
Peripheral CTA Imaging
57
PERIPHERAL CTA Richard L. Hallett, MD Chief, Cardiovascular Imaging Northwest Radiology Network Indianapolis, IN Adjunct Assistant Professor – Imaging Cardiovascular Imaging Section Stanford University Stanford, CA RC 312B 29 November 2016 0830 – 1000
-
Upload
sam-watermeier -
Category
Health & Medicine
-
view
189 -
download
0
Transcript of Peripheral CTA Imaging
PERIPHERALCTA
RichardL.Hallett,MDChief,CardiovascularImagingNorthwestRadiologyNetworkIndianapolis,INAdjunctAssistantProfessor–ImagingCardiovascularImagingSectionStanfordUniversityStanford,CA
RC312B 29November2016 0830–1000
Outline§ GoalsofLECTA§ CTAAcquisitionTechniques
ú ScanAcquisitionú ContrastMediuminjection
ú Reconstruction
§ ClinicalEfficacyinPAD
Handout:stanford.edu/~hallettchoosefolder“RSNA2016”
@CTterrific
GoalsofCTAimaginginPAD
Indications (n) (2001-05)
DSA
DiagnosisandStagingofPAD
=symptoms+ABI
poorcorrelationofsymptomsandABIwith
number,locationandseverityoflesions
Example:calfclaudicationcanbecausedby
isolateddiseaseorcombinationofiliacand/or
femoropopliteallesions
Indications (n) (2001-05)
DSA
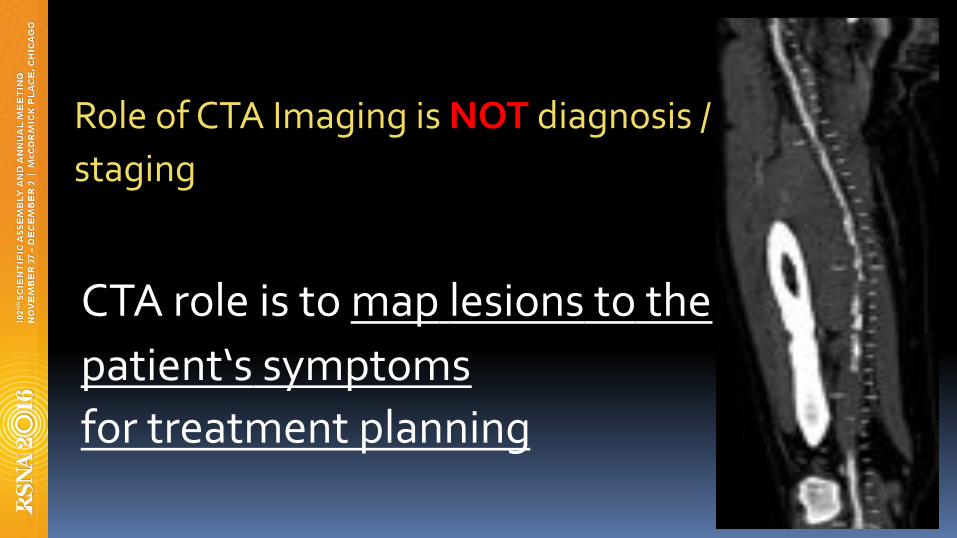
RoleofCTAImagingisNOTdiagnosis/
staging
CTAroleistomaplesionstothe
patient‘ssymptoms
fortreatmentplanning
GoalofReportingLECTA§ Answertheclinicalquestions
ú NEEDtogethistory
ú IntermittentClaudicationvsCriticalLimbIschemia?
§ Organizebyleg:ú Aorto-iliac(inflow)
ú Femoropopliteal
ú BelowKneerunoff
ú Pedalvessels(2crossankle)
IndicationsforCTAinPAD• IntermittentClaudication
• CriticalLimbIschemia
• AcuteIschemia(urgent)
• MonitoringofTherapy(complications)
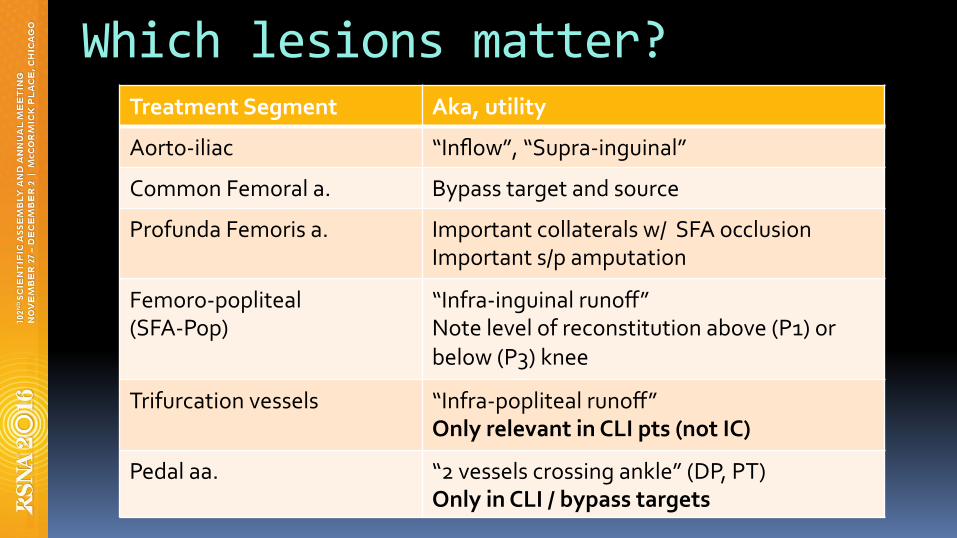
Whichlesionsmatter?TreatmentSegment Aka,utility
Aorto-iliac “Inflow”,“Supra-inguinal”
CommonFemorala. Bypasstargetandsource
ProfundaFemorisa. Importantcollateralsw/SFAocclusionImportants/pamputation
Femoro-popliteal(SFA-Pop)
“Infra-inguinalrunoff”Notelevelofreconstitutionabove(P1)or
below(P3)knee
Trifurcationvessels “Infra-poplitealrunoff”OnlyrelevantinCLIpts(notIC)
Pedalaa. “2vesselscrossingankle”(DP,PT)OnlyinCLI/bypasstargets

CTAScanAcquisition
Handout:stanford.edu/~hallettchoosefolder“RSNA2016”
@CTterrific
• ScanAcquisition• ContrastMediumInjection
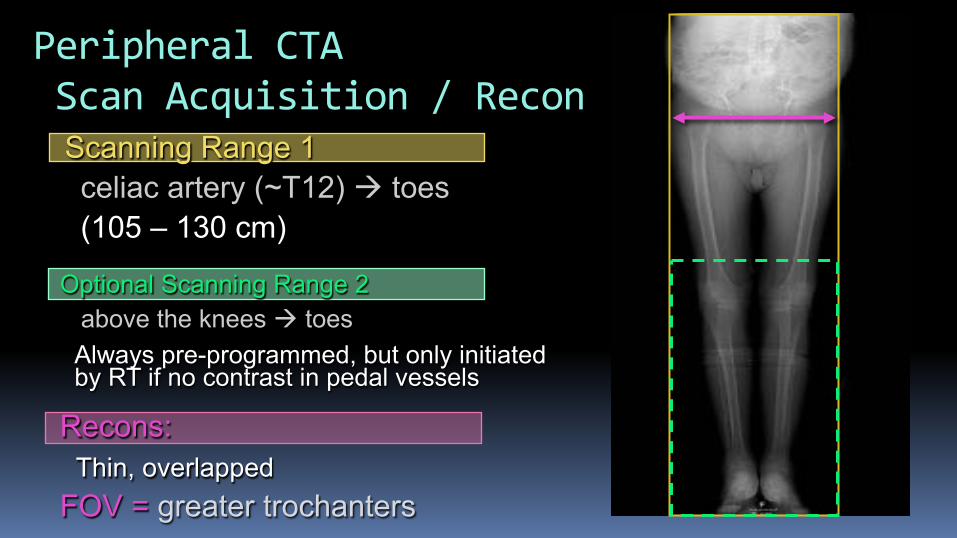
Optional Scanning Range 2 above the knees à toes Always pre-programmed, but only initiated by RT if no contrast in pedal vessels
Scanning Range 1 celiac artery (~T12) à toes (105 – 130 cm)
Recons: Thin, overlapped FOV = greater trochanters
PeripheralCTAScanAcquisition/Recon
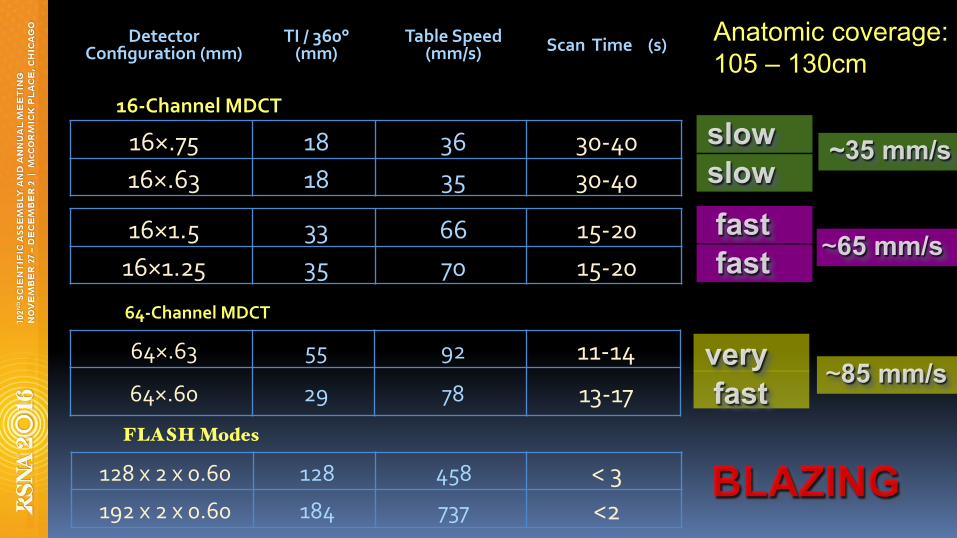
DetectorConfiguration(mm)
TI/360°(mm)
TableSpeed(mm/s) ScanTime(s)
16-ChannelMDCT
16×.75 18 36 30-40
16×.63 18 35 30-40
16×1.5 33 66 15-20
16×1.25 35 70 15-20
~35 mm/s slow slow
fast fast
Anatomic coverage: 105 – 130cm
64-ChannelMDCT
64×.63 55 92 11-14
64×.60 29 78 13-17 fast very
~85 mm/s
~65 mm/s
FLASH Modes
128x2x0.60 128 458 <3
192x2x0.60 184 737 <2 BLAZING
Speedconsiderationsfor>64sliceCTA
§ OutrunningBolus
§ Delayedfillingofdistalarteries
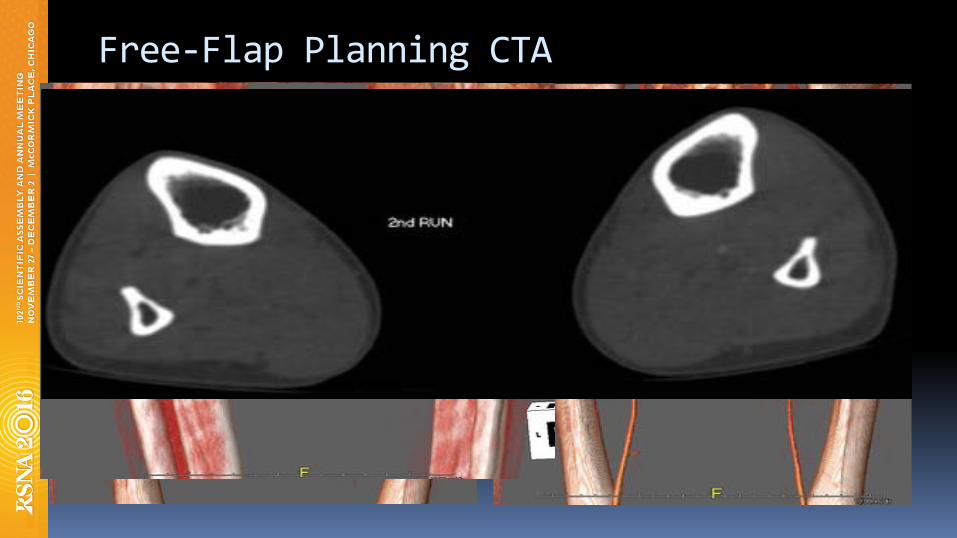
Free-FlapPlanningCTA

preprogrammed, optional 2nd acquisition
Arteriomegaly
1st acquisition
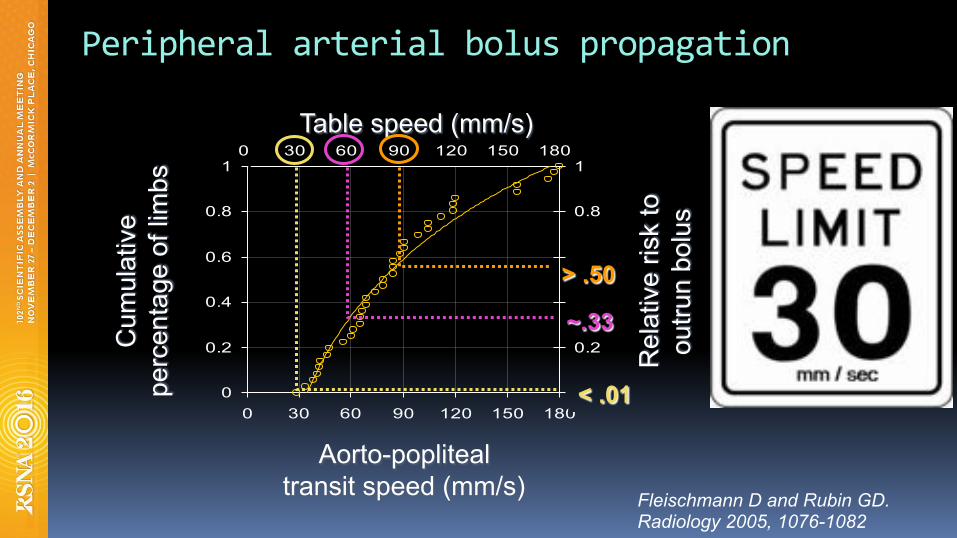
Table speed (mm/s)
0
0.2
0.4
0.6
0.8
1
0 30 60 90 120 150 180
vAO->POP (mm/s)
Cumu
lative
Pr
opor
tion o
f Lim
bs
0
0.2
0.4
0.6
0.8
1
Relat
ive R
isk to
Ou
trun B
olus
Cum
ulat
ive
pe
rcen
tage
of l
imbs
Table speed (mm/s)
Rel
ativ
e ris
k to
ou
trun
bolu
s
Aorto-popliteal transit speed (mm/s)
Table speed (mm/s)
0
0.2
0.4
0.6
0.8
1
0 30 60 90 120 150 180
vAO->POP (mm/s)Cu
mulat
ive
Prop
ortio
n of L
imbs
0
0.2
0.4
0.6
0.8
1
Relat
ive R
isk to
Ou
trun B
olus
Peripheralarterialboluspropagation
< .01
~.33
> .50
Fleischmann D and Rubin GD. Radiology 2005, 1076-1082
ContrastAdministrationforperipheralCTA
Fleischmann D. How to design injection protocols for multiple detector-row CT angiography (MDCTA). Eur Radiol. 2005 Dec 1;15 Suppl 5:E60–5.
ContrastconsiderationsforperipheralCTA
§ Aorto-poplitealtransittime:4-24sec(10sec)
ú Contrastspeed:29-177mm/s
§ Biphasicinjectionsyieldmoreconsistent
enhancementprofile
Fleischmann et al. JVIR 2006, 17(1) 3-26.
0
100
200
300
400
0 8 16 24 32 40 48 56 64 72 80
0
2
4
6
8
1 9 17 25 33
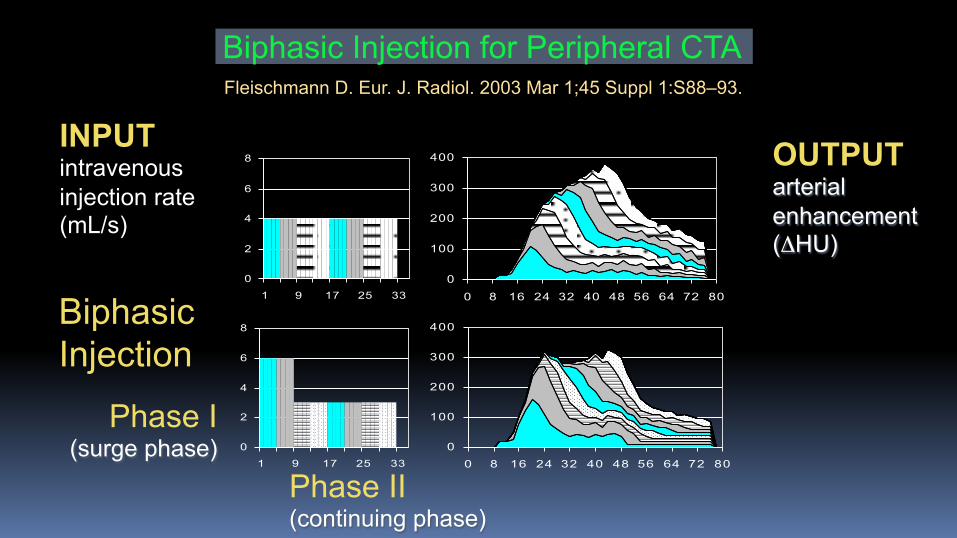
INPUT intravenous injection rate (mL/s)
OUTPUT arterial enhancement (ΔHU)
Phase I (surge phase)
Phase II (continuing phase)
Biphasic Injection for Peripheral CTA
0
100
200
300
400
0 8 16 24 32 40 48 56 64 72 80
0
100
200
300
400
0 8 16 24 32 40 48 56 64 72 80
0
100
200
300
400
0 8 16 24 32 40 48 56 64 72 80
0
2
4
6
8
1 9 17 25 33
0
2
4
6
8
1 9 17 25 33
0
2
4
6
8
1 9 17 25 33
Biphasic Injection
Fleischmann D. Eur. J. Radiol. 2003 Mar 1;45 Suppl 1:S88–93.
PatientFactors
§ Arterialenhancementisinverselyrelatedto:§ Cardiacoutput(CO)
§ Centralbloodvolume(CBV)
§ CO(andCBV)correlatewithbodyweight
§ atleastinpts.with~normalcardiacfunction
§ Weight-baseddosinghelpsconsistency
1) Hittmair & Fleischmann, JCAT 2001
usually unknown
IntegratedContrast/ScanProtocolSimple,weightbasedinjectionvolumesandflowrates,combinedwithafixedscantimeorscantime/diagnosticdelaysum.
automatedbolustriggering
Usephysiology(notscannerspeed)BENEFITS:
DecreasepatienttopatientvariabilityinscanqualityOptimizeimagingtimingImageallofthecontrastgiven!
(Potentially)savecontrast
STANFORDIntegratedScanning-InjectionProtocol:(Siemens)
§ Scantime: 40sforALLpatients(pitchvariable)§ Inj.duration:35sforALLpatients§ Delay: bolustriggering
weight Biphasic Injection <55kg 20 mL (4.0mL/s) + 96 mL (3.2mL/s) <65kg 23 mL (4.5mL/s) + 108 mL (3.6mL/s)
75kg 25 mL (5.0mL/s) + 120 mL (4.0mL/s) >85kg 28 mL (5.5mL/s) + 132 mL (4.4mL/s) >95kg 30 mL (6.0mL/s) + 144 mL (4.8mL/s)
ST.VINCENTIntegratedScanning-InjectionProtocol:(GEHD-750,VCT)
§ Scantime: Variable(can’tspecifytime)
§ Add�diagnosticdelay�tomake40sec§ Inj.duration:35sforALLpatients§ Delay: bolustriggering
weight Biphasic Injection <55 kg 20 mL (4.0mL/s) + 96 mL (3.2mL/s)
55-95 kg 25 mL (5.0mL/s) + 120 mL (4.0mL/s) >95 kg 30 mL (6.0mL/s) + 144 mL (4.8mL/s)

SpecialScenarios§ RenalDysfunction§ ContrastMediumSavings
AdaptationsforRenalDysfunction:LESSISMORE
§ DecreaseCMdose
§ DecreasekVimaging
§ Decreasescanrange
Background:§ ThereisclinicalevidencethatratioofCMto
eGFRcanpredictCINoccurrence
§ Bestdiscriminator:CMdose(mL)>3.7xeGFR
ú Correspondsto1xeGFRingramsofiodine(assuming
370mgI/mLcontrast)
§ ThereisalsoevidencethatCINriskisnotincreasedforvolumeslessthan2.0mLxeGFR
(PCIdata)Gurm HS, et al. J Am Coll Cardiol 2011; 58:907-14
eGFR-basedCMcalculation§ DetermineeGFR:http://touchcalc.com/e_gfr
§ IfeGFR<60ml/min/m2(e.g.CKD):
MAXvolume(mL)=eGFRx2
(thisisfor75kgbodyweight)
Then,adjustforBW:
MAXvolume=eGFRx2x(BW/75)
** Low concentration CM (300 mgI-/mL)
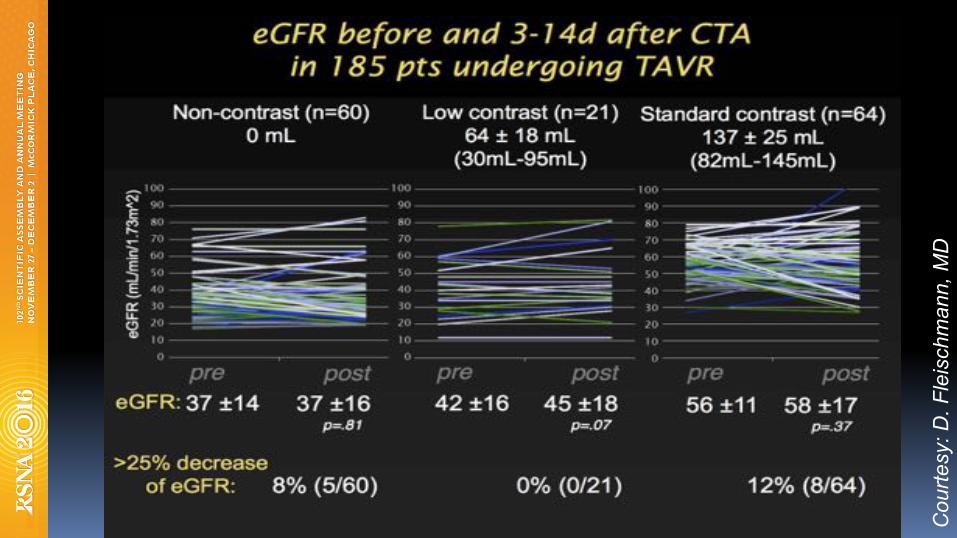
Cou
rtesy
: D. F
leis
chm
ann,
MD
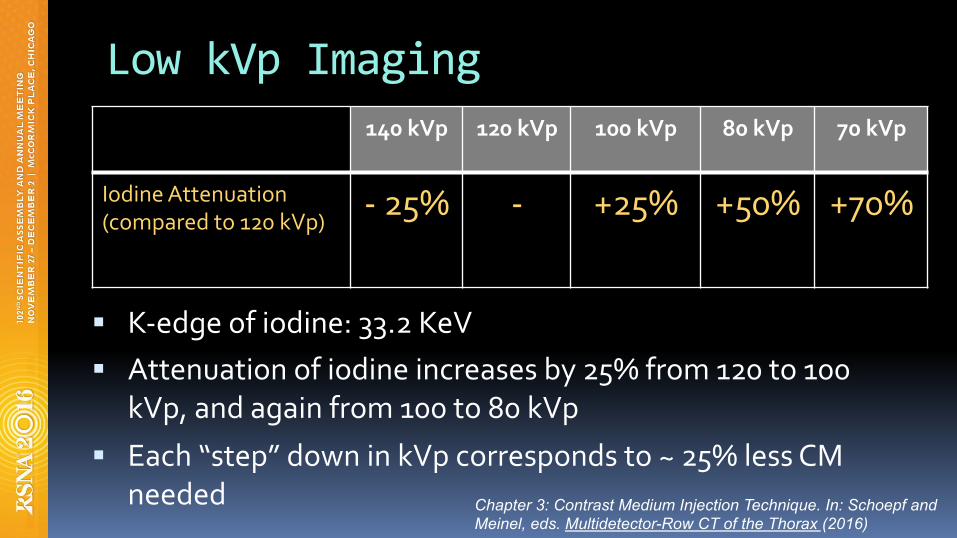
LowkVpImaging
§ K-edgeofiodine:33.2KeV§ Attenuationofiodineincreasesby25%from120to100
kVp,andagainfrom100to80kVp
§ Each“step”downinkVpcorrespondsto~25%lessCM
needed
140kVp 120kVp 100kVp 80kVp 70kVp
IodineAttenuation(comparedto120kVp)
-25% - +25% +50% +70%
Chapter 3: Contrast Medium Injection Technique. In: Schoepf and Meinel, eds. Multidetector-Row CT of the Thorax (2016)
LowkVpimaging-modifications
§ Keepinjectionduration,scan-time,andscandelaysconstant
§ Foreach“step”downinkVp,increasemAs30-50%
§ NoiseControloptions:ú Slowpitchdown
ú Slowgantryrotationtime
ú Keepnoiseindexthesame
ú MatchCTDIvolbetweenprotocols
OtherissuesinlowkVpimaging
§ Ca++blooming/metalbeamhardeningworsens
§ Largerfocalspotrequirementdecreasesspatialresolution(focalspotbloom)
ú Improvedwnewerscannertechnology

CTAReconstruction
Handout:stanford.edu/~hallettchoosefolder“RSNA2016”
@CTterrific
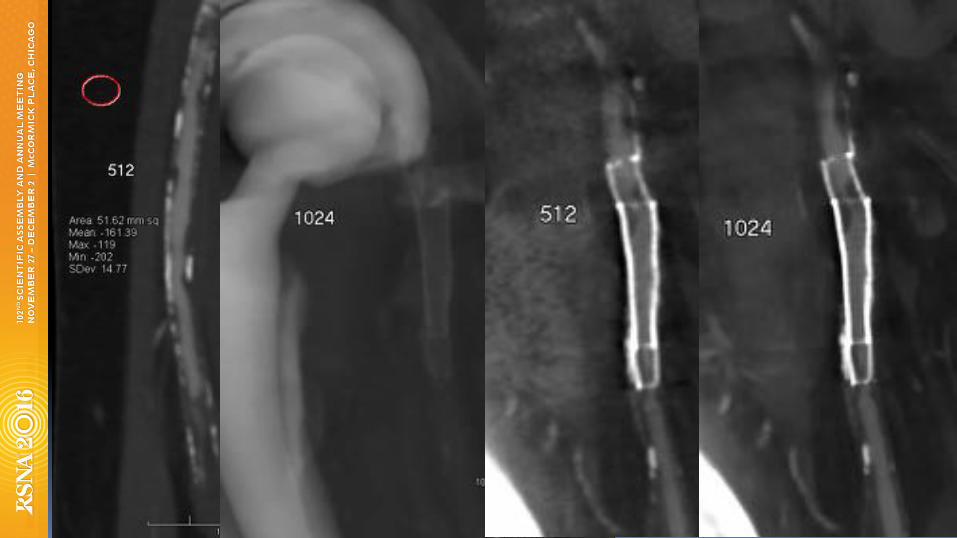
Tips:CTAReconstructionandInterpretation
§ UsesmallerFOV(trochantertotrochanter)
§ UseIterativeReconstruction§ Reconthin,overlappingimagesandreviewin3D
ú VR/MIPoverviewthenMPR,CPR
ú 3-5mmAxialsinA/P
§ Reconlargermatrix–1024x1024
** Fleischmann D, Hallett RL, Rubin GR. JVIR 2006, 17: 3-26.
CTAPost-processingTips§ BigchallengeinlowerextremityCTA:
differencebetweenquickreadvs.painful(literally)scrollingthroughimages
§ axial(transverse)imagesinadequate,exceptinacuteischemia(i.e.thromboembolic)
§ Volumetricreviewofvolumetricdatasets!
CTAPost-processingTips§ needlongitudinalcrosssections(MPR/CPR)
§ Maplesionswitha‘map’:
ú multipathcurvedplanarreformations(MPCPR)
ú CPRsmadeon3DSolution
§ trytodelegate(3D-Lab,trainedtechnologist)ifroutinelyperformingrunoffCTAs
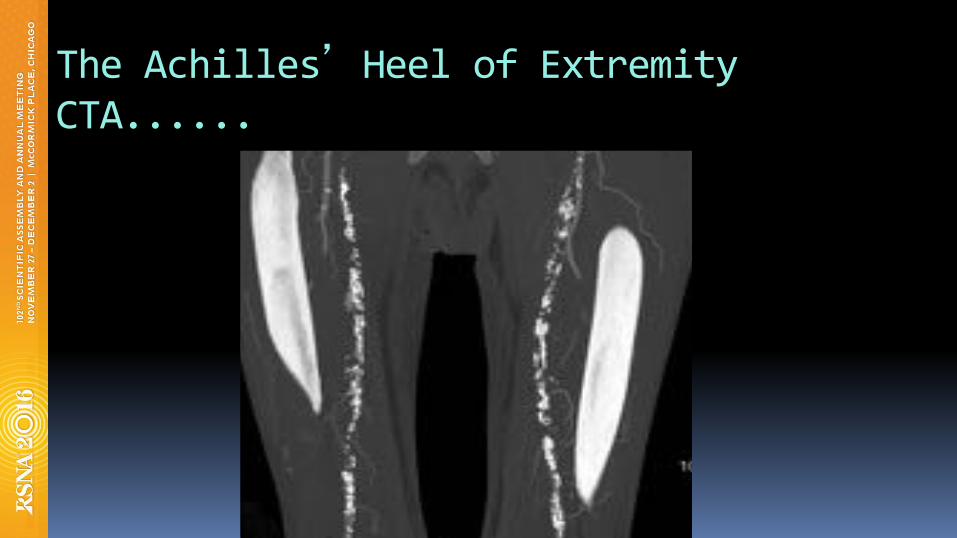
TheAchilles�HeelofExtremityCTA......
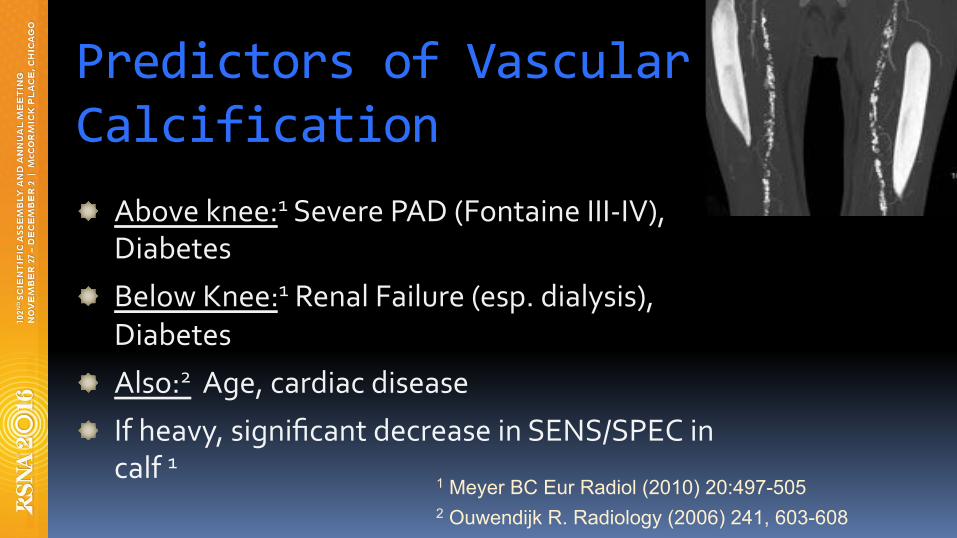
PredictorsofVascularCalcification
Aboveknee:1SeverePAD(FontaineIII-IV),Diabetes
BelowKnee:1RenalFailure(esp.dialysis),
Diabetes
Also:2Age,cardiacdisease
Ifheavy,significantdecreaseinSENS/SPECincalf1
1 Meyer BC Eur Radiol (2010) 20:497-505 2 Ouwendijk R. Radiology (2006) 241, 603-608
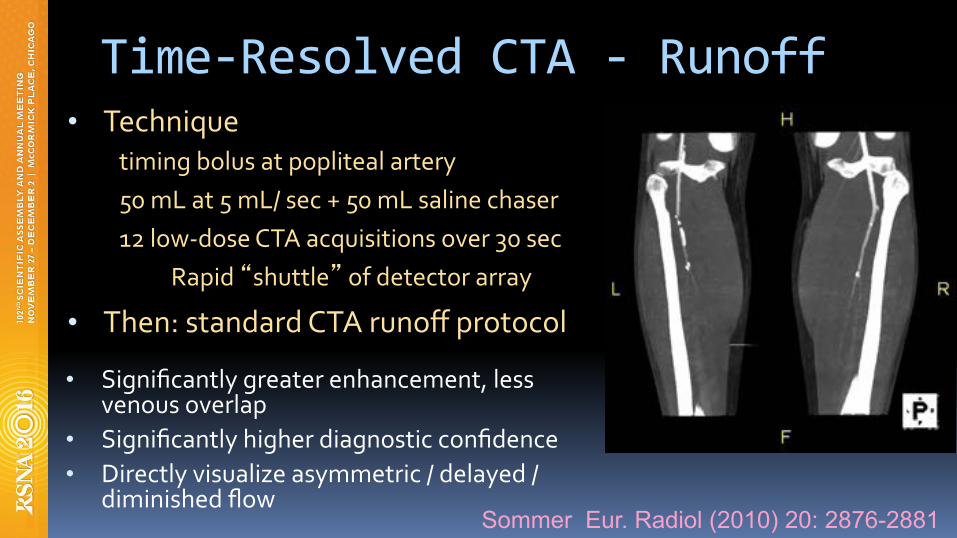
Time-ResolvedCTA-Runoff• Technique
timingbolusatpoplitealartery
50mLat5mL/sec+50mLsalinechaser
12low-doseCTAacquisitionsover30sec
Rapid�shuttle�ofdetectorarray
• Then:standardCTArunoffprotocol
• Significantlygreaterenhancement,lessvenousoverlap
• Significantlyhigherdiagnosticconfidence
• Directlyvisualizeasymmetric/delayed/diminishedflow
Sommer Eur. Radiol (2010) 20: 2876-2881
EfficacyofLECTAinPAD
Handout:stanford.edu/~hallettchoosefolder“RSNA2016”
@CTterrific
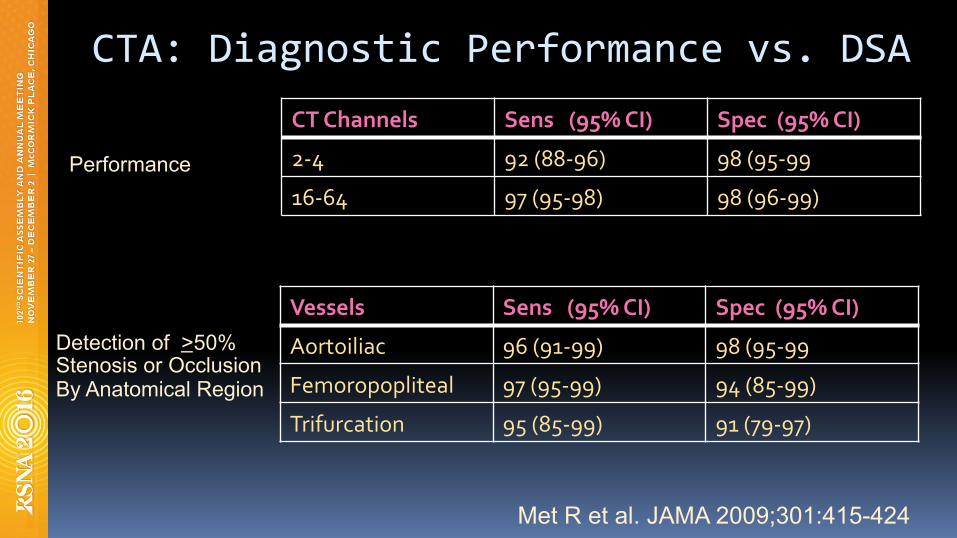
Detection of >50% Stenosis or Occlusion By Anatomical Region
Vessels Sens(95%CI) Spec(95%CI)
Aortoiliac 96(91-99) 98(95-99
Femoropopliteal 97(95-99) 94(85-99)
Trifurcation 95(85-99) 91(79-97)
CTA:DiagnosticPerformancevs.DSACTChannels Sens(95%CI) Spec(95%CI)
2-4 92(88-96) 98(95-99
16-64 97(95-98) 98(96-99)
Performance
Met R et al. JAMA 2009;301:415-424
DiagnosticPerformance:64-sliceCTA
§ SymptomaticPAD:242pts,7420segments
§ CTAandDSAperformed
§ For>70%stenosis:
ú SENS/SPEC96%PPV98%NPV99%
ú NosigdifferencevsDSAfindings
ú ResultssimilarinCa++vs.Non-Ca++lesions
Napoli A. Radiology. 2011 Dec 1;261(3):976–86.
ClinicalUtilityofLECTAinPAD
§ IntermittentClaudication(IC)
§ CriticalLimbIschemia(CLI)
Handout:stanford.edu/~hallettchoosefolder“RSNA2015”
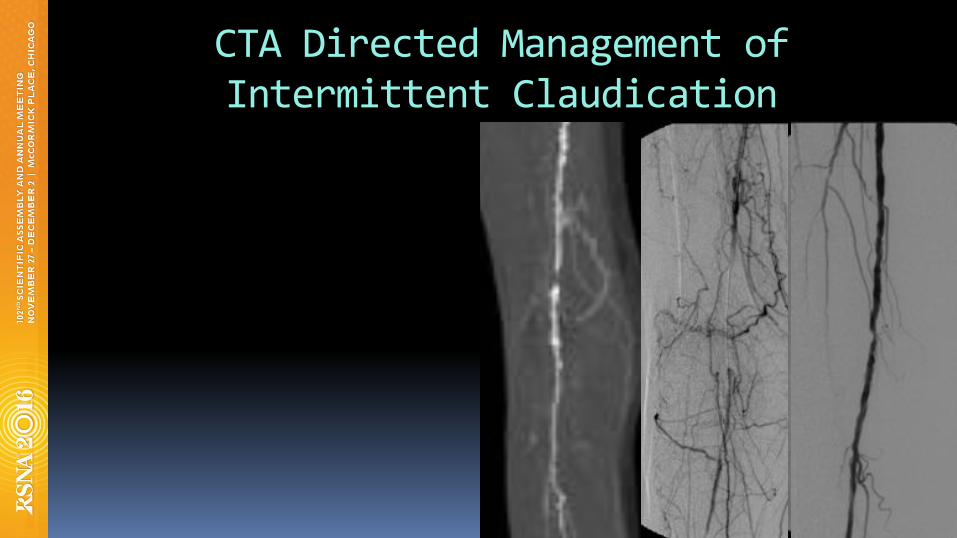
CTADirectedManagementofIntermittentClaudication
§ FontaineIIbpatients,TxdecisionsbyTASCIIcriteria
§ 57/58correctTxdecision-makingbyCTA
ú OneCFAstenosismissed
ú 29endovasc/surgTxú 29conservativemgmt
Schernthaner R, et al. AJR 2007; 189:1215-1222
CTADirectedManagementofIntermittentClaudication
CTADirectedManagementofCLI
§ 41pts,1435segments§ 64-CTA§ FontaineIIb,III,IV§ 2.2%segmentsnon-diagnostic
ú notincludedincalculationú 91%infrapopsegmentsevaluable
§ For>50%stenosis:ú Sens99% Spec98% Acc:98%
Fotiadis N, et al. Clinical Radiology 2011; 66: 945-52
CTADirectedManagementofCLI
§ 28pts,FontaineIV§ 64-detectorCTA§ 14/28àendovascularand/orsurg.Tx
§ correctdecision-makingforinterventions,amputation,andmedicalTxbasedonDSA
andTxresponse
Schernthaner R, et al. AJR 2009; 192: 1416-1424
CTADirectedManagementofCLI
ManagementofbothICandCLIbyCTA
§ TreatedusingTASCIIguidelinesú 49conservativeTXú 87Endovascularú 38surgeryú 17hybrid
§ TxrecommendationsfromCTAsameasDSA
inallbutONE
Napoli A. Radiology. 2011 Dec 1;261(3):976–86.
Examples:AtheroscleroticDisease-TherapyPlanning
CTAforpost-treatmentfollowup
Willmann JK, et al. Radiology 2003; 229: 465-474.
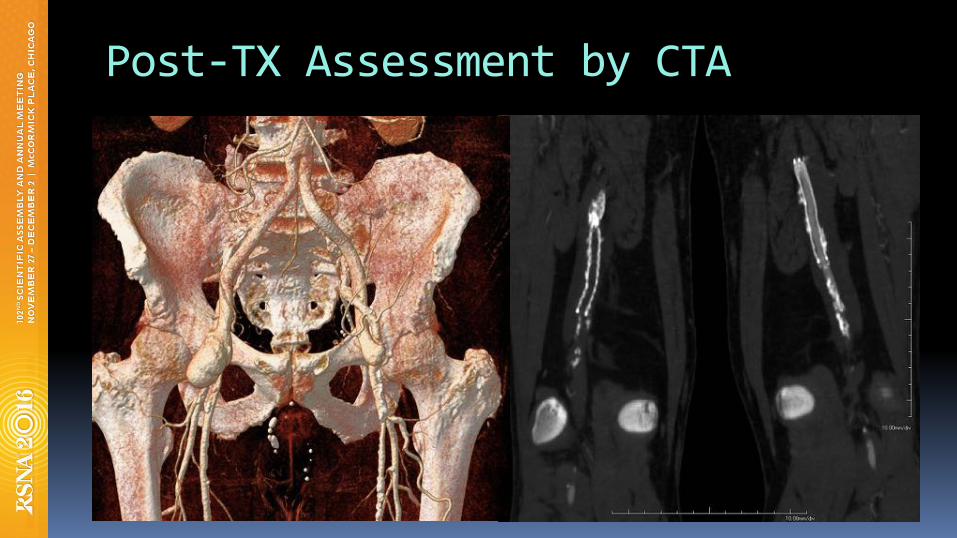
Post-TXAssessmentbyCTA
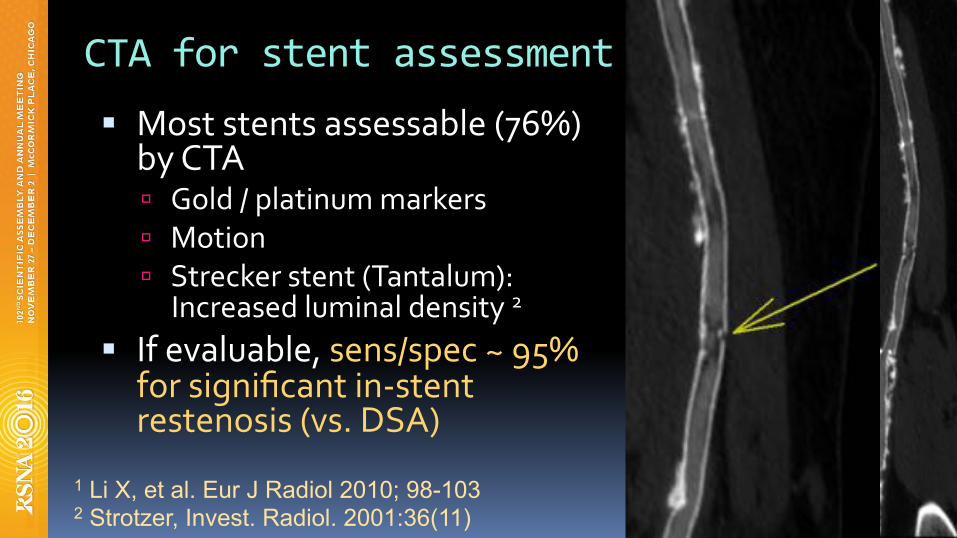
CTAforstentassessment§ Moststentsassessable(76%)
byCTAú Gold/platinummarkers
ú Motion
ú Streckerstent(Tantalum):Increasedluminaldensity2
§ Ifevaluable,sens/spec~95%forsignificantin-stentrestenosis(vs.DSA)
1 Li X, et al. Eur J Radiol 2010; 98-103 2 Strotzer, Invest. Radiol. 2001:36(11)
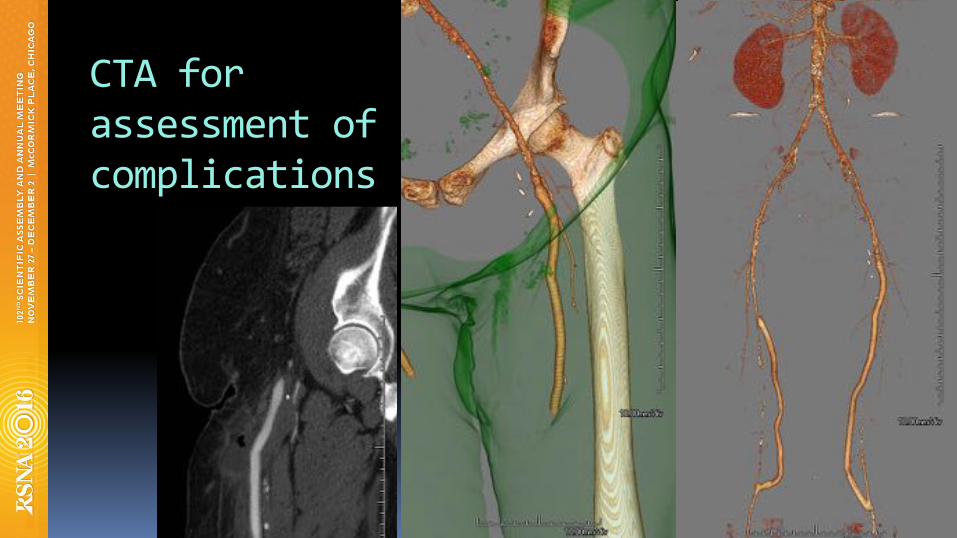
CTAforassessmentofcomplications

AcuteRlegpain
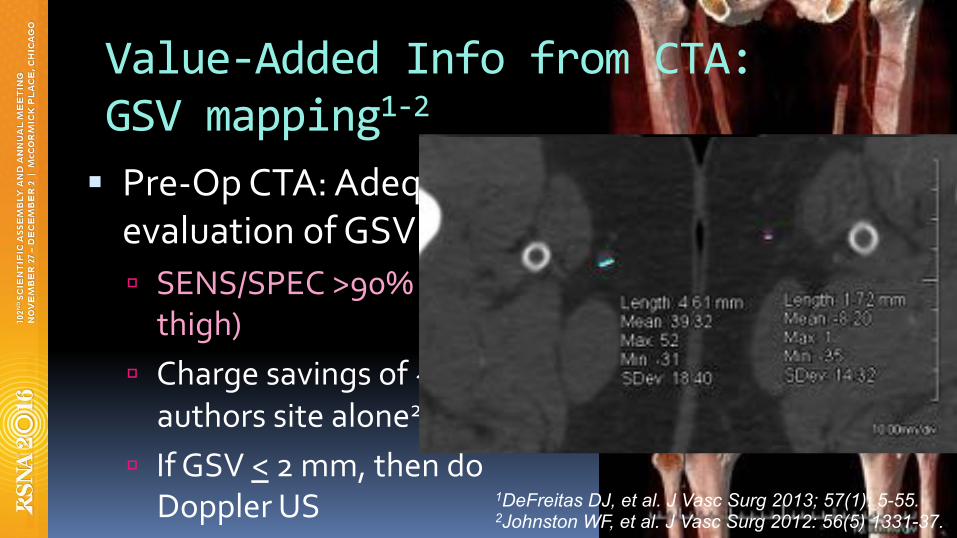
Value-AddedInfofromCTA:GSVmapping1-2§ Pre-OpCTA:AdequateforevaluationofGSVsize1-2
ú SENS/SPEC>90%(betterinthigh)
ú Chargesavingsof~50Katauthorssitealone2
ú IfGSV<2mm,thendoDopplerUS 1DeFreitas DJ, et al. J Vasc Surg 2013; 57(1): 5-55.
2Johnston WF, et al. J Vasc Surg 2012: 56(5) 1331-37.
Conclusions§ Goals: Maplesionstosymptomstodirecttherapy
Answertheclinicalquestions§ Implement:
IntegratedCM/scanprotocoltoimproveconsistency Injectlong,scanslow
Weight-basedCMdosing
§ 3DVolumetricReviewofDatasetsneeded
§ Specialthanksto…..
DominikFleischmann,MD
ThanksforyourAttention!
Handout:stanford.edu/~hallettchoosefolder“RSNA2016”
@CTterrific


















