Peptic Ulcer Diseases.. Necrotic Mucosal defects that extends through the Muscularis mucosae and...
27
Peptic Ulcer Diseases .
-
Upload
clara-casey -
Category
Documents
-
view
221 -
download
1
Transcript of Peptic Ulcer Diseases.. Necrotic Mucosal defects that extends through the Muscularis mucosae and...

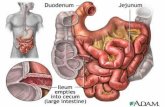
Peptic Ulcer Diseases .

Necrotic Mucosal defects that extends through the Muscularis mucosae and into the sunmucosa or deep layers.
Erosions: more superficial necrotic defects.



Symptoms : abdominal pain, unrelated to the presence or
absence of endoscopically documented ulcer ( in the absence of ulcer gastric visceral hypersensitivity is the likely explanation).
Duodenal ulcer pain occur 2-3 hrs after a meal ,relieved by food or antacids. Gastric ulcer pain occurs sooner after eating.
weight loss ,anorexia , may occur due to delayed gastric emptying.
5

Signs: no finding unless there is perforation/penetration/bleeding Investigations : CBC : anemia , Low
MCV , Radiology : Barium swallow Endoscopy : diagnostic and therapeutic
for complications
Pancreatitis Cholecystitis Hepatitis Mesentric Vascular ischemia Aortic aneurysm Lumbar Disc Prolapse Incisional hernia at the rectum abdominis M. Irritable bowel syndrome.

Gram negative spiral ,flagellated bactrium. Survives in the stomach because of
adaptaion using : Urease breakdown : Urea NH4+ CO2.
(Ammonia is alkaline medium). In developing countries children ( 2-8 years)
acquires H.P at a rate of 10% per year Implicated in Dudodenal ulcers
( 80%),Gastric ulcers ( 60%)

In a selected group of 1200 16-18-year-old students from three regions around KSA.
high H. pylori infection rate (47%) among this age group. Boys had a higher prevalence than girls (p = .03), and the
Al-Qaseem region had the highest prevalence (51%, p = .002).
SES did not contribute to the high prevalence rates (p = .83).
A cross-tabulation of data showed that 88 (8%) of the teenagers were seropositive and that 512 (44%) were negative for both H. pylori and HAV antibodies (χ(2) = 0.03, OR = 0.97, CI = 0.70-1.34).
The variables that were independently associated with seropositivity to H. pylori were being female (OR = 0.75, 95% CI = 0.60-0.95) and living in the Madinah region (OR = 0.72, 95% CI = 0.55-0.94).

Three hundred and fourteen school students, 103 at the intermediate level (grades 7-9) aged 12-15 years and 211 at the secondary level (grades 10-12) aged 15-18 years were tested for H. pylori. Urea breath test (UBT) was used for this purpose. Children with chronic RAP were identified as per the Apley criteria.
Overall, the UBT was positive in 86/314 (27.4%) students. It was positive in 45/103 (43.7%) intermediate school students and 41/211 (19.4%) secondary students.
Out of the 55 students with chronic RAP, 40 (73%) were positive for H. pylori. Further, 62.9% and 82.1% were positive among the intermediate and secondary school students with RAP, respectively.
The overall and specific odds ratios of RAP were 12.35 [95% confidence interval (C.I.) 6.30-24.22] and 10.40 (95% C.I. 1.75-11.73) for the intermediate school students and 22.69 (95% C.I. 7.99-64.44) for the secondary school students.

Diagnosis Endoscopy based tests: Histology-Rapid Urease Non Endoscopy based tests: Urea breath test-
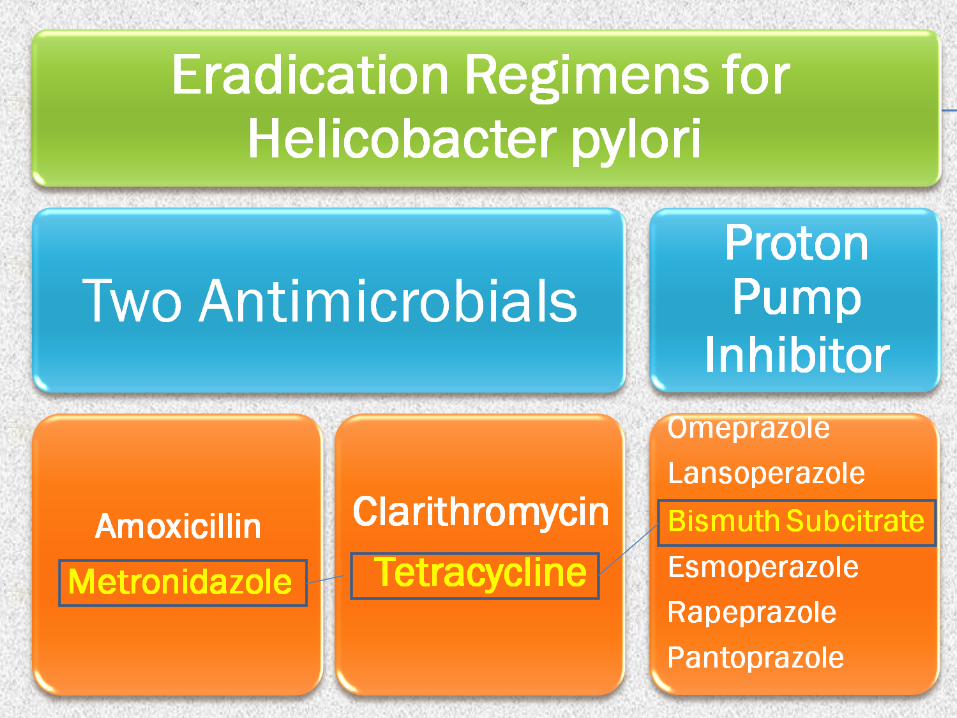
Stool Antigen-Serology.Treatment : Oral not IV ? Increase the concentration of
some drugs. PPI is used to prevent degradation of
antibiotics ( especially Clarithromycin), PPI decrease the viscosity of the gastric mucus
increase the delivery of all antibiotics.
Several countries published comparative studies.
USA, 7 vs. 10 day favored 10 day therapy.
Europe ,no difference between 1 vs. 2 week therapy.
Review of controlled trials suggested that 14 is superior vs. 7 day of therapy .

Eradication rate : PPI triple therapy ( 78%), quadruple Therapy
( 89%),14 day bismuth triple therapy ( 69%) Met analysis found that no significant between
PPI triple therapy and Quadruple therapy when clarithromycin resistance were less than 15%.
But when clarithromycin resistance is present Quadruple therapy is was significantly better than triple therapy.


Exerts its effects at topical and systemic effects
Risk Factors of NSAID induced ulcerations and Complications
History of previous peptic ulceration or GI bleeding
Advanced age Serious systemic disorders

Chemotherapy : 5-FU Potasium cholride supplement tablets Bisphosphonates

Gastrinoma Systemic Mastocytosis Myeloproliferative disorders Antral G cell hyperplasia.

How the ulcer Manifest inside?
20

21

Melena occurs in 20%,Hematemesis in 30%,Both in 50%.
Rationale of treatment: PPI Intragastric pH < 4,therefore Pepsin becomes inactive Enhance homeostasis by preventing peptic
digestion of blood vessels Prevents peptic digestion of blood clots overlying
the ulcer Improves platelets function that is impaired by
acid.
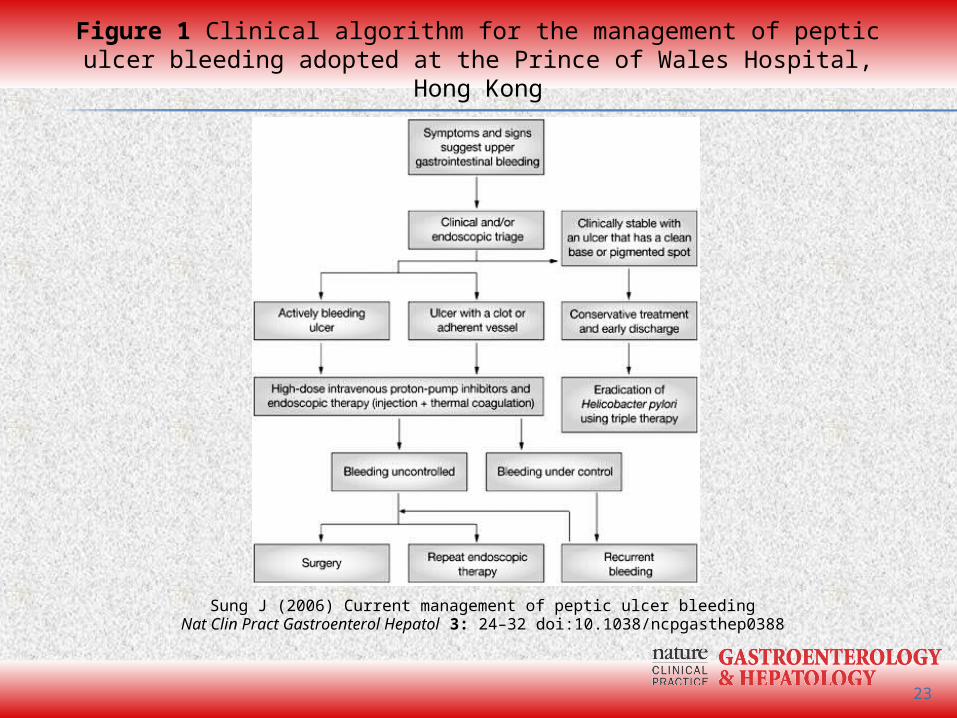
Sung J (2006) Current management of peptic ulcer bleedingNat Clin Pract Gastroenterol Hepatol 3: 24–32 doi:10.1038/ncpgasthep0388
Figure 1 Clinical algorithm for the management of peptic ulcer bleeding adopted at the Prince of Wales Hospital, Hong Kong
23

Occurs in the absence of prior hx in 10-25% Occurs with the crater of the ulcer into the
peritoneum. Risk factors:Elderly,NSAID use, smoking. Duodenal ulcer involve the anterior wall of
the duodenal bulb. Gastric ulcer involve the lesser curvature. Patient presents with features of peritonitis. Management : IV PPI and Surgical Referral Avoid Endoscopy .
Occurs with the crater of the ulcer into adjacent organ.
Gastric :to Left lobe of the liver, colon ( Gastrocolic fistula )
Duodenum: Posterior wall Pancreas. Common bile duct ( Choledocho-duodenal fistula ).
Described by the patient as a change in the pattern of pain.

Due edema and swelling at the antrum,pylorus or duodenum.
Symptoms: abdominal pain,bloating,early satiety, nausea and vomiting. Weight loss electrolytes disturbances.
Delayed gastric emptying : NGT aspirate at 4 hrs after a meal > 300 ml NGT aspirate of 200 ml after overnight fast. Treatment : Medical/Endoscopic in 70%. Surgical Treatment in 30 % of the patients.