Periodic Re-Evaluation in the Case Management Process · 2017-06-01 · Periodic Re-Evaluation in...
8
6/1/2017 1 Periodic Re-Evaluation in the Case Management Process Presented by: Kathy Mills Chang, MCS-P, CCPC, CCCA Goals of this Presentation • Deliver appropriate evaluation and management services along the way to justify continued care, assess progress, and discharge from this active care when the time is right • Report the mechanics of moving a patient through the phases of care necessary to bring the patient to maximum clinical improvement • Report the necessary components of documenting the transitional diagnosis and treatment plan after a periodic re- evaluation • Complete the fundamentals of documenting the assessment of change since the last evaluation as it applies to federal regulations in Medicare Why Re-evaluate? The reasons we reevaluate: – To assess progress – To improve patient care – To meet legal/3 rd party payer requirements – To get paid – To educate the patient Why Re-evaluate? To Assess Progress: – Changes in condition(s) New injury, decreased or increased symptoms, new co- morbidities… – Effectiveness of Tx Did the treatment so far help? How much? – What is needed to meet therapeutic goals? Does the patient need more care? Why? How much more? Why Re-evaluate? To Improve Patient Care: – A patient is more than their diagnosis… they want to see progress from symptoms – By seeing where they are in their healing, we can effectively change treatment to meet their needs – Sets clinical, professional, and financial boundaries to care provided Why Re-evaluate? To Meet Legal/3 rd Party Requirements: – There are legal and carrier guidelines that REQUIRE re-evaluations To Get Paid: – If you don’t follow their rules… they will not pay you! – Proof that the patient NEEDED the care or still NEEDS the care
Transcript of Periodic Re-Evaluation in the Case Management Process · 2017-06-01 · Periodic Re-Evaluation in...

6/1/2017
1
Periodic Re-Evaluation in the Case Management Process
Presented by:
Kathy Mills Chang, MCS-P, CCPC, CCCA
Goals of this Presentation• Deliver appropriate evaluation and
management services along the way to justify continued care, assess progress, and discharge from this active care when the time is right
• Report the mechanics of moving a patient through the phases of care necessary to bring the patient to maximum clinical improvement
• Report the necessary components of documenting the transitional diagnosis and treatment plan after a periodic re-evaluation
• Complete the fundamentals of documenting the assessment of change since the last evaluation as it applies to federal regulations in Medicare
Why Re-evaluate?
The reasons we reevaluate:
– To assess progress
– To improve patient care
– To meet legal/3rd party payer requirements
– To get paid
– To educate the patient
Why Re-evaluate?
To Assess Progress: – Changes in condition(s)
New injury, decreased or increased symptoms, new co-morbidities…
– Effectiveness of Tx
Did the treatment so far help? How much?
– What is needed to meet therapeutic goals?
Does the patient need more care? Why? How much more?
Why Re-evaluate?
To Improve Patient Care:– A patient is more than
their diagnosis… they want to see progress from symptoms
– By seeing where they are in their healing, we can effectively change treatment to meet their needs
– Sets clinical, professional, and financial boundaries to care provided
Why Re-evaluate?
To Meet Legal/3rd Party Requirements:
– There are legal and carrier guidelines that REQUIRE re-evaluations
To Get Paid:– If you don’t follow their
rules… they will not pay you!
– Proof that the patient NEEDED the care or still NEEDS the care

6/1/2017
2
Why Re-evaluate?
• To Educate the Patient:
– While secondary to documentation, equally important
– A follow-up report of findings is as important as the initial
– Patients want to know what is going on, how they’re doing
– Use as an opportunity
Choices, Choices, Choices
Various Re-evaluations
• Periodic re-evaluation to determine if further care is necessary
• New condition, new injury, new accident
• Evaluations for considering discharge
• Non-treatment related E/M services
Per the American Chiropractic Association"The physician work component of the CMT codes includes a brief pre-manipulation patient assessment. Additional evaluation and management services may be reported separately using the modifier -25 if, and only if, the patient's condition requires a significant separately identifiable E/M service, above and beyond the usual pre-service and post-service work associated with the procedure. The E/M service may be prompted by the symptom or condition for which the procedure and/or service was provided. (On any given visit, if the patient presents more than one specific area of complaint that necessitates separate and distinct clinical evaluations, evaluation/management service codes (E/M) should be the service that most accurately reflects the cumulative level of all services provided during the visit.) As such different diagnoses are not requiredfor the reporting of the E/M service on the same day."
Most Full Episodes Include Re-Evaluation
• Episodes are easy!
• There is a clear delineation of:
– The beginning
– The middle
– And the end of care
• They are Black & White
The 30-Day RuleIf a patient exhibits no change in the outcome assessment data for a maximum period of three consecutive re-examinations or 60 days, the patient should be considered for a clinical change in treatment. Considerations for changes in treatment may include the following:
• Modifying treatment approach
• Co-treat with an allied health provider
• Referral for a second opinion
• Determine that the patient has reached maximum improvement
• The clinical decision as to which, change in treatment, path should be followed is dependent on the individual practitioner‘s profession integration of outcome assessment data

6/1/2017
3
Components of a Periodic Re-EvaluationThe re-exam should be scheduled on a specific date in the treatment plan. At the re-exam you should:
• Update the history; consider getting hand-written update from pt.
• Re-examine all positives and significant negatives from the initial examination
• Patient completes new Outcome Assessment Questionnaires; score them and compare scores with original
• Assess the effectiveness of the previous course of treatments, in your assessment portion of the note
• Modify the diagnoses if appropriate and update a new treatment plan, if needed
Components of Other Re-Evaluations
• Are they really re-evals?
• Not really!
• Anything “new” is a new condition/episode
• Must mirror components of initial evaluation
• It’s a “re” only because you know the patient
E&M Coding/Documentation is Based on 7 Components
• 3 Key Components
– Patient History
– Examination
– Clinical Decision Making
• 3 Contributory Components– Counseling
– Coordination of Care
– Nature of Presenting Problem
• 1 Additional Component– Time
The Most “Missed” Component?
• You must update the history
• It’s a component of E/M
• If you don’t have the patient fill something out, do it verbally and document it
• EHR systems allow for this

6/1/2017
4
Our Gift to You!
Deliver appropriate evaluation and management services along the way to justify continued care, assess progress,
and discharge from this active care when the time is right
Re-evaluation Guidelines
– CCGPP stance• According to CCGPP (Council on Chiropractic Guidelines and
Practice Parameters, re-evaluations to determine your patient’s progress are required every 30 days.
30-Day Window to ‘Plan B’
A Recent IME and Audit
Projected Completion of Tmt Plan: _________
Functional Treatment Goal: By _________(when)

6/1/2017
5
Phases of Care are Clearly Documented
Report the mechanics of moving a patient through the phases of care necessary to bring the patient to maximum clinical improvement
Transitional DX
• Change of diagnosis to fit the patient’s current state
– If no longer right sciatica with LBP reduce the severity to what it is now
When to Release from Care
CCGPP
Arrive at Final Plateau (maximum therapeutic benefit)
• Complete or partial resolution of the condition and all reasonable treatment and diagnostic studies have been provided
• Patient is unlikely to improve further
Patient Not Ready for Release
Plan for the patient to be released:
• Set new treatment goals
• Write new treatment plan
Write down assessment of why you are not releasing
I, Dr. Awesome, believe the patient has not met maximum medical improvement because……..
Proper patient release is like ordering a stake. Some people like rare, some like well done. If you ordered well done don’t settle for rare. Send it back to the kitchen for more “treatment” with more explicit instructions
Therapeutic Withdrawal
• Strategically weening the patient off of medically necessary care to determine if they can maintain the therapeutic goals of treatment
• Final step before patient can begin maintenance care
Like a game of Jenga… Making sure the pieces you moved are where you want them before removing your hands
Therapeutic Withdrawal
• CCGPP - A trial withdrawal may be necessary once a patient reaches maximum therapeutic improvement.
– This helps to determine if the condition recovery is stable
– If the condition has deteriorated after the trial, then chronic or ongoing care may be necessary to maintain function and minimize symptoms.

6/1/2017
6
Therapeutic Withdrawal? Therapeutic Withdrawal
Maintenance
The patient is MAINTAINING THE CURRENT STATE and not expected to improve. On going treatment
Therapeutic Withdrawal
the doctor is not 100% that the patient will not relapse if MN care is discontinued.TESTING IF IT CAN BE MAINTAINED. Short term trial
Therapeutic Withdrawal
CCGPP
• Therapeutic withdrawal (TW) is included as proper case management
• Without TW
– There is no way to determine the stability of the spine
– Determine if a patient require on going care
Therapeutic Withdrawal• The Mercy Guidelines
“Periodic trials of therapeutic withdrawal fail to sustain previous therapeutic gains that would otherwise progressively deteriorate.
• Utilization review standpoint– The proof that a patient cannot
sustain therapeutic gains can only be demonstrated through periodic withdrawals from care, along with detailed documentation which clearly supports a subsequent regression in patient status
3rd Party Payer’s View of TW
BCBS of TN
Types of Therapeutic Withdrawal
• Gradual Withdrawal
– Where the patient’s care is tapered off
• Abrupt Withdrawal
– Patient instructed to return if the symptoms recur
– Patient is scheduled for an evaluation at a later date to determine if there is any regression
– Tends to be the typical MD approach
Times a Week # of Weeks
3 2
2 2
1 2
1 every other week 4
Total = 14 visits
6/1/2017
7
Examples
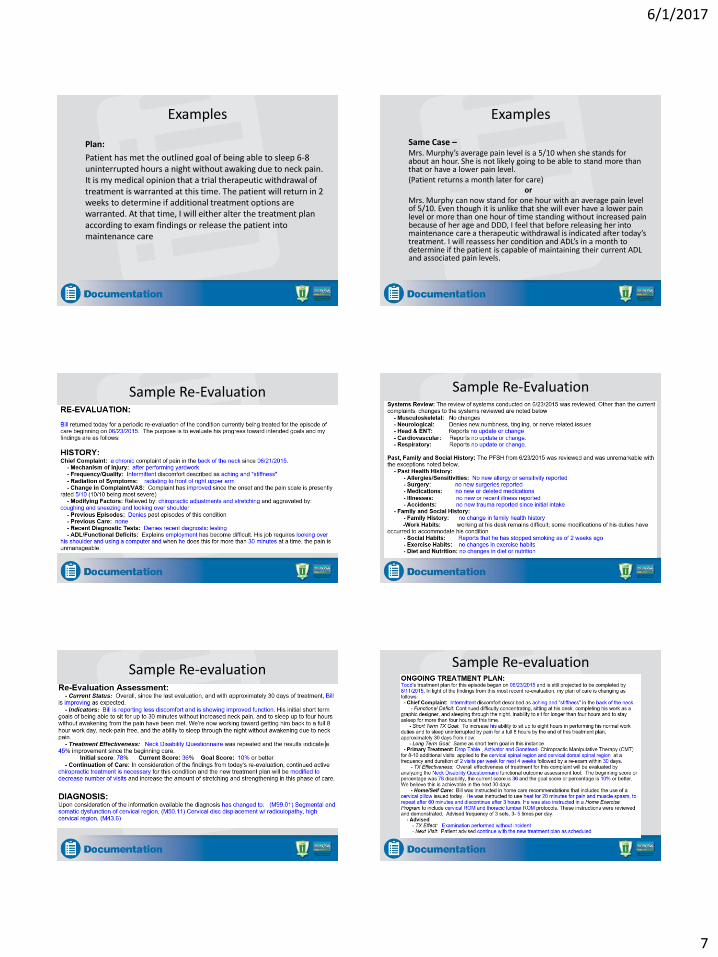
Plan:
Patient has met the outlined goal of being able to sleep 6-8 uninterrupted hours a night without awaking due to neck pain. It is my medical opinion that a trial therapeutic withdrawal of treatment is warranted at this time. The patient will return in 2 weeks to determine if additional treatment options are warranted. At that time, I will either alter the treatment plan according to exam findings or release the patient into maintenance care
Examples
Same Case –Mrs. Murphy’s average pain level is a 5/10 when she stands for about an hour. She is not likely going to be able to stand more than that or have a lower pain level. (Patient returns a month later for care)
orMrs. Murphy can now stand for one hour with an average pain level of 5/10. Even though it is unlike that she will ever have a lower pain level or more than one hour of time standing without increased pain because of her age and DDD, I feel that before releasing her into maintenance care a therapeutic withdrawal is indicated after today’s treatment. I will reassess her condition and ADL’s in a month to determine if the patient is capable of maintaining their current ADL and associated pain levels.
Sample Re-Evaluation Sample Re-Evaluation
Sample Re-evaluation Sample Re-evaluation

6/1/2017
8
What if You Don’t Get Paid?
• Carriers may have “policy” that re-evalsare not covered
• One E/M per year may be what you signed up for
• None of this dismisses your obligation to re-evaluate
Need [email protected]