
Exploring New paradigms for Health R&D Dr Shaidah Asmall October 2007.

ICDM/ICSM ANOVA-MOPANI
2014
Dr Shaidah Asmall

IDEAL CLINIC DESCRIPTION
Ideal ( concept) refers to perfect/ ultimate/ model Ideal clinic – in this context the concept refers to a facility (clinic) which has been developed to a perfect/ ultimate model to be used as an example for other facilities to benchmark.
DESCRIPTION
• A clinic that ensures the provision of quality health services to the community through: – Good infrastructure – Adequate staff – Adequate medicine and supplies – Adequate bulk supplies – Good administrative processes – Optimal clinical care -use of applicable policies, protocols,
guidelines pertaining to diagnoses and treatment – Leveraging partner and stakeholder support – Cooperation with other government departments as well as
with the private sector and non-governmental organizations to address the social determinants of health
3

District Health System that Supports the Ideal PHC Facility
• Capable District Management Team
• PTICRM
• Improved Procurement System
• Functional referral System
5

COMPONENTS AND ELEMENTS
Administration Clinical
Guidelines & ICDM
Medicines, supplies & lab
services
Staffing & professional
standards
Availability of a doctor
Communication Health
Information Management
Infrastructure & Support services
District Health Support Systems
Partners & stakeholders
ICSM Integrated Clinical Services
Management

ICSM Integrated Clinical Services Management
Acute and Minor Ailments
MCWH-Preventive /Promotive
Chronic Disease Management
Unplanned
Planned appointments
Planned Appointments

Integrated Chronic Disease Management Model


What is the ICDM?
Integrated Chronic Disease Management (ICDM) is a model of managed care that provides for integrated prevention, treatment and care of chronic patients at primary healthcare level (PHC) to ensure a seamless transition to ‘assisted’ self-management within the community by taking a patient-centric view that encompasses the full value chain of continuum of care and support.
11

Purpose of the ICDM • To achieve optimal clinical outcomes for patients
with chronic diseases (communicable and non-communicable) by: – Ensuring the coordination of care and
transitioning to self-management at a community level
– Using the health system building block framework, to improve the efficiency and decrease the strain on the health care system
– Maintaining the economic and social productivity of the patient
– By developing an individual's sense of responsibility for their own health
12

Conditions included as Chronic Diseases
–Non-communicable Diseases
Diabetes,Hypertension,IHD,COPD,Asthma
–Persistent Communicable Diseases
HIV(Pre-ART & on ART),TB
– Long term Mental Illness
Depression,Anxiety
–Persistent Physical Impairments
Strokes,Cerebral Palsy

Pillars of the ICDM
• Primary prevention- identification of high risk individuals at community and facility level and appropriate interventions
• Secondary prevention through planned, optimal evidence based clinical care using an interdisciplinary approach
• Cultivate a sense of individual responsibility through assisted self-management at community level
• These 3 pillars are supported through a sustained, strengthened and integrated health system.

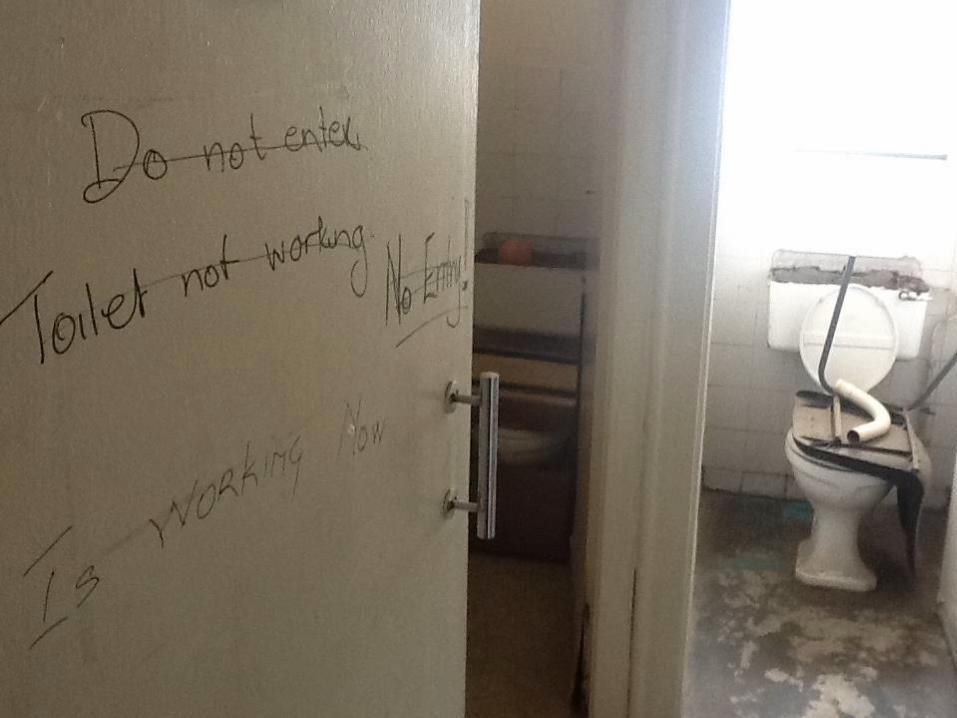
Baseline Assessment
• Vertical services
• Specific days for consulting chronic NCD patients or EPI /ANC i.e. service was not offered daily yet called supermarket approach
• Inefficient process flow at all facilities – – All patients wait in one area for vital signs monitoring-
resulting in bottlenecks and extending patient waiting times
– No signage directing patients to appropriate area for waiting
– No patient scheduling mechanism in place - given only return dates for follow up-thus inappropriate staff allocation.
• No mechanism for tracking defaulters
• Poor quality of clinical records
• Very little health promotion

16

Integrated Clinical Services Management
Facility Community
Optimal Clinical Outcomes
Operational Efficiency & QoC
Individual Responsibility
Re-organisation Clinical management Assisted self management
Health system
HR HMIS Pharmaceuticals Equipment Financing Partners
Stewardship and ownership

HEALTH SERVICE RE-ORGANISATION
•Re-organisation of patient flow
•Designated waiting areas
•Designated consultation area
•Designated vital signs station
•Appointment scheduling •Single administrative point •Pre-appointment retrieval of clinical records •Integration of clinical care •Pre-dispensing of medication
CLINICAL MANAGEMENT SUPPORT
• Chronic patient record
• PC 101 training and application of algorithmic based clinical guidelines
• Health promotion compendium- still to be developed
• Supervision and support by district clinical specialist teams
ASSISTED SELF MANAGEMENT
• Health promotion and education at communicty level
• Identification of at-risk patients within the household by point of care screening
• Point of care testing and screening
• Support groups and adherence clubs
• Medication delivery (courier service)
IDCM model components
18

Health Education & Awareness Screening Referrals
Mentoring & supervision and strengthening of referral
Primary prevention & Screening Household visits- adherence monitoring and identification of complications Referrals
PHC clinic level- treatment and prevention of complications
Oversight and addressing systemic challenges



Organised system
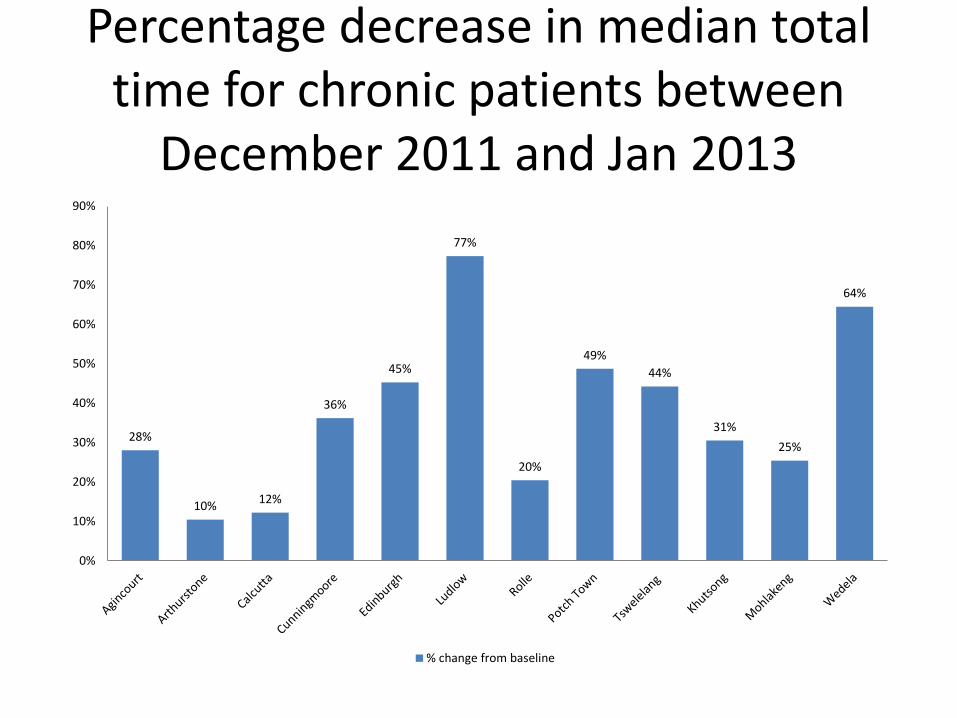
Percentage decrease in median total time for chronic patients between
December 2011 and Jan 2013
28%
10% 12%
36%
45%
77%
20%
49%
44%
31%
25%
64%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
% change from baseline

Change in quality of clinical records- baseline/3 and 6 months post training
76%
69% 65%
50%
22%
33%
90%
95%
81% 76%
33%
40%
92% 88%
83%
68%
35%
44%
0%
20%
40%
60%
80%
100%
120%
DKK DKK contr WRH WRH cont BBR BBR cont
Baseline 3 months 6 months


Cumulative Remaining in Care

Process for Scale up • Evolution of ICDM to ICSM (Integration of Clinical Service
Management ) • The implementation of the ICDM is feasible with limited resources. In
order to scale up the ICDM across all 52 districts it is recommended: • Provincial Senior management be briefed at a strategic level • Provincial programme managers are informed and the ICDM is
included in their key performance areas • The provincial team should select the districts to commence the
implementation • The district should select a sub-district/s to start the
implementation and based on the specific contextual lessons learnt scale up across the district
• A campaign using community media should be launched simultaneously to sensitize patients about the ICDM and changes in management of chronic conditions as well as other services .

Possible Role of Partner Organisations – Assist in rollout of ICDM-identify ~10 best performing
facilities
– Pharmaceutical System Strengthening
– Training of clinical & non clinical staff on appropriate policies, procedures and guidelines -NCS
– Mentorship of the clinical staff to enhance services
– WBOT-CHW training
– Supporting districts and facilities with human resources - not restricted to ART services only but on improving health service • Doctors
• Pharmacist
• Post Basic Pharmacy Assistants
• Data Capturers
• Quality Monitors and Mentors
















![STOCHASTIC LEARNING MODELS · [29], (4) stochastic learning models for simple psychological experiments. This paper deals with the fourth topic. There is asmall butgrowingbodyof literature](https://static.fdocuments.in/doc/165x107/5f0b825b7e708231d430dea4/stochastic-learning-models-29-4-stochastic-learning-models-for-simple-psychological.jpg)

