PERFORMANCE REVIEW WILLIAM R. SHARPE, JR. HOSPITAL · PERFORMANCE REVIEW WILLIAM R. SHARPE, JR....
33
PERFORMANCE REVIEW WILLIAM R. SHARPE, JR. HOSPITAL DEPARTMENT OF HEALTH AND HUMAN RESOURCES December 2019 PE 19-05-627 AUDIT OVERVIEW Sharpe Hospital’s Loss of Certification by the Centers for Medicare and Medicaid Services Severely Impacted Its Revenue Stream. Sharpe Hospital Is ADA Compliant After No Citations Issued by the Centers for Medicare and Medicaid Services. WEST VIRGINIA LEGISLATIVE AUDITOR PERFORMANCE EVALUATION & RESEARCH DIVISION
Transcript of PERFORMANCE REVIEW WILLIAM R. SHARPE, JR. HOSPITAL · PERFORMANCE REVIEW WILLIAM R. SHARPE, JR....
PERFORMANCE REVIEW
WILLIAM R. SHARPE, JR. HOSPITALDEPARTMENT OF HEALTH AND HUMAN RESOURCES
December 2019PE 19-05-627
AUDIT OVERVIEW
Sharpe Hospital’s Loss of Certification by the Centers for Medicare and Medicaid Services Severely Impacted Its Revenue Stream.
Sharpe Hospital Is ADA Compliant After No Citations Issued by the Centers for Medicare and Medicaid Services.
WEST VIRGINIA LEGISLATIVE AUDITOR
PERFORMANCE EVALUATION & RESEARCH DIVISION
JOINT COMMITTEE ON GOVERNMENT OPERATIONS
JOINT COMMITTEE ON GOVERNMENT ORGANIZATION
SenateMark Maynard, ChairChandler Swope, Vice-ChairCharles ClementsKenny MannMike MaroneyRandy SmithDave SypoltEric J. TarrDouglas E. FacemireWilliam D. IhlenfeldGlenn Jeffries Richard D. Lindsay IICorey PalumboMike Woelfel
House of DelegatesGary G. Howell, Chair Carl Martin, Vice-ChairRodney Pyles, Minority ChairPhillip W. Diserio, Minority Vice-ChairTom AzingerTom BibbyScott CadleDanny HamrickJohn Paul HottDean JeffriesJoe JeffriesChuck LittleEric NelsonChris Phillips
Eric PorterfieldTerri Funk SypoltEvan WorrellMichael AngelucciMike CaputoEvan HansenKenneth HicksMargaret StaggersRandy SwartzmillerTim TomblinDanielle Walker
Building 1, Room W-314State Capitol ComplexCharleston, West Virginia 25305(304) 347-4890
WEST VIRGINIA LEGISLATIVE AUDITOR
PERFORMANCE EVALUATION & RESEARCH DIVISION
SenateMark Maynard, ChairCharles ClementsChandler SwopeGlenn JeffriesCorey Palumbo
House of DelegatesGary G. Howell, Chair Chuck LittleCarl MartinRodney PylesTim Tomblin
Agency/ Citizen MembersVacancyVacancyVacancy VacancyVacancy
Aaron AllredLegislative Auditor
John SylviaDirector
Brandon BurtonResearch Manager
Lukas GriffithResearch Analyst
Cheyenne DeBoltReferencer
Performance Evaluation & Research Division | pg. 3
Performance Review
CONTENTS
Executive Summary ....................................................................................................................................................................... 5
Issue 1: Sharpe Hospital’s Loss of Certification by the Centers for Medicare and Medicaid Services Severely Impacted Its Revenue Stream ............................................................................................................ 7Issue 2: Sharpe Hospital Is ADA Compliant After No Citations Issued by the Centers for Medicare and Medicaid Services ..........................................................................................................................................23
List of Tables
Table 1: West Virginia State Hospitals .................................................................................................................................... 8Table 2: Sharpe Hospital Bed Capacity ................................................................................................................................. 9Table 3: Sharpe Hospital Admissions, Diversions and Diversion Costs ...................................................................13Table 4: Forensic and Civil Patients Served at Sharpe Hospital FY 2015-FY 2019 ...............................................15Table 5: Sharpe Hospital Expenditures and Revenues ..................................................................................................16Table 6: Sharpe Hospital Employee Turnovers .................................................................................................................17Table 7: Reasons Given for Resignations ............................................................................................................................17Table 8: Sharpe Hospital’s 2018 Treatment Plan Improvement Project ..................................................................19Table 9: Treatment Planning Improvement Results (2019) .........................................................................................20
List of Figures:
Figure 1: Sharpe Hospital Diversion Facilities ....................................................................................................................14Figure 2: Sharpe’s Forensic Inpatient Census Growth .....................................................................................................15
List of Appendices
Appendix A: Transmittal Letters ..............................................................................................................................................25Appendix B: Objectives, Scope and Methodology .........................................................................................................27Appendix C: Agency Response ...............................................................................................................................................29

pg. 4 | West Virginia Legislative Auditor
William R. Sharpe, Jr. Hospital
Performance Evaluation & Research Division | pg. 5
Performance Review
EXECUTIVE SUMMARY
ThePerformanceEvaluationandResearchDivision(PERD)withintheOfficeoftheLegislativeAuditorconductedanAgencyReviewoftheDepartmentofHealthandHumanResources(DHHR)pursuanttoWestVirginiaCode§4-10-8.Aspartofthisprocess,aPerformanceReviewofWilliamR.Sharpe,Jr.Hospital(Sharpe)wasconducted.TheobjectivesofthisreviewweretodeterminehowSharpewasimpactedafterlosingcertificationfromtheCentersforMedicareandMedicaidServices(CMS),andwhetherthefacilitycompliedwiththeAmericanswithDisabilitiesAct(ADA). The issues ofthisreportarehighlightedbelow.
Frequently Used Acronyms in This Report:
PERD – Performance Evaluation and Research Division
DHHR–DepartmentofHealthandHumanResources
CMS–CentersforMedicareandMedicaidServices
ADA–AmericanswithDisabilitiesAct
OHFLAC-OfficeofHealthFacilityLicensureandCertification
OASIS-OurAdvancedSolutionwithIntegratedSystems(thesystemusedbystateagenciestouploadfinancialinformation,documentation,andpayvendors)
DSH-DisproportionateShareHospital
ROC–RecertificationOversightCommittee
Report Highlights:
Issue 1: Sharpe Hospital’s Loss of Certification by the Centers for Medicare and Medicaid Services Severely Impacted Its Revenue Stream.
InSeptember2017,Sharpe’sCMScertificationwasrevokedasa resultofdeficientpatienttreatmentplans.The resultingconsequences includedadecrease in revenue,an increase inexpenditures, significant changes to thepatientpopulation, and the implementationofnewemploymentstandardsthatledtonotableturnoverswithinthehospital.
Followingthecertificationrevocation,Sharpecontractedtheservicesofarecognizednationalhealthcarecomplianceconsultingcompanytopursuetreatmentplancorrectionsandimproveoperationalperformance.
Sharpe established a recertification committee to implement necessary changes to itsinfrastructure,whichultimatelyledtosuccessfulCMSsurveysandformalrecertificationinAugust2019.
pg. 6 | West Virginia Legislative Auditor
William R. Sharpe, Jr. Hospital
Sharpehasdemonstratedtheability tocorrect internaldeficiencies;however,maintainingcompliancewithfederalhospitalguidelinesremainsimperativetoavoidingarepeatlossofCMScertification.
Issue 2: Sharpe Hospital Is ADA Compliant After No Citations Issued by the Centers for Medicare and Medicaid Services.
DuringastandardCMSsurveyofgeneralhospitals,federalguidelinesrequirethesurveyortocheckthefacilityforcompliancewithapplicablefederallawsrelatedtothehealthandsafetyofpatients,includingtheADAsinceitisafederallawbydefinition.Basedonthisstandard,asuccessfulCMSsurveywithoutanynoteddeficienciespertainingtotheapplicablefederallawsisindicativeofcompliancewiththeADA.
CMS survey procedures for confirming compliance with theADA-related code requiresurveyorstoreportnoncompliancetotheappropriateagencyhavingjurisdiction.InthecaseofSharpeHospital,therehavenotbeenreportsofnoncompliance.
ThemostrecentCMSsurveyofSharpeHospital,datedAugust14,2019,didnotfindanyADA-relateddeficiencies.
PERD’s Response to the Agency’s Written Response
OnDecember2,2019,PERDreceivedawrittenresponsetothereportfromtheagency’sCabinetSecretary,whichcanbefoundinAppendixC.Theagencyconcurredwithallrecommendationsandwillproceedtoimplementthem.
Recommendations
1. The Legislative Auditor recommends that Sharpe Hospital continue to follow all CMS guidelines pertaining to hospital regulations, psychiatric facility rules, and LSC to maintain certification and participation in the Medicare program. Emphasis should be placed on satisfying regulations related to treatment plans.
2. The Legislative Auditor recommends that Sharpe Hospital continue to comply with all ADA standards applicable to its facility.

Performance Evaluation & Research Division | pg. 7
Performance Review
ISSUE 1
In September 2017, Sharpe’s ability to bill or invoice for Medicare and Medic-aid funding was revoked by the Centers for Medicare and Medicaid Services (CMS) due to deficiencies found in pa-tient treatment plans.
Sharpe Hospital’s Loss of Certification by the Centers for Medicare and Medicaid Services Severely Impacted Its Revenue Stream.
Issue Summary
WilliamR.Sharpe, Jr.Hospital (Sharpe) isoneof sevenstate-ownedhospitalsinWestVirginia.Itisa200-bedacuteinpatientpsychiatricfacility that treats civil and forensic patients. In September 2017,Sharpe’s ability to bill or invoice forMedicare andMedicaid fundingwasrevokedbytheCentersforMedicareandMedicaidServices(CMS)duetodeficienciesfoundinpatienttreatmentplans.Followingthisevent,Sharpebegantransitioningitspatientpopulationto100percentforensicandpursuedvariousmethods tocorrect internaloperationalproblems.BecauseSharpecouldnolongerbillforMedicareorMedicaid,thehospitalwasforcedtoincreasetheoccurrenceofpatientdiversions,whereincivilpatientsweredeclinedforadmittanceandultimatelytransferredtootherCMS-certified facilities.Aside from the spike in diversions, Sharpe’slossofcertificationalsoincreasedexpenditures,decreasedrevenues,andinspiredsomeemployeeturnovers.
Upon losing certification, Sharpe established a specializedrecertificationcommittee,contractedtheservicesofarecognizednationalhealthcare compliance consulting company, and pursued other self-correctiveavenues.Afteraseriesofsuccessfulsurveys,SharpeachievedrecertificationfromCMSinAugust2019.Sharpeplanstoreadmitcivilpatients and fill the hospital to full capacity in the near future. TheLegislativeAuditorrecommendsthatSharpeshouldcontinuetofollowall CMS guidelines pertaining to hospital regulations and psychiatricfacility rules inorder tomaintain certification andparticipation in theMedicareprogram.Emphasisshouldbeplacedonsatisfyingregulationsrelatedtotreatmentplans.
Sharpe Is One of Seven State-Owned Hospitals.
SharpeHospitalisanacuteinpatientpsychiatricfacilitylocatedinWeston,WestVirginia.Originallyconstructedin1990,andopenedin1994,SharpereplacedtheagingWestonStateHospital.PursuanttoW.Va.Code§27-2-1onMentalHealthFacilities,SharpeoperatesundertheauthorityoftheDepartmentofHealthandHumanResources(DHHR)asoneof seven state-runhospitals (seeTable1).Effective July2018,allstatehospitalsweretransferredfromDHHR’sBureauforBehavioralHealthandHealthFacilities to thenewlyestablishedOfficeofHealthFacilities. Sharpe andMildredMitchell-Bateman Hospital, located inHuntington,WV, are the only twopsychiatric hospitals ownedby the
Upon losing certification, Sharpe es-tablished a specialized recertification committee, contracted the services of a recognized national healthcare compli-ance consulting company, and pursued other self-corrective avenues.

pg. 8 | West Virginia Legislative Auditor
William R. Sharpe, Jr. Hospital
State.AsofJune2019,Sharpeemployed350of456full-timepositions,leavingavacancyof106openpositions.
Table 1West Virginia State Hospitals
Hospital Name Location Built Type Bed Capacity
Hopemont TerraAlta,PrestonCounty 1913 NursingHome 98Licensed
JackieWithrow Beckley,RaleighCounty 1927 NursingHome 199Licensed144Available
JohnManchin,Sr.HealthCareCenter
Fairmont,MarionCounty 1899 NursingHome,OutpatientClinic 41NursingHome
Lakin WestColumbia,MasonCounty 1926 NursingHome 114Licensed
MildredMitchell-Bateman Huntington,CabellCounty 1950 Psychiatric
Hospital 110Licensed
WelchCommunity Welch,McDowellCounty 1902NursingHomeAcuteCareHospital
59NursingHome55AcuteCare
WilliamR.Sharpe,Jr. Weston,LewisCounty 1990 PsychiatricHospital 200Licensed
Source: DHHR Budget Presentation, 2019
Sharpe Hospital Is a 200-Bed Psychiatric Facility That Treats Forensic and Civil Patients.
With thecompletionofanadditional50-bedunit,whichbeganadmittingpatientsinApril2015,Sharpe’sfacilitiesincludeninedifferentunitswiththepotentialtoaccommodate200patientswhenoperatingatfullcapacity.Table2 illustratesSharpe’sunits,basicorganization,andlicensednumberofbeds.UnitsN-1,N-2,andN-3comprisetherecent50-bedaddition.
With the completion of an additional 50-bed unit, which began admitting patients in April 2015, Sharpe’s facilities include nine different units with the potential to accommodate 200 patients when operat-ing at full capacity.

Performance Evaluation & Research Division | pg. 9
Performance Review
Table 2Sharpe Hospital Bed Capacity
Unit Name Description Number of BedsC-1 Allmaleunitforcourt-orderedpatients 24C-2 Coedunitforcourt-orderedpatients 26E-1 Coedunit,generalpsychiatrics,ages55yearsandolder 23E-2 Coedunit,generalpsychiatrics,ages18-20 27G-1 Allmalegeneralpsychiatricunit 24G-2 Coedgeneralpsychiatricunit 26N-1 Forensic 22N-2 Civil* 20N-3 Civil 8
Total 200Source: Sharpe Hospital*Projected goal for December 2019.
Sharpe Hospital exclusively treats civil and forensic patients,bothof whichare involuntarilycommittedby thecourt system.Bothtypesofpatients require treatment fromstaffwith specialized trainingandaresubjecttouniquestipulationsunderWestVirginiaStateCode.
Civil patients are non-criminal patients who are deemed adangertothemselvesorothers.Sharpe’sCEOexplains,“Civil patients are involuntary patients admitted under Chapter 27 of the State Code. The probable cause hearing is presided over by a Mental Hygiene Commissioner appointed by the Circuit Judge. Civil commitments are discharged once their treatment improves their condition to the point that they are no longer deemed a danger to themselves or others and there is a safe discharge placement. The attending psychiatrist makes the decision to discharge civilly committed patients.”
Forensicpatientsaredefinedaspsychiatricpatientswhosementalillnesshasbrought themintocontactwith thecriminal justicesystem.Forensicpatientsundergoamulti-steplegalprocessbeforebeingcourt-orderedtoSharpe.AccordingtoW.Va.Code§27-6A,aforensicpatientcan include individualswho have been adjudicated as incompetent tostandtrial-inneedofrestoration,incompetenttostandtrial-unabletoberestored,ornotguiltybyreasonofmentalillness.
Civil patients are non-criminal patients who are deemed a danger to themselves or others.
Forensic patients are defined as psychiatric patients whose mental illness has brought them into contact with the criminal justice system.

pg. 10 | West Virginia Legislative Auditor
William R. Sharpe, Jr. Hospital
Beginning in early 2015, CMS launched multiple complaint investi-gation surveys at Sharpe Hospital as a result of Adult Protective Services complaints filed against the hospital.
Sharpe Hospital Lost CMS Certification in September 2017 Due to Inadequate Documentation of Treatment Plans.
CMSmaintainsoversightforcompliancewiththeMedicarehealthandsafetystandardsforvarioushealthcarefacilities,includingacutecareproviderssuchasSharpeHospital.InordertomeetandmaintainCMSregulations that permit participation in theMedicare program, Sharpemust faithfully satisfy federal guidelines for general hospitals, specialconditions for psychiatric hospitals, and the Life Safety Code, whichincludesfiresafetyandaspectsof theAmericanswithDisabilitiesAct(ADA).CMShasnosettimeframeforsurveysandcanthereforeauditfacilitiesforcomplianceatitsowndiscretion.Aspartofitsenforcementpolicy,CMSmayterminateanagreementwithaproviderofservicesifitisdeterminedthattheproviderisnotcomplyingsubstantiallywiththetermsoftheagreementorregulationspromulgatedthereunder.
AccordingtotheCMSenforcementpolicy,theinstitutionbeingsurveyedwillreceiveaStatementofDeficienciesifthecompletedsurveyfindsthefacilityoutofcompliancewithanyregulations.Theinstitutionisthengiven10calendardaystoproduceaplanofcorrectionforeachcited deficiency. Beginning in early 2015, CMS launched multiplecomplaintinvestigationsurveysatSharpeHospitalasaresultofAdultProtectiveServicescomplaintsfiledagainstthehospital.Theresultsofthosesurveysandsubsequentfollow-upauditsareasfollows:
• April 1, 2015 – December 30, 2015: Three out of eightsurveys conducted by the Office of Health Facility LicensureandCertification (OHFLAC)atSharpeciteddeficiencies,mostfrequentlyrelatingtopatientrightsorpatientsafety:
o medicationerrorsandmisplacementofMedicationRoomkeys,
o inadequatenumberofRNsonnightshift,o drugdiscrepancyforoxycodoneonpatient’smedication
records,o failure to properly document allegations of neglect
reportedbypatients,ando patientsbeing restrained forextendedperiodswithouta
physician’sdocumentedorder.
• February 24, 2016 – November 17, 2016: Five (5) out of 12OHFLACsurveyscompletedatSharpeciteddeficiencies,mostfrequentlyrelatingtopatientrightsandnursingsupervision:
o failuretoconductsafetychecksinatimelymanner,o failure to implement preventive measures, resulting in
patientself-harm,o staffmember falsified documents about routine checks,
and
In order to meet and maintain CMS regulations that permit participation in the Medicare program, Sharpe must faithfully satisfy federal guide-lines for general hospitals, psychiatric hospitals, and the Life Safety Code, which includes fire safety and aspects of the Americans with Disabilities Act (ADA).
Performance Evaluation & Research Division | pg. 11
Performance Review
As in past instances, Sharpe devised and submitted a plan of correction to remedy some of the deficiencies, but noncompliance persisted with Code of Federal Regulations (C.F.R.) §482.61 of the CMS State Operations Manual for Psychiatric Hospitals.
o failure to file proper paperwork regarding a physicalaltercationbetweenpatients.
• January 11, 2017 – August 14, 2017: Three (3) out of three(3)CMSsurveysforpsychiatrichospitalguidelinecompliance,and four (4)outof10OHFLACcomplaint surveys completedatSharpeciteddeficiencies,mostfrequentlyrelatingtonursingservices and special medical requirements for psychiatrichospitals:
o patientswerekeptinglass-encasedareasnotdesignedaspatientbedrooms,
o RNfailedtosuperviseandevaluatethecareofapatientinrestraint,
o failure to complete patient discharge summaries in atimelymanner,
o failurebytheMedicalDirectortomonitorservicequality,o “immediate jeopardy complaint investigation” found
patient was not permitted to submit a grievance, andhospitalstafffailedtofollowgrievanceprocess,
o suspected drug diversion involving a patient and LPN,and
o reportsofsexualactivitybetweentwopatients.
As in past instances, Sharpe devised and submitted a plan ofcorrection to remedy some of the deficiencies, but noncompliancepersistedwithCodeofFederalRegulations(C.F.R.)§482.61oftheCMSStateOperationsManualforPsychiatricHospitals.Thissectionrequires:“The medical records maintained by a psychiatric hospital must permit determination of the degree and intensity of the treatment provided to individuals who are furnished services in the institution.”Theregulationfurther specifies that patient records should contain information suchas “…treatment goals, changes in status of treatment and discharge planning, and follow-up and the outcomes experienced by patients.”
InSharpe’scase,CMS’reviewofmedicaltreatmentplansfoundthatonepatient“…had no psychiatrist or nursing interventions,”whileanother patient “…was not receiving alcohol abuse treatment even though substance abuse was listed as a problem.”Treatmentplansfailedtoidentifytreatmentgoals,didnotspeaktotheindividualneedsofthepatients,didnotconsistentlycontainproperplansforfollow-upcare,andfailedtomeetstandardsfortherapeuticcare(i.e.:patientswerenotgoingtotherapyandrecordsdidnotaddressalternativetreatments).Ultimately,thecontinuedviolationofC.F.R.§482.61ledCMStoterminateSharpe’sMedicareagreement,effectivelystoppingpaymentforservicesfurnishedtopatientsadmittedafterSeptember28,2017.Asaresult,SharpecouldnolongeradmitMedicareorMedicaidpatients.
Ultimately, the continued violation of C.F.R. §482.61 led CMS to terminate Sharpe’s Medicare agreement, effec-tively stopping payment for services furnished to patients admitted after September 28, 2017.

pg. 12 | West Virginia Legislative Auditor
William R. Sharpe, Jr. Hospital
Following the termination notice from CMS, Sharpe began transferring civil patients out of the hospital and tran-sitioning its patient population to 100 percent forensic.
Consequences of Decertification Impacted Diversions and Patient Population.
Following the termination notice from CMS, Sharpe begantransferringcivilpatientsoutofthehospitalandtransitioningitspatientpopulation to100percent forensic.Theactof relocatingpatientswhowouldhaveotherwisegonetoSharpeisknownas“diversion.”InSharpe’scase,diversionsgenerallyoccurwhenthehospitaldoesnothaveabedavailable,althoughfiscalyear(FY)2018-2019sawaheightenednumberofcivilpatientdiversionsduetothefacilitybeingdecertifiedbyCMS(seeTable3).AccordingtoSharpe’sCEO,“In response to the decertification, the civil population was diverted to other facilities and Sharpe Hospital began accepting an increased number of forensic patients.”
Manyfactorscontributetothecostofdivertingpatients,andtheexpenses associated with patients who are diverted to other facilitiesremains Sharpe’s responsibility even though the individual willphysicallyreceivetreatmentatanotherhospital.Sharpe’sCEOexplains,“As a rule, the diversion of a civil patient occurs at the time or shortly after the probable cause hearing. Sharpe Hospital staff are contacted by the community mental health center and Sharpe makes referrals to diversion facilities, attempting to place the patient in the facility that is closest to their home. The diversion per diem covers room and board and all psychiatric treatment. Additional expenses include medical services (professional fees, procedure fees, and emergency room fees) required by the patient for medical, vision, and dental care, over and above what is able to be provided in an inpatient psychiatric setting.”Majorconsequencesofdiversionsaretwo-fold:
• Thecostofpatient treatmentataprivate facilitycanbehigherinsomescenarioscomparedtotreatmentadministeredbyastatehospitalsuchasSharpe.TheperdiemratefortreatingapatientdivertedfromSharpetoanotherfacilitycancostupto$896,whiletheaveragecost to treatapatientatSharpe forFY2017–2018was$856perday.Sharpe’sCEO,however,estimatesthatthesecostswillbelowerforFY2019duetoanincreaseinthepatientcensus,whichhelpsthehospitalcoveroperationalexpenses.
• Physically transporting patients to a diversion facility cangeneratetravelexpendituresthatwouldotherwisenotoccur,andthe geographical distance to a diversion hospital maymake itdifficultforthepatient’sfamilymemberstovisit.
Asa result,civildiversioncosts significantly impactedSharpe.Table3reflectsthenumberofpatientsadmittedanddivertedfromSharpeHospitalduringFY2015-2019,aswellasthetrendindiversionexpenses.
The cost associated with patients who are diverted to other facilities remains Sharpe’s responsibility even though the individual will physically receive treatment at another hospital.
Performance Evaluation & Research Division | pg. 13
Performance Review
Eleven (11) different hospitals served as destinations for Sharpe’s civil diver-sions during FY 2015-2019.
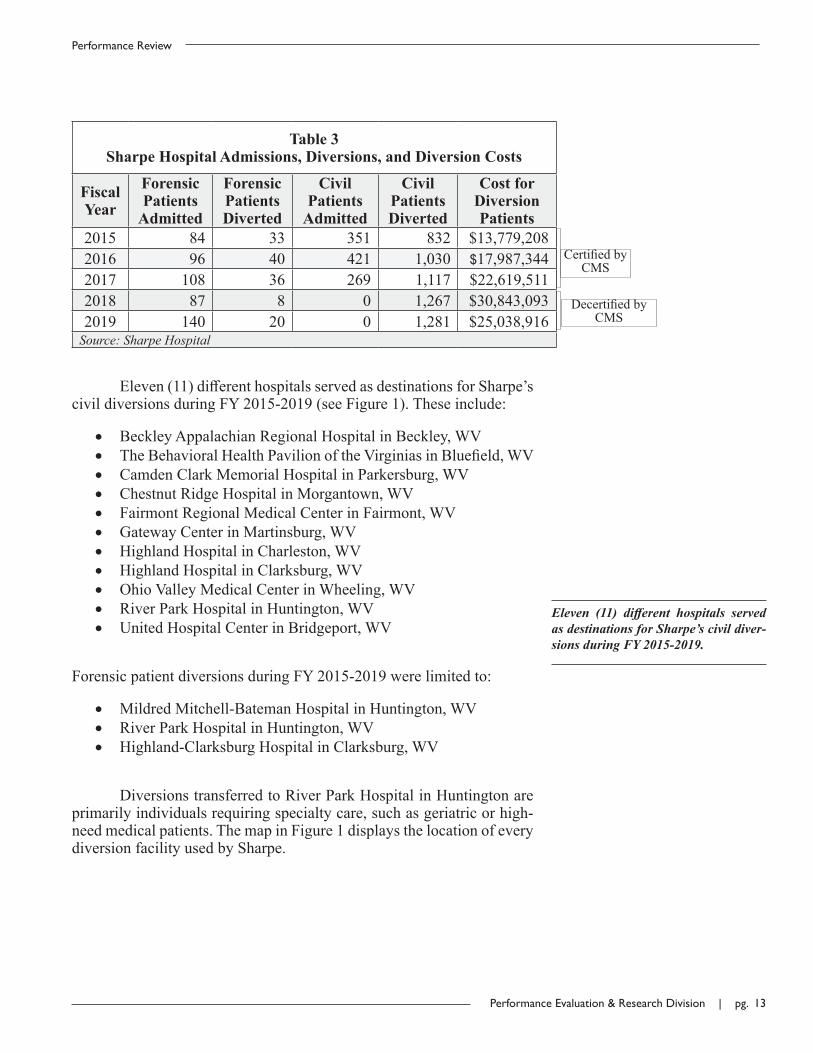
Table 3Sharpe Hospital Admissions, Diversions, and Diversion Costs
FiscalYear
Forensic Patients
Admitted
Forensic PatientsDiverted
Civil Patients
Admitted
Civil Patients Diverted
Cost for Diversion Patients
2015 84 33 351 832 $13,779,2082016 96 40 421 1,030 $17,987,3442017 108 36 269 1,117 $22,619,5112018 87 8 0 1,267 $30,843,0932019 140 20 0 1,281 $25,038,916
Source: Sharpe Hospital
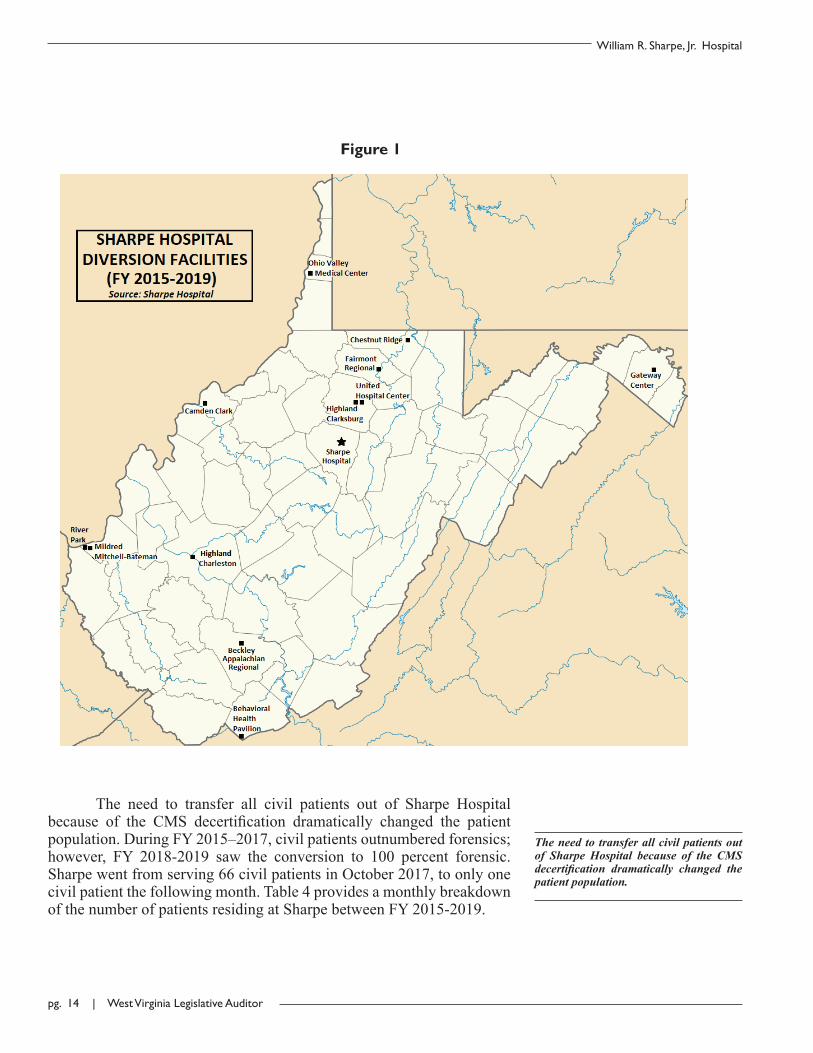
Eleven(11)differenthospitalsservedasdestinationsforSharpe’scivildiversionsduringFY2015-2019(seeFigure1).Theseinclude:
• BeckleyAppalachianRegionalHospitalinBeckley,WV• TheBehavioralHealthPavilionoftheVirginiasinBluefield,WV• CamdenClarkMemorialHospitalinParkersburg,WV• ChestnutRidgeHospitalinMorgantown,WV• FairmontRegionalMedicalCenterinFairmont,WV• GatewayCenterinMartinsburg,WV• HighlandHospitalinCharleston,WV• HighlandHospitalinClarksburg,WV• OhioValleyMedicalCenterinWheeling,WV• RiverParkHospitalinHuntington,WV• UnitedHospitalCenterinBridgeport,WV
ForensicpatientdiversionsduringFY2015-2019werelimitedto:
• MildredMitchell-BatemanHospitalinHuntington,WV• RiverParkHospitalinHuntington,WV• Highland-ClarksburgHospitalinClarksburg,WV
DiversionstransferredtoRiverParkHospitalinHuntingtonareprimarilyindividualsrequiringspecialtycare,suchasgeriatricorhigh-needmedicalpatients.ThemapinFigure1displaysthelocationofeverydiversionfacilityusedbySharpe.
DecertifiedbyCMS
CertifiedbyCMS
pg. 14 | West Virginia Legislative Auditor
William R. Sharpe, Jr. Hospital
The need to transfer all civil patients out of Sharpe Hospital because of the CMS decertification dramatically changed the patient population.
The need to transfer all civil patients out of Sharpe Hospitalbecause of the CMS decertification dramatically changed the patientpopulation.DuringFY2015–2017,civilpatientsoutnumberedforensics;however, FY 2018-2019 saw the conversion to 100 percent forensic.Sharpewentfromserving66civilpatientsinOctober2017,toonlyonecivilpatientthefollowingmonth.Table4providesamonthlybreakdownofthenumberofpatientsresidingatSharpebetweenFY2015-2019.
Figure 1

Performance Evaluation & Research Division | pg. 15
Performance Review
Table 4Forensic and Civil Patients Served at Sharpe Hospital
FY 2015 – FY 2019
FiscalYear
Patient Type JUL AUG SEP OCT NOV DEC JAN FEB MAR APR MAY JUN AVG.
2015 Forensic 77 78 81 75 74 71 73 71 75 73 72 72 74Civil 97 95 100 106 98 106 98 96 106 118 101 103 102
2016 Forensic 77 79 76 78 76 77 74 67 70 68 65 70 73Civil 116 111 123 114 93 99 112 114 121 128 125 116 114
2017 Forensic 70 71 67 69 68 74 73 71 75 77 75 82 73Civil 121 126 121 128 118 106 129 107 118 105 109 106 116
2018 Forensic 77 69 70 82 99 100 104 106 98 101 102 116 94Civil 99 102 85 66 1 1 1 1 1 1 1 1 30
2019 Forensic 121 120 120 121 119 119 125 128 136 133 135 130 126Civil 1 1 1 0 0 0 0 0 0 0 0 0 0
Source: Sharpe Hospital
Figure 2, provided by Sharpe’s CEO, illustrates the forensicinpatientcensusatthehospitalduringFY2015-2019,withcomparisonsbetweenadmissionsanddischarges.
Thenumberofforensicadmissions,discharges,andinpatientsatSharpeincreasedin2019incomparisonto2015,withallthreecategoriesreachingastatisticalfive-yearhigh.

pg. 16 | West Virginia Legislative Auditor
William R. Sharpe, Jr. Hospital
Sharpe’s expenditures and revenues were significantly impacted after los-ing CMS certification.
The Loss of Certification Triggered an Increase in Expenditures, Significant Loss in Revenues, and the Implementation of New Standards That Caused Some Employee Turnovers.
Sharpe’sexpendituresandrevenuesweresignificantlyimpactedafterlosingCMScertification.Theexpendituresnotablyincreasedasthenumberofdiversionsincreased.Forexample,inFY2015,31percentoftotalexpenditureswereduetodiversioncosts,whereasinFY2019,40percentoftotalexpenditureswerearesultofdiversions.
Because Sharpe was no longer eligible to bill Medicare orMedicaid after losing CMS certification, the hospital’s revenuesdramaticallydecreasedasthenumberofcivilpatientsdwindled.Sharpe’sCEOexplains,“Bateman and diversion facilities would be able to bill those sources for care provided, and given the structure of the diversion agreements, the state would not have to pay for days covered by the committed persons insurance. Civil patients are billed to their insurance coverage for the days that they meet medical necessity. There is no payer source for Forensic patients, they are 100% State funded.”Table5presentsSharpe’scompleteexpendituresandrevenuesfromFY2015–2019.
Table 5Sharpe Hospital Expenditures and Revenues
Fiscal Year Expenditures Revenues2015 $41,162,719 $12,495,9912016 $52,003,890 $12,712,5752017 $55,951,701 $12,559,8502018 $67,994,767 $3,713,1132019 $63,995,027 $45,640
Source: OASIS
When certified by CMS, Sharpe’s revenue stream normallyincludesMedicaidDisproportionateShareHospital(DSH)payments,ordisbursementsallottedtoqualifyinghospitalsthatservealargenumberofMedicaidanduninsuredindividuals.Duringthedecertificationperiod,theDSHpaymentshistoricallyallocatedtoSharpewerere-allocatedtoBatemanHospital.TheabsenceofthesepaymentstoSharpeduringpartofFY2018andallofFY2019isanimportantfactorwhenconsideringthereductioninrevenue.Priortodecertification,Sharpewasreceivinganannualaverageof$10.8millioninDSHallotment.
As a central part of the recertification strategy, the GreeleyCompany(Greeley)consultingfirmofDanvers,Massachusettswashiredtoprovide education, credentialingmanagement, external peer review,

Performance Evaluation & Research Division | pg. 17
Performance Review
Despite the contract with Greeley and issues with turnovers, Sharpe ultimate-ly pursued a successful path to recerti-fication over the next two years.
andsolutionsforSharpeanditsstafftocorrectthedeficienciescitedbyCMS.Greeley consultants first arrived at SharpeHospital onOctober30, 2017. They provided services throughout FY 2018 and FY 2019,ultimatelybillingSharpeforatotalof$1.5million.Whilecollaboratingwith Greeley and exploring new strategies to achieve recertification,Sharpeimplementedseveralchangestothehospital’sinternaloperations,which included enhancing expectations in terms of the quality of itsemployees. After introducing this new employee standard, severalturnoversoccurred,eitherduetoresignationsorchangesproactivelymadebySharpe’sadministrationtoimprovetheeffectivenessofkeypositionswithinthestaff.AccordingtoSharpe’sCEO,“Employment numbers were not significantly impacted by the loss of CMS certification. However, dissatisfaction with many of the changes Sharpe Hospital made in order to improve the supporting processes necessary for re-certification are thought to contribute to a large percentage of the 2017-2018 turnover.”
Tables6and7detailSharpe’semployee turnovers forFY2015-2019.Despite the contract with Greeley and issues with turnovers, Sharpeultimatelypursuedasuccessfulpathtorecertificationoverthenexttwoyears.
Table 6Sharpe Hospital Employee Turnovers
Fiscal Year 2015 2016 2017 2018 2019 - 8/31/2019*Resignations 24 46 62 42 27Retired 6 8 17 12 6Terminations 4 14 7 12 10Transfers 5 3 6 1 2Deaths 0 2 0 0 0Source: Sharpe Hospital
Table 7Reasons Given for Resignations
Fiscal Year 2015 2016 2017 2018 2019 - 8/31/2019*OtherEmployment 11 34 28 22 15
Personal 5 4 13 12 6No Reason Given 8 4 11 0 2
Dissatisfied 0 2 6 6 1School 0 2 1 1 0Relocated 0 0 3 1 3Source: Sharpe Hospital* Resignations for other employment were generally for better wages or more flexible hours.
According to Sharpe’s CEO, “Dissat-isfaction with many of the changes Sharpe Hospital made in order to im-prove the supporting processes neces-sary for re-certification are thought to contribute to a large percentage of the 2017-2018 turnover.”

pg. 18 | West Virginia Legislative Auditor
William R. Sharpe, Jr. Hospital
Sharpe Began Corrective Strategies Immediately After Losing Certification.
In addition to hiring Greeley, Sharpe formed a RecertificationOversightCommittee(ROC)inJanuary2018thatbeganholdingregularmeetingswithGreeleyrepresentatives,Sharpe’sCEO,andotherrankingmembers of hospital staff. Sharpe’s formal Performance ImprovementTeam, a complementary body to the ROC, additionally focused onidentifying multiple areas for review and correction, and delegatedstafftoaccomplishstatedgoalswithinatargettimeframe.Progresswasregularlymonitoredanddocumented.
Twelve (12) different designated areas of importance wereidentifiedasthemaintopicsofconcentrationforSharpetoreviewandrevise as an approach to reacquiring CMS accreditation. These areasincludedleadershipandoversight,environmentofcare,electronicmedicalrecords,patientrights,nursing,andtreatmentplanning.Bypinpointing,isolating, and identifying areas requiring correction for the hospital’smostimportantcomponents,theROCintroducedaspecific,formulatedapproachforSharpe’sstafftotroubleshootpotentiallydeficientsegmentsofthefacility.
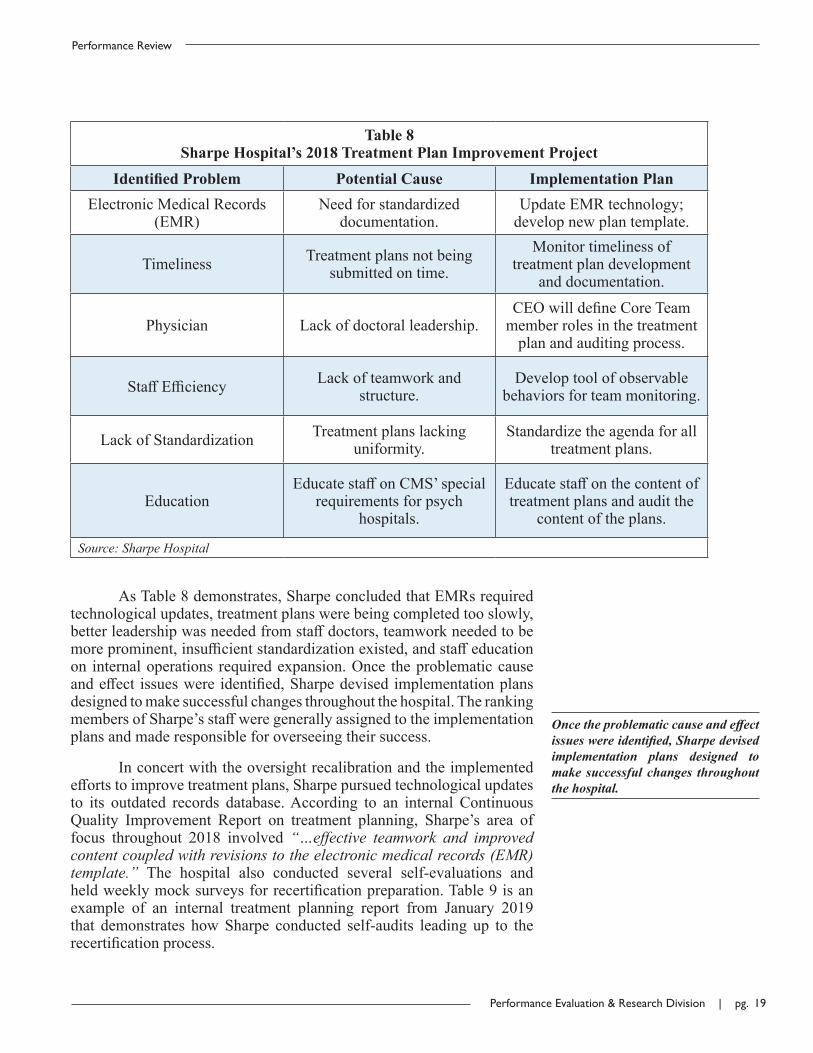
Table 8 was adapted from a January 2018 ComprehensiveTreatmentPlanPerformanceImprovementProjecttemplate.Itexemplifieshow Sharpe’s leadership approached the correctional phase of therecertificationprocess. In this example, sixdifferent internalproblemswere identified and juxtaposedwith the potential causes forwhy theyexistedwithinthehospital,aswellasthecorrelatingactionitemsneededtomakethechangessuccessful.
In addition to hiring Greeley, Sharpe formed a Recertification Oversight Committee (ROC) in January 2018 that began holding regular meetings with Greeley representatives, Sharpe’s CEO, and other ranking members of hospital staff.
Performance Evaluation & Research Division | pg. 19
Performance Review
Table 8Sharpe Hospital’s 2018 Treatment Plan Improvement Project
Identified Problem Potential Cause Implementation PlanElectronicMedicalRecords
(EMR)Needforstandardized
documentation.UpdateEMRtechnology;developnewplantemplate.
Timeliness Treatmentplansnotbeingsubmittedontime.
Monitortimelinessoftreatmentplandevelopment
anddocumentation.
Physician Lackofdoctoralleadership.CEOwilldefineCoreTeammemberrolesinthetreatmentplanandauditingprocess.
StaffEfficiency Lackofteamworkandstructure.
Developtoolofobservablebehaviorsforteammonitoring.
LackofStandardization Treatmentplanslackinguniformity.
Standardizetheagendaforalltreatmentplans.
EducationEducatestaffonCMS’special
requirementsforpsychhospitals.
Educatestaffonthecontentoftreatmentplansandauditthe
contentoftheplans.
Source: Sharpe Hospital
AsTable8demonstrates,SharpeconcludedthatEMRsrequiredtechnologicalupdates,treatmentplanswerebeingcompletedtooslowly,betterleadershipwasneededfromstaffdoctors,teamworkneededtobemoreprominent,insufficientstandardizationexisted,andstaffeducationon internaloperations requiredexpansion.Once theproblematiccauseandeffect issueswere identified,Sharpedevised implementationplansdesignedtomakesuccessfulchangesthroughoutthehospital.TherankingmembersofSharpe’sstaffweregenerallyassignedtotheimplementationplansandmaderesponsibleforoverseeingtheirsuccess.
Inconcertwiththeoversightrecalibrationandtheimplementedeffortstoimprovetreatmentplans,Sharpepursuedtechnologicalupdatesto its outdated records database.According to an internal ContinuousQuality Improvement Report on treatment planning, Sharpe’s area offocus throughout 2018 involved “…effective teamwork and improved content coupled with revisions to the electronic medical records (EMR) template.” The hospital also conducted several self-evaluations andheldweeklymocksurveysforrecertificationpreparation.Table9isanexample of an internal treatment planning report from January 2019that demonstrates howSharpe conducted self-audits leading up to therecertificationprocess.
Once the problematic cause and effect issues were identified, Sharpe devised implementation plans designed to make successful changes throughout the hospital.

pg. 20 | West Virginia Legislative Auditor
William R. Sharpe, Jr. Hospital
On January 9, 2019, Sharpe passed an unannounced initial survey that determined its facility was in substan-tial compliance with major federal codes related to the CMS condition of participation.
Table 9Treatment Planning Improvement Results (2019)
Month Mar Apr May Jun Jul Aug Sep Oct Nov Dec YTDGoal (%) 100 100 100 100 100 100 100 100 100 100 100
PercentageofCompliantTreatment Plans
95 94 97 93 96 94 91 95 92 97 94
NumberAudited 364 2,934 3,626 3,239 2,440 3,564 2,183 441 363 261 19,415
NumberinCompliance 344 2,761 3,498 3,015 2,346 3,342 1,994 418 334 253 18,305
Source: Sharpe Hospital
Afterreviewingthestructureofitstreatmentplanteams,educatingstaff members on patient care plan content, and practicing numerousself-audits,Sharpereachedthesurveyreadinessphaseandsubmittedanapplicationforre-enrollmenttoCMSonMay11,2018.
Sharpe Hospital Regained CMS Certification in August 2019.
CMS regulations state that an entity that has lost certificationmayreapplyatanytime.However,42C.F.R.§489.57stipulatesthattheproviderisfirstrequiredtooperateforacertainperiodoftimewithoutrecurrence of the deficiencies which were the basis for the originaltermination,andprovidereasonableassurancethatthesedeficiencieswillnotrecur.Participationcanonlyresumeif theproviderorsupplierhasmaintainedcompliancewithprogramrequirementsduringthereasonableassuranceperiod.
OnJanuary9,2019,Sharpepassedanunannouncedinitialsurveythat determined its facility was in substantial compliance with majorfederalcodesrelatedto theCMSconditionofparticipation.Followingsuccessful reasonable assurance, Sharpe was subject to three othersurveys,completedonAugust14,2019,tofinalizerecertification.Zerodeficiencies were found by surveyors during this extended series ofaudits:
• An initial certification survey deemed Sharpe compliant withtheMedicare conditions of participation for hospitals and nodeficiencieswerecited.
After reviewing the structure of its treatment plan teams, educating staff members on patient care plan content, and practicing numerous self-audits, Sharpe reached the survey readiness phase and submitted an application for re-enrollment to CMS on May 11, 2018.

Performance Evaluation & Research Division | pg. 21
Performance Review
• An unannounced initial survey conducted by federal andstate surveyors deemed Sharpe compliant with conditions ofparticipation, including 42 C.F.R. §482.62, Requirements forPsychiatricHospitals,relatedtotreatmentplans.
• Based on review of facility documentation, staff interviews,observations and performance testing, Sharpe was deemedcompliantwiththeLifeSafetyCodeandemergencypreparednessrequirements.
OnSeptember10,2019,SharpereceivedarecertificationletterfromCMSdeclaringtheeffectivedateofparticipationintheMedicareprogramtobeAugust14,2019.
Sharpe Hospital Plans to Reach Full Capacity in the Future.
NowthatSharpecanbeginacceptingcivilpatientsagain,futureplansincludeachangeinthepatientpopulation.AccordingtoSharpe’sCEO, “The plan underway is to open a civil unit at the hospital on December 9, (2019) with an approximate capacity of 28 patients. Efforts are currently underway to complete hiring and training of new staff for the civil unit.”Thefuturecivilunitwillbe locatedonN-2,whichcomprisespartoftherecentlycompleted50-bedaddition.Sharpeexpectstoacceptmorecivilpatientsbeyondtheinitial28inthefuture.Sharpe’sCEOadds,“It is anticipated that the total number of forensic patients receiving hospital care will diminish and it is anticipated that N1 (a unit that currently serves forensics) will convert to civil commitments that will increase available capacity to 50.”
ExternalforcesmayinterruptordelaySharpe’stransitiongoalforcivilpatients.Duetothenatureofmentallyillpatients,noteveryindividualadmittedtoSharpecansafelytolerateroomingwithanotherpatient.Inthesecases,theotherbed,or“blockedbed,”remainsvacant,andSharpeispreventedfromfilling100percentofitsbeds.Thenumberofpatientsthatcannotbehousedwitharoommateistraditionallyinconsistentanddifficulttopredict.Sharpe’sCEOelaborates,“The number varies based on the unique clinical and safety concerns of various patients, including aggression/violence, inappropriate sexual behavior, and psychosis. The number of blocked beds usually runs from a low of 5 to a high of 10 or more depending on patient safety needs.”Otherwise, Sharpe plans tomakeaprominentefforttofulfillthereintroductionofcivilpatientstothehospitalwithoutmajorinterruption.
On September 10, 2019, Sharpe re-ceived a recertification letter from CMS declaring the effective date of participation in the Medicare pro-gram to be August 14, 2019.

pg. 22 | West Virginia Legislative Auditor
William R. Sharpe, Jr. Hospital
Conclusion
Sharpe Hospital’s loss of CMS certification in September2017reduceditsrevenuestream,increasedcosts, impactedtheoverallpatient population, escalated the number of diversions, inspiredsignificantinternaloperationalchanges,andledsomestaffmemberstoresign employment.Without the ability to participate in theMedicareprogram,Sharpehad to transition its patient population to completelyserveforensics,andthus,removeanddivertanycivilpatientsfromitsfacility.SharpeincurredotherexpensesbyhiringGreeleyconsultantstomake the necessary changes for recertification.Although the resultinginternal changesnegatedmatters by causing a largepercentageof the2017-2018employeeturnover,thechangesultimatelyledtosuccessfulrecertificationandfutureplanstodiversifythepatientpopulation.Basedontherecentrecertification,Sharpehastheabilitytomaintainitsgoalsbycontinuingcarefulandresults-drivenoversightforallmajorhospitaldepartments, and by extending the solutions, training, and skill setsfosteredbyGreeley’sservices.
Recommendation
1. The Legislative Auditor recommends that Sharpe Hospital continue to follow all CMS guidelines pertaining to hospital regulations, psychiatric facility rules, and Life Safety Code to maintain certification and participation in the Medicare program. Emphasis should be placed on satisfying regulations related to treatment plans.
Based on the recent recertification, Sharpe has the ability to maintain its goals by continuing careful and results-driven oversight for all major hospital departments, and by extend-ing the solutions, training, and skill sets fostered by Greeley’s services.

Performance Evaluation & Research Division | pg. 23
Performance Review
During a standard CMS survey of general hospitals, federal guidelines require the auditor to check the fa-cility for compliance with applicable federal laws related to the health and safety of patients, which includes the ADA.
ISSUE 2
The survey results stating, “This facil-ity is in compliance with the Medicare Conditions of Participation for Hos-pitals and no deficiencies were cited as a result of the initial certification survey,” is the equivalent to declaring Sharpe to be ADA compliant.
Sharpe Hospital Is ADA Compliant After No Citations Issued by the Centers for Medicare and Medicaid Services.
Issue Summary
During a standard CMS survey of general hospitals, federalguidelinesrequiretheauditortocheckthefacilityforcompliancewithapplicablefederallawsrelatedtothehealthandsafetyofpatients,whichincludestheADA.Basedonthisprotocol,SharpeHospitalisdeterminedto be in compliancewith theADA because the facilitywas not citedforfederal lawdeficienciesduringitsmostrecentsuccessfulsurveyinAugust2019.TheLegislativeAuditorrecommendsthatSharpeHospitalcontinuetocomplywithallADAstandardsapplicabletoitsfacility.
CMS Reviews for Compliance With the Americans With Disabilities Act During Its Surveys.
Accordingto42C.F.R.§482.11(a)fromtheCMSsurveymanualfor hospital guidelines, “The hospital must be in compliance with applicable Federal laws related to the health and safety of patients.” Because theADA is a federal lawbydefinition, thisqualifies it as an“applicable Federal law related to the health and safety of patients,”assubject toCMS requirements.CMS survey procedures for confirmingcompliancewiththiscodeinclude:
• InterviewtheCEO,orappropriate individualdesignatedbythehospital,todeterminewhetherthehospitalisincompliancewithfederallawsrelatedtopatienthealthandsafety.
• Refer or report noted noncompliance with federal laws andregulations to the appropriate agency having jurisdiction (e.g.,hazardouschemical/wasteissuestoEPA,etc.).
Sharpe Has Not Been Cited for Non-Compliance By CMS.
Sharpe’sADAcompliancecanbeconfirmedbythemostrecentsuccessfulCMSsurveys,completedonAugust14,2019.CMSguidelinesrequirethehospitaltomeetallapplicableFederallawrequirements,andsurveyorsaretaskedwithreportingviolationsofthiscodeintheeventofnoncompliance.Bythisstandard,theabsenceofacitationforADAnon-compliance indicates Sharpe is in full compliance.The survey resultsstating,“This facility is in compliance with the Medicare Conditions of Participation for Hospitals and no deficiencies were cited as a result of the initial certification survey,”istheequivalenttodeclaringSharpetobeADAcompliant.

pg. 24 | West Virginia Legislative Auditor
William R. Sharpe, Jr. Hospital
Sharpe would have been cited for violations and reported to the appro-priate agency had CMS surveyors found ADA noncompliance deficien-cies.
Conclusion
CMS auditors check forADA compliance as a component ofthe hospital survey protocol. Sharpe Hospital is compliant with theADAbasedonitsabilitytosuccessfullypassarecentCMSsurveythatrequiredthefacilitytocomplywithapplicablefederallawsrelatedtothehealthandsafetyofpatients.SharpewouldhavebeencitedforviolationsandreportedtotheappropriateagencyhadCMSsurveyorsfoundADAnoncompliance deficiencies. Sharpe should also continue to maintainADA compliance in the event of future renovation or constructionprojectswithinitsexistingunits.
Recommendation
2. The Legislative Auditor recommends that Sharpe Hospital continue to comply with all ADA standards applicable to its facility.

Performance Evaluation & Research Division | pg. 25
Performance Review
Appendix ATransmittal Letter

pg. 26 | West Virginia Legislative Auditor
William R. Sharpe, Jr. Hospital
Performance Evaluation & Research Division | pg. 27
Performance ReviewAppendix B
Objectives, Scope and Methodology
The Performance Evaluation and Research Division (PERD) within the Office of the LegislativeAuditorconductedthisPerformanceReviewofWilliamR.Sharpe,Jr.Hospital(Sharpe)aspartoftheAgencyReviewoftheDepartmentofHealthandHumanResources(DHHR)asrequiredandauthorizedbytheWestVirginiaPerformanceReviewAct,Chapter4,Article10,oftheWest Virginia Code (WVC),asamended.ThepurposeofSharpeHospitalistoprovidequalitytreatmentandhealthcaretopatientseithercommittedtothehospitalthroughcivilcommitmentor,inthecaseofforensicpatients,orderedthroughthejudicialsystem.
Objectives
Theobjectivesof this revieware todeterminehowSharpewas impactedafter losingcertificationfromtheCentersforMedicareandMedicaidServices(CMS),andwhetherthehospitalcomplieswiththeAmericanswithDisabilitiesAct(ADA).
Scope
The performance review included an assessment of Sharpe Hospital’s major internal operationalcomponentssuchasexpenditures,revenues,employmenttrends,patientpopulations,patientdiversions,andthefacility’stimelinewithrelationtoCMSbetweenFY2015andFY2019.Forthesecondobjective,evidencewas collected and assessed to confirm Sharpe’s current compliance with theADA, including 42 C.F.R.§482.11(a) fromtheCMSsurveymanual forhospitalguidelinesandotherpertinent regulations involvingphysicalaccessibility.
Methodology
PERDgatheredandanalyzedseveralsourcesofinformationandconductedauditprocedurestoassessthesufficiencyandappropriatenessoftheinformationusedasauditevidence.Theinformationgatheredandauditproceduresaredescribedbelow.
TestimonialevidencewasgatheredforthisreviewthroughinterviewswiththeChiefExecutiveOfficer(CEO)ofSharpeHospitalandconfirmedbywrittenstatements.PERDstaffvisitedSharpeonJuly11,2019toviewthefacility,obtaininformationprovidedbytheCEO,andmeetwithrelevanthospitalstaff.PERDcollectedandanalyzedSharpe’smeetingminutes,internalcommitteetemplates,budgetaryinformation,annualreports, staff training procedures, awritten description of the different facility units, and correspondencewithCMSincludingakeyre-enrollmentapplication.RevenueandexpenditureamountswereretrievedfromtheOASISapplication,includingthetotalexpensesSharpeallottedtoanoutsidehealthcaresolutionsfirm.OtherdocumentationrelatedtobasicdetailsregardingSharpeandotherstatehospitalswasobtainedfromtheofficialWVDHHRwebsite.
PERD also collected documentation from theCMS regional office in Philadelphia, Pennsylvania,includingaseriesofsurveysconductedatSharpeHospitalbetweenFY2015andFY2019,surveymanuals,the written CMS auditing standards, and official correspondence between Sharpe and CMS. Writtencorrespondence between PERD and the regional CMS contact was also used to document and confirmtimelines.Additionally,PERDcollectedevidencetoachievethesecondobjectivebyobtainingADA-relatedtestimonialsfromCMSarchivesandtheFederalRegisteroftheU.S.NationalArchivestocorroboratetheinterpretivefederalguidelinesthatwereusedtoconfirmSharpe’scompliancewiththeADA.

pg. 28 | West Virginia Legislative Auditor
William R. Sharpe, Jr. Hospital
Weconducted this performance audit in accordancewith generally accepted government auditingstandards. Those standards require that we plan and perform the audit to obtain sufficient, appropriateevidencetoprovideareasonablebasisforourfindingsandconclusionsbasedonourauditobjectives.Webelievethattheevidenceobtainedprovidesareasonablebasisforourfindingsandconclusionsbasedonourauditobjectives.
Performance Evaluation & Research Division | pg. 29
Performance ReviewAppendix C
Agency Response

pg. 30 | West Virginia Legislative Auditor
William R. Sharpe, Jr. Hospital

Performance Evaluation & Research Division | pg. 31
Performance Review

pg. 32 | West Virginia Legislative Auditor
William R. Sharpe, Jr. Hospital

WEST VIRGINIA LEGISLATIVE AUDITOR
PERFORMANCE EVALUATION & RESEARCH DIVISION
Building 1, Room W-314, State Capitol Complex, Charleston, West Virginia 25305
telephone: 1-304-347-4890 | www.legis.state.wv.us /Joint/PERD/perd.cfm | fax: 1- 304-347-4939