Perinatal HIV Pediatric ID Previous presentation by Susan Schuval, MD.
20
Perinatal HIV Perinatal HIV Pediatric ID Pediatric ID Previous presentation by Previous presentation by Susan Schuval, MD Susan Schuval, MD
-
Upload
michael-walsh -
Category
Documents
-
view
219 -
download
1
Transcript of Perinatal HIV Pediatric ID Previous presentation by Susan Schuval, MD.

Perinatal HIV Perinatal HIV
Pediatric IDPediatric ID
Previous presentation by Susan Previous presentation by Susan Schuval, MDSchuval, MD
Case 1Case 1
An infant is born to a 30 year old HIV-infected An infant is born to a 30 year old HIV-infected
woman and you are called to evaluate the infant woman and you are called to evaluate the infant in the Well Baby Nurseryin the Well Baby Nursery
The infant is 4 hours old and doing well after a The infant is 4 hours old and doing well after a normal spontaneous vaginal deliverynormal spontaneous vaginal delivery Birth weight: 3 kgBirth weight: 3 kg Gestational age: 39 weeks Gestational age: 39 weeks
QUESTION 1QUESTION 1
Which information is most valuable in determining this Which information is most valuable in determining this infant’s risk for perinatal HIV acquisition? infant’s risk for perinatal HIV acquisition?
A.A. Maternal antiretroviral medications administered Maternal antiretroviral medications administered during pregnancyduring pregnancy
B.B. Date of maternal HIV diagnosis Date of maternal HIV diagnosis C.C. Maternal viral loadMaternal viral loadD.D. Maternal CD4 lymphocyte countMaternal CD4 lymphocyte count
QUESTION 1QUESTION 1
Which information is most valuable in determining this Which information is most valuable in determining this infant’s risk for perinatal HIV acquisition? infant’s risk for perinatal HIV acquisition?
A.A. Maternal antiretroviral medications administered Maternal antiretroviral medications administered during pregnancyduring pregnancy
B.B. Date of maternal HIV diagnosis Date of maternal HIV diagnosis C.C. Maternal viral loadMaternal viral loadD.D. Maternal CD4 lymphocyte countMaternal CD4 lymphocyte count

QUESTION 1-DISCUSSIONQUESTION 1-DISCUSSION
Maternal viral load is the most important
factor in determining whether HIV will be transmitted from mother to infant.
Caesarean section is performed routinely for HIV-infected women with viral loads > 1000 copies/mL.
The timing of perinatal HIV transmission is not known but probably occurs intrapartum
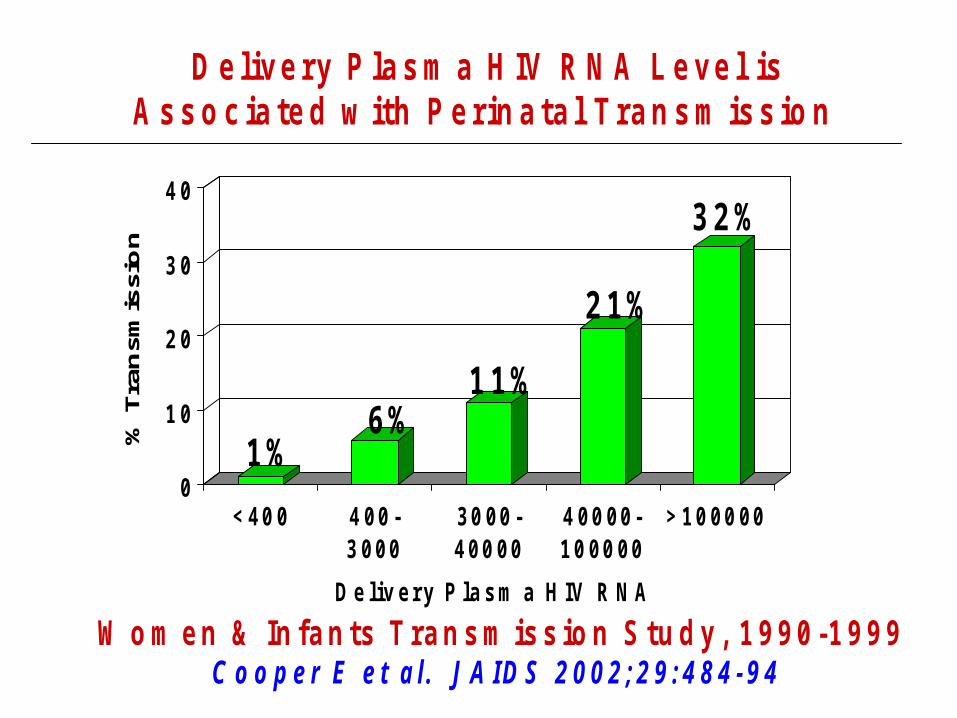
D e l iv e r y P la s m a H IV R N A L e v e l is A s s o c ia t e d w it h P e r in a t a l T r a n s m is s io n
1 %6 %
1 1 %
2 1 %
3 2 %
0
1 0
2 0
3 0
4 0
% T
ran
smis
sio
n
< 4 0 0 4 0 0 -3 0 0 0
3 0 0 0 -4 0 0 0 0
4 0 0 0 0 -1 0 0 0 0 0
> 1 0 0 0 0 0
D e l i v e r y P l a s m a H I V R N A
W o m e n & I n f a n t s T r a n s m is s io n S t u d y , 1 9 9 0 - 1 9 9 9C o o p e r E e t a l . J A ID S 2 0 0 2 ; 2 9 : 4 8 4 - 9 4
ADDITIONAL HISTORY ADDITIONAL HISTORY
The mother had an undetectable viral load one month prior to delivery and was treated with Reyataz, Norvir, and Sustiva during the 2nd and 3rd trimesters.
Her last CD4 count was 1200.
QUESTION 2 QUESTION 2
What is the best way to test the infant for What is the best way to test the infant for HIV infection?HIV infection?
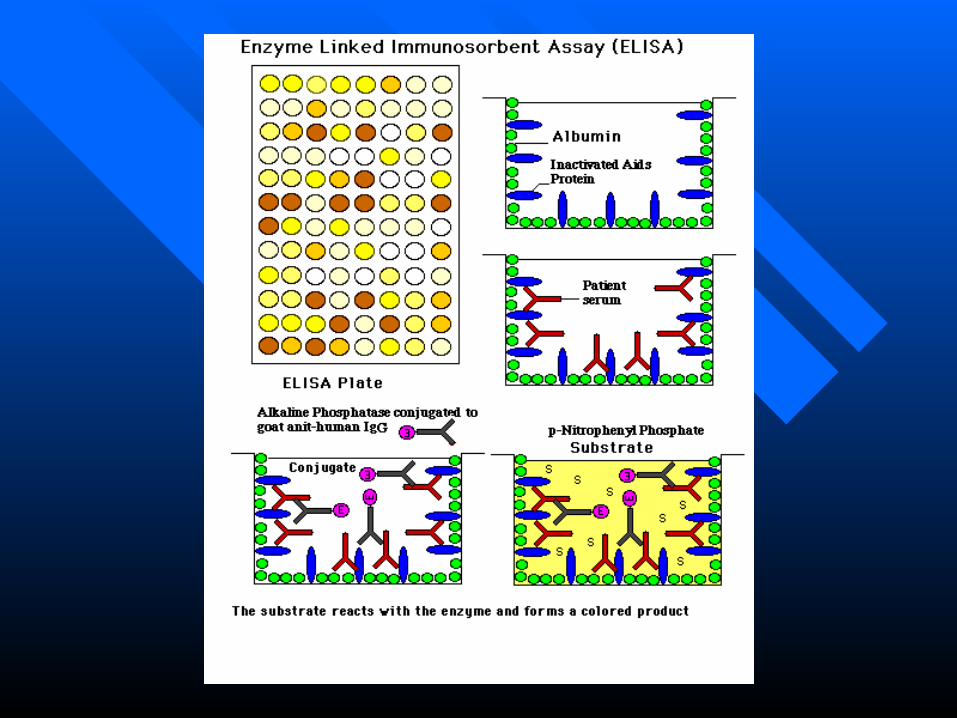
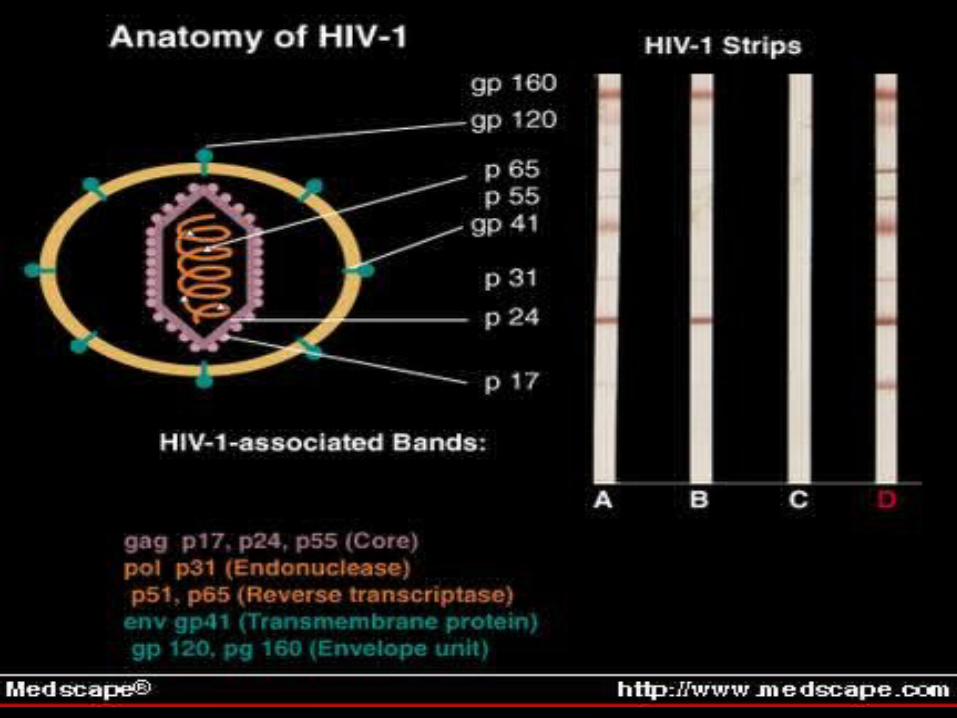
A. HIV serology: EIA/Western BlotA. HIV serology: EIA/Western Blot
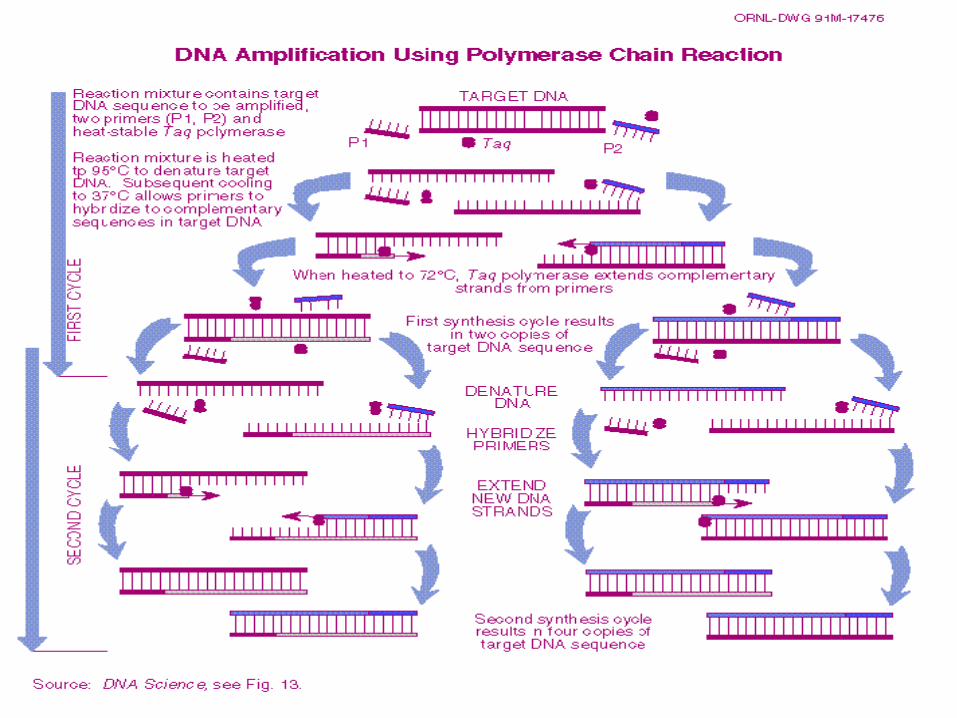
B. DNA PCRB. DNA PCR
C. RNA PCRC. RNA PCR
D. p24 antigen testD. p24 antigen test
QUESTION 2-DISCUSSIONQUESTION 2-DISCUSSION
HIV DNA PCR is the most sensitive assay HIV DNA PCR is the most sensitive assay available to test for HIV infection.available to test for HIV infection.
HIV-exposed infants followed by the HIV-exposed infants followed by the Pediatric ID Clinic are seen at birth, 2 Pediatric ID Clinic are seen at birth, 2 weeks of age, 6 weeks of age, 4 months and weeks of age, 6 weeks of age, 4 months and 18 months for PCR and serologic testing.18 months for PCR and serologic testing.
HIV Testing of Infants HIV Testing of Infants
Infants born to HIV-infected women will Infants born to HIV-infected women will routinely test positive for anti-HIV routinely test positive for anti-HIV antibodies because these are transmitted antibodies because these are transmitted from mother to infant.from mother to infant.
In the Pediatric ID Clinic, HIV-exposed In the Pediatric ID Clinic, HIV-exposed infants are followed until they infants are followed until they “serorevert”and lose the HIV antibodies, “serorevert”and lose the HIV antibodies, usually between 12-18 months of age.usually between 12-18 months of age.
QUESTION 3 QUESTION 3
Which regimen is most effective in reducing Which regimen is most effective in reducing perinatal HIV transmission?perinatal HIV transmission?
A. Maternal treatment with AZT during labor A. Maternal treatment with AZT during labor and delivery onlyand delivery only
B. Maternal treatment with AZT during B. Maternal treatment with AZT during pregnancy onlypregnancy only
C.C. Neonatal AZT for a 6 week courseNeonatal AZT for a 6 week courseD.D. All of the above All of the above
QUESTION 3-DISCUSSIONQUESTION 3-DISCUSSION
The 3-part regimen of:The 3-part regimen of: Maternal treatment with AZT during 2Maternal treatment with AZT during 2ndnd and 3 and 3rdrd
trimesters of pregnancy, trimesters of pregnancy, Maternal AZT during labor and delivery, Maternal AZT during labor and delivery, and and Neonatal AZT for a 6 week courseNeonatal AZT for a 6 week course
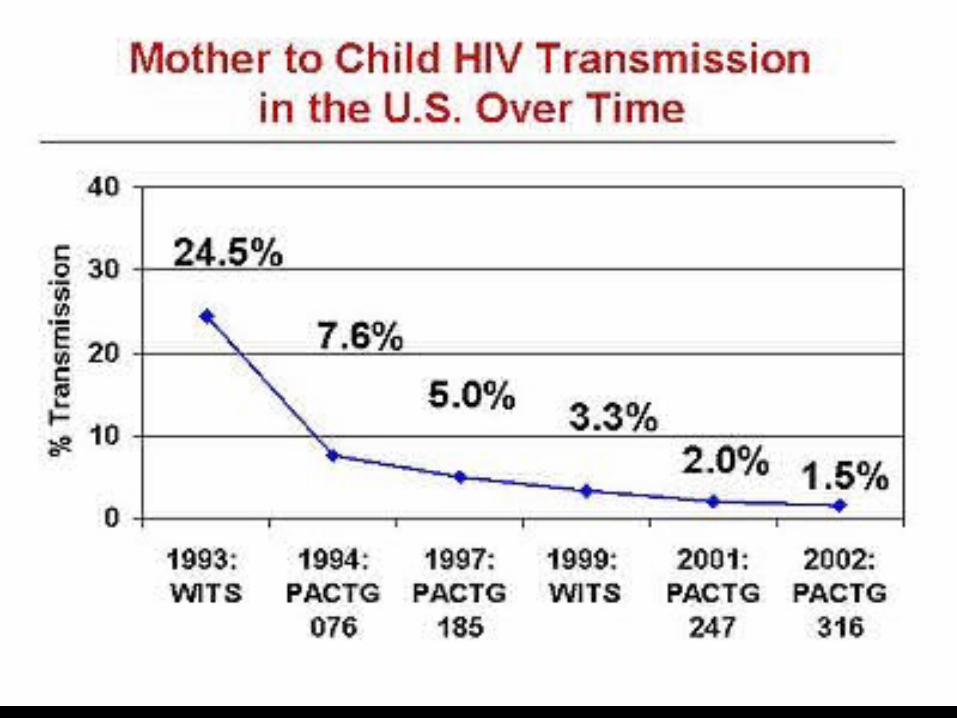
Has been shown to reduce perinatal HIV Has been shown to reduce perinatal HIV transmission from 24% to 8% (70% reduction).transmission from 24% to 8% (70% reduction).
EPIDEMIOLOGYEPIDEMIOLOGY
Over 90% of pediatric HIV infectionOver 90% of pediatric HIV infection
results from perinatal transmissionresults from perinatal transmissionU.S: 6000-7000 HIV+ women give U.S: 6000-7000 HIV+ women give
birth annuallybirth annually2004: 84 HIV+ infants born2004: 84 HIV+ infants born
Overview of Clinical Trials on Prevention of Mother-to-Child HIV Transmission
November 2003
Lynne M. Mofenson, MD, National Institutes of Health
Back to Slide Index
Slide 23: Mother to Child HIV Transmission in the U.S. Over Time
Download this individual powerpoint slide
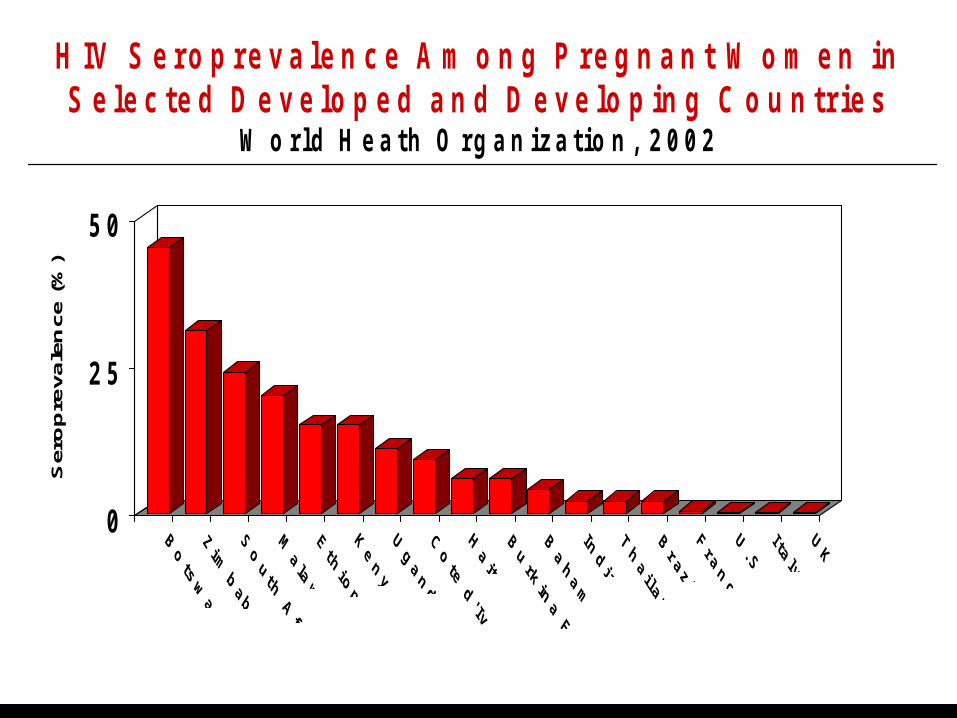
H I V S e r o p r e v a l e n c e A m o n g P r e g n a n t W o m e n i n S e l e c t e d D e v e l o p e d a n d D e v e l o p i n g C o u n t r i e s
W o r l d H e a t h O r g a n i z a t i o n , 2 0 0 2
0
2 5
5 0
Ser
op
reva
len
ce (
%)
QUESTION 4 QUESTION 4
How are infants who test HIV-positive How are infants who test HIV-positive
treatedtreated??A.A. AZT monotherapy AZT monotherapy
B.B. Bactrim aloneBactrim alone
C.C. ZithromaxZithromax
C.C. Highly active antiretroviral therapyHighly active antiretroviral therapy
QUESTION 4-DISUSSIONQUESTION 4-DISUSSION
Infants testing HIV DNA PCR-positive Infants testing HIV DNA PCR-positive are treated with combination are treated with combination
antiretroviral therapy (HAART=highly antiretroviral therapy (HAART=highly active retroviral therapy) and PCP active retroviral therapy) and PCP
prophylaxis.prophylaxis.