Presents: Diaton Tonometer Tonometry through the Eyelid! September 2006.

Peripheral arterial tonometry with ascending aortic waveform
analysis using the SphygmoCor system
February/March 2006
Application 1079
Assessment report

© Commonwealth of Australia 2006
ISBN (Print) 1 74186 032 6
ISBN (Online) 1 74186 033 4
ISSN (Print) 1443-7120
ISSN (Online) 1443-7139
First printed November 2006
Paper-based publications
© Commonwealth of Australia 2006 This work is copyright. Apart from any use as permitted under the Copyright Act 1968, no part may be reproduced by any process without prior written permission from the Commonwealth. Requests and inquiries concerning reproduction and rights should be addressed to the Commonwealth Copyright Administration, Attorney General’s Department, Robert Garran Offices, National Circuit, Canberra ACT 2600 or posted at http://www.ag.gov.au/cca
Internet sites
© Commonwealth of Australia 2006 This work is copyright. You may download, display, print and reproduce this material in unaltered form only (retaining this notice) for your personal, non-commercial use or use within your organisation. Apart from any use as permitted under the Copyright Act 1968, all other rights are reserved. Requests and inquiries concerning reproduction and rights should be addressed to the Commonwealth Copyright Administration, Attorney General’s Department, Robert Garran Offices, National Circuit, Canberra ACT 2600 or posted at http://www.ag.gov.au/cca Electronic copies of the report can be obtained from the Medical Service Advisory Committee’s Internet site at http://www.msac.gov.au/
Printed copies of the report can be obtained from:
The Secretary Medical Services Advisory Committee Department of Health and Ageing Mail Drop 106 GPO Box 9848 Canberra ACT 2601
Enquiries about the content of the report should be directed to the above address.
The Medical Services Advisory Committee (MSAC) is an independent committee which has been established to provide advice to the Commonwealth Minister for Health and Ageing on the strength of evidence available on new and existing medical technologies and procedures in terms of their safety, effectiveness and cost-effectiveness. This advice will help to inform Government decisions about which medical services should attract funding under Medicare.
This report was prepared by the Medical Services Advisory Committee with the assistance of Dr Suzanne Dyer, Mr Marc Bevan and Ms Jolie Hutchinson from the Medical Technology Assessment Group (M-TAG) a unit of IMS Health. Ms Ann Jones of M-TAG edited the report. The Commonwealth Minister for Health and Ageing endorsed the report on 6 June 2006.
Publication approval number: 3890
SphygmoCor system iii
Contents
Executive summary................................................................................................. ix The procedure ................................................................................................................. ix Medical Services Advisory Committee – role and approach .................................... ix MSAC’s assessment of peripheral arterial tonometry with ascending aortic
waveform analysis using the SphygmoCor system ............................................... ix Clinical need ............................................................................................................... ix Safety ............................................................................................................................ x Effectiveness and diagnostic accuracy..................................................................... x Cost-effectiveness...................................................................................................... xi
Recommendation ............................................................................................................ xi Introduction ..............................................................................................................1 Background.............................................................................................................. 2
Peripheral arterial tonometry with ascending aortic waveform analysis using the SphygmoCor system.................................................................................. 2
Blood pressure.................................................................................................................. 2 Blood pressure measurement ......................................................................................... 3 Pressure waveform........................................................................................................... 4 SphygmoCor system........................................................................................................ 9
The procedure ............................................................................................................. 9 Intended purpose........................................................................................................ 9
The reference standard.................................................................................................. 10 Existing tests ................................................................................................................... 10
Blood pressure measurement.................................................................................. 10 Angiography .............................................................................................................. 11 Electrocardiography ................................................................................................. 11 Stress testing .............................................................................................................. 11 Cardiac perfusion scan............................................................................................. 11 Echocardiography..................................................................................................... 12 Arterial compliance measures ................................................................................. 12
Hypertension .................................................................................................................. 13 Clinical need .............................................................................................................. 13 Mortality and morbidity ........................................................................................... 13 Current treatment ..................................................................................................... 14
Angina pectoris............................................................................................................... 14 Clinical need .............................................................................................................. 14 Mortality and morbidity ........................................................................................... 14 Current treatment ..................................................................................................... 15
Heart failure .................................................................................................................... 15 Clinical need .............................................................................................................. 15 Mortality and morbidity ........................................................................................... 15 Current treatment ..................................................................................................... 16
Potential impact of the test........................................................................................... 16 Marketing status of the device ..................................................................................... 16

iv SphygmoCor system
Current reimbursement arrangement.......................................................................... 17
Approach to assessment .........................................................................................18 Research questions and clinical pathways................................................................... 18
Hypertension ............................................................................................................. 18 Angina pectoris ......................................................................................................... 22 Heart failure............................................................................................................... 24
Assessment framework ................................................................................................. 26 Types of evidence ..................................................................................................... 26
Review of the literature ................................................................................................. 26 Search strategy........................................................................................................... 26 Selection criteria........................................................................................................ 28 Search results ............................................................................................................. 30
Data extraction ............................................................................................................... 31 Statistical methods ......................................................................................................... 31
Methodological considerations ............................................................................... 31 Appraisal of the evidence.............................................................................................. 32
Appraisal of the quality and applicability of individual studies.......................... 32 Ranking the evidence ............................................................................................... 32
Interpretation of the evidence...................................................................................... 33 Expert advice .................................................................................................................. 34
Results of assessment ............................................................................................ 35 Is it safe? .......................................................................................................................... 35 Is it effective?.................................................................................................................. 35
Direct evidence ......................................................................................................... 35 Linked evidence ........................................................................................................ 35
Conclusions............................................................................................................ 40 Safety................................................................................................................................ 40 Effectiveness................................................................................................................... 40
Diagnostic accuracy.................................................................................................. 40 Impact on patient management .............................................................................. 40 Impact on health outcomes..................................................................................... 40
Cost-effectiveness .......................................................................................................... 41 Recommendation................................................................................................... 42 Appendix A MSAC terms of reference and membership ...................................... 43 Appendix B Advisory Panel ................................................................................... 45 Appendix C Quality criteria ................................................................................... 46 Appendix D Literature search strategies ............................................................... 48 Appendix E Spurious systolic hypertension of youth............................................ 50 Appendix F Included studies................................................................................. 60 Appendix G Supplementary study ......................................................................... 68 Abbreviations ......................................................................................................... 70 References ...............................................................................................................71
SphygmoCor system v
Tables
Table 1 Classification of blood pressure levels..................................................................... 2 Table 2 Diagnosis of cardiovascular diseases using the SphygmoCor system................. 9 Table 3 PPICO criteria for the use of the SphygmoCor system in hypertension ......... 18 Table 4 PPICO criteria for the use of the SphygmoCor system in angina
pectoris ..................................................................................................................... 22 Table 5 PPICO criteria for the use of the SphygmoCor system in heart failure........... 24 Table 6 Electronic databases searched for the SphygmoCor hypertension
review........................................................................................................................ 26 Table 7 Selection criteria for included studies for hypertension...................................... 28 Table 8 Selection criteria for included studies for angina pectoris .................................. 29 Table 9 Selection criteria for included studies for heart failure........................................ 29 Table 10 NHMRC levels of evidence for studies of effectiveness................................... 32 Table 11 NHMRC levels of evidence for diagnosis ........................................................... 33 Table 12 Grading system used to rank included studies .................................................... 33 Table 13 Characteristics of the included SphygmoCor study ........................................... 36 Table 14 Likelihood ratios for the presence of coronary artery disease for
different AIx values ................................................................................................ 37 Table 15 Diagnostic accuracy of AIx for the presence of coronary artery
disease, according to different thresholds ........................................................... 38 Table 16 Post-test probabilities of coronary artery disease based on test result
for different AIx thresholds .................................................................................. 39 Table 17 SphygmoCor system Medline search strategy
(1966 to August Week 1, 2005)............................................................................. 48 Table 18 SphygmoCor system EMBASE search strategy
(1980 to Week 33, 2005) ........................................................................................ 48 Table 19 SphygmoCor system PreMedline search strategy (17 August, 2005)............... 49 Table 20 SphygmoCor system Cochrane Library search strategy (Issue 3, 2005).......... 49 Table 21 Characteristics of the included study of the SphygmoCor system in
spurious systolic hypertension of youth .............................................................. 50 Table 22 Characteristics of male subjects with spurious systolic hypertension of
youth, normotension or essential hypertension ................................................. 50 Table 23 Characteristics of the included studies reporting the technical
validation of measures of spurious systolic hypertension of youth................. 52 Table 24 Comparison of accuracy of derived aortic and upper limb blood
pressure measurement using direct measurement of aortic blood pressure with a transducer-tipped catheter ......................................................... 56
vi SphygmoCor system
Table 25 Comparison of accuracy of derived aortic and upper limb blood
pressure measurement using direct measurement of aortic blood pressure with a fluid-filled catheter ...................................................................... 57
Table 26 Accuracy of estimation of aortic AIx from derived aortic or radial waveforms................................................................................................................ 59
Table 27 Characteristics of the included study of the SphygmoCor system in coronary artery disease ........................................................................................... 60
Table 28 Characteristics and results of the included studies comparing the measurement of derived aortic, radial and measured aortic BP....................... 62
Table 29 Characteristics and results of the included study of the SphygmoCor system in spurious systolic hypertension of youth............................................. 67
Table 30 Characteristics and results of the ENIGMA study of the SphygmoCor system in spurious systolic hypertension of youth............................................. 69
SphygmoCor system vii
Figures
Figure 1 Typical arterial pressure waveforms according to age.......................................... 4 Figure 2 Typical aortic pressure waveforms in normotensive subjects
according to age ........................................................................................................ 5 Figure 3 Determination of the augmentation index from the aortic pressure
waveform derived from a radial artery waveform using the SphygmoCor system................................................................................................. 7
Figure 4 Derived aortic pressure wave and pulse wave analysis parameters .................... 8 Figure 5 Clinical pathway for the investigation of patients referred with
hypertension (< 25 years of age) .......................................................................... 20 Figure 6 Clinical pathway for the investigation of patients referred with
hypertension who are uncontrolled by multiple medication (more than two drugs) or who are experiencing adverse effects of medication................................................................................................................ 21
Figure 7 Clinical pathway for the investigation of patients with stable angina .............. 23 Figure 8 Clinical pathway for the investigation of patients with heart failure................ 25 Figure 9 Summary of the process used to identify and select studies for the
review........................................................................................................................ 30 Figure 10 Receiver-operating characteristic (ROC) curve for diagnostic accuracy
of AIx for coronary artery disease........................................................................ 38


SphygmoCor system ix
Executive summary
The procedure
The SphygmoCor system is a non-invasive diagnostic technology that enables pulse wave analysis of the central, ascending aortic pressure wave.
The SphygmoCor system allows a peripheral arterial pressure waveform to be obtained by applying an arterial applanation tonometer to the wrist. The tonometer partially compresses the radial artery and records a pressure wave over several cardiac cycles. This pressure wave is calibrated to brachial cuff blood pressure measurements. The averaged peripheral waveform is then converted to an ascending aortic waveform using a generalised mathematical transfer function.
Medical Services Advisory Committee – role and approach
The Medical Services Advisory Committee (MSAC) is a key element of a measure taken by the Commonwealth to strengthen the role of evidence in health financing decisions in Australia. MSAC advises the Commonwealth Minister for Health and Ageing on the evidence relating to the safety, effectiveness and cost-effectiveness of new and existing medical technologies and procedures; and under what circumstances public funding should be supported.
A rigorous assessment of the available evidence is thus the basis of decision making when funding is sought under Medicare. A team from the Medical Technology Assessment Group (M-TAG), a unit of IMS, was engaged to conduct a systematic review of literature on peripheral arterial tonometry with ascending aortic waveform analysis using the SphygmoCor system. An Advisory Panel with expertise in this area then evaluated the evidence and provided advice to MSAC.
MSAC’s assessment of peripheral arterial tonometry with ascending aortic waveform analysis using the SphygmoCor system
Clinical need
Hypertension is a common disorder. An estimated 3 million Australians over 25 years old have high blood pressure. This condition is a major financial burden on the Australian health care system. Blood pressure-lowering drugs available through the Pharmaceutical Benefits Scheme (PBS) cost $755 million in 2000. This corresponds to 16.5 per cent of government and patient costs for prescription PBS drugs (Australian Institute of Health and Welfare 2004a).
In addition to its direct burden, hypertension is a major contributor to deaths due to all cardiovascular diseases. In 2002, cardiovascular disease was responsible for 38 per cent
x SphygmoCor system
of all deaths and 7 per cent of all hospitalisations (Australian Institute of Health and Welfare 2004a).
Coronary artery disease (CAD) was the largest single cause of death in the Australian population in 2002, and was responsible for 19.5 per cent of all deaths. The 2001 National Health Survey reported 1.9 per cent of the surveyed population (corresponding to approximately 355,600 Australians) experiencing some manifestation of CAD. The majority of these individuals reported having angina and approximately one-third reported experiencing a heart attack.
Heart failure was the third largest cause of death from cardiovascular diseases in the Australian population in 2002, and was responsible for 2 per cent of all deaths.
The estimated prevalence for heart failure in Australia is based on international data, approximately 300,000 Australians have chronic heart failure with a further 30,000 diagnosed each year.
Safety
The SphygmoCor system is a non-invasive test and there are no adverse events associated with its use.
Effectiveness and diagnostic accuracy
No studies providing evidence for the accuracy of the SphygmoCor system for the diagnosis of hypertension, white coat hypertension or spurious systolic hypertension of youth were identified. A more detailed analysis of the spurious systolic hypertension of youth data did not yield persuasive evidence to support the ability of the SphygmoCor system to accurately diagnose spurious systolic hypertension of youth.
One single study was identified that provided evidence for diagnostic accuracy of the SphygmoCor system for the diagnosis of CAD. On the basis of this evidence, the augmentation index (AIx) measure as determined by the SphygmoCor system was recognised as having limited value for the diagnosis of CAD.
No studies providing evidence for the diagnostic accuracy of the SphygmoCor system for the diagnosis of heart failure were identified.
Impact on patient management
No studies providing evidence for the effect of SphygmoCor system on patient management were identified.
Impact on health outcomes
There was no evidence of equivalent or improved diagnostic accuracy using the SphygmoCor system relative to using the comparators or of changes to patient management. Therefore, evidence for the effectiveness of treatment on health outcomes was not necessary for this assessment
SphygmoCor system xi
Cost-effectiveness
In the absence of evidence supporting the effectiveness of SphygmoCor, a cost-effectiveness analysis was not undertaken.
Recommendation
Since there is currently insufficient evidence pertaining to peripheral arterial tonometry with ascending aortic waveform analysis using the SphygmoCor system, MSAC recommended that public funding should not be supported at this time for this procedure.
– The Australian Government Minister for Health and Ageing accepted this recommendation on 6 June 2006. –


SphygmoCor system 1
Introduction
The Medical Services Advisory Committee (MSAC) has reviewed the use of peripheral arterial tonometry with ascending aortic waveform analysis using the SphygmoCor system, which is a diagnostic test for the assessment of hypertension, angina pectoris and heart failure. MSAC evaluates new and existing health technologies and procedures for which funding is sought under the Medicare Benefits Scheme in terms of their safety, effectiveness and cost-effectiveness, while taking into account other issues such as access and equity. MSAC adopts an evidence-based approach to its assessments, based on reviews of the scientific literature and other information sources, including clinical expertise.
MSAC’s terms of reference and membership are at Appendix A. MSAC is a multidisciplinary expert body, comprising members drawn from such disciplines as diagnostic imaging, pathology, surgery, internal medicine and general practice, clinical epidemiology, health economics, consumer health and health administration.
This report summarises the assessment of current evidence for the use of peripheral arterial tonometry with ascending aortic waveform analysis using the SphygmoCor system for hypertension, angina pectoris and heart failure.
2 SphygmoCor system
Background
Peripheral arterial tonometry with ascending aortic waveform analysis using the SphygmoCor system
Blood pressure
Blood pressure is the pressure that is exerted on the walls of the arteries due to the ejection of blood from the heart. The peak pressure during the cardiac cycle is the systolic blood pressure (SBP), and the minimum pressure is the diastolic blood pressure (DBP). The difference between the systolic and diastolic pressure is the pulse pressure (PP).
The widely accepted World Health Organization definition of hypertension (high blood pressure) is an SBP of ≥ 140 mmHg and/or a DBP ≥ 90 mmHg. However, it should be noted that the cut-offs defining hypertension are arbitrary. The National Heart Foundation of Australia recommends the arterial blood pressure classifications shown in Table 1.
Table 1 Classification of blood pressure levels
Category Systolic (mmHg) Diastolic (mmHg) Normal < 120 < 80 High-normal 120–139 80–89 Grade 1 (mild) 140–159 90–99 Grade 2 (moderate) 160–179 100–109 Grade 3 (severe) > 180 > 110 Isolated systolic hypertension > 140 < 90
Source: (Australian Heart Foundation 2004).
Hypertension is a significant risk factor for cardiovascular and kidney diseases, and is a major cause of premature death and permanent disability in Australia. The Australian Institute of Health and Welfare’s publication Heart, stroke and vascular diseases: Australian facts 2001 states that:
• high blood pressure is a major risk factor for coronary heart disease, stroke, heart failure and peripheral vascular disease
• high blood pressure increases cardiovascular risk by 2–3 times
• the risk of disease increases as the blood pressure level increases.
Detection and treatment of hypertension is therefore essential in the primary prevention of cardiovascular disease, including coronary artery disease (commonly presenting as angina) and heart failure. However, hypertension is an asymptomatic condition and many people remain undiagnosed and untreated. The National Heart Foundation of Australia (2004) recommends that patients with normal blood pressure be checked every two years. The frequency of assessment should be greater in the presence of hypertension or high-normal blood pressure. Similarly, more frequent assessment is appropriate when other cardiovascular risk factors are present.

SphygmoCor system 3
Blood pressure measurement
Hypertension is usually diagnosed by taking standard blood pressure measurements using a sphygmomanometer. This involves placing a cuff around the upper arm and inflating it to a pressure greater than the systolic pressure, which compresses the brachial artery. As the cuff is deflated, the blood flow through the compressed artery resumes. The sounds associated with the changes in blood flow which occur as the pressure in the cuff is decreased, are known as the Korotkoff sounds. The physician determines blood pressure by listening for the Korotkoff sounds with a stethoscope.
Automated cuff blood pressure measurement devices are also available. These work by one of two techniques. The auscultatory technique operates on the same principle as standard blood pressure measurement, using a microphone or ultrasound device to detect the Korotkoff sounds. The oscillometric technique detects blood pressure by measuring the oscillations of the arterial wall.
Non-invasive blood pressure measurement by these methods is the standard means of estimating systemic blood pressure. However, misleading or erroneous readings may occur in subjects with significant hardening of the brachial artery (pseudohypertension). In addition, individuals who become stressed during the performance of blood pressure measurement may have a temporary increase in blood pressure (‘white coat hypertension’).
Individuals with hypertension are often further assessed by 24-hour ambulatory blood pressure monitoring (ABPM). ABPM utilises a portable sphygmomanometer (with an attached recording device) to measure blood pressure repeatedly over a 24-hour period. A trained technician is required to set up the ABPM device, and the subject then goes about their usual daily activities. The sphygmomanometer inflates at predefined times, and the blood pressures are recorded on a data storage unit. After the monitoring period is complete, the blood pressure data are analysed to determine the patient’s mean 24-hour blood pressure, mean daytime blood pressure and mean night-time blood pressure readings. This approach provides information on the subject’s blood pressure in their normal environment and routine (Australian Heart Foundation 2004; Lefevre et al 2001).
The most accurate method of measuring blood pressure and pressure waveforms is by passing a catheter into an artery to obtain direct pressure measurement. There are two basic types of catheters used for invasive blood pressure measurement: fluid-filled catheters with an external manometer and catheter-tipped transducers. Fluid-filled catheters rely on the transmission of the pressure wave through the fluid in the catheter lumen. An external pressure transducer can then record the pressure wave. The transducer must be reliably calibrated and the baseline set at atmospheric pressure. Air bubbles within the fluid interface can produce errors in pressure recording. Catheter-tipped transducers have a miniature pressure transducer at the end of the catheter which can be positioned within the heart. These manometers generally have higher fidelity for recording pressure waves, with resonant frequencies into the kHz range (Nichols et al 2005).
Cardiac catheterisation is used in several diagnostic applications in a clinical setting. Injection of dye through a cardiac catheter can be used to measure cardiac output or image coronary artery blood flow (angiography).

4 SphygmoCor system
Pressure waveform
Due to the pulsatile nature of blood flow, arterial blood pressure has a characteristic waveform. The contour of this pressure wave varies throughout the body, as well as with increasing age and cardiovascular disease states (Figure 1). In normal individuals, the pulse pressure is greater in the brachial artery than the aorta. However, this increase in pulse pressure between the aorta and peripheral arteries declines with age, as the elasticity of the large arteries decreases (Nichols et al 2005). Therefore, measurement of blood pressure by standard sphygmomanometry is more useful for estimating central aortic blood pressure in older subjects than in younger individuals.
Figure 1 Typical arterial pressure waveforms according to age From: A Clinical Guide: Pulse Wave Analysis (2005). http://www.atcormedical.com/users_guide.html
The pressure wave at any location in the body is a composite of an outgoing and a reflected pressure wave. The first is the pressure wave that travels from the heart to the peripheral arteries, generated by contraction of the left ventricle. The second is a pressure wave reflected back from the periphery, due to the resistance provided by the small calibre distal vessels. In a healthy adolescent, this reflected wave meets the central aortic pressure wave during the diastolic period, and does not augment the central systolic pressure. The increase in the central pressure during diastole assists in perfusion of the heart muscle (myocardium). The systolic pressure in more peripheral vessels is, however, increased due to summation with the reflected wave. Thus, there are differences between peripheral and central blood pressure, and the former may not always reflect the latter.

SphygmoCor system 5
In older adults, and individuals with vascular diseases such as atherosclerosis, the arteries are usually less compliant. This arterial stiffening is primarily due to degeneration of the elastic components of the large arteries. As the compliance decreases, the cushioning effect of the arteries on the pulsatile components of the pressure wave decreases. This decreased compliance results in the pressure wave travelling along the arteries at an increased rate – that is, the pulse wave velocity of both the outgoing and reflected wave is increased. The reflected wave therefore meets the initial wave at an earlier time, during the late systolic period. This results in an increase in, or augmentation of, the central systolic pressure with a late systolic peak (Figure 2). The systolic and diastolic blood pressures increase with ageing, with an increase in pulse pressure apparent from approximately 50 years of age (Nichols et al 2005).
Figure 2 Typical aortic pressure waveforms in normotensive subjects
according to age Note the increase in late systolic augmented pressure with age due to increased arterial stiffness and wave reflection.
From: A Clinical Guide: Pulse Wave Analysis (2005). http://www.atcormedical.com/users_guide.html
A few healthy, young people have isolated increased systolic blood pressure (greater than 140 mmHg) with normal diastolic blood pressure, as determined by standard sphygmomanometry (Mahmud and Feely 2003; O’Rourke et al 2000). Investigations usually reveal no abnormality in these individuals. They are typically young (approximately 15–25 years), tall, male and athletic. Their systolic pressure is higher in the upper limbs than in the ascending aorta or left ventricle (ie, the PP amplification that occurs between the aorta and brachial arteries in normal young people is increased). This ‘isolated spurious systolic hypertension of youth’ is thought to be due to increased amplification of the pulse wave in the upper limb. This contrasts with amplification of

6 SphygmoCor system
the central pressure wave seen in older individuals, which is due to augmentation by the reflected pressure wave. The increase in brachial systolic pressure is therefore due to different haemodynamic mechanisms than true central systolic hypertension. Hence, subjects with isolated systolic hypertension of youth will have an aortic pulse waveform with a normal systolic pressure and without a late systolic peak.
Pulse wave analysis of the central aortic pressure wave focuses on several technical measures of the waveform characteristics that are indicative of arterial disease. It is suggested that these measures may be used to determine the risk of cardiovascular events in individuals.
Key haemodynamic measures of cardiovascular function determined by the aortic waveform are the basic aortic blood pressures, augmentation index (AIx), the ejection duration and the subendocardial viability ratio (SEVR).
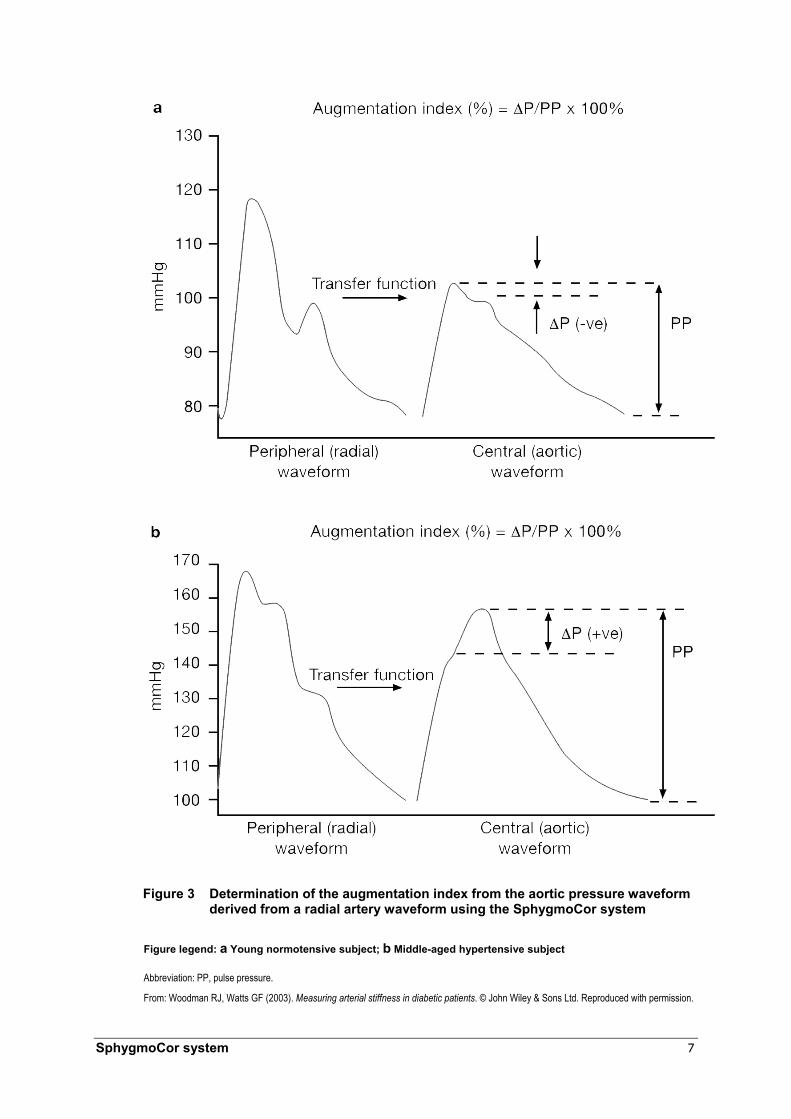
The augmentation pressure is the difference in pressure between the first systolic and second systolic peaks, due to the reflected wave (∆P = P2 – P1). The pulse pressure is the difference between the systolic and diastolic pressures (PP = SBP – DBP). The AIx provides an indirect measure of systemic arterial stiffness, and is calculated as the ratio of the augmentation pressure to the pulse pressure (Figure 3).
A second indirect measurement of arterial compliance is the time to wave reflection (Tr), which is calculated as the time from the wave foot to the systolic inflexion point (P1) (Figure 4). This represents the time taken for the reflected wave to reach the ascending aorta.
The ejection duration is the length of time from the beginning of the pulse to the closure of the aortic valve, as indicated by the dicrotic notch, or incisura (Figure 4). Lower ejection duration may be indicative of systolic dysfunction in heart failure patients. It has been suggested that two types of heart failure can be distinguished by determining whether the abnormality involves the expulsion of blood (systolic dysfunction) or the relaxation of the heart (diastolic dysfunction) (The Cardiac Society of Australia and New Zealand 2002). An ejection fraction of less than 40 per cent indicates systolic dysfunction, and an ejection fraction of greater than 40 per cent in a patient with unequivocal heart failure suggests diastolic dysfunction. However, these criteria are not definitive. Furthermore, in many patients with heart failure, these two conditions coexist.
The SEVR is reported to represent a ratio of the myocardial perfusion supply to demand. It evaluates the ability of the arterial system to meet the energy requirements of the heart. Using the ejection duration as determined from the peripheral pulse, the area under the systolic and diastolic portions of the aortic pressure wave curve are calculated. These two values are the tension time index (TTI), which correspond with the systolic portion of the pressure curve and the diastolic pressure time index (DPTI), corresponding with the diastolic portion of the pressure curve (Figure 4). The SEVR is calculated by applying the formula: DPTI/TTI. A decreased SEVR may indicate a decrease in myocardial perfusion.
SphygmoCor system 7
Figure 3 Determination of the augmentation index from the aortic pressure waveform derived from a radial artery waveform using the SphygmoCor system
Figure legend: a Young normotensive subject; b Middle-aged hypertensive subject
Abbreviation: PP, pulse pressure.
From: Woodman RJ, Watts GF (2003). Measuring arterial stiffness in diabetic patients. © John Wiley & Sons Ltd. Reproduced with permission.

8 SphygmoCor system
Figure 4 Derived aortic pressure wave and pulse wave analysis parameters Abbreviations: DPTI, diastolic pressure time index; P1, systolic inflexion point; P2, systolic peak; TTI, tension time index.
From: A Clinical Guide: Pulse Wave Analysis (2005). http://www.atcormedical.com/users_guide.html
Two measures of arterial compliance, PWV and carotid AIx, have been studied for their prognostic value. In hypertensive patients with baseline arterial stiffness, the carotid to femoral artery PWV has been found to be an independent predictor of both cardiovascular and all-cause mortality (Laurent et al 2001). This study demonstrated that a PWV of 5 m/s was significantly associated with all-cause mortality (odds ratio 2.14, 95% CI: [1.71, 2.67]) and cardiovascular mortality (odds ratio 2.35, 95% CI: [1.76, 3.14]).
Additionally, in people diagnosed with hypertension with baseline arterial stiffness but without a history of cardiovascular disease, PWV was demonstrated to be an independent predictor of the occurrence of cardiovascular events (Boutouyrie et al 2002). A PWV of 3.5 m/s was found to be significantly associated with the occurrence of coronary events (relative risk 1.42, 95% CI: [1.10, 1.82]) and cardiovascular events (relative risk 1.41, 95% CI: [1.17, 1.70]).
Aortic PWV has also be shown to be a predictor of mortality in patients with end-stage renal failure (Blacher et al 1999; London et al 2001; Safar et al 2002) and diabetes (Cruickshank et al 2002), both high risk populations for cardiovascular disease.
In patients with end-stage renal failure, carotid AIx has been found to be an independent predictor of both cardiovascular and all-cause mortality (London et al 2001). This study demonstrated that for each 10 per cent increase in carotid AIx, the odds ratio for both all-cause mortality (odds ratio 1.51, 95% CI: [1.23, 1.86]) and cardiovascular mortality (odds ratio 1.48, 95% CI: [1.16–1.90]) increased.

SphygmoCor system 9
SphygmoCor system
The procedure
The SphygmoCor system is a non-invasive diagnostic technology that enables pulse wave analysis of the central, ascending aortic pressure wave.
The SphygmoCor system obtains peripheral arterial pressure waveforms by applying an arterial applanation tonometer to the wrist. The tonometer partially compresses the radial artery and records a pressure wave over several cardiac cycles. This pressure wave is calibrated to brachial cuff blood pressure measurements. The averaged peripheral waveform is then converted to an ascending aortic waveform using a generalised mathematical transfer function.
The waveform parameters obtained using the SphygmoCor system is useful in the diagnosis of cardiovascular diseases, as indicated in Table 2.
Table 2 Diagnosis of cardiovascular diseases using the SphygmoCor system
Condition Surrogate marker SphygmoCor measure Hypertension Increased aortic stiffness Increase in AIx and a decrease in Tr Isolated systolic hypertension of youth N/A Normal ascending aortic systolic pressure Coronary artery disease Decreased myocardial perfusion Decrease in SEVR Heart failure – systolic dysfunction N/A Decrease in ED Heart failure – diastolic dysfunction N/A Increase in ED
Abbreviations: AIx, augmentation index; CAD, coronary artery disease; ED, ejection duration; HF, heart failure; SEVR, subendocardial viability ratio; Tr, time to wave reflection.
Intended purpose
The intended purpose of the SphygmoCor system for aortic pulse wave analysis is in the assessment of three different cardiovascular conditions – hypertension, stable angina pectoris and heart failure. A cardiologist or specialist physician would use the SphygmoCor system following referral from a patient’s general practitioner.
The SphygmoCor system’s ability to differentiate individuals with isolated spurious systolic hypertension of youth or pseudohypertension, from those with true isolated systolic hypertension, was considered. These individuals will have a raised systolic pressure as determined by standard brachial blood pressure measurement (sphygmomanometry). However, the central aortic waveform measures determined by SphygmoCor may differentiate individuals with true hypertension from those without central hypertension. In addition, the SphygmoCor system’s ability to identify individuals with white coat hypertension was considered.
The ability of the SphygmoCor system to influence therapeutic choices by providing information on the central aortic AIx was also considered. Individuals with a high AIx may benefit more from vasodilators than other antihypertensive agents.
The ability of the SphygmoCor system to determine the underlying cause of stable angina was also considered. If the SEVR is less than 1 at the time of onset of angina, this

10 SphygmoCor system
suggests that the cause of the angina is not a significant coronary artery stenosis, and investigation by angiography may be alleviated or deferred. In addition, these patients might also benefit from treatment with drugs that increase diastolic duration relative to systolic duration (such as β-blockers) or long-acting nitrates that decrease aortic systolic pressure relative to diastolic pressure.
The intended purpose of the SphygmoCor system in patients with heart failure is in diagnosing systolic versus diastolic dysfunction and in directing therapy. Lower ejection duration is suggestive of more severe systolic dysfunction. These patients may also benefit from treatment with sublingual nitrate. A long ejection duration and isolated systolic hypertension are suggestive of diastolic dysfunction resulting from left ventricular hypertrophy. These patients might benefit from treatment with drugs that decrease the heart rate (eg, β-blockers).
The reference standard
In order to investigate the accuracy of a new diagnostic test, the diagnosis made with the new test must be compared with the true disease status. The most accurate measure of the true disease status is the gold standard. Ideally, this should be used as the reference standard to assess a new diagnostic test. However, an alternative measure may be chosen as the reference standard (eg, if the gold standard is highly invasive).
Expert opinion within the Advisory Panel indicated that the assessment of hypertension is based on brachial blood pressure; therefore, the appropriate reference standard for the assessment of hypertension in this review is invasive brachial blood pressure measurement.
The reference standard for the assessment of angina in this review is coronary angiography.
The reference standard for the assessment of heart failure in this review is echocardiography.
Existing tests
Blood pressure measurement
Standard blood pressure measurement is performed by cuff sphygmomanometry. Individuals with hypertension are often further assessed by 24-hour ABPM. Details of these techniques are provided on page 3.
The SphygmoCor system would be used as an additional test in individuals with hypertension who are referred to a specialist. Therefore, current best conventional care (including the use of ABPM) is the main comparator for this indication. However, SphygmoCor may replace ABPM in some patients; therefore the replacement value of SphygmoCor by comparison with ABPM will also be reviewed.
SphygmoCor system 11
Angiography
Coronary angiography is the most commonly used diagnostic test for coronary artery disease.
Coronary angiography is an invasive procedure performed while the patient is under mild sedation. It involves inserting a catheter into a peripheral artery (usually the femoral artery) and advancing it as far as the heart and coronary arteries. A contrast agent is then injected and radiographic imaging provides real-time assessment of the patency of the coronary arteries.
The use of the SphygmoCor system for patients with stable angina pectoris may alleviate or defer the need for coronary angiography. As the SphygmoCor system may be used as an additional test (ie, incremental value of the SphygmoCor system), current best conventional care including the use of angiography is the main comparator for this indication. The replacement value of the SphygmoCor system by comparison with angiography will also be reviewed.
Electrocardiography
Electrocardiography (ECG) is a non-invasive test that records the electrical activity of the heart. Electrical impulses generated by the heart are transmitted to the body’s surface and detected by electrodes placed on the patient’s chest and limbs. A graphic recording of the difference in voltage between the ECG leads is taken, depicting the waves of excitation. The different components of the standard ECG wave are designated by the letters P–T.
Characteristics of the electrocardiogram can be useful as myocardial defects or damage affect the propagation of the electrical signal through the heart.
ECG is a prior test in the clinical pathway and is therefore not considered to be a comparator for the SphygmoCor system in this assessment.
Stress testing
In standard stress testing, ECGs are recorded while the patient is monitored during standard exercise. The test is continued until the patient achieves a target heart rate. This allows the effect of exercise on heart function to be determined. Abnormalities which arise only during periods of increased stress, such as stable angina, can be detected.
SphygmoCor may replace stress testing in some patients; therefore, the replacement value of SphygmoCor by comparison with stress testing will be reviewed.
Cardiac perfusion scan
Cardiac perfusion scans are also referred to as radionucleotide stress testing. These scans involve the introduction of a radiopharmaceutical tracer into the patient to assess coronary blood flow at rest and following either exercise or pharmacologically induced stress. The tracer is tracked within the myocardium using a gamma camera with the data converted to tomographic images. This procedure as with standard ECG stress testing

12 SphygmoCor system
allows for the detection of abnormalities that only arise during periods of increased stress (Mowatt et al 2004).
SphygmoCor may replace cardiac perfusion scans in some patients; therefore, the replacement value of SphygmoCor by comparison with cardiac perfusion scans will be reviewed.
Echocardiography
Echocardiography is a non-invasive diagnostic technique that uses ultrasound to create a real-time image of the heart. The ultrasound images can demonstrate structural and functional abnormalities of the chambers, walls and valves of the heart. By assessing the thickness of the heart wall, echocardiography can assess the severity of left ventricular hypertrophy. Doppler imaging during echocardiography allows evaluation of cardiac output and therefore assessment of ejection fraction, valvular insufficiency and stenosis. Echocardiography can assist in classifying heart failure by providing information on the left ventricular ejection fraction (LVEF). Patients with systolic dysfunction have decreased LVEF, while those with diastolic dysfunction usually have preserved LVEF and no valvular abnormalities (Hunt et al 2001).
The use of the SphygmoCor system for patients with heart failure may alleviate or defer the need for echocardiography. As the SphygmoCor system may be used as an additional test (ie incremental value of the SphygmoCor system), current best conventional care including the use of echocardiography is the main comparator for this indication. The replacement value of the SphygmoCor system by comparison with echocardiography will also be reviewed.
Arterial compliance measures
There are currently several non-invasive approaches used in the clinical estimation of arterial compliance. These methods are based on measuring various parameters that provide an indirect estimation of arterial stiffness.
Three basic approaches were reviewed by Pannier et al (2002), the most common of which is the measurement of pulse wave velocity. This approach estimates arterial stiffness based on the velocity at which the pressure wave travels between two points of known distance apart. The time difference between these two locations is known as the pulse transit time (PTT). The second approach, as utilised in the SphygmoCor system, is based on analysis of the arterial pressure waveform. These two methods both estimate arterial stiffness indirectly. The final option is a more direct estimation of arterial stiffness and involves measuring the artery diameter and distending pressure.
The Finapres®, Portapres® and Cardiopres® systems produced by TNO Biomedical Instrumentation provide similar capabilities to the SphygmoCor system. These devices allow non-invasive, continuous measurement of finger arterial pressure using an infrared plethysmograph system. The Portapres and Cardiopres monitors also enable ambulatory finger pressure measurement to be recorded. These three devices are packaged with Modelflow® and/or Beatscope in the accompanying software suite. These programs are used to analyse many cardiovascular haemodynamic parameters.
SphygmoCor system 13
The Modelflow analysis is based on the Windkessel model and allows an aortic flow waveform (as opposed to the pressure waveform) to be calculated. Therefore, this analysis differs from that of the SphygmoCor system. The Beatscope software includes the Modelflow software, and is also able to determine the brachial pressure wave from the recorded finger pressure wave. This can be further combined with a brachial to aortic transfer function to provide a generalised finger to aortic transfer function (Bos et al 2000). This allows conversion of finger to aortic pressure waves in a manner substantially similar to the SphygmoCor system.
Measures of arterial compliance are not used as diagnostic tests in clinical practice, and therefore are not considered comparators for this assessment.
Hypertension
Clinical need
The AusDiab study, which included 11, 247 Australian people over the age of 25, indicated that 30.6 per cent of men and 27.1 per cent of women (28.8% overall) are living with hypertension (Dunstan et al 2001). This equates to approximately 3 million Australians over 25 years of age with high blood pressure (Australian Institute of Health and Welfare 2004a).
Hypertension is an asymptomatic condition. Although simple to diagnose with standard blood pressure sphygmomanometry, hypertension remains undiagnosed and untreated in many patients. For example, it was estimated that 13 per cent of the population over 25 years of age were undergoing treatment for hypertension, whilst a further 15 per cent had untreated hypertension (Briganti et al 2003).
Mortality and morbidity
While hypertension is a common disorder, the aetiology of most diagnosed cases remains unknown. This is referred to as essential hypertension. Hypertension occurring secondary to another organic disease (eg, renal failure, endocrine disorders) is referred to as secondary hypertension.
This condition is a major financial burden on the Australian health care system. Blood pressure-lowering drugs available through the Pharmaceutical Benefits Scheme (PBS) cost $755 million in 2000. This corresponds to 16.5 per cent of government and patient costs for prescription PBS drugs (Australian Institute of Health and Welfare 2004a).
In addition to its direct burden, hypertension is a major contributor to deaths due to all cardiovascular diseases. In 2002, cardiovascular disease was responsible for 38 per cent of all deaths and 7 per cent of all hospitalisations (Australian Institute of Health and Welfare 2004a).
14 SphygmoCor system
Current treatment
Changes in lifestyle according to the SNAP (smoking, nutrition, alcohol, physical activity) risk factors may result in adequate control of mild hypertension (Australian Heart Foundation, 2004). However, in patients with more severe hypertension and those whose hypertension is not adequately controlled by lifestyle changes, pharmacological management is recommended. There are five main classes of antihypertensive drugs: low-dose thiazide diuretics, β-blockers, angiotensin-converting enzyme inhibitors, calcium channel blockers and angiotensin II receptor antagonists. The initial drug choice will be affected by a number of factors such as cardiovascular risk profile, presence of co-existing conditions, concomitant medications, effectiveness and cost. However, most individuals using antihypertensive medications will require a combination of drugs to manage their condition effectively. Detailed guidelines are provided in the hypertension management guide for doctors (Australian Heart Foundation, 2004).
Angina pectoris
Clinical need
Angina pectoris is a symptom of a disease rather than a disease itself. It is a sensation of chest discomfort that occurs when the oxygen supply to the heart muscle does not match metabolic demand. This usually occurs due to the narrowing of a coronary artery, leading to a reduction in the blood flow to the heart (coronary artery disease). Chest discomfort generally manifests as a feeling of pressure or squeezing. However, an angina attack may be accompanied by additional symptoms, such as fainting, nausea and light-headedness. Other conditions that may contribute to the occurrence of angina include congestive heart failure and anaemia.
In stable angina, the discomfort usually develops after exercise, excitement or a large meal, and the symptoms are stable over a long period of time. Unstable angina presents with more pain that lasts longer and frequently occurs when the person is at rest. Angina is usually diagnosed by stress testing (see page 11).
Mortality and morbidity
In 2002, coronary artery disease (CAD) was the largest single cause of death in the Australian population, and was responsible for 19.5 per cent of all deaths (Australian Institute of Health and Welfare 2004a).
The 2001 National Health Survey reported that 1.9 per cent of the surveyed population (corresponding to approximately 355,600 Australians) experienced some manifestation of CAD. The majority of these individuals reported having angina and approximately a third reported experiencing heart attack. High blood pressure is common (50.3%) in people with CAD (Australian Institute of Health and Welfare 2004a).
During 2001–2002 an estimated 48,700 CAD events occurred in Australia among 40–90 year olds. About half of these events were fatal (Australian Institute of Health and Welfare 2004a).
SphygmoCor system 15
CAD was responsible for 26,063 deaths (13,855 men, 12,208 women) in 2002. This equates to an age-standardised mortality (for Australia) of 169.7/100,000 for men and 97.8/100,000 for women. The age-standardised mortality for all persons was 129.7/100,000 (Australian Institute of Health and Welfare 2004b).
In 2001–2002, it was estimated that CAD was responsible for 2.5 per cent of all hospitalisations in Australia and accounted for 36 per cent of all hospitalisations for cardiovascular disease (Australian Institute of Health and Welfare 2004a).
Current treatment
The management of angina pectoris involves changes in lifestyle, including diet and exercise patterns, in order to reduce the symptoms and to prevent complications (Australian Institute of Health and Welfare: Mathur 2002). Long-term pharmacotherapy may also be used to control angina, using agents such as long-acting nitrates, β-blockers and calcium channel blockers. In addition, other medications may be used to treat hypertension, hyperlipidaemia and arrhythmias in order to control the underlying condition. In some angina patients, surgical revascularisation procedures may be necessary. Revascularisation procedures that are commonly performed are percutaneous transluminal coronary angioplasty (with or without stenting) and coronary artery bypass grafting.
Heart failure
Clinical need
Heart failure is a pathophysiological state in which there is an abnormality in the heart’s ability to pump blood. Most cases of heart failure involve defects in myocardial (heart muscle) contraction. These may be caused by coronary atherosclerosis, valvular disease or congenital heart disease. The defects increase the haemodynamic burden on the ventricles, which leads to ventricular hypertrophy. This in turn increases the stress on the myocardium.
Mortality and morbidity
In 2002, heart failure was the third largest cause of death from cardiovascular diseases in the Australian population, and was responsible for 2 per cent of all deaths (Australian Institute of Health and Welfare 2004a).
The estimated prevalence for heart failure in Australia is based on international data, approximately 300,000 Australians have chronic heart failure with a further 30,000 diagnosed each year (Australian Institute of Health and Welfare 2004a).
Heart failure was responsible for 2729 deaths in 2002 (1033 men, 1696 women). This equates to an age-standardised mortality (for Australia) of 14.1/100,000 for men and 13.0/100,000 for women. The age-standardised mortality in all persons was 13.5/100,000 (Australian Institute of Health and Welfare 2004b).

16 SphygmoCor system
Heart failure is estimated to account for 0.7 per cent of all hospitalisations in Australia and 9.5 per cent of all hospitalisations for cardiovascular disease (Australian Institute of Health and Welfare 2004a).
Current treatment
As with angina pectoris, the management of heart failure involves changes in lifestyle, such as diet and exercise patterns (Cardiac Society of Australia and New Zealand 2002). Heart failure also requires pharmacological management in order to decrease the effects of systolic and/or diastolic dysfunction, as well as treatment of any concomitant cardiovascular conditions. Patients with systolic heart failure should be treated with angiotensin-converting enzyme inhibitors and β-blockers. Patients with diastolic dysfunction may be treated with diuretics and/or nitrates; however, there is currently no strong evidence about whether or not these classes of drugs improve left ventricular function (Cardiac Society of Australia and New Zealand 2002). The American College of Cardiology and the American Heart Association recommend that patients with diastolic dysfunction be managed by controlling physiological factors such as blood pressure, heart rate, blood volume and ischaemia (Hunt et al 2001). Such management will have beneficial effects on ventricular relaxation. In some instances, the cause of heart failure may be known and surgery (such as valve replacement) may be an option. Healthy heart failure patients may require a heart transplant if they are not successfully managed by medication. Patients who cannot be managed by any therapies and are not candidates for heart transplantation are provided palliative care.
Potential impact of the test
Increased accuracy in the assessment of hypertension, stable angina pectoris and heart failure could lead to a reduction in unnecessary treatments, as well as a reduction in the use of other invasive diagnostic procedures such as angiography.
The SphygmoCor system has the potential to provide the attending specialist with more detailed information on the cardiovascular status of a patient, which could lead to a change in management. This could result in better control of the patient’s condition.
Marketing status of the device
There are three registered SphygmoCor systems on the market; all are listed with the Therapeutic Goods Administration (TGA) on the Australian Registry of Therapeutic Goods under the listing number L64615. These systems are approved for marketing in Australia, the United States of America, the European Union, Korea, China and Japan.
The SphygmoCor Px system is a non-invasive method of measuring peripheral arterial pressure waveforms that, through the use of a validated transfer function, allows calculation of the ascending aortic pressure waveform. The SphygmoCor Mx system measures radial waveforms and provides a real-time method of deriving aortic pressure waveforms. The SphygmoCor Vx system utilises an ECG in combination with a tonometer to measure the pressure waveform sequentially at two peripheral artery sites. This system provides a means of analysing pulse wave velocity in addition to pressure wave analysis.

SphygmoCor system 17
The US Food and Drug Administration (FDA) has determined that the SphygmoCor Mx system is substantially equivalent to a standard intravascular catheter attached to a conventional manometer and blood pressure monitor for obtaining calibrated central aortic blood pressure (K002742). It is stated that the system is designed for use with a conventional invasive radial artery blood pressure monitor in the hospital setting. The document states that the indication for use is “in those patients where information related to the ascending aortic pressure is desired, but in the opinion of the physician, the risks of cardiac catheterisation may outweigh the benefits”. This substantial equivalence is based on a study comparing the SphygmoCor Mx system using an invasive radial artery pressure transducer to pressures measured invasively with a catheter in the aorta (Pauca et al 2001). The FDA later determined that the SphygmoCor Px system was substantially equivalent to the SphygmoCor Mx system (K012487). This was based on a study comparing radial artery pressure waveforms determined invasively with a catheter to radial artery pressure waveforms determined by a non-invasive Millar tonometer.
Current reimbursement arrangement
The SphygmoCor system is not currently funded under the Medicare Benefits Schedule (MBS).
18 SphygmoCor system
Approach to assessment
Research questions and clinical pathways
Hypertension
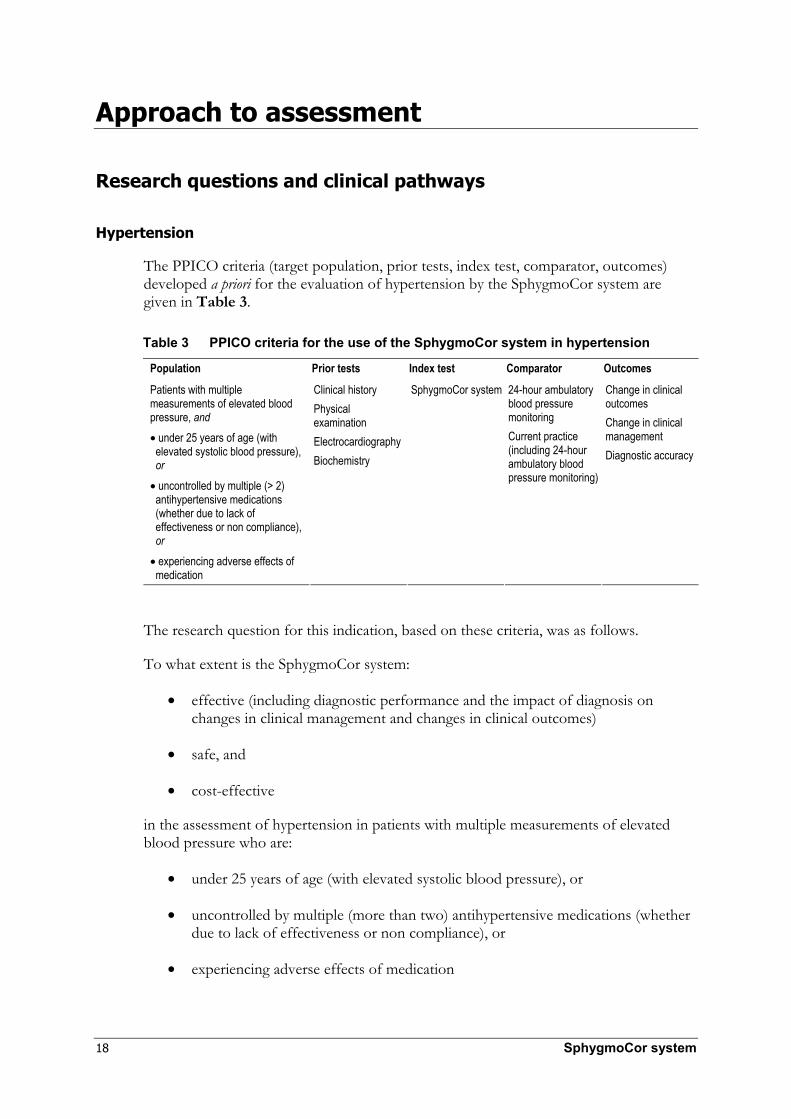
The PPICO criteria (target population, prior tests, index test, comparator, outcomes) developed a priori for the evaluation of hypertension by the SphygmoCor system are given in Table 3.
Table 3 PPICO criteria for the use of the SphygmoCor system in hypertension
Population Prior tests Index test Comparator Outcomes
Patients with multiple measurements of elevated blood pressure, and • under 25 years of age (with
elevated systolic blood pressure), or
• uncontrolled by multiple (> 2) antihypertensive medications (whether due to lack of effectiveness or non compliance), or
• experiencing adverse effects of medication
Clinical history Physical examination Electrocardiography Biochemistry
SphygmoCor system 24-hour ambulatory blood pressure monitoring Current practice (including 24-hour ambulatory blood pressure monitoring)
Change in clinical outcomes Change in clinical management Diagnostic accuracy
The research question for this indication, based on these criteria, was as follows.
To what extent is the SphygmoCor system:
• effective (including diagnostic performance and the impact of diagnosis on changes in clinical management and changes in clinical outcomes)
• safe, and
• cost-effective
in the assessment of hypertension in patients with multiple measurements of elevated blood pressure who are:
• under 25 years of age (with elevated systolic blood pressure), or
• uncontrolled by multiple (more than two) antihypertensive medications (whether due to lack of effectiveness or non compliance), or
• experiencing adverse effects of medication

SphygmoCor system 19
relative to 24-hour ambulatory blood pressure monitoring or relative to current best conventional care (clinical history, physical examination, electrocardiography, biochemical tests, 24-hour ambulatory blood pressure monitoring) in the absence of SphygmoCor?
The clinical pathway for the evaluation of patients referred with hypertension (less than 25 years of age) is shown in Figure 5. Figure 6 illustrates the clinical pathway for the evaluation of patients referred with hypertension who are either uncontrolled by multiple medication (more than two drugs) or experience adverse effects of medication. Both of these flowcharts display the clinical management pathway to the point of patient diagnosis.

20 SphygmoCor system
Primary care:
Young patients (< 25 years) with multiple elevated systolic blood pressure
readings, as determined by brachial cuff blood pressure measurements
Referral to a cardiologist or a physician
specialising in hypertension
Clinical history, physical examination (including brachial cuff blood pressure measurements), ECG, biochemistry,
24 hour ABPM
Current (comparator) pathway Concurrently with previous tests Proposed pathway
No SphygmoCor system SphygmoCor system
Normal SBPa
Increased SBPa Increased aortic
SBP Normal aortic
SBP
Clinical suspicion
Test for secondary causes of hypertension (eg, RA duplex
ultrasonography)
Clinical suspicion
No Yes Yes No
Echocardiogram Echocardiogram
Cease treatment
and further investigation
Appropriate treatment
Appropriate treatment/ Cease treatment
Appropriate treatment
Cease treatment
and further investigation
Figure 5 Clinical pathway for the investigation of patients referred with hypertension (<25 years of age)
Abbreviations: ABPM, ambulatory blood pressure monitoring; ECG, electrocardiogram; RA, renal artery; SBP, systolic blood pressure. a Blood pressure measurement based on 24 hour ABPM.

SphygmoCor system 21
Primary care:
Patients with multiple recordings of elevated blood pressure, as determined by brachial cuff blood pressure measurements, who
are uncontrolled by multiple (> 2) antihypertensive medications or who are experiencing adverse effects due to the medication
Referral to a cardiologist or a physician specialising in
hypertension
Clinical history, physical examination (including brachial cuff blood pressure measurements), ECG, biochemistry, chest X-ray
(10–20%) patients, 24 hour ABPMa
Current (comparator) pathway Concurrently with previous tests
Proposed pathway
No SphygmoCor systema SphygmoCor system
Normal BPb Increased BPb No hypertension
Stop treatment Hypertension with normal Tr/AIx
Hypertension with decreased Tr or increased AIx
Stop treatment
24 hour ABPM SphygmoCor system
Test for secondary causes of hypertension and end-organ damage
(eg. RA duplex ultrasonography, echocardiography, creatine levels
Normal BP
Increased BP
Normal aortic BP
Increased aortic BP
Diagnosis of white coat
hypertension
Diagnosis of white coat
hypertension
Appropriate treatment/
management
Cease treatment and
further investigation
Appropriate treatment/
cease management
Management change
(eg. treat with
vasodilators)
Cease treatment and
further investigation
Appropriate treatment/
management
Figure 6 Clinical pathway for the investigation of patients referred with hypertension who are uncontrolled by multiple medication (more than two drugs) or who are experiencing adverse effects of medication
Abbreviations: ABPM, ambulatory blood pressure monitoring; AIx, augmentation index; BP, blood pressure; ECG, electrocardiogram; RA, renal artery; Tr, time to reflection.
a 24 hour ABPM would be an appropriate comparator in some patients. b Blood pressure measurement based on 24 hour ABPM.
22 SphygmoCor system
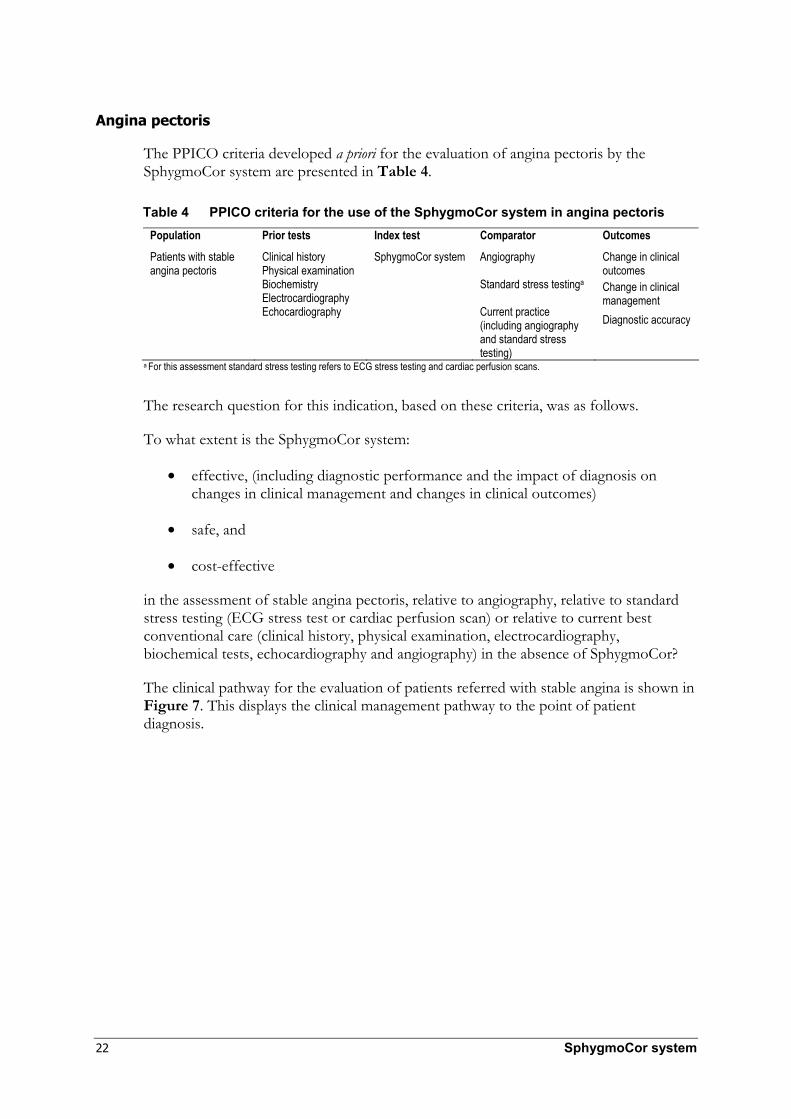
Angina pectoris
The PPICO criteria developed a priori for the evaluation of angina pectoris by the SphygmoCor system are presented in Table 4.
Table 4 PPICO criteria for the use of the SphygmoCor system in angina pectoris Population Prior tests Index test Comparator Outcomes
Patients with stable angina pectoris
Clinical history Physical examination Biochemistry Electrocardiography Echocardiography
SphygmoCor system Angiography Standard stress testinga Current practice (including angiography and standard stress testing)
Change in clinical outcomes Change in clinical management Diagnostic accuracy
a For this assessment standard stress testing refers to ECG stress testing and cardiac perfusion scans.
The research question for this indication, based on these criteria, was as follows.
To what extent is the SphygmoCor system:
• effective, (including diagnostic performance and the impact of diagnosis on changes in clinical management and changes in clinical outcomes)
• safe, and
• cost-effective
in the assessment of stable angina pectoris, relative to angiography, relative to standard stress testing (ECG stress test or cardiac perfusion scan) or relative to current best conventional care (clinical history, physical examination, electrocardiography, biochemical tests, echocardiography and angiography) in the absence of SphygmoCor?
The clinical pathway for the evaluation of patients referred with stable angina is shown in Figure 7. This displays the clinical management pathway to the point of patient diagnosis.

SphygmoCor system 23
Primary care: Patients with stable angina
Referral to a cardiologist or a physician specialising in coronary
artery disease
Clinical history, physical examination (including brachial cuff
measurements). ECG, standard stress testinga, biochemistry,
echocardiology
Negative results
Positive results Current (comparator) pathway
Positive results Proposed pathway
Consider an alternative diagnosis
Angiography SphygmoCor system
Negative Positive Positive Positive Negative
Consider an alternative diagnosis
Appropriate treatment for
coronary artery disease
Normal SEVR
Decreased SEVR
Cease further investigation
No response
Management change (eg. treat with beta-
blockers)
Response
Continue appropriate treatment
Figure 7 Clinical pathway for the investigation of patients with stable angina Abbreviations: ECG, electrocardiography; SEVR, subendocardial viability ratio. a Standard stress testing (ECG stress testing, cardiac perfusion scans) would be an appropriate comparator in some patients.

24 SphygmoCor system
Heart failure
The PPICO criteria developed a priori for the evaluation of heart failure by the SphygmoCor system are given in Table 5.
Table 5 PPICO criteria for the use of the SphygmoCor system in heart failure Population Prior tests Index test Comparator Outcomes
Patients with heart failure
Clinical history Physical examination Electrocardiography Biochemistry
SphygmoCor system Echocardiography Current practice (including echocardiography)
Change in clinical outcomes Change in clinical management Diagnostic accuracy
The research question for this indication, based on these criteria, was as follows.
To what extent is the SphygmoCor system:
• effective, (including diagnostic performance and the impact of diagnosis on changes in clinical management and changes in clinical outcomes)
• safe, and
• cost-effective
in the assessment of heart failure, relative to echocardiography, or relative to current best conventional care (clinical history, physical examination, ECG, biochemical tests and echocardiography) in the absence of SphygmoCor?
The clinical pathway for the evaluation of patients referred with heart failure is shown in Figure 8. This displays the clinical management pathway to the point of patient diagnosis.

SphygmoCor system 25
Primary care:
Patients with heart failure
Referral to a cardiologist or a physician
specialising in heart failure
Clinical history, physical examination (including brachial cuff blood pressure measurements), ECG, biochemistry
Current (comparator) pathway Concurrently with previous tests Proposed pathway
Echocardiogram SphygmoCor system
Diastolic dysfunction Systolic
dysfunction Decreased
ejection duration Normal or increased
ejection duration
Test for other causes of
heart failure
Appropriate treatment
Continue monitoring and treatment
No change
Echocardiogram Deterioration Evaluate disease status
Diastolic dysfunction
Systolic dysfunction
Test for other causes of heart
failure
Appropriate treatment
Figure 8 Clinical pathway for the investigation of patients with heart failure Abbreviation: ECG, electrocardiography.

26 SphygmoCor system
Assessment framework
Types of evidence
A systematic review of the medical literature was undertaken to identify relevant studies on the value of the SphygmoCor system. Direct evidence regarding the impact of the SphygmoCor system on health outcomes was sought. However, the literature search was not limited by outcomes or comparators. Therefore, in the absence of studies providing direct evidence, indirect evidence regarding the impact of the SphygmoCor system on clinical management and diagnostic accuracy was assessed. This indirect evidence was then combined with the evaluation of treatment effectiveness to assess the impact of the SphygmoCor system on health outcomes.
Review of the literature
The medical literature was searched to identify all relevant studies and reviews published to 2005. Searches were conducted in the primary databases indicated in Table 6.
Search strategy
Primary databases
Table 6 Electronic databases searched for the SphygmoCor hypertension review Database Period covered/date searched Medline 1966 to August, week 1, 2005 EMBASE 1980 to 2005, week 33 PreMedline 17 August 2005 Cochrane Library Issue 3, 2005 (17 August 2005)
The search terms included the following (as determined from the PPICO criteria):
• SphygmoCor, Finapres, Portapres, Cardiopres, aortic transfer function, central arterial transfer function, carotid transfer function, aortic mathematical transformation, central arterial mathematical transformation, carotid mathematical transformation, aortic pulse wave analysis, central arterial pulse wave analysis, carotid pulse wave analysis, aortic augmentation index, central arterial augmentation index, carotid augmentation index, aortic arterial tonometry, central arterial tonometry, carotid arterial tonometry.
Complete details of the literature searches performed using the Medline and EMBASE databases are presented in Appendix D.
SphygmoCor system 27
Secondary databases
Searches of the following secondary databases/sites were also performed:
• British Columbia Office of Health Technology Assessment (Canada)
• Canadian Coordinating Office for Health Technology Assessment (CCOHTA)
• Centre for Health Economics (Monash University, Australia) • Current Controlled Trials metaRegister and International Standard Randomised
Controlled Trial Number (ISRCTN) register
• Health Economics Research Group (Brunel University, UK)
• National Health and Medical Research Council Australia (publication list)
• National Health Service (UK)
• Scottish Intercollegiate Guideline Network (SIGN)
• Swedish Council on Technology Assessment in Health Care (SBU)
• The Blue Cross and Blue Shield Association (Technology Evaluation Centre).
Additional searches were conducted to source quality of life, epidemiological and economic information, as required.
Communication
The corresponding authors of relevant publications were contacted for any additional data applicable to this review.

28 SphygmoCor system
Selection criteria
Hypertension
Table 7 Selection criteria for included studies for hypertension Research question: to what extent is the SphygmoCor system effective, safe and cost-effective in the assessment of patients with multiple measurements of elevated blood pressure and under 25 years of age, or uncontrolled by multiple (> 2) medications, or experiencing adverse effects of medication, relative to 24-hour blood pressure monitoring or relative to current best conventional care (clinical history, physical examination, electrocardiography, biochemical tests, 24-hour ambulatory blood pressure monitoring) in the absence of SphygmoCor? Selection criteria Inclusion Exclusion Study design Trials with ≥ 10 patients
receiving SphygmoCora and comparatorb
Non-systematic reviews, letters and opinion pieces, non-human or in vitro studies
Population Patient population with hypertension
Patient populations with diabetes or renal insufficiencyc
Prior tests Not specified for inclusion or exclusion criteria Index test Use of the SphygmoCor systema
for PWA as currently approved by the TGA
Use of only pulse wave velocity or flow waveform measures to estimate arterial compliance Peripheral-to-carotid or carotid-to-aortic general transfer functions
Reference standard Transducer tipped catheter or fluid filled catheter with appropriate calibrationd
Comparator 24-hour ambulatory blood pressure monitoring Current best conventional care
Outcomes Diagnostic performance; effect on clinical management and/or health outcomes
Abbreviations: PWA, pulse waveform analysis; TGA, Therapeutic Goods Administration. a Or a substantially equivalent device deriving central aortic from peripheral pressure waveforms using a mathematical transfer function. b Studies with less than 10 patients will be included for the assessment of adverse event and safety data. c These populations were included but were not treated as separate patient populations d This refers to brachial blood pressure for this assessment.

SphygmoCor system 29
Angina pectoris
Table 8 Selection criteria for included studies for angina pectoris Research question: to what extent is the SphygmoCor system effective, safe and cost-effective in the assessment of stable angina, relative to angiography, relative to standard stress testing (ECG stress test or cardiac perfusion scan) or relative to current best conventional care (clinical history, physical examination, ECG, biochemical tests, echocardiography and angiography) in the absence of SphygmoCor? Selection criteria Inclusion Exclusion Study design Trials with ≥ 10 patients
receiving SphygmoCora and comparatorb
Non-systematic reviews, letters and opinion pieces, non-human or in vitro studies
Population Patient population with stable angina pectoris
Patient populations with diabetes or renal insufficiencyc
Prior tests Not specified for inclusion or exclusion criteria Index test Use of the SphygmoCor systema
as currently approved by the TGA
Use of only pulse wave velocity or flow waveform measures to estimate arterial compliance Peripheral-to-carotid or carotid-to-aortic general transfer functions
Reference standard Angiography
Comparator Angiography Standard stress testingd
Current best conventional care
Outcomes Diagnostic performance; effect on clinical management and/or health outcomes
Abbreviation: TGA, Therapeutic Goods Administration. a Or a substantially equivalent device deriving central aortic from peripheral pressure waveforms using a mathematical transfer function. b Studies with less than 10 patients will be included for the assessment of adverse event and safety data. c These populations were included but were not treated as separate patient populations d For this assessment standard stress testing refers to ECG stress testing and cardiac perfusion scans.
Heart failure
Table 9 Selection criteria for included studies for heart failure Research question: to what extent is the SphygmoCor system effective, safe and cost-effective in the assessment of heart failure, relative to echocardiography, or relative to current best conventional care (clinical history, physical examination, ECG, biochemical tests, echocardiography) in the absence of SphygmoCor? Selection criteria Inclusion Exclusion Study design Trials with ≥ 10 patients
receiving SphygmoCora and comparatorb
Non-systematic reviews, letters and opinion pieces, non-human or in vitro studies
Population Patient population with heart failure
Patient populations with diabetes or renal insufficiencyc
Prior tests Not specified for inclusion or exclusion criteria Index test Use of the SphygmoCor systema
as currently approved by the TGA
Use of only pulse wave velocity or flow waveform measures to estimate arterial compliance Peripheral-to-carotid or carotid-to-aortic general transfer functions
Reference standard Echocardiography
Comparator Echocardiography Current best conventional care
Outcomes Diagnostic performance; effect on clinical management and/or health outcomes
Abbreviation: TGA, Therapeutic Goods Administration. a Or a substantially equivalent device deriving central aortic from peripheral pressure waveforms using a mathematical transfer function. b Studies with less than 10 patients will be included for the assessment of adverse event and safety data. c These populations were included but were not treated as separate patient populations

30 SphygmoCor system
Search results
A total of 756 non-duplicate citations relating to peripheral to aortic general transfer functions were identified. One diagnostic accuracy study was identified, while a further 11 studies were identified that provided indirect evidence of the use of the SphygmoCor system in the diagnosis of spurious systolic hypertension of youth (Appendix E).
Quorum flowchart
Figure 9 Summary of the process used to identify and select studies for the review Adapted from Moher et al (1999).
Abbreviation: GTF, general transfer function. a Data presented in Appendix E.
Potentially relevant studies identified in the literature search and screened for retrieval (n = 756)
Studies retrieved for more detailed evaluation (n = 188)
Potentially appropriate studies to be included in the systematic review (n = 33)
Studies included in the systematic review (n = 12)
Studies with usable information by outcome (n = 12) Accuracy (n = 1) Indirect evidence (n = 11)a Change in management (n = 0) Patient outcomes (n = 0)
Studies excluded, with reasons (n = 155) Review, editorial, letter etc. (n = 44) Not human (n = 2) Not a peripheral to aortic GTF (n = 57) Inadequate reference standard (n = 49) Wrong comparator (n = 3)
Studies excluded, with reasons (n = 568) Review, editorial, letter etc (n = 23) Not human (n = 91) Not a peripheral to aortic GTF (n = 337) Inadequate reference standard (n = 115) <10 patients (n = 2)
Studies excluded with reasons (n = 21) Wrong outcomes (n = 21)
SphygmoCor system 31
Data extraction
Data extraction was performed with the aid of a pro forma based on the following key parameters: trial characteristics, study population characteristics, tests used and outcomes reported. This follows the procedure for the collection of data outlined in the Cochrane Reviewers’ Handbook (Alderson et al 2005).
Statistical methods
Methodological considerations
Evidence that the surrogate outcomes measured by SphygmoCor are risk factors for health outcomes provides only supplementary, theoretical information on the value of SphygmoCor. The evidence required to justify reimbursement under Medicare is direct comparative evidence of the value of SphygmoCor, when used in the relevant patient group. This should ideally be in the form of studies reporting effects on patient-centred health outcomes. Alternatively, evidence of greater diagnostic accuracy than the comparator, along with linked evidence of change in management and evidence that treatment will affect health outcomes is required.
In cases where a diagnostic test is to be used as an additional test in the clinical pathway, evidence for an effect on change in management is a key component of the evidence base. The most appropriate design for investigation of the effects on change in management is a pre-test post-test case series study. Where a pre-test management plan is not reported, the outcomes of a study are not truly change in patient management and the outcomes are likely to be biased.
The ideal design for a study of the comparative accuracy of diagnostic tests is that in which each test being compared is performed in all individuals, in a consecutive series of patients with a defined clinical presentation. The study should be an independent, blinded comparison with a valid reference standard (NHMRC 2005).
Diagnostic performance
The evaluation of the accuracy of a new diagnostic test involves comparing the new test with its comparators and the best available proxy for the true disease status, the reference standard. The new diagnostic test and its comparators can be independently compared with the reference standard to assess sensitivity, specificity, accuracy, diagnostic odds ratio and likelihood ratios.
The sensitivity is the proportion of all patients with the disease who test positive. The specificity is the proportion of all patients without the disease who test negative. The accuracy of a test is the proportion of patients that the test correctly identified as positive or negative. The diagnostic odds ratio (DOR) is the odds of a positive test in patients with the disease compared to those without the disease. A DOR of 100 provides convincing evidence of the test’s ability to discriminate the presence of absence of the disease.

32 SphygmoCor system
The likelihood ratio of a positive test is the probability that a positive test will be found in a person with, as opposed to without, the condition; the likelihood ratio of a negative test is the probability that a negative test will be found in a person with, as opposed to without, the condition. A positive ratio of greater than 10 and a negative ratio less than 0.1 provide convincing diagnostic evidence. A positive likelihood ratio of greater than 5 and a negative likelihood ratio of less than 0.2 provide strong diagnostic evidence (Medical Services Advisory Committee, 2004). Bayes’ theorem indicates that the post-test odds of disease equals the pre-test odds of disease times the likelihood ratio. Using this approach, the post-test probability of disease can be determined, for any given pre-test disease probability.
Appraisal of the evidence
Appraisal of the evidence was conducted at three stages, as follows.
Stage 1: Appraisal of the applicability and quality of individual studies included in the review.
Stage 2: Appraisal of the precision, size and clinical importance of the primary outcomes used to determine the safety and effectiveness of the test.
Stage 3: Integration of this evidence in order to draw conclusions about the net clinical benefit of the index test in the context of Australian clinical practice.
Appraisal of the quality and applicability of individual studies
The quality and applicability of the included studies was assessed according to pre-specified criteria according to the study design (Appendix C).
Ranking the evidence
Studies evaluating the direct impact of the test or treatment on patient outcomes were ranked according to the study design, using the levels of evidence designated by the National Health and Medical Research Council (NHMRC) shown in Table 10. However, there were no such trials identified in this review.
Table 10 NHMRC levels of evidence for studies of effectiveness Level of evidence Study design I Evidence obtained from a systematic review of level II studies II Evidence obtained from properly designed randomised controlled trials III-1 Evidence obtained from well-designed pseudo-randomised controlled trials (alternate allocation or
some other method) III-2 Evidence obtained from comparative studies with concurrent controls: non-randomised experimental
trials, cohort studies, case-control studies, or interrupted time series with a control group III-3 Evidence obtained from comparative studies without concurrent controls: historical control studies, two
or more single-arm studies, or interrupted time series without a parallel control group IV Evidence obtained from case series, either post-test or pre-test/post-test outcomes
Source: NHMRC, 2005.
Studies of diagnostic accuracy were ranked according to the NHMRC levels of evidence for diagnosis shown in Table 11.
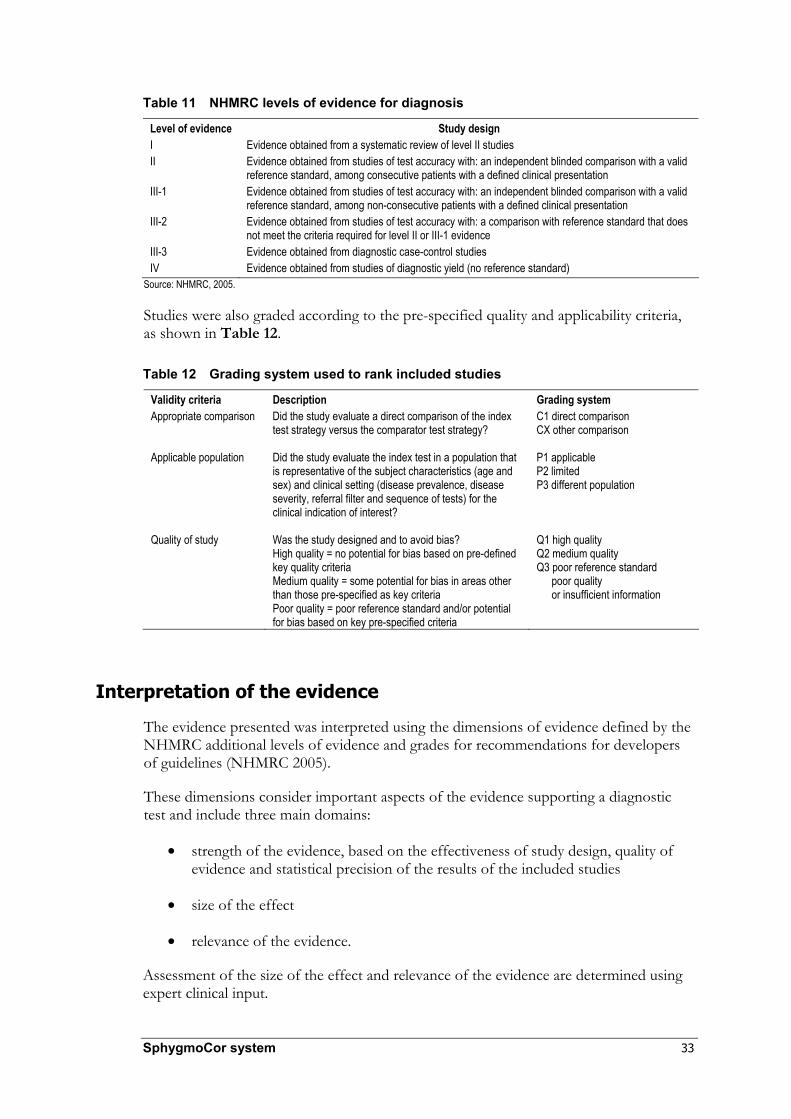
SphygmoCor system 33
Table 11 NHMRC levels of evidence for diagnosis
Level of evidence Study design I Evidence obtained from a systematic review of level II studies II Evidence obtained from studies of test accuracy with: an independent blinded comparison with a valid
reference standard, among consecutive patients with a defined clinical presentation III-1 Evidence obtained from studies of test accuracy with: an independent blinded comparison with a valid
reference standard, among non-consecutive patients with a defined clinical presentation III-2 Evidence obtained from studies of test accuracy with: a comparison with reference standard that does
not meet the criteria required for level II or III-1 evidence III-3 Evidence obtained from diagnostic case-control studies IV Evidence obtained from studies of diagnostic yield (no reference standard)
Source: NHMRC, 2005.
Studies were also graded according to the pre-specified quality and applicability criteria, as shown in Table 12.
Table 12 Grading system used to rank included studies
Validity criteria Description Grading system Appropriate comparison Did the study evaluate a direct comparison of the index
test strategy versus the comparator test strategy?
C1 direct comparison CX other comparison
Applicable population Did the study evaluate the index test in a population that is representative of the subject characteristics (age and sex) and clinical setting (disease prevalence, disease severity, referral filter and sequence of tests) for the clinical indication of interest?
P1 applicable P2 limited P3 different population
Quality of study Was the study designed and to avoid bias? High quality = no potential for bias based on pre-defined key quality criteria Medium quality = some potential for bias in areas other than those pre-specified as key criteria Poor quality = poor reference standard and/or potential for bias based on key pre-specified criteria
Q1 high quality Q2 medium quality Q3 poor reference standard
poor quality or insufficient information
Interpretation of the evidence
The evidence presented was interpreted using the dimensions of evidence defined by the NHMRC additional levels of evidence and grades for recommendations for developers of guidelines (NHMRC 2005).
These dimensions consider important aspects of the evidence supporting a diagnostic test and include three main domains:
• strength of the evidence, based on the effectiveness of study design, quality of evidence and statistical precision of the results of the included studies
• size of the effect
• relevance of the evidence.
Assessment of the size of the effect and relevance of the evidence are determined using expert clinical input.

34 SphygmoCor system
Expert advice
An Advisory Panel, whose membership included clinicians with particular expertise and interest in hypertensive disorders, was established to evaluate the evidence and provide advice to MSAC from a clinical perspective. In selecting members for Advisory Panels, MSAC’s practice is to approach the appropriate medical colleges, specialist societies and associations and consumer bodies for nominees. Membership of the Advisory Panel is listed in Appendix B.

SphygmoCor system 35
Results of assessment
Summaries of the design, population characteristics, test characteristics, outcomes and an assessment of quality and applicability for all studies used in the assessment are presented in Appendix F.
Is it safe?
The SphygmoCor system is a non-invasive test and therefore there are no adverse events associated with its use. In contrast, some of the comparators do have associated risks and potential adverse events. However in the absence of evidence for equal or greater effectiveness of the SphygmoCor system relative to the comparator, evidence for comparative safety is inconsequential.
Is it effective?
Direct evidence
Does it improve health outcomes?
No studies were identified that compared the effectiveness of the use of the SphygmoCor system with current clinical practice in the absence of SphygmoCor in any patient population.
Linked evidence
Is it accurate?
Hypertension No studies were identified that reported the performance of systems deriving a central aortic waveform using a radial to aortic transfer function compared with invasive brachial blood pressure.
White coat hypertension
No studies were identified that reported the diagnostic accuracy of systems deriving a central aortic waveform using a radial to aortic transfer function compared to 24-hour ambulatory blood pressure monitoring in the diagnosis of white coat hypertension.
Spurious systolic hypertension of youth
No studies were identified that reported on the performance of radial to central transfer functions compared with a valid reference standard in the diagnosis of spurious systolic hypertension of youth. It is considered unlikely that such studies could be performed ethically in this population. Because of this situation an assessment of the technical accuracy of the SphygmoCor system was undertaken (Appendix E) to determine whether the SphygmoCor system could accurately estimate central blood pressure

36 SphygmoCor system
compared with upper limb blood pressure measurement. The results of this assessment were linked to studies identifying the characteristics of spurious systolic hypertension of youth to determine if there is any indirect evidence to support the use of the SphygmoCor system.
Angina pectoris One study was identified that compared the association of a single pulse wave parameter (the augmentation index, AIx), as determined by SphygmoCor, with the presence of coronary artery disease, as determined by angiography. No studies were identified that provided information on the accuracy of other measures determined by SphygmoCor for the diagnosis of coronary artery disease (CAD).
The one identified study was designed to determine the relationship between CAD and AIx as determined by pulse waveform analysis (PWA) using the SphygmoCor system. The characteristics of this study are shown in Table 13. The authors reported the association between AIx and CAD as an odds ratio for the presence of disease, an outcome that does not provide information on diagnostic accuracy. However, enough raw data were presented to enable the calculation of diagnostic accuracy outcomes as required for inclusion in this review.
The applicability of this study to the population for the research question is limited because the study recruited only male patients and did not identify the prior tests that led them to be referred for angiography. The study is considered to be of medium quality, as it was not designed as a study of diagnostic accuracy. In addition, the study was potentially affected by selection bias. Nineteen per cent of patients initially recruited had inadequate pressure tracings using SphygmoCor and were not included in the final analysis. Therefore, the study population does not present a consecutive series of patients based on presenting symptoms.
Table 13 Characteristics of the included SphygmoCor study Authors (year) and country
Study design Patients (N)
SphygmoCor characteristics
Coronary angiography characteristics
Study quality
Weber (2004) Austria
Prospective, blinded study evaluating relationship between CAD and AIx
Consecutive male patients undergoing coronary angiography for the diagnosis or exclusion of CAD (465)
20 sequential radial artery waveforms acquired, normalisation to HR 75 bpm
Cathcor, Siemens, Judkins technique ≥ 3 highly experienced angiographers (> 5000 procedures each)
P2, Q2 Applicability: limited; males only, prior tests not reported Quality: medium; wrong outcomes reported; selection bias, test failures excluded
Abbreviations: bpm, beats per minute; CAD, coronary artery disease; AIx, augmentation index; HR, heart rate; PWA, pulse wave analysis.
Table 14 shows the calculated AIx strata-specific likelihood ratios for the presence of CAD. These data demonstrate the likelihood of the presence of CAD for a patient with an AIx in the given range. The data indicate that there is an increase in the likelihood ratio of the test as the AIx increases; however, the range of likelihood ratios across the strata is small. The spread of the likelihood ratios across the range of AIx increased when data from patients aged up to 60 years only was examined. However, the applicability of this patient group is limited.

SphygmoCor system 37
The highest likelihood ratio for this measure was in patients with an AIx of greater than or equal to 29 (likelihood ratio = 2.0 for all patients; likelihood ratio = 3.3 for patients aged less than 60 years). The lowest likelihood ratio was for an AIx of less than or equal to 9 per cent (likelihood ratio = 0.5 for all patients, likelihood ratio = 0.4 for patients aged less than 60 years). These likelihood ratios indicate that the test measure does not provide strong diagnostic accuracy information for the presence of CAD.
Table 14 Likelihood ratios for the presence of coronary artery disease for different AIx values
Aix (%)
Total patients (N)
CAD (n)
No CAD (n)
Likelihood ratio
Total patient population –24–9 73 56 17 0.48 10–21 145 125 20 0.91 22–28 131 117 14 1.21 29–60 116 108 8 1.96 Patients < 60 years –17–9 35 20 15 0.40 10–21 52 37 15 0.74 22–28 55 45 10 1.36 29–60 48 44 4 3.32
Abbreviations: AIx, augmentation index; CAD, coronary artery disease. Source: Data calculated from Weber et al (2004).
Table 15 shows the diagnostic accuracy of SphygmoCor for CAD, calculated by dichotomising the AIx according to different thresholds for diagnosis. These data confirm that the overall accuracy of the AIx for the diagnosis of CAD is low. A diagnostic odds ratio less than ten indicates that this test is poor at discriminating between the presence and absence of disease (Medical Services Advisory Committee, 2004). The highest sensitivity of the test measure for the diagnosis of CAD (86%) is seen when an AIx threshold for a positive test of greater than or equal to 10 is used. Given the potential management and clinical consequences of a negative test result in a patient with CAD (ie, delaying or avoiding angiography and, possibly, appropriate treatment), this sensitivity is considered to be low. In addition, at this threshold, the specificity of the test is very low (29% in the total population, 34% in patients aged less than 60 years). That is, a large proportion of patients without disease would be classified as having CAD.
The value of the AIx test measure for the diagnosis of CAD in the study by (Weber et al 2004) is considered to be low.
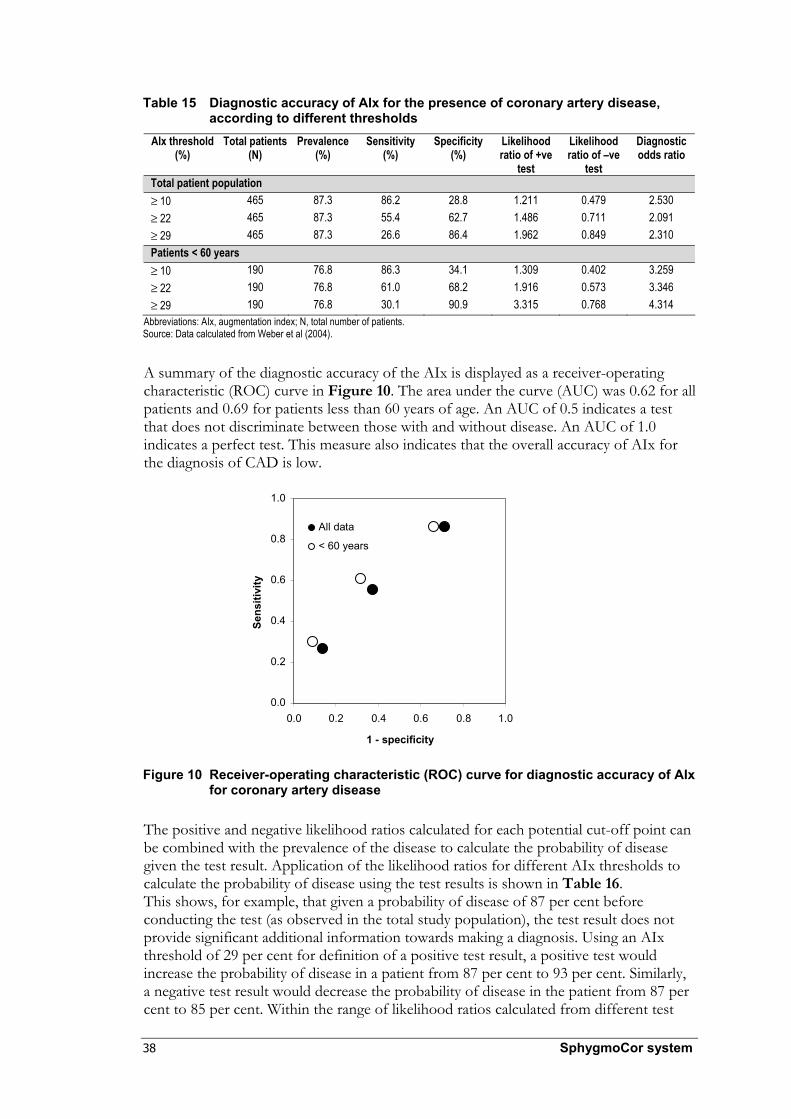
38 SphygmoCor system
Table 15 Diagnostic accuracy of AIx for the presence of coronary artery disease,
according to different thresholds
AIx threshold (%)
Total patients (N)
Prevalence (%)
Sensitivity (%)
Specificity (%)
Likelihood ratio of +ve
test
Likelihood ratio of –ve
test
Diagnostic odds ratio
Total patient population ≥ 10 465 87.3 86.2 28.8 1.211 0.479 2.530 ≥ 22 465 87.3 55.4 62.7 1.486 0.711 2.091 ≥ 29 465 87.3 26.6 86.4 1.962 0.849 2.310 Patients < 60 years ≥ 10 190 76.8 86.3 34.1 1.309 0.402 3.259 ≥ 22 190 76.8 61.0 68.2 1.916 0.573 3.346 ≥ 29 190 76.8 30.1 90.9 3.315 0.768 4.314
Abbreviations: AIx, augmentation index; N, total number of patients. Source: Data calculated from Weber et al (2004).
A summary of the diagnostic accuracy of the AIx is displayed as a receiver-operating characteristic (ROC) curve in Figure 10. The area under the curve (AUC) was 0.62 for all patients and 0.69 for patients less than 60 years of age. An AUC of 0.5 indicates a test that does not discriminate between those with and without disease. An AUC of 1.0 indicates a perfect test. This measure also indicates that the overall accuracy of AIx for the diagnosis of CAD is low.
Figure 10 Receiver-operating characteristic (ROC) curve for diagnostic accuracy of AIx for coronary artery disease
The positive and negative likelihood ratios calculated for each potential cut-off point can be combined with the prevalence of the disease to calculate the probability of disease given the test result. Application of the likelihood ratios for different AIx thresholds to calculate the probability of disease using the test results is shown in Table 16. This shows, for example, that given a probability of disease of 87 per cent before conducting the test (as observed in the total study population), the test result does not provide significant additional information towards making a diagnosis. Using an AIx threshold of 29 per cent for definition of a positive test result, a positive test would increase the probability of disease in a patient from 87 per cent to 93 per cent. Similarly, a negative test result would decrease the probability of disease in the patient from 87 per cent to 85 per cent. Within the range of likelihood ratios calculated from different test
0.0
0.2
0.4
0.6
0.8
1.0
0.0 0.2 0.4 0.6 0.8 1.0
1 - specificity
Sens
itivi
ty
All data
< 60 years
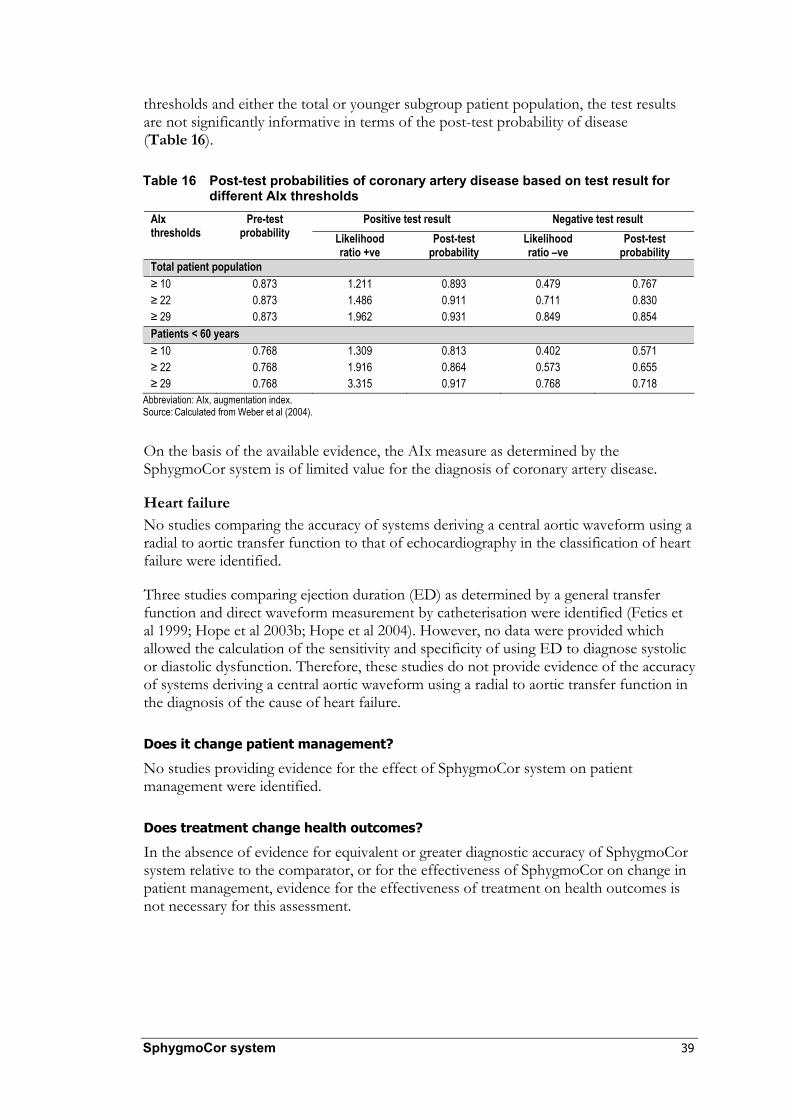
SphygmoCor system 39
thresholds and either the total or younger subgroup patient population, the test results are not significantly informative in terms of the post-test probability of disease (Table 16).
Table 16 Post-test probabilities of coronary artery disease based on test result for different AIx thresholds
Abbreviation: AIx, augmentation index. Source: Calculated from Weber et al (2004).
On the basis of the available evidence, the AIx measure as determined by the SphygmoCor system is of limited value for the diagnosis of coronary artery disease.
Heart failure No studies comparing the accuracy of systems deriving a central aortic waveform using a radial to aortic transfer function to that of echocardiography in the classification of heart failure were identified.
Three studies comparing ejection duration (ED) as determined by a general transfer function and direct waveform measurement by catheterisation were identified (Fetics et al 1999; Hope et al 2003b; Hope et al 2004). However, no data were provided which allowed the calculation of the sensitivity and specificity of using ED to diagnose systolic or diastolic dysfunction. Therefore, these studies do not provide evidence of the accuracy of systems deriving a central aortic waveform using a radial to aortic transfer function in the diagnosis of the cause of heart failure.
Does it change patient management?
No studies providing evidence for the effect of SphygmoCor system on patient management were identified.
Does treatment change health outcomes?
In the absence of evidence for equivalent or greater diagnostic accuracy of SphygmoCor system relative to the comparator, or for the effectiveness of SphygmoCor on change in patient management, evidence for the effectiveness of treatment on health outcomes is not necessary for this assessment.
Positive test result Negative test result AIx thresholds
Pre-test probability Likelihood
ratio +ve Post-test
probability Likelihood ratio –ve
Post-test probability
Total patient population ≥ 10 0.873 1.211 0.893 0.479 0.767 ≥ 22 0.873 1.486 0.911 0.711 0.830 ≥ 29 0.873 1.962 0.931 0.849 0.854 Patients < 60 years ≥ 10 0.768 1.309 0.813 0.402 0.571 ≥ 22 0.768 1.916 0.864 0.573 0.655 ≥ 29 0.768 3.315 0.917 0.768 0.718

40 SphygmoCor system
Conclusions
Safety
The SphygmoCor system is a non-invasive test and therefore there are no adverse events associated with its use.
Effectiveness
Diagnostic accuracy
No studies providing evidence for the accuracy of the SphygmoCor system for the diagnosis of hypertension or white coat hypertension were identified.
No studies providing evidence for the accuracy of the SphygmoCor system for the diagnosis of spurious systolic hypertension of youth were identified. A more detailed analysis in this area did not yield persuasive evidence to support the ability of the SphygmoCor system to accurately diagnose spurious systolic hypertension of youth.
One single study was identified that provided evidence for diagnostic accuracy of the SphygmoCor system for the diagnosis of CAD. On the basis of this evidence, the AIx measure as determined by the SphygmoCor system was recognised as having limited value for the diagnosis of CAD.
No studies providing evidence for the diagnostic accuracy of the SphygmoCor system for the diagnosis of heart failure were identified.
Impact on patient management
No studies providing evidence for the effect of SphygmoCor system on patient management were identified.
Impact on health outcomes
There was no evidence of equivalent or improved diagnostic accuracy using the SphygmoCor system relative to using the comparators or of changes to patient management.

SphygmoCor system 41
Cost-effectiveness
As clinical effectiveness was not demonstrated, no cost-effectiveness analysis was undertaken.
MBS reimbursement was sought for the combined costs of the technology and the corresponding consultation. The technology and consultation costs of the device as supplied by the applicant are shown in Table 17. The applicant estimated the cost per service of the device would be $105.26.
Table 17 Direct and Indirect costs for use of the SphygmoCor system
Description Costs Technology costs SphygmoCor system $22,000 Dedicated computer $3300 Consumables $1650a
Service and support contract $1650a
Consultation costs Physician $104.56b
Clinic staff $104.56b
Overheads $104.56b
a These refer to yearly recurrent costs. b These refer to hourly costs.

42 SphygmoCor system
Recommendation
Since there is currently insufficient evidence pertaining to peripheral arterial tonometry with ascending aortic waveform analysis using the SphygmoCor system, MSAC recommended that public funding should not be supported at this time for this procedure.
– The Minister for Health and Ageing accepted this recommendation on 6 June 2006. –

SphygmoCor system 43
Appendix A MSAC terms of reference and membership
MSAC’s terms of reference are to:
• advise the Minister for Health and Ageing on the strength of evidence pertaining to new and emerging medical technologies and procedures in relation to their safety, accuracy, effectiveness and cost-effectiveness and under what circumstances public funding should be supported;
• advise the Minister for Health and Ageing on which new medical technologies and procedures should be funded on an interim basis to allow data to be assembled to determine their safety, effectiveness and cost-effectiveness;
• advise the Minister for Health and Ageing on references related either to new and/or existing medical technologies and procedures; and
• undertake health technology assessment work referred by the Australian Health Ministers’ Advisory Council (AHMAC) and report its findings to AHMAC.
The membership of the MSAC comprises a mix of clinical expertise covering pathology, nuclear medicine, surgery, specialist medicine and general practice, plus clinical epidemiology and clinical trials, health economics, consumers, and health administration and planning:
Member Expertise or affiliation Dr Stephen Blamey (Chair) general surgery
Associate Professor John Atherton cardiology
Professor Syd Bell pathology
Dr Michael Cleary emergency medicine
Dr Paul Craft clinical epidemiology and oncology
Dr Mary Turner Australian Health Ministers’ Advisory Council representative
Dr Kwun Fong thoracic medicine
Dr Debra Graves medical administrator
Professor Jane Hall health economics
Professor John Horvath Chief Medical Officer, Department of Health and Ageing
Ms Samantha Robertson Department of Health and Ageing representative
Dr Terri Jackson health economics
Professor Brendon Kearney health administration and planning
Associate Professor Donald Perry-Keene endocrinology
Dr Ray Kirk health research
Dr David Gillespie gastroenterology

44 SphygmoCor system
Member Expertise or affiliation Dr Ewa Piejko general practice
Ms Sheila Rimmer consumer health issues
Dr David Wood orthopaedic surgery
Professor Frederick Khafagi nuclear medicine
Professor Ken Thomson radiology
Dr Douglas Travis urology

SphygmoCor system 45
Appendix B Advisory Panel
Advisory Panel for MSAC application 1079 SphygmoCor system
Dr Michael Cleary (Chair) FACEM, MHA Executive Director of Medical Services The Prince Charles Hospital Chermside, Qld
Member of MSAC
Professor Leonard Arnolda PhD, FRACP Department of Cardiology Royal Perth Hospital, Perth, WA
Nominated by the Cardiac Society of Australia and New Zealand
Dr Peter Blombery MBBS, PhD, FRACP, DDU Heart Centre Alfred Hospital, Prahran, Vic
Nominated by the Royal Australian College of Surgeons, Vascular Society
Dr Rod Lane MD, FRACS Vascular Surgeon, Castlecrag, NSW
Nominated by the Royal Australian College of Surgeons, Vascular Society
Mr Richard McCluskey Heart Support Australia Independent Consumer Representative Latham, ACT
Nominated by the Consumers’ Health Forum
Professor Jeffrey Robinson FRCOG, FRACOG Department of Obstetrics & Gynaecology Women’s and Children’s Hospital University of Adelaide North Adelaide, SA
Member of MSAC
Evaluators for MSAC application 1079
Dr Suzanne Dyer BSc(Hons) PhD GradCertPH
M-TAG Pty Ltd, A unit of IMS Health
Mr Marc Bevan BSc(Hons)
M-TAG Pty Ltd, A unit of IMS Health
Ms Jolie Hutchinson BSc(Hons)
M-TAG Pty Ltd, A unit of IMS Health
Members from the Department of Health and Ageing for MSAC application 1079
Ms Brenda Campe Project Manager
Health Technology Section Medicare Benefits Branch
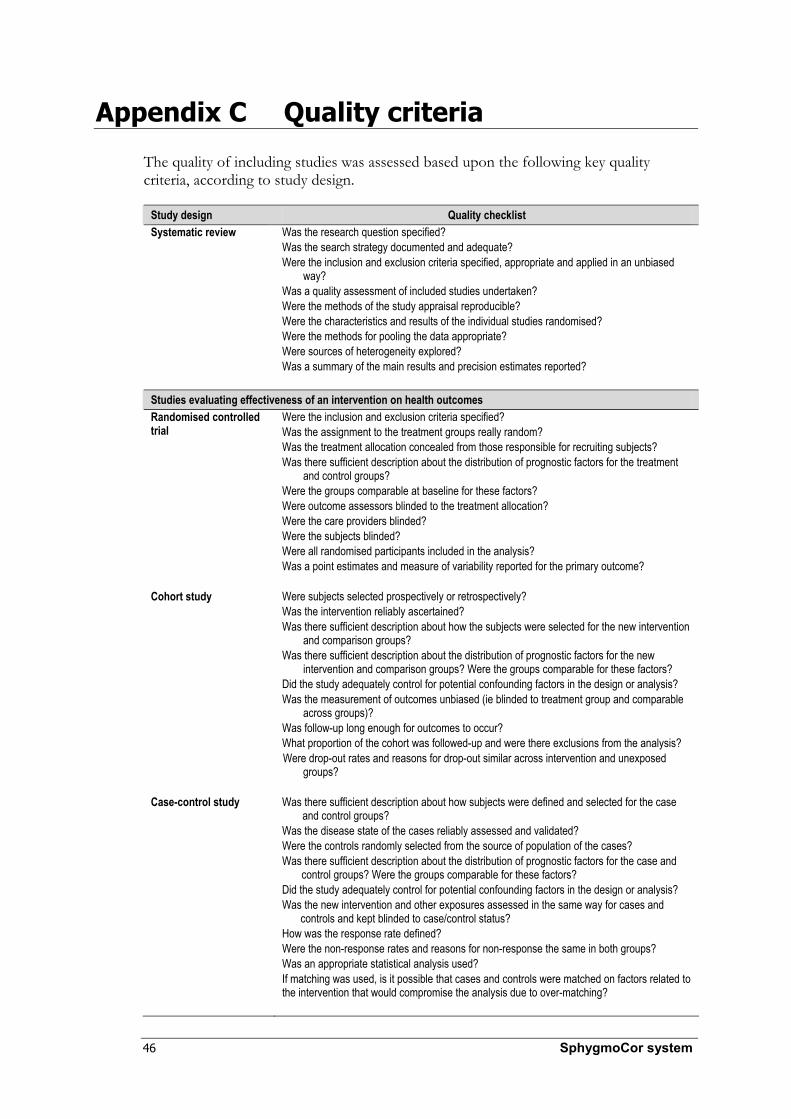
46 SphygmoCor system
Appendix C Quality criteria
The quality of including studies was assessed based upon the following key quality criteria, according to study design.
Study design Quality checklist Systematic review Was the research question specified?
Was the search strategy documented and adequate? Were the inclusion and exclusion criteria specified, appropriate and applied in an unbiased
way? Was a quality assessment of included studies undertaken? Were the methods of the study appraisal reproducible? Were the characteristics and results of the individual studies randomised? Were the methods for pooling the data appropriate? Were sources of heterogeneity explored? Was a summary of the main results and precision estimates reported?
Studies evaluating effectiveness of an intervention on health outcomes Randomised controlled trial
Were the inclusion and exclusion criteria specified? Was the assignment to the treatment groups really random? Was the treatment allocation concealed from those responsible for recruiting subjects? Was there sufficient description about the distribution of prognostic factors for the treatment
and control groups? Were the groups comparable at baseline for these factors? Were outcome assessors blinded to the treatment allocation? Were the care providers blinded? Were the subjects blinded? Were all randomised participants included in the analysis? Was a point estimates and measure of variability reported for the primary outcome?
Cohort study Were subjects selected prospectively or retrospectively? Was the intervention reliably ascertained? Was there sufficient description about how the subjects were selected for the new intervention
and comparison groups? Was there sufficient description about the distribution of prognostic factors for the new
intervention and comparison groups? Were the groups comparable for these factors? Did the study adequately control for potential confounding factors in the design or analysis? Was the measurement of outcomes unbiased (ie blinded to treatment group and comparable
across groups)? Was follow-up long enough for outcomes to occur? What proportion of the cohort was followed-up and were there exclusions from the analysis? Were drop-out rates and reasons for drop-out similar across intervention and unexposed
groups?
Case-control study Was there sufficient description about how subjects were defined and selected for the case and control groups?
Was the disease state of the cases reliably assessed and validated? Were the controls randomly selected from the source of population of the cases? Was there sufficient description about the distribution of prognostic factors for the case and
control groups? Were the groups comparable for these factors? Did the study adequately control for potential confounding factors in the design or analysis? Was the new intervention and other exposures assessed in the same way for cases and
controls and kept blinded to case/control status? How was the response rate defined? Were the non-response rates and reasons for non-response the same in both groups? Was an appropriate statistical analysis used? If matching was used, is it possible that cases and controls were matched on factors related to the intervention that would compromise the analysis due to over-matching?

SphygmoCor system 47
Case series Was the study based on a representative sample selected from a relevant population? Were the criteria for inclusion and exclusion explicit? Did all subjects enter the survey at a similar point in their disease progression? Was follow-up long enough for important events to occur? Were the techniques used adequately described? Were outcomes assessed using objective criteria or was blinding used? If comparisons of sub-series were made, were there sufficient description of the series and the
distribution of prognostic factors?
Study of diagnostic accuracy
Was the spectrum of patients representative of the patients who will receive the test in practice?
Were selection criteria clearly described? Is the reference standard likely to correctly classify the target condition? Is the time period between reference standard and index test short enough to be reasonably
sure that the target condition did not change between the two tests? Did the whole sample or a random selection of the sample, receive verification using a
reference standard of diagnosis? Did patients receive the same reference standard regardless of the index test result? Was the reference standard independent of the index test (ie the index test did not form part
of the reference standard)? Was the execution of the index test described in sufficient detail to permit replication of the
test? Was the execution of the reference standard described in sufficient detail to permit its
replication? Were the index test results interpreted without knowledge of the results of the reference
standard? Were the reference standards results interpreted without knowledge of the results of the index
test? Were the same clinical data available when test results were interpreted as would be available
when the test is used in practice? Were uninterpretable/ intermediate test results reported? Were withdrawals from the study explained?
Sources: How to use the evidence: assessment and application of scientific evidence. NHMRC (2000). Undertaking systematic reviews of research on effectiveness. NHS Centre for Reviews and Dissemination, (2001). QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. Whiting et al (2003).

48 SphygmoCor system
Appendix D Literature search strategies
Medline search strategy
The search strategy used to identify relevant studies of the SphygmoCor system in Medline is presented in Table 18.
Table 18 SphygmoCor system Medline search strategy (1966 to August Week 1, 2005) Keywords / search history Results 1. (sphygmocor or sphygmo cor or sphygmocardiograph$).ti,ab. 45 2. (finapres$1 or portapres$1 or cardiopres$1).ti,ab. 654 3. transfer function$1.ti,ab. 2704 4. mathematical transformation.ti,ab. 62 5. (pwa or pulse wave$ analys#s).ti,ab. 257 6. (augmentation index or aix or agix).ti,ab. 366 7. (arterial adj3 tonomet$).ti,ab. 143 8. or/2-7 4038 9. 8 and exp aorta/ 185 10. 8 and aort$.ti,ab. 318 11. 8 and exp arteries/ 546 12. 8 and arter$.ti,ab. 1079 13. 11 or 12 1148 14. 13 and (central or aort$ or carotid).ti,ab. 471 15. or/1,9-10,14 504
EMBASE search strategy
The search strategy used to identify relevant studies of the SphygmoCor system in EMBASE is presented in Table 19.
Table 19 SphygmoCor system EMBASE search strategy (1980 to Week 33, 2005) Keywords / search history Results 1. (sphygmocor or sphygmo cor or sphygmocardiograph$).ti,ab. 44 2. (finapres$1 or portapres$1 or cardiopres$1).ti,ab,dv,tn. 712 3. transfer function technique/ 1 4. transfer function$1.ti,ab. 2500 5. mathematical transformation.ti,ab. 65 6. (pwa or pulse wave$ analys#s).ti,ab. 239 7. (augmentation index or aix or agix).ti,ab. 344 8. (arterial adj3 tonomet$).ti,ab. 157 9. or/2-8 3863 10. 9 and exp aorta/ 99 11. 9 and aorta pressure/ 124 12. 9 and aort$.ti,ab. 311 13. 9 and exp artery/ 385 14. 9 and exp arterial pressure/ 566 15. 9 and arter$.ti,ab. 1083 16. or/13-15 1143 17. 16 and (central or aort$ or carotid).ti,ab. 452 18. (sphygmocor or sphygmo cor).dv,tn. 43 19. or/1,10-12,17-18 516

SphygmoCor system 49
PreMedline search strategy
The search strategy used to identify relevant studies of the SphygmoCor system in PreMedline is presented in Table 20.
Table 20 SphygmoCor system PreMedline search strategy (17 August, 2005) Keywords / search history Results 1. (sphygmocor or sphygmo cor or sphygmocardiograph$).ti,ab. 6 2. (finapres$1 or portapres$1 or cardiopres$1).ti,ab. 16 3. transfer function$1.ti,ab. 173 4. mathematical transformation.ti,ab. 5 5. (pwa or pulse wave$ analys#s).ti,ab. 16 6. (augmentation index or aix or agix).ti,ab. 24 7. (arterial adj3 tonomet$).ti,ab. 4 8. or/2-7 231 9. 8 and aort$.ti,ab. 16 10. 8 and arter$.ti,ab. 50 11. 10 and (central or aort$ or carotid).ti,ab. 24 12. or/1,9,11 28
Cochrane Library search strategy
The search strategy used to identify relevant studies of the SphygmoCor system in the Cochrane Library is presented in Table 21.
Table 21 SphygmoCor system Cochrane Library search strategy (Issue 3, 2005) Keywords / search history Results 1. sphygmocor or "sphygmo cor" or sphygmocardiograph* 11 2. finapres* or portapres* or cardiopres* 112 3. "transfer function" or "transfer functions" 39 4. "mathematical transformation" 3 5. pwa or “pulse wave” or “pulse waveform” 197 6. “augmentation index” or aix or agix 62 7. arterial near tonomet* 26 8. #2 or #3 or #4 or #5 or #6 or #7 382 9. aorta [explode this MeSH term] 515 10. aort* 3254 11. #9 or #10 3255 12. #8 and #11 88 13. arteries [explode this MeSH term] 3947 14. arter* 28893 15. #13 or #14 29303 16. central or aort* or carotid 458293 17. #8 and #15 and #16 249 18. #1 or #12 or #17 255

50 SphygmoCor system
Appendix E Spurious systolic hypertension of youth
One study conducted in an appropriate population was identified that reported measurement of waveform parameters using the SphygmoCor system, but without reference standard validation. This study did not report appropriate outcomes for the determination of diagnostic accuracy for spurious systolic hypertension of youth, but was included for review in the absence of any other studies. This study reported brachial cuff and derived aortic blood pressures in a population of young healthy individuals. The characteristics of this study are shown in Table 22.
Table 22 Characteristics of the included study of the SphygmoCor system in spurious systolic hypertension of youth
Author (year) Country
Study design Population (N) System and transfer function characteristics
Study quality
Mahmud & Feely (2003) Ireland
Case control study reporting SphygmoCor system measurements
Medical students aged 23 ± 0.5 years (174) Untreated male patients with essential hypertension (22)
SphygmoCor Radial artery waveforms acquired by applanation tomography calibrated to oscillometric cuff blood pressure (Omron model HEM-705 CP)
P1, Q3 Applicability: applicable Quality: low Wrong outcomes reported; no reference standard
Note: See also Appendix G
In a group of 174 healthy young medical students of both sexes, Mahmud and Feely (2003) identified a subset of subjects with elevated brachial systolic blood pressure (SBP). The characteristics of these individuals were compared with those who were normotensive or had essential hypertension. Those with spurious systolic hypertension of youth were all male. They also showed specific significant differences compared with the rest of the population: they were taller and had a decreased heart rate, all were non-smokers and all participated in active sports. The SphygmoCor system also identified differences in the derived aortic waveform characteristics between these three groups of subjects. The findings for males in these groups are shown in Table 23.
Table 23 Characteristics of male subjects with spurious systolic hypertension of youth, normotension or essential hypertension
Characteristic
Spurious systolic hypertension of youth
Mean (SD) (n = 11)
Normotensive Mean (SD) (n = 76)
Essential hypertensive Mean (SD) (n = 22)
Age 23.5 (0.9) 22 (0.5) 24.8 (0.9) Brachial SBP (mmHg) 147.3 (2)a 120.5 (1.3) 152 (2.6) Brachial DBP (mmHg) 70 (2.2)b 69.9 (1) 96.5 (1.4) Aortic SBP (mmHg) 115.9 (1)a,b 100 (1.5) 138.8 (2.5) Aortic DBP (mmHg) 70 (2.5)b 71 (1) 98 (1.4) Heart rate (bpm) 61.1 (1.9)a,b 68.3 (1.65) 72.4 (3.2) PP amplification (mmHg) 31.4 (1.5)a,b 20.5 (1.36) 14 (0.9) AIx (%) –8 (3)b –4 (1.4) 17 (1.9) Tr (msec) 160 (8)b 152 (2.3) 142 (1.6) Abbreviations: AIx, augmentation index; bpm, beats per minute; DBP, diastolic blood pressure; PP, pulse pressure; SBP, systolic blood pressure; SD, standard deviation; Tr, time to reflected wave. a Compared with normotensive males (p < 0.01). b Compared with hypertensive males (p < 0.01).
SphygmoCor system 51
The pulse pressure amplification that occurred between the aorta and the brachial artery in the spurious systolic hypertension of youth subjects was significantly greater than in both normotensive and hypertensive men. The spurious systolic hypertension of youth subjects also had significantly lower aortic SBP and a longer time to wave reflection (Tr) than the essential hypertensive subjects. The AIx of the spurious systolic hypertension of youth subjects was also significantly less than that of the essential hypertensive population.
Six patients with spurious systolic hypertension of youth repeated the assessment two years later with an echocardiogram. At this time, these individuals still had elevated brachial SBP and normal aortic SBP as derived using the SphygmoCor system.
The data from Mahmud and Feely (2003) did not allow calculation of the sensitivity and specificity of the measures determined by SphygmoCor in the diagnosis of spurious systolic hypertension of youth.
Therefore, the best evidence for diagnosis of spurious systolic hypertension of youth was the accuracy of derived central aortic blood pressure measurements to estimate the aortic blood pressure (as determined by an transducer-tipped catheter or fluid filled catheter with appropriate calibration located in the aorta) compared to upper limb brachial/radial blood pressure.
Ten publications were identified that compared the measurement of derived central blood pressure with upper limb brachial/radial blood pressure in patients undergoing an invasive cardiovascular procedure. These publications were not in the appropriate patient group but were included for review in the absence of other suitable publications.

52 SphygmoCor system
Tabl
e 24
C
hara
cter
istic
s of
the
incl
uded
stu
dies
repo
rtin
g th
e te
chni
cal v
alid
atio
n of
mea
sure
s of
spu
rious
sys
tolic
hyp
erte
nsio
n of
you
th
Auth
or (y
ear)
Coun
try
Stud
y des
ign
Popu
latio
n (N
) Sy
stem
and
trans
fer f
unct
ion
Com
para
tor
Refe
renc
e sta
ndar
d
Chen
(199
7)
Unite
d Stat
es of
Am
erica
Stud
y eva
luatin
g ma
thema
tical
trans
forma
tion o
f ra
dial w
avefo
rm
data
Non-
cons
ecuti
ve pa
tients
un
derg
oing c
ardia
c ca
theter
isatio
n (20
)
ARX
Mode
l TF
Autom
ated t
onom
eter (
Jento
w,
Colin
Med
ical In
strum
ents
Corp
) SB
P ca
libra
tion c
uff B
P; D
BP an
d MA
P ca
libra
tion i
nvas
ive ao
rtic
Untra
nsfor
med r
adial
wav
eform
(Je
ntow
tonom
eter)
SBP
calib
ratio
n auto
mated
cuff B
P (Je
ntow,
Coli
n Med
ical In
strum
ents
Corp
); DB
P an
d MAP
calib
ratio
n inv
asive
aortic
Osc
illome
tric cu
ff
Micro
mano
meter
-tippe
d cath
eter (
Milla
r SP
C 32
0) or
micr
oman
omete
r-tipp
ed m
ulti-
electr
ode p
ress
ure-
volum
e cath
eter (
Milla
r SS
D 76
8)
Asce
nding
aorta
Clou
d (20
03)
Unite
d King
dom
Stud
y eva
luatin
g the
use o
f non
-inv
asive
calib
ratio
n for
the
Sphy
gmoC
or
syste
m
Non-
cons
ecuti
ve pa
tients
with
an
ginal
symp
toms u
nder
going
ca
rdiac
cathe
terisa
tion (
30)
Sphy
gmoC
or sy
stem
RA to
nome
try
Calib
rated
, bra
chial
cuff B
P
Autom
atic o
scillo
metric
digit
al BP
mo
nitor
(Omr
on, H
EM-7
0 CP)
Om
ron H
EM-7
0 CP
syste
m
Reco
rded
imme
diatel
y befo
re
tonom
etry
Fluid-
filled
cathe
ter (C
ordis
6F pi
gtail
cathe
ter)
Marq
uette
Mida
s Sys
tem 40
00
Aortic
loca
tion N
R
Davie
s (20
03)
Unite
d King
dom
Pros
pecti
ve st
udy
comp
aring
ca
lculat
ed ao
rtic
with
perip
hera
l blo
od pr
essu
re
meas
urem
ents
Non-
cons
ecuti
ve pa
tients
un
derg
oing c
ardia
c ca
theter
isatio
n with
easil
y pa
lpated
left R
A; ex
cludin
g pa
tients
with
a his
tory o
f br
achia
l or s
ubcla
vian s
tenos
is (2
8)
Sphy
gmoC
or sy
stem
RA to
nome
try
Calib
ratio
n, br
achia
l cuff
BP
Oscil
lometr
ic br
achia
l cuff
(Omr
on
HEM-
705 C
P) sy
stem
Reco
rded
imme
diatel
y befo
re
tonom
etry
Cathe
ter w
ith T
rans
pac I
V mo
nitor
ing ki
t (A
bbott
Criti
cal C
are S
ystem
s, Ab
bott
Labo
rator
ies)a
Siem
ens R
ecor
V6 s
ystem
As
cend
ing ao
rta
Fetic
s (19
99)
Unite
d Stat
es of
Am
erica
Stud
y eva
luatin
g ma
thema
tical
trans
forma
tion o
f ra
dial w
avefo
rm
data
Non-
cons
ecuti
ve pa
tients
un
derg
oing d
iagno
stic c
ardia
c ca
theter
isatio
n (39
)
ARX
Mode
l Au
tomate
d ton
omete
r (Je
ntow,
Co
lin M
edica
l Instr
umen
ts Co
rp),
analo
gue f
iltere
d at 3
0 Hz
SBP
calib
ratio
n cuff
BP;
DBP
and
MAP
calib
ratio
n inv
asive
aortic
Untra
nsfor
med r
adial
wav
eform
(Je
ntow
tonom
eter)
SBP
calib
ratio
n, au
tomate
d cuff
BP
(Jento
w, C
olin M
edica
l Instr
umen
ts Co
rp);
DBP
and M
AP ca
libra
tion,
invas
ive ao
rtic
Micro
mano
meter
-tippe
d cath
eter (
Milla
r SP
C 32
0)
Asce
nding
aorta
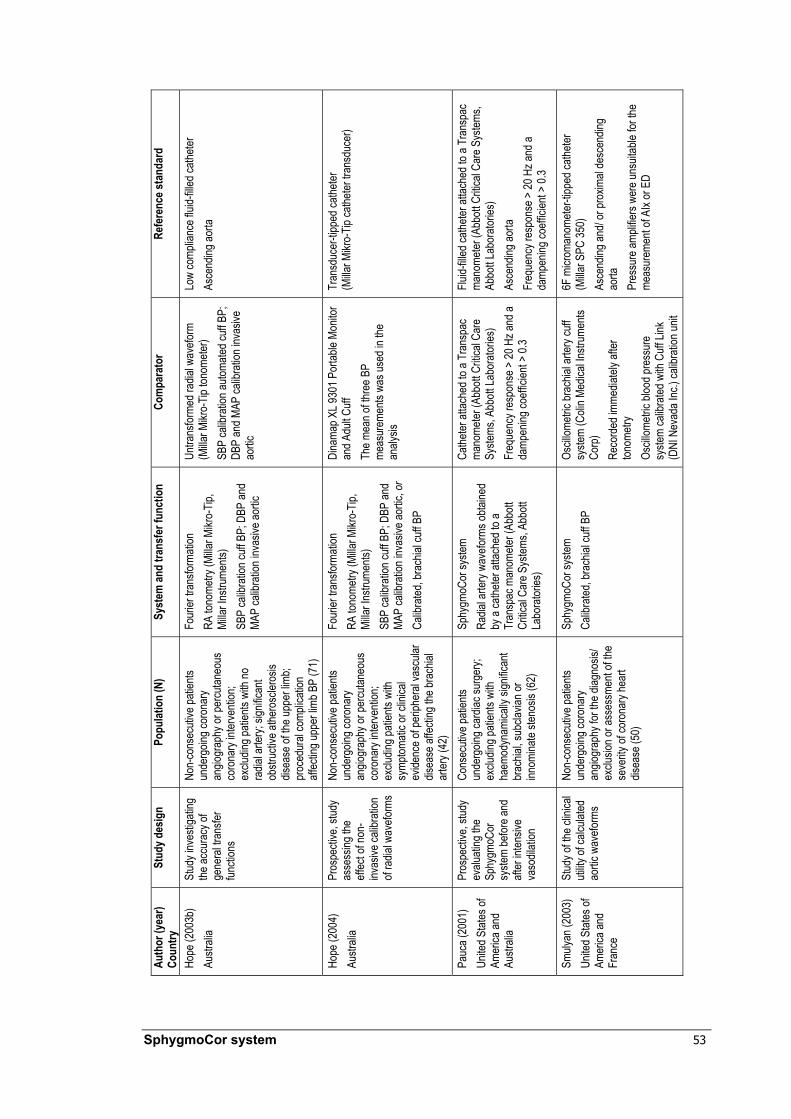
SphygmoCor system 53
Auth
or (y
ear)
Coun
try
Stud
y des
ign
Popu
latio
n (N
) Sy
stem
and
trans
fer f
unct
ion
Com
para
tor
Refe
renc
e sta
ndar
d
Hope
(200
3b)
Austr
alia
Stud
y inv
estig
ating
the
accu
racy
of
gene
ral tr
ansfe
r fun
ction
s
Non-
cons
ecuti
ve pa
tients
un
derg
oing c
oron
ary
angio
grap
hy or
percu
taneo
us
coro
nary
inter
venti
on;
exclu
ding p
atien
ts wi
th no
ra
dial a
rtery;
sign
ifican
t ob
struc
tive a
thero
scler
osis
disea
se of
the u
pper
limb;
proc
edur
al co
mplic
ation
aff
ectin
g upp
er lim
b BP
(71)
Four
ier tr
ansfo
rmati
on
RA to
nome
try (M
illar M
ikro-
Tip,
Milla
r Ins
trume
nts)
SBP
calib
ratio
n cuff
BP;
DBP
and
MAP
calib
ratio
n inv
asive
aortic
Untra
nsfor
med r
adial
wav
eform
(M
illar M
ikro-
Tip to
nome
ter)
SBP
calib
ratio
n auto
mated
cuff B
P;
DBP
and M
AP ca
libra
tion i
nvas
ive
aortic
Low
comp
lianc
e flui
d-fill
ed ca
theter
As
cend
ing ao
rta
Hope
(200
4)
Austr
alia
Pros
pecti
ve, s
tudy
asse
ssing
the
effec
t of n
on-
invas
ive ca
libra
tion
of ra
dial w
avefo
rms
Non-
cons
ecuti
ve pa
tients
un
derg
oing c
oron
ary
angio
grap
hy or
percu
taneo
us
coro
nary
inter
venti
on;
exclu
ding p
atien
ts wi
th sy
mptom
atic o
r clin
ical
evide
nce o
f per
ipher
al va
scula
r dis
ease
affec
ting t
he br
achia
l ar
tery (
42)
Four
ier tr
ansfo
rmati
on
RA to
nome
try (M
illar M
ikro-
Tip,
Milla
r Ins
trume
nts)
SBP
calib
ratio
n cuff
BP;
DBP
and
MAP
calib
ratio
n inv
asive
aortic
, or
Calib
rated
, bra
chial
cuff B
P
Dina
map X
L 930
1 Por
table
Monit
or
and A
dult C
uff
The m
ean o
f thre
e BP
meas
urem
ents
was u
sed i
n the
an
alysis
Tran
sduc
er-tip
ped c
athete
r (M
illar M
ikro-
Tip ca
theter
tran
sduc
er)
Pauc
a (20
01)
Unite
d Stat
es of
Am
erica
and
Austr
alia
Pros
pecti
ve, s
tudy
evalu
ating
the
Sphy
gmoC
or
syste
m be
fore a
nd
after
inten
sive
vaso
dilati
on
Cons
ecuti
ve pa
tients
un
derg
oing c
ardia
c sur
gery;
ex
cludin
g pati
ents
with
haem
odyn
amica
lly si
gnific
ant
brac
hial, s
ubcla
vian o
r inn
omina
te ste
nosis
(62)
Sphy
gmoC
or sy
stem
Radia
l arte
ry wa
vefor
ms ob
taine
d by
a ca
theter
attac
hed t
o a
Tran
spac
man
omete
r (Ab
bott
Critic
al Ca
re S
ystem
s, Ab
bott
Labo
rator
ies)
Cathe
ter at
tache
d to a
Tra
nspa
c ma
nome
ter (A
bbott
Criti
cal C
are
Syste
ms, A
bbott
Labo
rator
ies)
Freq
uenc
y res
pons
e > 20
Hz a
nd a
damp
ening
coeff
icien
t > 0.
3
Fluid-
filled
cathe
ter at
tache
d to a
Tra
nspa
c ma
nome
ter (A
bbott
Criti
cal C
are S
ystem
s, Ab
bott L
abor
atorie
s) As
cend
ing ao
rta
Freq
uenc
y res
pons
e > 20
Hz a
nd a
damp
ening
coeff
icien
t > 0.
3
Smuly
an (2
003)
Un
ited S
tates
of
Amer
ica an
d Fr
ance
Stud
y of th
e clin
ical
utility
of ca
lculat
ed
aortic
wav
eform
s
Non-
cons
ecuti
ve pa
tients
un
derg
oing c
oron
ary
angio
grap
hy fo
r the
diag
nosis
/ ex
clusio
n or a
sses
smen
t of th
e se
verity
of co
rona
ry he
art
disea
se (5
0)
Sphy
gmoC
or sy
stem
Calib
rated
, bra
chial
cuff B
P Os
cillom
etric
brac
hial a
rtery
cuff
syste
m (C
olin M
edica
l Instr
umen
ts Co
rp)
Reco
rded
imme
diatel
y afte
r ton
ometr
y Os
cillom
etric
blood
pres
sure
sy
stem
calib
rated
with
Cuff
Link
(D
NI N
evad
a Inc
.) ca
libra
tion u
nit
6F m
icrom
anom
eter-t
ipped
cathe
ter
(Milla
r SPC
350)
As
cend
ing an
d/ or
prox
imal
desc
endin
g ao
rta
Pres
sure
ampli
fiers
were
unsu
itable
for t
he
meas
urem
ent o
f AIx
or E
D

54 SphygmoCor system
Auth
or (y
ear)
Coun
try
Stud
y des
ign
Popu
latio
n (N
) Sy
stem
and
trans
fer f
unct
ion
Com
para
tor
Refe
renc
e sta
ndar
d
Sode
rstro
m (2
002)
Sw
eden
Stud
y eva
luatin
g the
valid
ity of
the
Sphy
gmoC
or
syste
m
Non-
cons
ecuti
ve pa
tients
with
an
gina p
ector
is sc
hedu
led fo
r PT
CA
Sphy
gmoC
or sy
stem
Radia
l arte
ry wa
vefor
ms ob
taine
d by
a ca
theter
attac
hed t
o a ex
terna
l pr
essu
re tr
ansd
ucer
(Pete
r van
Be
rg)
MAP
calib
ratio
n to r
adial
Radia
l arte
ry BP
mea
sure
ments
ob
taine
d by a
cathe
ter at
tache
d to
a exte
rnal
pres
sure
tran
sduc
er
(Pete
r van
Ber
g)
Natur
al fre
quen
cy 25
Hz a
nd a
damp
ing co
effici
ent o
f 0.35
–0.5
8F C
ordis
cathe
ter-tip
man
omete
r with
a pr
essu
re in
terfac
e (Se
ntron
) Fla
t freq
uenc
y res
pons
e up t
o 180
Hz
Asce
nding
aorta
Ao
rtic M
AP se
t iden
ticall
y to r
adial
MAP
Taka
zawa
(1
996)
NR
Stud
y eva
luatio
n the
valid
ity of
a tra
nsfer
func
tion
betw
een a
scen
ding
aorta
and r
adial
ar
tery
Non-
cons
ecuti
ve pa
tients
un
derg
oing d
iagno
stic c
ardia
c ca
theter
isatio
n (20
)
Unkn
own
Autom
ated t
onom
eter (
Jento
w 70
00, C
olin M
edica
l Instr
umen
ts Co
rp)
Calib
rated
, bra
chial
cuff B
P
Oscil
lometr
ic cu
ff bloo
d pre
ssur
e (C
olin M
edica
l Instr
umen
ts Co
rp,
JENT
OW 70
00 to
nome
ter)
Cathe
ter (M
illar M
ikro-
Tip ca
theter
) As
cend
ing ao
rta
Abbr
eviat
ions:
BP, b
lood p
ress
ure;
DBP,
dias
tolic
blood
pres
sure
; IV, in
trave
nous
; MAP
, mea
n arte
rial p
ress
ure;
NR, n
ot re
porte
d; PT
CA, p
ercu
taneo
us tr
anslu
mina
l cor
onar
y ang
ioplas
ty; R
A, ra
dial a
rtery;
SB
P sy
stolic
bloo
d pre
ssur
e. a It
is un
clear
from
the r
epor
ted st
udy w
hethe
r a tr
ansd
ucer
-tippe
d or f
luid-
filled
cathe
ter w
as us
ed, h
owev
er H
ope e
t al (2
003a
) hav
e ide
ntifie
d this
stud
y as u
sing a
tran
sduc
er-tip
ped c
athete
r.

SphygmoCor system 55
The same case series of patients were dealt with in two publications (Chen et al 1997; Fetics et al 1999). Only the study by Fetics et al (1999) was included in the review since it was the most recent publication dealing with this series of patients. The characteristics of the included studies are shown in Table 24. Six studies clearly reported the device being used for non-invasive brachial blood pressure measurement. All of these studies employed automated oscillatory devices in their methodologies.
The information reported in the studies is insufficient to evaluate the details of the catheters used as reference standards to determine if calibration or drift may have biased the results (Nichols et al 2005).
Five studies validated measures derived by the peripheral to central aortic transfer function with a transducer-tipped catheter (Fetics et al 1999; Hope et al 2004; Smulyan et al 2003; Soderstrom et al 2002; Takazawa et al 1996). A further study was unclear on the nature of the catheter, however, Hope et al (2003a) identified the paper by Davies et al (2003) as using a transducer-tipped catheter. Three studies used a fluid-filled catheter (Cloud et al 2003; Hope et al 2003b; Pauca et al 2001).
Four studies obtained the radial artery waveform data non-invasively with an applanation tonometer and calibrated the waveforms non-invasively (Cloud et al 2003; Davies et al 2003; Smulyan et al 2003; Takazawa et al 1996). Another two studies obtained the radial artery waveform data non-invasively but calibrated a component of this waveform using aortic pressures that were determined invasively (Fetics et al 1999; Hope et al 2003b). One additional study reported the use of applanation tonometry calibrated non-invasively or with a component of the radial waveform calibrated using aortic pressures that were determined invasively (Hope et al 2004). Of these seven studies, three clearly identified the transfer function used as the SphygmoCor system (Cloud et al 2003; Davies et al 2003; Smulyan et al 2003). Five of these studies used a transducer-tipped catheter (Davies et al 2003; Fetics et al 1999; Hope et al 2004; Smulyan et al 2003; Takazawa et al 1996). Two used a fluid-filled catheter to measure central aortic blood pressure directly (Cloud et al 2003; Hope et al 2003b).
Two studies reported obtaining the radial artery waveform by using invasive catheter measurement (Pauca et al 2001; Soderstrom et al 2002). Of these, one used a transducer-tipped catheter (Soderstrom et al 2002) and one used a fluid-filled catheter to measure central aortic blood pressure directly (Pauca et al 2001). These studies do not reflect how the SphygmoCor system would be used in clinical practice and therefore, have poor applicability.
The accuracy of the systems using a peripheral to central waveform transfer function when determining aortic blood pressure compared with upper limb blood pressure measurement is shown in Table 25. The table shows the difference between directly measured aortic blood pressure and the derived or peripheral blood pressures. These differences are calculated by subtracting the directly measured aortic pressures from derived or peripheral pressures. Thus, a positive value represents an overestimation by the test methods.

56 SphygmoCor system
Tabl
e 25
C
ompa
rison
of a
ccur
acy
of d
eriv
ed a
ortic
and
upp
er li
mb
bloo
d pr
essu
re m
easu
rem
ent u
sing
dire
ct m
easu
rem
ent o
f aor
tic
bloo
d pr
essu
re w
ith a
tran
sduc
er-ti
pped
cat
hete
r De
rived
– di
rect
aorti
c BP
Mean
diff
eren
ce (S
D)
Perip
hera
l – d
irect
aorti
c BP
Mean
diff
eren
ce (S
D)
Auth
or
(yea
r) Po
pulat
ion
(N)
Syst
em, t
rans
fer
func
tion
Dire
ct ao
rtic B
P (m
mHg
) (S
D)
SBP
(mm
Hg)
DBP
(mm
Hg)
PP (m
mHg
) SB
P (m
mHg
) DB
P (m
mHg
) PP
(mm
Hg)
Inde
x tes
t usin
g ra
dial
arte
ry w
avef
orm
obt
ained
by a
rteria
l ton
omet
ry w
ith ap
plica
ble c
alibr
atio
n Da
vies
(200
3)
Patie
nts un
derg
oing
CC (2
8)
Sphy
gmoC
or
Calib
ratio
n cuff
BP
SBP:
134 (
28)
DBP:
68 (1
2)
–7.2
(10.1
) 12
.2 (7
.1)
– 3.4
(10.5
) 11
.7 (7
.2)
–
Hope
(200
4)
Patie
nts un
derg
oing
CA or
percu
taneo
us
coro
nary
inter
venti
on (4
2)
Custo
m TF
a Ca
libra
tion c
uff B
P SB
P: 13
0 (23
) DB
P: 67
(9)
–7 (1
2)
–3 (6
) –4
(12)
5 (
16)
5 (7)
0 (
16)
Smuly
an
(200
3)
Patie
nts un
derg
oing
CA fo
r CHD
(50)
Sp
hygm
oCor
Ca
libra
tion c
uff B
P SB
P: 13
7.2
DBP:
74.4
–1.5
(11.3
) 10
.4 (1
2.7)
11.5
(13.6
) 10
.9 (1
2.7)
8.9 (1
2.9)
2.5 (1
6.3)
Taka
zawa
(1
996)
b Pa
tients
unde
rgoin
g CC
(20)
NR
, like
ly Sp
hygm
oCor
Ca
libra
tion c
uff B
P
SBP:
140 (
21)
DBP:
73 (1
1)
–11.0
b 8.0
b –
–2.0b
5.0b
–
Inde
x tes
t usin
g ra
dial
arte
ry w
avef
orm
obt
ained
by a
rteria
l ton
omet
ry an
d no
t app
licab
le ca
libra
tion
Fetic
s (19
99)
Patie
nts un
derg
oing
CC (3
9)
ARX
SBP
calib
ratio
n cuff
BP
; DBP
and M
AP
calib
ratio
n inv
asive
ao
rtic
– 0.4
(2.9)
–
– 13
.9 (6
.7)
– –
5 (16
)c 5 (
7)c
0 (16
)c Ho
pe (2
004)
Pa
tients
unde
rgoin
g CA
or pe
rcutan
eous
co
rona
ry int
erve
ntion
(42)
Custo
m TF
a SB
P ca
libra
tion c
uff
BP; D
BP an
d MAP
ca
libra
tion i
nvas
ive
aortic
SBP:
130 (
23)
DBP:
67 (9
) 1 (
8)
–9 (3
) 10
(9)
15 (1
1)
0 (0)
15
(11)
Inde
x tes
t usin
g ra
dial
arte
ry w
avef
orm
obt
ained
by r
adial
arte
ry ca
thet
erisa
tion
Sode
rstro
m (2
002)
Pa
tients
with
angin
a pe
ctoris
(12)
Sp
hygm
oCor
Inv
asive
ly de
termi
ned
perip
hera
l wav
eform
SBP:
168 (
SE 4)
DB
P: 71
(SE
2)
–8 (2
) 4 (
2)
– 1 (
5)
1 (2)
–
Abbr
eviat
ions:
AIx,
augm
entat
ion in
dex;
BP, b
lood p
ress
ure;
CA, c
oron
ary a
ngiog
raph
y; CC
, car
diac c
athete
risati
on; C
HD, c
oron
ary h
eart
disea
se; D
BP, d
iastol
ic blo
od pr
essu
re; M
AP, m
ean a
rteria
l pre
ssur
e; NR
, nor
repo
rted;
PP, p
ulse p
ress
ure;
SBP,
systo
lic bl
ood p
ress
ure;
SD, s
tanda
rd de
viatio
n; TF
, tran
sfer f
uncti
on.
Note:
Diffe
renc
es ar
e calc
ulated
by su
btrac
ting t
he di
rectl
y mea
sure
d aor
tic pr
essu
res f
rom
deriv
ed or
perip
hera
l pre
ssur
es. T
hus,
a pos
itive v
alue r
epre
sents
an ov
eres
timati
on by
the t
est.
a Cus
tom tr
ansfe
r fun
ction
deve
loped
at th
e Car
diova
scula
r Res
earch
Cen
tre, M
onas
h Med
ical C
entre
and M
onas
h Univ
ersit
y. b T
hese
value
s wer
e calc
ulated
from
the
findin
gs re
porte
d in T
akaz
awa (
1996
).
c Bra
chial
cuff b
lood p
ress
ure m
easu
reme
nts.
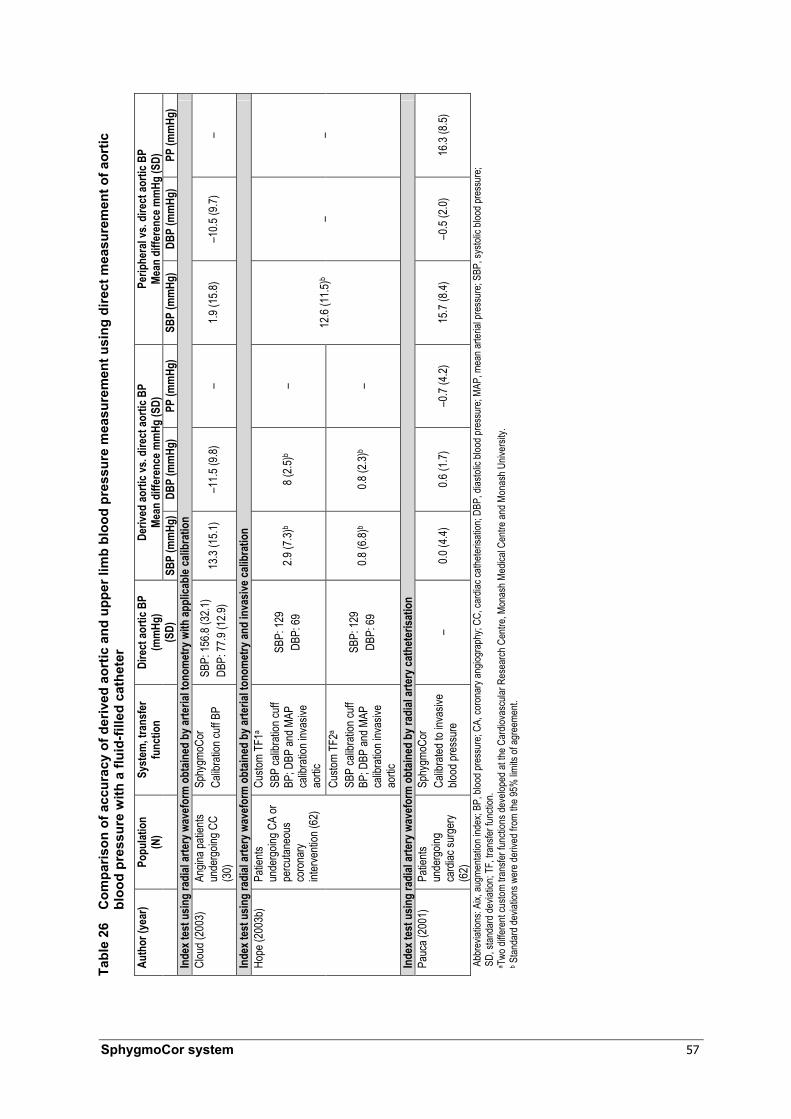
SphygmoCor system 57
Tabl
e 26
C
ompa
rison
of a
ccur
acy
of d
eriv
ed a
ortic
and
upp
er li
mb
bloo
d pr
essu
re m
easu
rem
ent u
sing
dire
ct m
easu
rem
ent o
f aor
tic
bloo
d pr
essu
re w
ith a
flui
d-fil
led
cath
eter
Ab
brev
iation
s: Ai
x, au
gmen
tation
inde
x; BP
, bloo
d pre
ssur
e; CA
, cor
onar
y ang
iogra
phy;
CC, c
ardia
c cath
eteris
ation
; DBP
, dias
tolic
blood
pres
sure
; MAP
, mea
n arte
rial p
ress
ure;
SBP,
systo
lic bl
ood p
ress
ure;
SD
, stan
dard
devia
tion;
TF, tr
ansfe
r fun
ction
. a T
wo di
ffere
nt cu
stom
trans
fer fu
nctio
ns de
velop
ed at
the C
ardio
vasc
ular R
esea
rch C
entre
, Mon
ash M
edica
l Cen
tre an
d Mon
ash U
niver
sity.
b Stan
dard
devia
tions
wer
e der
ived f
rom
the 95
% lim
its of
agre
emen
t.
Deriv
ed ao
rtic v
s. di
rect
aorti
c BP
Mean
diff
eren
ce m
mHg
(SD)
Pe
riphe
ral v
s. di
rect
aorti
c BP
Mean
diff
eren
ce m
mHg
(SD)
Au
thor
(yea
r) Po
pulat
ion
(N)
Syst
em, t
rans
fer
func
tion
Dire
ct ao
rtic B
P
(mm
Hg)
(SD)
SB
P (m
mHg
)DB
P (m
mHg
) PP
(mm
Hg)
SBP
(mm
Hg)
DBP
(mm
Hg)
PP (m
mHg
) In
dex t
est u
sing
radi
al ar
tery
wav
efor
m o
btain
ed b
y arte
rial t
onom
etry
with
appl
icabl
e cali
brat
ion
Clou
d (20
03)
Angin
a pati
ents
unde
rgoin
g CC
(30)
Sphy
gmoC
or
Calib
ratio
n cuff
BP
SBP:
156.8
(32.1
) DB
P: 77
.9 (1
2.9)
13.3
(15.1
) –1
1.5 (9
.8)
– 1.9
(15.8
) –1
0.5 (9
.7)
–
Inde
x tes
t usin
g ra
dial
arte
ry w
avef
orm
obt
ained
by a
rteria
l ton
omet
ry an
d in
vasiv
e cali
brat
ion
Custo
m TF
1a
SBP
calib
ratio
n cuff
BP
; DBP
and M
AP
calib
ratio
n inv
asive
ao
rtic
SBP:
129
DBP:
69
2.9 (7
.3)b
8 (2.5
)b –
Hope
(200
3b)
Patie
nts
unde
rgoin
g CA
or
percu
taneo
us
coro
nary
inter
venti
on (6
2)
Custo
m TF
2a
SBP
calib
ratio
n cuff
BP
; DBP
and M
AP
calib
ratio
n inv
asive
ao
rtic
SBP:
129
DBP:
69
0.8 (6
.8)b
0.8 (2
.3)b
–
12.6
(11.5
)b –
–
Inde
x tes
t usin
g ra
dial
arte
ry w
avef
orm
obt
ained
by r
adial
arte
ry ca
thet
erisa
tion
Pauc
a (20
01)
Patie
nts
unde
rgoin
g ca
rdiac
surg
ery
(62)
Sphy
gmoC
or
Calib
rated
to in
vasiv
e blo
od pr
essu
re
– 0.0
(4.4)
0.6
(1.7)
–0
.7 (4
.2)
15.7
(8.4)
–0
.5 (2
.0)
16.3
(8.5)
58 SphygmoCor system
The most applicable studies were the five that applied transfer functions to radial artery waveforms obtained by applanation tonometry and calibrated using non-invasive means. In these studies, the estimation of central aortic pressure using a transfer function was generally within 15 mmHg of the directly measured aortic pressures. The difference between the derived and directly measured aortic pressures varied significantly between these studies.
The comparative accuracy of transfer functions and cuff sphygmomanometry in estimating aortic blood pressure also showed large variation between studies. Four studies were validated with transducer-tipped catheters and one with a fluid-filled catheter. However, this is not expected to affect the comparative accuracy of the methods. Only one study demonstrated improved estimation of aortic systolic blood pressure (SBP) by derivation using SphygmoCor than by cuff sphygmomanometry (–1.5 ± 11.3 mmHg and 10.9 ± 12.7, mmHg respectively) (Smulyan et al 2003). The accuracy of estimation of central diastolic blood pressure (DBP) in this study was similar for both methods (SphygmoCor: 10.4 ± 12.7 mmHg; cuff: 8.9 ± 12.9 mmHg). In this study, which used a transducer-tipped catheter, some of the direct aortic blood pressure measurements were obtained in the proximal descending aorta, rather than the ascending aorta (Smulyan et al 2003). In addition, the automated sphygmomanometer was calibrated using a calibration unit (Cuff Link, DNI Nevada Inc).
A single study demonstrated improved estimation of aortic DBP by the use of a transfer function than by cuff sphygmomanometry (Hope et al 2004). The difference between indirect and direct measurement of aortic DBP using either method was considered small (–3 ± 6 mmHg for derived aortic blood pressure and +5 ± 7 mmHg for cuff blood pressure measurement). This study used a transducer-tipped catheter and a customised transfer function that was different from that used in the SphygmoCor system.
Three further studies employed applanation tonometry and calibration using invasive aortic blood pressure measurement; two of these studies used transducer-tipped catheters, while one study used a fluid-filled catheter. These studies all demonstrated that a transfer function provided better estimation of aortic SBP than cuff sphygmomanometric or scaled untransformed radial artery data. However, the method for calibration does not reflect that which would be used in clinical practice.
Two studies used transfer functions to derive aortic waveforms based on invasive radial artery data. These studies compared the accuracy of the derived aortic pressures with invasively measured radial pressures in the estimation of directly measured aortic pressures. Soderstrom et al (2002) demonstrated closer estimation of aortic SBP pressure by invasive radial SBP than derived SBP; however, the measured aortic mean arterial pressure (MAP) had been set as equivalent to the radial MAP, introducing a strong bias. Pauca et al (2001) measured aortic pressures using a fluid-filled catheter and compared these with invasive data obtained from the radial artery and radial data transformed using the SphygmoCor transfer function. This study demonstrated improved accuracy for estimation of aortic SBP by SphygmoCor than by invasive radial artery measurements.
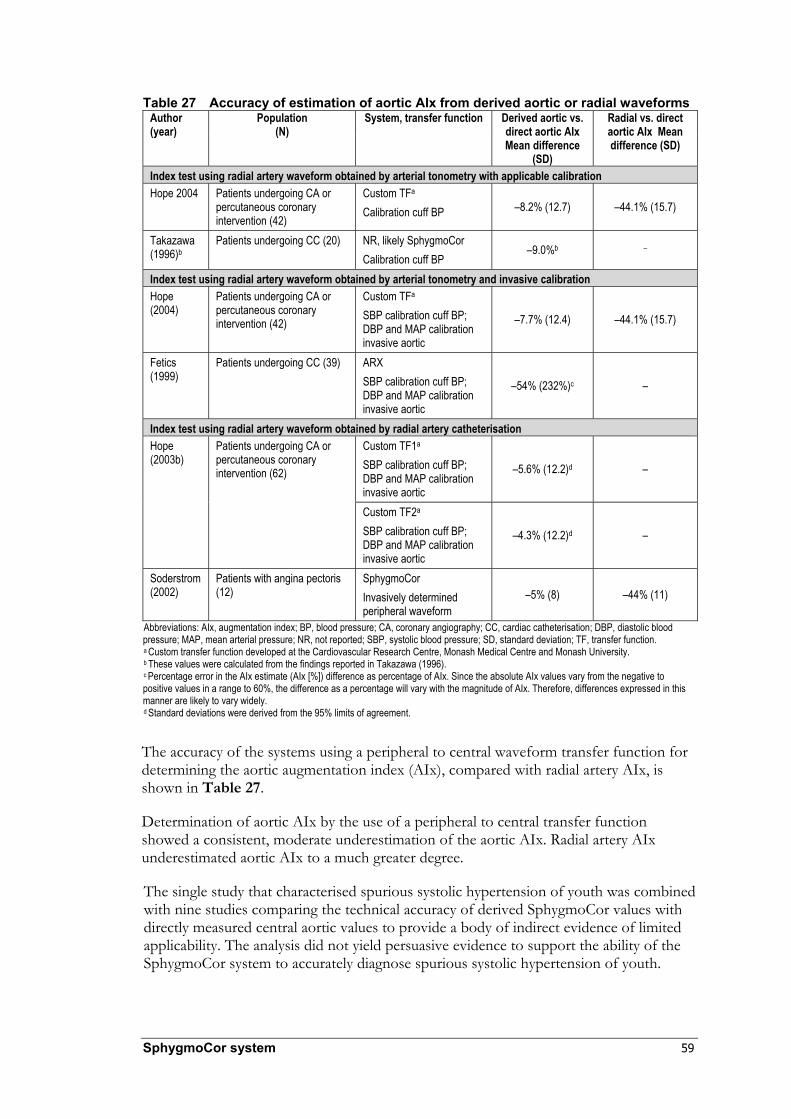
SphygmoCor system 59
Table 27 Accuracy of estimation of aortic AIx from derived aortic or radial waveforms
Author (year)
Population (N)
System, transfer function Derived aortic vs. direct aortic AIx Mean difference
(SD)
Radial vs. direct aortic AIx Mean difference (SD)
Index test using radial artery waveform obtained by arterial tonometry with applicable calibration Hope 2004 Patients undergoing CA or
percutaneous coronary intervention (42)
Custom TFa Calibration cuff BP –8.2% (12.7) –44.1% (15.7)
Takazawa (1996)b
Patients undergoing CC (20) NR, likely SphygmoCor Calibration cuff BP
–9.0%b –
Index test using radial artery waveform obtained by arterial tonometry and invasive calibration Hope (2004)
Patients undergoing CA or percutaneous coronary intervention (42)
Custom TFa SBP calibration cuff BP; DBP and MAP calibration invasive aortic
–7.7% (12.4) –44.1% (15.7)
Fetics (1999)
Patients undergoing CC (39) ARX SBP calibration cuff BP; DBP and MAP calibration invasive aortic
–54% (232%)c –
Index test using radial artery waveform obtained by radial artery catheterisation Custom TF1a
SBP calibration cuff BP; DBP and MAP calibration invasive aortic
–5.6% (12.2)d –
Hope (2003b)
Patients undergoing CA or percutaneous coronary intervention (62)
Custom TF2a
SBP calibration cuff BP; DBP and MAP calibration invasive aortic
–4.3% (12.2)d –
Soderstrom (2002)
Patients with angina pectoris (12)
SphygmoCor Invasively determined peripheral waveform
–5% (8) –44% (11)
Abbreviations: AIx, augmentation index; BP, blood pressure; CA, coronary angiography; CC, cardiac catheterisation; DBP, diastolic blood pressure; MAP, mean arterial pressure; NR, not reported; SBP, systolic blood pressure; SD, standard deviation; TF, transfer function. a Custom transfer function developed at the Cardiovascular Research Centre, Monash Medical Centre and Monash University. b These values were calculated from the findings reported in Takazawa (1996). c Percentage error in the AIx estimate (AIx [%]) difference as percentage of AIx. Since the absolute AIx values vary from the negative to positive values in a range to 60%, the difference as a percentage will vary with the magnitude of AIx. Therefore, differences expressed in this manner are likely to vary widely. d Standard deviations were derived from the 95% limits of agreement.
The accuracy of the systems using a peripheral to central waveform transfer function for determining the aortic augmentation index (AIx), compared with radial artery AIx, is shown in Table 27.
Determination of aortic AIx by the use of a peripheral to central transfer function showed a consistent, moderate underestimation of the aortic AIx. Radial artery AIx underestimated aortic AIx to a much greater degree.
The single study that characterised spurious systolic hypertension of youth was combined with nine studies comparing the technical accuracy of derived SphygmoCor values with directly measured central aortic values to provide a body of indirect evidence of limited applicability. The analysis did not yield persuasive evidence to support the ability of the SphygmoCor system to accurately diagnose spurious systolic hypertension of youth.

60 SphygmoCor system
Appendix F Included studies
Table 28 and Table 29 present summaries of the design, population characteristics, test characteristics, outcomes and an assessment of quality and applicability of the included studies. Diagnostic accuracy studies are presented in Table 28 while studies contributing to the indirect evidence for spurious systolic hypertension of youth are presented in Table 29.
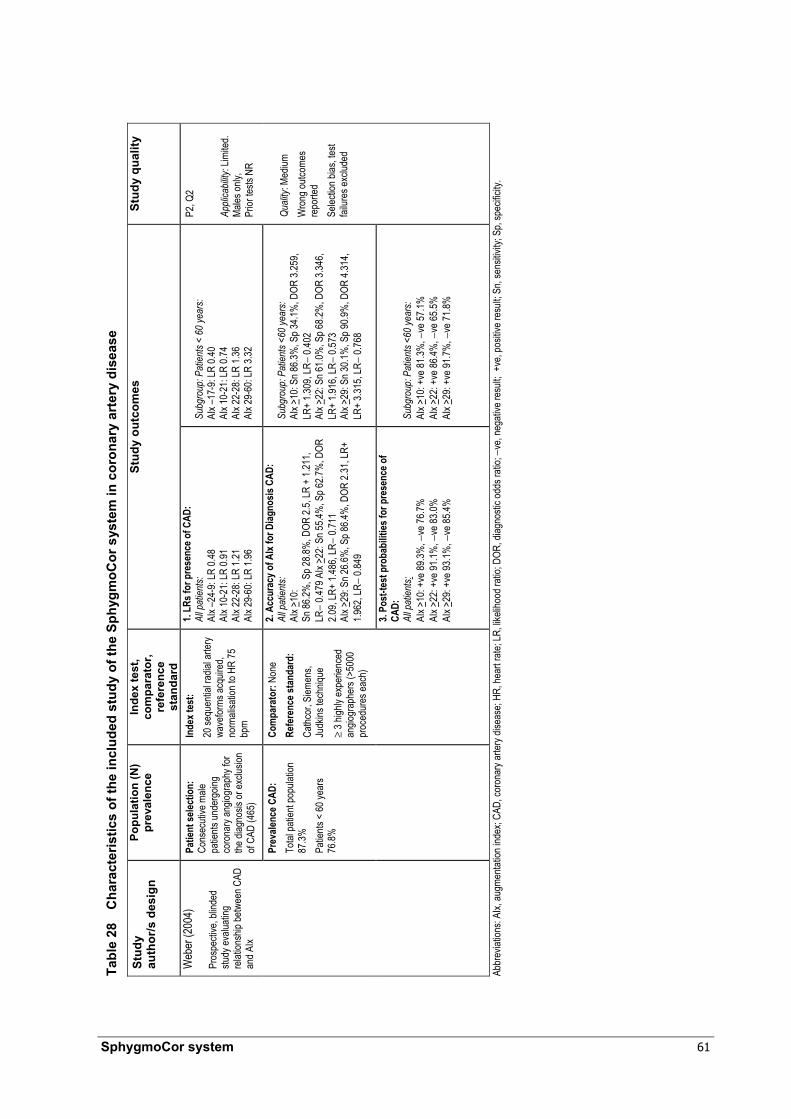
SphygmoCor system 61
Tabl
e 28
C
hara
cter
istic
s of
the
incl
uded
stu
dy o
f the
Sph
ygm
oCor
sys
tem
in c
oron
ary
arte
ry d
isea
se
Stud
y au
thor
/s d
esig
n
Popu
latio
n (N
) pr
eval
ence
In
dex
test
, co
mpa
rato
r, re
fere
nce
stan
dard
Stud
y ou
tcom
es
Stud
y qu
ality
Patie
nt se
lectio
n:
Cons
ecuti
ve m
ale
patie
nts un
derg
oing
coro
nary
angio
grap
hy fo
r the
diag
nosis
or ex
clusio
n of
CAD
(465
)
Inde
x tes
t:
20 se
quen
tial ra
dial a
rtery
wave
forms
acqu
ired,
norm
alisa
tion t
o HR
75
bpm
1. LR
s for
pre
senc
e of C
AD:
All p
atien
ts:
AIx –
24-9
: LR
0.48
AIx 1
0-21
: LR
0.91
AIx 2
2-28
: LR
1.21
AIx 2
9-60
: LR
1.96
Subg
roup
: Pat
ients
< 60
year
s:
AIx –
17-9
: LR
0.40
AIx 1
0-21
: LR
0.74
AIx 2
2-28
: LR
1.36
AIx 2
9-60
: LR
3.32
2. Ac
cura
cy o
f AIx
for D
iagno
sis C
AD:
All p
atien
ts:
AIx >
10:
Sn 86
.2%, S
p 28.8
%, D
OR 2.
5, LR
+ 1.
211,
LR−
0.479
AIx
>22:
Sn 55
.4%, S
p 62.7
%, D
OR
2.09,
LR+
1.486
, LR−
0.71
1 AI
x >29
: Sn 2
6.6%
, Sp 8
6.4%
, DOR
2.31
, LR+
1.9
62, L
R− 0.
849
Subg
roup
: Pat
ients
<60
year
s:
AIx >
10: S
n 86.3
%, S
p 34.1
%, D
OR 3.
259,
LR+
1.309
, LR−
0.40
2 AI
x >22
: Sn 6
1.0%
, Sp 6
8.2%
, DOR
3.34
6, LR
+ 1.9
16, L
R− 0.
573
AIx >
29: S
n 30.1
%, S
p 90.9
%, D
OR 4.
314,
LR+
3.315
, LR−
0.76
8
Web
er (2
004)
Pr
ospe
ctive
, blin
ded
study
evalu
ating
re
lation
ship
betw
een C
AD
and A
Ix
Prev
alenc
e CAD
: To
tal pa
tient
popu
lation
87
.3%
Patie
nts <
60 ye
ars
76.8%
Com
para
tor:
None
Re
fere
nce s
tand
ard:
Ca
thcor
, Siem
ens,
Judk
ins te
chniq
ue
≥ 3 h
ighly
expe
rienc
ed
angio
grap
hers
(>50
00
proc
edur
es ea
ch)
3. Po
st-te
st p
roba
bilit
ies fo
r pre
senc
e of
CAD:
Al
l pat
ients:
AI
x >10
: +ve
89.3%
, −ve
76.7%
AI
x >22
: +ve
91.1%
, −ve
83.0%
AI
x >29
: +ve
93.1%
, −ve
85.4%
Subg
roup
: Pat
ients
<60
year
s:
AIx >
10: +
ve 81
.3%, −
ve 57
.1%
AIx >
22: +
ve 86
.4%, −
ve 65
.5%
AIx >
29: +
ve 91
.7%, −
ve 71
.8%
P2, Q
2 Ap
plica
bility
: Lim
ited.
Ma
les on
ly,
Prior
tests
NR
Quali
ty: M
edium
W
rong
outco
mes
repo
rted
Selec
tion b
ias, te
st fai
lures
exclu
ded
Abbr
eviat
ions:
AIx,
augm
entat
ion in
dex;
CAD,
coro
nary
arter
y dise
ase;
HR, h
eart
rate;
LR, li
kelih
ood r
atio;
DOR,
diag
nosti
c odd
s rati
o; −v
e, ne
gativ
e res
ult; +
ve, p
ositiv
e res
ult; S
n, se
nsitiv
ity; S
p, sp
ecific
ity.

62 SphygmoCor system
Tabl
e 29
C
hara
cter
istic
s an
d re
sults
of t
he in
clud
ed s
tudi
es c
ompa
ring
the
mea
sure
men
t of d
eriv
ed a
ortic
, rad
ial a
nd m
easu
red
aort
ic B
P
Stud
y, a
utho
r/s,
desi
gn
Popu
latio
n (N
) In
dex
test
, com
para
tor,
refe
renc
e st
anda
rd
Stud
y ou
tcom
es
Chen
(199
7)
Same
patie
nt po
pulat
ion
as F
etics
(199
9)
Stud
y eva
luatin
g ma
thema
tical
trans
forma
tion o
f rad
ial
wave
form
data
Patie
nt se
lectio
n: N
on-co
nsec
utive
pa
tients
unde
rgoin
g car
diac
cathe
terisa
tion (
20)
Inde
x tes
t: AR
X Mo
del T
F Au
tomate
d ton
omete
r (Je
ntow,
Coli
n Med
ical In
strum
ents
Corp
) SB
P ca
libra
tion c
uff B
P; D
BP &
MAP
calib
ratio
n inv
asive
aortic
Co
mpa
rato
r: Un
trans
forme
d rad
ial w
avefo
rm (J
entow
tono
meter
) SB
P ca
libra
tion a
utoma
ted cu
ff BP
(Jento
w, C
olin M
edica
l Instr
umen
ts Co
rp);
DBP
& MA
P ca
libra
tion i
nvas
ive ao
rtic O
scillo
metric
cuff
Refe
renc
e sta
ndar
d: M
icrom
anom
eter-t
ipped
cathe
ter (M
illar S
PC 32
0) or
mi
croma
nome
ter-tip
ped m
ulti-e
lectro
de pr
essu
re-vo
lume c
athete
r (Mi
llar
SSD
768)
. Asc
endin
g aor
ta
See F
etics
(199
9)
Clou
d (20
03)
Stud
y eva
luatin
g the
use
of no
n-inv
asive
calib
ratio
n for
the S
phyg
moCo
r sy
stem
Patie
nt se
lectio
n: N
on-co
nsec
utive
pa
tients
with
angin
a sym
ptoms
un
derg
oing c
ardia
c cath
eteris
ation
(3
0)
Inde
x tes
t: Sp
hygm
oCor
syste
m RA
tono
metry
, cali
brate
d, br
achia
l cuff
BP
Com
para
tor:
Autom
atic o
scillo
metric
digit
al BP
mon
itor (
Omro
n, HE
M-70
CP
). Re
cord
ed im
media
tely b
efore
tono
metry
Re
fere
nce s
tand
ard:
Mar
quett
e Mida
s Sys
tem 40
00. A
ortic
loca
tion N
R
Outco
mes d
erive
d usin
g a flu
id-fill
ed ca
theter
1.
Inde
x tes
t usin
g ra
dial
arte
ry w
avef
orm
ob
tain
ed b
y arte
rial t
onom
etry
with
appl
icabl
e ca
libra
tion
Deriv
ed ao
rtic vs
. dire
ct ao
rtic B
P, m
ean d
iffere
nce
mmHg
(SD)
: SBP
: 13.3
(15.1
); DB
P: −
11.5
(9.8)
Pe
riphe
ral v
s. dir
ect a
ortic
BP,
mea
n diffe
renc
e mm
Hg (S
D): S
BP: 1
.9 (1
5.8);
DBP:
−10
.5 (9
.7)
Davie
s (20
03)
Pros
pecti
ve st
udy
comp
aring
calcu
lated
ao
rtic to
perip
hera
l bloo
d pr
essu
re m
easu
reme
nts
Patie
nt se
lectio
n: N
on-co
nsec
utive
pa
tients
unde
rgoin
g car
diac
cathe
terisa
tion w
ith ea
sily p
alpate
d lef
t RA;
exclu
ding p
atien
ts wi
th a
histor
y of b
rach
ial or
subc
lavian
ste
nosis
(28)
Inde
x tes
t: Sp
hygm
oCor
syste
m RA
tono
metry
, cali
brate
d bra
chial
cuff B
P Co
mpa
rato
r: Os
cillom
etric
brac
hial c
uff (O
mron
HEM
-705
CP)
syste
m Re
cord
ed im
media
tely b
efore
tono
metry
Re
fere
nce s
tand
ard:
Cath
eter w
ith T
rans
pac I
V mo
nitor
ing ki
t (Ab
bott
Critic
al Ca
re S
ystem
s, Ab
bott L
abor
atorie
s) Si
emen
s Rec
or V
6 sys
tem. A
scen
ding a
orta
Outco
mes d
erive
d usin
g a flu
id-fill
ed ca
theter
In
dex t
est u
sing
radi
al ar
tery
wav
efor
m
obta
ined
by a
rteria
l ton
omet
ry w
ith ap
plica
ble
calib
ratio
n De
rived
aortic
vs. d
irect
aortic
BP,
mea
n diffe
renc
e mm
Hg (S
D): S
BP: −
7.2 (1
0.1);
DBP:
12.2
(7.1)
Pe
riphe
ral v
s. dir
ect a
ortic
BP,
mea
n diffe
renc
e mm
Hg (S
D): S
BP: 3
.4 (1
0.5);
DBP:
11.7
(7.2)

SphygmoCor system 63
Stud
y, a
utho
r/s,
desi
gn
Popu
latio
n (N
) In
dex
test
, com
para
tor,
refe
renc
e st
anda
rd
Stud
y ou
tcom
es
Fetic
s (19
99)
Stud
y eva
luatin
g ma
thema
tical
trans
forma
tion o
f rad
ial
wave
form
data
Patie
nt se
lectio
n: N
on-co
nsec
utive
pa
tients
unde
rgoin
g diag
nosti
c ca
rdiac
cathe
terisa
tion (
39)
Inde
x tes
t: AR
X Mo
del
Autom
ated t
onom
eter (
Jento
w, C
olin M
edica
l Instr
umen
ts Co
rp),
analo
g filt
ered
at 30
Hz. S
BP ca
libra
tion c
uff B
P; D
BP &
MAP
calib
ratio
n inv
asive
ao
rtic
Com
para
tor:
Untra
nsfor
med r
adial
wav
eform
(Jen
tow to
nome
ter)
SBP
calib
ratio
n, au
tomate
d cuff
BP
(Jen
tow, C
olin M
edica
l Instr
umen
ts Co
rp);
DBP
& MA
P ca
libra
tion,
invas
ive ao
rtic
Refe
renc
e sta
ndar
d: M
icrom
anom
eter-t
ipped
cathe
ter (M
illar S
PC 32
0).
Asce
nding
aorta
Outco
mes d
erive
d usin
g a tr
ansd
ucer
-tippe
d ca
theter
In
dex t
est u
sing
radi
al ar
tery
wav
efor
m
obta
ined
by a
rteria
l ton
omet
ry an
d no
t ap
plica
ble c
alibr
atio
n De
rived
aortic
vs. d
irect
aortic
augm
entat
ion in
dex:
AIx %
mea
n diffe
renc
e (SD
): −5
4% (2
32%
)b De
rived
aortic
vs. d
irect
aortic
BP,
mea
n diffe
renc
e mm
Hg (S
D): S
BP: 0
.4 (2
.9)
Perip
hera
l vs.
direc
t aor
tic B
P, m
ean d
iffere
nce
mmHg
(SD)
: SBP
: 13.9
(6.7)
Hope
(200
3b)
Stud
y inv
estig
ating
the
accu
racy
of ge
nera
l tra
nsfer
func
tions
Patie
nt se
lectio
n: N
on-co
nsec
utive
pa
tients
unde
rgoin
g cor
onar
y an
giogr
aphy
or pe
rcutan
eous
co
rona
ry int
erve
ntion
; exc
luding
pa
tients
with
no ra
dial a
rtery;
sig
nifica
nt ob
struc
tive
ather
oscle
rosis
dise
ase o
f the u
pper
lim
b; pr
oced
ural
comp
licati
on
affec
ting u
pper
limb B
P (7
1)
Inde
x tes
t: Fo
urier
tran
sform
ation
RA
tono
metry
(Milla
r Mikr
o-Tip
, Milla
r Ins
trume
nts).
SBP
calib
ratio
n cuff
BP;
DB
P &
MAP
calib
ratio
n inv
asive
aortic
Co
mpa
rato
r: Un
trans
forme
d rad
ial w
avefo
rm (M
illar M
ikro-
Tip to
nome
ter)
SBP
calib
ratio
n auto
mated
cuff B
P; D
BP &
MAP
calib
ratio
n inv
asive
aortic
Re
fere
nce s
tand
ard:
Low
comp
lianc
e flui
d-fill
ed ca
theter
As
cend
ing ao
rta
Outco
mes d
erive
d usin
g a flu
id-fill
ed ca
theter
In
dex t
est u
sing
radi
al ar
tery
wav
efor
m
obta
ined
by a
rteria
l ton
omet
ry an
d no
t ap
plica
ble c
alibr
atio
n
Deriv
ed ao
rtic vs
. dire
ct ao
rtic au
gmen
tation
inde
x Tr
ansfe
r fun
ction
1a ; AI
x % m
ean d
iffere
nce
(CI):
−5.6
(24.4
) Tr
ansfe
r fun
ction
2a ; AI
x % m
ean d
iffere
nce
(CI):
−4.3
(24.3
) De
rived
aortic
vs. d
irect
aortic
BP,
mea
n diffe
renc
e mm
Hg (C
I):
Tran
sfer f
uncti
on 1a S
BP: 2
.9 (1
4.6);
DBP:
8 (5
.0)
Tran
sfer f
uncti
on 2a S
BP: 0
.8 (1
3.5) ;
DBP
: 0.8
(4.6)
Pe
riphe
ral v
s. dir
ect a
ortic
BP,
mea
n diffe
renc
e mm
Hg (C
I): T
rans
fer fu
nctio
n 1a :
SBP:
12.6
(22.9
)
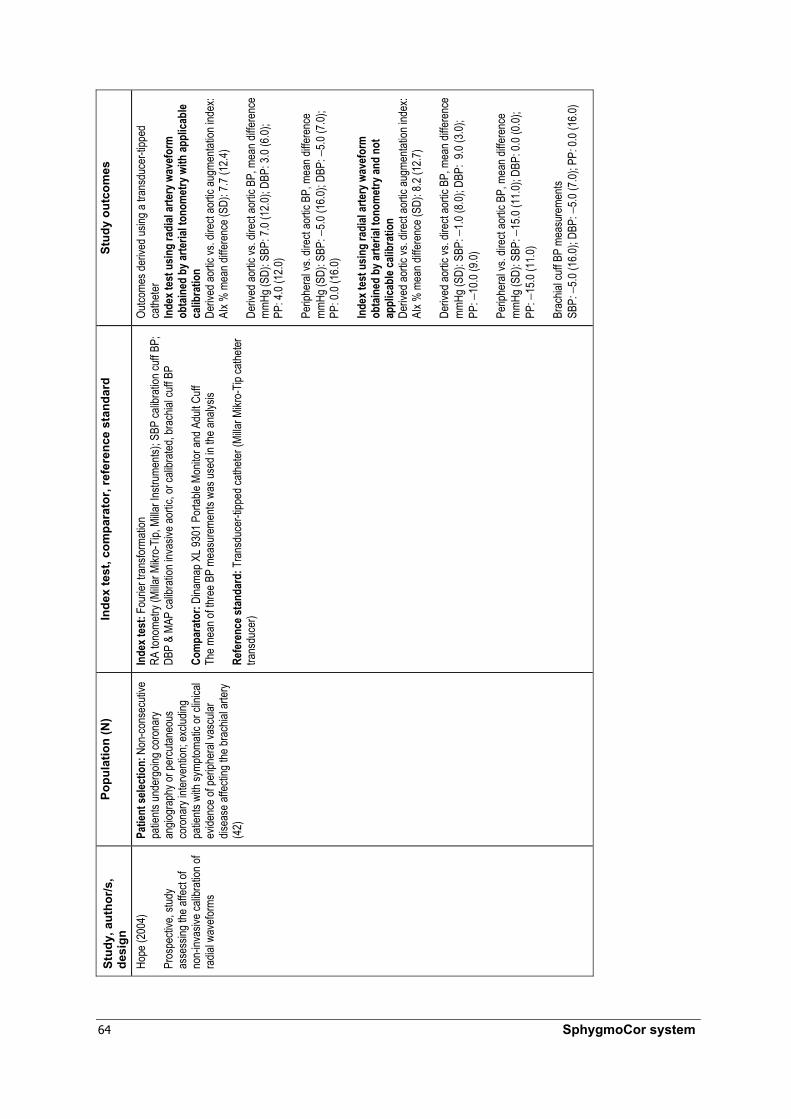
64 SphygmoCor system
Stud
y, a
utho
r/s,
desi
gn
Popu
latio
n (N
) In
dex
test
, com
para
tor,
refe
renc
e st
anda
rd
Stud
y ou
tcom
es
Hope
(200
4)
Pros
pecti
ve, s
tudy
asse
ssing
the a
ffect
of no
n-inv
asive
calib
ratio
n of
radia
l wav
eform
s
Patie
nt se
lectio
n: N
on-co
nsec
utive
pa
tients
unde
rgoin
g cor
onar
y an
giogr
aphy
or pe
rcutan
eous
co
rona
ry int
erve
ntion
; exc
luding
pa
tients
with
symp
tomati
c or c
linica
l ev
idenc
e of p
eriph
eral
vasc
ular
disea
se af
fectin
g the
brac
hial a
rtery
(42)
Inde
x tes
t: Fo
urier
tran
sform
ation
RA
tono
metry
(Milla
r Mikr
o-Tip
, Milla
r Ins
trume
nts);
SBP
calib
ratio
n cuff
BP;
DB
P &
MAP
calib
ratio
n inv
asive
aortic
, or c
alibr
ated,
brac
hial c
uff B
P Co
mpa
rato
r: Di
nama
p XL 9
301 P
ortab
le Mo
nitor
and A
dult C
uff
The m
ean o
f thre
e BP
meas
urem
ents
was u
sed i
n the
analy
sis
Refe
renc
e sta
ndar
d: T
rans
duce
r-tipp
ed ca
theter
(Milla
r Mikr
o-Tip
cathe
ter
trans
duce
r)
Outco
mes d
erive
d usin
g a tr
ansd
ucer
-tippe
d ca
theter
In
dex t
est u
sing
radi
al ar
tery
wav
efor
m
obta
ined
by a
rteria
l ton
omet
ry w
ith ap
plica
ble
calib
ratio
n De
rived
aortic
vs. d
irect
aortic
augm
entat
ion in
dex:
AIx %
mea
n diffe
renc
e (SD
): 7.7
(12.4
) De
rived
aortic
vs. d
irect
aortic
BP,
mea
n diffe
renc
e mm
Hg (S
D): S
BP: 7
.0 (1
2.0);
DBP:
3.0 (
6.0);
PP
: 4.0
(12.0
) Pe
riphe
ral v
s. dir
ect a
ortic
BP,
mea
n diffe
renc
e mm
Hg (S
D): S
BP: −
5.0 (1
6.0);
DBP:
−5.0
(7.0)
; PP
: 0.0
(16.0
) In
dex t
est u
sing
radi
al ar
tery
wav
efor
m
obta
ined
by a
rteria
l ton
omet
ry an
d no
t ap
plica
ble c
alibr
atio
n De
rived
aortic
vs. d
irect
aortic
augm
entat
ion in
dex:
AIx %
mea
n diffe
renc
e (SD
): 8.2
(12.7
) De
rived
aortic
vs. d
irect
aortic
BP,
mea
n diffe
renc
e mm
Hg (S
D): S
BP: −
1.0 (8
.0); D
BP: 9
.0 (3
.0);
PP: −
10.0
(9.0)
Pe
riphe
ral v
s. dir
ect a
ortic
BP,
mea
n diffe
renc
e mm
Hg (S
D): S
BP: −
15.0
(11.0
); DB
P: 0.
0 (0.0
);
PP: −
15.0
(11.0
) Br
achia
l cuff
BP
meas
urem
ents
SB
P: −
5.0 (1
6.0);
DBP:
−5.0
(7.0)
; PP:
0.0 (
16.0)

SphygmoCor system 65
Stud
y, a
utho
r/s,
desi
gn
Popu
latio
n (N
) In
dex
test
, com
para
tor,
refe
renc
e st
anda
rd
Stud
y ou
tcom
es
Pauc
a (20
01)
Pros
pecti
ve, s
tudy
evalu
ating
the
Sphy
gmoC
or sy
stem
befor
e and
after
inten
sive
vaso
dilati
on
Patie
nt se
lectio
n: C
onse
cutiv
e pa
tients
unde
rgoin
g car
diac s
urge
ry;
exclu
ding p
atien
ts wi
th ha
emod
ynam
ically
sign
ifican
t br
achia
l, sub
clavia
n or in
nomi
nate
steno
sis (6
2)
Inde
x tes
t: Sp
hygm
oCor
syste
m Ra
dial a
rtery
wave
forms
obtai
ned b
y a ca
theter
attac
hed t
o a T
rans
pac
mano
meter
(Abb
ott C
ritica
l Car
e Sys
tems,
Abbo
tt Lab
orato
ries)
Com
para
tor:
Cathe
ter at
tache
d to a
Tra
nspa
c man
omete
r (Ab
bott C
ritica
l Ca
re S
ystem
s, Ab
bott L
abor
atorie
s) Fr
eque
ncy r
espo
nse >
20Hz
and a
damp
ening
coeff
icien
t >0.3
Re
fere
nce s
tand
ard:
Cath
eter a
ttach
ed to
a Tr
ansp
ac m
anom
eter (
Abbo
tt Cr
itical
Care
Sys
tems,
Abbo
tt Lab
orato
ries)
Asce
nding
aorta
Fr
eque
ncy r
espo
nse >
20Hz
and a
damp
ening
coeff
icien
t >0.3
Outco
mes d
erive
d usin
g a flu
id-fill
ed ca
theter
In
dex t
est u
sing
radi
al ar
tery
wav
efor
m
obta
ined
by r
adial
arte
ry ca
thet
erisa
tion
De
rived
aortic
vs. d
irect
aortic
BP,
mea
n diffe
renc
e mm
Hg (S
D): S
BP: 0
.0 (4
.4); D
BP: 0
.6 (1
.7);
PP: −
0.7 (4
.2)
Perip
hera
l vs.
direc
t aor
tic B
P, m
ean d
iffere
nce
mmHg
(SD)
: SBP
: 15.7
(8.4)
; DBP
: −0.5
(2.0)
; PP
: 16.3
(8.5)
Smuly
an (2
003)
St
udy o
f the c
linica
l utili
ty of
calcu
lated
aortic
wa
vefor
ms
Patie
nt se
lectio
n: N
on-co
nsec
utive
pa
tients
unde
rgoin
g cor
onar
y an
giogr
aphy
for t
he di
agno
sis/
exclu
sion o
r ass
essm
ent o
f the
seve
rity of
coro
nary
hear
t dise
ase
(50)
Inde
x tes
t: Sp
hygm
oCor
syste
m Ca
libra
ted, b
rach
ial cu
ff BP
Com
para
tor:
Osc
illome
tric br
achia
l arte
ry cu
ff sys
tem (C
olin M
edica
l Ins
trume
nts C
orp)
. Rec
orde
d imm
ediat
ely af
ter to
nome
try
Oscil
lometr
ic blo
od pr
essu
re sy
stem
calib
rated
with
Cuff
Link
(DNI
Nev
ada
Inc) c
alibr
ation
unit
Refe
renc
e sta
ndar
d: 6F
micr
oman
omete
r-tipp
ed ca
theter
(Milla
r SPC
350)
As
cend
ing an
d/ or
prox
imal
desc
endin
g aor
ta. P
ress
ure a
mplifi
ers w
ere
unsu
itable
for t
he m
easu
reme
nt of
AIx o
r ED
Outco
mes d
erive
d usin
g a tr
ansd
ucer
-tippe
d ca
theter
In
dex t
est u
sing
radi
al ar
tery
wav
efor
m
obta
ined
by a
rteria
l ton
omet
ry w
ith ap
plica
ble
calib
ratio
n
Deriv
ed ao
rtic vs
. dire
ct ao
rtic B
P, m
ean d
iffere
nce
mmHg
(SD)
: SBP
: −1.5
(11.3
); DB
P: 10
.4 (1
2.7);
PP: 1
1.5 (1
3.6)
Perip
hera
l vs.
direc
t aor
tic B
P, m
ean d
iffere
nce
mmHg
(SD)
: SBP
: 10.9
(12.7
); DB
P: 8.
9 (12
.9);
PP: 2
.5 (1
6.3)

66 SphygmoCor system
Stud
y, a
utho
r/s,
desi
gn
Popu
latio
n (N
) In
dex
test
, com
para
tor,
refe
renc
e st
anda
rd
Stud
y ou
tcom
es
Sode
rstro
m (2
002)
St
udy e
valua
ting t
he
valid
ity of
the
Sphy
gmoC
or sy
stem
Patie
nt se
lectio
n: N
on-co
nsec
utive
pa
tients
with
angin
a pec
toris
sche
duled
for P
TCA
(12)
Inde
x tes
t: S
phyg
moCo
r sys
tem
Radia
l arte
ry wa
vefor
ms ob
taine
d by a
cathe
ter at
tach t
o a ex
terna
l pr
essu
re tr
ansd
ucer
(Pete
r van
Ber
g); M
AP ca
libra
tion t
o rad
ial
Com
para
tor:
Radia
l arte
ry BP
mea
sure
ments
obtai
ned b
y a ca
theter
attac
h to
a exte
rnal
pres
sure
tran
sduc
er (P
eter v
an B
erg)
Na
tural
frequ
ency
25Hz
and a
damp
ing co
effici
ent o
f 0.35
–0.5
Refe
renc
e sta
ndar
d: 8
F Co
rdis
cathe
ter-tip
man
omete
r with
a pr
essu
re
inter
face (
Sentr
on).
Flat fr
eque
ncy r
espo
nse u
p to 1
80 H
z. As
cend
ing ao
rta
Aortic
MAP
set id
entic
ally t
o rad
ial M
AP
Outco
mes d
erive
d usin
g a tr
ansd
ucer
-tippe
d ca
theter
In
dex t
est u
sing
radi
al ar
tery
wav
efor
m
obta
ined
by r
adial
arte
ry ca
thet
erisa
tion
De
rived
aortic
vs. d
irect
aortic
augm
entat
ion in
dex
AIx %
mea
n diffe
renc
e (SD
): −5
.0 (8
.0)
Deriv
ed ao
rtic vs
. dire
ct ao
rtic B
P, m
ean d
iffere
nce
mmHg
(SD)
: SBP
: −8.0
(2.0)
; DBP
: 4.0
(2.0)
Pe
riphe
ral v
s. dir
ect a
ortic
BP,
mea
n diffe
renc
e mm
Hg (S
D): S
BP: 1
.0 (5
.0); D
BP: 1
.0 (2
.0)
Taka
zawa
(199
6)
Stud
y eva
luatio
n the
va
lidity
of a
trans
fer
functi
on be
twee
n as
cend
ing ao
rta an
d rad
ial
arter
y
Patie
nt se
lectio
n: N
on-co
nsec
utive
pa
tients
unde
rgoin
g diag
nosti
c ca
rdiac
cathe
terisa
tion (
20)
Inde
x tes
t: Un
know
n Au
tomate
d ton
omete
r (Je
ntow
7000
, Coli
n Med
ical In
strum
ents
Corp
) Ca
libra
ted, b
rach
ial cu
ff BP
Com
para
tor:
Osc
illome
tric cu
ff bloo
d pre
ssur
e (Co
lin JE
NTOW
7000
ton
omete
r) Re
fere
nce s
tand
ard:
Cath
eter (
Milla
r Mikr
o-Tip
cathe
ter),
asce
nding
aorta
Outco
mes d
erive
d usin
g a tr
ansd
ucer
-tippe
d ca
theter
In
dex t
est u
sing
radi
al ar
tery
wav
efor
m
obta
ined
by a
rteria
l ton
omet
ry w
ith ap
plica
ble
calib
ratio
n
Deriv
ed ao
rtic vs
. dire
ct ao
rtic au
gmen
tation
inde
x AI
x diffe
renc
e betw
een m
eans
: −9.0
De
rived
aortic
vs. d
irect
aortic
BP,
diffe
renc
e be
twee
n mea
ns: S
BP: −
11.0;
DBP
: 8.0
Perip
hera
l vs.
direc
t aor
tic B
P, di
ffere
nce b
etwee
n me
ans:
SBP:
−2.0
; DBP
: 5.0
Abbr
eviat
ions:
AIx,
augm
entat
ion in
dex;
BP, b
lood p
ress
ure;
SBP,
systo
lic bl
ood p
ress
ure;
DBP,
dias
tolic
blood
pres
sure
; MAP
, mea
n arte
rial p
ress
ure;
PP, p
ulse p
ress
ure;
TF, tr
ansfe
r fun
ction
; CA,
coro
nary
angio
grap
hy; C
C,
card
iac ca
theter
isatio
n. a C
ustom
tran
sfer f
uncti
ons d
evelo
ped a
t the
Car
diova
scula
r Res
earch
Cen
tre, M
onas
h Med
ical C
entre
and M
onas
h Univ
ersit
y. b P
erce
ntage
erro
r of th
e mea
n per
centa
ge di
ffere
nce (
perce
ntage
SD)
.

SphygmoCor system 67
Tabl
e 30
C
hara
cter
istic
s an
d re
sults
of t
he in
clud
ed s
tudy
of t
he S
phyg
moC
or s
yste
m in
spu
rious
sys
tolic
hyp
erte
nsio
n of
you
th
Stud
y,
auth
or/s
, de
sign
Popu
latio
n (N
)
Inde
x te
st,
com
para
tor,
refe
renc
e st
anda
rd
Stud
y ou
tcom
es (S
D)
Stud
y qu
ality
1. Bl
ood
pres
sure
as
sess
men
ts (m
mHg
): Sp
uriou
s hyp
erte
nsion
of
yout
h:
Brac
hial S
BP: 1
47.3
(2)a
Brac
hial D
BP: 7
0 (2.2
)b Ao
rtic S
BP: 1
15.9
(1)a,b
Ao
rtic D
BP: 7
0 (2.5
)b Am
plific
ation
pres
sure
: 31.4
(1
.5)a,b
Norm
oten
sive
male
s: Br
achia
l SBP
: 120
.5 (1
.3)
Brac
hial D
BP: 6
9.9 (1
) Ao
rtic S
BP: 1
00 (1
.5)
Aortic
DBP
: 71 (
1)
Ampli
ficati
on pr
essu
re: 2
0.5
(1.36
)
Esse
ntial
hyp
erte
nsive
male
s: Br
achia
l SBP
: 152
(2.6)
Br
achia
l DBP
: 96.5
(1.4)
Ao
rtic S
BP: 1
38.8
(2.5)
Ao
rtic D
BP: 9
8 (1.4
) Am
plific
ation
pres
sure
: 14
(0.9)
2. Au
gmen
tatio
n in
dex:
Sp
uriou
s hyp
erten
sion o
f yo
uth:
AIx (
%):
−8 (3
)b
Norm
otens
ive m
ales:
AIx (
%):
−4 (
1.4)
Esse
ntial
hype
rtens
ive m
ales:
AIx (
%):
17 (1
.9)
3. He
art r
ate:
Sp
uriou
s hyp
erten
sion o
f yo
uth:
HR (p
er m
in):
61.1
(1.9)
a,b
Norm
otens
ive m
ales:
HR (p
er m
in):
68.3
(1.65
)
Esse
ntial
hype
rtens
ive m
ales:
HR (p
er m
in): 7
2.4 (3
.2)
Mahm
ud &
Fee
ly (2
003)
Ca
se co
ntrol
study
re
portin
g Sp
hygm
oCor
sy
stem
meas
urem
ents
Patie
nt se
lectio
n:
Medic
al stu
dents
ag
ed 23
+ 0.
5 ye
ars (
174)
Un
treate
d male
s wi
th es
senti
al hy
perte
nsion
(22)
Inde
x tes
t: Sp
hygm
oCor
Ra
dial a
rtery
wave
forms
ac
quire
d by
appla
natio
n tom
ogra
phy
calib
rated
to
Oscil
lometr
ic cu
ff BP
(Omr
on m
odel
HE
M-70
5 CP)
Co
mpa
rato
r: No
ne
Refe
renc
e st
anda
rd: N
one
4. Ti
me t
o re
flect
ed w
ave:
Sp
uriou
s hyp
erten
sion o
f yo
uth:
Tr (m
sec)
: 160
(8)b
Norm
otens
ive m
ales:
Tr (m
sec)
: 152
(2.3)
Esse
ntial
hype
rtens
ive m
ales:
Tr (m
sec)
: 142
(1.6)
P1, Q
3 Ap
plica
bility
: App
licab
le
Quali
ty: Lo
w W
rong
outco
mes r
epor
ted;
no re
feren
ce st
anda
rd
Abbr
eviat
ions:
AIx,
augm
entat
ion in
dex;
BP, b
lood p
ress
ure;
DBP,
dias
tolic
blood
pres
sure
; HR,
hear
t rate
; SBP
, sys
tolic
blood
pre
ssur
e; SD
, stan
dard
devia
tion;
Tr, ti
me to
refle
cted w
ave.
a Com
pare
d with
norm
otens
ive m
ales (
p < 0.
01).
b Com
pare
d with
hype
rtens
ive m
ales (
p < 0.
01).
68 SphygmoCor system
Appendix G Supplementary study
A potentially relevant study in regard to indirect evidence for the use of the SphygmoCor system in spurious systolic hypertension of youth was not detected using the literature search. This study was conducted in an appropriate population and reported measurement of waveform parameters using the SphygmoCor system, but without reference standard validation. This study did not report appropriate outcomes for the determination of diagnostic accuracy for spurious systolic hypertension of youth. This study reported brachial cuff and derived aortic blood pressures in a population of young healthy individuals. The details of this study are shown in Table 31.
McEniery et al (2005) examined a group of 1008 healthy young university students of both sexes. These researchers identified a subset of subjects with isolated systolic hypertension. The characteristics of these individuals were compared with those who were normotensive or had essential hypertension; a further group of patients with high-normal blood pressure readings were excluded from the analysis. Those with spurious systolic hypertension of youth were significantly taller than both people who were normotensive and people with essential hypertension. They also had significantly increased weight and BMI when compared with those who were normotensive. The spurious systolic hypertension of youth subjects also had significantly decreased heart rates when compared with people with essential hypertension. The SphygmoCor system also identified differences in the derived aortic waveform characteristics between these three groups of subjects.
Those with spurious systolic hypertension of youth had significantly higher blood pressure measurements, both in the peripheral and aortic arteries, compared with the normotensive group. The spurious systolic hypertension of youth subjects also had significantly lower peripheral diastolic blood pressure and lower aortic systolic and diastolic blood pressures than those with essential hypertension, while having increased pulse pressure and peripheral systolic blood pressure.
The augmentation index was significantly lower in the spurious systolic hypertension of subjects when compared with either of the other two groups. Additionally, these subjects also had significantly increased pulse pressure amplification when compared with those with essential hypertension.
The data from McEniery et al (2005) shows similar trends to the data presented by Mahmud and Feely (2003) (Appendix E). Both papers indicate that people with spurious systolic hypertension of youth have significant differences in blood pressure measurements and haemodynamic variables when compared with people with normotension and essential hypertension.
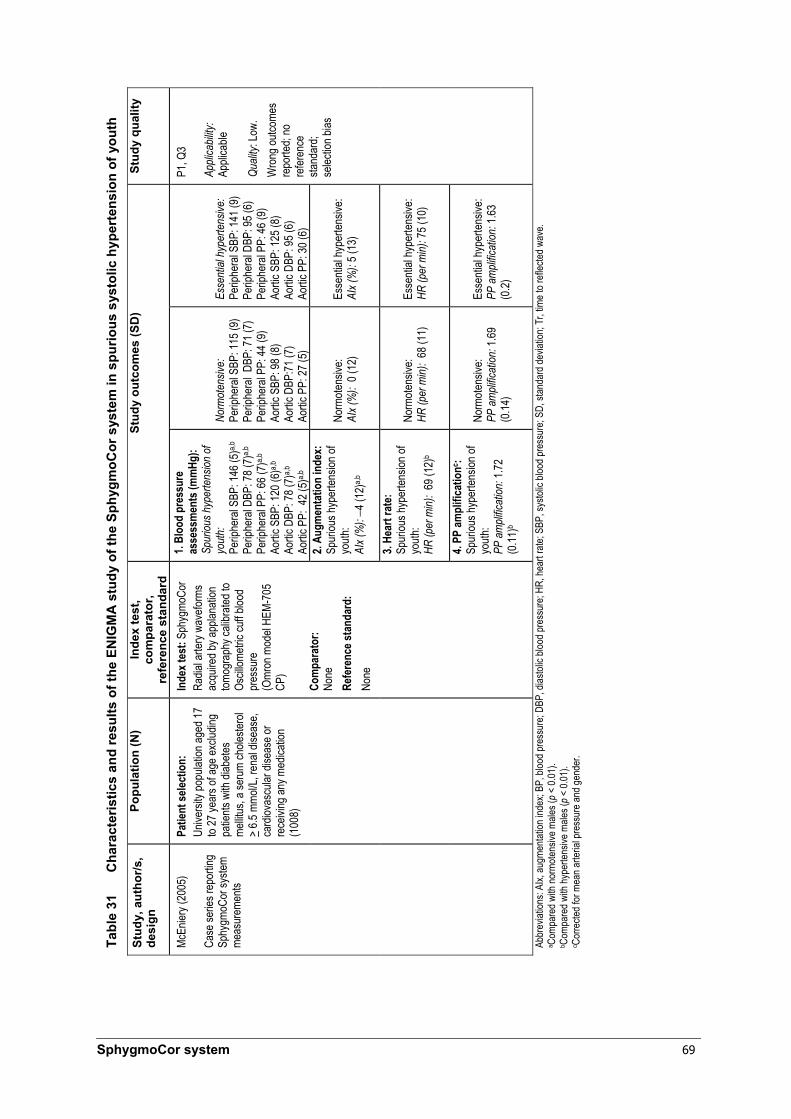
SphygmoCor system 69
Tabl
e 31
C
hara
cter
istic
s an
d re
sults
of t
he E
NIG
MA
stu
dy o
f the
Sph
ygm
oCor
sys
tem
in s
purio
us s
ysto
lic h
yper
tens
ion
of y
outh
Stud
y, a
utho
r/s,
desi
gn
Popu
latio
n (N
) In
dex
test
, co
mpa
rato
r, re
fere
nce
stan
dard
Stud
y ou
tcom
es (S
D)
Stud
y qu
ality
1. Bl
ood
pres
sure
as
sess
men
ts (m
mHg
): Sp
uriou
s hyp
erte
nsion
of
yout
h:
Perip
hera
l SBP
: 146
(5)a,b
Pe
riphe
ral D
BP: 7
8 (7)
a,b
Perip
hera
l PP:
66 (7
)a,b
Aortic
SBP
: 120
(6)a,b
Ao
rtic D
BP: 7
8 (7)
a,b
Aortic
PP:
42 (
5)a,b
Norm
oten
sive:
Pe
riphe
ral S
BP: 1
15 (9
) Pe
riphe
ral D
BP: 7
1 (7)
Pe
riphe
ral P
P: 44
(9)
Aortic
SBP
: 98 (
8)
Aortic
DBP
:71 (7
) Ao
rtic P
P: 27
(5)
Esse
ntial
hyp
erte
nsive
: Pe
riphe
ral S
BP: 1
41 (9
) Pe
riphe
ral D
BP: 9
5 (6)
Pe
riphe
ral P
P: 46
(9)
Aortic
SBP
: 125
(8)
Aortic
DBP
: 95 (
6)
Aortic
PP:
30 (6
) 2.
Augm
enta
tion
inde
x:
Spur
ious h
yper
tensio
n of
youth
: AI
x (%
): −4
(12)
a,b
Norm
otens
ive:
AIx (
%):
0 (1
2)
Esse
ntial
hype
rtens
ive:
AIx (
%):
5 (13
)
3. He
art r
ate:
Sp
uriou
s hyp
erten
sion o
f yo
uth:
HR (p
er m
in):
69 (1
2)b
Norm
otens
ive:
HR (p
er m
in):
68 (1
1)
Esse
ntial
hype
rtens
ive:
HR (p
er m
in): 7
5 (10
)
McEn
iery (
2005
) Ca
se se
ries r
epor
ting
Sphy
gmoC
or sy
stem
meas
urem
ents
Patie
nt se
lectio
n:
Unive
rsity
popu
lation
aged
17
to 27
year
s of a
ge ex
cludin
g pa
tients
with
diab
etes
mellit
us, a
seru
m ch
oleste
rol
> 6.5
mmo
l/L, r
enal
disea
se,
card
iovas
cular
dise
ase o
r re
ceivi
ng an
y med
icatio
n (1
008)
Inde
x tes
t: Sp
hygm
oCor
Ra
dial a
rtery
wave
forms
ac
quire
d by a
pplan
ation
tom
ogra
phy c
alibr
ated t
o Os
cillom
etric
cuff b
lood
pres
sure
(O
mron
mod
el HE
M-70
5 CP
) Co
mpa
rato
r:
None
Re
fere
nce s
tand
ard:
No
ne
4. PP
ampl
ifica
tionc :
Spur
ious h
yper
tensio
n of
youth
: PP
am
plific
ation
: 1.72
(0
.11)b
Norm
otens
ive:
PP a
mpli
ficat
ion: 1
.69
(0.14
)
Esse
ntial
hype
rtens
ive:
PP a
mpli
ficat
ion: 1
.63
(0.2)
P1, Q
3 Ap
plica
bility
: Ap
plica
ble
Quali
ty: Lo
w.
Wro
ng ou
tcome
s re
porte
d; no
re
feren
ce
stand
ard;
selec
tion b
ias
Abbr
eviat
ions:
AIx,
augm
entat
ion in
dex;
BP, b
lood p
ress
ure;
DBP,
dias
tolic
blood
pres
sure
; HR,
hear
t rate
; SBP
, sys
tolic
blood
pres
sure
; SD,
stan
dard
devia
tion;
Tr, ti
me to
refle
cted w
ave.
a Com
pare
d with
norm
otens
ive m
ales (
p < 0.
01).
b Com
pare
d with
hype
rtens
ive m
ales (
p < 0.
01).
c Cor
recte
d for
mea
n arte
rial p
ress
ure a
nd ge
nder
.
70 SphygmoCor system
Abbreviations
ABPM ambulatory blood pressure monitoring
AIHW Australian Institute of Health and Welfare
AIx augmentation index
AUC area under the curve
BP blood pressure
CAD coronary artery disease
DBP diastolic blood pressure
DOR diagnostic odds ratio
DPTI diastolic pressure time index
ECG electrocardiograph/ electrocardiography
HR heart rate
LR likelihood ratio
LVEF left ventricular ejection fraction
MBS Medicare Benefits Schedule
MSAC Medical Services Advisory Committee
NHMRC National Health and Medical Research Council
PP pulse pressure
PPICO population, prior tests, index test, comparators, outcomes
PTT pulse transit time
PWA pulse waveform analysis
PWV pulse wave velocity
RA renal artery
ROC receiver-operating characteristic
SBP systolic blood pressure
SEVR subendocardial viability ratio
Sn sensitivity
Sp specificity
TGA Therapeutic Goods Administration
Tr time to pressure wave reflection
TTI tension time index

SphygmoCor system 71
References
A clinical guide: pulse wave analysis [Internet]. http://www.atcormedical.com/users_guide.html [Accessed 28 June 2005].
Alderson P, Green S, Higgins JPT [eds.] (2005). Cochrane Reviewers’ Handbook 4.2.3 [updated November 2004]. John Wiley & Sons Ltd, Chichester, UK.
Australian Heart Foundation (2004). Hypertension management guide for doctors. National Heart Foundation of Australia, Australia.
Australian Institute of Health and Welfare: Mathur S (2002). Epidemic of coronary heart disease and its treatment in Australia. Australian Institute of Health and Welfare, Canberra.
Australian Institute of Health and Welfare (2004a). Heart, stroke and vascular diseases: Australian Facts 2004. AIHW; National Heart Foundation of Australia; National Stroke Foundation of Australia, Canberra.
Australian Institute of Health and Welfare (2004b). National cardiovascular disease and diabetes database [Internet]. http://www.aihw.gov.au/cvdhtml/cvd-menu.cfm [Accessed 9 May 2005b].
Blacher J, Guerin AP, Pannier BM, Marchais SJ, Safar ME, London GM (1999). ‘Impact of aortic stiffness on survival in end-stage renal disease’. Circulation. 99 (18): 2434–2439.
Bos WJ, Bruin S, van O, Keur I, Wesseling KH, Westerhof N, Krediet RT, Arisz LA (2000). ‘Cardiac and hemodynamic effects of hemodialysis and ultrafiltration’. American Journal of Kidney Diseases. 35 (5): 819–826.
Boutouyrie P, Tropeano AI, Asmar R, Gautier I, Benetos A, Lacolley P, Laurent S (2002). ‘Aortic stiffness is an independent predictor of primary coronary events in hypertensive patients: A longitudinal study’. Hypertension. 39 (1): 10–15.
Briganti EM, Shaw JE, Chadban SJ, Zimmet PZ, Welborn TA, McNeil JJ, Atkins RC (2003). ‘Untreated hypertension among Australian Adults: The 1999–2000 Australian diabetes, obesity and lifestyle study (AusDiab)’. Medical Journal of Australia 179 (3): 135–139.
Chen CH, Nevo E, Fetics B, Pak PH, Yin FC, Maughan WL, Kass DA (1997). ‘Estimation of central aortic pressure waveform by mathematical transformation of radial tonometry pressure. Validation of generalised transfer function’. Circulation. 95 (7): 1827–1836.
Cloud GC, Rajkumar C, Kooner J, Cooke J, Bulpitt CJ (2003). ‘Estimation of central aortic pressure by SphygmoCor requires intra-arterial peripheral pressures’. Clinical Science. 105 (2): 219–225.
Cruickshank K, Riste L, Anderson SG, Wright JS, Dunn G, Gosling RG (2002). ‘Aortic pulse-wave velocity and its relationship to mortality in diabetes and glucose intolerance: An integrated index of vascular function’. Circulation. 106 (16): 2085–2090.
72 SphygmoCor system
Davies JI, Band MM, Pringle S, Ogston S, Struthers AD (2003). ‘Peripheral blood pressure measurement is as good as applanation tonometry at predicting ascending aortic blood pressure’. Journal of Hypertension. 21 (3): 571–576.
Dunstan D, Zimmet P, Welborn T, Sicree R, Armstrong T, Atkins R, Cameron A, Shaw J, Chadban S (2001). Diabesity and associated disorders in Australia. International Diabetes Institute. Melbourne, Australia.
Fetics B, Nevo E, Chen CH, Kass DA (1999). ‘Parametric model derivation of transfer function for non-invasive estimation of aortic pressure by radial tonometry’. IEEE Transactions on Biomedical Engineering. 46 (6): 698–706.
Hope SA, Meredith IT, Cameron JD (2004). ‘Effect of non-invasive calibration of radial waveforms on error in transfer-function-derived central aortic waveform characteristics’. Clinical Science. 107 (2): 205–211.
Hope SA, Tay DB, Meredith IT, Cameron JD (2003a). ‘Use of arterial transfer function for the derivation of aortic waveform characteristics’ [Author’s reply]. Journal of Hypertension. 21 (11): 2197–2199.
Hope SA, Tay DB, Meredith IT, Cameron JD (2003b). ‘Use of arterial transfer functions for the derivation of aortic waveform characteristics’. Journal of Hypertension. 21 (7): 1299–1305.
Hunt S, Baker DW, Chin MH, Cinquegrani MP, Feldman AM, Francis GS, Ganiats TG, Goldstein S, Gregoratos G, Jessup ML, Noble RJ, Packer M, Silver MA, Stevenson LW (2001). ACC/AHA guidelines for the evaluation and management of chronic heart failure in the adult: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to revise the 1995 guidelines for the evaluation and management of heart failure). [Internet]. http://www.acc.org/clinical/guidelines/failure/hf_index.htm [Accessed 28 June 2005].
Laurent S, Boutouyrie P, Asmar R, Gautier I, Laloux B, Guize L, Ducimetiere P, Benetos A (2001). ‘Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients’. Hypertension. 37 (5): 1236–1241.
Lefevre FV, Aronson N (2001). Ambulatory blood pressure monitoring for adults with elevated office blood pressures. Blue Cross and Blue Shield Association. USA.
London GM, Blacher J, Pannier BM, Guerin AP, Marchais SJ, Safar ME (2001). ‘Arterial wave reflections and survival in end-stage renal failure’. Hypertension. 38 (3): 434–438.
Mahmud A, Feely J (2003). ‘Spurious hypertension of youth: fit young men with elastic arteries’. American Journal of Hypertension. 16 (3): 229–232.
McEniery CM, Yasmin, Wallace S, Maki-Petaja K, McDonnell B, Sharman JE, Retallick C, Franklin SS, Brown, MJ, Lloyd RC, Cockcroft JR, Wilkinson IB (2005). ‘Increased stroke volume and aortic stiffness contribute to isolated systolic hypertension in young adults’. Hypertension. 46 (1): 221–226.
Medical Services Advisory Committee (2004). Guidelines for the assessment of diagnostic technologies. Commonwealth of Australia. Canberra.
SphygmoCor system 73
Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF (1999). ‘Improving the quality of reports of meta-analyses of randomised controlled trials: the QUOROM statement, quality of reporting of meta-analyses’. The Lancet 354 (9193): 1896–1900.
Mowatt G, Vale L, Brazzelli M et al (2004). ‘Systematic review of the effectiveness and cost-effectiveness, and economic evaluation, of myocardial perfusion scintigraphy for the diagnosis and management of angina and myocardial infarction’. Health Technology Assessment 8: 30.
NHMRC (2005). NHMRC additional levels of evidence and grades for recommendations for developers of guidelines. National Health and Medical Research Council.
Nichols WW, O’Rourke MF, in McDonald’s Blood Flow in Arteries: Theoretical, Experimental and Clinical Principles 2005. Hodder Arnold. London, UK.
O’Rourke MF (1999). ‘Mechanical principles. Arterial stiffness and wave reflection’. Pathologie Biologie. 47 (6): 623–633.
O’Rourke MF, Vlachopoulos C, Graham RM (2000). ‘Spurious systolic hypertension in youth’. Vascular Medicine 5 (2): 141–145.
Pannier BM, Avolio AP, Hoeks A, Mancia G, Takazawa K (2002). ‘Methods and devices for measuring arterial compliance in humans’. American Journal of Hypertension. 15 (8): 743–753.
Pauca AL, O’Rourke MF, Kon ND (2001). ‘Prospective evaluation of a method for estimating ascending aortic pressure from the radial artery pressure waveform’. Hypertension. 38 (4): 932–937.
Safar ME, Blacher J, Pannier BM, Guerin AP, Marchais SJ, Guyonvarch PM, London GM (2002). ‘Central pulse pressure and mortality in end-stage renal disease’. Hypertension. 39 (3): 735–738.
Smulyan H, Siddiqui DS, Carlson RJ, London GM, Safar ME (2003). ‘Clinical utility of aortic pulses and pressures calculated from applanated radial-artery pulses’. Hypertension. 42 (2): 150–155.
Soderstrom S, Nyberg G, O’Rourke MF, Sellgren J, Ponten J (2002). ‘Can a clinically useful aortic pressure wave be derived from a radial pressure wave?’ British Journal of Anaesthesia. 88 (4): 481–488.
Takazawa K, O’Rourke MF, Fujita M et al (1996). ‘Estimation of ascending aortic pressure from radial arterial pressure using a generalised transfer function’. Zeitschrift für Kardiologie. 85 Suppl 3: 137–139.
The Cardiac Society of Australia & New Zealand (2002). Guidelines on the contemporary management of the patient with chronic heart failure in Australia. National Heart Foundation of Australia, Australia.
Weber T, Auer J, O’Rourke MF et al (2004). ‘Arterial stiffness, wave reflections, and the risk of coronary artery disease’. Circulation. 109 (2): 184–189.
Woodman RJ, Watts GF (2003). ‘Measuring arterial stiffness in diabetic patients’. Practical Diabetes International 20 (1): 25–30.





![UIHC Home Sleep Apnea Testing (HSAT) · 2018-10-12 · portable sleep-testing device (Peripheral Arterial Tonometry [PAT®]) and those measured by PSG. • Methods: 14 studies qualified](https://static.fdocuments.in/doc/165x107/5f792a255f98132bd25e45a4/uihc-home-sleep-apnea-testing-hsat-2018-10-12-portable-sleep-testing-device.jpg)