Perioperative seizures Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab.DCA, Dip. Software...
49
Perioperative seizures Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab.DCA, Dip. Software statistics- Phd Mahatma Gandhi Medical college and research institute , puducherry , India
-
Upload
bernadette-daniel -
Category
Documents
-
view
216 -
download
0
Transcript of Perioperative seizures Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab.DCA, Dip. Software...

Perioperative seizures
Dr. S. Parthasarathy MD., DA., DNB, MD (Acu),
Dip. Diab.DCA, Dip. Software statistics- Phd
Mahatma Gandhi Medical college and research institute , puducherry , India

Definition • A seizure can be defined as the clinical manifestation of
an abnormal and excessive discharge of neurones, seen
as alteration of consciousness, motor, sensory or
autonomic events.
• Epilepsy is defined as recurrent (two or more) epileptic
seizures unprovoked by any immediately identifiable cause.
• Epilepsy includes seizures but seizures ??

Incidence
• Only epilepsy – incidence • 0.5 – 1 %
• But peri operative seizures – incidence ??
• EEG monitoring in potential patients ?? • It can also miss ??

Classification
• General • Partial • Unclassified
Causes • Epilepsy • Tumours • Infections • Metabolic • Alcohol • Stroke
• Its Same

Differential diagnosis
• Syncope • Migraine • Narcolepsy • Non epileptic seizures

Investigations
• EEG • CT scan • MRI • PET scan

How does it relate to us ??
• Sudden seizures – periop• Epilepsy – anaesthetic considerations• ICU status epilepticus
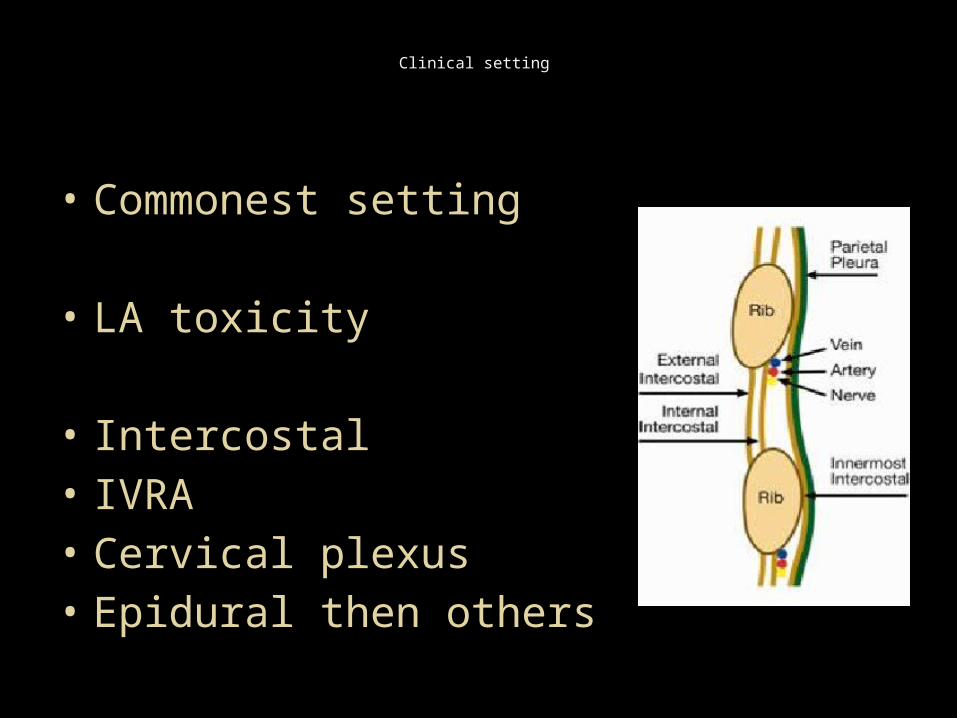
Clinical setting
• Commonest setting
• LA toxicity
• Intercostal • IVRA • Cervical plexus • Epidural then others

Test dose
• There may be premonitory symptoms, such as peri oral
tingling, or feelings of dissociation following a test dose.
• Epinephrine ??
• Catheter malfunction
• Catheter position change
• Axillary ??
• Field blocks

Maximum dose for infiltration (mg/kg)
• Lidocaine 3 - 4• With adrenaline 7• Bupivicaine 2• With adrenaline 3• Prilocaine 6• With adrenaline/octapressin 8• Additive

Basic treatment
• Airway • Oxygen • Ventilate • Support
• Other than benzodiazepines

Surgery – what type ??

What Type of Surgery Places the Patient at Risk for Seizures?
• Neuro surgery 20 %
• Leave alone head injury • Supratentorial tumors • Cerebral abscess 90 % • Drainage 15 – 20 %
• Preop seizure history -- incidence is very much higher

CAROTID AND CARDIAC SURGERY
• Clamping • Emboli • Stents and tubes

Other surgeries
• extensive bowel surgeries • Burns and plastic surgeries • Gut obstruction
• Fluid shifts – seizures

• Electrolytes
• Clinical settings

Hyponatremia – usually 115 is cut off
• TURP syndrome • Extensive bowel surgeries • Other scopies where irrigation is done • Plastic and burn reconstruction – massive fluid shifts • Drugs like diuretics • Water intoxication • SIADH. Vomiting • Renal and hepatic disorders

Hypocalcemia
• Low albumin; • abnormal acid-base status and electrolytes; • drugs used during the peri-operative period• transfusion of large volumes of citrated blood; • Parathyroid surgeries ,thyroid , CPBs• Sepsis , CRF • Calcium chelators in radiographic contrast

Eclampsia
In pregnant – other than
• Epilepsy, eclampsia, drugs
• Posterior reversible encephalopathy • Amniotic fluid embolism • Cortical vein thrombosis

Intraop seizures – wrong drugs
• Tranexemic acid into the intrathecal space


In an ICU
• Seizures
• Posttraumatic brain injury• CNS infections• Endocrine and metabolic disorders• Drugs or toxins

Seizure prone electrolyte disturbances
• Hyponatremia• Hypokalemia• Hypocalcemia• Hypoglycemia and hyperglycemia• Hypomagnesemia

Drugs
• Amphetamine • SSRIs • Tricyclics • Levodopa • Deriphyllin • Phencyclidine • Withdrawal of antiepileptics• Methergin
Alcohol related
• hyponatremia, hypomagnesemia, or hypoglycemia
• Thiamine

Anesthesia related
• Tramadol Pethidine ,• etomidate • Enflurane ,sevo • Atracurium• Flumezanil
• Ketamine methohexital ??, propofol • Hypocapnia ??

EEG monitoring in sevo

Other settings
• Renal failure --- erythropeitin ?? • Hepatic failure • Hypothyroidism • Hashimato s
• Inciting factors • Fever , infection , sleeplessness

Reflex Anoxic Seizures and Anaesthesia
• What is this ?? • ocular pressure, venepuncture, accidental
trauma and fear • Young female school children
• Grand mal like • EEG changes may not be present

What should we do
• Patient Should not fall • Oxygen • Bag and mask • Two IV lines • Glucose • Thiamine • Benzodiazepines

Settings at a glance
• Local anaesthetic toxicity • TURP • Eclampsia • Neuro surgeries • CPBs • Drug intake • Drug withdrawal

Post operative period
• Postoperative generalized shaking is usually because of shivering, which may be thermoregulatory or non-thermoregulatory.
• The latter is thought to be secondary to the
effects of volatile anaesthetics, pain or both.

Pseudoepileptic seizures
• common in the postoperative period. • resemble tonic–clonic seizures • NO abnormal electrical discharges• history of convulsions and/or psychosomatic illness. • flamboyant, last longer than 90 s , asynchronous limb
movements, side-to-side head movements, closed eyes (including a resistance to eye opening).
• There is no cyanosis or post-ictal period• may be incontinence or tongue-biting. • Seizures may settle with reassurance. • Plasma prolactin concentrations tend to be raised after epileptic
seizures and normal after pseudo-seizures.


In fits • Case ?? • Massive fluid shifts• Epileptic • Systemic illness • Drugs, alcohol • Hypoxemia • Electrolytes , blood glucose, RFT, LFT • CT brain • Oxygenation, benzodiazepines

Status epilepticus
• The traditional definition of status epilepticus as a seizure
lasting or recurring without regaining of consciousness over a
30 min period is primarily useful for epidemiological
purposes.
• Can we wait for 30 minutes ??
• In clinical practice, most convulsive seizures abate within 2–3
min and a seizure that continues for more than 5 min has a
low chance of terminating spontaneously.

Physiological changes • Increased cerebral metabolism • Increased blood flow, • increased glucose and lactate concentration• Increased catecholamine secretion
• 30 – 60 minutes
• hyponatraemia, potassium imbalance,• evolving metabolic acidosis, consumptive
coagulopathy, rhabdomyolysis, and multi-organ• failure

Stages
• Premonitory (0 -5 min) • Early (5-10 minutes) • Established ( 10 – 30 minutes )• Refractory ( 30 – 60 minutes)

• Pre-monitory stage (out of hospital or first 5 min)
• BUCCAL OR RECTAL MIDAZ

Early stage (first 5–10 min)
• Iv ACCESS • OXYGEN • GLUCOSE , THIAMINE • BENZODIAZIPINES

Established CSE (5–30 min)
• Phenytoin • Phenobarbital • Valproate • levetiracetam

Refractory status (30–60 min)
• Refractory CSE (RSE), where SE continues in spite of administration of two AEDs (e.g. benzodiazepines and phenytoin), is associated with a high risk of complications.
• These include tachyarrhythmias, pulmonary oedema, hyperthermia, rhabdomyolysis, and aspiration pneumonia.

To continue till ??
• Maximal therapy should be maintained until
12–24 h after the last clinical or electrographic
seizure, after which the dose should be
tapered. If seizures recur, therapy can be re-
instituted or altered

Non-convulsive status epilepticus
• Impaired consciousness • Automatism
• EEG patterns

Summarize
• Status definition • Complications • Stages • Treatment