Complications Associated with Laparoscopic Adjustable Gastric Banding for Morbid Obesity
description

APRIL 2003, VOL 77, NO 4
Home Study Program PERIOPERATWE CARE OF THE MTIENT WITH MORBID OBESITY
he article “Perioperative care of the patient with morbid obesity” is the basis for this AORN Journal independent study. The behav- ioral objectives and examination for this program were prepared by Rebecca Holm, RN, MSN, CNOR, clinical editor, with con- sultation from Susan Bakewell, RN, MS, education program pro-
fessional, Center for Perioperative Education. A minimum score of 70% on the multiple-choice examination is
necessary to earn 4.6 contact hours for this independent study. Participants receive feedback on incorrect answers. Each applicant who successfully completes this study will receive a certificate of comple- tion. The deadline for submitting this study is April 30,2006.
Send the completed application form, multiple-choice examination, learner evaluation, and appropriate fee to
AORN Customer Service c/o Home Study Program
2170 S Parker Rd, Suite 300 Denver, CO 8023 1-57 1 1
or fax the information with a credit card number to (303) 750-32 12.
BEHAVIORAL OBJECTWES After reading and studying the article on perioperative care of the
patient with morbid obesity, the nurse will be able to (1 ) describe overnutrition, (2) compare medical and surgical treatment options for patients with
morbid obesity, (3) define nursing considerations of caring for a patient undergoing
surgery for morbid obesity, (4) differentiate between the types of surgical procedures available to
treat morbid obesity, and (5) describe the postoperative course of a patient after having under-
gone surgical treatment for morbid obesity.
This program meets criteria for CNOR and CRNFA recertification, as well as other continuing education requirements.
80 1 AORN JOURNAL

APRIL 2003, VOL 77, NO 4 Graling Elariny
Perioperative Care of the Patient with Morbid Obesity
besity is the underlying pathogenesis of a number of disease processes that are among the top causes of mortality in industrialized societies. Recently, it has been called an 0 epidemic.' In the United States, more than
60% of adults are overweight.' Obesity differs great- ly from morbid obesity. Although obesity and morbid obesity share numerous etiological factors (eg, genet- ic, environmental, psychosocial, economic), accepted treatment options differ. Obesity deserves attention and treatment to prevent potential complications. Morbid obesity, however, requires urgent and defini- tive correction to treat both current and possible future complications and to help prevent a probable shortened lifespan. Currently, therapy for obesity and obesity-related medical conditions costs nearly $1 trillion dollars per decade in the United States alone.'
CLASSIFICATIONS OF OVBRNUTRmON States of overnutrition are classified based on
body mass index (BMI). This is calculated by dividing a person's weight in kilograms by his or her height in
of the categories of overnutrition as described by the American Society of Bariatric Surgery (ASBS) and the National Institutes of Health (NIH)?
Using BMI as a measure of obesity can be mis- leading for very muscular people or people with little to no central or abdominal fat. This problem, however, is limited to people with BMIs less than 35. When a person reaches a BMI greater than 35, measurements such as waist to hip ratio and sagittal abdominal diam- eter become less important.' Patients are considered candidates for surgical treatment if they previously failed at medical weight loss attempts and are current- ly severely obese (ie, BMI > 35) with one or more associated comorbidities or morbidly obese (ie, BMI > 40) with or without comorbidities.
EfJ i f s of obesity on body systems. Obesity adversely affects almost all body systems and has been associated with increased risk for a number of malignancies. Table 2 lists those conditions and comorbidities that occur more frequently in people who are obese. This clearly supports the justifica- tion that care providers should aggressively treat
meters squared. Table 1 provides a simplified version morbid obesity.
A B S T R A C T Obesity recently has been called an epidemic. In the United
States, more than 60% of adults are overweight. Although obesity and morbid obesity share numerous etiological factors (eg, genetic, environmental, psychosocial, economic), accepted treatment options differ. Morbid obesity requires urgent and definitive correc- tion to treat both current and possible future complications and to help prevent a probable shortened lifespan. Generally, it is accept- ed that nonsurgical approaches to weight loss for a person who is morbidly obese are unsuccessful. This Home Study describes the major surgical procedures currently available to treat morbid obesi- ty and discusses the information that nurses need to know about perioperative care of patients who are morbidly obese. AORN J 77 (April 2003) 802-81 9.
COMPARlSON OF MEDICAL VERSUS SURGICAL TREATMENT
Few people who are obese have benefited from medical attempts at excess body weight loss. Medical weight loss for peo- ple who are morbidly obese has a 95% failure rate and is extremely unlikely to provide sustained results, reduction of morbidity, or improved survival. Generally, it is accepted that nonsurgical approaches to weight loss for a person who is morbidly obese consistently are unsuccessful. No
P A U L A G R A L I N G , R N ; H A Z E M E L A R I N Y , M D
802 AORN JOURNAL

APRIL 2003, VOL 77, NO 4 Gmling Elariny
intervention, other than surgery, has provided any meaningful long-term success. This includes diet- ing, exercise regimens, psychotherapy, or prescrip- tion medications. The consensus, therefore, is that for a person who is morbidly obese, surgery is the only known effective treatment6
Success rate. Almost all available surgical interventions result in an approximately 70% excess body weight loss during the first year.’ Rather than facing a 95% failure rate for nonsurgical excess body weight loss interventions, the patient can be offered a range of surgical interventions that offer greater than 90% long-term success when using 35% excess body weight loss as the cutoff for suc- cess. When using 50% excess body weight loss as the cutoff, the success rate still is better than 70%, even for purely restrictive procedures. With bypass procedures and biliopancreatic diversion, success is even greater.
Complications. The international registry of bariatric surgeries provides data regarding surgical mortality and complications. Statistics demonstrate an overall surgical mortality of 0.17% for patients undergoing bariatric surgery and a complication rate of only 8.5%.8 Considering patients’ preexisting conditions and the risks these patients automatical- ly bring with them to the OR, these statistics repre- sent very low numbers, suggesting that surgical intervention not only is safe but also much safer than lack of intervention. Failure to intervene surgi- cally for these patients undoubtedly results in prom- ulgation of their comorbidities with eventual mor- bidity and early mortality.
For these reasons, people who are morbidly obese are candidates for surgical intervention. These surgical interventions have low morbidity and mortality and provide a significant and sus- tained excess body weight loss with reduction of comorbidity rates and improvement in both survival and quality of life for the patient.
SURGICAL APPROACHES TO THE TREATMENT OF MORBID OBESITY
At Inova Fairfax Hospital, Falls Church, Va, the approach to surgical treatment of morbid obesi- ty is patient centered; therefore, no particular weight loss procedure is preferred in comparison to another. A person who is morbidly obese has the right to choose between reasonably equal treatment options. All procedures currently available in the United States and generally accepted in the bariatric
Table 1 CLASSIFICATION OF WEIGHT BODY MASS INDEX (BMI)‘
BMI* Cateaorv < 18.5 Underweight
18.5 to 24.99 Normal
25 to 26.9 Overweight
27 to 30 Mild obesity
31 to35
36 to 40
Moderate obesity
Severe obesity
41 to45 Morbid obesity
> 50 Super obesity
* Measured in kilograms per meter squared
NOTE
and treatment of overweight and obesity in adults,’ National Institutes of Health, http://www.nhlbi.nih,gov /guidelines/obesity/ob-exsum.pdf (accessed 30 Jan 2003).
1. “Clinical guidelines on the identification, evaluation,
surgical community are offered to patients seeking primary treatment for their condition. Many patients are extensively self-educated about their condition and the available options and present with the deci- sion already made regarding the specific procedure desired. Others are unsure at the time of presenta- tion and have done little research on their own to learn about their options. Regardless of presenta- tion, staff members educate patients extensively regarding the history of bariatric surgical proce- dures and the evolution of procedures as a result of outcomes and complications. Patients are informed about procedures currently available in the United States and procedures or devices not available in the United States. Each surgical option is analyzed carefully, and pros, cons, risks, and benefits are dis- cussed in light of short- and long-term results, weight loss, vitamin and malnutrition risks, and early and late complication rates. Patients are told that the decision primarily is theirs to make, but that the decision should be based on
their specific physiology, their personal and health goals, a sound understanding of their eating behaviors, the etiology of their obesity (ie, source of excess caloric intake),
803 AORN JOURNAL

APRIL 2003, VOL 77, NO 4 Gruling Elurin!
Table 2 OBESlW-SPEClFK COMOABlDmES '
Cardiovascular Atherosclerotic disease Congestive heart failure Hypertension Varicose veins Venous insufficiency and stasis
Dermatologic Cellulitis Dermatitis Necrotizing infections Panniculitis
Endocrineheta bolic Diabetes mellitus Glomerulosclerosis and renal failure Gout Hyperlipidernia
Gastrointestinal Abdominal wall hernia Fatly liver Gallbladder disease Gastroesophageal reflux disease Irritable bowel syndrome
Genitourinarv disease Dysmenorrhea Hirsuitism Infertility Polycystic ovarian disease
NOTE
Urinary stress incontinence
Malignancies Breast cancer Colorectal cancer Endometrial cancer Gallbladder cancer Ovarian cancer Pancreatic cancer Prostate cancer Uterine cancer
Musculoskeletal Bane demineralization Carpel tunnel syndrome Low back pain Osteoarthritis
Neuropsychiatric Depression Idiopathic intracranial hypertension Stroke
Ophthalmologic Cataracts Glaucoma
Pulmonary Asthma Obesity hypoventilation syndrome Pulmonary hypertension Sleep apnea
1 . F Pi-Sunyer, "Comarbidities of oveweight and obesity: Current evidence and research issues,' Medical Science Sports and Exercise 31 no 1 1 suppl (November 1999) 602-608.
their risk tolerance, and then excessive
undergone a number of different procedures. At the meeting, the preoperative patient has the opportunity to discuss particular concerns. Only after this process is complete is the patient actually given an appointment to see the surgeon for a physical examina- tion. After the patient has been examined by the surgeon, he or she undergoes specific preopera- tive testing, and then the surgery is scheduled. This allows the patient ample opportunity to con- template his or her options and to give truly informed consent.
CALORIC INTAKE The concept of weight bal-
ance or caloric equilibrium is based on the concept of basal metabolic rate, which says that each individual has a certain daily caloric need that will result in neither weight gain (ie, anabolism) nor weight loss (ie, catabolism). For most people, this is about 1,800 calories per day; however, for some it is less, and for others it is more.
The simplified basics of weight balance. Patients who have gained excess body weight have done so by consuming more calories than their body needs on a daily basis for a sustained period of time. If weight gain is ongoing,
intake is ongoing. Weight loss their ability to tolerate or accept the conse- quences or side effects of the particular proce- dures contemplated.
The preoperative educational process involves a full variety of medical personnel, including the patient's surgeon, a perioperative nurse, an anesthe- sia care provider, a dietician, and a psychologist. The surgeon oversees the process, which generally is in the form of a two-hour presentation followed by a question and answer session. Immediately after this educational and information-gathering session, the patient attends a support group meeting where he or she is able to interact with patients who have
~~
requires that intake or absorption of intake be reduced below metabolic need on a daily basis for a sustained period of time. This process achieves bal- ance when the patient's total body size requires fewer calories for maintenance, and the patient is capable of consuming and absorbing an adequate quantity and quality of nutrients postoperatively. Weight loss, therefore, stops when this equilibrium is achieved.
Reducing intake. How then can the caloric intake of a patient be reduced? The best approach is to determine where the excess calories are coming from and eliminate (ie, restrict) that source or pre- vent that source of excess calories from being
804 AORN JOURNAL

APRIL 2003, VOL 71, NO 4 Gmling Elariny
absorbed. To target these sources, patients’ excess caloric intake sources are categorized. These excesses are classified as
bloating-vereating or eating large meals; choosing-hoosing the wrong foods at each meal (eg, high fat, fried, high carbohydrate, low fiber); grazing4onstant snacking during the day and between meals or at night; and sweeting-frequent ingestion of high calorie sim- ple sugar-containing foods, drinks, or shakes.
Patients are asked to classify themselves to determine where their excess calories come from. If a patient reports that currently he or she does not con- sume excess calories, then the patient is asked where the excess calories came from in the past. Most patients can classify themselves into one or two cate- gories. Patients who report that they have had stable weight for more than one year likely truly have mod- ified their diets to reach balance. These patients are classified as normal to low metabolizers, depending on their reported caloric intake.
The best judge of a patient’s need is the patient. The only limiting factor is the patient’s knowledge base. When the patient determines the source of his or her excess calories, the appropriate procedure can be chosen. This process is accomplished cooperatively with the patient and his or her health care providers, who consider all factors contributing to the decision, including the patient’s weight loss goals, short and long-term risk tolerance, and side-effect tolerance.
pAnw SELECTION The most important factor in achieving success
in bariatric surgery is patient selection and interven- tion selection. Most patients who present for evalu- ation for bariatric surgical procedures are self- referred, determined to achieve change, and willing to make personal lifelong sacrifices to achieve their goals. Candidates who are not self-referred general- ly are reluctant, uncertain, and attached to certain eating behaviors (eg, binge eating, specific food addiction). These patients need to be counseled extensively before undergoing surgery. Table 3 pro- vides a glossary of terms common to many bariatric surgical procedures.
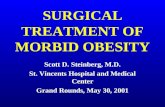
Anatomical and historical considerations. Figure 1 shows the normal anatomy of the gastroin- testinal tract. The esophagus is the first passageway into the stomach. Historically, interventions above or at the level of the esophagus have not been effec- tive for the treatment of morbid obesity. For exam-
Table 3 GLOSSARY OF BARIATRIC SURGICAL TERMS
Anastomosis A newly established connection between two hollow structures (ie, stomach to intestine, intestine to intestine, intestine to colon, bile duct to intestine). This con be a stapled, sewn, or mixed connection. Such connections con be end to end, end to side, or side to end. Band
~
A strip of tissue, mesh, tube, or device that is wrapped around the stomach, port of the stomach, or pouch thot serves to restrict the oufflow of food from one part of the stomach or the pouch to another part of the stomach or to on intestinal anastomosis,
Biliopancreatic limb The segment of smoll bowel that starts at the second portion of the duodenum where the bile duct enters the duodenum and ends when and where it enters into the Roux limb. This is the bile-carving limb.
Common channel The segment of smoll bowel thot starts where the bil- iopancreatic limb enters into the Roux limb and ends at the cecum. This is the segment where complex proteins, fats, and carbohydrates ore best digested.
Pouch The portion of the stomach that serves os o reservoir for food immediately after food exits the esophagus.
Roux limb The segment (ie, limb) of small bowel thot first receives food, starting where food enters it and ending where the biliopancreotic limb joins it.
Staple line A row of staples fired into the bowel or stomach by a sto- pling device. A staple line can be within an anastomosis, in a partition, or in o divided bowel end. One staple line sometimes is incorporated into another or into o fully hand-sewn anastomosis,
ple, wiring the teeth shut is ineffective because patients’ nutritional source becomes high-calorie liquids and shakes. Patients rapidly reach their homeostatic or baseline level of nutritional intake and, therefore, do not lose weight.
Some antireflux devices used in the past demon- strated that obstructive devices on the esophagus were fraught with complications, such as erosion and esophageal dilation. These devices, therefore, became a nonviable option.
The esophagogastric junction (EGJ) and its
805 AORN JOURNAL

APRIL 2003, VOL 77, NO 4 Graling - Eluriny
Figure 1 Normal anatomy of the gastrointestinal tract. All lengths are based on average findings of nearly 550 cm total small bowel length beyond the duodenum when measured laparoscoplcally and gently stretched.
physiological function to relax for food passage and tighten to prevent reflux is important. In patients with significant reflux disease, certain procedures should be avoided. The fundus of the stomach has a thin wall and a great propensity to stretch, so this portion of the stomach should not be used in the formation of a pouch. The body of the stomach produces acid and has a muscular digestive function for mixing chyme, so it is not ideal for use in formation of a pouch.
The lesser curvature of the stomach is the thick- er walled portion of the stomach that has less propen- sity to stretch and is more fixed in position. The pylorus (ie, stomach outlet) is important in
regulating the output of the stomach to properly limit acid output into the duodenum, controlling chyme and other fluid output from the stomach, and preventing bile reflux between meals.
Denervation of the pylorus results in spasm and obstruction. Disabling (ie, through pyloroplasty or pyloromyotomy) or bypassing the valve results in dumping syndrome because of unregulated emptying of high solute concentration liquids, specifically sweets, into the small bowel. Dumping syndrome is defined as a symptom complex usually occurring with sweet or sugar intake after a procedure that oblit- erates or bypasses the function of the pyloric sphinc- ter. Symptoms can include faintness, palpitations, nausea vomiting, low blood pressure, sweating, mild to explosive diarrhea, or pain.
The antrum (ie, lower one-third of the stomach) is important for two main reasons. First, it harbors G cells that secrete gastrin, which is a paracrine and endocrine hormone that stimulates acid production. This is important when considering the larger pouch of the biliopancreatic diversion procedure without duodenal switch in which the endocrine gastrin effects can increase pouch acid production and increase the rate of ulceration if the antrum is not removed. This is why a distal gastrectomy is recommended with larger pouch procedures, such as biliopancreatic diversion without duodenal switch. The acid also is important when considering the duodenal switch procedure (ie, longitudinal or lateral gastrectomy with preservation of the pylorus and anastomosis to the duodenum) in which preservation of antral acidification helps con- vert dietary iron to its absorbable oxidized ferric form. Parietal cells in the antrum also produce an intrinsic factor, a protein necessary for B,, absorption in the ileum. The duodenum is important in the secretion of a number of hormones, including secretin, cholecys- tokinin, and enteroglucagon. Leaving the duodenum in the digestive food channel is believed to allow for more normal gastrointestinal hormonal response to meals, which helps provide an improved physiological response to meals and improved satisfaction.
The bile duct, main pancreatic duct, and accesso- ry pancreatic ducts illustrate the anatomical and surgi- cal hazards associated with performance of the duode- nal switch procedure and allow for an understanding of its mechanism. Portions of the small bowel are shown with their approximate unstretched lengths to allow for understanding the sections of intestinal tract used in various parts of the surgical procedures.
NURSING CONSIDERATIONS It is important that perioperative team members
be familiar with the needs of a patient undergoing bariatric surgery. Caregivers should consider the
808 AORN JOURNAL

APRIL 2003, VOL 77, NO 4 8 Graling 9 Elarinv
patient’s physical and psychological needs. Ap- propriately sized gowns and blood pressure cuffs, as well as stretchers, must be readily available so that the patient is made to feel welcome and not embarrassed by the lack of attention to his or her size require- ments. Additionally, specific education regarding psychological needs of patients who are morbidly obese is provided to preoperative personnel, includ- ing the registration clerk and holding area reception- ist. Patients often view this day as the first day of the rest of their lives. Unsolicited or inappropriate com- ments can spoil the experience for them, much the same as spoiling a wedding day. Comments such as “you don’t look like you need this surgery” or “oh, but you really do carry your weight well” may be offered as compliments but can be perceived nega- tively by the patient. The patient’s family members already may have accused the patient of taking the easy way out by having surgery. Inappropriate com- ments may be reminiscent of past accusations of lack of willpower or effort.
Preoperutivephuse. The patient usually is admit- ted to the hospital on the same day of surgery. He or she is escorted directly from the registration area to the preoperative holding area. In the preoperative holding area, the preoperative nurse asks the patient to change into a patient gown and wait on a stretcher for consult with perioperative team members. The preoperative nurse completes a patient assessment of vital signs, reviews laboratory work for variations in normal val- ues, and reviews the chart for completion of necessary paperwork (eg, signed consent form, surgeon’s history and physical examination).
The circulating nurse arrives from the OR to greet the patient in the preoperative holding area. He or she performs a brief assessment of factors affect- ing positioning, reviews the planned procedure, and gives the patient and family members an opportunity to ask questions. The circulating nurse then develops a care plan specific to this patient and the procedure being performed (Table 4). The patient remains in the preoperative holding area until the anesthesia care provider completes a preoperative assessment, places an IV line, and administers a preoperative dose of antibiotics. When the surgeon arrives and confirms the planned procedure, the anesthesia care provider notifies perioperative nursing team members and transports the patient to the OR.
Intruoperutive phase. If at all possible, preop- erative sedative medications are kept to a minimum to facilitate patient transfer from the stretcher to the
OR bed. When in the room, the patient is assisted with moving to the bed, which has specialized hydraulics and padding to accommodate a patient with morbid obesity. The anesthesia care provider usually elevates the head of the bed to assist with the patient’s respiratory effort. Awake positioning is pre- ferred, particularly if the patient has multiple joint limitations.
Positioning. Intraoperative team members work cooperatively to place the patient in the supine posi- tion on the bariatric OR bed. The circulating nurse places side bed attachments, if needed, for patients with extra-wide girth. The circulating nurse places a padded footboard on the foot of the bed to prevent the patient from slipping when the bed is placed in reverse Trendelenburg’s position.
The anesthesia care provider helps the patient extend his or her arms on arm boards, places padding under bony prominences, and secures the patient’s arm with cotton cast padding and hook and loop fas- tening straps. If the patient is undergoing a duodenal switch procedure, the circulating nurse tucks the patient’s left arm at his or her side to facilitate surgeon positioning during measurement of the small bowel limb segments.
The circulating nurse places a urinary catheter. Several assistants may be needed to provide retrac- tion of the panniculus and thighs for access during catheter placement.
The circulating nurse places sequential compres- sion devices on the patient’s lower legs and then places a pillow under the patient’s knees to reduce back strain. The nurse securely wraps the patient’s legs with a soft blanket to support the legs in a com- fortable position of thigh adduction with physiologi- cal external rotation and to avoid pressure on the lat- eral aspect of the lower leg and feet.
The circulating nurse places an electrosurgical grounding pad on the patient’s left lateral thigh and then places upper and lower temperature-regulating blankets to maintain the patient’s body temperature. Finally, the circulating nurse places two sets of safety straps, one across the patient’s lower legs and the other across his or her thighs.
Inducing anesthesia. Before induction of anes- thesia, the circulating nurse and anesthesia care provider question the patient about his or her comfort to ensure that tissue is not pinched and placement of extremities is comfortable. Anesthetic techniques are the same as for any other abdominal procedure. The anesthesia care provider continuously monitors the
809 AOKN JOURNAL

APRIL 2003, VOL 77 , NO 4 Graling Elariny 9
Table 4 NURSING CARE PIAN FOR A IP#TIEM UNDERGOING SURGERY FOR MORBID OBESITY
Nursing Interim Outcome diagnosis Interventions outcome criteria statement
Altered nutrition, more than body require- ments related to specific eating patterns
Risk for anxiety related to knowl- edge deficit and stress of surgery
Risk for altered pulmonary function related to morbid obesity and hypoventilation
Risk for acute or chronic pain related to surgical procedure
Risk for injury related to perioperative experience
Provides instruction to enhance patient's understanding of mechanism for weight loss and need for nutritional supplements.
Determines knowledge level, assesses readiness to learn, and identifies barriers to communication.
Explains sequence of events and reinforces teaching about treatment options.
Provides instruction (ie, verbal, written) for surgical pro- cedure and discharge based on age and identified need and ensures availability of support group interaction.
Communicates patient concerns to appropriate surgical team members.
Helps patient maintain self-esteem by obtaining appropriately sized items (eg, gowns, wide stretchers, fitted blood pressure cuff).
Evaluates response to instruction.
Assists with endotracheal intubation and ensures availabil- ity of difficult airway cart in the OR and continuous positive airway pressure machine in the postanesthesia care unit.
Monitors change in respiratory status.
Assess patient's pain preoperatively.
Identifies patient's accepted postoperative pain threshold.
Provides pain management instruction and pain scale to assess pain control.
Evaluates patient's response to pain management interventions.
Verifies patient's identity, allergies, NPO status, and informed consent. Assesses skin integrity, sensory impairments, and muscu- loskeletal status.
Transfers patient while awake using appropriate number of assistive personnel, implementing protective measures to prevent positioning injury, and maintaining correct body alignment.
Evaluates for signs and symptoms of injury.
The patient verbalizes understanding of altered nutrition.
The patient verbalizes
decreased anxiety and an ability to cope, understanding of individualized procedure and sequence of events, that questions have been answered, and
outcomes. expected
The patient is extubated within 24 hours postoperatively.
The patient demonstrates adequate pain management.
The patient's skin remains smooth and intact, and neuromuscular functions are maintained or improved from baseline.
The patient demonstrates knowledge of nutritional requirements for selected surgery.
The patient demonstrates knowledge of the expected response to the procedure and discharge care.
The patient par- ticipates in deci- sions affecting his or her plan of care.
The patient's pulmonary func- tion is consis- tent with or improved from baseline levels.
The patient demonstrates and reports ade- quate pain con- trol throughout the perioperative period.
The patient is free from posi- tioning injury from extraneous objects.
810 AORN JOURNAL

APRIL 2003, VOL 77, NO 4 8 Gruling Elariny -
patient’s vital signs, including pulse, blood pressure, electrocardiogram, pulse oximetry, and end-tidal car- bon dioxide. The anesthesia care provider anes- thetizes the patient using a balanced technique of IV induction and inhalation maintenance. Nitrous oxide generally is avoided, as with most laparoscopic pro- cedures, because it tends to diffuse into gas-filled organs. This dilates the organs intraoperatively, thereby obstructing the laparoscopic surgical view. Nonsteroidal anti-inflammatory drugs (NSAIDs) and corticosteroids also are avoided for hematologic and gastric reasons. For example, some NSAIDs, such as IV ketorolac, are avoided because they can cause gastric irritation and slow the healing process of the fresh gastric staple and suture lines. Additionally, routine use of dexamethasone is avoid- ed to prevent gastritis and problems with healing and to avoid confounding factors when evaluating the patient’s laboratory results. The circulating nurse ensures that an anesthesia cart specially stocked for management of difficult airways, including a rigid fiberoptic laryngoscope, is available in the room. After intubation, the anesthesia care provider emp- ties the patient’s stomach with a nasogastric tube. The anesthesia care provider takes special care to ensure the removal of all esophageal tubes during insertion of sizing tubes, such as bougie dilators.
Prepping and draping. The nurse documents the patient’s skin condition and measures used to prevent injury intraoperatively. The circulating nurse per- forms an abdominal prep, including the skin folds under the panniculus (ie, overhang of abdominal tis- sue). The circulating nurse ensures that the scrub per- son has extra draping towels, as needed. Surgical team members perform standard draping for an abdominal incision. The anesthesia care provider places the OR bed in reverse Trendelenburg’s posi- tion for easy access to the patient’s upper stomach. For large patients, surgical team members may need step stools to work within the sterile field.
AVAILABLE PROCEDURES Numerous surgical procedures are available to
treat morbid obesity. These procedures differ in their approach to anatomy and the desired outcome. Weight loss or bariatric surgeries describe a broad group of procedures whose subcategories include purely restrictive (ie, limiting the amount of food intake), gastric bypass, biliopancreatic diversion, purely mal- absorptive (ie, reduced calorie and nutrient absorp- tion), and neurostimulatory procedures (Table 5).
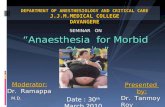
Vertical banded gastroplasty (VBC). Vertical banded gastroplasty is a purely restrictive procedure in which a small pouch (eg, approximately 15 mL to 30 mL) and a large liquid reservoir are created. No stomach tissue is removed. It is best suited for patients whose excess caloric intake source is bloat- ing. This procedure often fails with patients who are classified as grazers or whose excess caloric intake source is sweets. It offers a low malnutrition or vita- min deficiency risk (l%), and patients require only one multivitamin injection (MVI) daily. When suc- cessful, patients may expect a 60% excess body weight loss. Specific complications include esophagi- tis, band erosion, or staple line failure. If revision is needed as a result of liver or gastric scarring, an open procedure usually is necessary because the VBG may be difficult to revise (Figure 2).
Proximal gastric bypass. Proximal gastric bypass is considered a mostly restrictive procedure. Like the VBG, a small pouch is created without removal of stomach tissue. A small 1-cm anastomo- sis is created with an intestinal bypass using a 100- cm Roux limb, a short biliopancreatic limb, and an approximate 400-cm common channel. The proxi- mal gastric bypass works for patients who are clas- sified as sweeters and bloaters but can be overcome by patients who are classified as grazers. Patients have some dumping syndrome but usually have lit- tle acid reflux. When successful, a patient may expect 60% to 65% excess body weight loss. There is a low early failure rate, and 20% to 25% of patients experience a late (ie, after three years) weight gain of 20% to 30%. Specific complications include anastomotic ulcer and stricture and failures that are converted to a distal bypass or duodenal switch. (Figure 3 ) .
Distal gastric bypass. Distal gastric bypass is a partially restrictive and partially malabsorptive proce- dure. As with other restrictive procedures, a small pouch is created, and no stomach tissue is removed. The anastomosis is small (ie, 1 cm) with a long Roux limb, short biliopancreatic limb, and 100-cm com- mon channel. The distal bypass generally eliminates reflux but occasionally causes dumping. It is a viable option for patients who are classified as sweeters, grazers, and bloaters but can be overcome by persist- ent bad eating habits. There is a high malnutrition and vitamin deficiency risk with distal gastric bypass, and patients require 12 MVIs per day. Patients experience a 90% excess body weight loss with a low early fail- ure rate, but there is a possibility of mild weight
811 AORN JOURNAL

APRIL 2003, VOL 77, NO 4 * Grolirig * Elriinj*
Vertical banded gastroplasty Proximal gastric bypass Distal gastric bypass Small 15-mL to 30-mL pouch Features
(ie, 500 Large liquid reservoir pouch pouch cm un- No malabsorption Mostly restrictive Partially restrictive stretched Fails with sweeters and grazers Causes dumping syndrome Partly malabsorptive total bowel Best suited for bloaters Eliminates acid reflux Can possibly cause length) dumping syndrome
Small 15-mL to 30-mL Small 15-mL to 30-mL
May worsen reflux if poor lower eso-
No stomach removed
Works for sweeters and
Grazers can beat the surgi-
No stomach removed Small 1 -cm anastomosis 1 00-cm Roux limb Short (ie, 20 cm to 75 cm) biliopancreatic limb 400-cm common channel
phageal sphincter bloaters Usually eliminates reflux Reasonable for sweeters,
Can be beaten by persistent
No stomach removed Small 1 -cm anastomosis Long 400-cm Roux limb Short (ie, 20 cm to 75 cm)
1 00-cm common channel
cal procedure grazers, and bloaters
bad habits
biliopancreatic limb
Weight loss
When successful, can expect to lose Low early failure rate 20% to 25% late (ie, two to three years) weight gain Of 20% t0 30% When successful, can expect to lose 60% to 65% of excess body weight
Low early failure rate Possible mild weight regain
Can expect to lose 90% of
60% of excess body weight after two years
excess body weight
Malnutrition Low malnutrition or vitamin deficiencv Low malnutrition or vitamin High malnutrition and vita-
Revision
Possible late compli- cations
risk (ie, < 1 o/o)
(MVI) daily
deficiency risk (ie, < 1 YO to mi& deficiency risk (ie, 10% Requires 1 multiple vitamin injection 2%) to 20%)
Requires 1 MVI daily Requires 12 vitamin tablets
Difficult to revise; however, if a revision Failures are converted to dis- Sometimes needed to correct is necessary as a result of liver or stomach scarring, it usually requires an open procedure switch
daily
tal bypass or biliopancreatic malabsorption diversion with duodenal
Esophagitis Band erosion Staple line failure
0 Anastomotic ulcer or stricture Anastomotic ulcer or stricture
812 AORN JOURNAL

APRIL 2003, VOL 77, NO 4 - Gmling Elariny
COMPlWSON W THE TYPES OF SURGICAL PROCEDURES TO TREAT MORBID OBESlTY (CONTINUED)
Billopancreatic diversion with duo- denal switch and vertical gas- Vertical gastroplasty with sleeve
gastrectorny troplasty/sleeve gastrectomy Adjustable gastric band Features Large 90-mL to 150-mL tubular Large 90-mL to 150-mL Micropouch
stomach tubular stomach Purely restrictive Restrictive Partially restrictive Progressive slow compres- Does not change acid reflux but
Fails with sweeters and grazers Usually performed with duodenal switch Works for sweeters, grazers,
Mostly malabsorption May reduce acid reflux but not nonacid reflux
sion to prevent hunger reduces total acid producing capacity No stomach stapling
Can fail with sweets, shakes, and liquids
Performed alone to reduce risk in patients who are super morbidly obese with intent to perform duodenal switch after 100-lb to 200-lb weight loss
minimally obese patients (ie, < 350 Ibs) who wish to minimize bowel sur- gery risk and are highly motivated, nongrazers, and nonsweeters Preserves some antrum for better iron and vitamin B,, absorption Preserves pylorus to prevent dumping syndrome Stomach segment resected and removed from body
Little need for long-term follow-up Can expect to lose at least 65% of
Sometimes performed in selected
Weight loss
excess body weight
Malnutrition Minimal malnutrition risk Requires 1 MVI daily
Revision
Possible late compli- cations
Easy to convert to or add duodenal
May allow for increased efficacy of
Delayed gastric emptying and reflux
switch later
orlistat and phentermine
and bloaters
eating of sweets or fat and overeating
Port placed on abdominal Can be beat with excess wall
Wide open anastomosis 150-cm Roux limb 250-cm biliopancreatic limb 1 00-cm common channel Antral, pyloric, and duodenal preservation Stomach segment resected and removed from body
High weight loss success 0 Can expect to lose 70%
to 75% of excess body weight in first year
0 Can expect to lose 85% to 90% of excess body weight in second and third years
Variable
Low failure rate with good long-term follow-up
5% to 7% malnutrition and Low malnutrition risk vitamin deficiency risk, espe- Requires 1 MVI daily cially vitamins A, 0, E, and K and calcium
Revision may be needed to Simple low-risk procedure treat malnutrition Reversible
Some bowel obstruction risk Erosion Volvulus Slippage Foul smelling stools and gas Mega-esophagus Increased diarrhea, fre- quency, and urgency
813 AORN JOURNAL

APRIL 2003, VOL 77, NO 4 - Graling 9 Elariny
per day. Success of this procedure provides the patient with more than 65% excess body weight loss at one year, although there may be failure with patients who are classified as sweeters and grazers. Specific complications relate to delayed gastric emptying and reflux. The procedure may allow for the increased efficiency of weight loss medications and is easy to convert to a duodenal switch at a later time (Figure 5). It is very easy for patients to con- sume more than 700 calories per meal if they make poor food choices because of the larger remnant (ie, pouch). For this reason, this procedure, when per- formed as the only planned procedure, is limited to patients willing to carefilly monitor their caloric intake and diet after surgery.
Biliopancreatic diversion (BPD) with duode- nal switch, vertical gastroplasty/sleeve gastrecto- my. This procedure was introduced approximately 15 years ago as an alternative to the Scopinaro BPD and has several advantages. Specifically, the proce- dure depends more on malabsorption than restric- tion to accomplish weight loss, and this appears to improve the long-term success rate. The absence of
Figure 2 Vertical banded gastroplasty.
regain after two years. Specific complications are anastomotic ulcer or stricture, and sometimes revi- sion is needed to correct malabsorption (Figure 4). This procedure generally is discouraged because it carries the highest risk with regard to malnutrition as a result of the small pouch in combination with a short common channel. A duodenal switch procedure is preferable for patients who need malabsorption.
Vertical gastroplasty with sleeve gastrectomy. The vertical gastroplasty with sleeve gastrectomy is a restrictive procedure usually performed with a duodenal switch. It may be performed alone to reduce perioperative risk in a patient who is extreme- ly morbidly obese with the intent of performing the duodenal switch as a second stage after a 100-lb to 200-lb weight loss. Anatomically, the vertical gastro- plasty with gastrectomy leaves a tubular stomach, which preserves some antrum for better iron and B,, absorption. It does not change reflux, reduces total acid producing capacity, and preserves the pylorus so there is no dumping syndrome. There is little malnu- trition risk, and the patient usually takes one MVI Figure 3 Proximal gastric bypass.
814 AORN JOURNAL

APRIL 2003, VOL 77, NO 4 9 Gruling E1urin.v
a gastro-enteric anastomosis reduces marginal ulcer and stricture risk. Leaving the pylorus functional avoids the dumping syndrome, and antral acidifica- tion of iron and flow through the duodenum and antral gastrin secretion improves iron and vitamin BU absorption, thereby almost eliminating the risk of these deficiencies. The procedure generally has been reserved for patients with higher BMIs (ie, greater than 45) but in recent years has been offered to patients with lower BMIs (ie, 35 to 44) with good results and low morbidity. More than 250 laparo- scopic duodenal switch procedures have been per- formed at Inova Fairfax Hospital with no deaths, low morbidity, and excellent weight loss results. The duodenoenteric anastomosis was performed using a laparoscopic handsewn method without leaks in the last consecutive 200 procedures. The procedure is not without its drawbacks, however, and it does have a higher malnutrition risk (ie, 5% to 7%) than proximal bypass. It also has associated side effects of steatorrhea and foul stool and gas, especially with fatty and carbohydrate rich foods. There is a higher incidence of vitamin D and calci-
Figure 5 Vertical gastroplasty with sleeve gastrec- tomy without banding.
Figure 4 Distal gastric bypass.
um malabsorption, and vitamin A dosing becomes an issue during pregnancy. Patients who choose this procedure generally are very happy with it because the larger meal size is important to them and the absence of dumping syndrome also is relevant. Patients, however, must be compliant with vitamin and protein intake, or malnutrition will develop (Figure 6).
Adjustable gastric band (AGB). The AGB pro- cedure is ideal for patients who are afraid of highly invasive procedures and want a simple, easily reversible procedure to help with portion control. Patients might say that they like that there is no stom- ach stapling, removal, or rearrangement. Patients also must desire the adjustability, which allows them to ease into it with progressive needle adjustments, and they cannot mind the needle adjustments. Patients must be willing to comply with sweet and snack avoidance postoperatively to see success (Figure 7 ) .
Non-FDA approved options. Use of the gastric balloon has been difficult to revive in the United States. A variant of gastric balloon was available in
815 AORN JOURNAL

APRIL 2003, VOL 77, NO 4 Graling 8 Elariny
the United States in the 1980s but was banned due to the complication rate. The current version is modified and has lower bleeding or obstruction complication rates; however, the efficacy is short- lived and minimal compared with the better than 50% excess body weight loss seen in other current- ly used bariatric procedures. It usually is used in Europe as a bridge to weight loss in patients who are morbidly obese.
A modified cardiac pacemaker may be used to reduce appetite by inducing a feeling of satiety. The electrodes are placed in the muscle. Electrical impulses from the device reduce appetite and stimu- late the muscles and the nerves on the muscles to contract, which speeds up stomach emptying. The gastric pacemaker still is investigational. Very little literature exists regarding its effectiveness and com- plications (Figure 8).
AFCER C O M M O N OF THE PROCEDURE The surgeon performs an intraoperative endo-
scopy with pressure insufflation and leak test at the end of the surgical procedure. The surgeon places a drain before closure if the patient had an anastomosis, which facilitates early diagnosis of an anastomotic leak. At the completion of the procedure, the
Figure 6 Biliopancreatic diversion with duodenal switch and vertical gastroplasty/sleeve gastrectomy.
Figure 7 Adjustable gastric band. Figure 8 lntragastric balloon (0) and vagal pacing (b).
816 AORN JOURNAL

APRIL 2003, VOL 77. NO 4 Graling Elariny
incision is injected with 0.25% bupivicaine to assist with pain management. The anesthesia care provider extubates the patient in the OR, and surgical team members transfer the patient to a bed equipped with specialized padding and sturdy hydraulics. The anes- thesia care provider and nurse then transport the patient to the postanesthesia care unit (PACU).
POSTOPERATIVE CARE The patient spends approximately one hour in
the PACU and then is taken to the surgical floor. The patient may be admitted to a critical care unit if he or she is experiencing shortness of breath, needs con- tinuous positive airway pressure, or has complex medical conditions requiring continual observation and care.
Depending on the details of the surgery, patients may awaken with a nasogastric (NG) tube in place. It also may be necessary to perform an x-ray leak test after surgery. This usually is done on the first or sec- ond day after surgery, as needed. If it is needed, the patient is taken to the radiology department. The radiology technologist gives the patient clear x-ray contrast medium to sip at specified times during the procedure. The radiologist takes several x-rays as the patient swallows the contrast medium. The technolo- gist prints the x-rays, and the radiologist and surgeon carehlly review the results. A decision is made whether to leave the NG tube in place and when to start the patient on a liquid diet. At Inova Fairfax Hospital, the first 50 patients all had postoperative esophagograms. With program maturity and a leak rate of 0%, esophagograms now are used only for a select group of patients.
Each bariatric procedure has its own specific postoperative instructions, which are tailored in detail to the type of procedure. If surgery was performed laparoscopically and the patient is able to tolerate liq- uids, discharge to home may be accomplished on the same day as surgery. As with any laparoscopic proce- dure, patients have smaller scars, reduced pain, decreased length of stay, and shorter recovery time compared to open surgery. All patients receive antibi- otic coverage, respiratory support (eg, nebulizer, incentive spirometry), patient-controlled analgesia, and sequential compression stockings and enoxaparin sodium to minimize deep vein thrombosis. Table 6 is a sample set of orders for a patient’s day of surgery and first postoperative day.
Dietary instructions. For the first two days after surgery, dietary intake is limited to clear liquids.
Intake gradually is advanced during the next few days. For example, on days three and four, the diet is advanced according to tolerance. The patient is expected to walk daily and regularly and sit in a chair when not walking. If tolerating liquids well, the patient may advance to a low carbohydrate, full liquid diet as early as the third postoperative day. The patient stays on this diet for two days. Medications must be crushed or opened. Common medications include ursodiol (ie, if gallbladder was not removed), pain medications, lansoprazole, mul- tivitamin with iron, and medications previously pre- scribed for chronic medical conditions. On the fifth and sixth postoperative day, the diet continues to advance. The patient now should be able to safely begin eating pureed foods, including baby foods, applesauce, blended soft foods, and potted meats. The patient needs to drink constantly to remain hydrated. The patient will not need to supplement with protein powder during these early days. On the sixth and seventh day, the diet progresses to soft foods, including all of the previously mentioned pureed items, all allowed liquids, and soft foods, such as baked white fish without bones, imitation crab meat, hot dogs, canned fruits, and over-cooked vegetables. Hard meats, such as steak, pork, and chicken, are not allowed.
During the second through third weeks, the patient begins a regular food trial period. This includes all previously allowed items plus red meat, chicken, and well-cooked vegetables. This is called a trial period because patients are expected to try only one new item at a time. If adding one new regular food per day, 14 new items have been added by the end of this period. The patient also may begin trying to take whole pills, one at a time, during this period rather than crushing them.’
PosToPERAmfE rnUoW-UP The patient is instructed to be as active as pos-
sible, walking up to one mile per day by the postop- erative office visit. He or she also is instructed to wear an abdominal binder while active. Activity gradually is increased; however, the patient is instructed to avoid heavy lifting for three to six weeks after surgery to allow the incisions to heal solidly. The patient may return to work one week after surgery if he or she underwent a laparoscopic procedure. If the patient underwent an open proce- dure, he or she may be able to return to work approx- imately six weeks later.
817 AORN JOURNAL

APRIL 2003, VOL 77, NO 4 8 Gruling 8 Eluriny
Table 6 PO?STOPERATM ORDERS FOR LAP#ROSCOPIC GASTRIC BYPASS PROCEDURES'
Day of surgery
Activity: help patient out of bed and into bedside chair twice before bed- time; no straining or heavy lifting
Diet: nothing passed orally
IV: 5% dextrose in .5% normal saline (NS) with 20 mEq potassium chloride at 125 mVhr
o Check blood sugar every (9) 6 hrs, then administer subcuta- neous (SQ) humulin regular insulin using the sliding scale
Blood sugar Dose 180-200 2 units SQ 201 -250 4 units SQ 25 1 -300 6 units SQ 30 1 -350 8 units SQ 3 5 1 -400 10 units SQ 401 -450 10 units SQ and 5 units IV then
recheck blood sugar after 3 hrs
> 450 Same and call physician
o Cefotetan 2 g IV piggyback (IVPB) q 12 hrs for three postop- erative doses, if not allergic
o Famotidine 20 mg IVPB q 8 hrs for three postoperative doses
o Patient-controlled analgesia per anesthesia care providers; dis- continue (D/C) on postoperative day two and switch to fentanyl patch 50 mcg/hr
o Enoxaparin 40 mg SQ two times per day (bid) starting late tonight
o Pramethazine 25mg IV push
Medications:
(IVP) q 4 hrs PRN for nausea 0 Acetaminophen 100 mg suppo-
sitory per rectum (PR) q 4 hrs PRN for headache or temperature > 101" F (38.3" C)
0 Diphenhydramine 25 mg IVP q 6 hrs PRN for itching or insomnia
Oxygen at 2 L per nasal canula while awake; continuous positive aiiway pressure when sleeping
Albuterol 0.5 mL in 3 mL NS q 4 hrs and add intermittent positive- pressure breathing at 10 if poor effort identified
Bilateral lower extremity sequential compression devices (SCDs) over thromboemboletic stockings
Vital signs per routine
Postoperative day one
Activity: as tolerated; no straining
Diet
or heavy lifting
0 Call resident for diet when upper gastrointestinal series results have been received
o Advance diet to full liquids then to low carbohydrate (ie, diabetic) clear liquid diet; patient may dilute juices 50/50
I V D/C when diet started
Laboratory tests: complete blood count, chemistry profile, chest x-ray, electrocardiagram, and pulse oximetry
0 Medications: crush all medications to a powder or open capsules, then
administer in sherbet 0 Ursodiol 300 mg taken by mouth
(PO) bid if patient has not had a cholecystectomy
0 Fentanyl patch 25 mcg per hr PRN for pain
0 Acetaminophen/oxycodone one to two tablets q 4 to 6 hours PRN for pain if fentanyl patch is not adequate
0 lanoprasole 30 mg PO q day 0 Acetaminophen 1,000 mg liquid
PO q 4 hrs PRN for headache or temperature > 101 O F (38.3 C) if tolerating oral intake
o D/C meperidine
Bilateral lower extremity SCDs over thromboemboletic stockings 0 Remove SCDs when patient is
ambulating o Replace SCDs when patient is
lying in bed or sitting in chair
Discharge patient to home 0 Ensure patient is tolerating oral
medications and liquids o Provide patient with male urinal
or female toilet hat for at home monitoring of urine output
0 Fentanyl patch 25 mcg per hr PRN for pain
o Acetaminophen/oxycodone 1 to 2 tablets q 4 to 6 hrs PRN for pain if fentanyl patch is not adequate
o lanoprasole 30 mg PO q day o Ursodiol 300 mg PO bid o Promethazine 25 mg PR q 4 hrs
Provide prescriptions for
PRN for nausea
NOTES
General Surgery Associates, http://www.alagsa.com/GBP-lnstr.htm (accessed 30 Jan 2003). 1 . H A Elariny, 'Postoperative instructions after open and laparoscopic gastric bypass," Advanced Laparoscopic and
818 AORN JOURNAL

APRIL 2003, VOL 77, NO 4 - Gmling 9 Elariny
The patient must keep a record of exactly what and how much he or she eats and drinks at every meal for the first three weeks after surgery. This is the only way the surgeon can determine whether dietary protein intake is adequate. The patient should bring the dietary log to the first postoperative visit. If the patient has diabetes, he or she probably will have reduced or discontinued medicines and must check his or her blood glucose twice daily to determine whether adjustments are necessary. Follow-up appointments are scheduled once per month for the first year, during which the patient’s weight is checked. Laboratory work is completed (eg, hemoglobin, albumin, electrolytes, vitamin lev- els) six months after surgery, or sooner if the patient reports that he or she is eating poorly, to detect any vitamin deficiencies.
Long-term support. A bariatric support group for preoperative and postoperative patients is held once per month by the surgeon. Each week, patients of specific surgical types hold their own support group, which is moderated by a patient. After weight loss, the patient may need to return to the OR for a secondary procedure. Sagging skin in the face, arms, breasts, and abdomen may lead to functional and aesthetic deformities.’” Skin folds may con-
NOTES 1. A H Mokdad et al, “The
spread of the obesity epidemic in the United States, 199 1 - 1998,” JAMA 282 (Oct 27, 1999) 1519-1522.
2. Ibid. 3. M M Ellison, H E Mulcahy,
“Obesity: Weighing up the cardiovas- cular risks,” British Journal of Cardiology 8 (February 2001) 61-64.
4. “Rationale for the surgical treatment of morbid obesity,” American Society for Bariatric Surgery, http://www.asbs.orgihtml /ration.html (accessed 30 Jan 2003).
5. “Clinical guidelines on the identification, evaluation, and treat- ment of ovenveight and obesity in adults,” National Institutes of Health,
tribute to problems with hygiene and may cause chronic skin inflammation or infection. The patient may seek consultation with a plastic surgeon for a face lift, marnmoplasty, or abdominoplasty for removal of excess skin.
The commitment to the bariatric patient does not end when the immediate perioperative period is com- plete. Administration of a comprehensive bariatric program encompasses many aspects besides the surgi- cal intervention. A successful program includes nutri- tional support, psychological support, and availability of practitioners to help with any complications experi- enced by the patient. More than 500 procedures have been performed since inception of the program in 1999 at Inova Fairfax Hospital. Patients report a 100% satisfaction rate, a decrease in comorbidities, and greater enjoyment of their healthier lifestyle. A
Paula Craling, RN, MSN, CNOR, CNS, is the clinical nurse specialist for perioperative services at Inova Fairfar Hospital, Falls Church, k.
Hazem Elariny, MD, PhD, is a surgeon for Advanced Laparoscopic and General Surgery Associates, Arlington, k.
http://www.nhlbi.nih.gov/guide lines/obesity/ob-home.htm (accessed 30 Jan 2003).
6. G S Cowan, Jr, “A predicted hture for bariatric surgery: Using the surgical model,” Obesity Surgery 6 (February 1996) 12-16; S Abu- Abeid, A Keidar, A Szold, “Reso- lution of chronic medical conditions after laparoscopic adjustable silicone gastric banding for the treatment of morbid obesity in the elderly,” Surgical Endoscopy 15 (February 2001) 132-134; M Deitel, “Surgery for morbid obesity. Overview,” European Journal of Gastro- enterology and Hepatology 1 1 (February 1999) 57-61; A M Glenny et al, “The treatment and prevention
of obesity: A systematic review of the literature,” International Journal of Obesity and Related Metabolic Disorders 2 1 (September 1997) 7 15- 737.
7. A M Macgregor, “The patient factor,” Obesity Surgery 6 (August
8. “Obesity epidemic puts mil- lions at risk from related diseases: Press release 12 June 1997,” World Health Organization, http://www .who.int‘archives/inf-prl997/en/pr97 -46.html (accessed 30 Jan 2003).
1996) 325-329.
9. Ibid. 10. S J Pavlovich-Danis, “Bariatric
surgery update,” The Nursing Spectrum 1 1 (September 2001) 14- 17.
819 AORN JOURNAL