
Perioperative Considerations in Care of the Elderly Fred Weitz MD Emory University Dept. of...
70
-
Upload
barnard-warren -
Category
Documents
-
view
214 -
download
0
Transcript of Perioperative Considerations in Care of the Elderly Fred Weitz MD Emory University Dept. of...


Perioperative Considerations in Care of the Elderly
Fred Weitz MD
Emory University
Dept. of Anesthesiology
Realities for the Practicing Anesthesiologist
More than 35 million people in U.S. are > 65 They account for almost half of hospital care
days 25-35% surgical cases
Most anesthesiologists are geriatric anesthesiologists!

All Geriatric Patients are not Created Equal!


People age at different rates:Organ Function

Organ Functional Reserve:Safety Margin of Organ Capacity

Considerations:
Cardiovascular function Respiratory function Airway Management Pharmacokinetics Body temperature regulation Postoperative Mental function

CV Changes with Aging
Connective tissue changes– Loss of elasticity
Loss of SA node cells, slowed conduction Myocyte death without replacement Decreased response to beta-receptor
stimulation
Aging Does Not Diminish:
Intrinsic quality of muscle– Heart does not weaken with age alone
Peripheral vasoconstriction– Enhanced sympathetic nervous system activity at
rest– More prone to hypotension with loss of sympathetic
tone

Arterial Stiffening
Reflected pressure from “stiffened arteries” increases pressure in aortic root during late systole
Leads to ventricular hypertrophy, impaired diastolic filling
Decreased Venous Compliance
Veins, like arteries, stiffen with age Stiff veins are less able to “buffer” changes in
blood volume– Volume shifts cause exaggerated changes in
cardiac filling pressure

Myocyte Death
Cardiac muscle cells die over time Remaining cells do not divide in adequate
numbers in adulthood Remaining cells hypertrophy to compensate
Another cause of ventricular hypertrophy

Ventricular Contraction
Slows with Aging Ventricle may not be fully relaxed during
beginning of diastolic filling phase
Result: Early diastolic filling is impaired


Dependence on High Filling Pressure
Young
End-Diastolic Volume
En
d-D
iast
olic
Pre
ssu
re
Elderly
Frank-Starling Curve

Consequences of Delayed Relaxation
Late diastolic filling depends on high left atrial pressure and atrial kick– Tachycardia and atrial fibrillation not well tolerated
Narrow range between inadequate filling pressure and fluid overload
Diastolic dysfunction may be the most common cause of heart failure in > 75 y/o

Can the Elderly Heart Increase Output?

Aging and Contractility:Response to Exercise
55
60
65
70
Young
Eje
ctio
n F
ract
ion
(%)
At Rest Maximal Exercise
Elderly
Stratton et al., Circ 1994;89:1648

Decreased Beta-Receptor Responsiveness
Diminished increase in heart rate with stress– Reduced maximum heart rate
Increase their stroke volume– From increase in end diastolic volume

Response to Anesthesia
Anesthetics can:– Remove sympathetic tone
– Dramatic when baseline tone is very high
– Directly depress heart, vascular smooth muscle– Diminish baroreceptor reflexes

Add to That …
Changes in sympathetic tone from waxing and waning surgical stimulus variable depth of anesthesia
Changes in patient’s volume status
Results in LABILE BLOOD PRESSURE !

Summary: Volume Dependence of the Elderly Heart
Elderly heart depends on late filling that in turn depends on left atrial pressure
Elderly heart is also stiff, so the left atrial pressure must be high in order to fill the LV
prone to diastolic dysfunction poor venous buffering of blood volume makes
maintenance of left atrial pressure difficult

Summary: Decreased Response to Beta-Receptor Stimulation
Lessened ability to increase in heart rate Lessened ability to increase ejection fraction


Aging and Respiratory Function
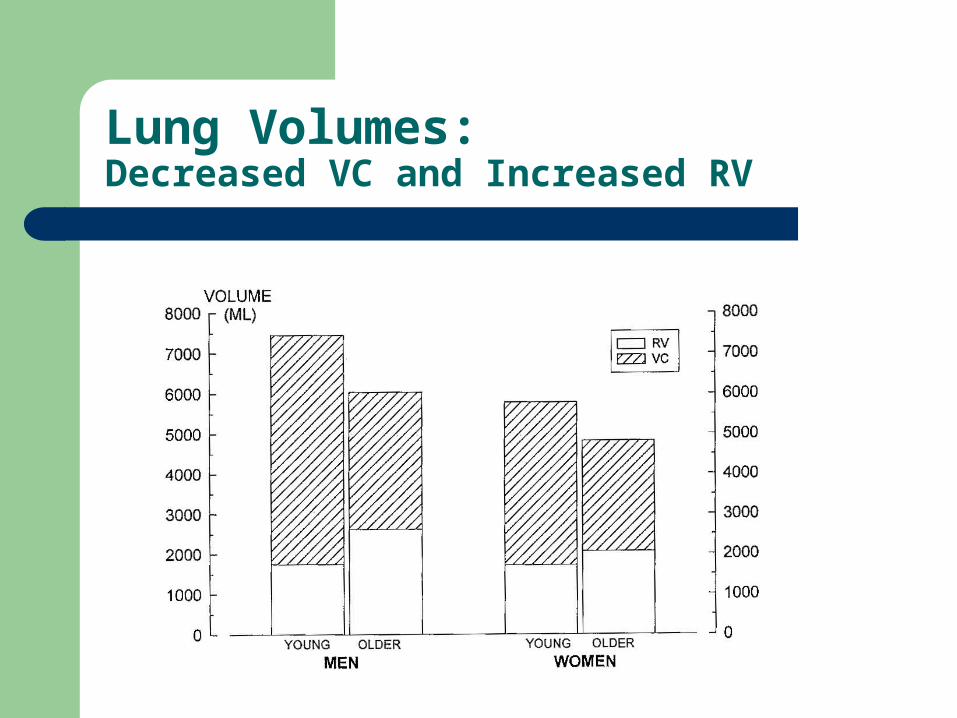
Lung Volumes:Decreased VC and Increased RV

Pulmonary Changes
Decreased thoracic elasticity
Decreased strength and endurance of respiratory muscles

Decreased Efficiency of Gas Exchange
Breakdown of elastin connections between connective tissue and alveolar tissue
Results in poor tethering of lung tissue to airways and other lung tissue
Airways are NOT held open Increases:
– Shunting– Dead space

Increased Shunt

Explains Effect of Age on paO2

Pre-oxygenation
Takes longer in elderly than in healthy young patients!

Airway Management:Diminished Afferentation
Stimulus threshold for vocal cord closure is increased
Increased risk of aspiration!
Airway Management:Changes with Aging
Arthritic Changes: Decreased cervical spine and neck mobility Smaller mouth opening Smaller glottic opening
– Smaller endotracheal tube
Fragile teeth

Remember…
Airway management may be more difficult Prone to airway collapse (risk of pneumonia) Higher work of breathing (risk of hypercarbia) Lower blood oxygen levels
(greater need for supplemental oxygen)
After leaving PACU, hypoxia more likely– from residual drug/CNS effects

Geriatric population is at significantly increased risk of respiratory failure in
the postoperative setting!


Pharmacology in the Elderly Patient

Increased Bolus Drug Effect
Decreased protein binding– Higher free, unbound plasma drug levels
Decreased volume of distribution Slower redistribution of drug
ALL of these INCREASE target organ levels!
Examples: Thiopental, Propofol

Increased Brain Sensitivity
Elderly brain is more sensitive to a given CNS level of a drug
Mechanism ??

Slowed Drug Metabolism:
Clearance decreases as– Liver blood flow decreases– Liver mass decreases– Kidney function decreases
Volume of distribution increases with– Increased body fat– Decreased albumin levels

Bolus Drug Strategy for the Elderly:
GO LOW !GO SLOW !You can always give more!

Temperature Regulation
Elderly prone to both hypo-, hyperthermia Lower body metabolism Decreased ability to change skin blood flow
(less able to hold or get rid of heat) Hypothermia
– Shivering increases metabolic demand Increased risk of myocardial ischemia


The Elderly Brain

CNS Structural Changes
Brain mass decreases with corresponding decreased cerebral blood flow
Decreased receptors– Acetylcholine
Cholinergic neurons in the basal forebrain regulate normal memory
– Dopamine– Norepinephrine

Postoperative Cognitive Disorders
Delirium
Mild neurocognitive disorder - POCD
Dementia (rare)– Multiple cognitive deficits – Impairment in activities of daily living

Postoperative Delirium
Most common form of perioperative CNS dysfunction Acute confusion, decreased alertness,
misperception Patient may show agitation or withdrawal Twice as common in the elderly
– 10-15% of elderly surgical patients– 30-50% if undergoing cardiac or orthopedic surgery
Seen after general, regional and MAC anesthetics Results in prolonged hospital stay and protracted
postoperative care

Postoperative Delirium:Predisposing Factors
Drug withdrawal– Use of benzodiazepines, tricyclic antidepressants– Alcohol abuse
Drug interactions– Anticholinergics, etc.
Pre-existing depression or dementia Metabolic disturbances

Can Postoperative Delirium be Prevented?
Marcantonio (2001) - Reduced postoperative delirium by 1/3 in hip fracture patients– Minimized benzodiazepines, anticholinergics,
antihistamines, meperidine– Maintained BP greater than 2/3 of baseline– Maintained O2 saturation > 90%– Maintained Hct > 30%– Mobilized patients ASAP– Provided appropriate environmental stimulation
Minimizing Postoperative Delirium:Try to Avoid:
Anticholinergics - atropine and scopolamine (NOT glycopyrrolate)
Ketamine Benzodiazepines Large doses of barbiturates and Propofol Meperidine

Common & Treatable Causes of Postoperative Delirium
Hypoxemia Hypercarbia Hypotension Pain Sepsis Metabolic

Management of Postoperative Delirium
Identify cause if possible Maintain or restore:
– Adequate oxygenation and ventilation– Normal hemodynamics– Normal metabolic state
Drugs– Benzodiazepines - if alcohol or sedative withdrawal– Haloperidol (if not contraindicated - i.e. Parkinson’s Disease)
Restraints - to prevent injury

Postoperative Cognitive Dysfunction (POCD)
Deterioration of intellectual function presenting as impaired memory or concentration.
Not detected until days or weeks after surgery Duration of several weeks to permanent Diagnosis is only warranted if:
– corroborated with neuropsychological testing and evidence of greater memory loss than one would expect due to normal aging

Implications of POCD:
Can lead to an abrupt decline in cognitive function
Ultimately– Loss of independence– Withdrawal from society– Death
Seattle Longitudinal Study of AgingBerlin Aging Study
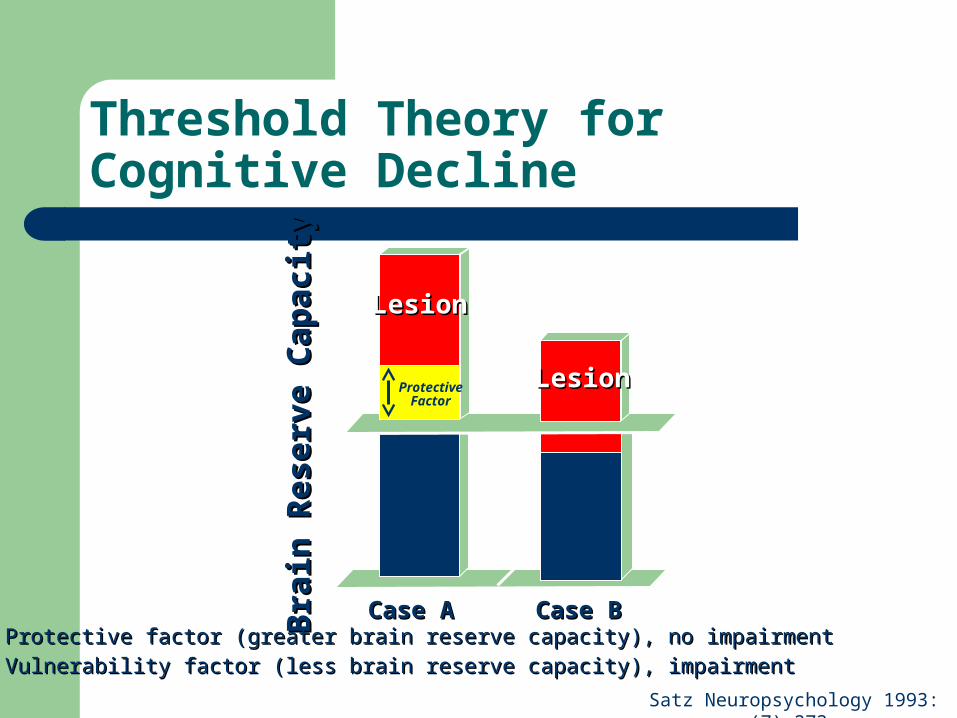
Threshold Theory for Cognitive Decline
LesionLesion
LesionLesionProtectiveFactor
Case ACase A Case BCase B
Bra
in R
eser
ve C
apac
ity
Bra
in R
eser
ve C
apac
ity
A: Protective factor (greater brain reserve capacity), no impairmentA: Protective factor (greater brain reserve capacity), no impairment
B: Vulnerability factor (less brain reserve capacity), impairmentB: Vulnerability factor (less brain reserve capacity), impairment
Satz Neuropsychology 1993:(7);273.

International Study of POCD
Long-term postoperative cognitive dysfunctionLong-term postoperative cognitive dysfunctionin the elderly: ISPOCD1 studyin the elderly: ISPOCD1 study
JT Moller P Cluitmans LS Rasmussen P Houx H Rasmussen J CanetJT Moller P Cluitmans LS Rasmussen P Houx H Rasmussen J CanetP Rabbitt J Jolles K Larsen CD Hanning O Langeron T Johnson PM LauvenP Rabbitt J Jolles K Larsen CD Hanning O Langeron T Johnson PM Lauven
PA Kristensen A Biedler H van Beem O Fraidakis, JH SilversteinPA Kristensen A Biedler H van Beem O Fraidakis, JH SilversteinJEW Beneken JS Gravenstein for the ISPOCD investigatorsJEW Beneken JS Gravenstein for the ISPOCD investigators
THE LANCET Saturday 21 March 1998Vol. 351 No. 9106 Pages 857-861
Collaborative research effort:– Members from 8 European countries and USA– 13 hospitals– Research conducted from 1994 - 1996

Incidence of POCD in Patients and Controls:Patients > 60 y.o.
Lancet 1998; 351:857Lancet 1998; 351:857
0
5
10
15
20
25
30
Pe
rce
nta
ge
(%
)
Early Late
Controls
Patients
*
10 %
* p < 0.004* p < 0.004
26 %

A Prospective Study EvaluatingThe Relationship Between Age and POCD
Single site - University of Florida: 1999 - 2002 1200 patients undergoing elective surgery
– Young - 18 to 39 years of age– Middle-aged - 40 to 59 years of age– Elderly - 60 years and older
Controls - primary family members Study design identical to ISPOCD study
– Same psychometric test battery– Outcome Endpoints:
POCD (primary) and mortality (secondary)
Monk et al. Anesthesiology 2001; 95: A-50

The Relationship Between Age and POCD:Inclusion/Exclusion Criteria
Inclusion criteria– Aged 18 years or older– General anesthesia > 2 hrs– Major abdominal/thoracic or orthopedic surgery– Mini-Mental Status Exam (MMSE) ≥ 24
Exclusion criteria– Cardiac or neurosurgical procedures– CNS disease– Alcoholism or drug dependence– Major depression– Patients not expected to live 3 months or longer
Monk et al. Anesthesiology 2001; 95: A-50
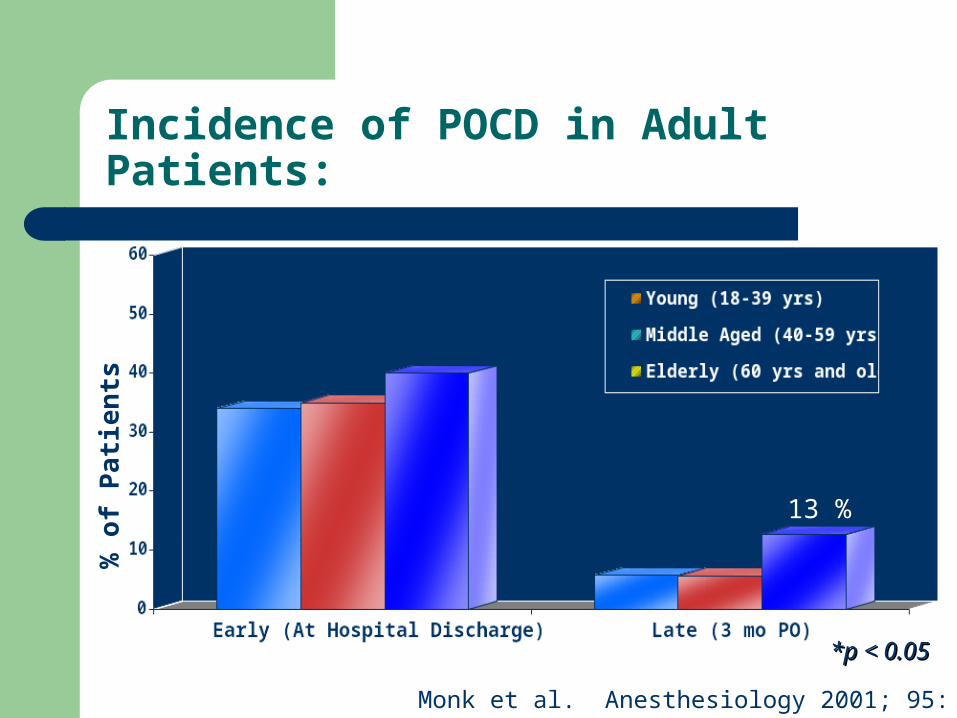
Incidence of POCD in Adult Patients:
*p < 0.05*p < 0.05
Monk et al. Anesthesiology 2001; 95: A-50
% o
f P
atie
nts
13 %

Predictors of POCD:3 Months After Surgery
NS0.046 History of MI
NS0.021 Baseline ComorbidityNS0.009 ASA Physical StatusNS0.003 History of Stroke
2.51 (p=0.057)0.001 Age0.86 (p=0.028) < 0.001 Years of Education
NS0.028 NYHA Status
NSNS Anesthesia TimeNSNS Baseline MMSENSNS GenderNSNS Surgery Type
Multivariate Odds Ratio Univariate P value Risk Factors for POCD
Multivariate c-statistic = 0.671 (p = 0.003)
Monk et al. Anesthesiology 2001; 95: A-50

One Year Mortality Rate and POCD in Elderly Patients
3.4%2.4%
6.5%
8.1%
0%
2%
4%
6%
8%
10%
Hospital Discharge Three Months
No Decline Cognitive Decline
* **
* P = 0.027 vs. No Decline; ** P = 0.014 vs. No Decline
Monk et al. Anesthesiology 2001; 95: A-50
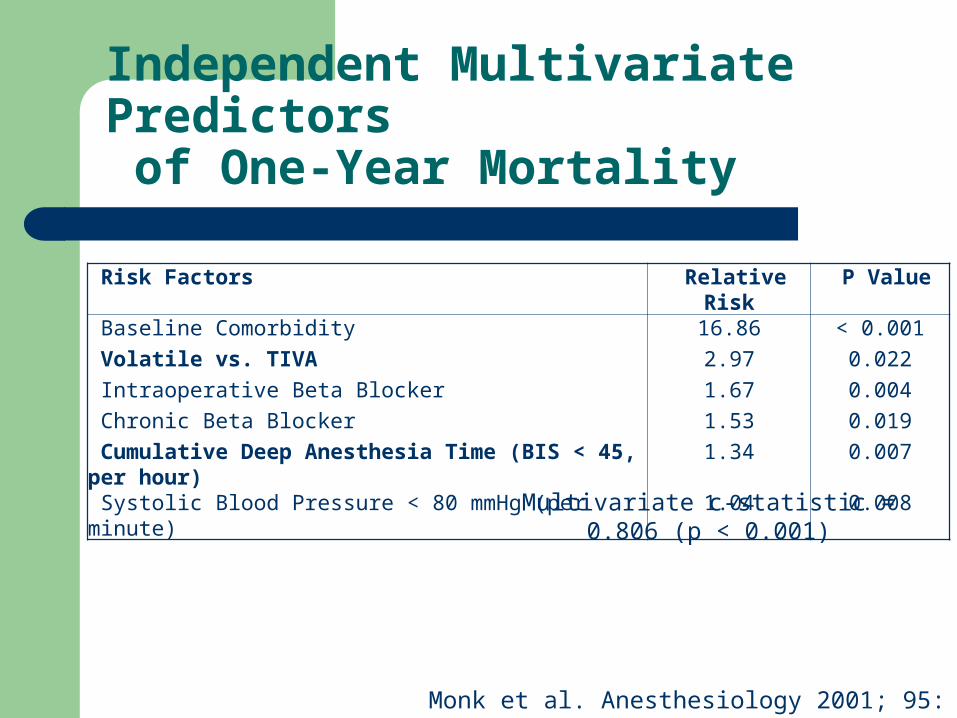
Independent Multivariate Predictors of One-Year Mortality
Risk Factors Relative Risk P Value
Baseline Comorbidity 16.86 < 0.001
Volatile vs. TIVA 2.97 0.022
Intraoperative Beta Blocker 1.67 0.004
Chronic Beta Blocker 1.53 0.019
Cumulative Deep Anesthesia Time (BIS < 45, per hour) 1.34 0.007
Systolic Blood Pressure < 80 mmHg (per minute) 1.04 0.008
Multivariate c-statistic = 0.806 (p < 0.001)
Monk et al. Anesthesiology 2001; 95: A-50

Is Mortality Data Reproducible?
Multi-center Prospective Trial (Sweden)– 5,057 General Anesthetics, Non-cardiac Surgery
Similar 1 Year Mortality Rate Deep anesthesia time is a significant
independent predictor of mortality– Increased Relative Risk: 19.7% / hr. vs. 34.1% in
Monk’s POCD/Mortality Study
Lennmarken et al, Anesthesiology 2003; 99:A-303

Laboratory Findings
Culley (2003) - Found that isoflurane-nitrous anesthesia without surgery in rats impairs spatial learning for weeks in elderly rats
Eckenhoff (2004) - Found increased toxicity of beta-amyloid in cell cultures induced by common general anesthetics

POCD: Multifactorial?
Pre-existing cognitive dysfunction Complexity and duration of surgery Micro emboli Inflammation Stress, social isolation, immobility




















