Pediatrics in Review-2013-Gregory-203-15 diabetes 1.pdf
15
DOI: 10.1542/pir.34-5-203 2013;34;203 Pediatrics in Review Justin M. Gregory, Daniel J. Moore and Jill H. Simmons Type 1 Diabetes Mellitus http://pedsinreview.aappublications.org/content/34/5/203 located on the World Wide Web at: The online version of this article, along with updated information and services, is Pediatrics. All rights reserved. Print ISSN: 0191-9601. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy of published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point publication, it has been published continuously since 1979. Pediatrics in Review is owned, Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly at Universidad Catolica de la Santisima Concepcion on March 4, 2014 http://pedsinreview.aappublications.org/ Downloaded from at Universidad Catolica de la Santisima Concepcion on March 4, 2014 http://pedsinreview.aappublications.org/ Downloaded from
-
Upload
valentina-paz-fuentes-conapiado -
Category
Documents
-
view
19 -
download
0
Transcript of Pediatrics in Review-2013-Gregory-203-15 diabetes 1.pdf
-
DOI: 10.1542/pir.34-5-2032013;34;203Pediatrics in Review
Justin M. Gregory, Daniel J. Moore and Jill H. SimmonsType 1 Diabetes Mellitus
http://pedsinreview.aappublications.org/content/34/5/203located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Pediatrics. All rights reserved. Print ISSN: 0191-9601. Boulevard, Elk Grove Village, Illinois, 60007. Copyright 2013 by the American Academy of published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1979. Pediatrics in Review is owned, Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly
at Universidad Catolica de la Santisima Concepcion on March 4, 2014http://pedsinreview.aappublications.org/Downloaded from at Universidad Catolica de la Santisima Concepcion on March 4, 2014http://pedsinreview.aappublications.org/Downloaded from
-
Type 1 Diabetes MellitusJustin M. Gregory, MD,*
Daniel J. Moore, MD, PhD,
Jill H. Simmons, MD
Author Disclosure
Drs Gregory and
Moore have disclosed
no financial
relationships relevant
to this article. Dr
Simmons has
disclosed she has
a research grant from
Alexion
Pharmaceuticals, Inc.
This commentary does
not contain discussion
of unapproved/
investigative use of
a commercial product/
device.
Practice Gaps
1. All children with type 1 diabetes mellitus (T1DM) should have their blood sugar
managed with basal-bolus insulin treatment by either multiple daily injections or an
insulin pump.
2. All children with T1DM should have access to a pediatric endocrinologist with
a diabetes management team with resources to support patients and families.
3. All children with T1DM should be monitored for symptoms and/or screened for
commonly associated conditions such as thyroid and celiac disease.
Objectives After completing this article, readers should be able to:
1. Recognize the presenting signs and symptoms of type 1 diabetes mellitus (T1DM).
2. Know the key principles of effective diabetes self-management and the diabetes care
teams role in facilitating effective self-management.
3. Know the acute and chronic complications of (T1DM).
4. Identify how different categories of insulin analogues are used in daily insulin
regimens.
True, it is a ght, but there is pleasure in the struggle. Victory comes to the courageous; and without cour-age and common sense, success awaits no one. I look upon the diabetic as charioteer and his chariot asdrawn by three steeds named Diet, Insulin, and Exercise. It takes skill to drive one horse, intelligenceto manage a team of two, but a man must be a very good teamster who can get all three to pull together.
EP Joslin, 1933
IntroductionType 1 diabetes mellitus (T1DM) is a disorder of glucose homeostasis characterized by au-toimmune destruction of the insulin-producing pancreatic b-cell that progressively leads to
insulin deciency and resultant hyperglycemia. If left un-treated, insulin deciency leads to progressive metabolicderangement, with worsening hyperglycemia, ketoacidosis,starvation, and death. In an effort to restore and maintaineuglycemia, treatment attempts to mimic the action of thenative b-cell by exogenously replacing insulin and includesfrequent monitoring of blood glucose levels.
As the visionary pioneer Dr. Elliott P. Joslin believed, thebest possible outcomes of T1DM treatment are realizedwhen a sense of empowerment, rather than victimization,is imparted to both patient and family. Achieving this em-powerment through diligence and education enables anindividual living with T1DM to attain optimal health and
Abbreviations:
ADA: American Diabetes AssociationDKA: diabetic ketoacidosisHbA1c: glycosylated hemoglobinI:C ratio: insulin-to-carbohydrate ratioIV: intravenousTDD: total daily doseT1DM: type 1 diabetes mellitusT2DM: type 2 diabetes mellitus
*Pediatric Endocrinology Clinical Fellow, Ian Burr Division of Pediatric Endocrinology and Diabetes, Vanderbilt University School of
Medicine, Nashville, TN.Assistant Professor of Pediatrics, Assistant Professor of Pathology, Microbiology, and Immunology, Ian Burr Division of Pediatric
Endocrinology and Diabetes, Vanderbilt University School of Medicine, Nashville, TN.Assistant Professor of Pediatrics, Ian Burr Division of Pediatric Endocrinology and Diabetes, Vanderbilt University School of
Medicine, Nashville, TN.
Article endocrine disorders
Pediatrics in Review Vol.34 No.5 May 2013 203
at Universidad Catolica de la Santisima Concepcion on March 4, 2014http://pedsinreview.aappublications.org/Downloaded from
-
well-being and constitutes the ultimate goalandchallengeof the medical team.
The epidemiology and pathophysiology of T1DM arediscussed in this article, followed by a practical review ofthe diagnosis and treatment of this chronic, lifelong con-dition emphasizing the goal of effective diabetes self-management as leading towards enduring wellness.
EpidemiologyThe prevalence of T1DM among patients younger thanage 20 years in the United States is estimated at 1.54 casesper 1,000 youth. (1) The highest prevalence is seen amongnon-Hispanic white children, with 2.0 cases per 1,000,which is 50% higher than that of black children (1.34 casesper 1,000) and double that of Hispanic children (1.0 casesper 1,000). (1) Girls and boys are almost equally affected,a fact that distinguishes T1DM from most autoimmuneillnesses, which tend to affect females more frequently.
The incidence of T1DM in the US pediatric populationis estimated to be 19.0 cases per 100,000 person-years.The highest incidence is in non-Hispanic white childrenfollowed by black and Hispanic children (23.8, 14.2,and 13.7 cases per 100,000 person-years, respectively).(2) The peak age of onset in the United States appearsto occur in early puberty to midpuberty. In most studies,a seasonal variation in onset has been observed in children,with the highest incidence of T1DM occurring during thewinter months and the lowest occurring during the sum-mer months. This nding may result from winter monthshaving higher rates of viral infections, which cause a meta-bolic stress that exceeds the ability of the residual b-cellmass to produce insulin sufcient to maintain euglycemia.Interestingly, the incidence rate of T1DM appears to beincreasing in the United States each year, with a mean an-nual increase in incidence of 2.3% per year, consistent witha rising trend observed globally of 2.8% per year. (35)
PathogenesisA predisposition for T1DM begins at birth with the in-heritance of genetic risk factors. Although most newlydiagnosed patients have no family history of T1DM, un-affected children who have a relative with T1DM are atincreased risk as compared to the general population. Themost strongly associated susceptibility genes for T1DMare located in the major histocompatibility complex re-gion on chromosome 6 and most likely operate by direct-ing immune development and permitting presentation ofautoantigens to autoreactive lymphocytes.
A triggering environmental factor probably plays anadditional role in evoking clinical disease. This hypothesis
is supported by the fact that monozygotic twins are notuniformly concordant for disease progression. Environ-mental factors such as infection may contribute to auto-immune activation by inciting cross-reactivity againstantigens on the b-cell that bear a similar molecular structureor in a non-specic way, such as promoting the productionof proinammatory cytokines that injure islet tissue.
The progression from immune activation to clinicallyrelevant islet cell loss may take many years and is markedearly by the presence of serum autoantibodies. Once theb-cell mass is insufcient to maintain euglycemia, clinicalsymptoms evolve.
Clinical PresentationNew-onset T1DMusually presents in one of three ways: withclassic presenting symptoms, with diabetic ketoacidosis(DKA), or more rarely, as an incidental nding.
Classic SymptomsNew-onset T1DM presents in the majority of pediatric pa-tients with the classic symptoms of polyuria and polydipsia(69%) and somewhat less frequently with polyphagia andweight loss (33%). (6) Patients and families usually reportthe duration of symptoms as lasting 1 to 2weeks, but some-times severalmonths.Often, these symptoms becomemoreapparent after an episode of enuresis or with the emergenceof nocturia. Patients frequently have vague complaints, suchas fatigue, and may note blurred vision.
Diabetic KetoacidosisIn roughly one-quarter of cases, a patient with new-onsetT1DM will present with DKA. These children and ado-lescents tend initially to have the same classic symptoms(polyuria, polydipsia, polyphagia, weight loss), which be-come more severe. As acidosis develops, these patientsfrequently lose their appetite and nausea, vomiting, andabdominal pain become the signicant symptoms. Tocompensate for the worsening ketoacidosis, hyperpnea de-velops (Kussmaul respirations). If unchecked, neurologicstatus progressively deteriorates as acidosis and hyperos-molality worsen, and the patient progresses from drowsi-ness to lethargy to obtundation. Risk factors associatedwith an initial presentation of DKA include youngerage, especially children younger than age 2 years, ethnicminority status, and lower socioeconomic and parentaleducation levels.
Incidental FindingA smaller number of children and adolescents are diag-nosed as having diabetes despite having none of the clas-sic symptoms of T1DM. These children usually have
endocrine disorders type 1 diabetes mellitus
204 Pediatrics in Review Vol.34 No.5 May 2013
at Universidad Catolica de la Santisima Concepcion on March 4, 2014http://pedsinreview.aappublications.org/Downloaded from
-
impaired glucose tolerance because of b-cell loss, buthave not yet had overt symptoms. As home blood glucosemonitoring has become more widespread, family mem-bers with diabetes may check blood glucose levels inother family members, and hyperglycemia will be de-tected despite a lack of symptoms. Families with diabetesconcerned about risk in their children should be directedto a T1DM TrialNet website where screening and longi-tudinal observation can be performed (www.diabetes-trialnet.org). In other situations, children will have aseemingly unrelated presenting complaint (eg, vulvovaginalcandidiasis) that leads to the detection of glycosuria andthen hyperglycemia caused by T1DM.
DiagnosisThe diagnostic criteria for all forms of diabetes mellitusare outlined in Table 1. In most cases, the clinical historyis strongly suggestive of new-onset diabetes, and labora-tory evaluation conrms the diagnosis. Once diabetes isdiagnosed, it is important to determine which type of di-abetes the patient has to form an appropriate treatmentregimen. During the initial assessment, it is imperativealso to determine whether potential associated acute co-morbidities, such as DKA and cerebral edema, are pres-ent. At a minimum, initial laboratory studies shouldinclude a serum glucose level to establish the degree ofhyperglycemia, and a low threshold should be maintainedin ill-appearing patients for obtaining serum electrolytesand a blood gas for detecting possible electrolyte abnormal-ities that must be corrected as well as the presence of DKA.
An increasingly frequent diagnostic dilemma is distin-guishing between T1DM and type 2 diabetes mellitus(T2DM) as the incidence of obesity and T2DM in thepediatric population rises. Differentiating between the
two in the obese patient with new-onset diabetes is com-plicated by presenting characteristics that often overlap.Several features, however, are useful in making a presump-tive diagnosis of T1DM versus T2DM in this situation;
- T2DM occurs after pubertal onset in the majority ofcases.
- T2DM is associated commonly with obesity, acanthosisnigricans, and features of the metabolic syndrome suchas hypertension and dyslipidemia; these features are lesscommon in T1DM.
- Patients with new-onset T1DM are more likely to pres-ent with the classic symptoms of new-onset diabetes.
- The presence of autoantibodies associated with T1DMare more suggestive of, but not exclusive to, T1DMthan T2DM, particularly when multiple autoantibodiesare elevated.
- Patients with new-onset T2DM are approximately vetimes more likely to have an affected rst-degree familymember who has T2DM than are patients with new-onset T1DM to have an affected rst-degree familymember with T1DM.
- The prevalence of T2DM is substantially higher amongNative-American, Hispanic, and African-American eth-nicities, compared to non-Hispanic white youth.
Patients with new-onset T1DM and T2DM can pres-ent with DKA, and the treatment of DKA will be thesame. Those patients who present initially in DKA shouldbe continued on insulin until the diagnosis is clear; somepatients with T2DM may be able to transition to oralmedications once stabilized.
Other causes for new-onset diabetes warrant consider-ation. These disorders include genetic defects of b-cell func-tion, diseases of the exocrine pancreas, and drug-induced
Table 1. Criteria for Diagnosis of Diabetes
HbA1c 6.5% (where the test is performed in a laboratory using a method that is National Glycohemoglobin StandardizationProgram certified and standardized to the Diabetes Complications and Control Trial assay)*
ORFasting plasma glucose level 126 mg/dL (where fasting is defined as no caloric intake for at least 8 hours)*
OR2-hour oral glucose tolerance test reading 200 mg/dL (where performed as described by the World Health Organization, using
a glucose load containing the equivalent of 75 g anhydrous glucose dissolved in water or 1.75 g/kg of body weight if weight is
-
effects. Genetic defects in insulin secretion are becom-ing recognized increasingly. Among these conditions,maturity-onset diabetes of the young (MODY) syn-dromes are a group of disorders characterized by mono-genic defects in b-cell function. These defects limitinsulin secretion by the b-cell, which leads to hyperglyce-mia; but the disease severity tends to be milder. The con-dition presents before age 25 years, is not associatedwith elevated autoantibodies, and is transmitted in anautosomal dominant fashion. Diseases that cause dam-age to the exocrine pancreas can lead to diabetes, mostcommonly in cystic brosisrelated diabetes and late inthe course of chronic pancreatitis. Additionally, a num-ber of drugs and chemicals are known to induce diabe-tes, including immunosuppressants such as tacrolimusand cyclosporine, glucocorticoids, and chemotherapeu-tics such as L-asparaginase.
TreatmentOnce the diagnosis of T1DM is established, initial carefocuses on restoring euglycemia and teaching the pa-tient and family the basic skills required to take careof diabetes at home. Initial management is inuencedby whether the patient is acutely ill at presentation(eg, whether DKA is present). The approach to initialcare should also be tailored to the developmental stageof the patient. Ideally, every child newly diagnosed ashaving T1DM should be evaluated by a diabetes teamconsisting of a pediatric endocrinologist, nurse educa-tor, dietician, social worker, child life specialist, andmental health professional.
At a minimum, during the initial visit with the diabetesteam, the family should learn how to check and recordblood glucose concentrations using a home blood glu-cose meter, how to draw up and deliver insulin using a sy-ringe, and how to detect and treat hypoglycemia. Onceinitial management is completed, care shifts toward on-going management. The patient and family, with the sup-port of the diabetes team, progressively assume greaterownership of diabetes care, with the support of the dia-betes team. Ultimately, optimal diabetes managementseeks to strike a balance between restoring blood glucoseinto the euglycemic range in order to minimize the mi-crovascular and macrovascular complications associatedwith chronic hyperglycemia while simultaneously mini-mizing a childs unique vulnerability to hypoglycemia.
Initial Insulin RegimenInsulin therapy is prescribed to mimic the action of theb-cell by achieving three basic goals:
1. Facilitate metabolism and storage of consumed food.During feeding, insulin is needed to facilitate trans-port of glucose from blood into the cells of insulin-dependent tissues such as muscle, fat, and the liver.In the physiologic state, insulin is secreted almost im-mediately upon eating. By contrast, insulin therapy inT1DM utilizes subcutaneous delivery of rapid orshort-acting insulin with meals and snacks. Usually,the dosage of insulin given is proportional to theamount of carbohydrates being ingested. For example,a patient may take 1 unit of insulin for every 10 gramsof carbohydrates being consumed. This insulin-to-carbohydrate (I:C) ratio is titrated frequently duringthe initial weeks of management, and then routinely dur-ing ongoing management. The Rule of 500 some-times is used to calculate this initial I:C ratio dose bydividing 500 by the estimated total daily dose (TDD)of insulin (estimation of TDD is discussed below).
2. Normalize hyperglycemia. One key to tight glycemiccontrol is to minimize the magnitude and durationof hyperglycemic excursions throughout the day. Toaccomplish this goal, an additional correction factordose of rapid or short-acting insulin is added to theamount of insulin given to cover carbohydrates atmealtimes. The correction factor dose is proportionalto the degree of hyperglycemia. To calculate the initialcorrection factor dose, many clinicians will utilize theRule of 1,800 by dividing 1,800 by the estimatedTDD. The number estimates how much 1 unit of in-sulin should drop the blood glucose concentration. Forexample, a patient with an estimated total daily dose of18 units of insulin would be expected to have a 100mg/dL drop in blood glucose for each unit of insulindelivered. Therefore, if the target blood glucose level is100 mg/dL, the patient should receive an additional 1unit for a blood glucose of 200 to 299 mg/dL, 2 unitsfor 300 to 399 mg/dL, 3 units for 400 to 499 mg/dL,and so on as a correction factor dose. As with the I:Cratio dose, the correction factor dose is titrated accord-ing to the patients blood glucose trends.
3. Maintain euglycemia during fasting. Because glucose-increasing counter-regulatory hormones retain theirability to stimulate hepatic glucose production, basalinsulin is needed to maintain a euglycemic balance be-tween meals. For this reason, one or two daily doses oflong-acting insulin are given to maintain a low level ofinsulin during fasting.
When the initial insulin regimen is being designed, it ishelpful to approximate the initial TDDof insulin. Childrenwith long-standing diabetes usually require somewhere
endocrine disorders type 1 diabetes mellitus
206 Pediatrics in Review Vol.34 No.5 May 2013
at Universidad Catolica de la Santisima Concepcion on March 4, 2014http://pedsinreview.aappublications.org/Downloaded from
-
between 0.5 and 1.0 units/kg per day of insulin. Prepu-bertal children tend to require a lower TDD, and pubertalchildren usually need a higher TDD. In most cases, half ofthe TDD is given as long-acting insulin and the other halfis given as rapid or short-acting insulin to cover meals.With the guidance of the diabetes care team, these dosesare adjusted empirically for each patient based on the pa-tients blood glucose log.
It is also important to be mindful of the honeymoonphase that follows initial diagnosis and treatment with in-sulin. During this time, endogenous insulin secretion fromremaining b-cells continues, and in many cases, insulindoses must be lowered to prevent hypoglycemia. The hon-eymoon phase tends to occur more frequently and lastslonger in those patients who are older and have a milderinitial presentation. Usually, the insulin dose reaches its na-dir at approximately 3 months into therapy and the hon-eymoon phase ends by 7 months, although this interval ishighly variable. This period offers a great opportunity forachieving tight control, and it has been suggested thattight initial control begets improved long-term control.
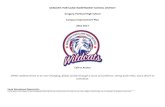
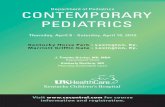
Insulin analogues are categorized by their time courseof action as rapid, short, intermediate, or long-acting, asoutlined in Table 2 and shown in Figure 1. These phar-macodynamic characteristics form the basis of the frame-work for a daily insulin regimen that seeks to mimic theb-cell. Figure 2 illustrates a basalbolus, or multipledaily injection regimen, in which rapid-acting insulinis given with meals and snacks and long-acting insulin
to provide a steady amount of insulin with little to nopeak between mealtimes. This protocol is the most widelyused injection regimen. Short- and intermediate-actinginsulin sometimes are utilized in regimens to minimizethe number of daily injections. In a mixed-split regi-men, a short-acting insulin is mixed in the same syringewith an intermediate analogue, and two daily doses aregivenone with breakfast and one with dinner. Theshort-acting insulin covers breakfast and dinner, whilethe delayed action of the intermediate-acting insulin isutilized to cover lunch and a bedtime snack. A major ad-vantage of the basalbolus regimen over the mixedsplitregimen is greater exibility for when meals and snackscan be eaten and how many carbohydrates can be con-sumed. Good results can be obtained with a mixed-splitregimen, but this treatment requires a patient to eat thesame amount at the same time each day.
Diabetic KetoacidosisInitial Assessment and Monitoring
The biochemical criteria for DKA include a blood glucoselevel greater than 200 mg/dL and venous pH less than7.30 or a bicarbonate level less than 15 mmol/L. The se-verity of DKA can be classied according to the severity ofthe acidosis, as shown in Table 3. (7,8) Precipitating fac-tors that could lead to the onset of DKAsuch as infec-tion, or in the case of patients with known T1DM, insulinomission, insulin pump failure, or failure to match insulindosing to metabolic requirements during illnessshould
be investigated. Medication noncom-pliance is frequently the cause ofrecurrent DKA. In one study,85% of hospital admissions for DKAinvolved discontinuation of medica-tion use. (9) The degree of dehydra-tion should be appraised clinically atpresentation and monitored for im-provement during treatment. Un-fortunately, it is difcult in thissetting to estimate dehydration ac-curately according to the clinicalndings more frequently associatedwith acute dehydration because wa-ter losses occur over a longer periodof time and are both intracellular andextracellular. The majority of pa-tients who present with DKA are be-tween 5% and 10% dehydrated.
Because all patients who haveketoacidosis do not haveDKA, otherconditions with similar presentations
Table 2. Approximate PharmacodynamicCharacteristics of Insulin Analogues
Insulin analogueOnset ofaction
Peakaction (h)
Effectiveduration (h)
Rapid actingLispro (Humalog, Eli Lilly) 15 min 0.5-1.5 4-6Aspart (NovoLog, Novo-Nordisk)Glulisine (Apidra, Sanofi-Aventis)
Short actingRegular 30-60 min 2-3 8-10
Intermediate actingNPH 2-4 h 4-10 12-18
Long actingGlargine (Lantus, Sanofi-Aventis) 2-4 h None 20-24Detemir (Levemir, Novo-Nordisk) 2-4 h 3-9 6-24*
*Duration of action is dose dependent.- Humalog, Eli Lilly and Company World Headquarters, Lilly Corporate Center, Indianapolis, Indiana46285.- NovoLog, Levemir, Novo Nordisk, Corporate Headquarters, Novo All, 2880 Bagsvaerd,Denmark.- Apidra, Lantus, Sano-Aventis, 54 rue La Botie, 75008 Paris, France.
endocrine disorders type 1 diabetes mellitus
Pediatrics in Review Vol.34 No.5 May 2013 207
at Universidad Catolica de la Santisima Concepcion on March 4, 2014http://pedsinreview.aappublications.org/Downloaded from
-
should be considered. For instance, starvation ketosis andalcoholic ketoacidosis can present with ketoacidosis and el-evated blood glucose concentrations but rarely are associ-ated with a blood glucose greater than 250 mg/dL. DKAalso should be distinguished from other causes of increased
aniongapmetabolic acidosis, includinglactic acidosis, ingestions (eg, meth-anol, ethylene glycol, salicylates),and renal failure.
After the initial assessment, thekey elements of early treatment in-clude frequent monitoring of clini-cal and biochemical parameters,uid and electrolyte replacement,correction of hyperglycemia andketoacidosis, and if necessary, treat-ment of cerebral edema. During theinitial phase of treatment, the pa-tients heart rate, respiratory rate,blood pressure, neurologic status,capillary glucose level, and uid out-put and input status should be as-sessed hourly. In cases of severeDKA, electrocardiographic monitor-ing is useful to monitor for evidenceof hyperkalemia (eg, peaked T wave,reduced P wave, and widening ofQRS complex as severity worsens)or hypokalemia (eg, attened or in-verted T wave, ST segment depres-sion, the presence of a U wave, anda widened PR interval), both ofwhich can lead to cardiac arrhythmia.Checking levels of serumelectrolytes,glucose, andbloodgasses every2 to4hours is needed to assess response totreatment and to guide adjustmentsin therapy.
Cerebral EdemaOnce the diagnosis of DKA is estab-lished, the patient should be as-sessed for comorbidities associatedwith DKA. Most critically, the med-ical team should monitor for signsand symptoms of cerebral edemabefore and during treatment forDKA. Although rare (occurring in0.5% to 1% of pediatric cases ofDKA), (10) cerebral edema hasbeen associated with a mortality rate
of 21% to 24% and permanent neurologic impairment inan additional 15% to 32% of cases. (10) In most cases, ce-rebral edema occurs 4 to 12 hours after the initiation oftreatment for DKA (10,11) but can sometimes occur be-fore treatment has been initiated. (8)
Figure 1. Pharmacodynamic profiles of insulin analogs.
Figure 2. Sample basalbolus regimen, with breakfast, lunch, and dinner.
Table 3. Grades of Diabetic Ketoacidosis Severity
Mild Moderate Severe
Venous pH 7.21-7.30 7.11-7.20
-
Muir and colleagues proposed a bedside, evidenced-based protocol for the early detection of patients at riskfor cerebral edema, outlined in Table 4. (11) The authorsfound that bedside ndings of either two major criteria orone major criterion with two minor criteria could identifycerebral edema sufciently early for intervention. Diagnos-tic criteria are listed in Table 4 also, but once these signsare present, advanced cerebral edema with the likelihoodof signicant neurologic injury is also present.
It is important to note that cerebral edema is a clinical,not radiologic, diagnosis because a substantial number ofpatients with cerebral edema and impending neurologiccollapse will have no positive ndings on computed to-mography of the brain. (11) Thus, imaging studiesmay be warranted to rule out other causes of neurologicdeteriorationalthough never needed to conrm cere-bral edemabut treatment for cerebral edema shouldnot be delayed for conrmatory neuroimaging.
If clinical evidence suggests the presence of cerebraledema, prompt treatment is needed. Early treatment withmannitol (0.25 to 1.0 g/kg) or hypertonic (3%) salineover 30 minutes (5 to 10 mL/kg) may prevent long-termneurologic consequences or death.
Fluid and Electrolyte TherapyOnce intravenous (IV) access is obtained, water and elec-trolyte decits need to be replaced in order to restore thecirculating volume and the glomerular ltration rate andimprove renal clearance of glucose and ketones from theblood. To replace these decits, most experts recom-mend using isotonic saline initially and caution against re-hydrating the patient too aggressively, suggesting thatrehydrating too rapidly using hypotonic solution for ini-tial volume expansion is associated with increased risk forcerebral edema. (7,8) In general, in children with mod-erate to severe DKA, initial rehydration with 10 to 20mL/kg isotonic solution (either 0.9% saline or Ringerlactate) over 1 to 2 hours is recommended.
Following the initial uid resuscitation, the rate of IVuid should be calculated to run at a rate designed to re-hydrate evenly over the next 48 hours. This goal usuallycan be achieved by running uids at a rate of 1.5 to 2times the calculated maintenance rate. Because largeamounts of replacement with 0.9% saline has been asso-ciated with hyperchloremic metabolic acidosis, (7,8) theIV uids can be changed to a solution with 0.45% orgreater saline with added potassium after at least 4 to 6
hours of uid replacement with iso-tonic solution. As insulin is beingreplaced, an intracellular shift of po-tassium that leads to a drop in potas-sium level is seen. For this reason,frequent monitoring is needed asthe potassium is replaced and IV u-ids are administered.
InsulinAs the uid and electrolyte decitis corrected, insulin replacement isneeded to normalize the elevatedblood glucose and suppress ketogen-esis and lipolysis. After the initial 1 to2 hours of uid rehydration, contin-uous IV insulin infusion is started ata rate of 0.1 unit/kg per hour. Aninitial IV insulin bolus is contraindi-cated and will cause a rapid drop inblood glucose that may precipitatecerebral edema; in addition, IV insu-lins half-life is approximately 7 min-utes and therefore cannot suppressketosis. (7) Ideally, the continuousinsulin infusion should lead to a dropin blood glucose at a rate of 50 to100 mg/dL per hr. In most cases,
Table 4. Bedside Evaluation of Neurologic Stateof Children with Diabetic Ketoacidosis
Diagnostic Criteria for Cerebral EdemaAbnormal motor or verbal response to painDecorticate or decerebrate postureCranial nerve palsy (especially III, IV, and VI)Abnormal neurogenic respiratory pattern (eg, grunting, tachypnea, Cheyne-Stokes
respirations, apneusis)Major Criteria
Altered mentation or fluctuating level of consciousnessSustained heart rate decelerationAge-inappropriate incontinence
Minor criteriaVomitingHeadacheLethargy or not being aroused from sleepDiastolic pressure >90 mmHgAge < 5 years
Data from Muir AB, Quisling RG, Yang MC, Rosenbloom AL. Cerebral edema in childhood diabeticketoacidosis: natural history, radiographic ndings, and early identication. Diabetes Care. 2004;27(7):1541-1546. (11)- The presence of any of the rst four diagnostic criteria in the table indicates that advanced cerebraledema is present with the likelihood of signicant neurologic injury. Prompt intervention is indicated tolimit neurologic injury.- The presence of two major criteria or one major criterion and two minor criteria represent the presenceof early cerebral edema; prompt intervention is indicated to prevent long-standing neurologic injury.- Signs that occur before treatment should not be considered in the diagnosis of cerebral edema (eg,vomiting before initial treatment should not be counted).
endocrine disorders type 1 diabetes mellitus
Pediatrics in Review Vol.34 No.5 May 2013 209
at Universidad Catolica de la Santisima Concepcion on March 4, 2014http://pedsinreview.aappublications.org/Downloaded from
-
the hyperglycemia normalizes before the correction ofketoacidosis.
In order to continue infusing insulin to clear the ke-toacidosis without inducing hypoglycemia, dextrosecan be added to the IV uids. Many protocols will beginusing IV uids containing 5% dextrose when the bloodglucose level drops below 300 mg/dL, then 10% dex-trose when blood glucose is less than 200 mg/dL. Asinsulin continues to be infused and the uid decit is re-placed, ketoacidosis will resolve. (10) No other interven-tion besides insulin and IV uids is indicated to treat theacidosis; bicarbonate should not be used because its usehas been associated with cerebral edema. The continuousinsulin infusion should be maintained until the ketoaci-dosis has resolved (ie, pH greater than 7.30 or bicarbon-ate greater than 17 mmol/L) and the patient is wellenough to tolerate oral intake. At this point, IV insulincan be transitioned to a subcutaneous insulin regimen,as described for the patient who initially presents withoutDKA.
Ongoing ManagementOnce the medical problems related to the initial presen-tation have resolved, care shifts towards ongoing man-agement. T1DM is a chronic condition that requiresfrequent monitoring of blood glucose, frequent dose cal-culations of numerous injections of insulin analogueswith different pharmacokinetic properties, and continualadjustment for alterations in homeostasis, such as stress.Once diagnosed, the initial adjustments in a patients dailyregimen required to achieve effective self-managementcan seem dramatic and overwhelming.
Yet, in spite of this need for adjustment, the individ-uals who have T1DM have distinguished themselves indiverse elds. Such individuals include a Supreme Courtjustice, Olympic gold medalists, internationally recog-nized scientists, and famous musicians and artists. Theirsuccess proves that despite the challenges of T1DMself-management, patients can ourish in the pursuit oftheir ambitions; however, effective ongoing diabetes ed-ucation and care is essential for realizing these goals.
EducationAfter teaching the essential skills of self-management, ed-ucation transitions towards an ongoing phase seeking tointegrate effective diabetes self-management into a dailyroutine. The patient and family should learn how to handlecommon contingencies that will affect self-care, such as ex-ercising, dealing with sick days, and traveling. The careteam should help facilitate a gradual shift in responsibilityfor self-care from the parents to the maturing child.
Blood Glucose MonitoringIn order to approach near-normalization of blood glu-cose concentration, frequent blood glucose monitoringis needed to minimize glycemic excursions and to eval-uate the effectiveness of an insulin regimen.More frequentblood glucose monitoring is associated with betterglycemic control, and for this reason, four or more testsper day are recommended. (12) Patients and their familiesshould be encouraged to log their blood glucose data, notonly to help the diabetes team adjust the insulin regimenbut also to gain insight into patterns associated withtheir own diabetes regimen. The blood glucose log andthe glycated hemoglobin (HbA1c) level are useful in quan-tifying glycemic control and directing titration of insulindoses.
Because glucose becomes irreversibly attached to he-moglobin at a rate proportional to blood glucose con-centration, and because the average life span of a redblood cell is roughly 3 months, a measurement of HbA1ccorrelates well with the average glucose level over thepreceding 3 months. In some cases, a fructosamine levelis useful because it reects an average glucose level overa shorter period of 2 to 3 weeks. This test is helpfulwhen patients have a concurrent condition in which he-moglobin turnover is higher, such as hemoglobinopathiesor hemolytic anemia, or in situations in which a physiciandesires an earlier objective assessment of a recent change intherapy.
Insulin PumpThe insulin pump has increased in popularity as an insulindelivery tool over the past two decades. The essentialcomponents of most insulin pumps consist of the pumpitself, a disposable insulin reservoir, and a disposable in-fusion set (including a cannula and tubing that connectsthe cannula to the pump and reservoir). In a manner sim-ilar to the basalbolus regimen, continuous subcutaneousinsulin infusion via an insulin pump attempts to mimicthe action of the pancreatic b-cell by delivering rapid-acting insulin with basal and bolus components.
Most current-generation pumps allow the user to en-ter in the number of grams of carbohydrates being eatenand the current blood glucose level and then calculate anappropriate bolus dose according to the patients I:C ra-tio and correction factor. The pump can also factor in amathematical estimate of the amount of active insulin inthe circulation at the time of the bolus. Instead of usinglong-acting insulin analogues, the pump delivers basal in-sulin by slowly infusing frequent, small aliquots of rapid-acting insulin on a continual basis, effectively giving basalinsulin as a continuous infusion.
endocrine disorders type 1 diabetes mellitus
210 Pediatrics in Review Vol.34 No.5 May 2013
at Universidad Catolica de la Santisima Concepcion on March 4, 2014http://pedsinreview.aappublications.org/Downloaded from
-
This approach to basal insulin delivery is a key advan-tage of the insulin pump over multiple daily injections inthat it allows different basal rates at various times of day,which can be used to tailor an insulin regimen to t var-iations in insulin sensitivity through a daily cycle. For ex-ample, many patients experience an overnight dawnphenomenon when circadian rises in growth hormoneand cortisol have a glucose-raising effect. To balance thisphysiologic effect, the overnight insulin basal rate can betitrated up without increasing the daytime basal rate.
NutritionMedical nutrition therapy is an important aspect ofachieving optimal glucose control. A meal plan shouldseek to meet the nutritional requirements needed for nor-mal growth and development and t within the familysroutine of meal and snack times, exercise, and culturalnorms. Although the nutritional needs are the same forchildren who have diabetes as for children who do not,intensive insulin therapy to achieve tight glycemic controlrelies on an accurate assessment of the total amount ofcarbohydrates being consumed. For these reasons, a medi-cal nutritionists guidance is needed to help establish a mealplan that meets these needs and to teach families how tomeasure the carbohydrates in meals and snacks accurately.
A common lay misconception of medical nutritiontherapy in T1DM is that calories should be restricted orthat certain foods are off-limits. In general, these princi-ples are inuenced by greater familiarity with lifestyle inter-ventions needed in T2DM.Additionally, earlier approachesto insulin therapy relied on xed doses of mixed insulinsand required rigid mealtimes and carbohydrate amounts.
The overall guiding principal for medical nutritionin T1DM today is that the same healthy diet that wouldbe ideal for an individual without diabetes would be idealfor an individual with T1DM. Thus, an appropriate dietseeks to obtain approximately 50% of calories from car-bohydrates, 30% from protein, and 20% from fat while lim-iting saturated fat and cholesterol intake. The medical teamshould monitor weight gain, keeping inmind that the samefactors inuencing the rising obesity epidemic also affectpatients with T1DM, and that long-term morbidity andmortality associated with obesity can be compounded bythe macrovascular and microvascular complications ofpoorly controlled T1DM. For this reason, any trend to-ward becoming overweight and obese should be addressedwithout delay.
HypoglycemiaHypoglycemia, biochemically dened as a plasma glucoselevel of 70 mg/dL or less, is a serious and common
drawback to insulin regimens that seek to control bloodglucose tightly. On average, hypoglycemia occurs twiceweekly in patients intensively treated for T1DM; and se-vere hypoglycemia, dened as an event in which a patientrequires the assistance of another person to administercarbohydrate or glucagon, has an incidence of 1.1 to1.5 episodes per patient-year. (13,14) Initial symptomsof hypoglycemia include tremor, pallor, weakness,sweating, anxiety, hunger, tachycardia, and transientcognitive impairment. Severe hypoglycemia is associatedwith signicant morbidity and mortality, including car-diac dysrhythmias, seizures, focal neurologic abnormali-ties, and rarely, permanent neurologic impairment anddeath.
Diabetes education should teach the patient and fam-ily to recognize the symptoms of early hypoglycemia,to check the blood glucose level, and to administer15 g of rapidly absorbable glucose (eg, glucose tablets)when the blood glucose level is less than 70 mg/dL.The blood glucose should then be rechecked 15 mi-nutes later, with the goal of a glucose level rise to 100mg/dL or greater. If the glucose level does not rise to100 mg/dL or greater, another 15 g should be givenand the process repeated until the concentration rises toat least 100 mg/dL. Families also should be taught to in-ject 0.5 to 1.0 mg of glucagon intramuscularly in situationsin which the patient has lost consciousness or is otherwiseunable to take oral glucose.
ExerciseExercise positively affects the overall physical, mental, andsocial health in youth with T1DM. The ability to enjoyphysical activity and to develop social skills and condencethrough sports participation helps to form a framework forfuture health as an adult. Exercise presents a challenge tomany patientswithT1DM,however, because of its propen-sity to induce hypoglycemia both during and after exerciseas glucose utilization and insulin sensitivity increase.
For this reason, patients should be counseled to checkblood glucose levels before, during, and after exercise.Before the start of exercise, blood glucose levels shouldbe greater than 100 to 120 mg/dL to decrease the likeli-hood of exercise-induced hypoglycemia, although, aswith all aspects of diabetes, this target should be adjustedempirically based on self-monitoring. During exercise,the glucose level should be checked each hour to targeta stable glucose concentration. Families should be coun-seled that the hypoglycemic effect of exercise can be de-layed (eg, occurring overnight after daytime exercise),a process thought to be related to repletion of muscle gly-cogen stores.
endocrine disorders type 1 diabetes mellitus
Pediatrics in Review Vol.34 No.5 May 2013 211
at Universidad Catolica de la Santisima Concepcion on March 4, 2014http://pedsinreview.aappublications.org/Downloaded from
-
Rather than increasing glucose consumption prior toexercise to prevent hypoglycemia, a preferable approachis to decrease the insulin doses that could affect glycemiclevels during exercise. This approach requires consider-ation of several variables, such as the intensity and dura-tion of exercise as well as the amount of insulin on board.These factors tend to make planning for exercise a processof trial and error.
Sick Day ManagementBecause the bodys stress response to acute illness tends totrigger stress hormones that increase glucose, childrenwith T1DM who experience acute illness should bemonitored closely by checking blood glucose and urineketone concentrations to prevent progression into wors-ening dehydration and DKA. Although many algo-rithms for home treatment during illness have beenderived, the basic tenants of sick day management arethat blood glucose and urine ketones should be checkedfrequently (eg, every 3-4 hours), that insulin should notbe withheld even when oral intake is limited, and thatsupplemental doses of rapid-acting insulin should begiven to correct hyperglycemia and suppress ketogenesis(eg, every 3-4 hours). Also, dehydration and subsequentacceleration towards DKA should be prevented by fre-quent, small sips of uids.
By carrying out the steps of diabetes sick day manage-ment early in the course of an illness, patients who oftenare in mild to moderate DKA can reverse and resolve ac-idosis. One algorithm of diabetes sick day rules is pre-sented in Table 5. Patients using insulin pumps shoulddeliver the rst dose of rapid-acting insulin with a syringesubcutaneously instead of using the pump to ensure thatthe insulin is delivered. In most cases, the pumps infu-sion set should be replaced with a new infusion set to en-sure insulin delivery is not being hindered by a crimp,injection site lipohypertrophy, or other abnormality withthe pump or infusion site. Families should be instructedabout factors that indicate worsening DKA or impendingcerebral edema, such as those listed in Table 4, thatwould warrant prompt evaluation by a medical team. Apostcard with diabetes sick day management steps forpatients can be found at http://www.childrenshospital.vanderbilt.org/uploads/documents/vdc_u_postcard.pdf.
Psychosocial IssuesThe diagnosis of T1DM presents a signicant stressor tothe patient and family as they deal with making signicantadjustments to their daily lives to manage the condition.During this time of initial adaptation, many childrenstruggle to make this adjustment, and those who do
struggle tend to have difculty with depression in theearly years of living with diabetes. Adolescents in partic-ular often will go through periods of anxiety, denial, andrejection of their diagnosis.
Children who have T1DM are, in general, more likelyto suffer from psychological disorders, particularly depres-sion and anxiety, than their unaffected peers. Patients whohave psychological disorders are much more likely to havepoor glycemic control and hospitalizations for DKA thanthose who do not. Because of the tendency for patientsand families to set self-management patterns and habitsin the early years of living with diabetes that are difcultto break, early identication of psychiatric illness is impor-tant. Family-based behavioral interventions, such as goalsetting, self-monitoring, positive reinforcement, behav-ioral contracts, supportive parental communication, andshared responsibility for diabetes management at an age-appropriate level, have been shown to affect glycemic man-agement positively. It is important to know that the levelof both parents involvement and acceptance of the con-dition plays a positive role in optimal glucose control.
Associated Autoimmune ConditionsPatients aficted with T1DM carry an increased risk forthe development of other autoimmune conditions. Auto-immune thyroid dysfunction is the most frequently
Table 5. Diabetes Sick Day RulesAlgorithm
Management Steps1. Check blood glucose level every 3-4 hours until feeling
well2. Give a correction factor dose with rapid-acting insulin
every 3-4 hours based upon the blood glucose check(even if not eating)
3. Check urine ketone concentrations every 3-4 hours4. Encourage fluid intake. Ideally give 1 oz. (30 mL) per
year of age per hour in small, frequent sips- If glucose level is 200 mg/dL, sugar-free fluids shouldbe given
- If glucose level is < 200 mg/dL, sugar-containingfluids should be included
Factors warranting medical evaluation1. Persistent vomiting (eg vomiting more than twice after
starting sick day rules) with moderate to large urineketone levels (or blood ketone levels greater than 1.5mmol/L)
2. Inappropriately rapid breathing3. Altered mental status4. Inability to perform sick day rules
endocrine disorders type 1 diabetes mellitus
212 Pediatrics in Review Vol.34 No.5 May 2013
at Universidad Catolica de la Santisima Concepcion on March 4, 2014http://pedsinreview.aappublications.org/Downloaded from
-
acquired autoimmune condition, with a prevalence ofapproximately 20% in patients with T1DM. (12) TheAmerican Diabetes Association (ADA) therefore recom-mends measuring a thyroid-stimulating hormone (TSH)level after metabolic control has been established toscreen for thyroid dysfunction and then every 1 to 2 yearsdespite previously normal TSH levels, and at any time ifgrowth is abnormal or if clinical suspicion exists for thy-roid dysfunction.
When both T1DM and thyroid disease are present, thepossibility of coexistent adrenal insufciency should beconsidered because the constellation of autoimmuneadrenalitis, autoimmune thyroiditis, and T1DM is pres-ent commonly in autoimmune polyglandular syndrometype 2.
Patients who have T1DM also are at increased risk forceliac disease, with an estimated prevalence of 4.5%, ascompared to approximately 1% in the general population.(12) The ADA additionally recommends that soon afterdiagnosis, patients with T1DM be screened for celiacdisease using tissue transglutaminase antibody or endo-mysial antibody assays, and subsequently if growth failureor gastrointestinal symptoms occur. (12) Many expertsperiodically rescreen patients who have negative antibodylevels initially. If symptoms are persistent but antibodylevels are negative, gastroenterology consultation and en-doscopic evaluation should be considered because thesensitivities of these screening antibody tests are modest.
ComplicationsLong-term complications from T1DM result from thetoxic effect of chronic hyperglycemia and manifest as bothmicrovascular disease (nephropathy, retinopathy, neurop-athy) and macrovascular disease (coronary artery disease,peripheral vascular disease, stroke). The importance oftight glycemic control to mitigate these effects has beenconrmed in large prospective studies. (15,16) Althoughclinical evidence of these vascular complications usuallydoes not become apparent until the adult years, the under-lying pathophysiologic process begins near the time of di-agnosis. Additionally, modiable or treatable risk factorsthat compound the risk for these comorbidities, such assmoking, hypertension, and hyperlipidemia, become ap-parent during the adolescent years. For these reasons,the pediatric years present a key opportunity for early de-tection of these processes and for interventions that wouldprevent or minimize future morbidity.
- NEPHROPATHY. The earliest evidence of diabetic ne-phropathy is microalbuminuria (dened as an albumin-to-creatinine ratio of 30 to 299 mg/g in a spot urine sample).
(12) If left unchecked, there is a substantial risk of de-terioration to gross proteinuria and, ultimately, to end-stagerenal disease. The early detection of microalbuminuria,however, presents an opportunity to reverse the trend to-ward nephropathy with careful glycemic and blood pressurecontrol. For this reason, the ADA recommends annualscreening for microalbuminuria once the patient is age 10years or older and has had diabetes for at least 5 years. (12)
- RETINOPATHY. Poor glycemic control is associatedwith substantially increased risk for diabetic retinopathy,a process that begins frequently during the pediatricyears; improving glycemic control can minimize the pro-gression of retinopathy. Because retinopathy usually isnot recognized earlier than 5 to 10 years after diagnosisand after pubertal onset, the ADA recommends that therst ophthalmologic examination should be obtained af-ter the child is age 10 years and has had T1DM for 3 to 5years, and routinely thereafter. (12)
- NEUROPATHY. Clinically evident diabetic neuropathyis rare in children and adolescents; but as with the othermicrovascular complications of T1DM, increased risk isassociated with poor glycemic control and disease dura-tion. The ADA recommends annual foot examinationsbeginning at puberty. (12)
- MACROVASCULAR COMPLICATIONS. Atheroscleroticdisease is a major complication of poorly controlledT1DM. Although macrovascular complications rarely be-come apparent before adulthood, studies evaluating ca-rotid intima media thickness, a sensitive marker forcoronary and cerebral vascular disease, have shown theintima to have greater thickness in children, adolescents,and young adults who have T1DM than in their age-matched counterparts. Studies evaluating intensive insu-lin therapy have demonstrated a signicant benet overstandard therapy for reducing the risk of excessive carotidintima media thickness, nonfatal myocardial infarction,stroke, and death from cardiovascular disease. Thesestudies also suggested that long-lasting and fundamentalvascular changes occur early in the course of suboptimallycontrolled T1DM, further emphasizing the importanceof tight glycemic control in the pediatric years. (17)
ProgressDespite the diseases challenges, patients with T1DMonce a uniformly fatal conditioncan lead lives markedby wellness and achievement through the diligence ofeffective self-management with assistance from membersof a diabetes care team. Emerging research continuesto broaden our understanding of the pathogenesis of
endocrine disorders type 1 diabetes mellitus
Pediatrics in Review Vol.34 No.5 May 2013 213
at Universidad Catolica de la Santisima Concepcion on March 4, 2014http://pedsinreview.aappublications.org/Downloaded from
-
T1DM and guide future treatment modalities to improveblood glucose control, lower the rate of diabetes-relatedcomplications, and reduce the daily burden of living withT1DM. Immunomodulating therapies, novel insulin ana-logues, and the articial pancreas are areas of researchthat seek to prevent, treat, and cure this condition. Asemerging research continues to advance treatment ofdiabetes, the principles of effective self-managementchampioned by Dr. Joslin will continue to form thefoundation for living successfully with T1DM.
References1. Liese AD, DAgostino RB Jr, Hamman RF, et al; SEARCH forDiabetes in Youth Study Group. The burden of diabetes mellitusamong US youth: prevalence estimates from the SEARCH forDiabetes in Youth Study. Pediatrics. 2006;118(4):151015182. Dabelea D, Bell RA, DAgostino RB Jr, et al; Writing Group for theSEARCH for Diabetes in Youth Study Group. Incidence of diabetes inyouth in the United States. JAMA. 2007;297(24):27162724
3. DIAMOND Project Group. Incidence and trends of child-hood Type 1 diabetes worldwide 1990-1999. Diabet Med. 2006;23(8):8578664. Sperling M. Pediatric endocrinology, 3rd ed. Philadelphia, PA:Saunders/Elsevier; 20085. Vehik K, Hamman RF, Lezotte D, et al. Increasing incidence oftype 1 diabetes in 0- to 17-year-old Colorado youth. Diabetes Care.2007;30(3):5035096. Roche EF, Menon A, Gill D, Hoey H. Clinical presentation oftype 1 diabetes. Pediatr Diabetes. 2005;6(2):75787. Dunger DB, Sperling MA, Acerini CL, et al; ESPE; LWPES.ESPE/LWPESconsensus statement ondiabetic ketoacidosis in childrenand adolescents. Arch Dis Child. 2004;89(2):1881948. Wolfsdorf J, Glaser N, Sperling MA; American DiabetesAssociation. Diabetic ketoacidosis in infants, children, and adoles-cents: A consensus statement from the American Diabetes Associ-ation. Diabetes Care. 2006;29(5):115011599. Newton CA, Raskin P. Diabetic ketoacidosis in type 1 and type 2diabetes mellitus: clinical and biochemical differences. Arch InternMed. 2004;164(17):1925193110. Glaser N, Barnett P, McCaslin I, et al; Pediatric Emer-gency Medicine Collaborative Research Committee of the Amer-ican Academy of Pediatrics. Risk factors for cerebral edema inchildren with diabetic ketoacidosis. N Engl J Med. 2001;344(4):26426911. Muir AB, Quisling RG, Yang MC, Rosenbloom AL. Cerebraledema in childhood diabetic ketoacidosis: natural history, radio-graphic ndings, and early identication. Diabetes Care. 2004;27(7):1541154612. Silverstein J, Klingensmith G, Copeland K, et al; AmericanDiabetes Association. Care of children and adolescents with type 1diabetes: a statement of the American Diabetes Association. Di-abetes Care. 2005;28(1):18621213. McCrimmon RJ, Sherwin RS. Hypoglycemia in type 1 di-abetes. Diabetes. 2010;59(10):2333233914. Pramming S, Thorsteinsson B, Bendtson I, Binder C. Symp-tomatic hypoglycaemia in 411 type 1 diabetic patients. Diabet Med.1991;8(3):21722215. The Diabetes Control and Complications Trial ResearchGroup. The effect of intensive treatment of diabetes on thedevelopment and progression of long-term complications ininsulin-dependent diabetes mellitus. N Engl J Med. 1993;329(14):97798616. Nathan DM, Lachin J, Cleary P, et al; Diabetes Control andComplications Trial; Epidemiology of Diabetes Interventions andComplications Research Group. Intensive diabetes therapy and carotidintima-media thickness in type 1 diabetes mellitus. N Engl J Med.2003;348(23):2294230317. Moore DJ, Gregory JM, Kumah-Crystal YA, Simmons JH.Mitigating micro-and macro-vascular complications of diabetesbeginning in adolescence. Vasc Health Risk Manag. 2009;5:1015103118. American Diabetes Association. Standards of medical care indiabetes2011. Diabetes Care. 2011;34(Suppl 1):S11S61
Summary
Type 1 diabetes mellitus (T1DM) is a chronic, lifelongdisorder of glucose homeostasis characterized byautoimmune destruction of the insulin-producingpancreatic b-cell, leading progressively to insulindeficiency and resultant hyperglycemia.
New-onset T1DM can present with the classic findingsof polyuria, polydipsia, polyphagia, and weight loss; asdiabetic ketoacidosis (DKA), with vomiting, abdominalpain, and lethargy in addition to the classic symptoms;or as an incidental finding discovered on urine orblood testing performed for other reasons.
DKA is a life-threatening acute complication of T1DMthat requires close monitoring for comorbidities,especially cerebral edema. Treatment focuses onrehydration and insulin replacement.
Because T1DM is a chronic illness, the best possiblemanagement is achieved when patients and theirfamilies attain ownership of their condition as part ofa continuing, empowering relationship with theirdiabetes care team.
Optimal health and wellness is achieved when bloodglucose is controlled tightly. Intensive controlsignificantly decreases the likelihood of developingthe microvascular and macrovascular complicationsof T1DM.
endocrine disorders type 1 diabetes mellitus
214 Pediatrics in Review Vol.34 No.5 May 2013
at Universidad Catolica de la Santisima Concepcion on March 4, 2014http://pedsinreview.aappublications.org/Downloaded from
-
PIR QuizThis quiz is available online at http://www.pedsinreview.aappublications.org. NOTE: Learners can take Pediatrics in Review quizzes and claim creditonline only. No paper answer form will be printed in the journal.
New Minimum Performance Level RequirementsPer the 2010 revision of the American Medical Association (AMA) Physicians Recognition Award (PRA) and credit system, a minimum performancelevel must be established on enduring material and journal-based CME activities that are certified for AMA PRA Category 1 CreditTM. In order tosuccessfully complete 2013 Pediatrics in Review articles for AMA PRA Category 1 CreditTM, learners must demonstrate a minimum performance levelof 60% or higher on this assessment, which measures achievement of the educational purpose and/or objectives of this activity.
In Pediatrics in Review, AMA PRA Category 1 CreditTM may be claimed only if 60% or more of the questions are answered correctly. If you score lessthan 60% on the assessment, you will be given additional opportunities to answer questions until an overall 60% or greater score is achieved.
1. You see a 12-year-old boy with a complaint of frequent urination. His mother is concerned because her fatherhas had type 2 diabetes mellitus for several years. Urinalysis in the office shows the presence of glucose. Yoususpect that the boy may have type 1 diabetes mellitus because he also has
A. Acanthosis nigricans.B. An elevated body mass index.C. Hispanic heritage.D. Hypertension.E. Weight loss.
2. A 6-year-old girl is admitted for new-onset hyperglycemia (ie, a fasting blood glucose level greater than 250mg/dL). She has had symptoms for approximately 2 weeks and looks ill. The most appropriate of the followingserum levels to measure first is
A. Autoantibodies.B. Electrolytes.C. Insulin.D. lipids.E. Transaminases.
3. You are reviewing dosage and management of insulin with a 9-year-old girl who weighs 35 kg and has hadtype 1 diabetes mellitus for several years. You calculate her total daily dose of insulin; she states she isreceiving 25 units per day. The following statement that is true and relevant to her dosage is that
A. After diagnosis of type 1 diabetes mellitus, the honeymoon phase lasts approximately 24 months.B. Approximately 50% of the total daily insulin prescribed is long acting, with the other 50% being short acting.C. The mixed-split regimen of insulin dosing allows for greater flexibility in diet than the basalbolus regimen.D. Prepubertal children tend to require a higher total daily dose of insulin.E. The usual total daily dose of insulin is between 2 and 3 units/kg per day.
4. A 3-year-old boy presents to the emergency department in diabetic ketoacidosis (ie, a blood sugar level of 450mg/dL). You resuscitate him with isotonic solution and admit him to your intensive care unit for monitoring.He is treated with normal saline and insulin at a rate of 0.1 unit/kg per hour. His blood glucose level graduallyfalls to 180 mg/dL, but ketosis persists, and the serum bicarbonate concentration is 13 mg/dL. At this time, themost appropriate medical management is to
A. Add bicarbonate to IV fluids, continue insulin infusion.B. Add bicarbonate to IV fluids, discontinue insulin infusion.C. Add dextrose to IV fluids, continue insulin infusion.D. Add dextrose to IV fluids, discontinue insulin infusion.E. Discontinue IV fluids, change to subcutaneous insulin.
5. A 5-year-old girl is undergoing treatment for diabetic ketoacidosis. Her level of consciousness fluctuates, sheis vomiting repeatedly, and her diastolic blood pressure is 105 mmHg. You should immediately
A. Add bicarbonate to the intravenous fluids.B. Administer mannitol.C. Administer potassium.D. Infuse hypotonic saline solution.E. Obtain neuroimaging to look for cerebral edema.
endocrine disorders type 1 diabetes mellitus
Pediatrics in Review Vol.34 No.5 May 2013 215
at Universidad Catolica de la Santisima Concepcion on March 4, 2014http://pedsinreview.aappublications.org/Downloaded from
-
DOI: 10.1542/pir.34-5-2032013;34;203Pediatrics in Review
Justin M. Gregory, Daniel J. Moore and Jill H. SimmonsType 1 Diabetes Mellitus
ServicesUpdated Information &
http://pedsinreview.aappublications.org/content/34/5/203including high resolution figures, can be found at:
Referenceshttp://pedsinreview.aappublications.org/content/34/5/203#BIBLThis article cites 17 articles, 8 of which you can access for free at:
Subspecialty Collections
tus_subhttp://pedsinreview.aappublications.org/cgi/collection/diabetes_melliDiabetes Mellitus_subhttp://pedsinreview.aappublications.org/cgi/collection/endocrinologyEndocrinologyfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://pedsinreview.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://pedsinreview.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
at Universidad Catolica de la Santisima Concepcion on March 4, 2014http://pedsinreview.aappublications.org/Downloaded from