also be indicated in morbidly obese or very muscular patients.
approach and the patient population--e.g., adult vs. pediatric,
36
25-150 mm20-25G

INSULATED B-BEVEL NEEDLE
37

TOUHY SET FOR CATHETERIZATION
38

TOUHAY SET FOR PERIPHERAL NERVE CATHETERIZATION
39
Stimulating catheter

CURRENT ADJUSTABLE INSULATED NEEDLE SET
40

41

CONTINUOUS PNB SYSTEM
42

43
ELASTOMERIC BALOON PUMP

MEDIAN NERVE CATHETER
44
postoperative pain relief after hand surgery. Continuous infusion of levo-bupivacaine 0,125% - 2-5 ml/h

ULTRASOUND MACHINE
45

46
LAPTOP U
LTRASOU
ND
MACH
INE

Direct visualization of nerves & other structures
Visualization of LA spread
Re-position of needle in case of misdistribution of LA
Avoidance of side effect- due to excess dose of LA
ADVANTAGES OF USG
47

Avoidance of painful muscle contractions due to PNS
Faster onset
Longer duration of blocks
Improved quality
Blocks under GA
48

Short Axis (SAX) –
• probe is aligned perpendicular to the axis of the nerve, the nerve is seen in cross section
Long Axis (LAX) –
• probe is aligned parallel to the axis of the nerve
Short Axis View is preferred due to easy identification of nerves, more stable view & allows to visualise circumferential spread of LA------ “Doughnut” sign
BASIC VIEWS ON USG49

Ultrasound scanned image obtained in the infragluteal fossa midway between the greater trochanter and ischial tuberosity with the probe oriented along the long axis of the sciatic nerve. The sciatic nerve is
seen as a long tubular structure located deep to the muscles
50

51
Ultrasound scanned image of the femoral nerve surrounded byHypoechoic (dark) local anesthetic (L) creating a “doughnut” sign
Doughnutsign

In plane (IP) – long axis of the needle is oriented to the long axis of the probe
• Entire needle can be seen
Out of plane (OP) – the long axis of the needle is the oriented perpendicular to long axis of the probe
• Only part of the needle is seen
Contd…NEEDLE APPROACHES
52

53

54

55
Schematic representation of the views and needle approaches for nerve blocks with ultrasound imaging. A. Short axis view of a nerve with an out-of-plane needle approach. B. Short axis view of a nerve with an in-plane needle approach. C. Long axis view of a nerve with an out-of-plane needle approach. D. Long axis view of a nerve with
an in-plane needle approach. Modified6.

56
Picture showing the orientation of the ultrasound probe and the needle for placement of an interscalene block with
the in-plane needle approach
VIEW SHORT /LONG ?

TECHNIQUES
Single injection
• Intermittent dose• Continuous
Multiple injections---axillary block
• Large vol of LA in general location of cutaneous N• Minor/superficial surgery• Supplement to PNB & Neuraxial blocks
Using catheters
Field block---superficial cervical plexus block
57

FEMORAL NERVE CATHETERIZATION
58

CHOICE OF LOCAL
ANAESTHETICSPurpose of block
• Anaesthesia or analgesia
Onset
Duration of block
Site & area of block—vol
Degree of sensory Vs motor block
Maximum toxic dose
59

LA USED FOR PNB60

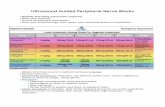
CONCENTRATION
ANAESTHESTHETIC BLOCK
• 1.5-2% Plain Lignocaine----------max 3 mg / kg • 1.5-2% Lignocaine with adrenaline--- 7mg / kg • 0.5% Bupivacaine---------max 2 mg / kg• Mepivacaine 2%• o.75 % Ropivacaine-------max 2-3 mg / kg
ANALGESIC BLOCK
• 0.125% Bupivacaine, 0.2% Ropivacaine, • Opiods, Clonidine.
61

PNB PLACEMENT TECHNIQUES
Anatomy
Evoked paresthesia
Nerve stimulator (goal 0.2-0.5 mA)
Ultrasound guided
Percutaneous electrical guidance
12
3
4
5
6
62
OTHERS1.Droppler2.CT3.MRI
LA-- in Perineural
area

CONCLUSION
Not as a first case
Centralize your equipment
Select proper block
Good knowledge of anatomy
Know about potential complications on treatment
63

Select right patient
Pick the right surgeon
Be confident about your block
But still if you fail--Failures are the stepping stones for success
64

QUESTION 1
Anaesthetist was performing a peripheral nerve block with help of neve stimulator & ultrasound ……he introduces insulated short bevel 22G needle at location…….& observe muscle contractions in nerve related area at 0.3 mA(n=0.2-o.5 mA).after injecting 1ml of LA muscle cotractions disappear.He injects rest of 10ml sol in incremental doses.Surgeon strat surgery after5 minutes but Pt feels pain……..Anaesthetist is quite sure about block……WHY Pt. feels pain ??
65

QUESTIOIN 2
Anaesthetist introduced linsulated long bevel needle to block a peripheral nerve & observes muscle contractions at 0.2 mA ……….while he injected 1ml of LA ,……he had to stop the injection due to severe pain………moreover muscle contraction did not disappeared ..
• WHY SEVERE PAIN ON INJECTION…?• WHY MUSCLE CONTRACTIONS DID NOT DISAPPEAR ON INJECTING
LA….?• WHAT SHOULD BE THE ACTION OF ANAESTHETIST NOW…?
66

THANKS
67