Pelvic Girdle Differential Diagnosis - Continuing ED Eval - tablet view; single... · Pelvic Girdle...
39
Pelvic Girdle Differential Diagnosis Jason Zafereo, PT, OCS, FAAOMPT Cli i l O th di R h bilit ti Ed ti Clinical Orthopedic Rehabilitation Education 1
Transcript of Pelvic Girdle Differential Diagnosis - Continuing ED Eval - tablet view; single... · Pelvic Girdle...
Pelvic Girdle Differential Diagnosis
Jason Zafereo, PT, OCS, FAAOMPTCli i l O th di R h bilit ti Ed tiClinical Orthopedic Rehabilitation Education
1

Objectives
Describe the relevant findings from the history and examination indicating the source of symptoms as:examination indicating the source of symptoms as:
– Contractile tissue – Non-contractile tissue
Nerve SIJ Hip
Describe the relevant findings from the history and examination indicating a primary impairment of:
Stiffness– Stiffness– Weakness
2

CONTRACTILE TISSUE PATHOLOGY
3

Subjective Exam Findings
Chief complaint: Pelvis pain Nature: Constant and
excruciating (G Min) Aggravating: Pain with
walking (G. Med and Min) uphill (G Max), Pain with firstuphill (G Max), Pain with first movements after sitting (G. Min), Pain with ipsilateral sidelying (G. Med and Min), Pain with cross-legged sittingPain with cross legged sitting (G Min/piriformis), Pain with slumped (G Med) sitting (G Max/piriformis)
4
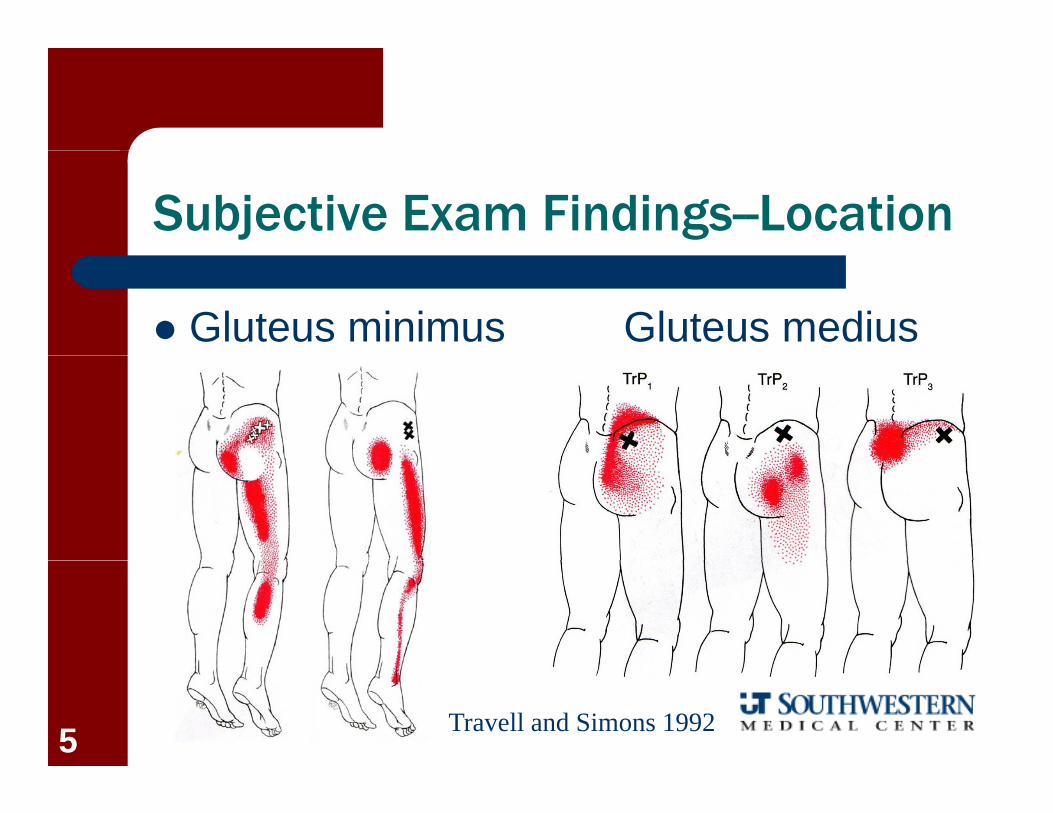
Subjective Exam Findings--Location
Gluteus minimus Gluteus medius
Travell and Simons 19925

Subjective Exam Findings--Location
Gluteus maximus Piriformis
Travell and Simons 19926
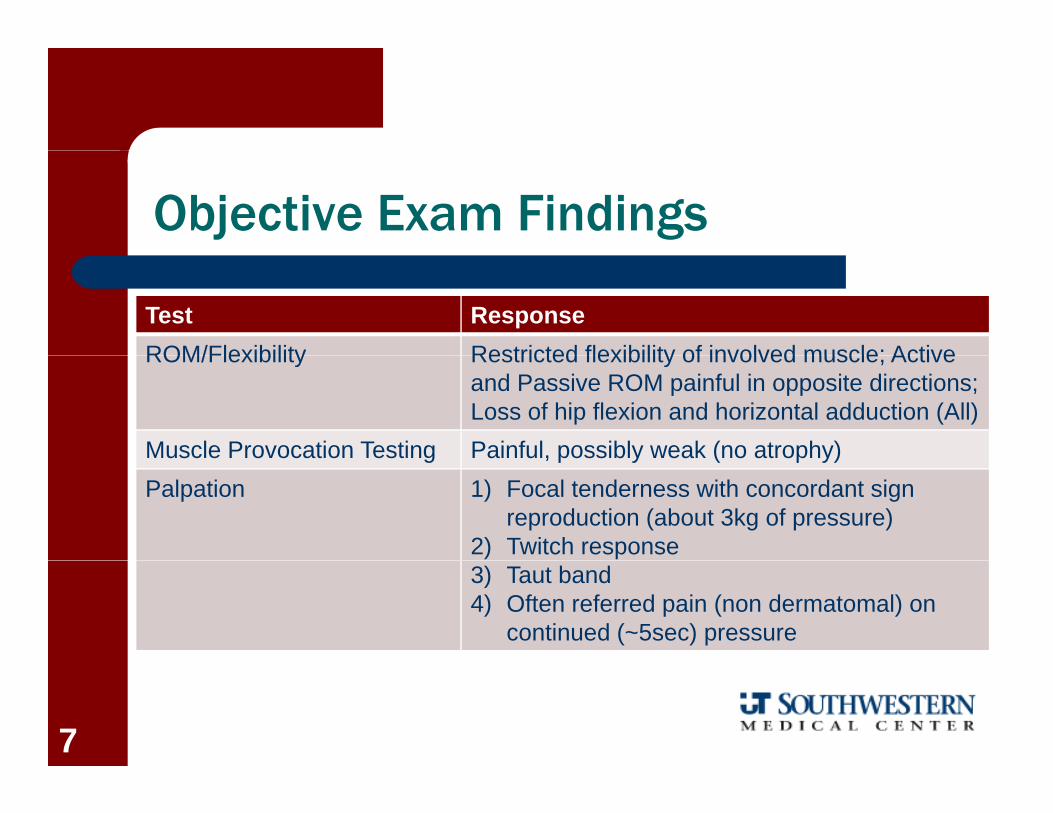
Objective Exam Findings
Test ResponseROM/Flexibility Restricted flexibility of involved muscle; ActiveROM/Flexibility Restricted flexibility of involved muscle; Active
and Passive ROM painful in opposite directions; Loss of hip flexion and horizontal adduction (All)
Muscle Provocation Testing Painful, possibly weak (no atrophy)usc e o ocat o est g a u , poss b y ea ( o at op y)Palpation 1) Focal tenderness with concordant sign
reproduction (about 3kg of pressure)2) Twitch response3) Taut band4) Often referred pain (non dermatomal) on
continued (~5sec) pressure
7
NON-CONTRACTILE TISSUE PATHOLOGY
8
Differential Diagnosis
The SI joint and pubic symphysissymphysis
Peripheral nerve entrapmentsp
– Lateral femoral cutaneous– Obturator
Femoral– Femoral– Sciatic
Hip non-contractile tissue
9
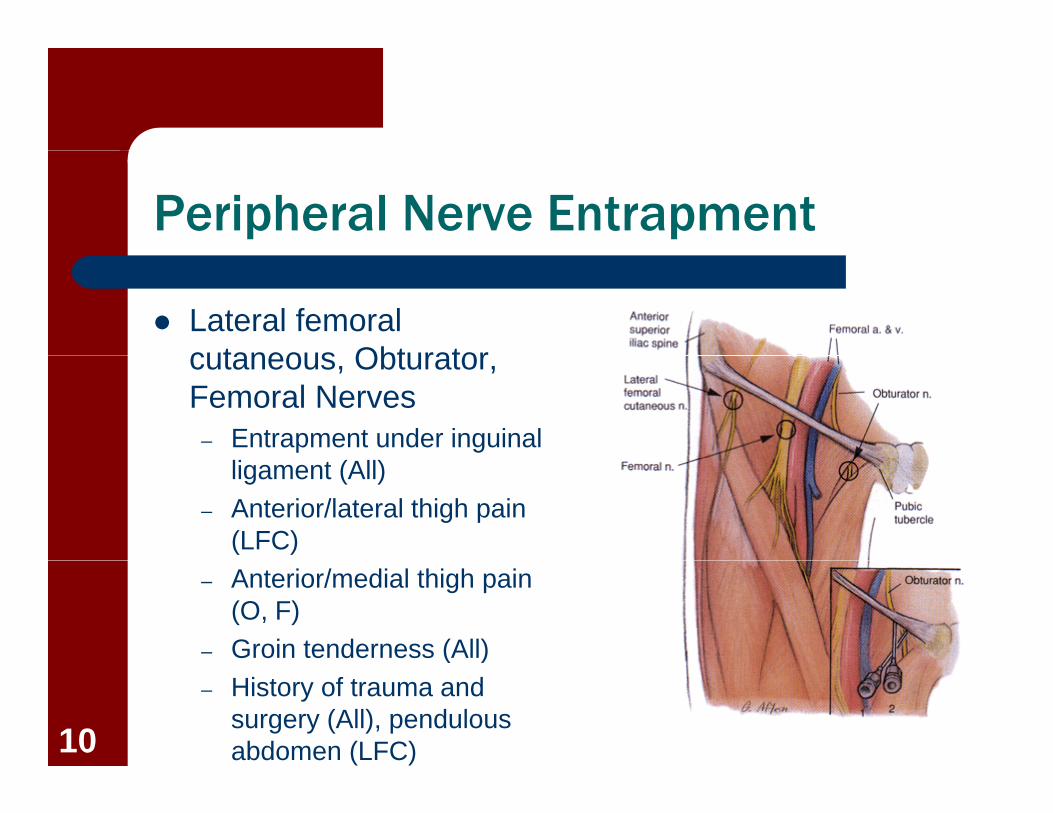
Peripheral Nerve Entrapment
Lateral femoral cutaneous Obturatorcutaneous, Obturator, Femoral Nerves
– Entrapment under inguinal ligament (All)
– Anterior/lateral thigh pain (LFC)
– Anterior/medial thigh pain (O, F)
– Groin tenderness (All)( )– History of trauma and
surgery (All), pendulous abdomen (LFC)10
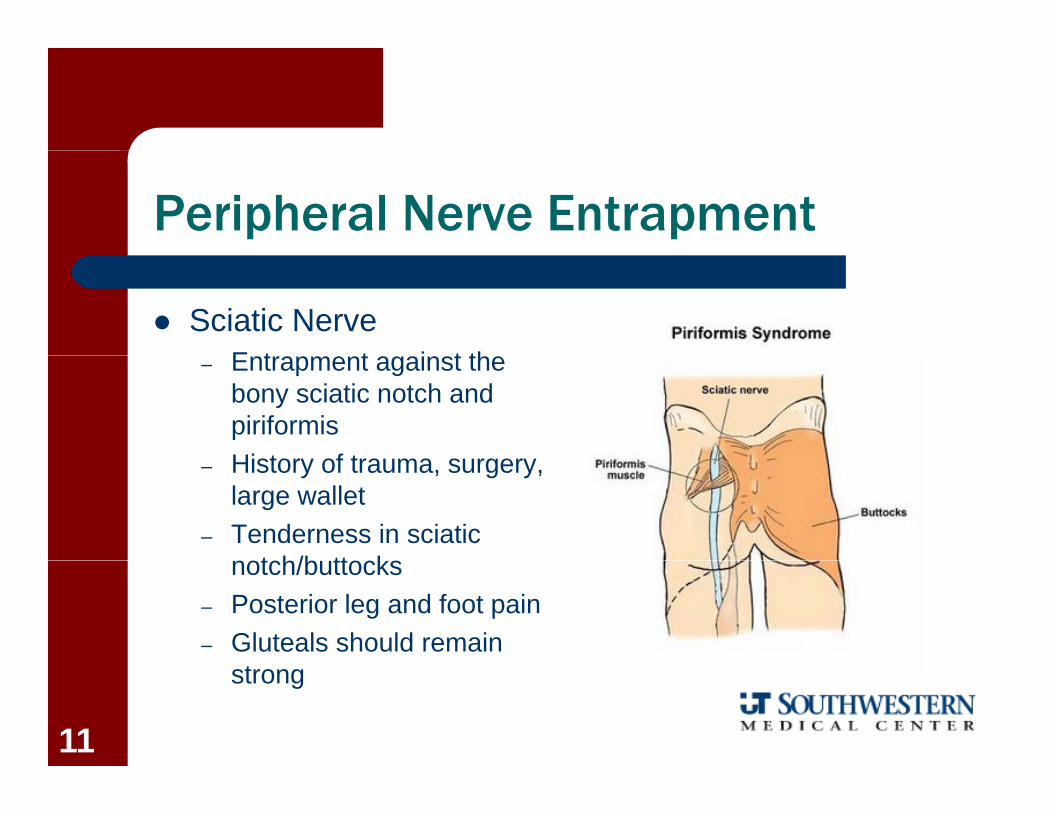
Peripheral Nerve Entrapment
Sciatic NerveE t t i t th– Entrapment against the bony sciatic notch and piriformisHi t f t– History of trauma, surgery, large wallet
– Tenderness in sciatic t h/b tt knotch/buttocks
– Posterior leg and foot pain– Gluteals should remain
strong
11

Hip Non-Contractile Tissue
Joint– Groin and anterior
thigh pain Bursa Bursa
– Greater trochanter or ischium pain, may p , yextend down lateral thigh
12
Subjective Exam Findings—SI Joint
Age 25-45F l
Aggravating factorsW i ht b i i itti Female
– Joint surfaces smaller, flatter, smoother
– Weight bearing via sitting, standing, gait, or stair climbingF d b di /lifti
– Longer lever arm hip to gravity line
– Hormonal
– Forward bending/lifting– Supine lying– Rolling over in bed
changes/pregnancy
History of trauma or pregnancy
– Sidelying semi-fowler with painful side up
– Sit to standpregnancy– Lifting, Loading (Fall),
Torsion13

Subjective Exam Findings- Pelvic Joint Location
SI jointU i b tt k (S1– Upper, inner buttock (S1, S2)
– Lower buttock– Posterior thigh and calf– PSIS highly correlated
with SIJ afflictions
Pubic symphysis– Local, midline to unilateral
Perineum groin abdomen– Perineum, groin, abdomen
Fortin et al 1994; Dreyfus et al 199614

SI Objective Exam Findings
Test ResponseROM Active and Passive ROM painful in same direction.
No centralization or peripheralization with repeated movements. Decreased hip ROM
Special Tests Positive SI provocation tests: Thigh thrust*, Distraction*, Compression*, Sacral thrust, Gaenslen’s; FABERs, Resisted Abduction. ASLR: 98% of severe pelvic pain patients with a positive98% of severe pelvic pain patients with a positive ASLR have the long dorsal ligament as the pain generator (Vleeming, et al. 2002)
Palpation Tenderness medial/inferior to PSIS. Long dorsalPalpation Tenderness medial/inferior to PSIS. Long dorsal ligament tenderness is common (Fortin et al 1999); Sn = .98, LR- = .02 (Vleeming et al 2002)
15
SI Provocation Testing
Goal is to stress SIJ structures and provoke concordant signand provoke concordant sign
Tests may take up to 2 minutes to yield painy p
– Immediate pain consistent with hypermobility or systemic condition
– Delayed pain consistent with stiffness Sizer et al 2002; Winkel et al Sizer et al 2002; Winkel et al
1997
16
SI Provocation Testing
Tests have limited validity when taken individually butwhen taken individually, but become powerful when combined
Validity– 3 or more positive tests out of 6
+LR = 4 4 3 LR = 08 19– +LR = 4-4.3, -LR = .08-.19 Laslett et al 2005; van der
Wurff et al 2006; Szadek et al 2009al 2009
17

SI Provocation Testing
Combination of 3 or more tests with absencemore tests with absence of centralization
– Improved specificity from .78 to .87, sensitivity remained at .91 (+LR = 6.97)
– Currently the most valid clinical examination cluster available Laslett et al, Aust J
Physiother, 200318

SI Provocation Testing
ReliabilityThi h Th t– Thigh Thrust K = .4-.76
– Compression K = .48-.67
– Distraction K = .46-.63
– Gaenslen’s K = .58
– Sacral thrust K = .4-.6
Robinson et al 2007; Arab et al 2009;Kokmeyer et al 200219

SI Provocation Testing
Resisted AbductionSN 87 SP 1 0– SN = .87; SP = 1.0
– K = .5-.78
FABERs– SN = .10; SP = .86– K = .44-.62
Results not validated (ABD) Results not validated (ABD) Tests double as provocation
tests for hipp– Broadhurst and Bond, J Spinal
Disorders, 1998; Kokmeyer et al 200220
PRIMARY STIFFNESS IMPAIRMENT
21
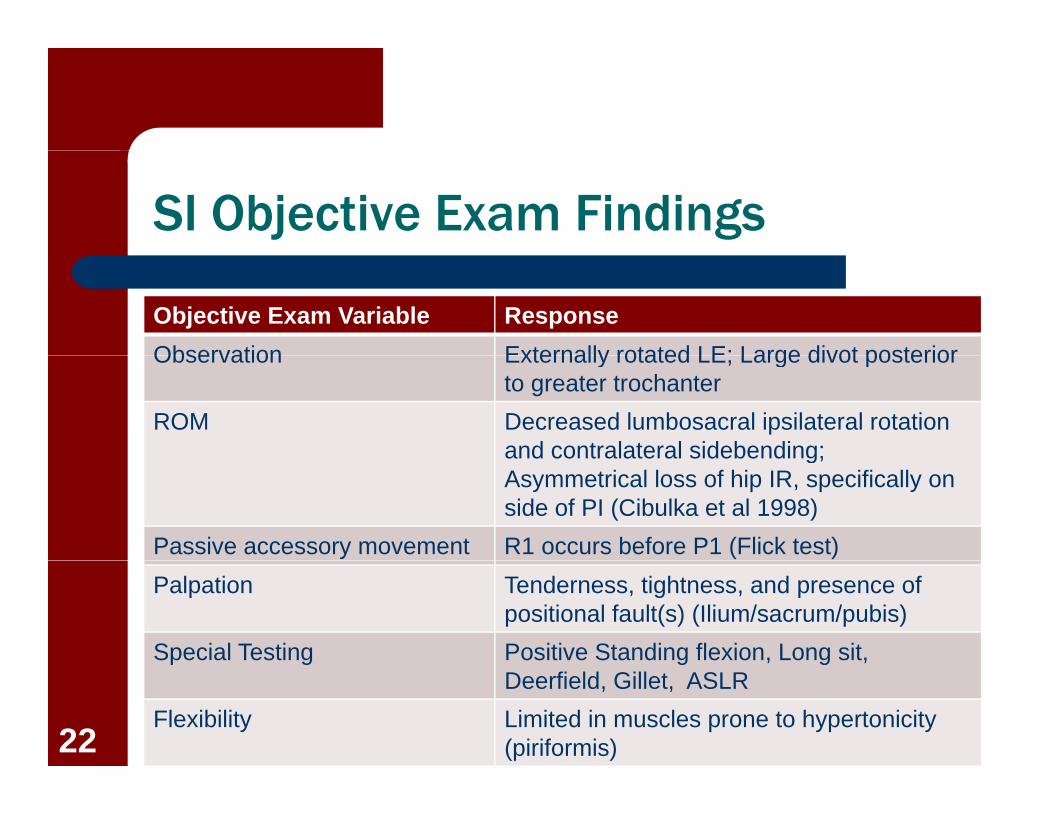
SI Objective Exam Findings
Objective Exam Variable ResponseObservation Externally rotated LE; Large divot posteriorObservation Externally rotated LE; Large divot posterior
to greater trochanterROM Decreased lumbosacral ipsilateral rotation
and contralateral sidebending;and contralateral sidebending; Asymmetrical loss of hip IR, specifically on side of PI (Cibulka et al 1998)
Passive accessory movement R1 occurs before P1 (Flick test)Palpation Tenderness, tightness, and presence of
positional fault(s) (Ilium/sacrum/pubis)Special Testing Positive Standing flexion, Long sit, p g g , g ,
Deerfield, Gillet, ASLRFlexibility Limited in muscles prone to hypertonicity
(piriformis)22

Reliability of Palpation/Motion Testing
ReliabilitySt di fl i
ReliabilityFlick/Spring Test– Standing flexion
K = .32-.55– Deerfield
– Flick/Spring Test K = -.06
– Gillet K = 34- 41
K = .26-.58– Supine long sit
K = .19
K .34 .41
Arab et al 2009; Bowman and Gribble 1995; O’Haire
– Palpation for position (PSIS, sacral sulcus, ILA) K = .04-.08
and Gribble 1995; O Haire and Gibbons 2000; Riddle and Freburger 2002;Robinson et al 2007
23
Validity of Palpation/Motion Testing
Gillet– Sn = .43; Sp = .68Sn .43; Sp .68– Mean rotation of sacrum .2deg posterior– Mean translation .3mm
Spring testingp g g– Sn = .75; Sp = .35
Standing flexion, PSIS position, Long sit, Deerfield– 3 of 4 positive resulted in Spec 88% and Sens of 82% for3 of 4 positive resulted in Spec 88% and Sens of 82% for
identifying LS pain– Standing flexion clinically meaningful only in concert with
positive provocation testing Cibulka et al JOSPT 1999; Winkel et al 1997 Dreyfuss et al Cibulka et al, JOSPT, 1999; Winkel et al 1997 Dreyfuss et al,
Spine, 1996; Sturesson et al, Spine, 2000
24
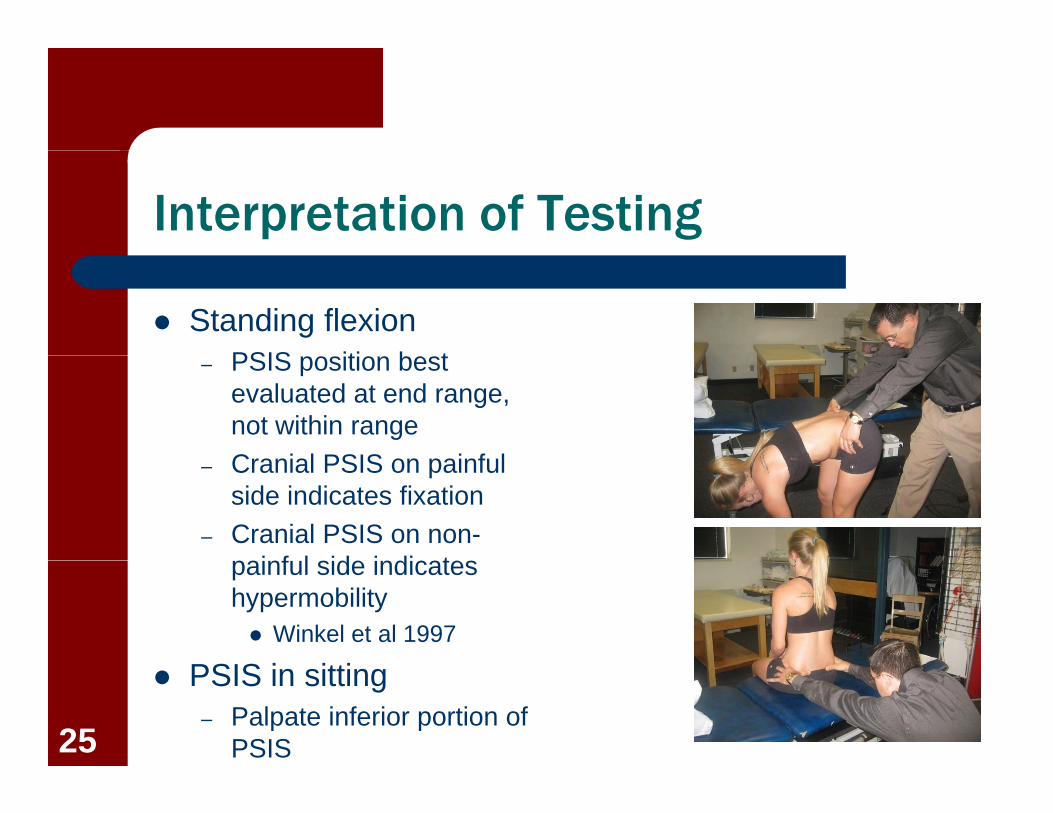
Interpretation of Testing
Standing flexionPSIS iti b t– PSIS position best evaluated at end range, not within rangeC i l PSIS i f l– Cranial PSIS on painful side indicates fixation
– Cranial PSIS on non-i f l id i di tpainful side indicates
hypermobility Winkel et al 1997
S S PSIS in sitting– Palpate inferior portion of
PSIS25

Interpretation of Testing
Supine long sit– Assist patient with
movement to avoid shifting of pelvisof pelvis
– Importance of crossover Deerfield
– Assess with shoes on and vertical compression th h h lthrough heels
26
Interpretation of Cibulka Cluster Testing
Anterior innominate rotationP iti t di fl i t t– Positive standing flexion test
– PSIS high on involved side– Long sit test-leg long to shortg g g– Deerfield test-leg long to short
Posterior innominate rotation– Positive standing flexion test– PSIS low on involved side– Long sit test- leg short to longo g s t test eg s o t to o g– Deerfield test-leg short to long
27
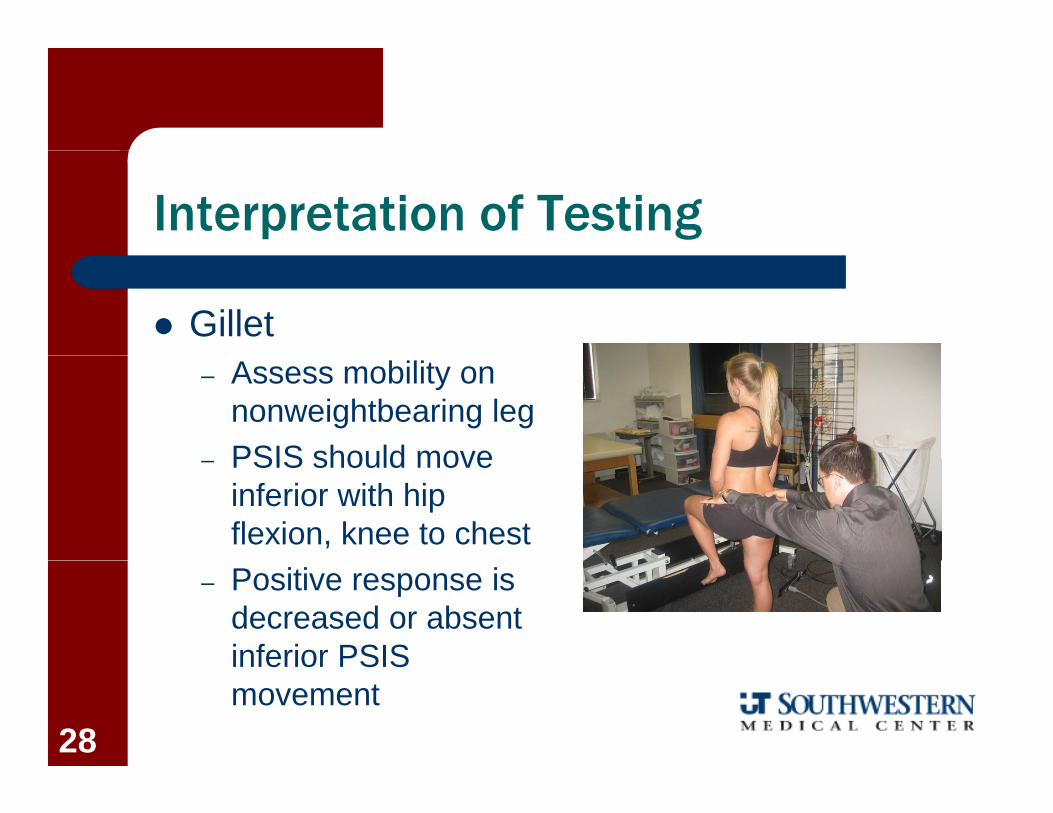
Interpretation of Testing
Gillet– Assess mobility on
nonweightbearing legPSIS should move– PSIS should move inferior with hip flexion, knee to chest
– Positive response is decreased or absent inferior PSISinferior PSIS movement
28
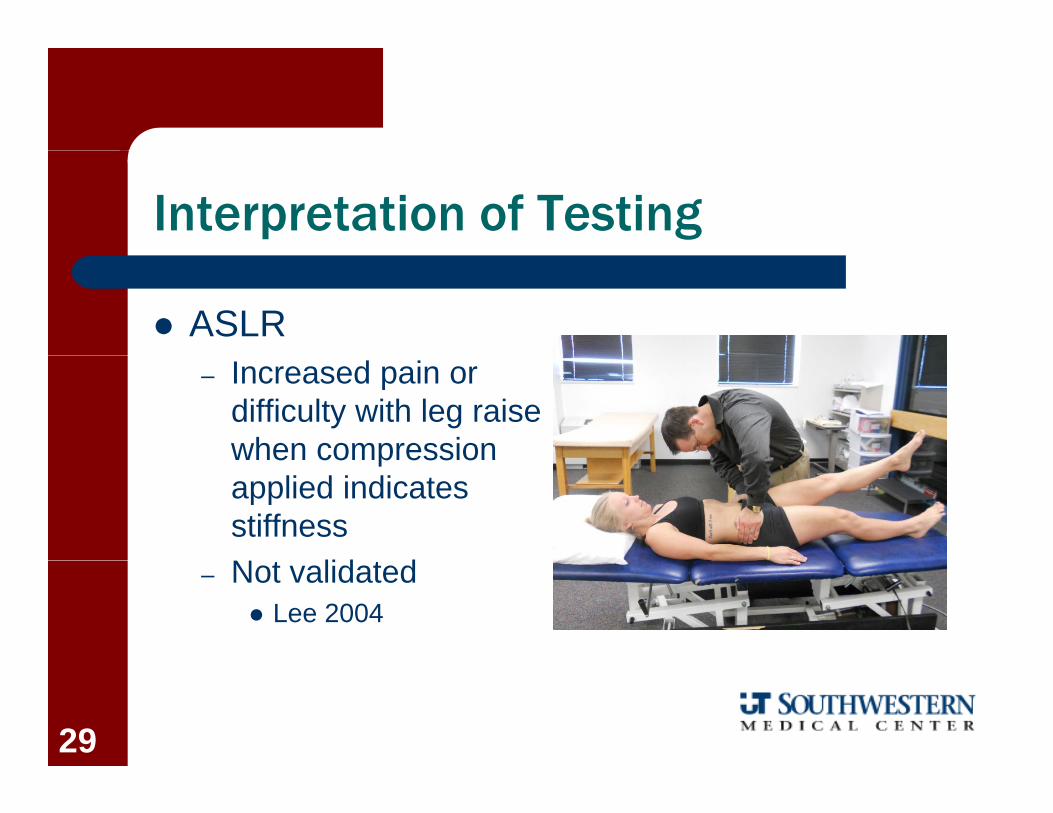
Interpretation of Testing
ASLR– Increased pain or
difficulty with leg raise when compressionwhen compression applied indicates stiffnessN t lid t d– Not validated Lee 2004
29
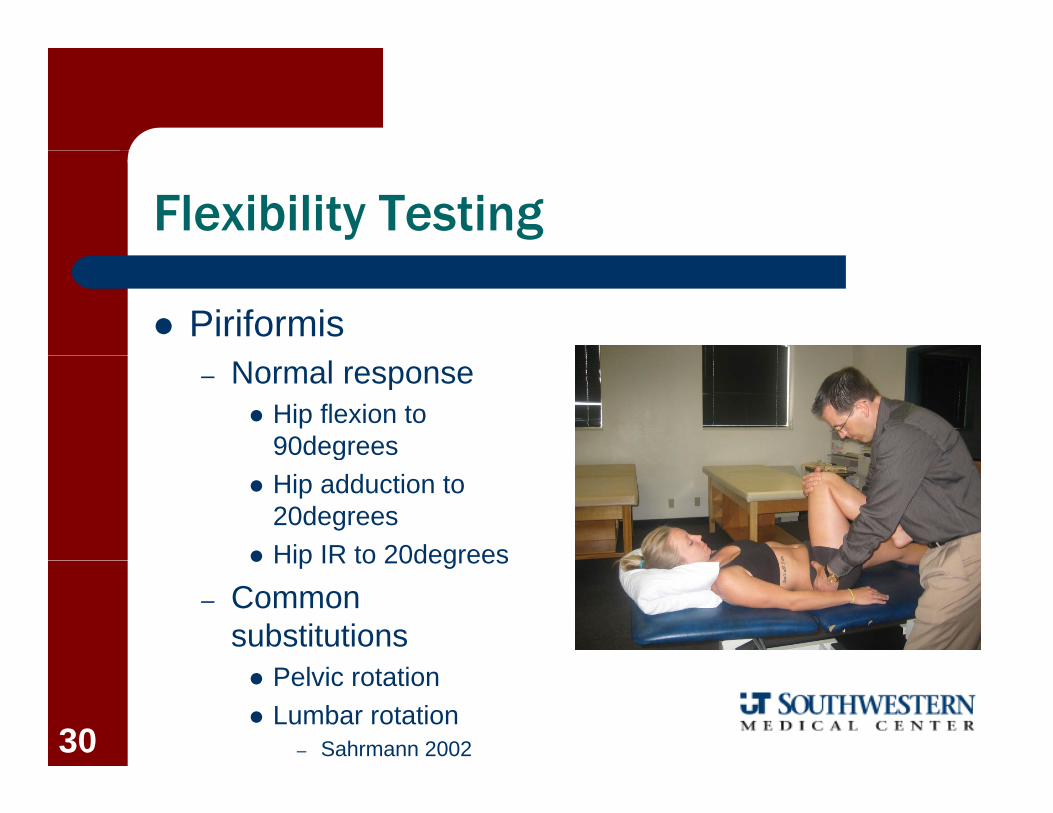
Flexibility Testing
Piriformis– Normal response
Hip flexion to 90degreesg
Hip adduction to 20degrees
Hip IR to 20degrees Hip IR to 20degrees
– Common substitutions Pelvic rotation Lumbar rotation
– Sahrmann 200230
Summary of Findings
Displacement– Cibulka cluster
Stiffness– Gillet– ASLR (pain
increased)increased)– Piriformis tightness– Flick test stiffness– “Butt gripper”
alignment31

PRIMARY WEAKNESS IMPAIRMENT
32
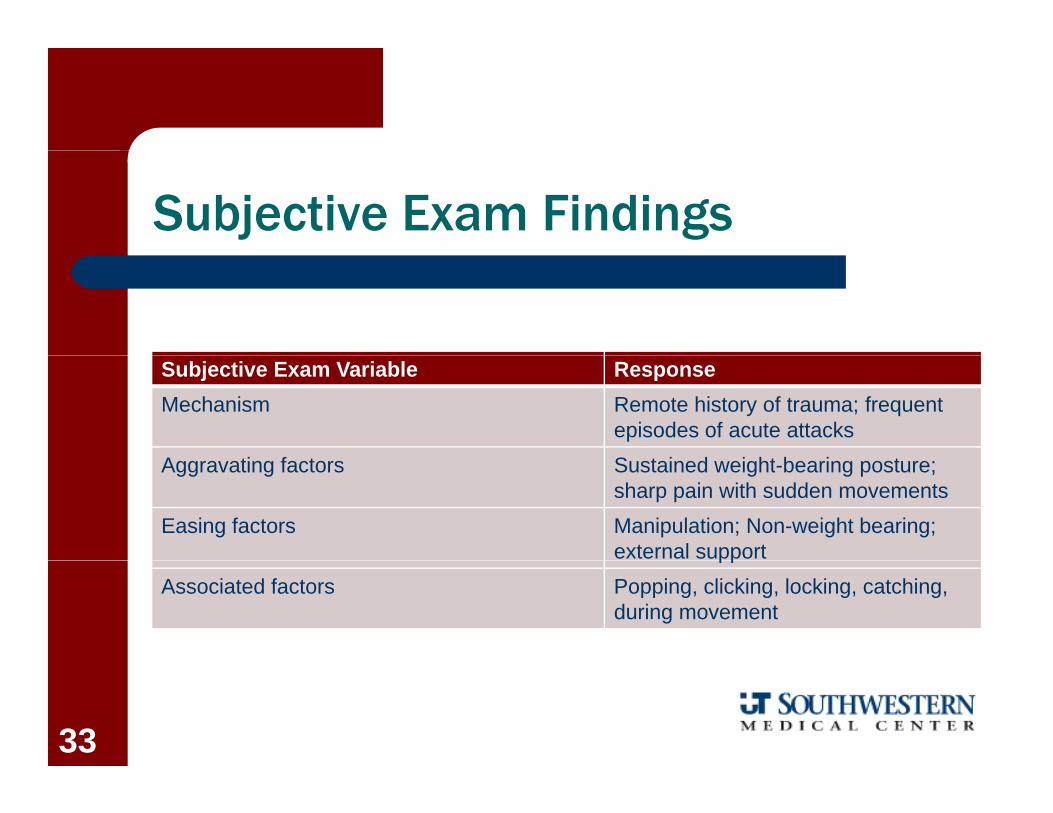
Subjective Exam Findings
Subjective Exam Variable ResponseMechanism Remote history of trauma; frequent
episodes of acute attacksA ti f t S t i d i ht b i tAggravating factors Sustained weight-bearing posture;
sharp pain with sudden movementsEasing factors Manipulation; Non-weight bearing;
external supportppAssociated factors Popping, clicking, locking, catching,
during movement
33
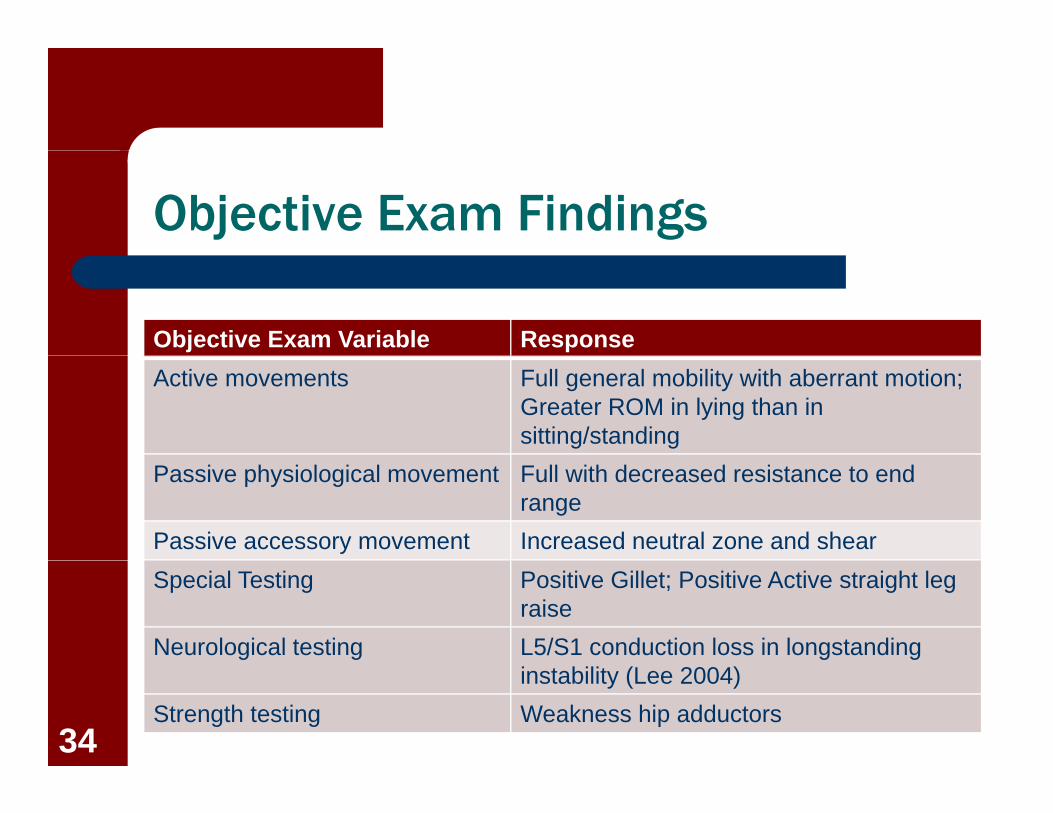
Objective Exam Findings
Objective Exam Variable ResponseActive movements Full general mobility with aberrant motion;
Greater ROM in lying than in sitting/standing
Passive physiological movement Full with decreased resistance to end range
Passive accessory movement Increased neutral zone and shearSpecial Testing Positive Gillet; Positive Active straight leg
raiseNeurological testing L5/S1 conduction loss in longstanding
instability (Lee 2004)Strength testing Weakness hip adductors
34
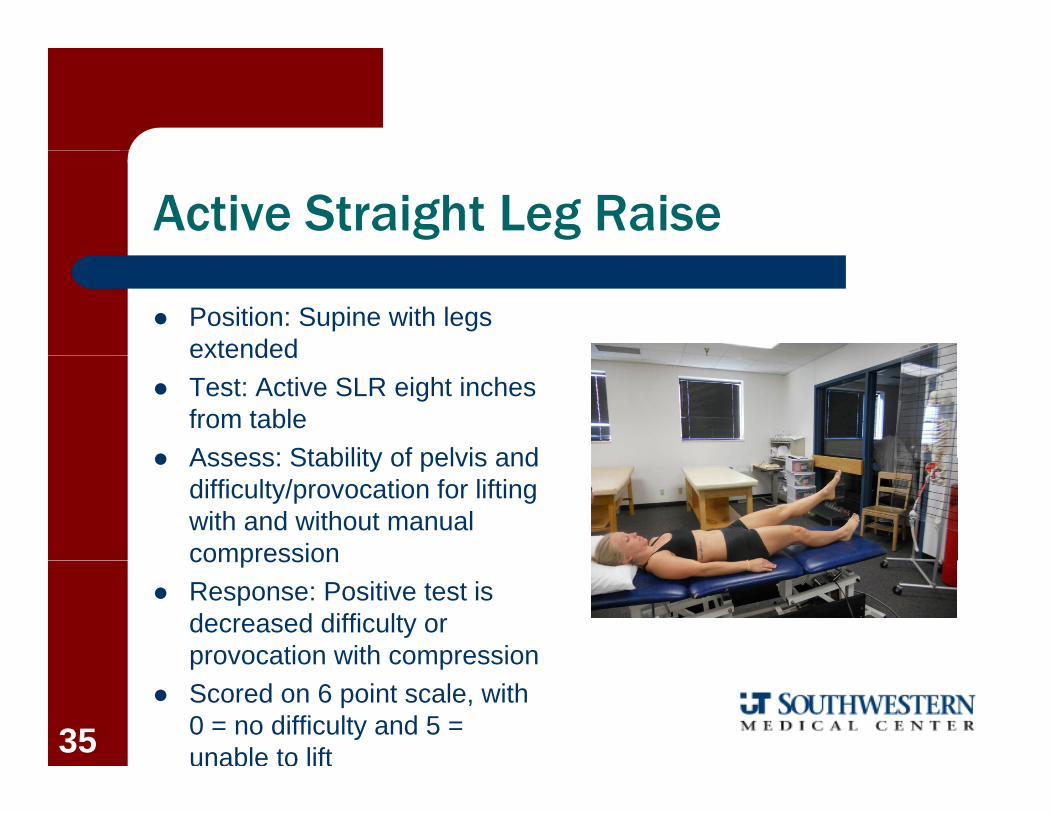
Active Straight Leg Raise
Position: Supine with legs extendedextended
Test: Active SLR eight inches from table
Assess: Stability of pelvis and Assess: Stability of pelvis and difficulty/provocation for lifting with and without manual compressioncompression
Response: Positive test is decreased difficulty or provocation with compressionprovocation with compression
Scored on 6 point scale, with 0 = no difficulty and 5 = unable to lift35

Active Straight Leg Raise
Locations of external compressioncompression
– Applied anterior ilium Pelvic floor and TRA
– Applied posterior ilium Sacral multifidus
– Applied pubic ramus Rectus abdominus or Hip adductors
– Applied thorax to pelvis Internal/external obliques Lee 2004
36

Active Straight Leg Raise
Reliability– ICC = .83
Validity– Identification of posterior pelvic
pain during and after pregnancy– Cut score set between 0 and 1– Cut score set between 0 and 1– SN = .54 - .87; SP = .88 - .94 – Diagnostic accuracy highest g y g
post-partum Mens et al, 2001 and 201237
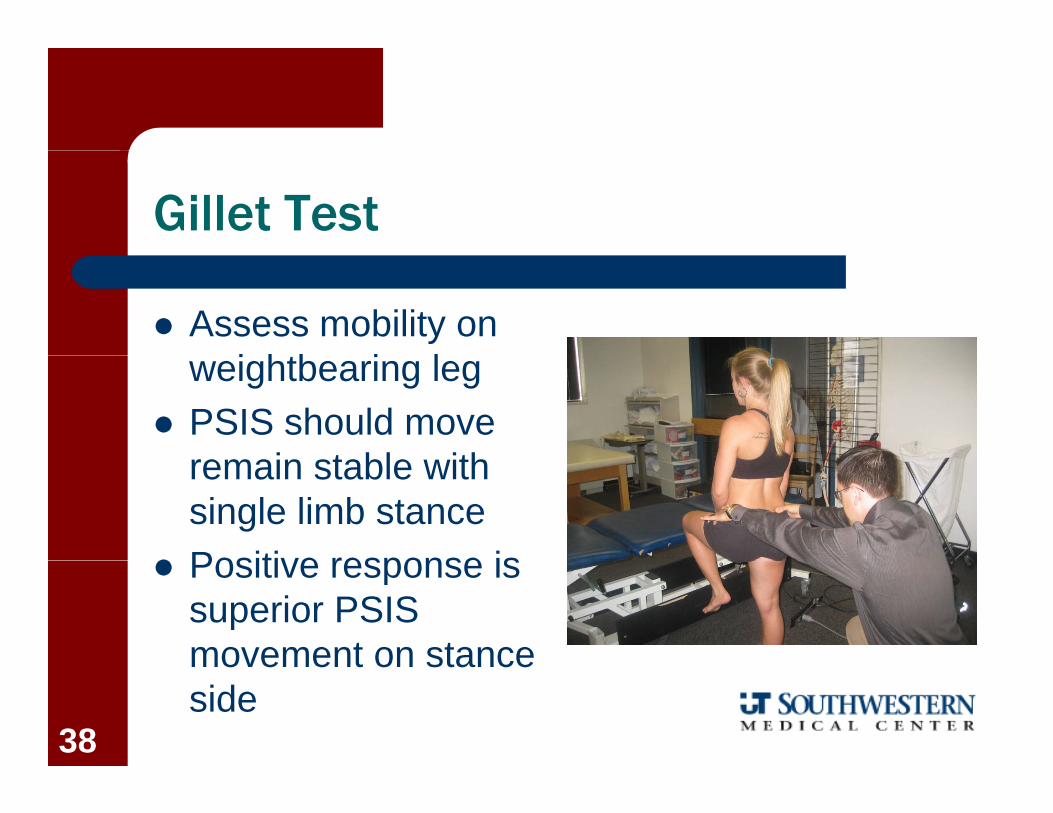
Gillet Test
Assess mobility on i htb i lweightbearing leg
PSIS should move i t bl ithremain stable with
single limb stance Positive response is Positive response is
superior PSIS movement on stancemovement on stance side
38
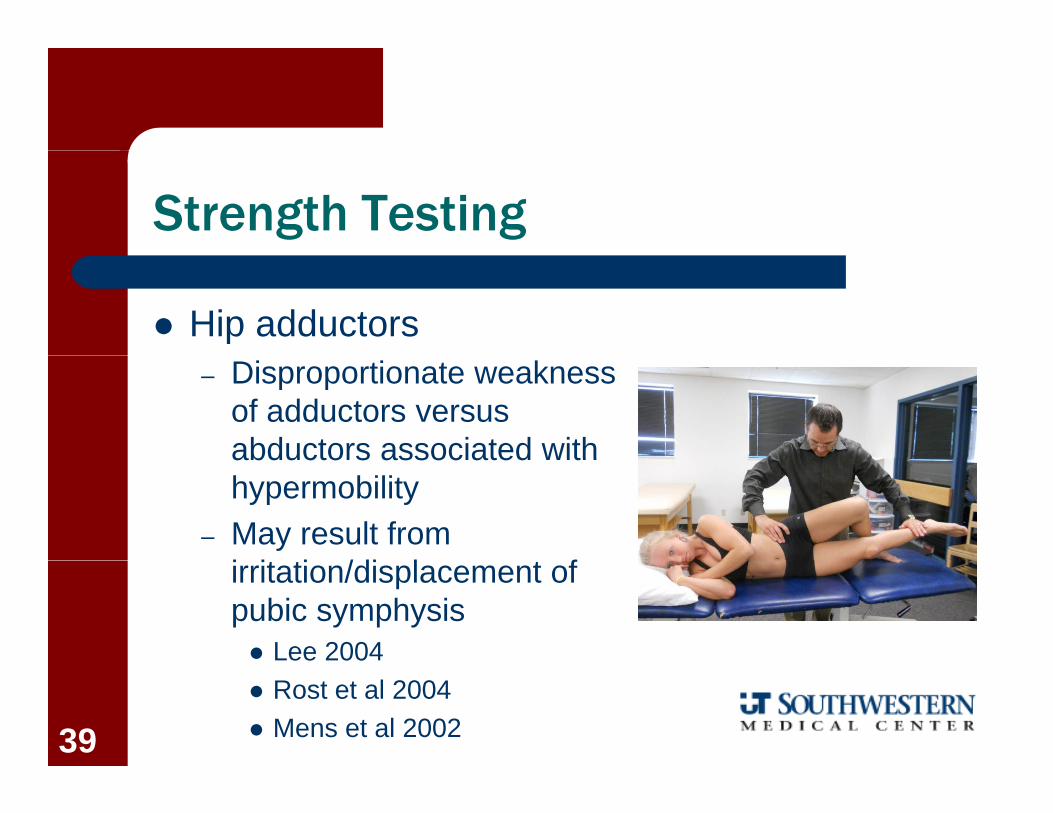
Strength Testing
Hip adductors– Disproportionate weakness
of adductors versus abductors associated withabductors associated with hypermobility
– May result from i it ti /di l t firritation/displacement of pubic symphysis Lee 2004 Rost et al 2004 Mens et al 200239