Per-oral Endoscopic Myotomys3.gi.org/wp-content/uploads/2015/03/15ACG_LGS_Regional_Course... ·...
23
Abraham Mathew, MD, FACG POEM with the Flexible Scope Abraham Mathew MD, MSc Professor of Medicine Per-oral Endoscopic Myotomy ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology 1
Transcript of Per-oral Endoscopic Myotomys3.gi.org/wp-content/uploads/2015/03/15ACG_LGS_Regional_Course... ·...

Abraham Mathew, MD, FACG
POEM with the Flexible Scope
Abraham Mathew MD, MScProfessor of Medicine
Per-oral Endoscopic Myotomy
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
1

Abraham Mathew, MD, FACG
Objectives
• Review diagnosis and management of h l i d Z k ’ di ti lachalasia and Zenker’s diverticulum
• Describe the benefits and risk of treatment strategies
• Demonstrate endoscopic myotomy techniquetechnique.
Achalasia
• Motor disorder of esophagus• Frequency: 1/100000• Autoimmune neuron degeneration
– Excitatory nerves variable affected– Inhibitory nerves invariably affected
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
2

Abraham Mathew, MD, FACG
Symptoms
• Dysphagia 82-100%• Regurgitation/aspiration 60-80%• Chest pain, esophageal type 17-95%• Weight loss 32%• Minor symptoms:
• Heartburn, halitosis, slow eating, stereotypical manoeuvers at eating, inability to burp, dental caries, nocturnal coughing or choking
Diagnosis
• SymptomatologyBarium swallow• Barium swallow
• Bird beak, sigmoid esophagus, diverticulum, absence of gastric gas bubble
• Esophageal manometry• Sensitive, picks up early
• EGD• More than diagnosis, rules out pseudo achalasia
• CT/EUS• With significant weight loss
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
3

Abraham Mathew, MD, FACG
Subtypes of Achalasia – diagnosed by HREM
Type INo distal
pressurization
Type IIPan esophageal
pressurization
Type IIISpastic
contractions
Rohof, WO et al: Outcomes of treatment for achalasia depend on manometric subtype. Gastroenterol 2013; 144: 718-25
Types of Achalasia
• EG outlet obstruction: treated like h l iachalasia
– Normal peristalsis
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
4

Abraham Mathew, MD, FACG
Treatments
• Incurable disease– Traditional treatment more effective for
dysphagia than for chest pain
Treatment
• MedicationsC l i h l bl k• Calcium channel blockers: poor response
• Endoscopic• Botox• Pneumatic dilations
• Surgicalg• Heller Myotomy• Trans esophageal Endoscopic Myotomy• esophagectomy
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
5

Abraham Mathew, MD, FACG
Figure 3 Type II achalasia has a higher success rate compared with type I achalasia ( P < .01) and type III achalasia (P < .001), as shown in a Kaplan–Meier curve.
Wout O. Rohof , Renato Salvador , Vito Annese , Stanislas Bruley des Varannes , Stanislas Chaussade , Mario Costan...
Outcomes of Treatment for Achalasia Depend on Manometric Subtype
Gastroenterology, Volume 144, Issue 4, 2013, 718 - 725
http://dx.doi.org/10.1053/j.gastro.2012.12.027
Pneumatic Dilatation
• Dilatation to 30 – 40 mm90% ff ti• >90% effective
• Advantages• OP procedure, endoscopic• Immediate symptom relief
• Disadvantagesg• Need fluoroscopy• Technical skill, 1-3 sessions• 1% - 15% Perforation, 33% complications
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
6

Abraham Mathew, MD, FACG
Pneumatic dilation
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
7

Abraham Mathew, MD, FACG
Heller Myotomy
• Open and laparoscopic techniques• >90% effective
• Advantages• Recurrence rates lower
• Disadvantage• Mobilization of GEJ attachments
2% 5% Perforation• 2% - 5% Perforation• Post fundoplication syndrome
• Surgery most costly– cost-effective if relief lasts >10 years
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
8

Abraham Mathew, MD, FACG
Surgery vs PD
• Two small, randomized studies, 1 yr f/u• first (16 PD, 14 LM) : no difference• second (26 PD, 25 LM) : 6 vs 1 failure (p=0.04)
• European achalasia trial :Randomized• 94 PD (3.0 & 3.5 cm) vs106 to LM with Dor
– recurrent symptoms after PD retreated X 3• comparable success at 2 years• 92% for dilation and 87% for myotomy.
• Canadian longitudinal : 1741 patientsg• cumulative risk of subsequent treatment after 1, 5 and
10 years – 36.8%, 56.2% and 63.5% after PD– 16.4%, 30.3% and 37.5% after initial myotomy
» hazard risk: 2.37; CI 1.86 to 3.0)
Figure 4 Kaplan–Meier curves comparing PD and LHM are shown for the 3 subtypes for up to 60 months after treatment. Success rates are comparable in type I achalasia ( P = .84). Pneumodilation has a significantly higher success rate in type II achalasia ( ...
Wout O. Rohof , Renato Salvador , Vito Annese , Stanislas Bruley des Varannes , Stanislas Chaussade , Mario Costan...
Outcomes of Treatment for Achalasia Depend on Manometric Subtype
Gastroenterology, Volume 144, Issue 4, 2013, 718 - 725
http://dx.doi.org/10.1053/j.gastro.2012.12.027
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
9

Abraham Mathew, MD, FACG
Totally Endoscopic Esophageal Myotomy
• Liquid diet for several days• Consider antifungals• NPO past midnight• Intra-procedure antibiotics
Totally Endoscopic Esophageal Myotomy
• Trans esophageal myotomy• > 90% effective• > 90% effective
• Advantages• Totally endoscopic• Easy redo• Myotomy length to your hearts desire!
• Disadvantages• New• Skill for advanced tissue dissection and basic
endoscopy• Acid reflux 5-30%
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
10

Abraham Mathew, MD, FACG
Post procedure
• Pneumoperitoneum 30% : caused by the non-pressure controlled insufflation of carbon pdioxide
• Post procedural care • admission for one night• water soluble contrast X-ray the next morning • semi-solid diet for 14 days after the procedure. • Routine upper endoscopy 1 or 2 days byRoutine upper endoscopy 1 or 2 days by
some centers• Acid suppression for 2 weeks postoperatively• Barium study in 3-4 weeks
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
11

Abraham Mathew, MD, FACG
2 week follow up
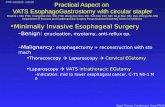
Other applications
• Louis H, Covas A, Coppens E, Deviere J. Distal esophageal spasm treated byDistal esophageal spasm treated by peroral endoscopic myotomy. Am J Gastroenterol 2012;107:1926–7.
• Shiwaku H, Inoue H, Beppu R et al. Successful treatment of diffuse esophageal spasm by peroralendoscopic myotomy. GastrointestEndosc 2013;77:149–50.
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
12

Abraham Mathew, MD, FACG
Algorithm
• Short life expectancy or poor surgical did t B tcandidate: Botox
• Surgical candidate: offer POEM vs Pneumatic dilation vs Heller
• Patients choice
Decision making
• Prefer not to stay for a day, do not i d th d + 2 5%mind more than one procedure + 2-5%
perforation: Pneumatic dilation• Prefer one stop shopping: Heller or
POEM• Prefer Minimal invasion over• Prefer Minimal invasion over
established procedure: POEM
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
13

Abraham Mathew, MD, FACG
Mega esophagus
• >6–9 cm with a horizontal fi ticonfiguration
– failure of myotomy is controversial – up to 50% having persistent dysphagia – esophagectomy for the failures
• 2–5%
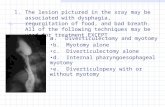
Per oral –upper- esophageal endoscopic myotomy
• Zenkers diverticulotomy
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
14

Abraham Mathew, MD, FACG
Technique of Diverticulotomy
Pre Post
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
15

Abraham Mathew, MD, FACG
Pre procedure
Pre op Post op
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
16

Abraham Mathew, MD, FACG
Pre op Post op
Pre op Post op
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
17

Abraham Mathew, MD, FACG
Pre op Post op
Pre op Post op
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
18

Abraham Mathew, MD, FACG
Pre op Post op
Pre op Post op
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
19

Abraham Mathew, MD, FACG
Pre op Post op
Outcome
• > 90% near total resolution of tsymptoms
• Pouch persists, but empties much better
• More than one session may be needed may depend on initialneeded, may depend on initial aggressiveness.
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
20

Abraham Mathew, MD, FACG
POEM vs Lap Heller’s
• All patients are candidates
• All patients are candidatescandidates
– Botox: no added difficulty
• Easy redo• Complication1-5 %• Low recurrence
• (5yr follow up or less)
candidates– Botox: difficult
procedure• Re do is difficult• Complication :1-5 %• Low recurrence
• Long follow up(5yr follow up or less)
• GEJ intact• Extended myotomy
easy
Long follow up
• Fundoplication must• Extended myotomy
difficult
POEM vs pneumatic
• Similar efficacy• Similar complication rates• Perforation managed by endoscopy• Endoscopic suturing device may
change equationi• Poem likely have recurrence rate
similar to laparoscopic myotomy
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
21

Abraham Mathew, MD, FACG
Recurrence of dysphagia
• Result of an incomplete myotomy : gastric sideside– Repeat pneumatic dilation– POEM
• Other factors– esophageal scarring – obstruction by the fundoplication– Mega esophagus– severe GERD
Efficacy of POEM
Study N Outcome measure Reported efficacy Follow-up
Inoue, 2010 17 Dysphagia score (0–10) 1.3 5 months average
Von Renteln, 2012 16 Eckardt score ≤3 94% 3 months
Von Renteln, 2013 70 Eckardt score ≤3 97%, 89% and 82% 3, 6 and 12 months
Zhou, 2012 205 Dysphagia relief 97% 8.5 months average
Costamagna, 2012 11 Eckardt score ≤3 91% 1 month
Minami, 2013 28 Eckardt score ≤3 100% 3 months
Swanstrom, 2012 18 Eckardt score ≤3 94 and 100% 1 and 6 months
Hungness, 2013 18 Eckardt score ≤3 89% 6 months average
Lee, 2013 13 Eckardt score ≤3 100% 3 months
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
22

Abraham Mathew, MD, FACG
Thank you for your attention
Questions?
ACG/LGS Regional Postgraduate Course - New Orleans, LA Copyright 2015 American College of Gastroenterology
23