Periodontal Conditions and Mucogingival Surgical Treatment ... · derma, sistemik kollajen doku...
6
ABSTRACT ÖZET Scleroderma, which usually begins as a dermatologic disorder, is also known as a systemic collagen dise- ase. There are limited reports of dental treatment and periodontal surgical procedures for patients with scleroderma. This case report presents oral and peri- odontal changes, surgical and non-surgical periodon- tal therapy and 18-months follow-up of a 33 year-old female patient with scleroderma. The healing was uneventful after surgical therapy and stable during 1,5-year follow-up. Mucogingival surgery procedures may result successfully in patients with scleroderma, despite limited mouth opening, vascular changes and stiffness of the oral tissues. Dermatolojik bir bozukluk olarak başlayan sklero- derma, sistemik kollajen doku hastalığı olarak bilinir. Skleroderma hastalannın dental tedavileri ve peri- odontal cerrahi tedavileri hakkında çok az çalışma vardır. Bu vaka raporunda 33 yaşında bayan sklero- derma hastasındaki oral ve periodontal değişimler, cerrahi ve cerrahi olmayan periodontal tedavisi ve kli- nik takibi verilmiştir. Cerrahi tedaviden sonra iyileşme sorunsuz olmuştur ve 1,5 yıllık takibi sonunda stabil olduğu görülmüştür. Skleroderma hastalarının oral dokulardaki sertlik, damarsal değişiklikler ve sınırlı ağız açıklıklaına rağmen mukogingival cerrahi prose- dürlerin başarı ile uygulanabileceği gösterilmiştir. Hacettepe Diş Hekimliği Fakültesi Dergisi Cilt: 33, Sayı: 1, Sayfa: 41-46, 2009 Periodontal Conditions and Mucogingival Surgical Treatment of A Patient with Scleroderma Skleroderma Hastasında Periodontal Durum ve Mukogingival Cerrahi İle Tedavisi *Özlem ÖZER YÜCEL DDS, PhD, **Esra ERCAN, DDS *Private Practice **Hacettepe University Faculty of Dentistry Department of Periodontlogy KEYWORDS Skleroderma, mucogingival surgery ANAHTAR KELİMELER Skleroderma, mukogingival cerrahi OLGU RAPORU (Case Report)
Transcript of Periodontal Conditions and Mucogingival Surgical Treatment ... · derma, sistemik kollajen doku...

ABSTRACT ÖZET
Scleroderma, which usually begins as a dermatologic
disorder, is also known as a systemic collagen dise-
ase. There are limited reports of dental treatment
and periodontal surgical procedures for patients with
scleroderma. This case report presents oral and peri-
odontal changes, surgical and non-surgical periodon-
tal therapy and 18-months follow-up of a 33 year-old
female patient with scleroderma. The healing was
uneventful after surgical therapy and stable during
1,5-year follow-up. Mucogingival surgery procedures
may result successfully in patients with scleroderma,
despite limited mouth opening, vascular changes and
stiffness of the oral tissues.
Dermatolojik bir bozukluk olarak başlayan sklero-
derma, sistemik kollajen doku hastalığı olarak bilinir.
Skleroderma hastalannın dental tedavileri ve peri-
odontal cerrahi tedavileri hakkında çok az çalışma
vardır. Bu vaka raporunda 33 yaşında bayan sklero-
derma hastasındaki oral ve periodontal değişimler,
cerrahi ve cerrahi olmayan periodontal tedavisi ve kli-
nik takibi verilmiştir. Cerrahi tedaviden sonra iyileşme
sorunsuz olmuştur ve 1,5 yıllık takibi sonunda stabil
olduğu görülmüştür. Skleroderma hastalarının oral
dokulardaki sertlik, damarsal değişiklikler ve sınırlı
ağız açıklıklaına rağmen mukogingival cerrahi prose-
dürlerin başarı ile uygulanabileceği gösterilmiştir.
Hacettepe Diş Hekimliği Fakültesi DergisiCilt: 33, Sayı: 1, Sayfa: 41-46, 2009
Periodontal Conditions and Mucogingival Surgical Treatment of A Patient with
Scleroderma
Skleroderma Hastasında Periodontal Durum ve Mukogingival Cerrahi İle Tedavisi
*Özlem Özer YüCel DDS, PhD, **esra erCAn, DDS*Private Practice
**Hacettepe University Faculty of Dentistry Department of Periodontlogy
KEYWORDSSkleroderma, mucogingival surgery
ANAHTAR KELİMELERSkleroderma, mukogingival cerrahi
OLGU RAPORU (Case Report)

42
INTRODUCTION
Scleroderma, is a chronic disease of un-known etiology, is characterized by diffuse scle-rosis of the connective tissues of skin and vis-ceral organs, vasculopathy, and autoantibodies. The disease is uncommon, onset usually begins in middle age and occasionally familial, although there is no definite pattern of inheritance. Three to four times as many females are affected as males. The disease presents in a wide spectrum both systemic and localized forms1,
Approximately 80 % of the patients have manifestations in the head and neck region, with dysphagia and reflux esophagitis being in com-mon 2. Scleroderma also affects oral and perioral tissues. Oral manifestations reported in these pa-tients include fibrosis and rigidity of tongue and oral tissues, limited mouth opening, telengiecta-sis, xerostamia, increased frequency of caries and periodontal disease and increased periodontal lig-ament width1. Structural changes of the jawbone as well as widening of the periodontal ligament space have been revealed on radiographs3.
CASE REPORT
A 33-year-old female was referred to our clinic for evaluation of gingival recession in November 2005. She reported diagnosis of scleroderma in 2001. Furthermore, the patient was prescriped drugs for osteoporosis. She also prescriped de-flazacort, azathioprine, acetylsalicylic acid, nifedip-ine, famotidine and pentoxifylin. She never smoked and was brushing her teeth once two days.
She was found to have a poor dentition with caries and periodontal disease affecting all re-maining teeth. A marked xerostomia was also noted. We detected telengiectasia of face and mouse rigidity by physical examination (Fig. 1). Clinical evaluation revealed severe gingival recession depth of 10 mm. and 9 mm. with a 3-mm probing depth on the mid-buccal of the mandibular right first premolar teeth and left first premolar teeth respectively. Radiographic changes included uniform widening of the peri-odontal ligament space with an associated loss of radicular lamina dura (Fig.2 and 3). The patient
FIGURE 1
The telengiectasia of face and mouth rigidity
FIGURE 2
The panaromic radiograph of the patient
FIGURE 3
Periapical radiographs exhibiting extreme widening of the periodontal ligament space

43
complained about xerostomia. As xerostomia rampant caries were widely observed especially in the anterior teeth (Fig.4.), we prescribed Bio-tene® oral care set. After motivating for oral hy-giene, the patient was referred to Department of Conservative Dentistry for fillings.
After consultation with the patient’s doctor, the patient was prescribed Amoxiciline 1 gr. tablet before surgical treatments for bacteriamia risk. Initial therapy consisted of oral hygene instructions, scaling and root planing by quad-rants, and re-evalution. The periodontal pockets responded well to scaling and root planing and improved oral hygiene required no further treat-ment. The areas of gingival recession exhibited root surface sensitivity, and narrow zones of at-tached gingiva. A decision to treat the areas of recession with mucogingival surgery was made after careful consideration (Figs. 5 and 6).
Local anesthesia was obtained with 2% lido-caine 1:100,000 epinephrine. Teeth #34 and #45 were treated with free gingival grafts ob-tained from palate using the modified technique described by Langer and Langer (Figs.7 and 8.). The grafts were sutured with 5.0 silk sutures. Sur-gical dressing were placed at the recipient sites. The sutures were removed 10 days after surgery.The patient was prescribed 0.12% clorhexidine mouthwash two times a day for 2 weeks. The pa-tient was prescriped systemic analgesic (naprox-en sodium) 1 tablet every 6 hours if needed for pain and an antibiotic (amoxicilin) for 7 days. The postoperative course was uneventful. Follow-up controls were made at 6 months, 1 year and 18 months postoperatively. Six months postopera-tive healing is demonstrated in Figures 9 and 10. After the periodontal treatment was completed, the patient was referred to Department of Prosth-odontics for removable partial dentures.
Clinical measurements, including plaque in-dex, gingival index, recession depth, probing depth, clinical attachment level and bleeding on probing were recorded before surgery and at 6 months, 1 year, 18 months postoperatively. Mea-surements of recession depth, probing depth, and clinical attachment level were made at the mid-labial aspect of the teeth
FIGURE 5
Before surgery (lower left first premolar teeth)
FIGURE 6
Before surgery (lower right first premolar teeth)
FIGURE 4
The rampant caries because of xerostomia

44
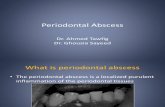
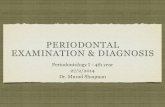
(Table 1 and 2). The probing depth was reduced 3 mm. to 1 mm. for both teeth from baseline to 6 months. Also gingival index and plaque index values reduced at 12 months and 18 months according to baseline. Furthermore, the patient could provide brushing in these re-gions more effectively.
DISCUSSION
The most common problem with dental treat-ment of scleroderma patients is the physical one caused by the narrowing of the oral opening and the rigidity of the tongue4. Patients with sclero-derma often show up with caries and moderate-to-advanced periodontal disease due to poor oral hygiene and patient susceptibility 5. Oral hygiene measures and dental treatment become more dif-ficult as the severity of the soft tissue involvement increases 1,6,7.
Radiographic changes have been classically described as a uniform widening of the peri-odontal ligament space with an associated loss of radicular lamina dura 3,8. White et al. found 37% of the patients heve abnormally thickened peri-odontal ligament spaces 9. In a controlled study, Wood et al. reported 29% of the patients with systemic sclerosis had resorptive lesions (ero-sions) of the mandible involving the mandibular angle, the digastric region, the condylar head, and the coronoid process 10. In our patient, no resorptive lesions of the condyl and coronoid
FIGURE 7
During surgery (lower left first premolar teeth)
FIGURE 8
During surgery (lower right first premolar teeth)
FIGURE 9
6 months after surgery for lower left first premolar teeth
FIGURE 10
6 months after surgery for lower right first premolar teeth
45
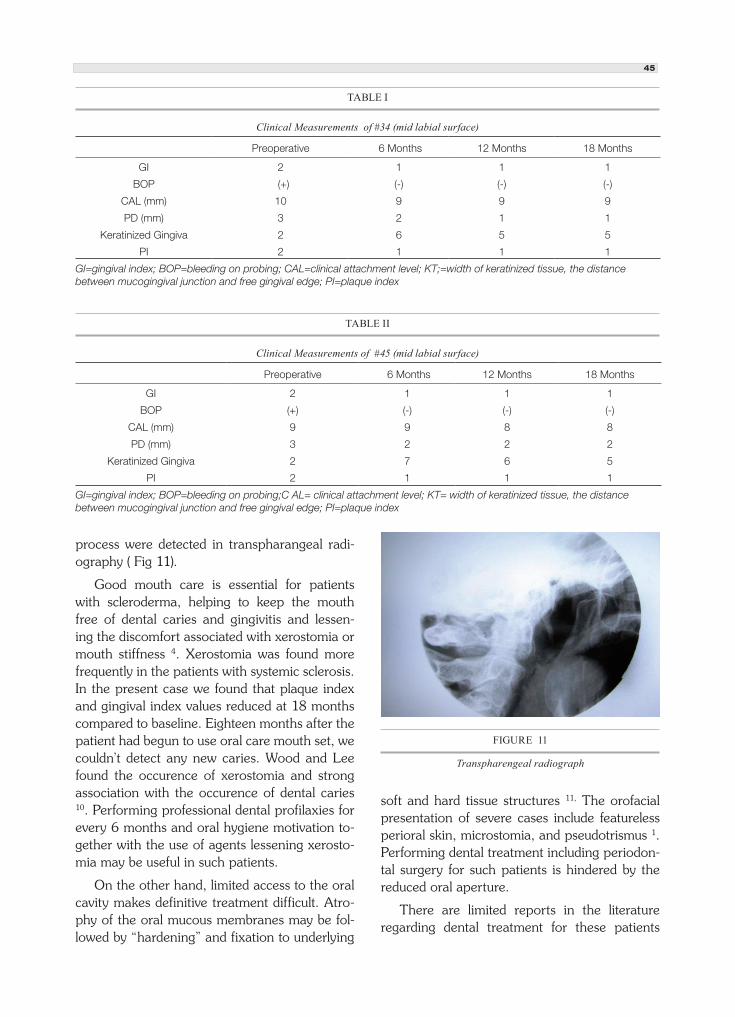
process were detected in transpharangeal radi-ography ( Fig 11).
Good mouth care is essential for patients with scleroderma, helping to keep the mouth free of dental caries and gingivitis and lessen-ing the discomfort associated with xerostomia or mouth stiffness 4. Xerostomia was found more frequently in the patients with systemic sclerosis. In the present case we found that plaque index and gingival index values reduced at 18 months compared to baseline. Eighteen months after the patient had begun to use oral care mouth set, we couldn’t detect any new caries. Wood and Lee found the occurence of xerostomia and strong association with the occurence of dental caries 10. Performing professional dental profilaxies for every 6 months and oral hygiene motivation to-gether with the use of agents lessening xerosto-mia may be useful in such patients.
On the other hand, limited access to the oral cavity makes definitive treatment difficult. Atro-phy of the oral mucous membranes may be fol-lowed by “hardening” and fixation to underlying
soft and hard tissue structures 11, The orofacial presentation of severe cases include featureless perioral skin, microstomia, and pseudotrismus 1. Performing dental treatment including periodon-tal surgery for such patients is hindered by the reduced oral aperture.
There are limited reports in the literature regarding dental treatment for these patients
TABLE II
Clinical Measurements of #45 (mid labial surface)
Preoperative 6 Months 12 Months 18 Months
GI 2 1 1 1
BOP (+) (-) (-) (-)
CAL (mm) 9 9 8 8
PD (mm) 3 2 2 2
Keratinized Gingiva 2 7 6 5
PI 2 1 1 1
GI=gingival index; BOP=bleeding on probing;C AL= clinical attachment level; KT= width of keratinized tissue, the distance between mucogingival junction and free gingival edge; PI=plaque index
TABLE I
Clinical Measurements of #34 (mid labial surface)
Preoperative 6 Months 12 Months 18 Months
GI 2 1 1 1
BOP (+) (-) (-) (-)
CAL (mm) 10 9 9 9
PD (mm) 3 2 1 1
Keratinized Gingiva 2 6 5 5
PI 2 1 1 1
GI=gingival index; BOP=bleeding on probing; CAL=clinical attachment level; KT;=width of keratinized tissue, the distance between mucogingival junction and free gingival edge; PI=plaque index
FIGURE 11
Transpharengeal radiograph

46
CORRESPONDING ADRESS
Esra Ercan DDSHacettepe University Faculty of Dentistry Department of Periodontology, Ankara, Turkey
Phone: +903123052219 (business) Fax: +903123104440 e-mail: [email protected]
Geliş Tarihi : 10.02.2009 Received Date : 10 February 2009 Kabul Tarihi : 15.05.2009 Accepted Date : 15 May 2009
and only one report of periodontal surgical pro-cedures 1. That paper presents a case report of periodontal surgical treatment in a 38-year-old female patient with systemic scleroderma. Stan-ford et al. treated the teeth with localized gingi-val recession with subepithelial connective tissue grafts and free gingival grafts from palatal donor site using a modification of the technique first described by Björn. They reported that healing was uneventful demonstrating two years follow-up in accordance with the present case 1. The only limitation of the report is the lack of pre-op and post-op periodontal measurements.
Creeping attachment, which was described by Goldman and Cohen, is known as the postop-erative migration of the gingival margin tissue in a coronal direction over portions of a previously denuded root 12. This phenomen can be detected 1 to 12 months after graft surgery with an aver-age coverage of ~1 mm 13. In the present case, the creeping attacment occured after 6 months and and probing depth reduced 3 to 1 mm. after 12 months. The creeping attachment became stable 12 months after the surgery.
The oral circumference may be reduced by up to 30%, making even the insertion of den-tures difficult. Correction of microstomia has been attempted using exercises and appliances but with significant relapse 14. Another solution to the problem of denture wearing is the use of osseointegrated dental implants. In the present case bilateral sinus lifting procedure was required for dental implant treatment, which was so diffi-cult to perform due to microstomia. The preven-tion of tooth loss in such patients with regular periodontal treatment, including mucogingival surgery is of great importance because of the diffuculties in wearing dentures.
The periodontal surgical procedure includ-ing free gingival grafts, achieved in this patient
with scleroderma and the treatment outcomes were stable for 1,5-year follow-up despite some limitations. These limitations are xerostomia, microstomia, and atrophy of the oral mucous membranes, which make definitive periodontal surgical treatment difficult.
REFERENCES
1. Stanford TW, Peterson J, Machen RL. CREST Syndrome and periodontal surgery: a case report. J Periodontol. 1999; 70(5): 536-41
2. Prime SS, Pring M, Davies M, Patrson IC. TGF-β Signal transduction in oro-facial health and non-malignant disease (Part-I). Crit Rev Oral Biol Med. 2004;15(6):324-36
3. Marmary Y, Glaiss R, Pisanty S. Scleroderma: Oral manifestations. Oral Surgery. 1981; 52(1): 32-3
4. Suzuki Y, Abe M, Hosoi T, Kurtz KS. Sectional collapsed denture for a partially edentulous patient with microstomia: a clinical report. J Prosthet Dent. 2000;84:256-9
5. Yenisey M, Külünk T, Kurt Ş, Ural Ç. A prosthodontic management alternative for scleroderma patients. J Oral Rehabilitation. 2005;32:696-700
6. Spackman GK. Scleroderma: what the general dentist should know. Gen Dent. 1999; 47(6): 576-9
7. Ashok L, Rao BB, Chandraskear HR. Progressive systemic sclerosis: a case report. Indian J Dent Res. 1997; 8(3):78-81
8. Auluck A, Pai KM, Shetty C, Shenoi SD. Mandibular resorption in progressive systemic sclerosis: a report of three cases. Dentomaxillofacial Radiol. 2005; 34(6):384-6
9. White SC, Frey NW, Blaschke DD, Ross MD, Clements PJ, Fust DE, Paulus HE. Oral radiographic changes in patients with progressive systemic sclerosis (scleroderma). J AM Dent Assoc. 1997; 94(6):1178-82
10. Wood RE, Lee P. Analysis of the oral manifestations of systemic sclerosis (scleroderma). Oral Surg.1988; 65 (2):172-8
11. Nagy G, Kovacs J, Zeher M, Czirjak L. Analysis of the oral manifestations of systemic sclerosis. Oral Surgery Oral Medicine Oral Pathology. 1994; 77(2):141-6
12. Goldman HM, Cohen DW. Periodontal Therapy, 5th ed. St. Louis:C.V. Mosby; 1973:715-58.
13. Matter J, Creeping attachment of free gingival grafts. A five year follow-up study. J Periodontol 1980;51:681-85.
14. Paley M, McLoughlin. Oral problems associated with CREST syndrome: a case report. British Dental Journal. 1993; 23: 295-6