Perinatal Health Indicators...86.6Lawndale Christian Health Center 88.2Community Health Centers of...
57
Authors Rajesh Parikh, M.D., MPH – Vice President of Clinical Services & Workforce Development, IPHCA Naila Quraishi, MPH – Program Manager, IPHCA Illinois Primary Health Care Association Perinatal Health Indicators PERFORMANCE & PROMISING PRACTICES Based on Uniform Data Systems (UDS) Reports 3 rd Edition IPHCA Organizational Member Edition
Transcript of Perinatal Health Indicators...86.6Lawndale Christian Health Center 88.2Community Health Centers of...

AuthorsRajesh Parikh, M.D., MPH – Vice President of Clinical Services & Workforce Development, IPHCANaila Quraishi, MPH – Program Manager, IPHCA
Illinois Primary Health Care Association
Perinatal Health IndicatorsPerformance & Promising Practices
Based on Uniform Data Systems (UDS) Reports
3rd Edition
IPHCA Organizational Member Edition

Acknowledgement ............................................................................................................................................. iIntroduction ........................................................................................................................................................ ii
Performance & Promising Practices for Perinatal Health Indicators
Access to Prenatal Care ..................................................................................................................................... APerformance ....................................................................................................................................................... A-iReferences .......................................................................................................................................................... A-R
Low Birth Weight ............................................................................................................................................... BPerformance ....................................................................................................................................................... B-iReferences .......................................................................................................................................................... B-R
Promising Practices on Perinatal Health - 2013 .............................................................................................. C-iPromising Practices on Perinatal Health - 2014 .............................................................................................. C-iiReferences .......................................................................................................................................................... C-R
QI and System-Level Strategies ........................................................................................................................ C-1
AppendicesAppendix A – Health Center Stratification by Number of Patients Served .................................................... App AAppendix B – Prenatal Care Quality Tool ........................................................................................................ App BAppendix C – Referrals for High-Risk Prenatal Conditions ............................................................................ App CAppendix D – Postpartum Transition Strategies ............................................................................................. App DAppendix E – HITEQ Resources ....................................................................................................................... App EAppendix F – Guide to Patient and Family Engagement ................................................................................. App FAppendix G – The Joint Commission Health Literacy & Self-Management Tools........................................ App G
table of contents

i
As we continue to build on the Promising Practices and Performances document to foster peer to peer learning and develop a comprehensive resource of evidence-based recommendations, we are thankful for all the support and positive feedback we have received.
We are extremely thankful to Sachin Vispute for the initial draft of the document on performance section and to Samantha McCurties for the section on promising practices. In addition, we express our gratitude to Illinois Primary Health Care Association (IPHCA)’s Clinical Support Committee and IPHCA’s Chief Operating Officer, Kelly Carter* for their valuable feedback since the beginning. IPHCA’s Communications team provided tremendous support in editing and designing this resource.
Last, but not the least, without whom this report would be incomplete, a special thank you to all the health centers for their valuable time in discussing their successful strategies with us.
Finally, we want to express our profound admiration to all the health centers for their tremendous efforts in addressing health disparities.
Naila QuraishiRajesh Parikh
Authors:• Naila Quraishi, MPH – Intern• Rajesh Parikh, M.D., MPH – Vice President of Clinical Services & Workforce Development• Manasi Jayaprakash, M.D., MPH – Manager of Quality Improvement*
Health centers interviewed:• Promising Practices for 2013 data:
o PCC Community Wellness Centero Asian Human Services Family Health Centero Rural Health, Inc.o Shawnee Health Serviceo Community Health Improvement Centero Esperanza Health Centerso VNA Health Care
• Promising Practices for 2014 data:o Cass County Health Departmento Heartland Health Centerso Lawndale Christian Health Centero Heartland Community Health Clinic
* No longer with Association.
acknowledgement

ii
Illinois Primary Health Care Association (IPHCA) member performances are based on Uniform Data System (UDS) quality of chronic disease management indicators and its comparison with Healthy People 2020 (HP 2020) goals that were available. Community health centers (CHCs) reach populations that face the most burdens when accessing and maintaining health care. They have made admirable strides in bridging the gap between unaffordability and health care in this population group. However, with an influx of more patients through the Affordable Care Act and the existing burden of chronic diseases, health centers face multiple challenges. These include establishing continuity of care, need for culturally tailoring the services, transition to electronic health record (EHR) systems, shortage of a primary care workforce, resource constraints, and the challenge of navigating the Medicaid environment within the state. In the face of these challenges, there is a need for tracking performances against benchmarks and compilation of evidence-based guidelines and promising practices that are adaptable to primary care settings.
Methods IPHCA member health center performances for eight indicators on preventive health screening and services have been graphed using percentiles from 2010 to 2015 with data from Health Resources and Services Administration (HRSA). The HP 2020 targets are used as benchmarks to measure performance. In addition, evidence-based recommendations from experts such as Community Preventive Services Task Force and/or U.S. Preventive Services Task Force (The Task Force) and Promising Strategies Identified Through Literature Review are highlighted.
Purpose The essential purpose of this document is to provide a resource for health centers that consists of not only evidence-based recommendations, but also includes promising practices from some of the best performing health centers. Therefore, this document provides a platform to generate discussions on how to overcome challenges and how to best adapt successful practices to primary care settings. It is important to remember that health center characteristics, such as population group, location, revenue source, prevalence of diseases, and availability of resources are varied, which might contribute to significant challenges for some. In Appendix B, health centers are stratified by patient population size.
Current Limitations of Using UDS Data
introduction
Performance is not 100% reliable and generalizable as the reporting varies between health centers; some report a sample while others report universal data. However, it is the only publicly available data, which can be used to track performance and generate discussion.
IPHCA Member Characteristics In 2015-16, there were 44 member health centers from Illinois, two from Iowa and one from Missouri and therefore a total of 47 IPHCA member health centers for which UDS data was available. As of June 2017, the total number of patients served by Illinois grantees was 1,229,655; 78% of Illinois grantees are accredited as Patient Centered Medical Home (PCMH) and 93% of Illinois grantees have transitioned into Electronic Health Record (EHR) systems. Both the centers in Iowa are PCMH recognized and have EHR systems. The health center in Missouri also has an EHR system.
Using this Resource Strategies for improving preventive health screening and services are categorized into the following sections: Illinois Health Center Spotlights, The Task Force Recommendations and Strategies Identified Through Literature Search. Recommendations from the U.S. Preventive Services Task Force and Community Preventive Services Task Force are included under The Task Force recommendations. Both the task force recommendations are based on a scientific systematic review process that identifies recommendations from numerous existing studies with strong or sufficient evidence. The U.S. Preventive Services Task Force develops recommendations for clinical preventive services, while Community Preventive Services Task Force develops recommendations about community preventive services, programs and policies to improve health.

A
Access to Prenatal Care Rationale: If women enter care in their first trimester, then the probability of an adverse birth outcome will be reduced.
UDS Performance Measure: “Proportion of prenatal care patients who entered treatment during their first trimester.”
(Includes prenatal patients referred outside during their first trimester)
HP 2020 Objective: The objective for comparison is under Maternal, Infant, and Child Health (MICH) section.
MICH-10.1: Increase the proportion of pregnant women who receive prenatal care beginning in the first trimester to 77.9%.
National & State Comparison:Illinois’ average has been consistently higher than the national average. In 2015, although 75th and 25th percentile improved, a decline in the 25th percentile might have contributed to a slightly decreased average for Illinois. Close to 50% of health centers have met the Healthy People (HP) 2020 target.
Performance on Perinatal HealtH measures
Figure A: Comparison of UDS averages (Illinois & National) and IPHCA member health center percentiles based on UDS data for Access to Prenatal Care

A-i-1
6
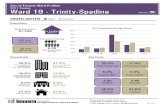
Figure 1.2: 2010 Access to Prenatal Care data (%) of IPHCA member health centers and their percentiles
44.6 51.8 53.3
58.0 62.0 62.0 63.5 65.2 65.9 65.9 65.9
68.0 68.0 68.6 69.9 70.9 71.6 72.0 72.6 73.1 73.3 73.5 73.7 74.0
77.9 77.9 78.0 79.6 79.7 79.7
83.4 84.4 85.5 85.7 86.0 86.6
90.4 94.2
0.0 10.0 20.0 30.0 40.0 50.0 60.0 70.0 80.0 90.0 100.0
Circle Family HealthCare NetworkTCA Health, Inc.
Mile Square Health CenterBeloved Community Family Wellness Center
Near North Health Service CorporationPCC Community Wellness Center
Community Health Care, Inc.Aunt Martha's Youth Service Center, Inc.Community Health Improvement Center
Family Christian Health Center25th PERCENTILE
Friend Family Health Center, Inc.Will County Community Health Center
Access Community Health NetworkHeartland Health Centers
Community Health & Emergency Services, Inc.Lake County Health Department
Heartland Community Health Clinic50th PERCENTILE
Greater Elgin Family Care CenterHeartland Health Outreach, Inc.
VNA Health CareCentral Counties Health Centers, Inc.
Southern Illinois Healthcare FoundationCrusader Community Health
HP 2020 TARGETChicago Family Health Center
Shawnee Health Service75th PERCENTILE
Lawndale Christian Health CenterChristopher Rural Health Planning Corporation
Community Health Centers of Southeastern…Alivio Medical Center
PrimeCare Community Health, Inc.Erie Family Health Center, Inc.
Christian Community Health CenterRural Health, Inc.
Asian Human Services Family Health Center
Figure A-i-1: 2010 Access to Prenatal Care data (%) of IPHCA member health centers and their percentiles
2010
Performance on access to Prenatal care

A-i-2
7
1Four health centers without prenatal patients
Figure 1.3: 2011 Access to Prenatal Care data (%) of IPHCA member health centers and their percentiles
1 Cass County Health Department, Community Health Partnership of Illinois, Eagleview Community Health System, and Whiteside County Community Health Clinic.
52.2 53.8
58.9 59.4 61.6 62.9 63.1 64.3 64.5 65.2 67.3 68.0 68.4
71.0 72.0 74.0 74.8 75.4 75.8 76.2 77.2 77.3 77.9 78.7 79.2 81.4 81.7 81.7 83.0 83.5 84.1 86.1 86.6 88.2
91.2 91.5
98.0 100.0
0.0 20.0 40.0 60.0 80.0 100.0 120.0
Circle Family HealthCare NetworkAunt Martha's Youth Service Center, Inc.
Mile Square Health CenterTCA Health, Inc.
Community Health & Emergency Services, Inc.Community Health Improvement Center
Beloved Community Family Wellness CenterPCC Community Wellness Center
Central Counties Health Centers, Inc.25th PERCENTILE
Crusader Community HealthFriend Family Health Center, Inc.
Community Health Care, Inc.Family Christian Health Center
Will County Community Health CenterChristian Community Health Center
Lake County Health DepartmentSouthern Illinois Healthcare Foundation
50th PERCENTILEHeartland Community Health Clinic
Shawnee Health ServiceAsian Human Services Family Health Center
HP 2020 TARGETChicago Family Health Center
Alivio Medical CenterAccess Community Health Network
Greater Elgin Family Care CenterHeartland Health Centers
75th PERCENTILEPrimeCare Community Health, Inc.
VNA Health CareChristopher Rural Health Planning Corporation
Lawndale Christian Health CenterCommunity Health Centers of Southeastern…
Near North Health Service CorporationErie Family Health Center, Inc.
Rural Health, Inc.Heartland Health Outreach, Inc.
Figure A-i-2: 2011 Access to Prenatal Care data (%) of IPHCA member health centers and their percentiles
Four health centers without prenatal patients.2
2011
Performance on access to Prenatal care

A-i-3
Six health centers without any prenatal patients.3 8
2Six health centers without any prenatal patients
Figure 1.4: 2012 Access to Prenatal Care data (%) of IPHCA member health centers and their percentiles
2 Cass County Health Department, Community Health Partnership of Illinois, Eagle View Community Health System, Macoupin County Health Department, and Whiteside County Community Health Clinic.
44.9 56.9 58.8 58.9 60.1 61.1 61.7 63.3
67.9 67.9 67.9 69.3 70.4 70.9 71.7 71.9 73.5 74 74.3 74.3 74.8 75.2 75.5 76.8 77.9 78 79.2 80 80.9 80.9 80.9 82.7 84.6 85.2 85.5 85.7 86.9 87.1
94.3
0 10 20 30 40 50 60 70 80 90 100
Circle Family HealthCare NetworkBeloved Community Family Wellness Center
PCC Community Wellness CenterTCA Health, Inc.
Christian Community Health CenterNear North Health Service Corporation
Community Health Improvement CenterMile Square Health Center
25th PERCENTILESIU Center for Family Medicine
Community Health Care, Inc.Aunt Martha's Youth Service Center, Inc.
Heartland Health CentersChristopher Rural Health Planning Corporation
Access Community Health NetworkHeartland Community Health Clinic
Family Christian Health CenterFriend Family Health Center, Inc.
50th PERCENTILEWill County Community Health Center
Lake County Health DepartmentEsperanza Health Centers
Chicago Family Health CenterCentral Counties Health Centers, Inc.
HP 2020 TARGETVNA Health Care
Alivio Medical CenterSouthern Illinois Healthcare Foundation
75th PERCENTILECrusader Community Health
Shawnee Health ServiceAsian Human Services Family Health Center
Greater Elgin Family Care CenterCommunity Health Centers of Southeastern Iowa,…
Erie Family Health Center, Inc.Heartland Health Outreach, Inc.
Lawndale Christian Health CenterPrimeCare Community Health, Inc.
Rural Health, Inc.
Figure A-i-3: 2012 Access to Prenatal Care data (%) of IPHCA member health centers and their percentiles
2012
Performance on access to Prenatal care

A-i-4
Eight health centers without any prenatal patients and4 One health center did not report data for 2013.5
10
Figure 1.5: 2013 Access to Prenatal Care data (%) of IPHCA member health centers and their percentiles
5Eight health centers without any prenatal patients
5 Cass County Health Department, Community Health Partnership of Illinois, Henderson Co. Rural Health Center, Inc. (Eagleview Community Health System), Whiteside County Community Health Clinic, Chestnut Health Systems, Community Nurse Health Association, Knox County Health Department, and Community Health Care, Inc.
48.3 55.2 55.7 57.1
60.3 60.7 61.4 62.5 64.5 65.6 65.9 67.7 69.1 69.3 69.3 69.6 69.6 69.9
72.8 73.5 74.1 74.3 74.5 74.6 76.4 76.7 76.8 77.9 78.1 78.4 79.1 81 81.2 81.8
84 85.8 86.2 86.2 87.4
92.9
0 10 20 30 40 50 60 70 80 90 100
Circle Family HealthCare NetworkTCA Health, Inc.
Christian Community Health CenterHeartland Health Outreach, Inc.
Community Health & Emergency Services, Inc.Beloved Community Family Wellness Center
Near North Health Service CorporationMacoupin County Public Health Department
Community Health Improvement Center25th PERCENTILE
SIU Center for Family MedicineFamily Christian Health Center
Aunt Martha's Youth Service Center, Inc.Lake County Health Department
Heartland Community Health ClinicChristopher Rural Health Planning Corporation
Friend Family Health Center, Inc.Southern Illinois Healthcare Foundation
Will County Community Health Center50th PERCENTILE
Chicago Family Health CenterPCC Community Wellness Center
Heartland Health CentersVNA Health Care
Access Community Health NetworkMile Square Health Center
Crusader Community HealthHP 2020 TARGET
Asian Human Services Family Health CenterPrimeCare Community Health, Inc.
75th PERCENTILECommunity Health Centers of Southeastern…
Shawnee Health ServiceAlivio Medical Center
Esperanza Health CentersCentral Counties Health Centers, Inc.
Greater Elgin Family Care CenterLawndale Christian Health Center
Erie Family Health Center, Inc.Rural Health, Inc.
Figure A-i-4: 2013 Access to Prenatal Care data (%) of IPHCA member health centers and their percentiles
2013
Performance on access to Prenatal care

A-i-5
2014
Performance on access to Prenatal care
Figure A-i-5: 2014 Access to Prenatal Care data (%) of IPHCA member health centers and their percentiles.
Three health centers without prenatal patient data.6

A-i-6
2015
Performance on access to Prenatal care
Figure A-6: 2015 Access to Prenatal Care data (%) of IPHCA member health centers and their percentiles

A-R
1. Three health centers without any prenatal data: Knox County Health Department, Hamdard Center for Health & Human Services, Preferred Family Healthcare, Inc
2. Cass County Health Department, Community Health Partnership of Illinois, Eagle View Community Health System, and Whiteside County Community Health Clinic.
3. Cass County Health Department, Community Health Partnership of Illinois, Eagle View Community Health System, Macoupin County Health Department, and Whiteside County Community Health Clinic.
4. Cass County Health Department, Community Health Partnership of Illinois, Eagle View Community Health System, Macoupin County Health Department, Whiteside County Community Health Clinic, Chestnut Health Systems, Community Nurse Health Association, and Knox County Health Department.
5. Community Health and Emergency Services, Inc.6. Three health centers without any prenatal data: Knox County Health Department, Hamdard Center for
Health & Human Services, and Preferred Family Healthcare, Inc.
access to Prenatal care – references

B
Low Birth Weight
Rationale: If there are fewer low birthweight (birth weight under 5.5 pounds or 2500 grams) children born, then there will be fewer children who suffer the multiple negative sequela of low birthweight, such as delayed or diminished intellectual and/or physical development.
UDS Performance Measure:“Proportion of patients born to health center patients whose birth weight was below normal (less than 2500 grams).”
(Includes prenatal patients referred outside of health center for delivery)
HP 2020 Objective: The objective for comparison is under Maternal, Infant, and Child Health (MICH) section. MICH-8 Reduce low birth weight (LBW) and very low birth weight (VLBW).
MICH08.1: To reduce the low birth weight percent to below 7.8%.
National & State Comparison:Illinois average has improved since 2010, and in 2015, it has surpassed the HP 2020 target and is nearing the National average. Majority of IPHCA member health centers have surpassed the HP 2020 target. Since 2010, 25th percentile has remained the same and improvement is called for among the health centers around the 25th percentile.
Note: The lower the percentage on this indicator, the better the performance.
Performance on low birtH weigHt
Figure B: Comparison of UDS averages (Illinois & National) and IPHCA member health center percentiles based on UDS data for Low Birth Weight

B-i-1
12
Figure 2.2: 2010 Low Birth Weight data (%) of IPHCA member health centers and their percentiles
7Health center names without any prenatal patient delivery
7 Cass County Health Department, Community Health Partnership of Illinois, Eagleview Community Health System, and Whiteside County Community Health Clinic.
24.0 21.4
13.6 11.2 11.0 10.9
10.5 10.3
9.8 9.8 9.8 9.8
9.4 9.1 8.9 8.8 8.7 8.6 8.6 8.5 8.3
8.0 7.9 7.8
7.1 6.8
6.0 5.9 5.9 5.9
5.3 5.3
4.2 4.0
2.2 2.1
1.7 0.0
0.0 5.0 10.0 15.0 20.0 25.0
Christian Community Health CenterTCA Health, Inc.
Rural Health, Inc.Aunt Martha's Youth Service Center, Inc.
Friend Family Health Center, Inc.Lawndale Christian Health Center
VNA Health CareCentral Counties Health Centers, Inc.
Access Community Health NetworkGreater Elgin Family Care Center
Shawnee Health Service25th PERCENTILE
Crusader Community HealthAlivio Medical Center
Heartland Community Health ClinicSouthern Illinois Healthcare Foundation, Inc.
Christopher Rural Health Planning CorporationCircle Family HealthCare Network
50th PERCENTILEPCC Community Wellness Center
Heartland Health CentersNear North Health Service Corporation
Family Christian Health CenterHP 2020 TARGET
Chicago Family Health CenterLake County Health Department
Will County Community Health CenterCommunity Health Improvement Center
Erie Family Health Center, Inc.75th PERCENTILE
Beloved Community Family Wellness CenterCommunity Health Care, Inc.
Community Health Centers of Southeastern…Mile Square Health Center
PrimeCare Community Health, Inc.Community Health & Emergency Services, Inc.
Asian Human Services Family Health CenterHeartland Health Outreach, Inc.
Figure B-i-1: 2010 Low Birth Weight data (%) of IPHCA member health centers and their percentiles
Health center names without any prenatal patient delivery.2
2010
Performance on low birtH weigHt

B-i-2
13
Figure 2.3: 2011 Low Birth Weight data (%) of IPHCA member health centers and their percentiles
8Health Center names without any prenatal patient delivery 9Unreported for 2011 8 Cass County Health Department, Community Health Partnership of Illinois, Eagleview Community Health System, Macoupin County Health Department, Whiteside County Community Health Clinic 9 Heartland Health Outreach
14.2 12.0
11.3 11.0 10.8
10.0 9.9
9.6 9.2 9.2 9.2 9.1
8.5 8.4 8.3 8.1 7.9 7.8
6.6 6.6 6.4 6.3 6.3 6.3 6.1
5.8 5.8
5.5 5.5 5.4
4.9 4.8 4.8 4.6 4.4
2.4 0.0
0.0 5.0 10.0 15.0 20.0 25.0
VNA Health CareFriend Family Health Center, Inc.
TCA Health, Inc.Alivio Medical Center
Aunt Martha's Youth Service Center, Inc.Access Community Health Network
PCC Community Wellness CenterLawndale Christian Health Center
25th PERCENTILEAsian Human Services Family Health Center
Shawnee Health ServiceCrusader Community Health
Central Counties Health Centers, Inc.Christian Community Health Center
Family Christian Health CenterSouthern Illinois Healthcare Foundation, Inc.
Rural Health, Inc.HP 2020 TARGET50th PERCENTILE
Chicago Family Health CenterWill County Community Health Center
Erie Family Health Center, Inc.Community Health & Emergency Services, Inc.
PrimeCare Community Health, Inc.Heartland Community Health Clinic
Heartland Health CentersChristopher Rural Health Planning Corporation
75th PERCENTILELake County Health Department
Near North Health Service CorporationCommunity Health Centers of Southeastern…
Greater Elgin Family Care CenterCommunity Health Care, Inc.
Circle Family HealthCare NetworkCommunity Health Improvement Center
Mile Square Health CenterBeloved Community Family Wellness Center
Figure B-i-2: 2011 Low Birth Weight data (%) of IPHCA member health centers and their percentiles
Health Center names without any prenatal patient delivery3 and unreported for 2011.4
2011
Performance on low birtH weigHt

B-i-3
14
Figure 2.4: 2012 Low Birth Weight data (%) of IPHCA member health centers and their percentiles
10Health center names without any prenatal patient delivery 10 Cass County Health Department, Community Health Partnership of Illinois, Henderson Co. Rural Health Center, Inc. (Eagleview Community Health System), Macoupin County Health Department, Whiteside County Community Health Clinic, Chestnut Health Systems, Community Nurse Health Association, and Knox County Health Department.
12.7 12.6
11.3 10.7
10.2 10 9.8 9.7 9.7 9.7 9.6 9.4
9.1 8.9 8.7 8.6 8.5 8.4 8.3 8.3 8.2
7.9 7.8
7.5 7.2
6.7 6.7
6.3 6.1 5.9 5.8 5.8 5.6 5.5 5.4
5.1 4.5
3.6 0 0
0 5 10 15 20 25
Central Counties Health Centers, Inc.Mile Square Health Center
Alivio Medical CenterAccess Community Health Network
Friend Family Health Center, Inc.Community Health Centers of Southeastern Iowa,…
VNA Health Care25th PERCENTILE
Crusader Community HealthSouthern Illinois Healthcare Foundation, Inc.
Family Christian Health CenterEsperanza Health Centers
Christopher Rural Health Planning CorporationCommunity Health Improvement Center
Shawnee Health ServicePCC Community Wellness CenterLawndale Christian Health Center
SIU Center for Family Medicine50th PERCENTILE
Chicago Family Health CenterHeartland Community Health Clinic
Asian Human Services Family Health CenterHP 2020 TARGET
Circle Family HealthCare NetworkCommunity Health & Emergency Services, Inc.
Christian Community Health CenterWill County Community Health Center
TCA Health, Inc.Aunt Martha's Youth Service Center, Inc.
Near North Health Service Corporation75th PERCENTILERural Health, Inc.
Lake County Health DepartmentGreater Elgin Family Care Center
Erie Family Health Center, Inc.Community Health Care, Inc.
Heartland Health CentersPrimeCare Community Health, Inc.
Beloved Community Family Wellness CenterHeartland Health Outreach, Inc.
Figure B-i-3: 2012 Low Birth Weight data (%) of IPHCA member health centers and their percentiles
Health center names without any prenatal patient delivery5
2012
Performances on low birtH weigHt

B-i-4
15
Figure 2.5: 2013 Low Birth Weight data (%) of IPHCA member health centers and their percentiles
16.7 14.8
12.1 11.7 11.6
10.9 10.2 10.2 10.2
9.8 9.6
9.2 8.8
8.5 8.3 8.3 8.2 8.1 7.9 7.8 7.8 7.6 7.5 7.5 7.4 7.3
6.9 6.4 6.3
5.9 5.9 5.7 5.6
4.8 4.4
3.5 3.5
2.9 2.1
0
0 5 10 15 20 25
Heartland Health Outreach, Inc.TCA Health, Inc.
Christian Community Health CenterCentral Counties Health Centers, Inc.
PCC Community Wellness CenterCommunity Health & Emergency Services, Inc.
Lawndale Christian Health CenterSouthern Illinois Healthcare Foundation, Inc.
Mile Square Health Center25th PERCENTILE
Shawnee Health ServiceCommunity Health Improvement Center
VNA Health CareAccess Community Health Network
Crusader Community HealthMacoupin County Public Health Department
Chicago Family Health CenterAunt Martha's Youth Service Center, Inc.
Heartland Community Health ClinicHP 2020 TARGET50th PERCENTILE
Greater Elgin Family Care CenterFriend Family Health Center, Inc.
Will County Community Health CenterFamily Christian Health Center
Lake County Health DepartmentNear North Health Service Corporation
Asian Human Services Family Health CenterCommunity Health Centers of Southeastern Iowa,…
Erie Family Health Center, Inc.75th PERCENTILE
PrimeCare Community Health, Inc.Alivio Medical Center
SIU Center for Family MedicineChristopher Rural Health Planning Corporation
Heartland Health CentersEsperanza Health Centers
Rural Health, Inc.Beloved Community Family Wellness Center
Circle Family HealthCare Network
Figure B-i-4: 2013 Low Birth Weight data (%) of IPHCA member health centers and their percentiles
2013
Performances on low birtH weigHt
Health center names without any prenatal patient delivery6

B-i-5
2014
Performances on low birtH weigHt
Figure B-i-5: 2014 Low Birth Weight data (%) of IPHCA member health centers and their percentiles7

2015
Performances on low birtH weigHt
Figure B-i-6: 2015 Low Birth Weight data (%) of IPHCA member health centers and their percentiles
B-i-6

B-R
low birtH weigHt – references
1. 41 health centers were included for the 2014 percentiles.2. Cass County Health Department, Community Health Partnership of Illinois, Eagle View Community Health
System, and Whiteside County Community Health Clinic.3. Cass County Health Department, Community Health Partnership of Illinois, Eagle View Community Health
System, Macoupin County Health Department, Whiteside County Community Health Clinic, and Heartland Health Outreach.
4. Cass County Health Department, Community Health Partnership of Illinois, Eagle View Community Health System, Macoupin County Health Department, Whiteside County Community Health Clinic, Chestnut Health Systems, Community Nurse Health Association, and Knox County Health Department.
5. Cass County Health Department, Community Health Partnership of Illinois, Eagle View Community Health System, Whiteside County Community Health Clinic, Chestnut Health Systems, Community Nurse Health Association, Knox County Health Department, and Community Health Care, Inc.
6. Health center names without any deliveries: Knox County Health Department, Hamdard Center for Health & Human Services, Preferred Family Healthcare, Inc., and Community Health Centers of Southeastern Iowa, Inc.
7. Two health centers with ‘0’ ‘Prenatal Patients who Delivered’ have been excluded from percentile calculation

C-i-1
Due to commonality of strategies for prenatal care and lowering the risk of low birth weight, strategies will be considered together under perinatal health.
Illinois Health Center Spotlight
1 Erie Family Health Center, Inc. – Chicago, ILErie has consistently performed above the HP 2020 target in maintaining high access to prenatal care
for pregnant women and low percentage of LBW since 2010 (Figure 1 on page 5-9 and Figure 2 on pages 10-14 ). In 2012, Erie had 86% of its pregnant women enter into prenatal care in first trimester and its LBW was 5.4%. Success behind this can be attributed to a successful program of pre-pregnancy testing, an active workforce of women’s health promoters, and an emphasis on continuous team-based provision of care. Based on Erie’s successful model of care for prenatal patients, they were highlighted by Health Resources Service Administration (HRSA) in their grantee spotlight.1 Strategies discussed during interview and identified through grantee spotlight are below:
• Free pre-pregnancy test – Women undergo a free walk-in pre-pregnancy test; and, if found positive, a women’s health promoter talks to them and immediately links them to a primary care physician of their choice ensuring the first access to prenatal care.
• Women’s health promoter – They are part of interdisciplinary women’s health care teams. They play a crucial role in facilitating early entry into prenatal care by being the first point of contact for pregnant women and women who suspect they might be pregnant. If pregnant, their roles can be identified as:○ Follow a standardized prenatal care intake
procedure.○ Recording patient’s health history.○ Assessing pregnancy risk status.○ Providing health education.○ Linking patients to case managers and social
services.• Centering Pregnancy – Group care is provided
in accordance with Centering Pregnancy. Also, women’s health promoters work as centering pregnancy facilitators and breast feeding counselors throughout a woman’s pregnancy.
• Continuous provision of care and care coordination – This is aided by the presence of a robust Electronic Medical Record (EMR) system. A standardized assessment tool aids the women’s health promoter in inputting all the necessary data. In addition, a spread sheet has been developed by
Erie’s Women’s Health Department and quality improvement staff, which is used by the women’s health promoter to track patients’ estimated date of delivery, including provider capacity and availability. It helps them assign new prenatal patients to providers on the date pregnancy is confirmed.
• Quality Improvement (QI) strategies – In addition to the above specific strategies for prenatal care, some QI strategies were also identified that are applicable to other indicators. They are:○ Goals are set collaboratively where various clinical
groups come together and share quality data and set goals for the following 18 months.
○ Peer review – Individual providers are benchmarked against other providers every quarter which helps in engaging providers in a competitive spirit.
2 Rural Health, Inc. – Anna, ILRural Health has maintained high performance in access to prenatal care since 2010 (Figure 1, on pages
5-9); in 2012, the percentage of prenatal patients having their first prenatal check-up was 94%. With respect to low birth weight (Figure 2, on pages 10-13), Rural Health has improved considerably; in 2010, LBW was 13.6%, which decreased to an impressive 5.8% in 2012 and crossed HP 2020 target of 7.8%. A comprehensive approach to prenatal care and a strong emphasis on health education at every visit has helped lower the percentage of low birth weight and maintain adequate prenatal care. Strategies practiced are:
• Comprehensive care – Being located in a rural area, most of the patients face challenges in reaching health centers. To overcome this and to avoid patients making multiple trips, a comprehensive approach is taken when prenatal patients visit the health center:○ During the first visit, patient meets with a nurse
and then the doctor. ○ While waiting, patient undergoes glucose tolerance
screening and watches health education videos.• Health education - at each visit that stresses on high
risk behaviors such as smoking, exposure to second hand smoke, alcohol consumption, drug use, and consequences due to these on perinatal health.
• Provider - The obstetrician is committed to seeing patients even if they are late, and maintaining a strong relationship with the area hospital, which is highly beneficial in a rural setting.
• QI strategies - Some QI strategies identified are also applicable to other indicators. ○ Monthly medical staff meetings and provider
education led by QI Nurse at each meeting are conducted.
Promising Practices on Perinatal HealtH – 2013

C-i-2
○ Flow sheet – Three years ago, an adult preventative flow sheet was created that includes majority of the questions for providers to follow related to UDS indicators. Several flow sheets are utilized for other services which help in auditing and patient care.
• Other Common Strategies - Some common strategies were also identified that are applicable to multiple indicators. In March 2012, NotifyMD helped create a patient outreach call system for certain diagnoses. ○ The system can include daily appointment
reminders or automated reply for no-show calls (e.g. missed appointment in case of prenatal care).
○ It could also include a routine call for reminder appointments. This has dropped the no-show rate from 16-18% to < 9% in the past two years.
The Community Guide
The Task Force recommendations are geared toward reducing fetal abnormalities through targeting alcohol consumption, smoking cessation, and weight loss. This recommendation is highly relevant especially with the investigation on alcohol and illicit drugs in newborns done by Stanley Manne Children’s Research Institute of Ann & Robert H. Lurie Children’s Hospital of Chicago. They investigated the rates in which Illinois newborns tested positive for alcohol, narcotics, hallucinogenic agents, and cocaine during the years 2008-12 using ICD-9 codes from hospital discharge data. The key findings of the data released by them in 2014 are:2
• The rates at which newborns test positive for alcohol is lower than for illicit drugs. It was identified that alcohol is metabolized much more quickly than illicit drugs, and thus it is assumed to be underestimated.
• The rates at which newborns test positive for cocaine has decreased significantly over time. However, cocaine is the highest detected substance (148.6 per 100,000 live hospital births in Illinois, 2008-12), followed by narcotics (108.3), hallucinogenic agents (48.8), and alcohol (17.7).
• A significant finding is the variation by race of the rates at which newborns test positive for narcotics and cocaine.○ Black newborns have the highest rate of substance
detection for all the tested substances.○ Hispanic newborns have the lowest rates of
substance detection when compared to blacks and whites.
○ The difference between black babies and both white and hispanic babies were greatest for alcohol and hallucinogens.
• Another important finding is the variation by region.
○ All regions had the same pattern as overall rates, except Peoria, where rates of testing positive for narcotics was three times higher than the rate of testing positive for cocaine (215.1 and 128.7 respectively).
• Chicago had the highest rate of testing positive for cocaine at 251.5 per 100,000 live hospital births.○ In the far South region of Chicago, detection of
narcotics and cocaine was nearly equal.○ The West, South, Southwest, and Far South
regions had dramatically higher rates of substance detection compared to the North, Northwest and Central regions.
The above data is of high value for Illinois health centers depending on the location of the health center and the patient population served. Moreover, national data reveals that 18% of pregnant women drink alcohol during early pregnancy and 9% of all pregnant women reported to have consumed alcohol.3 The Task Force recommendations address some of the problems as revealed by above data and are:
• Preventing Excessive Alcohol Consumption – Based on strong evidence of effectiveness, The Task Force recommends electronic screening and brief intervention (e-SBI) in reducing self-reported excessive alcohol consumption and alcohol-related problems. E-SBI uses electronic devices such as computers, telephones, or mobile devices to facilitate the delivery of key elements of traditional screening and brief intervention (SBI). SBI involves screening individuals for excessive drinking and delivering a brief intervention that provides personalized feedback about the risks and consequences of excessive drinking.4
• Tobacco Use Among Pregnant Women – 15.9% of pregnant women reported to have smoked cigarettes in the past month, based on 2011 and 2012 data.5 The Task Force therefore recommends quitline interventions, especially proactive quitlines where follow-up counseling calls are offered to increase tobacco cessation among clients interested in quitting.6 Mobile phone-based interventions for smoking cessation are also recommended where these interventions use interactive features to deliver evidence-based information, strategies, and behavioral support directly to tobacco users interested in quitting.7
• Weight Loss – Technology-supported multicomponent coaching or counseling interventions intended to reduce or maintain weight are recommended in improving weight-related behaviors or weight-related outcomes. Technology-supported components may include computers, video conferencing, personal digital assistants, pagers, pedometers with computer interaction, or computerized telephone system interventions.8
Promising Practices on Perinatal HealtH – 2013

C-i-3
Other Strategies From Literature Search
1 Recommendations to address alcohol and illicit drug use among prenatal patients:In the investigative report by Child Health Data Lab
of Ann & Robert H. Lurie Children’s Hospital of Chicago, some recommendations have been made on how best to address alcohol and illicit substance use among prenatal patients. Considering the underserved population that the health centers serve and some of the underserved locations, these recommendations are highly valuable.9
• Incorporating a screening tool for misuse or abuse of alcohol, legal medication, illegal drugs and smoking into every prenatal intake and history form. ○ It is identified that quick and brief questionnaires
can be effective in prenatal care for assessing alcohol and drug use.
○ Questions when asked in a health context can lessen the stigma associated with the topic, which also expresses concern for the health of the mother and baby.
○ Treatment for substance abuse during pregnancy is significantly more effective than at other times in a woman’s life.
○ Even if mothers do not disclose the use, many pregnant women reduce their use of drugs or alcohol following supportive advice from a health care professional.
• Finding an approach that is comfortable to the provider and being nonjudgmental and supportive while screening can identify more at-risk prenatal patients.
• Identifying places to refer a patient for further assessment and treatment.
2 Nurse-Family Partnership Program:Nurse-Family Partnership (NFP) is a non-profit organization. The program is derived from an
evidence-based model that partners public health nurses with first-time mothers to empower them to make the right choices in lifestyle to improve pregnancy outcomes; help parents to provide responsible and competent care to improve child health and development; and help parents achieve economic self-sufficiency. The key elements of the model are to enroll first-time, low-income mothers early in their pregnancies; trained public health nurses deliver home-visits over two-and-a-half years; and establish support for the program within an implementing organization.10
In Illinois, NFP was launched in 2000 as an Illinois charity.11 The partnership serves clients in DuPage, Jefferson, Kane, Lake and Marion Counties and in South Chicago. The 2013 Illinois state report identifies client demographics and positive outcomes. Key client demographics were: 87% Medicaid recipients, Median age of 18 years, 68% white, 27% African American, and 49%
Hispanic/Latina. Some of the positive outcomes for clients served by Illinois’ Nurse-Family Partnership are:12
• 92% of babies were born full term and 92% were born at a healthy weight – at or above 5.5 lbs.
• 62% reduction in domestic violence during pregnancy.
• 83% of mothers initiated breast feeding. • 94% of children receive all recommended
immunizations by 24 months.
For those health centers located in the above mentioned counties, local agencies can be contacted; for those health centers who would like to inquire about bringing NFP into their communities, the NFP business development manager can be contacted. To contact, visit www.nursefamilypartnership.org/locations/Illinois.
3Summary from a peer learning conversation on early prenatal care entry:The peer learning call was presented by National
Academy for State Health Policy (NASHP) in collaboration with HRSA in April 2014. The goal was to share promising practices from health centers performing well on creating early access to prenatal care. Health centers featured were Harbor Health Services in Massachusetts, Seattle Indian Health Board in Washington, and other participating health centers.
Designing protocols to facilitate early entry into prenatal care and address the need of pregnant mother.
• Harbor Health Services’ policy ensured that a patient expecting to be pregnant not only met with a provider, but was also started on prenatal vitamins, connected with social and community services, received healthy pregnancy counseling, and received a next appointment. They also created ‘Perinatal Collaborative’ with representatives from the health center’s Women’s Health Department, on-site Women, Infants, and Children (WIC), pediatrics, social services, and behavioral health. The collaborative goal is to meet every month for developing programs and initiatives to improve perinatal care outcomes.
• Seattle Indian Health Board created walk-in, same day appointments for women who might be pregnant. They created ‘Prenatal Thursdays’ and made available providers to see prenatal patients for pregnancy testing and early prenatal visits, including a pharmacist, nutritionist, and breastfeeding educator.
Promising Practices on Perinatal HealtH – 2013

C-i-4
• To address provider and space shortages, one health center started a group prenatal welcome visit prior to the initial exam that included an hour-long health education presentation by a nurse or health educator. Educational materials are distributed on issues such as prenatal appointment schedules, labs, prenatal screening tests, health center’s call system to reach providers, dietary changes, community resources, and relevant state programs.
Utilizing EHR in establishing continuity of care, care coordination, and for monitoring and tracking performance. Although all health centers found the transition to EHR challenging, the benefits over time clearly outweighed the difficulties of transition.13
Additional resources from Illinois State Medical Society on screening pregnant women for alcohol, tobacco and drug use can be found at: www.isms.org/Resources/For_Physicians/Pregnancy/Screening_Pregnant_Women_for_Alcohol,_Tobacco_and_Drug_Use/.
Application To Health Centers
Not all of these strategies can be implemented in all health center settings, nevertheless social determinants of health plays a critical role in perinatal health and must be tackled when possible. Health centers should seek to address social determinants through health education and collaboration with community organizations. Key strategies are:
• A comprehensive approach addressing clinical assessment and health education during the same visit will help those patients who have barriers to frequently access care.
• Culturally and linguistically appropriate women’s health promoter might play a key role in ensuring regular follow-up of prenatal patients.
• Health education tailored to patients background (level of education, socioeconomic status, availability of resources) will help in lowering the chances of low birth weight.
• Connecting early with pregnant women, assessing risk factors, providing tailored education, and connecting with community and social services will help in retention and ensure provision of quality prenatal care.
• Extra effort needs to be taken in health centers to address the racial disparities and geographic differences in illicit substance and alcohol use among prenatal patients.
Erie Family Health Center – Chicago, ILErie serves more than 50,000 patients from 12 sites. Erie is PCMH-accredited and has EHR. According to 2013 UDS data, 94% of its patients belong to racial/ethnic minority group – 78% Hispanic/Latino, 46% African American, 9% Asian. 53% of the patients are best served in a language other than English. 98% of patients are below 200% of Federal Poverty Line. 33% are uninsured. In 2013, Erie saw 3,479 prenatal patients of whom 1,730 were delivered by Erie providers. www.eriefamilyhealth.org.
Rural Health Care, Inc. – Anna, ILRural Health serves close to 12,000 patients from 7 sites. 9.8% of its patients belong to racial/ethnic minority group – 3.3% Hispanic/Latino, 5% African American. Majority of the patients (93.5%) were white. 76.2% of patients were below 200% of Federal Poverty Line. 16.6% were uninsured and 35.9% had Medicaid. In 2013, Rural Health saw 210 prenatal patients of whom 105 delivered. www.ruralhealthinc.org.
Promising Practices on Perinatal HealtH – 2013

C-ii-1
Promising Practices on Perinatal HealtH – 2014
Illinois Health Center Spotlight
1 Heartland Health CentersHeartland Health Centers (HHC) is located in Chicago, Illinois. Over the past few years, Heartland Health
Centers has significantly improved and maintained a high percentage of women receiving prenatal care in the first trimester. Access to prenatal care at HHC increased from 69.9% in 2010 to 84.6% in 2014. In addition, HHC has maintained a low percentage of low birth weight (LBW) performing above the 75th percentile since 2012. The LBW decreased from 4.5% in 2012 to 3.5% in 2013 to 2.8% in 2014. These achievements in improvement can be attributed to the following strategies:
• Patient Tracking and Follow-up: Once patients are identified, they are enrolled in prenatal care immediately. Aggressive follow-up of missed appointment helps ensure good prenatal care. Some of the follow-up methods are:o Obstetrics RN Care Coordinator conducts
education and outreach to patients.o Additional staff were added to schedule
appointments where follow-up is beyond mailing reminders.
• Behavioral Health Integration: To reduce LBW, an integrated care approach identifies prenatal patients with anxiety and depression. o Health center staff work diligently around smoking
cessation among prenatal patients. o Referrals to specialists are tracked to ensure
continuity of care.
2 Christopher Greater Area Rural Health Planning CorporationChristopher Greater Area Rural Health Planning
Corporation is located in Christopher, Illinois. Christopher Rural has significantly improved access to prenatal care performance from 2013 to 2014: access to prenatal rate care increased from 69.6% to 87.2%. In addition, LBW has also significantly reduced from 8.7% in 2013 to 4.7% in 2014 putting it well above the HP 2020 target. Focused strategies include:
• Utilizing a mid-level provider, who is available five days a week to see prenatal patients, has greatly improved access to prenatal care.
• Availability of free pregnancy tests daily at sites and immediate enrollment and referral to provider for patients with a positive pregnancy test.
• Access to a dietitian for prenatal patients. • Continuous tracking by nurses to ensure
appointment scheduling for adequate routine prenatal care:o Prenatal patients are educated on the importance
of keeping appointments.o Nurses also ensure missed appointments are
rescheduled right away.
Task Force Recommendations
The United States Preventive Services Task Force (Task Force) released its recommendation in January 2016 on screening for depression in the general adult population, including pregnant and postpartum women: Screening should be implemented with adequate systems in place to ensure accurate diagnosis, effective treatment, and appropriate follow-up. The recommendation expands on its earlier recommendation of 2009 and broadens the scope by including pregnant and postpartum women. The Task Force also concludes with certainty that there is a moderate net benefit to screening for depression in pregnant and postpartum women who receive care in clinical practices that have cognitive behavioral therapy or other evidence-based counseling available after screening.14
Other Strategies
1 Local Initiatives:a. Preconception, Postpartum and Inter-conceptional
Care Health Communication Toolkit
This toolkit has been developed with funding from Children’s Health Insurance Program Reauthorization Act (CHIPRA) grant. The toolkit has been designed for providers as a resource to help inform their patients. It can be customized to include health center logos and contact information.15
On the next page, there is a table that outlines the content and description of the toolkit.16

C-ii-2
Promising Practices on Perinatal HealtH – 2014Illinois Department of Healthcare and Family Services
CHIPRA Quality Demonstration GrantPerinatal Education Toolkit – Content and Uses
Tools Description Format Suggested Use
For Patients
Health Education and Social Marketing Materials
Directed at women of childbearing age, all of these materials include an image and a clear message on preconception, prenatal, postpartum, and interconception health topics.
Electronic and print-ready. All materials can be reproduced on business cards, flyers, billboards, and posters. The organization’s logo can be easily added to each item.
- Display/distribute posters, brochures, and flyers in waiting rooms, exam rooms, and private consulting areas.- Print educational handouts to reinforce education provided.- Display on billboards, bus ads, or giveaways to raise awareness throughout the community.
Prenatal and Postpartum Checklist Brochures
These brochures are intended to educate women about the importance of prenatal and postpartum care, what to expect at visits, and includes questions women can ask their providers.
Electronic with the ability to add the organization’s logo and print.
- Use to reinforce one-on-one education and patient engagement in care. - Display/distribute in waiting areas.
text4baby Brochure and Poster
These materials are intended to educate women about how to sign up for the free text4baby mobile health information service.
Electronic and print-ready. - Use to supplement one-on-one education and educational materials provided.- Display/distribute in waiting areas, exam rooms, and private consulting areas.- Distribute brochures during prenatal visits.
For Providers
Prenatal Care Quality Tool (Appendix C)
This is a compilation of minimum prenatal care services based on ACOG and IAFP guidelines. The information is organized by visit/trimester and includes clinical services, labs, education, and referrals.
Paper checklist or integration in an electronic health record.
- Use the tool in either format to assure recommended prenatal care services are provided to women at the appropriate times.
High-Risk Referral Crosswalk (Appendix D)
This tool crosswalks ACOG guidance for high-risk referrals with the Illinois Perinatal Code.
Paper or electronic. - Use as a reference guide for assuring that high-risk women are appropriately referred for consultation or higher level care.
Health Education Resources Matrix
This is a comprehensive electronic guide of resources on preconception, prenatal, postpartum and interconception health topics for use by medical and social service providers for educating women of childbearing age on perinatal and well-woman topics. Educational topics align with those on the Prenatal Care Quality Tool.
Electronic access to fact sheets, health information, and websites that provide easy click and print capability. Available here: http://healthychoiceshealthyfutures.org/education-matrix.
- Use for one-on-one patient education.- Use to supplement and reinforce one-on- one education.- Recommend and provide websites for patient self-education.
Postpartum Visit and Perinatal Care Transitions
The HFS Provider Notice dated September 29, 2015 shares best practices for perinatal care transitions.
Paper or electronic. - Use the best practices checklist to assess performance and identify gaps.Paper or electronic. - Use the best practices checklist to assess performance and identify gaps.- Incorporate applicable best practices into the workflow and adopt as policy.- Use the Quick Reference tool to assist in identifying the patient’s PCP
Postpartum Transition Strategies (Appendix E)
Proposed strategies for consideration by providers who have contact with women at various points during the perinatal period, including prenatal providers (obstetricians, family physicians, APNs), hospital labor and delivery units, and pediatricians. The strategies are intended to increase the number of women who receive postpartum services.
Electronic. - Implement one or more of the strategies by incorporating into the work flow and adopting as policy.- Use the proposed strategies as a springboard to explore other ways to increase the number of women who receive postpartum services.

C-ii-3
Promising Practices on Perinatal HealtH – 2014b. Illinois Perinatal Quality Collaborative
The Illinois Perinatal Quality Collaborative (ILPQC) was formed in late 2012, with support from Illinois CHIPRA Quality Demonstration grant and March of Dimes, by the coming together of Perinatal Quality Collaborative of Illinois (PQCI), a neonatology-focused collaborative and obstetric quality improvement leadership to form a statewide quality collaborative that would work closely with the Illinois Regionalized Perinatal System (RPS) on both obstetric and neonatal quality improvement initiatives. It is an ongoing collaborative that is seeking perinatal health-related providers for their participation in their Obstetrics, Neonatal and Data Advisory Workgroups. More information can be found at http://ilpqc.org/node/40.
2 National Initiatives: Perinatal Quality CollaborativesState perinatal quality collaboratives (PQCs) are
networks of perinatal care providers and public health professionals working to improve pregnancy outcome for women and newborns by advancing evidence-based clinical practices and processes through continuous quality improvement (CQI). PQC members identify care processes that need to be improved and use the best available methods to make changes and improve outcomes. State PQCs include key leaders in private, public, and academic health care settings with expertise in evidence-based obstetric and neonatal care and quality improvement. Some available resources are:
a. Ohio PQC Quality Improvement Resources https://opqc.net/projects/improvement%20resources
b. Improving Health Care Response to Preeclampsia: A California Quality Improvement Toolkit17 – This is an extensive toolkit covering a series of articles on best practices for hypertensive disorders that range in topic from diagnostic challenges to appropriate implementation of accepted medical therapy and recognition of institutional limitations in providing care for these complex maternal patients.
CMQCC PREECLAMPSIA TOOLKIT PREECLAMPSIA CARE GUIDELINES
CDPH-MCAH Approved: 12/20/13
31
PREECLAMPSIA EARLY RECOGNITION TOOL (PERT)
Adapted from the Modified Obstetric Early Warning System (MEOWS) in “Saving Mothers Lives: Reviewing maternal deaths to make motherhood safer (2003-2005). The Seventh Report of the Confidential Enquiries into Maternal Deaths in the United Kingdom 2007
11.8.13.v1
YELLOW = WORRISOME Increase assessment frequency
#Triggers TO DO
1 •Notify provider ≥2 •Notify charge RN
•In-person evaluation •Order labs/tests •Anesthesia consult •Consider magnesium sulfate •Supplemental oxygen
**Physician should be made aware of worsening or new-onset proteinuria
Preeclampsia Early Recognition Tool (PERT)
ASSESSNORMAL(GREEN)
WORRISOME (YELLOW)
SEVERE(RED)
Awareness Alert/oriented• Agitated/confused • Drowsy • Difficulty speaking
• Unresponsive
Headache None • Mild headache • Nausea, vomiting • Unrelieved headache
Vision None • Blurred or impaired • Temporary blindness
Systolic BP(mm HG) 100-139 140-159 ≥160
Diastolic BP (mm HG) 50-89 90-105 ≥105
HR 61-110 111-129 ≥130
Respiration 11-24 25-30 <10 or >30 SOB Absent Present Present
O2 Sat (%) ≥95 91-94 ≤90
Pain: Abdomen or Chest None
• Nausea, vomiting •Chest pain•Abdominal pain
• Nausea, vomiting •Chest pain• Abdominal pain
Fetal Signs • Category I • Reactive NST
• Category II • IUGR • Non-reactive NST
• Category III
Urine Output (ml/hr) ≥50 30-49 ≤30 (in 2 hrs)
Proteinuria(Level of proteinuria is not an accurate predictor of pregnancy outcome)
Trace • > +1** • 300mg/24 hours
Platelets >100 50-100 <50AST/ALT <70 >70 >70
Creatinine <0.8 0.9-1.1 >1.2MagnesiumSulfate Toxicity
• DTR +1 • Respiration 16-20 • Depression of patellar reflexes • Respiration <12
= WORR
GREEN = NORMAL Proceed with protocol
RED = SEVERE Trigger: 1 of any type listed below TO DO
1 of any type • Immediate evaluation • Transfer to higher acuity level • 1:1 staff ratio
Awareness Headache Visual
• Consider Neurology consult • CT Scan • R/O SAH/intracranial hemorrhage
BP
• Labetalol/hydralazine in 30 min • In-person evaluation • Magnesium sulfate loading or
maintenance infusion Chest Pain • Consider CT angiogram Respiration SOBO2 SAT
• O2 at 10 L per rebreather mask • R/O pulmonary edema • Chest x-ray
•Respiration <12
One of the tools, Preeclampsia Early Recognition Tool:
Quality Improvement Strategies
1 Heartland Health Centers – Chicago, IL• HHC has implemented a health information
exchange with a hospital that allows real-time data exchange on labs, discharges and notes from ER.
• E-prescribing and medication reconciliation are carried out.
• HHC participated in a 12 month Institute for Healthcare Improvement (IHI) learning collaborative, which included weekly meetings to satisfy deliverables. IHI also provided the structure to collect data and provided access to external resources and tools. Best practices were also shared as part of this learning collabrotive.

C-ii-4
• HHC has created two different kinds of roles: o Integrated Care Specialist – works with Medical
Home Network (MHN) Connect. They work on patients discharged from hospital and emergency rooms (ER) and look at preventive care measures to facilitate follow-up for diabetes, colon cancer, Hepatitis C and cervical cancer screening. In addition, care specialists receive a list of patients and preventive care measures from Illinois Health Connect and other insurers.
o Referral Specialist – works with provider-identified referrals. They aid in navigating managed care for their patients and identifying specialists.
2 Christopher Greater Area Rural Health Planning Corporation – Christopher, IL• Continuous tracking by nurses to ensure
appointments are scheduled for adequate routine prenatal care. Nurses also ensure missed appointments are rescheduled right away.
• Patient Care Coordinators track the Illinois Health Connect roster to bring in patients due for preventive screenings.
Promising Practices on Perinatal HealtH – 2014

C-R
1. Health Resources and Services Administration. Facilitating Early Prenatal Care Entry. Retrieved on 5/13/2014. http://bphc.hrsa.gov/spotlight/eriefamilyhc/.
2. Child Health Data Lab. Injuries to Illinois and Chicago Youth: Alcohol and Illicit Drugs in Newborns. Stanley Manne Children’s Research Institute. State and Community Reports on Injury Prevalence and Targeted Solutions (SCRIPTS). Issue 11, July 2014.
3. Substance Abuse and Mental Health Services Administration. The National Survey on Drug Use and Health Report: 18 percent of pregnant women drink alcohol during early pregnancy. Sep 9 2013. Accessed from: www.samhsa.gov/data/spotlight/spot123-pregnancy-alcohol-2013.pdf.
4. Guide to Community Preventive Services. Preventing excessive alcohol consumption: electronic screening and brief intervention (e-SBI). Accessed from: www.thecommunityguide.org/alcohol/eSBI.html.
5. Substance Abuse and Mental Health Services Administration. Results from the 2012 National Survey on Drug Use and Health: Summary of National Findings. Accessed from: www.samhsa.gov/data/nsduh/2012summnatfinddettables/nationalfindings/nsduhresults2012.htm#ch4.3.
6. Guide to Community Preventive Services. Reducing tobacco use and secondhand smoke exposure: quitline interventions. Accessed from: www.thecommunityguide.org/tobacco/quitlines.html.
7. Guide to Community Preventive Services. Reducing tobacco use and secondhand smoke exposure: mobile phone-based cessation interventions. Accessible from: www.thecommunityguide.org/tobacco/mobilephone.html
8. Guide to Community Preventive Services. Obesity prevention and control: technology-supported multicomponent coaching or counseling interventions to reduce weight and maintain weight loss. Accessible from: www.thecommunityguide.org/obesity/TechnologicalCoaching.html.
9. Child Health Data Lab. Injuries to Illinois and Chicago Youth: Alcohol and Illicit Drugs in Newborns. Stanley Manne Children’s Research Institute. State and Community Reports on Injury Prevalence and Targeted Solutions (SCRIPTS). Issue 11, July 2014.
10. Nurse-Family Partnership, helping first-time parents succeed. Accessed from: www.nursefamilypartnership.org/about/what-we-do.
11. Nurse-Family Partnership, helping first-time parents succeed. Nurse-Family Partnership of Illinois Accessed from: www.nursefamilypartnership.org/locations/Illinois.
12. Nurse-Family Partnership, helping first-time parents succeed. State profile 2013: Nurse-Family Partnership in Illinois. Accessed from: www.nursefamilypartnership.org/assets/PDF/Communities/State-profiles/IL_State_Profile.
13. National Academy for State Health Policy. Creating change in early prenatal care entry: a peer learning conversation April 9, 2014. Accessible from: http://bphc.hrsa.gov/technicalassistance/trainings/creatingchangeearlyprenatalcare.pdf.
14. Final Recommendation Statement: Depression in Adults: Screening. U.S. Preventive Services Task Force. January 2016. www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/depression-in-adults-screening1
15. Healthy Choices Healthy Futures – Perinatal Health Toolkit. September 2015. Accessed from: http://healthychoiceshealthyfutures.org/
16. Reprinted with permission from IL CHIPRA Quality Demonstration Grant.17. Maurice L. Druzin, MD; Laurence E. Shields, MD; Nancy L. Peterson, RNC, PNNP, MSN; Valerie Cape, BSBA.
Preeclampsia Toolkit: Improving Health Care Response to Preeclampsia (California Maternal Quality Care Collaborative Toolkit to Transform Maternity Care) Developed under contract #11-10006 with the California Department of Public Health; Maternal, Child and Adolescent Health Division; Published by the California Maternal Quality Care Collaborative, November 2013. Accessible from: http://ilpqc.org/docs/htc/CDPH_Approved_Preeclampsia_Toolkit__Errata_v3.5.13.14_with_slideset.pdf
Promising Practices – references

C-1
Qi & system-level strategies
Resources for System-Level Strategies
1Enhancing Quality Improvement Approach a.HITEQ Collaboration Health Information Technology, Evaluation and
Quality Center (HITEQ) is a HRSA-funded National Cooperative Agreement that collaborates with HRSA partners including Health Center Controlled Networks, Primary Care Associations, and other National Cooperative Agreements to support health centers in full optimization of their EHR/Health IT systems.
IPHCA collaborated with HITEQ to provide 11 health centers with Health IT/Quality Improvement (QI) through strategies and tools discussed in learning sessions. These learning sessions were based on the QI approach outlined in the “Guide to Improving Care Processes and Outcomes in Health Centers.” The approach provides a framework as well as tools to enhance current QI approaches or use as the basis of a new QI approach. HITEQ leader Jillian Maccini conducted four monthly online learning sessions with health centers from February through May 2017 that involved the following:
• Move toward optimal care delivery through care transformation supported by Health IT-enabled QI.
• Reinforce organizational foundations for QI with tools for engaging stakeholders and validating data.
• Select QI targets using health IT-informed data, current outcomes, and prioritization tools.
• Use comprehensive CDS/QI worksheet to document and analyze
This learning collaborative culminated in a final in-person session that took place in Springfield, IL on June 6, 2017. At this session, health centers were able to present and showcase their targeted QI project and the progress they had made thus far. Throughout the collaborative, HITEQ resources and tools were provided to participants and can be found in Appendix B.
2Care Coordination a. Toolkit for Coordinating Care “Reducing Care Fragmentation: A Toolkit
for Coordinating Care” was developed by Group Health’s MacColl Institute for Healthcare Innovation and support by The Commonwealth Fund. This toolkit was designed to improve care coordination by enhancing patient referrals and transitions at clinics, practices, and health systems. The toolkit includes a Care Coordination Model as well as six key changes to support the model with resources to help facilitate change:
1. Decide as a primary care clinic to improve care coordination
2. Develop a tracking system3. Organize a practice team to support patients and
families4. Identify, develop, and maintain relationships
with key specialist groups, hospitals, and community agencies
5. Develop agreements with these key groups6. Develop and implement information transfer
system The complete toolkit can be accessed from http://www.improvingchroniccare.org/downloads/reducing_care_fragmentation.pdf.
b. Team-Based Care The Primary Care Team Guide was developed by a national program of the Robert Wood Johnson Foundation called “The Primary Care Team: Learning from Effective Ambulatory Practices” – also known as “LEAP.” The Guide provides a number of resources to engage the health care team in patient-centered care and build the care team to be more effective. The guide provides tools to improve teamwork, expand roles of health care professionals, and improve efficiency in primary care practices.
The first section of the Primary Care Team Guide is composed of “Build the Team” learning modules which provide the roles and responsibilities of each primary care team in order to make up an effective team. The “Do the Work” learning modules describe the necessary functions needed for high-performing primary care practices. The learning modules under “Do the Work” highlight taking on the following functions to improve the primary care practice:
• Improving Care Through Teamwork• Enhancing Access• Self-Management Support• Population Management• Planned Care• Care Management• Medication Management• Referral Management• Behavioral Health Integration• Communication Management • Clinic-Community Connections
All learning modules include assessments, action steps to implement, and useful resources and tools in order to achieve team-based care.
• “Build the Team” learning modules can be accessed from: http://www.improvingprimarycare.org/team
• “Do the Work” learning modules can be accessed from: http://www.improvingprimarycare.org/work

C-2
3 Patient and Family Engagement a. 6 Step Toolkit Patient-Centered Primary Care Collaborative Support
worked in collaboration with Planetree International and Alignment Network, with support from the Institute for Patient and Family-Centered Care (IPFCC) to develop a toolkit called “6 Steps to Creating a Culture of Person and Family Engagement.” This toolkit provides practices with strategies to improving person and family engagement through creating a culture in the practice that emphasizes patient and family perspectives in order to improve quality of care. The six steps detailed in the toolkit include:
1. Engage Leaders2. Empower and Energize Staff3. Equip, Enable and Support Patients to Engage4. Enlist Patients and Families as Partners5. Encourage Family Participation in Care6. Emphasize Patient and Family Engagement in All
You Do
Further details on these six steps can be found in Appendix G along with a 30 Day Kick-Start Plan to take action on these steps.
b. Improving Patient Safety Guide The Agency for Healthcare Research and Quality (AHRQ) is developing “The Guide to Improving Patient Safety in Primary Care Settings by Engaging Patients and Families” to help health professionals in primary care work together with patients and families in order to promote stronger engagement and improve care. The final guide will be released in early 2018, however four strategies with supporting materials have already been provided by AHRQ:
• Teach-Back: Health care providers can use this technique to ensure they have explained medical information clearly to patient and family and also understand what is communicated to them.
• ‘Be Prepared to Be Engaged’: This toolkit is to help patients and their families prepare for the medical appointment and become fully engaged by being ready for the appointment, speaking up, asking questions, and taking notes.
• Medication Management: These tools will help health care professionals engage with patients and caregivers to create a complete and accurate medication list using the ‘brown bag method.’ This will also help to identify risks of an adverse drug event or other factors that limit adherence.
• Warm Handoff: This strategy allows a transfer of care between two members of the health care team in front of the patient and family. This allows the patient and their family to hear what is said and engages them in communication – which gives them the opportunity to clarify information or ask questions.
Supporting material for each strategy can be accessed at:
https://www.ahrq.gov/professionals/quality-patient-safety/patient-family-engagement/pfeprimarycare/interventions/index.html
c. Improving Self-Management Goals On April 6, 2017 The Joint Commission hosted a teleconference around ‘Health Literacy and Self-Management Goals Made Simple.’ This recording is archived and can be streamed from https://www.jointcommission.org/hrsa_grantee_technical_assistance_teleconference_list/. In addition, The Joint Commission has shared the following tools (Appendix D) to aid in improving health literacy and self-management goals.
• Health Literacy Assessment Tool – This resource provides multiple sample screening tools for health literacy.
• Handout on Self-Management Goals – This tool, available in English and Spanish, helps patients set their own self-management goals to improve health behaviors.
• Bookmark for Goals – This bookmark helps patients set goals and easily mark off
4 Improving Preventive Screeningsb. Proactive Office Encounter Intervention The University of Kentucky collaborated with a
federally qualified health center (FQHC) known as White House Clinics (WHC) that serves over 30,500 patients in a rural, medically underserved, and economically stressed population in Appalachian Kentucky. In order to ensure patients are up-to-date with preventive screenings, the collaboration launched the Proactive Office Encounter (POE) intervention. This system-level approach aims to provide a preventive health assessment in addition to the actual office visit purpose. POE provides medically tailored and evidence-based protocol for each patient with the following process:
• Pre-encounter > Reviewing patient’s EMR for cancer screening completion; creating summary of patients recent screening history and socio-demographics; allowing provider to address health needs; and ordering referrals to the visit.
• Appointment > More time with provider for shared-decision making and encouraging patient for recommended cancer screenings.
• Post-encounter > Track patients’ screening completion
The POE procedures were also integrated into the EMR system to include care guidelines templates and reports to identify gaps in preventive care. The POE model was launched at 4 out of 8 WHC clinics in January 2015. As of December 2015, UDS measures indicate an increase in breast and CRC, HIV, and HCV screenings. In addition, influenza, pneumonia, and shingles vaccination rates have increased. Between 2014 and 2015, WHC had a 36% increase in CRC screenings; five times the number of HIV screenings (831 vs. 4,371) and eight times the number of HCV screenings (378 vs. 3,334).
Qi & system-level strategies

C-3
HealtH center information – 2014
Heartland Health Centers – Chicago, ILHeartland Health Centers (HHC) has 15 locations and served 26,096 patients according to UDS 2014 data. Heartland is PCMH certified through The Joint Commission and has EHR. In 2015, it was awarded the Health Center Quality Leader award from HRSA and it is also a part of the Million Hearts Initiative. Age distribution of the patient population includes: 26.7% children, 69.8% adults, and 3.5% older adults (age 65 and over). A majority (70.1%) of the patients belong to a racial and/or ethnic minority: 36.2% Hispanic/Latino, 25.5% African American, and 7.7% Asian. 94.6% of patients lived at or below 200% of the poverty level in 2014. 36.3% of patients were uninsured and 18.8% of children were uninsured. 40.5% of patients were on Medicaid/CHIP. 75.7% of the female patient population was in the 15-64 year age group. The number of prenatal patients in 2014 was 481 and the number of patients who delivered was 249.www.heartlandhealthcenters.org
Christopher Greater Area Rural Health Planning Corporation – Christopher, ILChristopher Greater Area Rural Health Planning Corporation (CRHPC) served 45,387 patients from its 17 locations in 2014. CRHPC is PCMH recognized and has EHR. Age distribution of its patients includes: 32.5% children, 52.6% adults, and 14.8% older adults. The majority (92.9%) of the patient population was white and 7.1% belong to a racial and/or ethnic minority. In 2014, 85.9% of patients lived at or below 200% of the poverty level. 14.0% of the patient population was uninsured in 2014. 38.0% of patients were on Medicaid/CHIP, 16.6% had Medicare, and 31.4% had different third party insurance. The number of prenatal patients in 2014 was 265 and the number of patients who delivered was 193.www.crhpc.org

APP-A-1
aPPendix a – HealtH center stratification by number of Patients served - 2014
Health Centers Serving <5,000 Patients
Health Center Name Number of Sites Total Patient Population
Hamdard Center for Health & Human Services 2 783
Preferred Family Health Care, Inc. (MO) 2 1,505
Chestnut Health Systems 1 1,659
Beloved Community Family Wellness Center 3 3,152
Community Nurse Health Center 4 3,908
Knox County Health Department 1 3,938
Cass County Health Department 2 4,097
Macoupin County Public Health Department 2 4,539
Health Centers Serving 5,000 to < 10,000 Patients
Health Center Name Number of Sites Total Patient Population
Eagle View Community Health System 2 5,623
TCA Health Inc. – NFP 2 6,965
Heartland Health Outreach, Inc. 55 7,661
Asian Human Services Family Health Center, Inc. 3 9,303
Community Health Partnership of Illinois 5 9,717
Health Centers Serving 10,000 to < 20,000 Patients
Health Center Name Number of Sites Total Patient Population
Rural Health, Inc. 5 10,972
Whiteside County Community Health Clinic 1 12,478
Christian Community Health Center 6 12,569
SIU Center for Family Medicine 1 13,040
Will County Community Health Center 2 14,103
Central Counties Health Centers, Inc. 3 15,443
Community Health Centers of Southeastern Iowa, Inc. (IA) 4 16,163
Heartland Community Health Clinic 5 17,207
Esperanza Health Centers 4 17,241

APP-A-2
Health Centers Serving 20,000 to < 40,000 Patients
Health Center Name Number of Sites Total Patient Population
PrimeCare Community Health, Inc. 5 20,374
Family Christian Health Center 2 21,234
Crossing Healthcare 9 21,633
Alivio Medical Center 7 23,302
Heartland Health Centers 15 26,096
Friend Family Health Center, Inc. 5 27,197
Chicago Family Health Center, Inc. 5 30,235
Shawnee Health Service 11 30,351
Mile Square Health Center 13 30,585
Near North Health Service Corporation 9 34,076
Community Health Care, Inc. (IA) 12 35,305
Greater Elgin Family Care Center 28 37,590
Lake County Health Department/CHC 7 39,155
Health Centers Serving ≥ 40,000 Patients
Health Center Name Number of Sites Total Patient Population
Christopher Rural Area Health Planning Corporation 17 45,387
Lawndale Christian Health Center 7 45,570
PCC Community Wellness Center 13 47,418
Crusader Community Health 14 47,787
Aunt Martha’s Youth Service Center, Inc. 31 56,802
VNA Health Care 13 59,901
Erie Family Health Center, Inc. 13 61,860
Southern Illinois Healthcare Foundation, Inc. 35 106,054
Access Community Health Network 35 176,389
aPPendix a – HealtH center stratification by number of Patients served - 2014

APP-A-3
aPPendix a – HealtH center stratification by number of Patients served – 2015
Health Centers Serving <5,000 Patients
Health Center Name Number of Sites Total Patient Population
Hamdard Center For Health & Human Services 2 1,654
Chestnut Health Systems 2 2,010
Preferred Family Healthcare Inc. (MO) 3 3,246
Beloved Community Family Wellness Center 2 3,727
Community Nurse Health Center 2 4,187
Cass County Health Department 2 4,297
Knox County Health Department 1 4,721
Macoupin County Public Health Department 2 4,885
Health Centers Serving 5,000 to < 10,000 Patients
Health Center Name Number of Sites Total Patient Population
Eagle View Community Health System 2 5,018
TCA Health Inc. – NFP 3 7,049
Heartland Health Outreach, Inc. 3 8,972
Asian Human Services Family Health Center, Inc.
4 10,119
Community Health Partnership of Illinois 8 10,981
Health Centers Serving 10,000 to < 20,000 Patients
Health Center Name Number of Sites Total Patient Population
Whiteside County Health Department 2 12,545
Rural Health, Inc. 5 12,652
Will County Community Health Center 2 12,887
Central Counties Health Centers, Inc. 3 13,649
Christian Community Health Center 4 13,398
Community Health Centers of Southeastern Iowa, Inc. (IA)
4 17,459
Heartland Community Health Clinic 5 17,656
Esperanza Health Centers 3 18,517
SIU Center for Family Medicine 1 20,116

APP-A-4
Health Centers Serving 20,000 to < 40,000 Patients
Health Center Name Number of Sites Total Patient Population
Family Christian Health Center 2 20,824
PrimeCare Community Health, Inc. 8 21,091
Alivio Medical Center 6 23,021
Crossing Healthcare 7 25,982
Heartland Health Centers 16 29,609
Shawnee Health Service 12 30,175
Chicago Family Health Center, Inc. 5 30,318
Friend Family Health Center, Inc. 7 30,706
Community Health Care, Inc. (IA) 9 33,095
Near North Health Service Corporation 9 34,736
Mile Square Health Center 12 37,717
Greater Elgin Family Care Center 26 40,666
Lake County Health Department 10 40,322
Health Centers Serving ≥ 40,000 Patients
Health Center Name Number of Sites Total Patient Population
Christopher Rural Health Planning Corporation 11 43,203
PCC Community Wellness Center 12 47,184
Crusader Community Health 6 48,234
Lawndale Christian Health Center 15 49,141
Aunt Martha’s Youth Service Center, Inc. 17 49,746
VNA Health Care 10 61,717
Erie Family Health Center, Inc. 13 68,417
Southern Illinois Healthcare Foundation, Inc. 26 101,624
Access Community Health Network 36 180,981
aPPendix a – HealtH center stratification by number of Patients served – 2015

APP-B-1
aPPendix b – Prenatal care Quality tool
Pren
atal
Car
e Q
ualit
y To
ol C
heck
list
This
doc
umen
t was
dev
elop
ed u
nder
gra
nt C
FDA
93.
767
from
the
U.S
. Dep
t. of
Hea
lth a
nd H
uman
Ser
vice
s, C
ente
rs fo
r Med
icar
e &
Med
icai
d S
ervi
ces.
H
owev
er, t
hese
con
tent
do
not n
eces
saril
y re
pres
ent
the
polic
y of
the
U.S
. Dep
t. of
Hea
lth a
nd H
uman
Ser
vice
s, a
nd s
houl
d no
t ass
ume
endo
rsem
ent b
y th
e Fe
dera
l gov
ernm
ent.
Dat
e: _
____
____
____
____
__
____
Trim
este
r
X La
bs
U
rine
anal
ysis
/cul
ture
Pap
Tes
t as
clin
ical
ly
indi
cate
d
GC
/Chl
amyd
ia
C
BC
Ant
ibod
y sc
reen
Blo
od T
ype
R
h Ty
pe
R
ubel
la
R
PR
Hep
atiti
s B
H
IV
H
emog
lobi
n el
ectro
phor
esis
if
indi
cate
d (1
)
Ear
ly s
cree
ning
for
Dia
bete
s if
risk
fact
ors
(3)
U
ltras
ound
if L
MP
is
unkn
own
or u
ncer
tain
or
if n
ot c
onsi
sten
t with
ex
am
O
ffer a
neup
loid
y sc
reen
ing
(ser
um)
and/
or N
IPS
(non
-in
vasi
ve p
rena
tal
scre
enin
g; m
ater
nal
seru
m c
ell-f
ree
feta
l D
NA
) and
/or
diag
nost
ic te
stin
g (a
mni
o/C
VS)
X C
linic
al E
lem
ents
His
tory
(inc
ludi
ng
med
icat
ions
/ sup
plem
ents
, fa
mily
or p
erso
nal h
isto
ry
of g
enet
ic d
isor
ders
) P
hysi
cal E
xam
inat
ion
(incl
udin
g br
east
and
pel
vic
exam
)
Cou
nsel
and
offe
r gen
etic
an
d an
eupl
oidy
sc
reen
ing/
diag
nost
ic
optio
ns a
ppro
pria
te to
the
patie
nt
H
t/Wt,
BP,
BM
I
Scr
een
for i
llici
t su
bsta
nces
, alc
ohol
and
to
bacc
o
Scr
een
for i
mm
uniz
atio
ns
Offe
r inf
luen
za v
acci
ne
durin
g flu
sea
son
(Sep
t-M
ay)
S
cree
n fo
r pre
term
labo
r ris
k fa
ctor
s: in
par
ticul
ar
prio
r pre
term
del
iver
y,
mul
tiple
ges
tatio
n, u
terin
e an
omal
ies,
sho
rt ce
rvix
Dom
estic
vio
lenc
e sc
reen
Scr
een
for p
erin
atal
men
tal
heal
th d
isor
ders
(e.g
. de
pres
sion
) (4)
X Ed
ucat
ion
P
rovi
der c
onta
ct/e
mer
genc
y nu
mbe
rs/h
ospi
tal i
nfor
mat
ion
Ant
icip
ated
cou
rse
of p
erin
atal
car
e
War
ning
sig
ns o
f mis
carr
iage
Nut
ritio
n in
pre
gnan
cy
A
ppro
pria
te w
eigh
t gai
n in
pr
egna
ncy
P
hysi
cal a
ctiv
ity in
pre
gnan
cy
Li
fest
yle
educ
atio
n: w
ork,
sex
ual
activ
ity a
nd tr
avel
Pre
nata
l vita
min
s/fo
lic a
cid
supp
lem
enta
tion
M
edic
atio
n av
oida
nce
- pr
escr
iptio
n an
d ov
er th
e co
unte
r/ su
pple
men
ts a
nd v
itam
ins
P
reca
utio
ns -
caffe
ine/
to
xopl
asm
osis
/Lis
teria
/fish
/ V
aric
ella
/hot
tub/
en
viro
nmen
tal/o
ccup
atio
nal
S
ubst
ance
Use
/ Alc
ohol
/Tob
acco
C
essa
tion-
5 A
's (2
)
Sea
tbel
ts/ S
mok
e de
tect
ors/
Gun
sa
fety
in h
ome
R
evie
w s
tress
fact
ors
D
iscu
ss s
igns
of p
reec
lam
psia
if >
20
wks
ges
tatio
n
Pro
vide
info
rmat
ion
on c
hild
birth
an
d br
east
feed
ing
clas
ses
V
BA
C c
ouns
elin
g if
appr
opria
te
B
reas
t fee
ding
ben
efits
Sel
ectio
n of
a h
ealth
care
pro
vide
r or
med
ical
hom
e fo
r the
new
born
Cou
nsel
ing
for H
IV te
stin
g
X R
efer
rals
Ref
erra
l to
WIC
Ref
erra
l to
Fam
ily C
ase
Man
agem
ent
Pro
vide
info
rmat
ion
on c
hild
birth
cl
asse
s
Pro
vide
info
rmat
ion
on
brea
stfe
edin
g cl
asse
s
X H
igh-
Ris
k R
efer
rals
Hig
h-R
isk
cond
ition
iden
tifie
d?
Rea
son:
___
____
____
____
____
__
R
efer
ral t
o m
enta
l hea
lth
prof
essi
onal
or s
ocia
l wor
ker i
f in
dica
ted
R
efer
ral t
o O
B o
r MFM
if in
dica
ted
1.
Med
iterr
anea
n, S
outh
east
Asi
an, o
r Af
rican
Am
eric
an d
esce
nt
2.
5 A’
s –
Ask,
Adv
ice,
Ass
ess,
Ass
ist,
Arra
nge
follo
w-u
p 3.
O
besi
ty (B
MI>
30),
stro
ng fa
mily
his
tory
of
dia
bete
s, p
rior G
DM
or d
eliv
ered
in
fant
>9l
bs, g
lyco
suria
, or k
now
n im
paire
d gl
ucos
e m
etab
olis
m
4.
HFS
app
rove
d as
sess
men
ts: E
dinb
urg
Post
nata
l Dep
ress
ion
Scal
e, B
eck
Dep
ress
ion
Inve
ntor
y, P
rimar
y C
are
Eval
uatio
n of
Men
tal D
isor
ders
Pat
ient
H
ealth
Que
stio
nnai
re (P
HQ
9), P
ost-
partu
m D
epre
ssio
n Sc
reen
ing
Scal
e,
Cen
ter f
or E
pide
mio
logi
c St
udie
s D
epre
ssio
n Sc
ale.
1st P
rena
tal V
isit,
Reg
ardl
ess
of G
esta
tiona
l Age
Plac
e pa
tient
stic
ker h
ere.

APP-B-2
aPPendix b – Prenatal care Quality tool
Pren
atal
Car
e Q
ualit
y To
ol C
heck
list
This
doc
umen
t was
dev
elop
ed u
nder
gra
nt C
FDA
93.
767
from
the
U.S
. Dep
t. of
Hea
lth a
nd H
uman
Ser
vice
s, C
ente
rs fo
r Med
icar
e &
Med
icai
d S
ervi
ces.
H
owev
er, t
hese
con
tent
do
not n
eces
saril
y re
pres
ent
the
polic
y of
the
U.S
. Dep
t. of
Hea
lth a
nd H
uman
Ser
vice
s, a
nd s
houl
d no
t ass
ume
endo
rsem
ent b
y th
e Fe
dera
l gov
ernm
ent.
Dat
e: _
____
____
____
____
__
X C
linic
al E
lem
ents
Vis
it fre
quen
cy s
houl
d be
eve
ry
4 w
ks
W
t, B
P at
eve
ry v
isit
In
fluen
za v
acci
ne o
ffere
d du
ring
flu s
easo
n if
not p
revi
ousl
y gi
ven
(Sep
t-May
)
X La
bs
U
rine
dip
for
prot
ein/
gluc
ose
X R
efer
rals
Ref
erra
l to
WIC
Ref
erra
l to
Fam
ily C
ase
Man
agem
ent
X H
igh-
Ris
k R
efer
rals
Hig
h-R
isk
cond
ition
iden
tifie
d?
Rea
son:
____
____
____
____
___
R
efer
ral t
o m
enta
l hea
lth
prof
essi
onal
or s
ocia
l wor
ker i
f in
dica
ted
R
efer
ral t
o O
B o
r MFM
if
indi
cate
d
X Ed
ucat
ion
R
evie
w o
f abn
orm
al la
b re
sults
17-a
lpha
Hyd
roxy
prog
este
rone
ca
proa
te fo
r pat
ient
s w
ith
hist
ory
of p
rete
rm b
irth
due
to
pret
erm
labo
r or P
PR
OM
to
begi
n at
16
wee
ks
1st T
rimes
ter,
1-12
Wee
ks (i
n ad
ditio
n to
firs
t pre
nata
l vis
it)
Plac
e pa
tient
stic
ker h
ere.

APP-B-3
aPPendix b – Prenatal care Quality tool
Pren
atal
Car
e Q
ualit
y To
ol C
heck
list
This
doc
umen
t was
dev
elop
ed u
nder
gra
nt C
FDA
93.
767
from
the
U.S
. Dep
t. of
Hea
lth a
nd H
uman
Ser
vice
s, C
ente
rs fo
r Med
icar
e &
Med
icai
d S
ervi
ces.
H
owev
er, t
hese
con
tent
do
not n
eces
saril
y re
pres
ent
the
polic
y of
the
U.S
. Dep
t. of
Hea
lth a
nd H
uman
Ser
vice
s, a
nd s
houl
d no
t ass
ume
endo
rsem
ent b
y th
e Fe
dera
l gov
ernm
ent.
Dat
e: _
____
____
____
____
___
X Ed
ucat
ion
S
igns
and
sym
ptom
s of
pr
eter
m la
bor
A
war
enes
s of
feta
l m
ovem
ent/
teac
h ki
ck c
ount
s
Rev
iew
lab
resu
lts if
ne
cess
ary
B
reas
tfeed
ing
rein
forc
emen
t at
eve
ry v
isit
R
evie
w s
igns
of
pree
clam
psia
Offe
r chi
ldbi
rth a
nd
brea
stfe
edin
g cl
asse
s
P
ostp
artu
m b
irth
cont
rol p
lan
(sig
n co
nsen
t for
tuba
l lig
atio
n af
ter 2
0 w
eeks
if
indi
cate
d)
X La
bs
U
rine
dip
for
prot
ein/
gluc
ose
D
iabe
tic s
cree
n be
twee
n 24
-28
wee
ks w
ith 1
hou
r G
TT (5
0 gm
glu
cose
lo
ad)
C
BC
bet
wee
n 24
-28
wee
ks
O
ffer u
ltras
ound
for
stru
ctur
e an
d da
ting
at
18-2
0 w
eeks
X C
linic
al E
lem
ents
Vis
it fre
quen
cy s
houl
d be
ev
ery
4 w
ks u
nles
s m
ore
frequ
ent v
isits
are
clin
ical
ly
indi
cate
d
Wt,
BP,
Fun
dal h
eigh
t at
ever
y vi
sit
Fe
tal h
eart
tone
s at
eve
ry v
isit
17
-alp
ha
Hyd
roxy
prog
este
rone
ca
proa
te to
beg
in a
t 16
wee
ks, i
f clin
ical
ly in
dica
ted
X R
efer
rals
Ref
erra
l to
WIC
Ref
erra
l to
Fam
ily C
ase
Man
agem
ent
X H
igh-
Ris
k R
efer
rals
Hig
h-R
isk
cond
ition
iden
tifie
d?
Rea
son:
____
____
____
____
____
_
Ref
erra
l to
men
tal h
ealth
pr
ofes
sion
al o
r soc
ial w
orke
r if
indi
cate
d
Ref
erra
l to
OB
or M
FM if
indi
cate
d
2nd T
rimes
ter,
12-2
8 W
eeks
Plac
e pa
tient
stic
ker h
ere.

APP-B-4
aPPendix b – Prenatal care Quality tool
Pren
atal
Car
e Q
ualit
y To
ol C
heck
list
This
doc
umen
t was
dev
elop
ed u
nder
gra
nt C
FDA
93.
767
from
the
U.S
. Dep
t. of
Hea
lth a
nd H
uman
Ser
vice
s, C
ente
rs fo
r Med
icar
e &
Med
icai
d S
ervi
ces.
H
owev
er, t
hese
con
tent
do
not n
eces
saril
y re
pres
ent
the
polic
y of
the
U.S
. Dep
t. of
Hea
lth a
nd H
uman
Ser
vice
s, a
nd s
houl
d no
t ass
ume
endo
rsem
ent b
y th
e Fe
dera
l gov
ernm
ent.
Dat
e: _
____
____
____
____
X La
bs
U
rine
dip
for
prot
ein/
gluc
ose
H
emog
lobi
n or
he
mat
ocrit
Rep
eat G
C/C
hlam
ydia
if
high
risk
(5) , b
efor
e 36
w
eeks
Rep
eat H
ep B
if h
igh
risk,
bef
ore
36 w
eeks
Rep
eat H
IV if
hig
h ris
k,
befo
re 3
6 w
eeks
Rep
eat R
PR
if h
igh
risk,
bef
ore
36 w
eeks
If R
hoga
m is
indi
cate
d,
antib
ody
scre
en a
t the
tim
e of
adm
inis
tratio
n
Gro
up B
Stre
p cu
lture
at
35-
36 w
eeks
X Ed
ucat
ion
S
igns
and
sym
ptom
s of
pre
term
la
bor a
nd p
reec
lam
psia
Aw
aren
ess
of fe
tal m
ovem
ent/k
ick
coun
t edu
catio
n an
d ex
pect
atio
n
Rev
iew
labo
r and
del
iver
y ex
pect
atio
n (in
clud
ing
anes
thes
ia)
and
the
patie
nt’s
pla
n fo
r tra
nspo
rtatio
n to
the
hosp
ital
B
reas
tfeed
ing
rein
forc
emen
t
Fina
lize
post
partu
m b
irth
cont
rol
plan
s
Rev
iew
circ
umci
sion
pla
n
Dis
cuss
pla
n fo
r new
born
's
heal
thca
re p
rovi
der/m
edic
al h
ome
R
evie
w n
eed
for c
ar s
eat
R
evie
w n
umbe
rs to
cal
l for
em
erge
ncie
s/la
bor
Im
porta
nce
of a
void
ing
elec
tive
deliv
erie
s pr
ior t
o 39
wee
ks
Fa
mily
med
ical
leav
e
Saf
e nu
rser
y se
t up
to p
reve
nt
SID
S –
Bac
k to
Sle
ep C
ampa
ign
R
evie
w s
igns
and
sym
ptom
s of
pe
rinat
al m
enta
l hea
lth d
isor
ders
(e
.g. d
epre
ssio
n)
O
ffer c
hild
birth
and
bre
astfe
edin
g cl
asse
s
X C
linic
al E
lem
ents
Vis
it fre
quen
cy s
houl
d be
eve
ry
2 w
eeks
unt
il 35
-36
wee
ks th
en e
very
w
eek
until
del
iver
y un
less
mor
e fre
quen
t vi
sits
are
clin
ical
ly
indi
cate
d.
W
t, B
P, F
unda
l hei
ght
at e
very
vis
it
Feta
l hea
rt to
nes
at
ever
y vi
sit
P
erin
atal
men
tal h
ealth
sc
reen
ing
(4)
B
egin
NST
/AFI
whe
n/if
clin
ical
ly in
dica
ted
G
ive
Rho
gam
at 2
8 w
eeks
if in
dica
ted
H
erpe
s pr
ophy
laxi
s st
artin
g at
36
wee
ks if
in
dica
ted
O
ffer T
dap
vacc
ine
afte
r 27
wee
ks
X R
efer
rals
Tran
sfer
of m
edic
al re
cord
s to
an
ticip
ated
del
iver
y ho
spita
l
Ref
erra
l to
WIC
Ref
erra
l to
Fam
ily C
ase
Man
agem
ent
X H
igh-
Ris
k R
efer
rals
Hig
h-R
isk
cond
ition
iden
tifie
d?
Rea
son:
____
____
____
____
____
_
Ref
erra
l to
men
tal h
ealth
pr
ofes
sion
al o
r soc
ial w
orke
r if
indi
cate
d
Ref
erra
l to
OB
or M
FM if
indi
cate
d
3rd T
rimes
ter,
28-3
9 W
eeks
Plac
e pa
tient
stic
ker h
ere.

APP-B-5
aPPendix b – Prenatal care Quality tool
Pren
atal
Car
e Q
ualit
y To
ol C
heck
list
This
doc
umen
t was
dev
elop
ed u
nder
gra
nt C
FDA
93.
767
from
the
U.S
. Dep
t. of
Hea
lth a
nd H
uman
Ser
vice
s, C
ente
rs fo
r Med
icar
e &
Med
icai
d S
ervi
ces.
H
owev
er, t
hese
con
tent
do
not n
eces
saril
y re
pres
ent
the
polic
y of
the
U.S
. Dep
t. of
Hea
lth a
nd H
uman
Ser
vice
s, a
nd s
houl
d no
t ass
ume
endo
rsem
ent b
y th
e Fe
dera
l gov
ernm
ent.
Dat
e: _
____
____
____
____
_
X La
bs
U
rine
dip
for
prot
ein/
gluc
ose
G
roup
B S
trep
cultu
re,
if no
t don
e at
35-
36
wee
ks
X R
efer
rals
Ref
erra
l to
WIC
Ref
erra
l to
Fam
ily C
ase
Man
agem
ent
X H
igh-
Ris
k R
efer
rals
Hig
h-R
isk
Con
ditio
n Id
entif
ied?
R
easo
n: _
____
____
____
____
__
R
efer
ral t
o m
enta
l hea
lth
prof
essi
onal
or s
ocia
l wor
ker i
f in
dica
ted
R
efer
ral t
o O
B/M
FM if
indi
cate
d
X Ed
ucat
ion
A
war
enes
s of
feta
l mov
emen
t
Sig
ns a
nd s
ympt
oms
of p
rete
rm
labo
r and
pre
ecla
mps
ia
La
bor a
nd D
eliv
ery
expe
ctat
ion
and
plan
(inc
ludi
ng a
nest
hesi
a) a
nd th
e pa
tient
’s p
lan
for t
rans
porta
tion
to
the
hosp
ital
Fa
mily
med
ical
leav
e
Rei
nfor
ce B
reas
tfeed
ing
impo
rtanc
e
R
evie
w b
irth
cont
rol p
lans
Rev
iew
nee
d fo
r car
sea
t-ref
er to
D
HS
if in
nee
d of
a c
ar s
eat
Im
porta
nce
of a
void
ance
of e
lect
ive
deliv
erie
s pr
ior t
o 39
wee
ks
R
evie
w n
umbe
rs to
cal
l for
em
erge
ncie
s/la
bor
Im
porta
nce
of p
ostp
artu
m v
isit
and
ongo
ing
heal
thca
re a
fter d
eliv
ery
S
afe
nurs
ery
set u
p to
pre
vent
SID
S –
Bac
k to
Sle
ep C
ampa
ign
D
iscu
ss im
porta
nce
of p
ostp
artu
m
visi
t and
try
to s
ched
ule
post
partu
m
visi
t if f
easi
ble
D
iscu
ss im
porta
nce
of o
ngoi
ng
heal
thca
re a
fter d
eliv
ery
and
iden
tify
med
ical
car
e ho
me/
PC
P
X C
linic
al E
lem
ents
Vis
it fre
quen
cy s
houl
d be
w
eekl
y
Wt,
BP,
Fun
dal h
eigh
t at
ever
y vi
sit
Fe
tal h
eart
tone
s at
eve
ry
visi
t
Cer
vica
l exa
m if
indi
cate
d
Con
firm
feta
l pos
ition
Con
side
r offe
ring
vers
ion
if no
n-ce
phal
ic p
rese
ntat
ion
N
ST,
BP
P if
clin
ical
ly
indi
cate
d
3rd T
rimes
ter,
38 W
eeks
to D
eliv
ery
Plac
e pa
tient
stic
ker h
ere.

APP-B-6
aPPendix b – Prenatal care Quality tool
Pren
atal
Car
e Q
ualit
y To
ol C
heck
list
This
doc
umen
t was
dev
elop
ed u
nder
gra
nt C
FDA
93.
767
from
the
U.S
. Dep
t. of
Hea
lth a
nd H
uman
Ser
vice
s, C
ente
rs fo
r Med
icar
e &
Med
icai
d S
ervi
ces.
H
owev
er, t
hese
con
tent
do
not n
eces
saril
y re
pres
ent
the
polic
y of
the
U.S
. Dep
t. of
Hea
lth a
nd H
uman
Ser
vice
s, a
nd s
houl
d no
t ass
ume
endo
rsem
ent b
y th
e Fe
dera
l gov
ernm
ent.
Dat
e: _
____
____
____
____
__
___
Wee
ks P
ost D
eliv
ery
X La
bs
P
ap T
est i
f due
(c
olpo
scop
y if
need
ed)
2
hour
GTT
scr
eeni
ng
or a
ppro
pria
te s
cree
ning
fo
r all
gest
atio
nal
diab
etic
s
X C
linic
al E
lem
ents
Phy
sica
l inc
ludi
ng b
reas
t, ab
dom
inal
and
pel
vic
ex
amin
atio
n
Per
inat
al m
enta
l hea
lth
scre
en
S
cree
n fo
r inc
ontin
ence
(fe
cal,
urin
ary
and
gas)
Scr
een
for b
reas
tfeed
ing
diffi
culti
es
B
irth
cont
rol m
etho
d re
ceiv
ed
Hig
hly
effe
ctiv
e m
etho
d:
IUD
, im
plan
t M
oder
atel
y ef
fect
ive
met
hod:
inj
ectio
n, p
ills,
patc
h, v
agin
al ri
ng
X R
efer
rals
Ref
erra
l to
men
tal h
ealth
pr
ofes
sion
al o
r soc
ial w
orke
r if
indi
cate
d
Ref
er to
lact
atio
n co
nsul
tant
or
hotli
ne if
indi
cate
d
Ref
erra
l to
PC
P /m
edic
al h
ome
for
ongo
ing
care
Ref
erra
l to
WIC
Ref
erra
l to
and
Fam
ily C
ase
Man
agem
ent
X Ed
ucat
ion
R
ecom
men
d ex
clus
ive
brea
stfe
edin
g fo
r at l
east
6
mon
ths
dura
tion,
add
ress
co
ncer
ns
P
ostp
artu
m s
exua
l act
ivity
and
bi
rth c
ontro
l met
hods
Ben
efits
of i
nter
preg
nanc
y sp
acin
g
Res
ume
phys
ical
act
ivity
R
etur
n to
wor
k/sc
hool
Rev
iew
sig
ns a
nd s
ympt
oms
of
post
partu
m m
ood
diso
rder
s
Saf
e nu
rser
y se
t up
to p
reve
nt
SID
S –
Bac
k to
Sle
ep
Cam
paig
n
Post
partu
m
Plac
e pa
tient
stic
ker h
ere.

APP-C-1
aPPendix c – referrals for HigH-risk Prenatal conditions
Referrals for High-Risk Prenatal Conditions
January 2014
Page 1 of 4
This document was developed under grant CFDA 93.767 from the U.S. Dept. of Health and Human Services, Centers for Medicare & Medicaid Services. However, these content do not necessarily represent the policy of the U.S. Dept. of Health and Human Services, and should not assume endorsement by the Federal government.
Reproductive History
Perinatal Code
ACOG Referral / Consultation
1st Trimester loss No Referral
Successive 1st trimester losses
MFM and Reproductive Endocrinologist if available
2nd Trimester loss MFM -perinatal death mid trimester loss
OB OB or MFM if available
3rd Trimester loss MFM perinatal death mid trimester loss
OB or MFM if available
History of LBW or VLBW OB OB or MFM
History of preterm delivery <34 wks
MFM - 34 weeks OB (or prior PROM) OB or MFM
History of Preeclampsia/eclampsia
OB or MFM
Family history of genetic disorder
MFM MFM or Genetic Specialist
Developmental or Intellectual Disability
MFM
Birth with congenital anomalies
MFM MFM MFM/ultrasound
Uterine abnormalities OB OB or MFM
Abnormal Pap OB for possible Colposcopy referral when indicated
Prior birth with complication resulting in handicap
MFM OB or MFM
Prior fetal/neonatal death
OB OB or MFM
Prior cervical insufficiency
MFM
Prior myomectomy or C-section
OB OB
Prior gynecological malignancy
OB or MFM

APP-C-2
aPPendix c – referrals for HigH-risk Prenatal conditions
Referrals for High-Risk Prenatal Conditions
January 2014
Page 2 of 4
This document was developed under grant CFDA 93.767 from the U.S. Dept. of Health and Human Services, Centers for Medicare & Medicaid Services. However, these content do not necessarily represent the policy of the U.S. Dept. of Health and Human Services, and should not assume endorsement by the Federal government.
Active Medical Conditions
Perinatal Code
ACOG Referral / Consultation
Pregestational Diabetes MFM- IDDM class B or >
Class A-C (OB) Class D or> (MFM)
MFM
Controlled Hypertension
MFM -Essential HTN on medications
MFM- with renal/cardiac dis. OB-w/o cardiac dis.
OB or MFM
Uncontrolled Hypertension
MFM
MFM- with renal/cardiac dis. OB-w/o cardiac dis.
MFM
Cardiovascular disease MFM MFM MFM and Cardiology
Sickle Cell disorders MFM MFM MFM
HIV OB or MFM (based on CD4 counts
MFM and ID
Active Hepatitis B or C MFM and GI
Autoimmune disorders (including SLE)
MFM and Rheumatologist
Seizure disorders OB MFM and Neurologist
Renal disease MFM
Creat>3-MFM Chronic-OB Proteinuria-OB
MFM and Nephrologist
Cystic Fibrosis MFM
Thyroid disease OB and Endocrinologist or MFM
ITP MFM
Thromboembolic disease
OB- Hx of PE/DVT MFM
Anemia (HCT<28%, unresponsive to iron therapy)
Hemophilia MFM and Hematologist
Malignancy MFM
Physical disability OB or MFM
Pulmonary Disease MFM -Severe OB-Moderate
OB and Pulmonologist or MFM
Asthma on steroids OB- on meds MFM- if multiple hospitalizations
MFM
Perinatal code- Chronic medical problems with known increase in perinatal morbidity and mortality ACOG- Any systemic disease that adversely affects pregnancy should have an MFM consultation

APP-C-3
aPPendix c – referrals for HigH-risk Prenatal conditions
Referrals for High-Risk Prenatal Conditions
January 2014
Page 3 of 4
This document was developed under grant CFDA 93.767 from the U.S. Dept. of Health and Human Services, Centers for Medicare & Medicaid Services. However, these content do not necessarily represent the policy of the U.S. Dept. of Health and Human Services, and should not assume endorsement by the Federal government.
Obstetrical Complications
Perinatal Code
ACOG Referral / Consultation
Di/Di twin gestation MFM -multiple gestation OB- multigestation OB
Mono/Di or Mono/Mono twin gestation
MFM-multiple gestation MFM
Triplets or greater MFM -multiple gestation MFM
Positive Quad screen MFM - abnormal genetic evaluation
OB OB or MFM
Cervical insufficiency OB MFM
Short cervix MFM
IUGR MFM OB OB or MFM
Polyhydramnios OB- hydramnios by ultrasound
OB or MFM
Oligohydraminos OB OB or MFM
Viral exposure (TORCH) during pregnancy
OB or MFM
Gestational Hypertension/ Preeclampsia/eclampsia
MFM OB - diastolic >90, w/o proteinuria
OB or MFM
Abnormal fetal presentation at 3rd trimester
OB
Induction of labor prior to term
OB or MFM
Abnormal antenatal testing
OB
Abnormal labor OB
IUFD OB OB or MFM consult
Premature/Preterm labor
MFM < or = 36 weeks OB< 37 weeks OB
PPROM, PROM OB OB
Anticipated elective C-section
OB
Severe postpartum hemorrhage
OB
Repair of 3rd or 4th degree laceration
OB
3rd trimester bleeding MFM OB> 14 weeks OB
Post date > or = 42 wks MFM OB OB
Abnormal fetal ultrasound
OB or MFM MFM
Isoimmunization MFM MFM MFM

APP-C-4
aPPendix c – referrals for HigH-risk Prenatal conditions
Referrals for High-Risk Prenatal Conditions
January 2014
Page 4 of 4
This document was developed under grant CFDA 93.767 from the U.S. Dept. of Health and Human Services, Centers for Medicare & Medicaid Services. However, these content do not necessarily represent the policy of the U.S. Dept. of Health and Human Services, and should not assume endorsement by the Federal government.
Psych/Social Perinatal Code
ACOG AAFP Referral / Consultation
Bipolar Psych OB and Psych if available
Depression Psych OB and Psych if available
Schizophrenia Psych OB and Psych if available
Anxiety disorder Psych OB and Psych if available
History of Post-partum depression/psychosis
Psych OB and Psych if available
Active substance disorder
Other OB - drug and alcohol use
MFM -drug addiction
Actively suicidal Admission to inpatient Admission to inpatient
Domestic/Partner violence
Social service Social Service
Housing Social service Social Service

APP-D-1
aPPendix d – PostPartum transition strategies
Strategies for Improving the Postpartum Visit Rate for HFS-Enrolled Women
Health Care Provider
Strategy
Timing
Intervention
Prenatal Provider
Education During last scheduled prenatal visit
EHR alert to provide postpartum education Discuss the importance of the postpartum visit
and encourage the woman to schedule and complete the appointment
Provide a patient postpartum checklist to the woman (in combination with verbal education above)
Schedule Appointment
During the last scheduled prenatal visit
EHR alert to schedule postpartum appointment Schedule postpartum appointment
After delivery Upon notification of delivery by hospital, outreach to patient to schedule postpartum appointment
Hospital Notification Prior to discharge Develop a system to provide immediate notification of delivery to prenatal care provider
Education Prior to discharge EHR alert and/or checklist to provide postpartum education
Discuss the importance of the postpartum visit and encourage the woman to schedule and complete the appointment
Provide a patient postpartum checklist to the woman (in combination with verbal education above)
Schedule Appointment
Prior to discharge Develop a system to ensure that the woman has a postpartum visit scheduled
Following education (above), encourage the woman to make the postpartum appointment
Confirm that appointment was made; offer assistance
Pediatrician Education During the first well baby visit
EHR alert to provide postpartum education Ask the woman if she has a postpartum
appointment scheduled Discuss the importance of the postpartum visit
and encourage the woman to schedule and complete the appointment
Provide a patient postpartum checklist to the woman (in combination with verbal education above)

aPPendix e – HiteQ resources
APP-E-1
The HITEQ Center is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number U30CS29366 titled Training and Technical Assistance National Cooperative Agreements (NCAs) for grant amount $500,000. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS or the U.S. Government.
HEALTH IT ENABLED QUALITY IMPROVEMENT: A GUIDE TO IMPROVING CARE PROCESSES AND OUTCOMES
Available on HITEQCenter.org
1
CHECK/ REINFORCE FOUNDATIONS
Cultivate shared commitment and shared understanding
Ensure leadership support and buy-in from the whole team
Ensure access to and validate data that will underpin the QI efforts.
Ensure stable and reliable health IT systems (including people, processes, and technology related to systems)
o Recommended tools, all available on HITEQcenter.org, under Health IT Enabled QI :
Health IT enabled Quality Improvement Project Charter: The first step in a QI project (link) Accessing your Data: Questions to Consider with your EHR vendor (link) Analytics Capability Assessment, from Center for Care Innovations (link) Health Center Data Validation Tool (link for Adult BMI, others coming to HITEQCenter.org)
UNDERSTAND HEALTH IT ENABLED QUALITY IMPROVEMENT
Everyone participating in the QI work should have a shared understanding of key definitions, frameworks (e.g., CDS 5 Rights, below), strategies (e.g., the QI process outlined under the Implement and Evaluate Changes heading.), tools (e.g., Essential CDS/QI Worksheet), and key QI project success factors.
1 Osheroff, Jerome A. "Improving Care Processes and Outcomes in Health Centers. HRSA Health Information Technology, Evaluation and Quality Center. 9 Sept. 2016. Web. 21 Nov. 2016

aPPendix e – HiteQ resources
APP-E-2
The HITEQ Center is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number U30CS29366 titled Training and Technical Assistance National Cooperative Agreements (NCAs) for grant amount $500,000. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS or the U.S. Government.
The CDS 5 Rights framework, a recommended CMS best practice QI approach to support decisions and actions that drive performance targeted for improvement, says that improving care processes for optimal outcomes requires getting the right information to the right people in the right formats through the right channels at the right times.2
Be sure to consider people, processes, and technology, in that order!, when considering processes and engaging in quality improvement. Improvement to care processes and other quality drivers must be done WITH people, not to them.
o Recommended tools, all available on HITEQcenter.org, under Health IT Enabled QI :
Guide to Improving Care Processes and Outcomes in Health Centers (link)
SELECTING QUALITY IMPROVEMENT TARGET, INITIATE QI PROJECT
What quality improvement target should be selected? Consider the following: o Business imperatives, such as value-based payment initiatives or awards (such as HRSA Quality
Leader or Technology awards). o Seek QI synergies with pertinent initiatives such as PCMH recognition and HRSA Health Center
Quality Improvement Grant Awards. o Those measures or outcomes that have experienced unexpected change in performance
o Operational initiatives such as: Behavioral health integration Oral health integration Collecting and operationalizing sexual orientation/ gender identity data Collecting and operationalizing social determinants of health data
Document the selected target, including specific quality measure when possible as well as time period, specific population, and so on. Also document current performance.
o Recommended tools, all available on HITEQcenter.org, under Health IT Enabled QI :
Prioritization Matrix, to select from multiple target options (link) Document selected target in first section (target and current performance) of Essential
CDS/ QI Worksheet (link)
DOCUMENT AND ANALYZE FLOWS, IDENTIFY IMPROVEMENTS
Consider the following questions about workflow and information flow, as it relates to your selected target:
o What are we currently doing? What are we trying to improve and what is the baseline? [using analytics]
o What should we be doing to produce better processes and results? [using best practices]
2 TMIT Consulting, 2016.

aPPendix e – HiteQ resources
APP-E-3
The HITEQ Center is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number U30CS29366 titled Training and Technical Assistance National Cooperative Agreements (NCAs) for grant amount $500,000. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS or the U.S. Government.
o What changes might we make to produce better processes and results? [adoption]
Consider individual patient activities, such as what is done to support the given target when the patient is in the clinic, as well as population management activities, such as tools or activities used to identify and address care gaps across the patient panel, and foundational activities, such as the health IT systems, policies, and protocols that support all activities in the health center.
o Recommended tools, all available on HITEQcenter.org, under Health IT Enabled QI :
Collaboratively, with your team representing all stakeholders, document What are we currently doing [related to our selected target]? in the Current Workflow/ Information Flow lines of the Essential CDS/ QI Worksheet (link)
Complete the Individual Patient Activities section, in Orange, as well as Population Management activities, in Blue, and Foundational Activities, in Green of the worksheet, as each section relates to your selected target.
Document What should we be doing? in the Potential Enhancement lines of the Essential CDS/ QI Worksheet (link)
When considering improvements/ potential enhancements using this worksheet, consider the following:
o Cells or sections where the current flow is not known o Instances where stakeholders are not aligned on processes (i.e. different
providers or care teams do different things or have different workflows) o Instances where no policy/ protocol is in place o Instances where the 5 Rights are not well orchestrated; i.e. the right
information is not available at the right time through the right channels o Instances where policies and workflows are in place, but outcomes are still
suboptimal– are there population factors?
IMPLEMENT AND EVALUATE CHANGES
Using a QI methodology such as PDSA cycles, engage frontline staff and all key stakeholders in care processes and results to design, implement and evaluate one selected enhancement.
o Be sure to do this work with all the stakeholders and not to them (i.e., seek and act on team member and patient input and feedback throughout the process).
Monitor implementation activities with structured tools that help you document and manage who’s doing what when, as well as the results.
Evaluate the impact of the change based on results and feedback from those involved, determine final action related to the tested enhancement: adopt, adapt, or abandon. Recommended tools:
o For assistance in selecting one potential enhancement to test first, use the prioritization matrix again.
o PDSA Worksheet, such as this one from Oregon Primary Care Association, or this one from the Institute for Healthcare Improvement
o Data collection tools and plan for monitoring, such as these from Oregon Primary Care Association o Monitoring Worksheets from Chapter 8: Putting Interventions into Action and Chapter 9: Measuring
Results and Continuously Refining the Program in “Improving Outcomes with Clinical Decision Support: An Implementer’s Guide. Second Edition” provided with permission from HIMSS

aPPendix e – HiteQ resources
APP-E-4
The HITEQ Center is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number U30CS29366 titled Training and Technical Assistance National Cooperative Agreements (NCAs) for grant amount $500,000. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS or the U.S. Government.
IMPLEMENT AND EVALUATE CHANGES
Apply this learning and these results to strengthen ongoing ‘maintenance’ efforts on the current target and other target-focused QI initiatives.
o Transition target-related QI efforts from ‘project-focused’ to ‘this is how we do business.’ Build in ability to detect the need for, and implement, tweaks to target-related processes when required because of changes to people/processes/technology.
i.e., Feedback loops! o Be sure to incorporate the insights and results from each QI project into subsequent QI initiatives.
Although a particular target-focused QI project may be time-limited, the QI and clinical teams should remain alert for ways to continually improve care across all targets.
For example, learning from a QI project might indicate opportunities to more broadly modify clinical and quality work and roles, as well as health IT configurations or integrations.
Recommended tools/ references: o Harnessing the Power of Feedback Loops, Wired.com. o Zikmund-Fisher BJ, et al. Graphics help patients distinguish between urgent and non-urgent
deviations in laboratory test results. Journal of the American Medical Informatics Association 2017;24(3):520-528.
o Developing Effective Data Dashboards, a primer on a process and tips in developing a data dashboard from HITQ.
o Data Monitoring: Population Health Data Strategies (Webinar) o Worth a Thousand Words: How to Display Health Data from California Healthcare Foundation

APP-F-1
aPPendix f – guide to Patient and family engagement
Steps to Creating a Culture of Person and Family Engagement
Engage LeadersLeadership sets the tone for any organizational culture. Through words and actions, it falls to leaders to cultivate a supportive and trusting workplace culture, facilitate a continuous learning environment, and ensure that person and family engagement is integrated into organizational structure and strategy.
Enlist Patients and Families as PartnersCreate systems and processes to harness insights from patients and families about their experiences, gaps in care, and opportunities for continuous improvement. Examples include focus groups, participation on practice improvement teams, and patient and family advisory councils.
Empower and Energize StaffJoy in practices is created in part by feeling a sense of purpose that transcends specific tasks. To create this shared purpose, reserve time for staff to share stories of the positive impact they have made on patients’ lives. Introduce systems that invite all staff to participate in improving care and making the practice a better place to work.
Encourage Family Participation in CareFamily can be a vital source of continuity and coordination across episodes and settings of care. Invite patients to identify a family Care Partner. Then, elicit Care Partners’ observations and questions during visits. Equip Care Partners with tools for monitoring their loved one’s health and managing their care.
Equip, Enable and Support Patients to Engage
Patients’ goals, preferences and cultural norms cannot be integrated into care without their engagement in treatment planning and self-management. Adopt strategies such as teach back, medication management, and shared decision-making to support patients to become active members of the care team.
Emphasize PFE in All You DoPerson and family engagement isn't one more thing to do. It is the tie that binds all that you do together. With patients and family members as advisors, consider ways to modify the physical environment to promote engagement. Seek out community partners that will enable you to better engage patients and their family caregivers where they live, work, learn, worship and play.
The culture of a practice encompasses its attitudes, behaviors, practices and norms. The six steps below are designed to guide genuine transformation in culture to promote person and family engagement.
© 2017 Planetree - may be reproduced for non-commercial purposes

APP-F-2
Not sure where to start? This 30-day kick-start plan maps out concrete actions you can take in each of the six culture change steps within the next month. These early activities establish the vision of culture change, emphasize this as an inclusive effort built on partnership, and generate enthusiasm for the changes to come.
Engage Leaders• Complete this leadership self-assessment to identify opportunities to lead change.
• During your next staff meeting, walk the entire team through these 6 steps of culture change. Invite them to weigh in on how the steps can be applied in your office.
Enlist Patients and Families as PartnersTrain a team member to conduct brief patient and family interviews during wait times. Ask patients and family members what has kept them loyal to the office. Invite them to complete this sentence: “I wish this office would…” Use these ideas to guide improvements.
Empower and Energize Staff• Kick off your next staff meeting with a patient story.
• Invite all staff to complete a personal commitment card where they identify a specific way they will contribute to the office’s culture of person and family engagement.
Encourage Family Participation in Care• Develop a process for identifying and documenting family care partners in a patients’ record.
• Audit your exam rooms to ensure that there is ample space and seating to accommodate the presence of family. Ask patients for feedback as well!
Equip, Enable and Support Patients to EngageInvite patients to partner with you to identify practical tools for making their visits even more constructive. Share a selection of tools for them to review, trial and provide feedback on. Examples include: the I Wish I Had Asked That tool, Ask Me 3 and this Patient Note Sheet.
30 Day Kick-Start Plan
Emphasize PFE in All You DoConsider how the set-up of the office and exam rooms is welcoming and conducive to building relationships. Every space should facilitate personal connection, engagement and eye contact. Examine the front office overall; in exam rooms assess placement of the computer screen and keyboard, availability and height of chairs, positive diversions for patients, etc.
© 2017 Planetree - may be reproduced for non-commercial purposes
aPPendix f – guide to Patient and family engagement

APP-G-1
aPPendix g – tHe Joint commission HealtH literacy and self-management tools
Health Literacy
AHRQ defines Health literacy is the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions.
Differences in health literacy level were consistently associated with increased hospitalizations, greater emergency care use, lower use of mammography, lower receipt of influenza vaccine, poorer ability to demonstrate taking medications appropriately, poorer ability to interpret labels and health messages, and, among seniors, poorer overall health status and higher mortality.
Sample Screening Tools for Health Literacy:
Rapid Estimate of Adult Literacy in Medicine—Short Form (REALM-SF)
The Rapid Estimate of Adult Literacy in Medicine—Short Form (REALM-SF) is a 7-item word recognition test to provide clinicians with a valid quick assessment of patient health literacy.
The REALM-SF has been validated and field tested in diverse research setting, and has excellent agreement with the 66-item REALM instrument in terms of grade-level assignments.
SAHLSA (Short Assessment of Health Literacy for Spanish-speaking Adults)
The SAHLSA consists of a word-recognition section, designed after the REALM, in addition to a comprehension test that employs multiple choice questions. It was designed to assess the health literacy for adults who speak Spanish.
SILS (Single Item Literacy Screener)
The SILS is a single item instrument designed to identify patients who need help with reading health-related information. The instrument asks one question “How often do you need to have someone help you when you read instructions, pamphlets, or other written material from your doctor or pharmacy?” with possible responses ranging from “1” (never) to “5” (always).
In this primary care population, one in six had limited reading ability. With the known negative impact of limited reading ability on health outcomes, enhancing communication for this population is critical. The SILS performs moderately well at ruling out limited reading ability in adults and allows providers to target additional assessment to those most in need. Application of the SILS in clinical settings has the potential to improve outcomes and processes of care for chronically ill individuals with limited reading ability.
S-TOFHLA
The S-TOFHLA, a 7-minute test, with 36 reading comprehension items in 2 passages. The passages on the S-TOFHLA use a modified Cloze procedure where every fifth to seventh word is omitted and subjects select the correct word from among a set of four options. The passages contain information about an upper gastrointestinal tract x-ray procedure, and the “Rights and Responsibilities” section from a Medicaid application, Each selection is scored a “1” for correct or a “0” for incorrect and scores are summed over items to create a total score. The 36-point scale of the S-TOFHLA is divided into three categories of functional literacy: inadequate (0-16), adequate (17-22) and functional (23-36)
In early developmental studies, the reading comprehension passages in the S-TOFHLA had a reliability coefficient of 0.97 and correlation with the Rapid Estimate of Adult Literacy in Medicine (REALM) of 0.81.
NVS (Newest Vital Sign)
The NVS consists of a nutrition label with 6 accompanying questions to assess literacy. It takes approximately 3 minutes to administer, and is meant to allow healthcare providers to make a quick assessment of patients’ literacy, which can then allow them to adapt communication to achieve better outcomes. It assesses literacy and numeracy, and is available in both English and Spanish versions.
Since the Newest Vital Sign was published in the Annals of Family Medicine (December 2005), it has appeared in more than 25 peer-reviewed studies. The NVS has been used to assess health literacy in populations ranging from parents of young children to older adults, among racial/ethnic minorities, and applied to a wide variety of health conditions.
(Measuring Adult Literacy in Health Care: Performance of the newest Vital Sign, Am. J Health Behav 2007)
“In comparison to the REALM and the S-TOFHLA, the NVS – which was developed as a screening tool – has high sensitivity for detecting limited literacy. Its specificity varies depending on whether the REALM or S-TOFHLA is used as the comparison standard. The performance of the NVS in both of these studies suggests it may be useful as a clinical screening tool when high sensitivity is acceptable, but less in research settings that require precision in measurement. It should be noted that health literacy experts do not currently recommend literacy screening in the clinical setting unless healthcare professionals and the healthcare system are willing to implement communication strategies appropriate for patients with limited literacy.”
“In this set of studies, we found the NVS to be more strongly correlated with the S-TOFHLA than the REALM. The NVS was also not found to be associated with health knowledge or outcomes, whereas the S-TOFHLA was linked to these variables. This gives the S-TOFHLA a stronger predictive validity than the NVS, which should be considered when deciding which instrument to use for research purposes.”
Used with Permission from The Joint Commission

APP-G-2
aPPendix g – tHe Joint commission HealtH literacy and self-management tools
Used with Permission from The Joint Commission

APP-G-3
aPPendix g – tHe Joint commission HealtH literacy and self-management tools
Used with Permission from The Joint Commission

APP-G-4
aPPendix g – tHe Joint commission HealtH literacy and self-management tools
Used with Permission from The Joint Commission