Perioperative Nurses Role Anterior THA[1]
20
The Perioperative Nurse’s Role in Table-Enhanced Anterior Total Hip Arthroplasty CASSENDRA A. MUNRO, RN, MSN, CNOR N ursing care of the patient in surgery has naturally evolved along the same trajectory as the development of the technology used in the OR. Today, most surgical services use computer technology and an increasing amount of specialized equipment, making cross-training of personnel more challenging. With the addition of such technology comes the need for perioperative nurses to be more educated and knowledgeable about new equipment so they can ef- fectively participate in caring for their patients. Orthopedics is no exception as advances in equipment and tech- niques change rapidly for many types of orthopedic surgical procedures (eg, new approaches for traditional joint re- placement procedures). Performing the anterior approach for total hip arthroplasty (THA) with the patient in a supine position on an or- thopedic OR table requires exposure, dislocation, and reduction of the hip joint. As with any surgical procedure, the circulating nurse is directly in- volved and an integral member of the surgical team. The nurse must have an understanding of the surgical interven- tion and a willingness to participate in this innovative approach. There are distinct advantages to the anterior approach. The orthopedic table promotes ease of THA by increasing femoral access with adduction, exten- sion, and proximal femoral hook place- ment. Improved exposure of the femur limits soft tissue trauma. The supine po- sition and use of a radiolucent orthope- dic table facilitates use of fluoroscopy. Patient selection criteria are not limited as they may be with the conventional lat- eral approach. 1 HISTORY OF ANTERIOR APPROACH THA Traditionally, most THAs have been performed with the patient in the later- al position and the use of the lateral or posterior approach on a standard OR bed. In 1947, Robert Judet, MD, per- formed the first anterior-approach THA in France using the Judet-Tasserit orthopedic table. 2,3 This table provided unique ways to position a patient for The anterior approach to total hip arthroplasty (THA), when performed with the patient in the supine position, is enhanced by the use of a radiolucent, orthopedic table. This technique has numerous advantages: enhanced in- traoperative fluoroscopy because of the patient’s supine position on a radiolucent table, improved femoral expo- sure, and reduced soft tissue trauma. Criteria for patient selection is not limited as it may be for other arthroplas- ty techniques. The role of the perioperative nurse during an anterior THA is to ensure optimal function of the orthopedic table and provide safe patient care. A clear understand- ing of the surgical techniques used and the functions of the table are imperative. Key words: anterior total hip arthroplasty, anterior ap- proach THA, radiolucent orthopedic table-enhanced THA. AORN J 90 (July 2009) 53-68. © AORN, Inc, 2009. ABSTRACT 3.7 © AORN, Inc, 2009 JULY 2009, VOL 90, NO 1 • AORN JOURNAL • 53 New! Complete this CE activity online at aorn.org/CE indicates that continuing education contact hours are available for this activity. Earn the con- tact hours by reading this article and taking the examination on pages 69-70 and then completing the answer sheet and learner evaluation on pages 71-72. The contact hours for this article expire July 31, 2012.
-
Upload
crystal-thomas-vollstaedt -
Category
Documents
-
view
167 -
download
0
Transcript of Perioperative Nurses Role Anterior THA[1]
![Page 1: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/1.jpg)
The Perioperative Nurse’s Rolein Table-Enhanced Anterior
Total Hip ArthroplastyCASSENDRA A. MUNRO, RN, MSN, CNOR
Nursing care of the patient insurgery has naturally evolvedalong the same trajectory as
the development of the technologyused in the OR. Today, most surgicalservices use computer technology andan increasing amount of specializedequipment, making cross-training ofpersonnel more challenging. With theaddition of such technology comes theneed for perioperative nurses to bemore educated and knowledgeableabout new equipment so they can ef-fectively participate in caring for theirpatients. Orthopedics is no exceptionas advances in equipment and tech-niques change rapidly for many typesof orthopedic surgical procedures (eg,new approaches for traditional joint re-placement procedures).
Performing the anterior approach fortotal hip arthroplasty (THA) with thepatient in a supine position on an or-thopedic OR table requires exposure,dislocation, and reduction of the hipjoint. As with any surgical procedure,the circulating nurse is directly in-volved and an integral member of thesurgical team. The nurse must have anunderstanding of the surgical interven-tion and a willingness to participate inthis innovative approach.
There are distinct advantages to theanterior approach. The orthopedic tablepromotes ease of THA by increasingfemoral access with adduction, exten-sion, and proximal femoral hook place-ment. Improved exposure of the femurlimits soft tissue trauma. The supine po-sition and use of a radiolucent orthope-dic table facilitates use of fluoro scopy.Patient selection criteria are not limitedas they may be with the conventional lat-eral approach.1
HISTORY OF ANTERIOR APPROACH THATraditionally, most THAs have been
performed with the patient in the later-al position and the use of the lateral orposterior approach on a standard ORbed. In 1947, Robert Judet, MD, per-formed the first anterior-approachTHA in France using the Judet-Tasseritorthopedic table.2,3 This table providedunique ways to position a patient for
The anterior approach to total hip arthroplasty (THA),when performed with the patient in the supine position,is enhanced by the use of a radiolucent, orthopedic table.
This technique has numerous advantages: enhanced in-traoperative fluoroscopy because of the patient’s supineposition on a radiolucent table, improved femoral expo-sure, and reduced soft tissue trauma. Criteria for patientselection is not limited as it may be for other arthroplas-ty techniques.
The role of the perioperative nurse during an anteriorTHA is to ensure optimal function of the orthopedictable and provide safe patient care. A clear understand-ing of the surgical techniques used and the functions ofthe table are imperative.
Key words: anterior total hip arthroplasty, anterior ap-proach THA, radiolucent orthopedic table-enhanced THA.AORN J 90 (July 2009) 53-68. © AORN, Inc, 2009.
ABSTRACT
3.7
© AORN, Inc, 2009 JULY 2009, VOL 90, NO 1 • AORN JOURNAL • 53
New! Complete this CE activity online at aorn.org/CE
indicates that continuing education contacthours are available for this activity. Earn the con-tact hours by reading this article and taking theexamination on pages 69-70 and then completingthe answer sheet and learner evaluation on pages71-72. The contact hours for this article expireJuly 31, 2012.
![Page 2: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/2.jpg)
JULY 2009, VOL 90, NO 1 Munro
54 • AORN JOURNAL
orthopedic procedures rather than having toplace the patient in the standard lateral position.During a visit to France in 1981, Joel Matta, MD,of Los Angeles, California, observed this surgicaltechnique as performed by Emil Letournel, MD,a former resident under Dr Judet. Dr Mattabegan to perform the technique in the UnitedStates in 1996 using the Judet-Tasserit orthopedictable. When production of this orthopedic tablewas discontinued in 2003, Dr Matta began to usethe ProFX® and Hana® radiolucent orthopedictables. With the advent of new, American-madetables, courses teaching the anterior technique forTHA began to be offered to orthopedic surgeonsin the United States, and interest in the procedurehas grown (J. Matta, MD, founder and director,Hip and Pelvis Institute, St John’s Health Center;verbal communication; June 9, 2008).
From November 1996 to November 2008,Dr Matta performed 1,723 primary, anterior-
approach THAs. According to Dr Matta’s pa-tient data, a mean time of 64 minutes and a me-dian time of 85 minutes was required to performthe surgical procedure. Average blood loss hasbeen estimated to be approximately 400 mL. Pa-tients have had an average (ie, mode) length ofstay (LOS) in the hospital of three days. Thelength of the incision is almost always 10 cm(Figure 1). Only three patients have experienceddislocation of their prostheses. The hip prosthe-ses implanted included cemented, uncemented,and surface replacement THA (J. Matta, MD; un-published data, August 2007).
Among the 1,723 THAs, 494 consecutive,single-incision, anterior-approach THAs on anorthopedic table were performed by Dr Mattaand several surgical fellows from September1996 to September 2004. The surgical time ofthese 494 procedures averaged 90 minutes withan average LOS of four days. The majority of
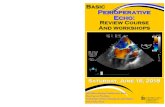
Surgical Approaches for Total Hip Arthroplasty (THA)
The approaches for THA vary in the invasiveness ofthe hip musculature: (a) the posterior approach,
(b) the lateral or tansgluteal approach, (c) the an-terolateral approach, and (d) the anterior approach.a. The posterior approach (ie, Kocher-Langenbeck
approach) splits the gluteus maximus muscleand detaches the posterior external rotatormuscles (ie, the piriformis, obturator internusand externus, superior and inferior gemellus).
b. The lateral or transgluteal approach (ie, Hardingapproach) splits the gluteus medius muscleand detaches the gluteus minimus and the anterior third of the gluteus medius musclesfrom the femur.
c. The anterolateral approach (ie, Watson-Jonesapproach) is performed posterior to the tensorfascia lata and anterior to the gluteus mediusand splits the hip deltoid muscle, which con-sists of the gluteus maximus and tensor fascialata muscles.
d. The anterior approach (ie, short Smith-Petersenand Hueter approach) does not split or detachmuscles. This approach is performed over thetensor fascia lata, inside the tensor sheath,anterior and medial to the tensor fascia lataand lateral to the sartorius and rectus femorismuscles.
gluteus medius
gluteusmaximus
biceps femoris
the tensor fascia lata is
under the tensor sheath
sartorius
the rectusfemoris isunder the sartorius
vastuslateralus
ilio tibialband
patella
the obturatorexternus isunder the inferior
gemellus,which is underthe obturator
internus, whichis under the
superior gemellus,
which is underthe piriformis,which is under
the gluteusmaximus
the gluteusminimus isunder thegluteusmedius
tensor fascia lata
a
b
c
d
Illustration by Kurt Jones
![Page 3: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/3.jpg)
Table-Enhanced Anterior Total Hip Arthroplasty JULY 2009, VOL 90, NO 1
aornjournal.org • 55
these patients were walkingpostoperatively without exter-nal support by 10 days. Thepostoperative complications re-ported included one infection,three dislocations, and onetemporary nerve palsy.4
In general, other surgeonsreport that the muscle-sparing,anterior approach is versatileand has favorable long-termoutcomes with minimal com-plications.5 In a study of 1,037THAs, there were only 10 hipdislocations. The authors ofthat study corroborate that theprocedure is safe with a lowdislocation rate.6 Anotherstudy of 100 consecutive THAsconcluded that this techniquewas safe and advantageous be-cause of reduced • blood loss,• postoperative pain, and• LOS with more rapid rehabilitation.7
In a study of 195 THAs, a mini-posteriorapproach (MPA) performed on 96 patientswas compared to a direct, anterior approach(DAA) performed on 99 patients.8 The resultsshowed that patients who underwent theDAA had a more rapid recovery of hip func-tion and gait ability. The average surgical timefor MPA was 100.4 minutes and for DAA was104.7 minutes. The LOS was 30.4 days forMPA patients and 22.2 days for DAA patients.Blood loss averaged 426.9 mL during MPAprocedures and 526.1 mL during DAA proce-dures. There was one dislocation experiencedby a patient who had undergone MPA andnone reported for patients who had under-gone DAA. According to the researchers, theblood loss during DAA was greater because oftechnical difficulty with femoral preparation.A comparison of this study and Matta’s statis-tics is shown in Table 1.
PATIENT SELECTION AND ADVANTAGESThe anterior approach is a treatment option
for all patients requiring hip arthroplasty in-cluding patients suffering from the effects of
osteoarthritis, rheumatoid arthritis, traumaticarthritis, and avascular necrosis. Furthermore,there is less subcutaneous and deep fat to dis-sect over the hip joint using this approach. Pa-tients requiring a revision whose hips werepreviously replaced using the lateral or poste-rior approach or who previously had post-traumatic hip or pelvic surgery are not exclud-ed. This technique also is suitable for patientswho need bilateral hip replacements.4
Patient advantages with the anterior ap-proach include: • less postoperative pain;7
• shorter hospitalization;7
• a single, small incision;4
• no postoperative dislocation precautionsand very low risk of postoperative disloca-tion;2,4,5,7 and
• immediate weight bearing on the surgical leg.2
The procedure offers better access to the hipbecause the hip is superficial in the supine po-sition and subcutaneous fat is thinner at theincision site. Placing the patient supine alsoallows for better control of pelvic position. Inaddition, the anterior approach preservespelvic and femoral muscle attachments, thus
Figure 1 • Typical 10-cm incision for an orthopedic table-enhanced anterior-approach total hip arthroplasty procedure.
![Page 4: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/4.jpg)
JULY 2009, VOL 90, NO 1 Munro
56 • AORN JOURNAL
reducing the risk for dislocation and allowingfor a more rapid recovery.4
PREPARATION FOR THAThe circulating nurse assesses the function
of the orthopedic table (Figure 2) before eachprocedure to ensure that it is working proper-ly. This includes pressing the “return to level”button, which returns the base of the table to aneutral position and lowers the height of thetable when the leveling process is complete.After testing both femoral lifts for function, thecirculating nurse lowers the lifts and securesthem in a locked position at the base of the liftwhere it attaches to the table. The nurse checksthe femoral lift switch to ensure that the tablehas been lowered and leveled and confirmsthat both spars of the table are tightly locked.A spar is a radiolucent extension from thetable base. The patient’s foot is placed in a se-cured boot that is locked with a swivel joint toa mount on the spar to allow mobility of theleg. Lowering the table and locking both
femoral lifts facilitates safe transfer of the pa-tient to the table.
Other procedure preparation responsibilitiesof the circulating nurse include ensuring thatall necessary equipment is in the room andfunctioning properly. As with any orthopedicsurgical procedure, in addition to the orthope-dic table, a mobile x-ray viewing box is used.The nurse places the viewing box on the pa-tient’s surgical side. When performing bilateralTHAs, the perioperative nurse moves the view-ing box to the opposite side after the first hipprocedure is complete. The radiology technolo-gist places the fluoroscopy unit (ie, C-arm) onthe opposite side of the surgical site and situ-ates the C-arm monitor on the opposite sidebut distal to the C-arm. The nurse ensures thatan upper-body warming blanket, which is usedfor thermoregulation, is available and function-ing, and that the warming unit is near the headof the OR bed. The autotransfusion device,which may be used particularly during bilateralTHAs, and the electrosurgery unit (ESU) are
TABLE 1Data for Different Approaches to Total Hip Arthroplasty
Table-enhanced anterior1 Direct anterior2 Mini-posterior2
(N = 1,723) (N = 99) (N = 96)Surgical time
Mean 64 minutes 104.7 minutes 100.4 minutesMedian 85 minutes Not reported (NR) NR
Length of incision10 cm NR NR
Length of stayMode 3 days NR NRMean NR 22.2 days 30.4 days
Blood lossAverage 400 mL 526.1 mL 426.9 mL
Number of dislocations
3 hips 0 hips 1 hip
1. J Matta, MD, Founder and Director, Hip and Pelvis Institute, St John’s Health Center, Santa Monica, CA;unpublished data; June 9, 2008.2. Nakata K, Nishikawa M, Yamamoto K, Hirota S, Yoshikawa H. A clinical comparative study of the directanterior approach with mini-posterior approach two consecutive series. J Arthroplasty. 2008 Jun 12. [Epubahead of print].
![Page 5: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/5.jpg)
Table-Enhanced Anterior Total Hip Arthroplasty JULY 2009, VOL 90, NO 1
also positioned near the head of the bed. Theroom layout for a left THA is shown in Figure 3.
PREOPERATIVE ASSESSMENTAs part of performing a routine systematic
and thorough review of the surgical patient,the perioperative nurse meets the patient andhis or her family members in the preoperativeholding area, verifies the patient’s identity,and performs an assessment. Preoperative as-sessment and physical findings provide animportant baseline with which to comparepostoperative assessment data. The nurse’sphysical assessment of the patient scheduledfor anterior THA includes • assessing the patient’s current level of pain
using a rating scale of zero to 10,• identifying prior orthopedic injuries or mo-
bility issues,• identifying prior orthopedic procedures, and• performing a skin assessment.The perioperative nurse also confirms theavailability of blood products (eg, autologousor direct donor blood) and the completion ofblood typing and cross-matching. He or shethen verifies allergies and NPO status.
To protect the patient during transfer andpositioning, the nurse may need additionalpadding to support the patient’s arms. The
nurse alerts perioperative team members if thepatient has any limited range of motion, previ-ous injuries, mobility issues, or any other restric-tions. This information alerts surgical teammembers to use caution when manipulating thetable during the procedure or while rotating thepatient’s leg. The nurse notes whether the pa-tient has an ankle injury on the surgical side orhas any implanted hardware so that he or sheknows to take care when placing the ESUgrounding pad and avoid placement areas thatwould allow electrical current to pass throughthat area. The perioperative nurse notes anddocuments any altered skin integrity.
The perioperative nurse reviews the med-ical record for pertinent laboratory values anddiagnostic studies (eg, chest x-ray, completeblood count) and ensures the presence ofproper documentation. The anesthesia careprovider meets the patient and obtains in-formed consent for anesthesia before trans-porting the patient to the surgical suite.
After the patient and surgeon have initiatedverification of the hip to be replaced, the circu-lating nurse confirms this information by • reviewing the surgical consent, • checking how the procedure is scheduled,• conferring with the surgeon, and • confirming all the information with the patient.
Figure 2 • Orthopedic table used to place patients in the supine position for anterior-approach total hip arthroplasty. The model isseen with the right leg in flexion and external rotation. The purpose of this photograph is to identify the intricate table parts butdoes not necessarily reflect best practices in patient positioning. Photograph courtesy of Mizuho OSI, Union City, CA.
perineal postfemoral hook leg support
spar handle
rotation lock
spar lock
spar
gross traction lockfemoral liftfoot control
femoral lift
lateral traction bar
rotationhandle
hand control
fine tractionhandleboot lock
aornjournal.org • 57
![Page 6: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/6.jpg)
JULY 2009, VOL 90, NO 1 Munro
After identifying the correct surgical site, thenurse compares that information with the sur-gical site marking performed by the surgeon.The nurse resolves discrepancies in this infor-mation before leaving the preoperative hold-ing area with the patient.
Patient education, which is provided by theperioperative nurses working in the preopera-tive admissions area and in the OR, includes • care that will be provided during surgery,• postoperative pain management,• signs and symptoms of infection, and• the recovery process (see Patient Education
Sheet).The nurse explains the intraoperative and im-mediate postoperative periods and assesses thepatient’s level of understanding. The nurse
gives the patient and family members an oppor-tunity to ask questions and express fears or con-cerns before transporting the patient from thepreoperative holding area to the OR. The nursethen develops a plan of care specific for this pa-tient and the proposed procedure (Table 2).
INTRAOPERATIVE CAREWhen the circulating nurse, surgeon, and
anesthesia care provider have completed theirpatient assessments, the circulating nurse trans-ports the patient to the OR and assists the anes-thesia care provider in applying monitoringequipment. The anesthesia care provider anes-thetizes the patient on the transport cart beforethe patient is moved to the orthopedic table. Be-fore transfer, the perioperative nurse places the
58 • AORN JOURNAL
surgeon
autotransfusiondevice
Mayostand
fluoroscopy unit
circulating nurse
assistant
radiologytechnologist
fluoroscopy
monitor
assistant
second circulating nurse
back table
scrub person
forced-air warming unit
x-ray viewing box
electrosurgical unit
anesthesia care provideranesthesia
cart
Figure 3 • Setup of the OR for a left anterior approach total hip arthroplasty. Scrubbed personnel are in sterile blue scrubgowns; unscrubbed personnel are in green scrub attire.
![Page 7: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/7.jpg)
Table-Enhanced Anterior Total Hip Arthroplasty JULY 2009, VOL 90, NO 1
aornjournal.org • 59
Anterior-Approach Total Hip Replacement1
OverviewThe hip is a ball-and-socket joint made up of the ball(femoral head) and socket (acetabulum). As you getolder, you may suffer from diseases of the hip (arthri-tis) or injuries (broken hip). If you suffer from painand poor hip movement, it may be difficult for youto perform normal activities of daily living and physi-cal exercise. You may need a total hip replacement(THR), which is also called total hip arthroplasty.
Advantages to the anterior approachTraditionally, THR surgery is performed with the pa-tient in the lateral (side-lying) position. A newer ap-proach is to perform the procedure with the patientsupine (lying on his or her back). There are numer-ous advantages to surgery in this position, such as• spending less time in the hospital and recover-
ing faster because the hip is replaced withouttaking the muscles off the pelvis or femur;
• less risk of the hip dislocating (coming out ofthe socket) after surgery and no limit to hipmovement;
• being able to have both hips replaced at onetime, if needed, instead of having to undergotwo surgeries because you do not have to beturned over to get to the second hip;
• having a smaller incision; and• being able to have x-rays taken during surgery
to make sure the artifical hip is in the correctposition rather than waiting to have x-raystaken after surgery.
Risks of undergoing a hip replacementAs with any THR surgery, there are risks. Possiblecomplications of anterior THR surgery include hipdislocation, infection, injury to nerves or bloodvessels, and need for the surgery to be redone.
How is anterior approach THR performed?Your surgeon, anesthesia care provider, and ORnurse will meet you in the preoperative area tomake sure you are ready for surgery and to answerany questions. You will then be taken to the OR ona stretcher. After you go to sleep with anesthesia,the OR team will put you into the supine positionon the special orthopedic OR bed. This bed allowsthe OR nurse to move your leg during the surgery,which helps the surgeon remove your old hip andput in the new hip implants. After surgery, the ORteam will move you to your recovery bed and takeyou to the recovery room.
Postoperative careTypically, patients stay in the hospital 1 to 3 daysafter undergoing anterior THR of one hip or 2 to 5days after having both hips replaced.• While you are recovering from surgery, you may
• feel tired or uncomfortable,• not have a bowel movement for several days, or • lose your appetite or have nausea or vomiting.
• You will have no hip movement restrictions andwill have physical therapy several times a day.
What happens after I go home?When you are discharged from the health care facility, you • will continue with physical therapy to regain
mobility and normal activity;• may shower but should not immerse the incision
in water (bath, pool) until two weeks after surgery;• may have some thigh soreness, swelling, or
bruising but these should gradually improve; and• may have clicking in your new hip that will go away
as the swelling decreases and your muscles tighten.
Call your physician immediately if you experienceany of the following postoperative complications:• swelling or excessive bleeding from the surgical site;• coldness or numbness in your legs;• sudden weakness or dizziness; or• back, chest, abdominal, or groin pain.
1. Matta J. Hip replacement surgery—the anteriorapproach: what you need to know. Hip & Pelvis Insti-tute, Saint John’s Health Center. Santa Monica, CA.http://www.hipandpelvis.com. Accessed May 28, 2009.Revised with permission.
Patient Education
normal hip jointhip joint affectedby osteoarthritis
artificial joint
Illustration by Kurt Jones
![Page 8: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/8.jpg)
JULY 2009, VOL 90, NO 1 Munro
60 • AORN JOURNAL
TABLE 2Nursing Care Plan for a Patient Undergoing Anterior-Approach Total Hip Arthroplasty
Nursing interventions• Transports according to individual needs.• Evaluates for signs and symptoms of skin
and tissue injury as a result of transfer ortransport.
• Identifies physical alterations that requireadditional precautions for procedure-specificpositioning.
• Verifies presence of prosthetics or correctivedevices.
• Positions the patient.• Evaluates for signs and symptoms of injury
as a result of positioning.
• Confirms identity before the operative or in-vasive procedure and verifies operative pro-cedure, surgical site, and laterality.
• Implements protective measures before theoperative or invasive procedure.
• Applies safety devices.• Implements protective measures to prevent
skin/tissue injury due to mechanical sources.• Performs required counts.• Uses supplies and equipment within safe
parameters.• Records devices implanted during the oper-
ative or invasive procedure.• Maintains continuous surveillance.• Evaluates for signs and symptoms of physi-
cal injury to skin and tissue.
• Assesses susceptibility for infection.• Implements aseptic technique.• Classifies surgical wound.• Performs skin preparations.• Protects from cross-contamination.• Minimizes the length of invasive procedure
by planning care.• Initiates traffic control.• Administers prescribed prophylactic
treatments.• Encourages deep breathing and coughing
exercises.• Administers care to wound site.• Monitors for signs and symptoms of
infection.• Assesses knowledge regarding wound care and
OutcomestatementThe patient is free fromsigns andsymptoms of injury related totransfer/transport.
The patient is free fromsigns andsymptoms of injury related to positioning.
The patient is free fromsigns andsymptoms of injurycaused byextra neousobjects.
The patient isfree fromsigns andsymptoms ofinfection.
The patientdemonstratesknowledge of woundmanagement.
DiagnosisRisk for impaired skinintegrity
Risk for perioperativepositioning injury
Risk for injury
Risk for infection andknowledgedeficit regard-ing woundcare
Interim outcomestatementThe patient is freefrom signs andsymptoms of injury related to transfer/transport on dis-charge from the OR.
The patient’s peripheral tissueperfusion is consistent with preoperative statusat discharge fromthe OR.
The patient’s skin condition, other than incision, is unchanged between admissionand discharge from the OR.
The patient is freefrom unplanned retained objects after surgery.
The patient isafebrile and freefrom signs andsymptoms of infection.
At the time of dis-charge, the patientverbalizes signs and symptoms ofwound infection toreport immediatelyto the surgeon.
The patient and family members
![Page 9: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/9.jpg)
Table-Enhanced Anterior Total Hip Arthroplasty JULY 2009, VOL 90, NO 1
aornjournal.org • 61
TABLE 2 (CONTINUED)Nursing Care Plan for a Patient Undergoing Anterior-Approach Total Hip Arthroplasty
Nursing interventionsphases of wound healing.
• Provides instruction about wound care andphases of wound healing.
• Evaluates responses to instruction aboutwound care and phases of wound healing.
• Assesses pain control.• Identifies cultural and value components
related to pain.• Implements pain guidelines.• Collaborates in initiating patient-controlled
analgesia.• Implements alternative methods of pain
control.• Provides pain management instruction.• Evaluates response to pain management
interventions and instruction.
• Notes sensory impairments.• Identifies barriers to communication.• Determines knowledge level.• Assess readiness to learn, identifies psychoso-
cial status, and assesses coping mechanisms.• Explains expected sequence of events.• Implements measures to provide psycholog-
ical support.• Provides status reports to family members.• Elicits perceptions of surgery.• Evaluates psychosocial response to plan of
care and to instructions.
• Provides instruction based on age and iden-tified need.
• Identifies expectations of home care.• Evaluates environment for home care.• Evaluates response to instruction.
Outcomestatement
The patientdemonstratesand/or reports adequatepain controlthroughoutthe perioper-ative periodand demon-stratesknowledge of pain management.
The patientdemon-stratesknowledgeof the ex-pected re-sponses tothe operativeor invasiveprocedure.
The patientparticipatesin the rehabilitationprocess.
Diagnosis
Acute pain
Anxiety andcompromisedfamily coping
Impairedphysical mobility, ineffectivetherapeuticregimen management,and knowledgedeficit regarding therehabilitationprocess
Interim outcome statementdemonstrate correcttechnique for applying a wounddressing at time ofdischarge.
The patient verbal-izes control of pain.
The patient participates in management of pain control beforeand immediatelyafter surgery.
The patient andfamily membersverbalize realisticexpectations re-garding discomfortafter surgery.
The patient verbalizes the sequence of eventsto expect before and immediatelyafter surgery andstates realistic expectations regarding recoveryfrom procedure.
The patient andfamily membersverbalize realisticexpectations regarding rehabili-tation after surgery.
The patient describes the prescribed rehabilitation regimen to followimmediately afterdischarge from thefacility.
![Page 10: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/10.jpg)
JULY 2009, VOL 90, NO 1 Munro
patient’s feet into boots that will be fastened tothe table spars. The nurse may apply pneumaticcompression sleeves to both of the patient’s legsto reduce the risk of deep vein thrombosis. Allsurgical team members actively participate in asurgical time out to verify the correct patient,correct site and laterality, and correct surgeryand also ensure that all equipment and supplies,including implants, are immediately available.
POSITIONING. Surgical team members (eg, sur-geon, fellow, resident, assistant, circulatingnurses) help transfer the patient to the orthope-dic table and assist with positioning. If the teammembers are temporarily unavailable, the circu-lating nurse recruits assistive personnel and,with the help of the anesthesia care provider,transfers the patient to the orthopedic table andpositions him or her, assessing for pressurepoints and body alignment. The surgeon ulti-mately is responsible for checking the final po-sition and ensuring that it is acceptable.
Team members position the patient close tothe perineal post, which is used to accommodatetraction on the leg. The nurse places both the pa-tient’s arms on arm boards extended at less than90-degree angles to the bed. After placing a sup-port under the patient’s nonsurgical leg, thenurse places both of the patient’s legs in slightinternal rotation (Figure 4). The nurse then as-sesses the patient for possible pressure pointsand places additional padding to support thepatient or relieve pressure as needed.
SURGICAL SKIN PREP. The surgical prep site for aTHA spans from the patient’s midline ab-domen laterally to the level of the bed, distalto the middle of the thigh, and proximal to thenavel (Figure 5). The surgeon may want thecirculating nurse to expand proximal expo-sure above the patient’s navel to ensure thatthe anterior superior iliac spine is included inthe prep. This surgical approach allows bilat-eral THA preps to be conveniently performedwith a single preparation and draping of bothhips. After the prep, the nurse applies a smallamount of gross traction, as well as a mildamount of abduction, before locking the tablein position. This position enhances the land-marks of the hip for surgical exposure (Figure6). The nurse positions both of the patient’slegs similarly, as the nonsurgical side will be
62 • AORN JOURNAL
Figure 4 • The nurse attaches the boots on the patient’s legsin slight internal rotation to the table spar.
Figure 5 • Typically, the patient is prepped from the midlineabdomen laterally to the level of the bed, distally to themiddle of the thigh, and proximally to the navel.
Figure 6 • Hip landmarks are identified for surgical exposure.
![Page 11: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/11.jpg)
Table-Enhanced Anterior Total Hip Arthroplasty JULY 2009, VOL 90, NO 1
used as a radiographic reference. The circulating nurse confirms correct posi-
tioning with the physician before the scrubperson applies the surgical drapes becausevariations of anatomy and physique may re-quire alterations. It is also important that thecirculating nurse ensure that each table con-trol has been locked (ie, the boots at the junc-tion of the attachment to the bed, the swiveljoint, the rotation of the legs, the gross tractionfor both spars).
FLUOROSCOPY. Anterior to posterior x-rays arehard to obtain when the patient is in the lateralposition because hip alignment may not besymmetric. Most traditional THAs are per-formed in the lateral position; therefore, thesurgeon orders x-ray films to be obtained aftersurgery in the postanesthesia care unit (PACU)to confirm component placement. The pa-tient’s supine position on the radiolucent or-thopedic table during an anterior approachTHA facilitates the use of fluoroscopy duringthe surgery. Intraoperative use of fluoroscopynot only facilitates accurate component posi-tion, but also greatly reduces the risk of a sec-ond procedure for exchange of implants whenpostoperative x-rays are taken after the pa-tient has left the surgical suite. The surgeoncompares radiographic landmarks to confirmequal leg length and correct offset during sur-gery before wound closure.
Dr Matta calculated an average fluoroscopytime of 24.9 seconds on 102 of his most recentarthroplasties (J. Matta, MD; unpublisheddata, August 2007).5 Published reports of fluo-roscopy time for these procedures are notavailable currently, and not all surgeons usefluoroscopy during these procedures. Annualradiation exposure limits established by theNuclear Regulatory Commission are set at atotal effective dose equivalent of 5 roentgenequivalent units (REMs) for radiation workersand 0.1 REMs for members of the public.9
As with any procedure in which fluo-roscopy is used, the surgical team should ad-here to recommended safety measures to re-duce their exposure to ionizing radiation.AORN’s “Recommended practices for reduc-ing radiologic exposure in the perioperativepractice setting,” states, “The greater the dis-
tance an individual or target is from thesource of radiation, the less the amount of ra-diation exposure.”10(p1000) Radiation exposurecan be reduced by one-quarter when the dis-tance from the source is doubled.10 Radiationexposure time is minimal but the use of dis-tance and shielding and the consistent use ofdosimeters can reduce radiation risks.
The radiology technologist positions thefluoroscopy unit on the opposite side of thesurgical team next to the nonsurgical hip andperpendicular to the patient. The circulatingnurse also places a thyroid shield on the pa-tient’s neck for radiation exposure protection.According to Dr Matta’s data, the ionizing ra-diation exposure for both the patient and sur-gical team during the procedure is minimal (J. Matta, MD; unpublished data, August 2007).
Use of the fluoroscopy unit and the ortho-pedic table are based on the surgeon’s prefer-ence. The surgeon may choose not to use fluo-roscopy or may limit its use throughout theprocedure. The surgeon may also decide toperform the surgery without the use of the or-thopedic table. The anterior approach to THAperformed without the use of the orthopedictable increases the difficulty of access to thefemur, and patient selection is more limitedbecause surgeons must avoid operating on
aornjournal.org • 63
Surgical team members should adhere
to recommended safety measures to
reduce their exposure to ionizing
radiation, such as using distance
and shielding to decrease the
amount of radiation exposure and
consistently using dosimeters to
monitor radiation risks.
![Page 12: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/12.jpg)
JULY 2009, VOL 90, NO 1 Munro
heavy and/or muscular patients because ofthe difficulty of accessing the femur.
SURGICAL PROCEDURE AND TABLE OPERATIONTo better anticipate the circulating role dur-
ing an orthopedic table-enhanced procedure,the nurse must have a thorough understand-ing of what occurs (Table 3). Understandingand using proper body mechanics duringtable manipulation is essential to prevent in-jury to both the patient and the circulatingnurse. More than one circulating nurse is re-quired during this procedure. One nursestands at the foot of the orthopedic tablethroughout the procedure to perform neededtable operations, always giving direct atten-tion to the surgeon and to the progress of theprocedure. Another circulating nurse is re-quired to provide direct patient care and meetall additional circulating responsibilities dur-ing the procedure.
The circulating nurse operating the table pro-vides individualized care to ensure safety of thepatient during orthopedic table-enhanced THA.For instance, osteopenic bone is at higher riskof fracture and the force of external rotationmay lead to a tibial or ankle fracture. The forceused on a patient with osteopenia, therefore, ismore gentle. The nurse assigned to assist thesurgical team performs all table operationsunder the direction of the surgeon throughoutthe procedure using the table controls (eg, finetraction, gross traction, rotation) on the foot ofthe orthopedic table, which are not within thesterile field (Figure 7). The nurse does not ro-tate the patient’s leg to the extent of his or herrange of motion, but rather stops rotationwhen resistance is met. The surgeon directsthe circulating nurse regarding the amount ofrotation to apply based on the amount of re-sistance met and will direct the nurse if fur-ther rotation is indicated. This rotation can beapplied safely with clear communication anddirection from the surgeon combined withcareful consideration of the patient’s physicalstatus. The nurse’s preoperative assessmentplays a large role in this aspect of the proce-dure. Before the beginning of the procedure,the surgeon and the circulating nurse whoperformed the preoperative physical assess-
ment on the patient discuss the patient’s con-dition and the individualized plan of care, in-cluding the degree of rotation anticipated. Astable movements are being performed, thenurse communicates with the surgeon regard-ing the extent of force being used and, if addi-tional exposure is requested, the nurse de-scribes the force being used and resistance, ifany, that he or she feels.
The surgeon removes the femoral headwith assistance from the nurse, who uses thetable controls at the foot of the table to manip-ulate the degree of fine traction and externalrotation. Several turns of fine traction controlwhile the gross traction mechanism is stilllocked creates a space between the femoralhead and the acetabulum where the surgeoninserts a bone skid (ie, flat instrument with adip/scoop on the distal ends in which to dis-tract the femoral head from the acetabulum).The circulating nurse then releases the finetraction almost entirely by reversing the turns.For example, if three turns of traction wereinitially applied, then two turns in reversemay be sufficient. The circulating nurse thenexternally rotates the hip approximately 20degrees to allow the surgeon to insert acorkscrew, after which both the surgeon andcirculating nurse apply further external rota-tion to dislocate the hip.
The circulating nurse may apply fine trac-tion to distract the neck osteotomy and facili-tate the surgeon’s extraction of the femoralhead. The surgeon may cut the femoral headin situ without dislocation, but this may makeextraction more difficult. While the surgeonprepares the acetabulum, the circulating nurseexternally rotates the leg approximately 45 de-grees and maintains a slight amount (ie, oneturn) of fine traction to provide better expo-sure. The surgeon may initiate fluoroscopy atthis point to confirm depth of reaming andprosthesis insertion.
After the acetabular components have beeninserted, the circulating nurse must positionthe patient for femoral preparation. After un-locking the gross traction on the spar, the cir-culating nurse applies some internal rotationto assist the surgeon in posterior placement ofthe femoral hook. The circulating nurse then
64 • AORN JOURNAL
![Page 13: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/13.jpg)
Table-Enhanced Anterior Total Hip Arthroplasty JULY 2009, VOL 90, NO 1
aornjournal.org • 65
TABLE 3Surgeon Preference Card for
Orthopedic Table-Enhanced Total Hip ArthroplastyMedicationsPreoperative antibiotic: 1 g vancomycin IVIrrigation and glove-rinse solution: 1 L normal
saline with 50,000 units bacitracin and 500,000 units polymyxin
InstrumentsTotal hip arthroplasty setsAcetabular reamers and osteotome setPower drill and batteryAnterior traction set
Sterile suppliesSelected implants and trial sizersTotal hip arthroplasty pack#1 polyglycolic acid suture CT-2 (anterior
capsule)#1 polyglycolic acid suture CT-1 (deep fascia)2-0 polyglycolic acid suture CT-2 (fascia)3-0 poliglecaprone 25 suture PS-1 (subcuta-
neous closure)
Room setup and equipment settingsElectrocautery machine (settings: 60/60)x-ray view boxFluoroscopy unit and monitorSequential compression device (SCD) leggings
and unitForced-air warming unit (109.4° F/43° C) and
upper-body blanketAutotransfusion device (bilateral THAs only)Room furniture• Double-decker back table• Small back table• Double ring stand x 1• Single ring stands x 4• 1 jumbo and 1 regular Mayo stand
Steps: place 1 under the OR bed, 1 near armboard on surgical side if observer present
Hair removalRemove patient’s hair at surgical site, only if
necessary.Perform hair removal in preoperative area, if
at all possible, using tape to contain hair.
Position• Insert indwelling urinary catheter after
induction of anesthesia but before patient is transferred onto orthopedic table
• Wrap perineal post with soft roll• Wrap patient’s feet with soft roll, if he or
she is not wearing socks• Apply SCDs after putting on the table boots
but before transferring patient to table.• Place patient in supine position on the
orthopedic table with padded arm boards
Prep2% chlorhexidine gluconate/70% isopropyl
alcohol solution
DrapingBenzoinHand towelsU-shaped, antimicrobial surgical drapeIncise drapes4 3/4 sheets (x 2 distal, x 2 proximal)Full sheet x 21 x-large and 1 regular Mayo coverPlastic split sheet x 2: 1 proximal, 1 distalPaper split sheet x 2: 1 proximal, 1 distal
DressingsLiquid skin adhesiveSelf-adhesive wound approximating stripsNonadherent dressing pad and 4” x 4” gauzeSoft, cloth surgical tape
Terms for using the orthopedic table• Traction on
3 turns of fine traction (more if requested);count out loud.
• Traction off2 turns of fine traction; count out loud.
• External and internal rotationUsed for femoral head removal and acetab-ular reaming.Twist knob once to lock and unlock.
• Unlock rotationAllows surgeon to guide the foot position.Lock when the surgeon lets go of the foot. Keep holding the rotation handle while the surgeon is positioning, but allow him to move the patient’s leg.
• Externally rotate, unlock the gross traction,extend and adduct the patient’s legUsed for femoral broaching.Place leg under nonsurgical leg on the floor.No need to lock spar when extended.
• Flex the hipBring leg up level with the nonsurgical leg.
• Reduce the hipInternally rotate the leg at the same time as pulling gross traction.
• Dislocate the hipExternally rotate the leg at the same time as pulling gross traction.
![Page 14: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/14.jpg)
JULY 2009, VOL 90, NO 1 Munro
externally rotates the patient’s leg approxi-mately 90 degrees, to the extent of the pa-tient’s maximum range of motion as directedby the surgeon. The circulating nurse then ex-tends the patient’s hip with the table spar po-sitioned to the floor and adducted so the pa-tient’s leg is crossed under the other spar. Thecirculating nurse must ensure that the grosstraction mechanism is unlocked before ex-tending the hip to prevent stretching of thefemoral nerve. To further expose the femur,the surgeon raises the femoral lift after he orshe has placed the femoral hook into position.
After the surgeon inserts the trial componentsand removes the femoral hook, the circulatingnurse flexes the hip and returns it to its originalneutral position. The circulating nurse reduces thehip with simultaneous application of internal ro-tation and gross traction by manually pulling androtating the gross traction handle of the table. Theamount of pulling should be just enough to ac-commodate reducing the hip. A gentle push of thegross traction handle after reduction is achievedensures that no traction tension remains.
The surgeon obtains fluoroscopic views ofboth hips and compares them with printedimages on transparency film (Figure 8). Ifneeded, the surgeon may request abductionand adduction of the spars to match the align-ment of both hips. The circulating nurseshould identify the last position of the sparsplacement so he or she can readjust the sparsto this position when the hip is returned to aneutral position.
To dislocate the hip for removal of the trialcomponents, the circulating nurse externally ro-tates the hip and applies gross traction. This isdone simultaneously and similarly to the reduc-tion of the hip. The surgeon reinserts the femoralhook, after which the circulating nurse externallyrotates the leg and extends and adducts the pa-tient’s hip. Reduction and dislocation occurs asoften as is necessary for the surgeon to inserttrial components and determine the best compo-nent sizes for the patient. After the surgeon in-serts the components (Figure 9), the circulatingnurse performs a reduction of the hip (ie, adjuststhe spars to the desired position) and ensuresthat flexion and rotation are the same for both ofthe patient’s hips. The radiology technologisttakes and prints final views via fluoroscopy.
POSTOPERATIVE CAREThe circulating nurse reassesses the circula-
tion of both of the patient’s feet and the condi-tion of the skin around the perineal area after theprocedure to ensure that no injury has occurred
66 • AORN JOURNAL
Figure 8 • The surgeon compares fluoroscopic views of bothhips and with printed images on transparency film of thereplaced total hip.
Figure 7 • Table controls on the foot of the orthopedic tableare not within the sterile field.
![Page 15: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/15.jpg)
Table-Enhanced Anterior Total Hip Arthroplasty JULY 2009, VOL 90, NO 1
before helping to transport the patient to thePACU. If the patient has not been given a re-gional anesthetic and is able to obey com-mands, the nurse assesses the mobility of thepatient’s lower extremities through passiverange of motion. The circulating nurse’s hand-off communication includes the surgery per-formed, outcomes related to the procedure,the patient’s allergies, and the patient’s cur-rent condition. The PACU receiving nurse ver-ifies the information received and asks the cir-culating nurse questions as needed.
The location of the incision and lack of mus-cle dissection in a patient who has undergoneanterior THA decrease the patient’s postopera-tive pain, allow for early ambulation, and re-duce the risk of dislocation. Proper postopera-tive wound care reduces the risk of infection.Physical therapy begins within hours after sur-gery. Activity is not restricted because the pa-tient can bear weight immediately, and activityis increased according to the patient’s tolerancelevel. Many patients use a walker to begin am-bulating with assistance on the same day oftheir surgical procedure or the following day,depending on the time of day that the surgerywas performed, and most patients can walkwith a cane by the time they are discharged.Some patients may use an assistive device, suchas a walker or crutches, while others do not re-quire any assistance at discharge. Generally,most patients are walking without aids within
seven to 10 days after surgery. For those patientswho continue to use aids beyond the seven- to10-day period, use of these aids is usually dis-continued after two to three weeks (J. Matta,MD, e-mail communication, June 10, 2008).
There are no dislocation precautions for thepatient who has undergone an anterior THA.This eliminates the postoperative need for anabduction pillow, a traction sling, a raised toi-let seat, or a hip cushion. The use of sequen-tial compression devices on both legs duringthe postoperative period helps prevent deepvein thrombosis. Typically, a patient is dis-charged home from one to three days after un-dergoing a unilateral anterior THA and two tofive days after a bilateral procedure.
CONCLUSIONThe use of an orthopedic table enhances the
surgeon’s ability to perform an anterior ap-proach for THA. The supine position of the pa-tient and the radiolucency of the orthopedictable create ideal conditions for the use of fluo-roscopy, which increases accuracy of componentplacement and ensures matching leg length.
The perioperative nurse plays a vital role inthe successful execution of the orthopedic table-enhanced, anterior-approach THA in the supineposition. Under the direction of the surgeon, thecirculating nurse is responsible for maneuver-ing the orthopedic table to provide acetabularand femoral exposure to accommodate hip re-placement. These table functions have multiplebenefits that appeal to surgeons and patients,including decreased soft tissue trauma; lesspain after surgery; shorter hospitalization; a sin-gle, smaller incision; and a very low risk ofpostoperative hip dislocation.
An understanding of the complete anteriorapproach procedure, proper technique whileoperating the orthopedic table, and clear com-munication between members of the surgicalteam help minimize complications. Coordina-tion between the surgeon and perioperativenurse, as always, is imperative.
Acknowledgement: The author thanks Joel Matta,MD; Founder and Director, Hip and Pelvis Institute,Saint John’s Health Center, Santa Monica, CA, forallowing use of his data and consulting on the article.
aornjournal.org • 67
Figure 9 • The surgeon inserts the femoral hook and retrac-tors to insert the components during a resurfacing total hiparthroplasty (ie, surface replacement). The femoral headshown is larger than the implant for a total hip replacement.
![Page 16: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/16.jpg)
JULY 2009, VOL 90, NO 1 Munro
Editor’s note: ProFX® and Hana® are registeredtrademarks of Misuho OSI, Union City, CA. Publi-cation of this article does not imply AORN endorse-ment of companies or products mentioned herein.
REFERENCES1. Matta JM, Ferguson TA. The anterior approachfor hip replacement. Orthop. 2005;28(9):927-928.2. Matta JM. The anterior approach for total hiparthroplasty: background and operative technique.August 2005. Hip and Pelvis Institute. http://www.hipandpelvis.com/patient_education/totalhip/index.html. Accessed April 28, 2008. 3. Matta JM. The anterior approach for total hip arthro-plasty: background and operative technique. In: MISTechniques in Orthopedics. Scuderi GR, Tria AJ, BergerRA, eds. New York, NY: Springer; 2007:121-140.4. Matta JM, Shahrdar C, Ferguson TA. Single-incisionanterior approach for total hip arthroplasty on anorthopaedic table. Clin Orthop Relat Res. December2005;441:115-124.5. Kennon RE, Keggie JM, Wetmore RS, Zatorski LE,Huo MH, Keggi KJ. Total hip arthroplasty through aminimally invasive anterior surgical approach. J BoneJoint Surg Am. 2003;85-A(Suppl 4):39-48.6. Siguier T, Siguier M, Brumpt B. Mini-incision an-terior approach does not increase dislocation rate: a
study of 1037 total hip replacements. Clin OrthopRelat Res. September 2004;426:164-173.7. Rachbauer F. Minimally invasive total hiparthroplasty via direct anterior approach [In Ger-man]. Orthopade. 2005;34(11):1103-1110.8. Nakata K, Nishikawa M, Yamamoto K, Hirota S,Yoshikawa H. A clinical comparative study of thedirect anterior approach with mini-posterior ap-proach two consecutive series. J Arthroplasty. 2008Jun 12. [Epub ahead of print].9. Part 20—standards for protection against radia-tion. United States Nuclear Regulatory Commis-sion. http://www.nrc.gov/reading-rm/doc-collections/cfr/part020/. Accessed May 19, 2009.10. Recommended practices for reducing radiologi-cal exposure in the perioperative practice setting.In: Perioperative Standards and Recommended Practices.Denver, CO: AORN, Inc; 2009:455-466.
68 • AORN JOURNAL
Cassendra A. Munro, RN, MSN, CNOR,is a perioperative clinical nurse specialist atSaint John’s Health Center, Santa Monica,CA. Ms Munro has no declared affiliation thatcould be perceived as a potential conflict of in-terest in publishing this article.
![Page 17: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/17.jpg)
1. Advantages to the orthopedic table-enhanced anterior approach for perform-ing THA include
1. improved ability to use fluoro scopy.2. limited soft tissue trauma.3. improved exposure of the femur.4. increased femoral access.
a. 1 and 4b. 2 and 3c. 1, 3, and 4d. 1, 2, 3, and 4
2. One advantage for patients who undergoTHA using the anterior approach is imme-diate weight bearing on the surgical leg.a. trueb. false
3. The perineal post is used toa. prevent perineal nerve injury.b. accommodate traction on the legc. provide a landmark during fluoroscopy.d. prevent exposure of patient’s genitals.
4. Intraoperative use of fluoroscopy 1. facilitates accurate component position.2. reduces the risk of a second procedure
for implant exchange.
3. unnecessarily exposes the patient to large quantities of ionizing radiation.
a. 1 and 2b. 1 and 3b. 2 and 3c. 1, 2, and 3
5. More than one circulating nurse is re -quired during table-enhanced THA. a. trueb. false
6. The nurse’s preoperative assessmenthelps determine the degree of hip rota-tion anticipated. a. trueb. false
7. The circulating nurse uses the table con-trols at the foot of the table to
1. manipulate the degree of fine traction and external rotation to create a space between the femoral head and the acetabulum.
2. release the fine traction to create the space to insert the skid.
3. externally rotate the hip to allow the surgeon to insert a corkscrew.
ExaminationThe Perioperative Nurse’s Role in Table-Enhanced
Anterior Total Hip ArthroplastyPURPOSE/GOAL
To educate perioperative nurses about caring for patients undergoing orthopedic table-enhancedanterior-approach total hip arthroplasty (THA).
BEHAVIORAL OBJECTIVESAfter reading and studying the article on anterior-approach THA, nurses will be able to
1. identify advantages of performing THA using the anterior approach with a radiolucent orthopedic table,
2. discuss nursing care of a patient who is undergoing anterior THA,
3. describe the anterior THA procedure, and
4. explain the nurse’s role in operating the orthopedic table used for anterior THA.
QUESTIONS
3.7
JULY 2009, VOL 90, NO 1 • AORN JOURNAL • 69© AORN, Inc, 2009
![Page 18: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/18.jpg)
ExaminationJULY 2009, VOL 90, NO 1
4. apply further external rotation to dis-locate the hip.
5. apply fine traction to distract the neck osteotomy and facilitate the surgeon’s extraction of the femoral head.
6. externally rotate the leg and maintain a slight amount of fine traction to pro-vide better exposure.
a. 1, 3, and 5b. 2, 4, and 6c. 2, 3, 4, 5, and 6d. 1, 2, 3, 4, 5, and 6
8. The location of the incision and lack ofmuscle dissection in a patient who has un-dergone anterior THA
1. allows for early ambulation.2. decreases the patient’s postoperative
pain.3. necessitates use of an adduction pillow.4. reduces the risk of dislocation.
a. 1 and 3b. 2 and 4c. 1, 2, and 4d. 1, 2, 3, and 4
9. Generally, most patients are walking with-
out aids within _________________ daysafter surgery. a. one to twob. two to threec. five to sevend. seven to 10
10. When discharging a patient who has un-dergone THA from the health care facility,the nurse should instruct the patient thathe or she
1. may have some thigh soreness, swell-ing, or bruising, which is normal and will gradually improve.
2. may shower but should not immerse the incision in water until two weeks after surgery.
3. should call the surgeon if there is clicking in the new hip, which is not normal.
4. will continue with physical therapy to regain mobility and normal activity.
a. 1 and 3b. 2 and 4c. 1, 2, and 4d. 1, 2, 3, and 4
70 • AORN JOURNAL
The behavioral objectives and exam -ination for this program were preparedby Rebecca Holm, RN, MSN, CNOR,clinical editor, with consultation fromSusan Bakewell, RN, MS, BC, direc-tor, Center for Perioperative Educa-tion. Ms Holm and Ms Bakewell haveno de clared affiliations that could beperceived as potential conflicts of in-terest in publishing this article.
This program meets criteria for CNOR and CRNFA recertification, as well asother continuing education requirements.
AORN is accred ited as a provider of continuing nursing education by theAmerican Nurses Creden tialing Center’s Commission on Accredit ation.
AORN recognizes these activities as continuing education for registerednurses. This recognition does not imply that AORN or the American Nurses Credentialing Center approves or endorses products mentioned in the activity.
AORN is provider-approved by the California Board of Registered Nursing,Provider Number CEP 13019. Check with your state board of nursing foracceptance of this activity for relicensure.
![Page 19: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/19.jpg)
The Perioperative Nurse’s Role in Table-Enhanced Anterior Total Hip Arthroplasty
© AORN, Inc, 2009
Event #09112Session #1087
Please fill out the application and answer formon this page and the evaluation form on the back
of this page. Tear the page out of the Journal or makephoto copies and mail with appropriate fee to:
AORN Customer Servicec/o AORN Journal Continuing Education
2170 S Parker Rd, Suite 300Denver, CO 80231-5711
or fax with credit card information to (303) 750-3212.
Additionally, please verify by signature that you have reviewed the objectives and read the
article, or you will not receive credit.
Signature ______________________________________
1. Record your AORN member identification number inthe appropriate section below. (See your membercard.)
2. Completely darken the spaces that indicate your an-swers to examination questions 1 through 10. Use blueor black ink only.
3. Our accrediting body requires that we verify the timeyou needed to complete this 3.7 continuing educationcontact hour (222-minute) program. ______
4. Enclose fee if information is mailed.
AORN (ID) #_________________________________________
Name_______________________________________________
Address_____________________________________________
City ___________________________________________________ State __________ Zip __________
Phone number _______________________________________
RN license #____________________________________________ State __________
Fee enclosed ___________________________________________
or bill the credit card indicated ■■ MC ■■ Visa ■■ American Express ■■ Discover
Card # __________________________________ Expiration date _____________________
Signature _______________________________________________________________ (for credit card authorization)
Answer Sheet 3.7
JULY 2009, VOL 90, NO 1 • AORN JOURNAL • 71
Fee: Members $23.50 (includes $5 processing fee); Nonmembers $42 (includes $5 processing fee)
New! Save time and money by completing this CE activity online. No processing fees at aorn.org/CE.
Program offered July 2009; The deadline for this program is July 31, 2012.
A score of 70% correct on the examination isrequired for credit. Participants receive feed-back on incorrect answers. Each applicant
who successfully completes this program willreceive a certificate of completion.
![Page 20: Perioperative Nurses Role Anterior THA[1]](https://reader034.fdocuments.in/reader034/viewer/2022051207/5448ce5cb1af9f5f618b4b47/html5/thumbnails/20.jpg)
72 • AORN JOURNAL • JULY 2009, VOL 90, NO 1 © AORN, Inc, 2009
This evaluation is used to determine theextent to which this continuing education
program met your learning needs. Rate theseitems on a scale of 1 to 5.
PURPOSE/GOALTo educate perioperative nurses about caringfor patients undergoing orthopedic table-enhanced anterior-approach total hip arthro-plasty (THA).
OBJECTIVESTo what extent were the following objectives ofthis continuing education program achieved?1. Identify advantages of performing THA
using the anterior approach with a radi-olucent orthopedic table,
2. Discuss nursing care of a patient who isundergoing anterior THA.
3. Describe the anterior THA procedure.4. Explain the nurse’s role in operating the
orthopedic table used for anterior THA.
CONTENTTo what extent5. did this article increase your know ledge
of the subject matter?6. was the content clear and organized?7. did this article facilitate learning?8. were your individual objectives met?9. did the objectives relate to the overall
purpose/goal?
TEST QUESTIONS/ANSWERSTo what extent10. were they reflective of the content?11. were they easy to understand?12. did they address important points?
LEARNER INPUT13. Will you be able to use the information
from this article in your work setting?a. yesb. no
14. I learned of this article viaa. the AORN Journal I receive as an AORN
member.b. an AORN Journal I obtained elsewhere.
c. the AORN Journal web site.15. What factor most affects whether you take
an AORN Journal continuing educationexamination?a. need for continuing education contact
hoursb. pricec. subject matter relevant to current
positiond. number of continuing education contact
hours offered
What other topics would you like to see ad-dressed in a future continuing education arti-cle? Would you be interested or do you knowsomeone who would be interested in writingan article on this topic?Topic(s): ____________________________________________________________________________Author names and addresses: _____________________________________________________________________________________________________________________________________________
Learner EvaluationThe Perioperative Nurse’s Role in
Table-Enhanced Anterior Total Hip Arthroplasty
3.7