
PERINATAL PSYCHIATRY Dr N U Mir Consultant in Perinatal Psychiatry Hon Senior Clinical Lecturer...
46
PERINATAL PSYCHIATRY Dr N U Mir Consultant in Perinatal Psychiatry Hon Senior Clinical Lecturer Perinatal Mental Health Service Michael Carlisle Centre Sheffield
-
Upload
peregrine-stone -
Category
Documents
-
view
237 -
download
1
Transcript of PERINATAL PSYCHIATRY Dr N U Mir Consultant in Perinatal Psychiatry Hon Senior Clinical Lecturer...

PERINATAL PSYCHIATRY
Dr N U MirConsultant in Perinatal PsychiatryHon Senior Clinical LecturerPerinatal Mental Health ServiceMichael Carlisle CentreSheffield
KEY TOPICS
History and role of perinatal psychiatry
Clinical presentation of common perinatal psychiatric disorders
Baby blues
Antenatal and postnatal depression
Postpartum (puerperal) psychosis
Prescribing in pregnancy and breastfeeding
HISTORY
Louis Victor Marcé
Paris
1828-1864
‘Traité de la Folie des femmes enceintes, des nouvelles accouchées et des nourrices’
NEED FOR PERINATAL PSYCHIATRY
Depression leading cause of world wide disability WHO Global burden of disease study
Suicide third leading cause of indirect maternal death CEMACE: Saving Mothers’ lives 2006 - 2008
Untreated perinatal disorders => morbidity / bonding / risk Pre-existing psychiatric disorders => increased relapse risk Bipolar disorder => Puerperal psychosis risk
Confidential Enquiry into Maternal Deaths in UK, Saving Mothers’ Lives 2006 – 2008, RCOG 2011
Lopez et al. Global and regional burden of disease and risk factors, 2001:systematic analysis of populationHealth data. Lancet 2006 367:1747-57

MEDIA SPOTLIGHT
ROLE OF PERINATAL PSYCHIATRY
Managing high risk women with previous postnatal episodes or complex circumstances
Treating antenatal moderate / severe anxiety and mood disorders
Managing pre-existing psychoses (eg. Bipolar disorder) during pregnancy
Pre-conceptual counselling
Advising on risks of medication during pregnancy and breastfeeding
CLINICAL PRESENTATION -IN CONTEXT-
ANTENATAL
Depression Generalised anxiety Panic disorder Pre-existing psychoses
(eg. Schizophrenia,
Bipolar disorder)
POSTNATAL
Baby blues Depression Postpartum (Puerperal)
psychosis
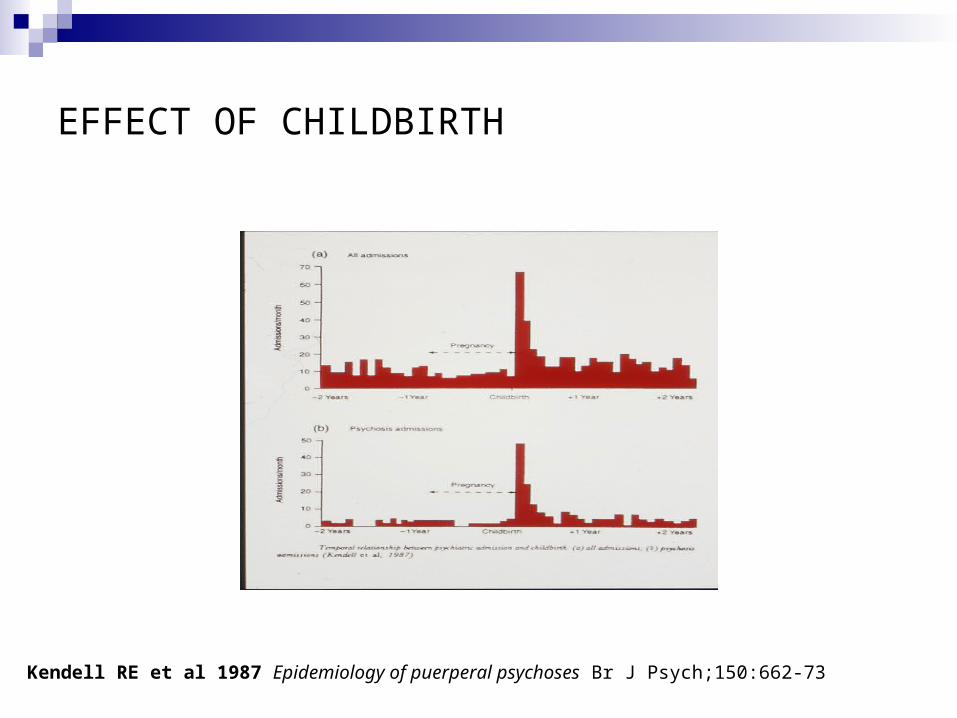
EFFECT OF CHILDBIRTH
Kendell RE et al 1987 Epidemiology of puerperal psychoses Br J Psych;150:662-73
NOSOLOGY
Wide variety of disorders occur in relation to parturition
Psychiatric illness may be precipitated by pregnancy and childbirth
New onsets or recurrence
Pregnancy can influence pre-existing psychiatric illness
Psychiatric disorders can influence obstetric course
ANTENATAL DEPRESSION
Estimated rates vary: 7-15% developed countries / 19-25% in developing countries
Poverty, lack of education, young age, poor social support, unplanned pregnancy associated with antenatal depression
50% postnatal depression starts during pregnancy
2/3 women with recurrent depression will relapse if discontinue antidepressants after conception
Association with low birth weight and IUGR, preterm delivery
Chung et al. 2001. Antepartum depressive symptomatology is associated with adverse obstetric and neonatal outcomes. Psychosom Med 63:830-4
CLINICAL PRESENTATION
Negativity towards pregnancy
Thoughts re termination of pregnancy
Worry about course and outcome of pregnancy - will I have a miscarriage? - will baby be healthy? - I won’t be able to cope with labour - I will be a bad mother
Ideas and acts of self harm
Relationship difficulties

TREATMENT OF ANTENATAL DEPRESSION
Treatment dependent on severity
Mild depression – psychological interventions counselling, CBT
Moderate depression – Risk benefit analysis - Antidepressant therapy (NICE) - CBT
Severe depression – Antidepressant therapy (NICE) CBT CMHT / Perinatal service follow up
PSYCHOSIS DURING PREGNANCY
Early referral to Perinatal Mental Health Service Regular community follow up by Perinatal Mental Health Service Maintenance antipsychotic therapy for high risk patients Schizophrenia, schizoaffective disorder, bipolar disorder with history
of relapse, residual symptoms or previous postnatal episodes Consider change to trifluoperazine Care coordinator CPA Planning meeting pre-childbirth Liaison with Children & Families / Social Services
POSTNATAL DISORDERS
Baby Blues
Postnatal Depression
Postpartum (Puerperal)Psychosis
BABY BLUES
Incidence per delivery: ~ 50%
Typical onset after delivery: Around 2 – 5 days
Symptoms: Depressed mood, irritability, lability of mood, crying
Prognosis: Transient. Increased risk of subsequent postnatal
depression
Treatment: Requires no intervention. Self limiting.
POSTNATAL DEPRESSION
Incidence per delivery: 10 – 15%
Typical onset: Within 6 months of delivery
Distinct from non-postpartum depression?
Little evidence to support distinction
Lack of consistent data on hormonal aetiology
DEPRESSIVE EPISODE (ICD-10 F32)
Group A symptoms Depressed mood, loss of interest and enjoyment, decreased energy
Group B symptoms a) reduced concentration and attention b) reduced self-esteem and self-confidence c) ideas of guilt and worthlessness d) bleak and pessimistic outlook e) ideas of self harm and suicide f) disturbed sleep g) diminished appetite
Four, six or eight symptoms required for TWO weeks Mild, Moderate, severe
RISK FACTORS FOR POSTNATAL DEPRESSION
Antenatal depression or anxiety
Past history of depression
Past history other psychiatric illness
Recent stressful life events
Poor social support
Musters et al. 2008. Management of postnatal depression. BMJ, 37, 399 - 403
CLINICAL PRESENTATION
Persistent low mood and tearfulness Low confidence / self esteem (‘bad mother’) Difficulty coping with childcare Difficulty bonding Extreme anxiety about health of baby Overconcern about feeding / sleeping regime Odd / overvalued ideas - eg. ‘Cord still attached to baby’ ‘Baby’s eyes are eyes of the devil’ Physical anxiety symptoms / panic attacks Suicidal thoughts Infanticidal thoughts Relationship difficulties / conflict
ASSESSMENT OF RISK
History
- Feelings of worthlessness, hopelessness- History of attempted suicide or harm to baby- Situational or environmental factors affecting risk
- Mental state
- Thoughts of suicide or harm to baby- Psychotic symptoms, delusions / hallucinations re baby
SCREENING – THE WHOOLEY QUESTIONS
Recommended by NICE
If the answer to either of first two questions is positive, proceed to third question
During the past month have you often been bothered by feeling down, depressed or hopeless?
During the past month have you often been bothered by having little interest or pleasure in doing things?
Is this something you feel you need or want help with?
Whooley et al. 1997. Case-finding instruments for depression: two questions are as good as many. J Gen Intern Med, 12:439-45
EDINBURGH POSTNATAL DEPRESSION SCALE
Developed for diagnosis of Postnatal depression
Simple self-rating 10 item scale
Effective screening tool
0-3 scoring
13 and above => Depressive illness likely
Cox et al. 1987. Detection of postnatal depression: development of the 10-item Edinburgh PostnatalDepression Scale. Br J Psychiatry 150: 782-786
TREATMENT OF POSTNATAL DEPRESSION (I)
MILD to MODERATE DEPRESSION
Self help strategies Non-directive counselling Brief Cognitive behaviour therapy Interpersonal therapy Support groups / organisations eg. Surestart
TREATMENT OF POSTNATAL DEPRESSION (II)
MODERATE DEPRESSION
Psychological therapy Antidepressant therapy* - if psychological therapy declined - if psychological therapy ineffective / partial response - if history of severe depression - requested by patient
*Consider breastfeeding issue
TREATMENT OF POSTNATAL DEPRESSION (III)
MODERATE to SEVERE
Combination therapy Psychological + Pharmacological Referral to Secondary care / Specialist Perinatal service CMHT follow up – CC Clinical psychology / Psychotherapy Inpatient care – Mother – Baby Unit - if risk issues - if community care ineffective - ECT

POSTPARTUM (PUERPERAL) PSYCHOSIS
Incidence: 1-2 / 1000 deliveries
Typical onset: Acute within 2-4 weeks of delivery
Mean age of onset: 26.3 yr
Risk factors: Past history of PP Family history of PP History of Bipolar disorder
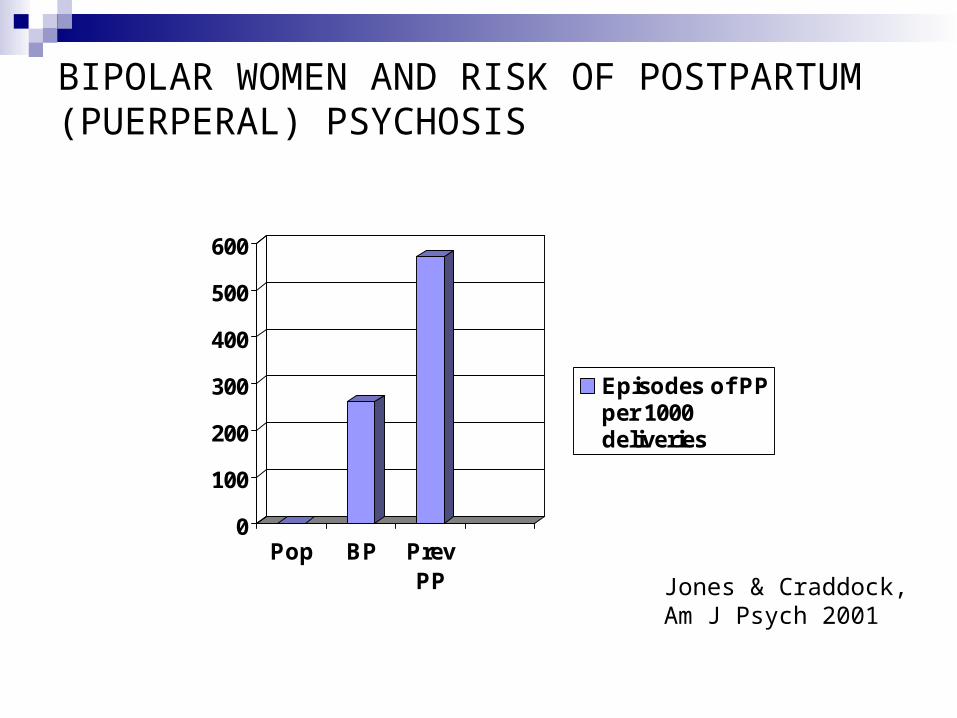
BIPOLAR WOMEN AND RISK OF POSTPARTUM (PUERPERAL) PSYCHOSIS
0
100
200
300
400
500
600
Pop BP PrevPP
Episodes of PPper 1000deliveries
Jones & Craddock,Am J Psych 2001
TYPES of PSYCHOSIS IN RELATION TO CHILDBIRTH
Chronic - Schizophrenia
Acute - Organic psychoses (becoming rarer) - Schizophrenia (rare) - Affective – manic / depressed / mixed / schizoaffective “Puerperal Psychosis”
CLINICAL FEATURES
ICD 10 F53.1
Severe mental and behavioural disorder associated with puerperium, not elsewhere classified
‘Kaleidoscopic’
Quickly changing from one thing to another
CLINICAL FEATURES
Mood symptoms - Depressed mood, lability, elation, rambling speech, overactivity
Psychotic symptoms - Delusions – fleeting not fixed, systemetisation not usual - re baby, mood incongruent, persecutory, reference, jealous, grandiose - Hallucinations – Auditory, visual, olfactory
Perplexity and confusion
Sit et al. 2006. A review of postpartum psychosis. J Women’s Health, 15, 4: 352-68
SUICIDE AND INFANTICIDE
CEMACH: Saving Mothers Lives 2003 – 2005 - Suicide second leading cause of indirect deaths
1000 women with PP => 2 suicides
More likely to be violent means eg. Hanging, self incineration, jumping from height
More likely to express homicidal ideation though homicidal behaviour rare
Confidential enquiry into Maternal deaths, Saving Mothers Lives 2003 – 2005, RCOG 2007
Sit et al. 2006. A review of postpartum psychosis. J Women’s Health, 15, 4: 352-68

TREATMENT OF POSTPARTUM (PUERPERAL) PSYCHOSIS
1) Inpatient (M-B) Unit admission – under MHA if necessary
2) Symptom focussed pharmacotherapy - Atypical antipsychotic - Antidepressant 3) Lithium - bottle feeding v breast feeding - Regular level checks – neonatal toxicity risk - Prophylaxis if past history of PP
4) - Valproate, Carbamazepine, Lamotrigine
TREATMENT OF POSTPARTUM (PUERPERAL) PSYCHOSIS
5) ECT - Deteriorating self care - Suicidality - physical risk
6) Maintenance pharmacotherapy / follow up
7) Consider past treatment response / side effects profile / acuity of illness as guide
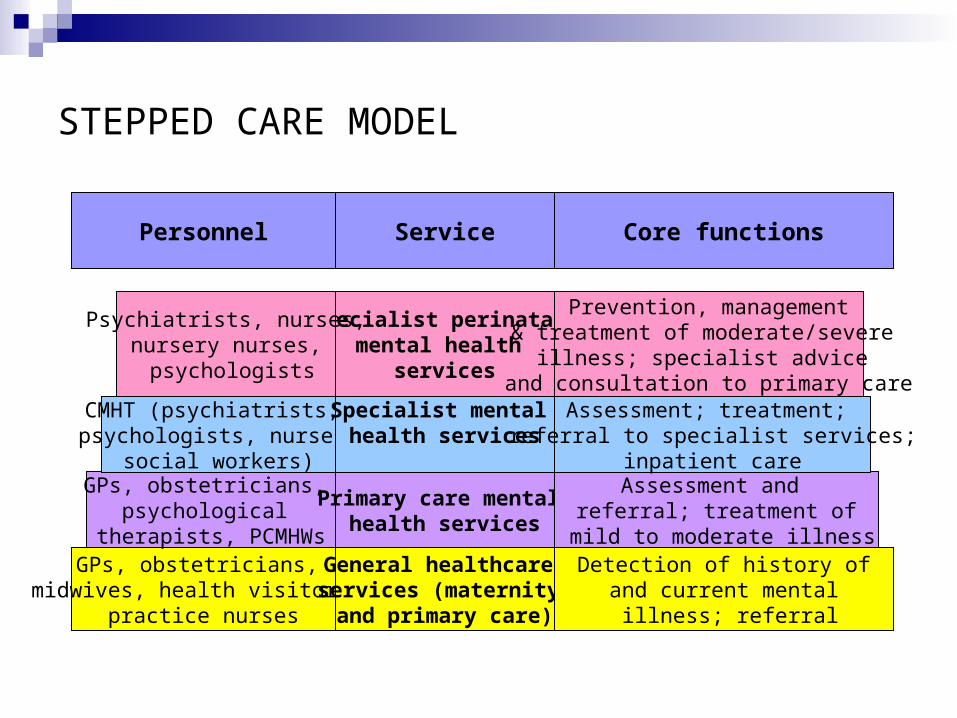
STEPPED CARE MODEL
GPs, obstetricians, midwives, health visitors,
practice nurses
General healthcare services (maternity and primary care)
Detection of history ofand current mental
illness; referral
GPs, obstetricians, psychological
therapists, PCMHWs
Primary care mental health services
Assessment and referral; treatment of
mild to moderate illness
CMHT (psychiatrists, psychologists, nurses
social workers)
Specialist mental health services
Assessment; treatment; referral to specialist services;
inpatient care
Specialist perinatal mental health
services
Psychiatrists, nurses,nursery nurses, psychologists
Prevention, management& treatment of moderate/severe
illness; specialist advice and consultation to primary care
Personnel Service Core functions
PRINCIPLES OF PRESCRIBING PSYCHOTROPIC MEDICATION
Careful risk-benefit assessment If mild to moderate severity, use non-pharmacological intervention Avoid first trimester exposure if at all possible Choose drugs with lower risk profiles for mother / foetus / infant Start lowest effective dose and increase slowly Tricyclic antidepressants (amitryptiline, imipramine, nortripyline)
lowest known risks in pregnancy but dangerous in overdose SSRI’s: Relatively safe, fluoxetine lowest risk, Sertraline (breast
feeding) Trifluoperazine, haloperidol antipsychotics of choice Avoid polypharmacy if at all possible
RISK-BENEFIT ANALYSIS
RISK OF DRUGS
Risk of teratogenicity Risk of neonatal withdrawal Risk of longer-term
neurobehavioural / cognitive problems
Risks in breastfeeding
RISK OF ILLNESS
Untreated illness may affect birth weight and gestational age at delivery
Possible detrimental effect of sress in pregnancy on foetus
May impact on mother-infant attachment and later infant development
ANTIDEPRESSANTS IN PREGNANCY
Tricyclic antidepressants (amitryptiline, imipramine, nortriptyline) lowest known risks in pregnancy but more dangerous in overdose
SSRI’s: Fluoxetine lowest risk; Sertraline, citalopram Association with Persistent pulmonary hypertension, septal heart
defect (Tuccori et al, 2009; Pedersen et al, 2009) though absolute risk small
Neonatal withdrawal symptoms possible with antidepressants - taper if clinically appropriate prior to delivery
Tuccori et al. 2009. Safety concerns associated with the use of Serotonin Reuptake inhibitors and other Serotonergic/Noradrenergic antidepressants during pregnancy: a review. Clinical Therapeutics 31:1426-1453Pedersen et al. 2009. Selective serotonin reuptake inhibitors in pregnancy and congenital malformations:Population based cohort study. BMJ 339, 3569-3575
ANTIDEPRESSANTS AND BREASTFEEDING
Antidepressants transfer readily into human milk though often at levels far below clinical range
Certain considered safer than others though in general long term outcomes for exposure unknown
Low levels in breast milk: Imipramine, nortripyline, sertraline
Higher levels in breast milk: fluoxetine, citalopram
Other SSRI’s / SNRI’s / newer antidepressants should be avoided until more data available
BENZODIAZEPINES
Associated with cleft palate, neonatal withdrawal and floppy baby syndrome
Only for short-term treatment of extreme anxiety and agitation
Consider gradually stopping in pregnant women
If prescribed, keep to lowest possible dose for shortest possible time
Avoid if possible or decrease in late pregnancy
Dolovich et al. 1998. Benzodiazepine use in pregnancy and major malformations or oral cleft: meta-analysis of cohort and case-control studies. BMJ, 317, 839-43
LITHIUM
Ebstein’s anomaly risk raised from 1 in 20,000 to 10 in 20,000
Do not prescribe routinely esp 1st trimester or breastfeeding
Well and LOW RISK => stop gradually over 4 weeks
Not well and HIGH RISK=> switch gradually to antipsychotic
stop & restart 2nd trimester
continue if high risk
monthly level monitoring
National Institute for Health and Clinical Excellence. Antenatal and postnatal mental health: clinicalmanagement and service guidance. Clinical guideline 45
VALPROATE
Neural tube defects risk raised from 6 in 10,000 to 100 -200 in 10,000
Developmental problems / Autistic spectrum disorder
‘Foetal valproate syndrome’
Do not routinely prescribe to women of childbearing potential
Explain risks
Consider alternative in bipolar (eg. Antipsychotic)
If no alternative, limit to maximum 1g daily in divided doses and slow release form, with 5mg folic acid
Kini, U 2006. Fetal valproate syndrome: a review. Ped & Perinatal Drug Ther 7(3) 123 - 30
ANTIPSYCHOTICS
Trifluoperazine : safest in pregnancy and breastfeeding
Risperidone, amisulpiride: raised prolactin levels
Olanzapine: weight gain, gestational diabetes
Clozapine: Do not routinely prescribe but some case reports of its successful use
Avoid depot medication
Current evidence not suggestive that antipsychotics are major teratogens. Possibly small risk of cardiovascular malformation
(1-1.5%) though no specific drug implicated
Reis & Kallen 2008. Maternal use of antipsychotics in early pregnancy and delivery outcome. J Clin Psychopharmacol 28(3):279-88
EXPLAINING RISKS
Before making treatment decisions discuss absolute and relative risks associated with treating and not treating the mental disorder during pregnancy and postnatal period
Acknowledge uncertainty surrounding risks Explain background risk of fetal malformations for pregnant women
without mental disorder (2-4%) Describe risks using natural frequencies (1 in 10 vs 10%) Use decision aids Written material Audiotaped records of consultation if possible
PSYCHOLOGICAL TREATMENTS
Women requiring psychological treatment during pregnancy should have rapid access to it
Should be seen normally within 1 month and no longer than 3 months afterwards
Lower threshold for access due to time-limited nature of pregnancy and changing risk-benefit ratio for psychotropic medication
Counselling
Cognitive behaviour therapy (CBT)
Interpersonal therapy
Psychodynamic therapy
SOCIAL INTERVENTIONS
Housing
Employment
Benefits
Support network (Surestart, postnatal groups)
Children & Families (Social Services) liaison
SUMMARY
Role for Perinatal Psychiatry in recognition and management of mental disorders during pregnancy and child birth
Antenatal & postnatal depression, baby blues common may be managed in primary care
Puerperal psychosis needs secondary care / perinatal service
Special consideration of risk / benefit issues in pregnancy & breastfeeding
Outcomes after treatment of most perinatal disorders good


















