Pediatrics 2014 Aliaga 236 42
9
DOI: 10.1542/peds.2013-0671 ; originally published online January 20, 2014; 2014;133;236 Pediatrics and P. Brian Smith Hope, Daniel K. Benjamin, David Kaufman, Antonio Arrieta, Daniel K. Benjamin Jr Sofia Aliaga, Reese H. Clark, Matthew Laughon, Thomas J. Walsh, William W. Changes in the Incidence of Candidiasis in Neonatal Intensive Care Units http://pediatrics.aappublications.org/content/133/2/236.full.html located on the World Wide Web at: The online version of this article, along with updated information and services, is of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point publication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly at Indonesia:AAP Sponsored on March 3, 2014 pediatrics.aappublications.org Downloaded from at Indonesia:AAP Sponsored on March 3, 2014 pediatrics.aappublications.org Downloaded from
-
Upload
emil-salim -
Category
Documents
-
view
8 -
download
0
description
good article
Transcript of Pediatrics 2014 Aliaga 236 42

DOI: 10.1542/peds.2013-0671; originally published online January 20, 2014; 2014;133;236Pediatrics
and P. Brian SmithHope, Daniel K. Benjamin, David Kaufman, Antonio Arrieta, Daniel K. Benjamin Jr
Sofia Aliaga, Reese H. Clark, Matthew Laughon, Thomas J. Walsh, William W.Changes in the Incidence of Candidiasis in Neonatal Intensive Care Units
http://pediatrics.aappublications.org/content/133/2/236.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on March 3, 2014pediatrics.aappublications.orgDownloaded from at Indonesia:AAP Sponsored on March 3, 2014pediatrics.aappublications.orgDownloaded from

Changes in the Incidence of Candidiasis in NeonatalIntensive Care Units
WHAT’S KNOWN ON THIS SUBJECT: The incidence of invasivecandidiasis in hospitalized infants is related to postnatalexposures, but large-scale studies relating the incidence ofinvasive candidiasis to changes in exposures over time are notavailable.
WHAT THIS STUDY ADDS: This study describes the associationbetween the incidence of invasive candidiasis and changes in useof antifungal prophylaxis, empirical antifungal therapy, and broad-spectrum antibacterial antibiotics over time.
abstractOBJECTIVE: Neonatal invasive candidiasis is associated with significantmorbidity and mortality. We describe the association between invasivecandidiasis and changes in use of antifungal prophylaxis, empirical anti-fungal therapy, and broad-spectrum antibacterial antibiotics over time.
METHODS: We examined data from 709 325 infants at 322 NICUs man-aged by the Pediatrix Medical Group from 1997 to 2010. We deter-mined the cumulative incidence of invasive candidiasis and use ofantifungal prophylaxis, broad-spectrum antibacterial antibiotics, andempirical antifungal therapy by year.
RESULTS: We identified 2063 (0.3%) infants with 2101 episodes of in-vasive candidiasis. Over the study period, the annual incidence of in-vasive candidiasis decreased from 3.6 episodes per 1000 patients to 1.4episodes per 1000 patients among all infants, from 24.2 to 11.6 epi-sodes per 1000 patients among infants with a birth weight of 750–999 g, and from 82.7 to 23.8 episodes per 1000 patients among infantswith a birth weight ,750 g. Fluconazole prophylaxis use increasedamong all infants with a birth weight ,1000 g (or ,1500 g), with thelargest effect on birth weights ,750 g, increasing from 3.8 per 1000patients in 1997 to 110.6 per 1000 patients in 2010. The use of broad-spectrum antibacterial antibiotics decreased among all infants from275.7 per 1000 patients in 1997 to 48.5 per 1000 patients in 2010. Theuse of empirical antifungal therapy increased over time from 4.0 per1000 patients in 1997 to 11.5 per 1000 patients in 2010.
CONCLUSIONS: The incidence of invasive candidiasis in the NICU de-creased over the 14-year study period. Increased use of fluconazoleprophylaxis and empirical antifungal therapy, along with decreaseduse of broad-spectrum antibacterial antibiotics, may have contributedto this observation. Pediatrics 2014;133:236–242
AUTHORS: Sofia Aliaga, MD, MPH,a Reese H. Clark, MD,b
Matthew Laughon, MD, MPH,a Thomas J. Walsh, MD,c,d,e
William W. Hope, MD, PhD,f Daniel K. Benjamin, PhD,g DavidKaufman, MD,h Antonio Arrieta, MD,i Daniel K. Benjamin Jr,MD, PhD,j,k and P. Brian Smith, MD, MPH, MHSj,k
aDivision of Neonatal-Perinatal Medicine, University of NorthCarolina, Chapel Hill, North Carolina; bPediatrix-Obstetrix,Greenville, South Carolina; cTransplantation-Oncology InfectiousDisease Program and Departments of dPediatrics andeMicrobiology, Weill Cornell Medical Center, New York, New York;fDepartment of Molecular and Clinical Pharmacology, Universityof Liverpool, Liverpool, United Kingdom; gDepartment ofEconomics, Clemson University, Clemson, South Carolina;hDepartment of Pediatrics, University of Virginia Health Systems,Charlottesville, Virginia; iDepartment of Pediatrics, Children’sHospital of Orange County, Orange, California; jDepartment ofPediatrics, Duke University, Durham, North Carolina; and kDukeClinical Research Institute, Durham, North Carolina
KEY WORDSinvasive candidiasis, fluconazole prophylaxis, premature infants
ABBREVIATIONSCI—confidence intervalELBW—extremely low birth weightOR—odds ratio
Drs Aliaga and Benjamin contributed to the conception anddesign of the study, analysis and interpretation of data, draftingof the manuscript, and revising of the article for importantintellectual content; Dr Clark contributed to the conception anddesign of the study and revising of the article for importantintellectual content; Drs Laughon, Walsh, Hope, Kaufman, Arrieta,and Benjamin contributed to the drafting of the manuscript andrevising of the article for important intellectual content; DrSmith contributed to the conception and design of the study,analysis and interpretation of data, and revising of the articlefor important intellectual content; and all authors approved thefinal version to be published.
www.pediatrics.org/cgi/doi/10.1542/peds.2013-0671
doi:10.1542/peds.2013-0671
Accepted for publication Nov 14, 2013
Address correspondence to P. Brian Smith, MD, MPH, MHS,Department of Pediatrics, Duke Clinical Research Institute, DukeUniversity, PO Box 17969, Durham, NC 27715. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2014 by the American Academy of Pediatrics
(Continued on last page)
236 ALIAGA et al at Indonesia:AAP Sponsored on March 3, 2014pediatrics.aappublications.orgDownloaded from

Invasive candidiasis is an importantcause of sepsis in the NICU. Candidainfections in infants are associatedwith significant mortality and morbidity,including neurodevelopmental impair-ment, among survivors.1–3 The incidenceof invasive candidiasis ranges from 2.6%to 13.2% in very low birth weight infants(,1500 g) and from 6.6% to 26.0% inextremely low birth weight (ELBW)infants (,1000 g).1–11
Previously identified risk factors forinvasive candidiasis in the NICU includelowbirthweight, prematurity, presenceof central catheters, days ofmechanicalventilation, abdominal surgery, andexposure to broad-spectrum antibac-terial antibiotics (eg, third-generationcephalosporins).1,11,12 The incidence ofinvasive candidiasis varies significantlyby center.1,3,13 Variation in the incidenceof invasive candidiasis and its associa-tion with poor outcomes should promptevaluation of how changes or differencesin clinical practices might influence therisk of acquiring this disease.
Invasive candidiasis inhospitalized infantsappears to be decreasing. We hypothe-sized that increased use of antifungalprophylaxis and empirical antifungaltherapy as well as avoidance of broad-spectrum antibacterial antibiotics mayexplain thedecreasing incidence. Herein,we use a large multicenter cohort todescribe the incidence of candidiasis inthe NICU and parallel changes in the useof antifungal prophylaxis, broad-spectrumantibacterial antibiotics, and empiricalantifungal therapy overa 14-yearperiod.
METHODS
We examined a cohort of all infantsdischarged from322NICUsmanagedbythe Pediatrix Medical Group from 1997to 2010. Data were collected pro-spectively from daily progress notesgenerated by clinicians. We determinedthe cumulative incidence of invasivecandidiasis and the use of antifungalprophylaxis,broad-spectrumantibacterial
antibiotics, and empirical antifungaltherapy by year.
Definitions
Evaluations for infectionwereperformedby using standard-of-care practices ateach NICU. We defined invasive candidi-asis as the presence of a positive culture(blood, urine, cerebrospinal fluid, or acombination of these). Urine cultureswere included only if obtained via in-and-outcatheterizedorsuprapubicaspiration.Multiple positive cultures for Candidawithin 21 days were considered a sin-gle episode of infection.
We defined antifungal prophylaxis asa combination of the following: (1) an-tifungal started in the first 5 postnataldays, (2) course of treatment lasting.7 days, and (3) no positive Candidaculture before or on the day the anti-fungal prophylaxis was started. Wedefined empirical antifungal therapyas a combination of the following: (1)presence of a culture obtained whilethe patient was receiving antifungaltherapy, (2) no positive Candida cul-tures within the previous 14 days, and(3) excluding therapy defined as anti-fungal prophylaxis. We defined theadministration of a broad-spectrumantibacterial antibiotic as exposure toa third-generation cephalosporin orcarbapenem at any time during theNICU hospitalization.
Statistical Analysis
We organized our data in 3 separateways: at the national level for each year,at the site level for each year, and at theculture level for each patient. At thenationalandsite levels, foreachyearwecalculated the incidence (episodes per1000 patients) of invasive candidiasis.We also calculated the use (per 1000patients)of antifungalprophylaxis, broad-spectrum antibacterial antibiotics, andempirical antifungal therapy. Both na-tionally and by site, the annual incidenceofcandidiasis,useofantifungalprophylaxis,
use of broad-spectrum antibacterial anti-biotics, and use of empirical antifungaltherapy were calculated for all infantsin our sample, as well as for those ineach of 4 birth weight groups:$1500 g,1000–1499 g, 750–999 g, and ,750 g.
To examine the association betweenbroad-spectrum antibacterial antibioticuse and the incidence of invasive can-didiasis at the site level, we accountedfor 2 key aspects of the data. In manycases, especially among heavier infants,the incidence of invasive candidiasis ata site was 0. In addition, the number ofobservationsvariedsubstantiallyacrosssites over time. We used Tobit models toaccount for the censoring of the data at0 and weighted the observations by thenumber of patients at each site in eachyear toaccount fordifferences insamplesize across sites.14
Weusedmultivariable logistic regressionto examine the relationship between ex-posure to broad-spectrum antibacterialantibiotics in the 7 days before a cultureand the development of invasive candi-diasis, controlling forgestationalage. Theunit of observation for this analysis wasthe culture. Because cultures wereobtained on widely varying days of lifeacross infants, we used conditional lo-gistic regression in which infants werestratified according to the postnatal daythe culture was obtained.12 All analyseswere performed by using Stata 12.0(StataCorp, College Station, TX). The DukeUniversity Institutional Review Board andthe Western Institutional Review Boardapproved this study.
RESULTS
We included 709 325 infants in the finalanalysis. A total of 2063 (0.3%) infantshad 2101 episodes of invasive candidi-asis. The median gestational age ofinfants with invasive candidiasis was26 weeks (interquartile range: 24–29weeks) compared with 35 weeks (33–38 weeks) for those without invasivecandidiasis (P , .001) (Table 1). The
ARTICLE
PEDIATRICS Volume 133, Number 2, February 2014 237 at Indonesia:AAP Sponsored on March 3, 2014pediatrics.aappublications.orgDownloaded from

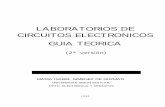
median birth weight for infants withinvasive candidiasis was 791 g (640–1193 g) compared with 2486 g (1825–3200 g) for those without invasivecandidiasis (P , .001). Mortality washigher for infants with invasive candi-diasis (19.9% vs 2.1%; P , .001). Overthe 14-year period, the annual incidenceof invasive candidiasis decreased from3.6 per 1000 infants to 1.4 per 1000infants, with the greatest decreaseamong infants with a birth weight,750 g (82.7 to 23.8 per 1000 infants)and infants with a birth weight of 750–999 g (24.2 to 11.6 per 1000 infants)(Fig 1). The incidence of invasive can-didiasis decreased beginning in 2001and continued to decrease through theremainder of the study period.
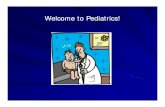
We identified 2831 (0.4%) infants whoreceived antifungal prophylaxis. Flucon-azole was the antifungal drug mostfrequently used for prophylaxis (n =2625, 92.7%). We observed increasinguse of fluconazole antifungal prophylaxisbeginning in 2002 (Fig 2). Over the studyperiod, the use of fluconazole for anti-fungal prophylaxis increased among allinfants from 0.1 per 1000 patients to 7.4per 1000 patients. The greatest increasewas observed among infantswith a birthweight,750 g, from3.8 to 110.6 per 1000patients.
We identified 7494 (1.1%) infants whoreceived $1 courses of empirical an-tifungal therapy, including 1417 infantswho received$2 courses. The medianduration of empirical courses was 8days (4, 14 IQR). Empirical treatmentincluded 3959 courses of amphotericinproducts and 4209 courses of flucona-zole. Among infants who received em-pirical antifungal therapy, 599 (8.0%)developed invasive candidiasis whilereceiving therapy. Over the study period,we observed an increase in empiricalantifungal therapy among all infants,from 4.0 per 1000 patients in 1997 to11.5 per 1000 patients in 2010. We ob-served the greatest increase among
infants with birth weight ,750 g, from67.7 to 206.0 per 1000 patients.
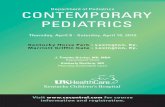
Over the study period, the use of broad-spectrum antibiotics decreased amongall infants from 275.7 to 48.5 per 1000patients (Fig 3). Exposure to broad-spectrum antibacterial antibiotics wasassociated with an increased risk ofinvasive candidiasis (adjusted odds ratio
[OR]: 1.88; 95% confidence interval [CI]:1.72–2.07; c statistic = 0.87). This find-ing was broadly mirrored at the level ofdifferent sites. Among the 3 smallerbirth weight groups (1000–1499 g, 750–999 g, and,750 g), each 10% decreasein the incidence of broad-spectrumantibacterial antibiotic use was asso-ciated with a 2.9% to 7.3% decrease in
TABLE 1 Demographic Characteristics
Invasive Candida Infection No Invasive Candida Infection
N 2063 707 262Gestational age, %,26 weeks 48.0 2.926–28 weeks 26.0 5.229–33 weeks 15.1 22.234–36 weeks 5.3 29.8$37 weeks 5.6 40.0
Birth weight, %,750 g 43.5 2.8750–999 g 24.2 3.51000–1499 g 15.4 9.2$1500 g 16.9 84.5
Race/ethnicity, %White 40.3 53.9African American 29.5 17.1Hispanic 27.1 24.2Other 3.1 4.9
Gender, %Male 57.1 56.1
Apgar score (5 min), %0–3 8.1 1.74–6 25.4 6.67–10 66.5 91.8
Inborn, % 75.0 85.1Died, % 19.9 2.1Antenatal steroid use, % 66.1 34.1Cesarean delivery, % 50.7 54.9
FIGURE 1Candidiasis by year and birth weight.
238 ALIAGA et al at Indonesia:AAP Sponsored on March 3, 2014pediatrics.aappublications.orgDownloaded from

the incidence of invasive candidiasis(Table 2). There was no significant as-sociation between broad-spectrumantibacterial antibiotic use and in-vasive candidiasis among infants witha birth weight of $1500 g (P = .18).
DISCUSSION
In this large cohort of hospitalizedinfants we observed a decrease in theincidence of invasive candidiasis overthe study period. We observed thelargest decrease among infants withbirth weights of,750 g and 750–999 g.During this same time period, we alsoobserved an increased use of antifungal
prophylaxis and empirical antifungaltherapy, as well as decreased use ofbroad-spectrum antibacterial antibiotics.These changes in clinical practice mayhave contributed to the decreased in-cidence of invasive neonatal candidiasis.
The decreasing incidence of invasivecandidiasis found in this study is sim-ilar to previously published data from130 523 infants admitted to 128 NICUsparticipating in the National Nosoco-mial Infections Surveillance System.13
Data from the system revealed a smalldecrease in the incidence of Candidabloodstream infection in infants witha birth weight ,1000 g, from 6.6% in
1995–1999 to 5.1% in 2000–2004.13 Ourdata reveal further decreases in in-vasive candidiasis among infants,1000 g after 2004. Changes in neonatalclinical practice are at least partiallyresponsible for the decreasing trend ofinvasive candidiasis. These changes inpractice, including increased use ofantifungal prophylaxis and decreaseduse of broad-spectrum antibacterialantibiotics, are supported by findingsfrom randomized clinical trials andobservational studies. A meta-analysisof 656 infants from 5 randomized trialsfound that fluconazole antifungal pro-phylaxis in high-risk infants reducesthe incidence of invasive candidiasis invery low birth weight infants by 52%(number needed to treat = 11; 95% CI:7–33).8,9,15 Results from the first ran-domized controlled trials of flucona-zole prophylaxis published in 2001 andthe first Cochrane review published in2004 likely influenced practice in NICUsin our data set.5,9,16 Our findings sug-gest that providers are administeringantifungal prophylaxis according to themost common recommendations thatprophylaxis should target infants withbirth weights ,1000 g, although themajority of infants with a birth weight,1000 g are not exposed to antifungalprophylaxis.17,18
Previous studies support an associa-tion between invasive Candida infec-tions and exposure to broad-spectrumantibacterial antibiotics.2,11,12,19 Broad-spectrum antibacterial antibiotic ex-posure in a cohort of 3702 ELBW infantswas associated with invasive candidi-asis (OR: 2.16; 95% CI: 1.42–3.27).11
Similarly, we observed an associationbetween broad-spectrum antibacterialantibiotics and increased risk of in-vasive candidiasis at the culture level(OR: 1.88; 95% CI: 1.72–2.07). In our co-hort, use of broad-spectrum antibac-terial antibiotics decreased over time,mirroring the decrease in invasivecandidiasis. Indeed, the Tobit regression
FIGURE 2Fluconazole prophylaxis by year and birth weight.
FIGURE 3Broad-spectrum antibacterial antibiotic use by year and birth weight.
ARTICLE
PEDIATRICS Volume 133, Number 2, February 2014 239 at Indonesia:AAP Sponsored on March 3, 2014pediatrics.aappublications.orgDownloaded from

results imply that, on average, sites thatreduced broad-spectrum antibiotic usethe most had the largest decrease incandidiasis.
Many ELBW infants are exposed toempirical courses of antifungal agentsfor suspected fungal sepsis. The in-creased use of empirical antifungaltherapy observed during the study pe-riod likely reflects an increased aware-ness of the need for early therapeuticintervention for improvedoutcome fromCandida sepsis and of the associationbetween invasive candidiasis and mor-tality and neurodevelopmental impair-ment in this high-risk population. Thediagnosis of invasive candidiasis ismade difficult by the nonspecific clinicalpresentation of the disease and lowsensitivity of current microbiologic di-agnostic techniques.17 Widespread useof empirical antifungal therapy couldpotentially contribute to a reduction inthe incidence of invasive candidiasis bydecreasing or eliminating fungal colo-nization. The effect of empirical anti-fungal therapy on outcomes will likelybemore significant if treatment coursestarget infants at higher risk of fungalsepsis.3,12,20
Weacknowledge thatotherunmeasuredpractice changes could contribute tothe decrease in invasive candidiasis. Agrowing number of NICU quality im-provement initiatives targeting centralcatheter management and designedto decrease central line–associatedbloodstream infections may have con-tributed to our findings. From 1999 to2009, data from the National Nosoco-mial Infections Surveillance Systemand the National Healthcare Safety
Network revealed that the overallincidence of central line–associatedbloodstream infections due to Candidaspp. decreased from 0.92 to 0.2 per1000 central line days.21 Hand-washinghas been identified as an importantpractice to decrease hospital-acquiredinfections.22,23 The introduction of cen-tral catheter management bundles andhand-washing compliance was notmeasured but may have contributed tothe reduction in invasive candidiasis.However, the incidence of bacteremiaremained stable at 30 per 1000 infantsin the years 1997–2001 versus 32 per1000 infants from 2006 to 2010. Anti-fungal treatment of neonatal candidi-asis has also changed over the pastdecade, with higher dosing recom-mendations for fluconazole therapyand the introduction of newer antifun-gal agents, such as the class of echi-nocandins.24–28 Decreased exposure toother risk factors might also explainthe decreased incidence of candidiasis.For example, overall histamine-2 blockeruse decreased from 66 per 1000 infantsin the years before the decrease incandidiasis (1997–2001) to 52 per 1000infants later in the study period (2006–2010). Similarly, exposure to mechanicalventilation decreased from 280 to 229per 1000 infants.
The decline in the incidence of invasivecandidiasis has a profound effect onrequired sample size for well-poweredtrials to evaluate the efficacy of anti-fungal agents for both prophylaxis andtreatment. For example, fluconazoleprophylaxis results in a relative riskreduction in the incidence of invasivecandidiasisofbetween50%and80%.15,29
The sample size required to observethis difference in the context of a clini-cal trial is now dramatically higher,given the decrease in the incidence ofneonatal candidiasis. The decrease inthe incidence of invasive candidiasiswill also have a large impact on en-rollment in antifungal efficacy trials.Most moderately sized NICUs admit∼500 infants per year. We estimatethat, given difficulties obtaining pa-rental consent, exposure of infectedinfants to previous empirical antifun-gal agents, and exclusion criteria, onlyone-third of infected infants could beenrolled in a randomized efficacy trial.Given a cumulative incidence of 1.4infections per 1000 infants, a 250-infantstudy would require 10 years and 100NICUs to complete enrollment.
Strengths of this study include thelarge number of infants in the analysis,particularly a significant proportion ofhospitalized ELBW infants from acrossthe United States. Given that the ma-jority of episodes of neonatal invasivecandidiasis occur in ELBW infants andin the NICU setting, our findings arelikely representative of the actual bur-den of disease in this population. Thisstudy provides evidence for an overalldownward trendof invasive candidiasisin the NICU population across thecountry. Of course, not all individualunits may have experienced the samedegree of change. Given the retro-spectivenatureof thesedata,wearenotable to examine causal relationshipsbetween changes in all clinical practi-ces and the reduced incidence of in-vasive candidiasis. It is also possiblethat later use of fluconazole (after thefirst 5days)was targetedprophylaxis ininfants being treated with prolongedantibiotics or that necrotizing entero-colitis was included in the empiricalantifungal category. We also acknowl-edge the possibility that other changesin clinical care, such as changes inventilator management, central line
TABLE 2 Effect of a 10% Decrease in Antibiotic Use on Incidence of Candidiasis (TobitRegressions)
Birth Weight, g Decrease in Candidiasis, per 1000 Infants Decrease in Candidiasis, % P
,750 3.0 7.3 ,.001750–999 1.3 5.7 ,.0011000–1499 0.2 2.9 ,.001$1500 ,0.1 0.4 .18
240 ALIAGA et al at Indonesia:AAP Sponsored on March 3, 2014pediatrics.aappublications.orgDownloaded from

care, and feeding practices, may haveinfluenced the riskof acquiring invasivecandidiasis. For example, although in-vasive candidiasis began to decrease in2001, the increase in antifungal pro-phylaxis did not begin until 2002.
CONCLUSIONS
Our findings show a substantial de-crease in the incidence of invasivecandidiasis in the NICU setting. This
decrease was likely the result of pro-gressive changes in neonatal clinicalpractice. The decreased incidence ofinvasive candidiasis will likely not onlyreduce overall health care costs butalso improve neonatal outcomes. EachNICU should closely monitor its in-cidenceof invasive candidiasis becauselow rates are achievable. Similar topreventing central line–associatedbloodstream infections and group B
Streptococcus, we want to eliminatethese infections. Additional clinical tri-als addressing the efficacy of antifungalprophylaxis and empirical antifungaltherapy may not be feasible given thecurrent incidence of the disease. Acomparison of practices between NICUswith high and low rates of candidiasismay be helpful in providing further evi-dence for best practices in the pre-vention of this disease.
REFERENCES
1. Stoll BJ, Hansen N, Fanaroff AA, et al. Late-onset sepsis in very low birth weightneonates: the experience of the NICHDNeonatal Research Network. Pediatrics.2002;110(2 pt 1):285–291
2. Benjamin DK Jr, Stoll BJ, Fanaroff AA, et al;National Institute of Child Health and HumanDevelopment Neonatal Research Network.Neonatal candidiasis among extremely lowbirth weight infants: risk factors, mortalityrates, and neurodevelopmental outcomesat 18 to 22 months. Pediatrics. 2006;117(1):84–92
3. Benjamin DK Jr, Stoll BJ, Gantz MG, et al;Eunice Kennedy Shriver National Instituteof Child Health and Human DevelopmentNeonatal Research Network. Neonatal candi-diasis: epidemiology, risk factors, and clinicaljudgment. Pediatrics. 2010;126(4). Available at:www.pediatrics.org/cgi/content/full/126/4/e865
4. Stoll BJ, Gordon T, Korones SB, et al. Late-onset sepsis in very low birth weightneonates: a report from the National In-stitute of Child Health and Human De-velopment Neonatal Research Network. JPediatr. 1996;129(1):63–71
5. Kicklighter SD, Springer SC, Cox T, HulseyTC, Turner RB. Fluconazole for prophylaxisagainst candidal rectal colonization in thevery low birth weight infant. Pediatrics.2001;107(2):293–298
6. Bertini G, Perugi S, Dani C, Filippi L, PratesiS, Rubaltelli FF. Fluconazole prophylaxisprevents invasive fungal infection in high-risk, very low birth weight infants. JPediatr. 2005;147(2):162–165
7. Uko S, Soghier LM, Vega M, et al. Targetedshort-term fluconazole prophylaxis amongvery low birth weight and extremely lowbirth weight infants. Pediatrics. 2006;117(4):1243–1252
8. Manzoni P, Stolfi I, Pugni L, et al; Italian TaskForce for the Study and Prevention of
Neonatal Fungal Infections; Italian Societyof Neonatology. A multicenter, randomizedtrial of prophylactic fluconazole in pretermneonates. N Engl J Med. 2007;356(24):2483–2495
9. Kaufman D, Boyle R, Hazen KC, Patrie JT,Robinson M, Donowitz LG. Fluconazoleprophylaxis against fungal colonization andinfection in preterm infants. N Engl J Med.2001;345(23):1660–1666
10. Healy CM, Baker CJ, Zaccaria E, CampbellJR. Impact of fluconazole prophylaxis onincidence and outcome of invasive candi-diasis in a neonatal intensive care unit. JPediatr. 2005;147(2):166–171
11. Cotten CM, McDonald S, Stoll B, GoldbergRN, Poole K, Benjamin DK Jr; National In-stitute for Child Health and Human De-velopment Neonatal Research Network. Theassociation of third-generation cephalo-sporin use and invasive candidiasis in ex-tremely low birth-weight infants. Pediatrics.2006;118(2):717–722
12. Benjamin DK Jr, DeLong ER, Steinbach WJ,Cotton CM, Walsh TJ, Clark RH. Empiricaltherapy for neonatal candidemia in verylow birth weight infants. Pediatrics. 2003;112(3 pt 1):543–547
13. Fridkin SK, Kaufman D, Edwards JR, ShettyS, Horan T. Changing incidence of Candidabloodstream infections among NICU patientsin the United States: 1995-2004. Pediatrics.2006;117(5):1680–1687
14. Wooldridge J. Economietric Analysis ofCross Section and Panel Data. Cambridge,MA: MIT Press; 2002
15. Clerihew L, Austin N, McGuire W. Pro-phylactic systemic antifungal agents toprevent mortality and morbidity in very lowbirth weight infants. Cochrane DatabaseSyst Rev. 2007;(4):CD003850
16. McGuire W, Clerihew L, Austin N. Pro-phylactic intravenous antifungal agents to
prevent mortality and morbidity in very lowbirth weight infants. Cochrane DatabaseSyst Rev. 2004;(1):CD003850
17. Pappas PG, Kauffman CA, Andes D, et al;Infectious Diseases Society of America.Clinical practice guidelines for the man-agement of candidiasis: 2009 update by theInfectious Diseases Society of America. ClinInfect Dis. 2009;48(5):503–535
18. Kaufman DA. Fluconazole prophylaxis: canwe eliminate invasive Candida infections inthe neonatal ICU? Curr Opin Pediatr. 2008;20(3):332–340
19. Pera A, Byun A, Gribar S, Schwartz R,Kumar D, Parimi P. Dexamethasone therapyand Candida sepsis in neonates less than1250 grams. J Perinatol. 2002;22(3):204–208
20. Procianoy RS, Enéas MV, Silveira RC. Em-piric guidelines for treatment of Candidainfection in high-risk neonates. Eur JPediatr. 2006;165(6):422–423
21. Chitnis AS, Magill SS, Edwards JR, ChillerTM, Fridkin SK, Lessa FC. Trends in Candidacentral line–associated bloodstream infec-tions among NICUs, 1999-2009. Pediatrics.2012;130(1). Available at: www.pediatrics.org/cgi/content/full/130/1/e46
22. Kilbride HW, Powers R, Wirtschafter DD,et al. Evaluation and development of po-tentially better practices to prevent neo-natal nosocomial bacteremia. Pediatrics.2003;111(4 pt 2). Available at: www.pediat-rics.org/cgi/content/full/111/4/e504
23. Kilbride HW, Wirtschafter DD, Powers RJ,Sheehan MB. Implementation of evidence-based potentially better practices to de-crease nosocomial infections. Pediatrics.2003;111(4 pt 2). Available at: www.pediat-rics.org/cgi/content/full/111/4/e519
24. Wade KC, Benjamin DK Jr, Kaufman DA,et al. Fluconazole dosing for the preventionor treatment of invasive candidiasis in
ARTICLE
PEDIATRICS Volume 133, Number 2, February 2014 241 at Indonesia:AAP Sponsored on March 3, 2014pediatrics.aappublications.orgDownloaded from

young infants. Pediatr Infect Dis J. 2009;28(8):717–723
25. Wade KC, Wu D, Kaufman DA, et al; NationalInstitute of Child Health and DevelopmentPediatric Pharmacology Research UnitNetwork. Population pharmacokinetics offluconazole in young infants. AntimicrobAgents Chemother. 2008;52(11):4043–4049
26. Smith PB, Walsh TJ, Hope W, et al. Phar-macokinetics of an elevated dosage ofmicafungin in premature neonates. PediatrInfect Dis J. 2009;28(5):412–415
27. Benjamin DK Jr, Smith PB, Arrieta A, et al.Safety and pharmacokinetics of repeat-dose micafungin in young infants. ClinPharmacol Ther. 2010;87(1):93–99
28. Hope WW, Smith PB, Arrieta A, et al. Pop-ulation pharmacokinetics of micafungin inneonates and young infants. AntimicrobAgents Chemother. 2010;54(6):2633–2637
29. McGuire W, Clerihew L. The effect of fluconazoleprophylaxis in very low birthweight infants isoverestimated by before-after studies. Arch DisChild Fetal Neonatal Ed. 2010;95(3):F182–F187
(Continued from first page)
FINANCIAL DISCLOSURE: Dr Benjamin receives support from the US government for his work in pediatric and neonatal clinical pharmacology (1R01HD057956-05,1K24HD058735-05, and Eunice Kennedy Shriver National Institute of Child Health and Human Development [NICHD] contract HHSN275201000003I) and the nonprofitorganization Thrasher Research Fund for his work in neonatal candidiasis (www.thrasherresearch.org); he also receives research support from industry forneonatal and pediatric drug development (www.dcri.duke.edu/research/coi.jsp). Dr Smith receives support for research from the National Institutes of Healthand the US Department of Health and Human Services (NICHD 1K23HD060040-01, DHHS-1R18AE000028-01, and HHSN267200700051C); he also receives researchsupport from industry for neonatal and pediatric drug development (www.dcri.duke.edu/research/coi.jsp). Dr Walsh is a scholar of the Henry Schueler Foundation,receives support from the SOS Kids Foundation (NHLBIR34), as well as research grants for experimental and clinical antimicrobial pharmacotherapeutics fromAstellas, ContraFect, Merck, and Novartis. He also serves as consultant to Astellas, ContraFect, Drais, iCo, Merck, Novartis, Pfizer, Sigma Tau, and Trius. The otherauthors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Supported by the National Institutes of Health and the US Department of Health and Human Services (NICHD 1K23HD060040-01 and with support from theAmerican Recovery and Reinvestment Act, DHHS-1R18AE000028-01) (Dr Smith). Funded by the National Institutes of Health (NIH).
POTENTIAL CONFLICT OF INTEREST: Drs Benjamin, Smith, and Laughon have consulted for Astellas, which makes micafungin, and Pfizer, which makes anidulafunginand fluconazole. Dr Benjamin has consulted for Merck, which makes caspofungin. Dr Walsh is on the board of iCo; has consulted for Novartis, Astellas, andMethylgene; and has grants/grants pending from Novartis, Merck, Astellas, Pfizer, and Gilead, all of which manufacture antifungal agents with activity againstCandida spp. The other authors have indicated they have no potential conflicts of interest to disclose.
242 ALIAGA et al at Indonesia:AAP Sponsored on March 3, 2014pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2013-0671; originally published online January 20, 2014; 2014;133;236Pediatrics
and P. Brian SmithHope, Daniel K. Benjamin, David Kaufman, Antonio Arrieta, Daniel K. Benjamin Jr
Sofia Aliaga, Reese H. Clark, Matthew Laughon, Thomas J. Walsh, William W.Changes in the Incidence of Candidiasis in Neonatal Intensive Care Units
ServicesUpdated Information &
mlhttp://pediatrics.aappublications.org/content/133/2/236.full.htincluding high resolution figures, can be found at:
References
ml#ref-list-1http://pediatrics.aappublications.org/content/133/2/236.full.htat:This article cites 28 articles, 13 of which can be accessed free
Rs)3Peer Reviews (PPost-Publication
http://pediatrics.aappublications.org/cgi/eletters/133/2/236
R has been posted to this article: 3One P
Subspecialty Collections
munization_subhttp://pediatrics.aappublications.org/cgi/collection/vaccine:imVaccine/Immunization
_diseases_subhttp://pediatrics.aappublications.org/cgi/collection/infectiousInfectious Diseases
gy_subhttp://pediatrics.aappublications.org/cgi/collection/neonatoloNeonatology
orn_infant_subhttp://pediatrics.aappublications.org/cgi/collection/fetus:newbFetus/Newborn Infantthe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on March 3, 2014pediatrics.aappublications.orgDownloaded from