Pediatrics 2013 Harutyunyan Peds.2012 2351
12
DOI: 10.1542/peds.2012-2351 ; originally published online November 4, 2013; Pediatrics Frances Stillman Arusyak Harutyunyan, Narine Movsisyan, Varduhi Petrosyan, Diana Petrosyan and Trial Reducing Children's Exposure to Secondhand Smoke at Home: A Randomized http://pediatrics.aappublications.org/content/early/2013/10/30/peds.2012-2351 located on the World Wide Web at: The online version of this article, along with updated information and services, is of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point publication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly at Philippines:AAP Sponsored on December 2, 2013 pediatrics.aappublications.org Downloaded from at Philippines:AAP Sponsored on December 2, 2013 pediatrics.aappublications.org Downloaded from
description
xxxx
Transcript of Pediatrics 2013 Harutyunyan Peds.2012 2351

DOI: 10.1542/peds.2012-2351; originally published online November 4, 2013;Pediatrics
Frances StillmanArusyak Harutyunyan, Narine Movsisyan, Varduhi Petrosyan, Diana Petrosyan and
TrialReducing Children's Exposure to Secondhand Smoke at Home: A Randomized
http://pediatrics.aappublications.org/content/early/2013/10/30/peds.2012-2351
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Philippines:AAP Sponsored on December 2, 2013pediatrics.aappublications.orgDownloaded from at Philippines:AAP Sponsored on December 2, 2013pediatrics.aappublications.orgDownloaded from

Reducing Children’s Exposure to Secondhand Smokeat Home: A Randomized Trial
WHAT’S KNOWN ON THIS SUBJECT: The World Health Organizationestimates that !700 million children breathe tobacco smokepolluted air, particularly at home. Educational strategies eitherdirectly or indirectly targeting household decision-makersthrough other family members are effective in reducing children’sexposure in private homes.
WHAT THIS STUDY ADDS: Intensive intervention was effective indecreasing children’s personal exposure to secondhand smoke (SHS),educating mothers about SHS, and promoting smoking restrictions athome. However, superiority over minimal intervention to decreasechildren’s personal exposure to SHS was not statistically signi!cant.
abstractOBJECTIVE: To develop and test an intervention to reduce children’sexposure to secondhand smoke (SHS) at homes in Yerevan, Armenia.
METHODS: A single-blind, randomized trial in 250 households with 2- to6-year-old children tested an intensive intervention (counseling sessions,distribution of tailored educational brochures, demonstration of homeair pollution, and 2 follow-up counseling telephone calls) against minimalintervention (distribution of standard lea"ets). At baseline and 4-monthfollow-up, researchers conducted biomonitoring (children’s hair) andsurveys. The study used paired t tests, McNemar’s test, and linear andlogistic regression analyses.
RESULTS: After adjusting for baseline hair nicotine concentration,child’s age and gender, the follow-up geometric mean (GM) of hairnicotine concentration in the intervention group was 17% lower thanin the control group (P = .239). The GM of hair nicotine in theintervention group signi!cantly decreased from 0.30 ng/mg to 0.23ng/mg (P = .024), unlike in the control group. The follow-up surveyrevealed an increased proportion of households with smokingrestrictions and decreased exposure of children to SHS in bothgroups. The adjusted odds of children’s less-than-daily exposure toSHS at follow-up was 1.87 times higher in the intervention groupthan in the control group (P = .077). The GM of mothers’ knowledgescores at follow-up was 10% higher in the intervention group than inthe control group (P = .006).
CONCLUSIONS: Intensive intervention is effective in decreasing child-ren’s exposure to SHS through educating mothers and promotingsmoking restrictions at home. However, superiority over minimal in-tervention to decrease children’s exposure was not statistically sig-ni!cant. Pediatrics 2013;132:1–10
AUTHORS: Arusyak Harutyunyan, MD, MPH,a NarineMovsisyan, MD, MPH,a Varduhi Petrosyan, MS, PhD,a DianaPetrosyan, MD, MPH,a and Frances Stillman, EdD, EdMb
aCollege of Health Sciences, American University of Armenia,Yerevan, Armenia; and bInstitute for Global Tobacco Control,Bloomberg School of Public Health, Johns Hopkins University,Baltimore, Maryland
KEY WORDSchildren, nicotine, personalized feedback, randomized controlledtrial, secondhand smoke
ABBREVIATIONSGM—geometric meanOR—odds ratioPM—particulate matterSHS—secondhand smoke
Dr Harutyunyan contributed to the study design, coordinated thedata collection, performed data analysis, conceptualized thescope of the paper, and drafted the manuscript; Dr Movsisyan,Dr Stillman, and Dr V. Petrosyan contributed to the studyconcept and design, accuracy and completeness of dataanalysis, interpretation of the results, and revision of themanuscript for important intellectual content; and Dr D.Petrosyan contributed to the study design, data collection, andinterpretation of the results. All authors approved the !nalversion of the manuscript.
This trial has been registered at www.clinicaltrials.gov(identi!er NCT01630356).
www.pediatrics.org/cgi/doi/10.1542/peds.2012-2351
doi:10.1542/peds.2012-2351
Accepted for publication Sep 3, 2013
Address correspondence to Arusyak Harutyunyan, MD, MPH,Baghramyan 40, Yerevan, Armenia. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno !nancial relationships relevant to this article to disclose.
FUNDING: Funded by FAMRI (Flight Attendant Medical ResearchInstitute) Center of Excellence in Translational Research atJohns Hopkins University.
POTENTIAL CONFLICT OF INTEREST: The authors have indicatedthey have no potential con"icts of interest to disclose.
PEDIATRICS Volume 132, Number 6, December 2013 1
ARTICLE
at Philippines:AAP Sponsored on December 2, 2013pediatrics.aappublications.orgDownloaded from

Secondhand smoke (SHS), a complexmixture of gases and particles thatcontains many carcinogenic and toxiccompounds,1,2 results from tobaccosmoking indoors. The US Environmen-tal Protection Agency has classi!edtobacco smoke as a known humancarcinogen, with no safe level of expo-sure.3 The scienti!c evidence is clearthat SHS exposure causes diseasesin adults and children. Children’s ex-posure is involuntary and primarilyoccurs through adults smoking in pla-ces where children live and play.
Given that.1 billion adults worldwidesmoke, the World Health Organizationestimates that !700 million, or al-most one-half of the world’s children,breathe air polluted by tobacco smoke,particularly at home.4 In children,SHS exposure leads to reduced birthweight, lower respiratory tract ill-nesses, chronic respiratory symptoms,middle ear disease, and reduced lungfunction.5 The large number of childrenexposed to SHS suggests a substantialpublic health threat worldwide.
Armenia has high rates of tobacco use(63.0% of men; 2.0% of women), with themajority of households (82.2%) having atleast 1 smoker.6,7 Approximately 70.0% of
households do not have any restrictionson smoking.8
The World Health Organization recom-mends legislation and education to pro-tect children from SHS exposure.9
However, legislation is of limited value inreducing exposure in private homes, andeducational strategies, including educa-tion about the risks to children from SHSexposure and steps to eliminate expo-sure, are suggested to be more effectivein these settings. Educational programsmust strategically target householddecision-makers, either directly or in-directly through other family members.4
Randomized studies of culturally ap-propriate tobacco-related interventions,particularly SHS reduction inter-ventions, are rare. Although certaingeneric approaches may be effective,many agree that an intervention ap-proach that takes into considerationcultural attitudes, norms, expectations,and values would be more likely to in-crease acceptance and adoption of theprogramand improve its effectiveness.10
The goal of the current studywas to testthe hypothesis that an interventionwhich uses motivational interviewingalong with immediate feedback andfollow-up counseling telephone calls
would be effective in educating house-holdmembersabout thehealthhazardsof smoking and SHS exposure and re-ducing children’s exposure to SHS inhouseholds in Armenia.
METHODS
Study Design
The study was a randomized controlledtrial with 2 arms (intervention and con-trol groups) conducted from May 2010to November 2010 (Fig 1). A pilot study of10 households preceded the clinical trialto test the recruitment strategy, studyprotocols, and instruments and to !nal-ize intervention strategies.
Study Population
The sample population included house-holds with a nonsmoking mother and atleast 1 child 2 to 6 years of age residingwith at least 1 daily smoker. The studytargeted homes with young children forwhom the major source of exposure totobacco smoke was smoking by parentsor other household members.4 The ex-clusion criteria weremother’s pregnancyand residency outside of Yerevan.
The study team recruited the house-holds through pediatrician’s of!ces in
FIGURE 1Study design. a Educational brochure, “Secondhand Tobacco Smoke and the Health of Your Family.” b Lea"et by the US Environmental Protection Agency.
2 HARUTYUNYAN et al at Philippines:AAP Sponsored on December 2, 2013pediatrics.aappublications.orgDownloaded from

polyclinics (primary health care facili-ties) by using multistage random sam-pling. First, the study team randomlyselected 10 polyclinics from the list of 19providing services to the population ofYerevan, the capital city of the Republicof Armenia. At each polyclinic, the studyteam selected 5 pediatrician of!ces(those that were open at the time of thestudy) and randomly selected medicalrecords of children aged 2 to 6 years.The study team recruited 5 eligiblehouseholds from each pediatrician.
Interviewers telephoned each house-hold selected to check for eligibility,provide information about the studyand its procedures, and arrange the!rst home visit upon oral consent. The250 households recruitedwere assignedrandom numbers from 1 to 250; house-holds with odd numbers were includedin the intervention group (intensive in-tervention) and those with even num-bers were included in the control group(minimal intervention). Study partic-ipants were unaware of their assign-ment status.
Data Collection
Trained interviewers made 2 baselinevisits (1 week apart) and two 4-monthfollow-up household visits to conductmeasurements, surveys, and the in-tervention (Fig 1). Measurements in-cluded hair samples from children toassess changes in nicotine concentra-tion over time; this biomarker is a val-idated method to quantify personaluptake of nicotine.11,12 Given that eachcentimeter of hair re"ects!1 month ofexposure to SHS, a small sample of hair(!30–50 strands, 2–3 cm) was cut nearthe hair root from the back of the scalpwhere there is the most uniform growthpattern between individuals; thismethodminimizes the variability of the results.12
Surveys were conducted among non-smoking mothers and 1 of the dailysmokers in each household. The !rstchoice was the father, if he was a daily
smoker. If the father did not smoke, thecounseling was conducted with 1 of thehousehold smokers who spent moretime with the child at home. Theinterviewer-administered question-naire required!15minutes to completeand covered demographic information,knowledge about health hazards of SHS,and household smoking-related practi-ces. The instrument was adapted fromthe Global Adult Tobacco Survey: CoreQuestionnaire With Optional Questions.13
The study team translated the question-naire into Armenian and pretested itduring the pilot phase.
Intervention
The intervention included an in-personcounseling session with the nonsmokingmotherandat least 1daily smoker ineachhousehold, with distribution of a tailorededucational brochure and demonstra-tion of measurement of indoor particu-late matter (PM2.5) (at second baselinevisit); it also included 2 follow-up coun-seling telephone calls 1 and 2 monthsafter the initial session. The interventionwas based on the motivational inter-viewing technique, which is a directive,client-centered counseling techniquefor eliciting behavior change that hasbeen shown to be effective in smokingcessation and SHS reduction inter-ventions.14–16 The control group re-ceived only a brief educational lea"et onthe hazards of SHS developed by the USEnvironmental Protection Agency.17
In-person Counseling Session
The study team provided counseling oneliminating child exposure to tobaccosmoke to at least 1 daily smoker and tothe mother in the household. Thecounseling session emphasized thefollowing issues: (1) importance ofa healthy environment at home; (2)health dangers of smoking and expo-sure to SHS; (3) why and how to quitsmoking; and (4) how to keep home airsmoke-free. At the end of the 40-minute
counseling session, each family re-ceiveda tailoredandculturallyadjustededucational brochure developed by thestudy team.
Demonstration of PM2.5 Pollution
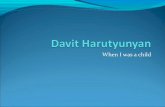
The study teammeasured the PM2.5 in theair by using the TSI AM 510 AerosolSidePak18 to compare the quality of in-door air with outdoor air and demon-strate the effect of smoking on indoor airquality in the intervention households.After completing the PM2.5 measurement,the interventionist immediately down-loaded the data to a laptop to visualize theresults through graphical presentation ofthe PM2.5 "uctuations for immediatefeedback (Fig 2). Feedback, as part of anintervention, has been extensively used inhealth promotion, particularly for addic-tive behavior change.19 Demonstrationof the indoor PM2.5 pollution was a risk-based personalized feedback requiringless effort from participants to make theinformation personally relevant.
Follow-up Counseling Telephone Calls
Interventionists made 2 follow-up coun-seling telephone calls to nonsmokingmothers at 1 and 2 months after the in-person counseling session. These callsaimed at: (1) assessing the progress inmeeting the goals set earlier; (2) coun-seling on barriers to change; and (3)encouraging study participants to main-tain progress made or to set new goals.These calls also provided an opportunityto ask questions or clarify issues.
Sample Size Calculation
Thesample size calculationwasbasedondata from an earlier study.20 Using theformula for comparison of 2 groups ofequal size and assuming a type I errorof 0.05 to detect a 30% reduction in hairnicotine concentration in the inter-vention group and a 10% reduction in thecontrol group, 62 households wereneeded in each group to detect the hairnicotine concentration changeswith 80%
ARTICLE
PEDIATRICS Volume 132, Number 6, December 2013 3 at Philippines:AAP Sponsored on December 2, 2013pediatrics.aappublications.orgDownloaded from

power.21 Adjusting for 10% potential re-fusal to provide hair samples and 40%potential losses to follow-up, the studyestimated the sample size to be equalto 250.
Data Analysis
The data were analyzed by using Stataversion 10 (Stata Corp, College Station,TX). The study team compared thebaseline and follow-upmeasurements inboth groups by using paired t tests forcomparison of continuous measuresand McNemar’s test for paired pro-portions. The primary outcome variablewas child’s hair nicotine concentra-tion. Self-reported household smokingrestrictions, frequency of smoking in thepresence of the child, and participants’knowledge scores were the secondaryoutcomes. We assessed the respon-dents’ knowledge by asking whethersmoking or SHS caused a list of healthconditions, with 1 point for each correctanswer. The knowledge score was cal-culated as the sum of all scores on theknowledge questions.
Time-weighted average of hair nicotinewas assayed at the Exposure Assess-ment Facility at Johns Hopkins Bloom-berg School of Public Health.20 Theskewed hair nicotine concentrationdata were log-transformed for statis-tical analysis. In addition, to comparehair nicotine concentrations at base-line and follow-up, we estimated thegeometric mean (GM) and 95% con!-dence intervals of the hair nicotineconcentrations.
The study team also compared thechange in the outcome variables frombaseline to follow-up between the in-tervention and control groups by usingmultiple logistic and linear regressionmodels. The follow-up measurementswere considered as dependent varia-bles, baselinemeasurements andotherpotential confounders as independentvariables, and the intervention as themain dichotomous independent vari-able of interest.
The study used an intention-to-treatapproach during statistical analysesto avoid the drop-out effect by imputing
all themissing follow-up datawith theirbaseline values.22
Ethical Considerations
The institutional reviewboardsof JohnsHopkins Bloomberg School of PublicHealth and American University of Arme-nia approved the study.
RESULTS
Participants’ Recruitment andRetention
More than one-half of the contactedhouseholds (58.2%) were not eligiblefor participation, 30.3% refused toparticipate (most of them refused be-fore the eligibility criteria screening),and 0.7% agreed but were not availablefor baseline data collection. Overall, 250households were enrolled in the study,and 250 mothers and 230 smokersparticipated in the baseline survey. Atbaseline, 173 households agreed toprovide hair samples from their child(83 intervention, 90 control). Of 244households eligible for the follow-up
FIGURE 2Example of the graphical presentation of the PM2.5 measurement taken from an intervention household.
4 HARUTYUNYAN et al at Philippines:AAP Sponsored on December 2, 2013pediatrics.aappublications.orgDownloaded from

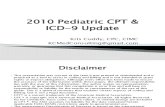
measurement, 224 completed the study(110 intervention, 114 control) (Fig 3).Among them, 137 households (67 in-tervention, 70 control) provided theirchild’s hair samples at follow-up, andthe remaining were treated by using anintention-to-treat approach. Comparisonof sociodemographic characteristics be-tween those who completed the studyand thosewhodropped out did not revealany signi!cant differences.
Participants’ Characteristics
The mean 6 SD age of nonsmokingmothers was 30.0 6 5.2 years. Almostone-half (53.6%) were employed, andmore than one-third (36.3%) had gradu-ated with a university degree. The meanage of smokers was 38.2 6 11.4 years,and the overwhelming majority (81%)were the children’s fathers. Approxi-mately 31.3% of smokers had a universitydegree, and 72.1% were employed overthe past 12 months. The mean age ofchildren was 4.06 1.2 years, and 49.1%were girls. Demographic characteristicsof participants were similar in the in-tervention and control groups (Table 1).
Children’s Hair NicotineConcentration
Table 2 presents the summary of thehair nicotine concentrations at base-line and follow-up. The GM of hair nic-otine levels of control group children atbaseline and follow-up was 0.29 ng/mgand 0.27 ng/mg, respectively (P = .613).For the intervention group, GM de-creased from 0.30 ng/mg to 0.23 ng/mg, and this 23.3% decrease was sta-tistically signi!cant (P = .024).
Multiple linear regression analysisdemonstrated that after adjusting forthe baseline hair nicotine concentra-tion, child’s age, and child’s gender, thefollow-up GM of hair nicotine concen-tration was 17% lower in the in-tervention group compared with thecontrol group (P = .239) (Table 3).
Smoking Practices in Households
At baseline, there were 1.56 0.8 smok-ers in each household smoking a meanof 25.5 6 11.5 cigarettes per day.Smoking was allowed in all households,with some restrictions in approximatelyone-half of homes. According to moth-ers, 5 (4.5%) intervention householdsand 6 (5.4%) control households com-pletely banned indoor smoking at follow-up. In addition, 5 (4.5%) smokers in theintervention group and 1 (0.9%) in thecontrol group have reportedly stoppedsmoking at follow-up.
Table 4 presents the proportion ofhouseholds with smoking restrictionsat baseline and follow-up. Based onmothers’ report, the odds of having anysmoking restriction at follow-up wasstatistically signi!cantly higher than atbaseline in both the intervention (oddsratio [OR]: 4.67) and control (OR: 3.14)households. According to the smokers,the increase in the proportion ofhouseholds with smoking restrictionsat follow-up was statistically signi!cantonly in the intervention group (OR: 2.62).At follow-up, mothers and smokers inboth groups reported statistically sig-ni!cantly less exposure of children toSHS (Table 5).
Multiplelogisticregressionanalysisfoundthat, based on mothers’ report, at follow-up the adjusted odds of child’s less-than-daily exposure to SHS was marginallysigni!cantly higher in the interventiongroup compared with the control group(OR: 1.87, P = .077) (Table 6).
Knowledge About Hazards ofSmoking and SHS
Paired analysis of knowledge scoresrevealed that the knowledge of in-tervention and control group partic-ipants increased signi!cantly frombaseline to follow-up. The mothers’mean knowledge score increased from9.5 to 11.3 in the intervention group andfrom 9.8 to 10.5 in the control group.
Among smokers, it increased from 7.1to 8.6 and 7.1 to 7.9, respectively. Linearregression analysis suggests that theGM of the mothers’ knowledge score atfollow-up was 10% higher in the in-tervention group comparedwith controlgroup, after controlling for baselineknowledge score (P = .006).
DISCUSSION
Protecting children from SHS exposureat homes is a complex and sensitiveissue and has many social and politicalimplications; hence, it is dif!cult tomonitor and regulate people’s behaviorat home.23 There is a large disparitybetween male and female smokingrates in Armenia, which poses an addi-tional unique challenge for protectingyoung children from tobacco smoke insimilar societies. This study was the !rstclinical trial in Armenia designed to de-velop and test a culturally appropriateintervention to encourage implementa-tion of smoke-free homes and reducechildren’s exposure to SHS.
The results of this trial suggest thatadjusted follow-up GM of hair nicotineconcentration in the intervention groupwas 17% lower compared with thecontrol group. However, this differencewas not statistically signi!cant, whichcould be due to insuf!cient power, asfewer numbers of families providedhair samples at follow-up. The com-parison of children’s hair nicotineconcentration at baseline and follow-up revealed statistically signi!cantdecreases only in the interventiongroup.
A higher proportion of households atfollow-up in both groups had smokingrestrictionsanddecreasedsmokingnexttothechild.Mothersreportedmarginallysigni!cantly less daily exposure ofchildren to SHS in the interventiongroup than in the control group.Knowledge score improved in boththe intervention and control groups;
ARTICLE
PEDIATRICS Volume 132, Number 6, December 2013 5 at Philippines:AAP Sponsored on December 2, 2013pediatrics.aappublications.orgDownloaded from

however, improvement of themothers’knowledge score was statisticallysigni!cantly higher in the interventiongroup only.
Some of the observed changes in bothgroups might have been prompted byparticipation in the study, focusingon children’s exposure to SHS at
homes.24 Moreover, other research-ers have also reported dif!cultiesin detecting the true difference be-tween groups when the control
FIGURE 3Flow of participants.
6 HARUTYUNYAN et al at Philippines:AAP Sponsored on December 2, 2013pediatrics.aappublications.orgDownloaded from

group receives a low-intensity in-tervention.25
The current study evaluated the effec-tivenessof an interventionpackage thatincluded PM2.5 measurement at hometo demonstrate the effect of smokingon indoor air quality in the interventionhouseholds. PM2.5 measurement doesnot require laboratory analysis as dopassive air and hair nicotine mea-surements, and it allows an immediatepersonalized feedback to householdmembers. Several other studies thatprovided feedback to parents, such as
levels of air nicotine in the home orbiochemical markers of SHS exposureas part of the intervention, were effec-tive in SHS reduction and smoking ces-sation.19,26 A pilot study by Wilson et al26
provided information to 54 participantsabout PM2.5 levels in their homes andsuggested that personalized data couldmake the concept of SHS dangers morereal to participants than if they hadmerely heard or read about it.
A number of studies have investigatedmethods to reduce children’s SHSexposure by targeting parental smoking
behavior change or smoking cessation.Some of them demonstrated successthrough decreased children’s SHSexposure measured according toself-reported parental smoking,27–30
reduced levels of air nicotine con-centrations,15,28,30 or reduced urinecotinine assays.10,27–29 The currentstudy used participants’ self-reportedand biochemical (hair nicotine) mea-sures for outcome analysis. Hair nico-tine concentrations provide betterinformation on long-term SHS expo-sure than biomarker measures inurine, saliva, or serum because of theshorter half-life of the latter bio-markers.12 Studies investigating thecorrelation between self-reported andobjective measures demonstrated thatself-reported exposure to SHS maybe both a valid and reliable measureto characterize SHS exposure.28,31,32
Adams et al33 suggested that parallelbiological or environmental measure-ments and anonymity of the surveyenhance the accuracy of self-reportedmeasurements. We targeted both non-smoking mothers and smoking familymembers of the household (mainlychildren’s fathers) to increase thelikelihood of smoking behavior changein the household, considering that themajority of households in Armenia(75%) make joint decisions regardinghealth-seeking behavior.6
TABLE 1 Baseline Demographic Characteristics of Respondents a
Characteristic Mothers Household Smokers
Intervention Group (n = 125) Control Group (n = 124) Intervention Group (n = 118) Control Group (n = 112)
Age, mean 6 SD, y 30.4 6 5.2 29.7 6 5.2 38.2 6 10.6 38.2 6 12.3EducationSecondary/less than secondary school 45 (36.0) 53 (43.1) 56 (47.5) 69 (61.6)2-year college 30 (24.0) 30 (24.4) 18 (15.3) 15 (13.4)University/postgraduate degree 50 (38.4) 40 (32.5) 44 (37.3) 28 (25.0)
Employed 66 (52.8) 67 (54.5) 87 (73.7) 79 (70.5)Male gender, child 61 (49.2) 69 (55.2) — —
Relationship to the childMother 125 (100) 124 (100) — —
Father — — 79 (81.4) 71 (79.8)Grandfather — — 11 (11.3) 12 (13.5)Grandmother — — 5 (5.2) 3 (3.4)Uncle — — 2 (2.1) 3 (3.4)
Unless otherwise noted, values are given as n (%).a No statistically signi!cant differences between the intervention and control groups (P . .05).
TABLE 2 Hair Nicotine Concentration (Nanogram/Milligram) According to Intervention andControl Groups
Variable Intervention Group Control Group
Baseline (n = 83) Follow-up (n = 83) P a Baseline (n = 90) Follow-up (n = 90) Pa
Mean (95% CI) 0.54 (0.42–0.67) 0.40 (0.30–0.50) .024 0.71 (0.48–0.98) 0.51 (0.38–0.65) .613Median (IQR) 0.30 (0.14–0.87) 0.27 (0.11–0.52) 0.30 (0.12–0.68) 0.30 (0.11–0.65)GM (95% CI) 0.30 (0.23–0.39) 0.23 (0.18–0.29) 0.29 (0.22–0.39) 0.27 (0.21–0.35)
CI, con!dence interval; IQR, interquartile range.a Paired t test using log-transformed data.
TABLE 3 Multiple Linear Regression Model for Children’s Follow-up Hair Nicotine Concentration
Variable Ratio of GM 95% CI P
GroupControl 1.00 — —
Intervention 0.83 0.61–1.14 .238Child’s age, y 0.94 0.83–1.08 .396Baseline hair nicotine concentration, ng/mg 1.57 1.39–1.77 ,.001Child’s genderMale 1.00 — —
Female 1.04 0.76–1.42 .825
CI, con!dence interval.
ARTICLE
PEDIATRICS Volume 132, Number 6, December 2013 7 at Philippines:AAP Sponsored on December 2, 2013pediatrics.aappublications.orgDownloaded from

This study was a single-blind trial: theparticipants did not knowwhether theywere assigned to the intervention orcontrol group; theywere also blinded tothe study hypothesis and details of theintervention and control group proce-dures, which minimized the possibilityof differential reporting regarding theoutcome variables.34,35
Seasonal variations were shown to affectthe level of indoor SHS exposure in earlierstudies.23 The current study conducted
measurements in late spring and earlyautumn (with similarweather conditions)to adjust for seasonal "uctuations in in-door smoking behavior; therefore, wehad to limit the follow-up period to 4months. However, this limited time in-terval does not allow for evaluation oflonger-term effects of the intervention.
This intervention was not designed toachieve smoking cessation; however,a few smokers did quit. Several studieshaveshownthatstrategieswhich target
SHS reduction may indirectly lead tosmoking cessation.10,23,28,36 The meta-analysis of published controlled trialsfound that interventions targeting chil-dren had tangible potential for modi!-cation of parental behavior, includingparental smoking cessation rate.37
The!ndings of this study emphasize theimportance of motivational interview-ing and providing immediate person-alized feedback for addictive behaviorchange. They could be relevant not onlyfor Armenia but other countries, par-ticularly former Soviet Republics withsimilar rates of smoking and high ex-posure to SHS, and for other countrieswith large disparities in male/femalesmoking rates. This intervention canbe tested in other settings. In Armenia,pediatricians and pediatric nursesare required to make 2 home visits tonewborns. Moreover, monthly well-check visits to primary health careclinics are covered by the state forinfants aged ,1 year. Such a system
TABLE 4 Smoking Restrictions Before and After the Intervention
Respondent Group Follow-up Baseline, n (%) ORa (95% CI)
Any Restriction No Restriction
Mother Intervention Any restriction 45 (36.0) 28 (22.4) 4.67 (1.89–13.78)No restriction 6 (4.8) 46 (36.8)
Control Any restriction 55 (44.4) 22 (17.7) 3.14 (1.30–8.71)No restriction 7 (5.6) 40 (32.3)
Smoker Intervention Any restriction 61 (50.8) 21 (17.8) 2.62 (1.12–6.85)No restriction 8 (6.8) 28 (23.7)
Control Any restriction 59 (53.2) 18 (16.2) 2.25 (0.93–5.98)No restriction 8 (7.2) 26 (23.4)
CI, con!dence interval.a McNemar’s test for matched pairs.
TABLE 5 Children’s Exposure to SHS Before and After the Intervention
Respondent Group Follow-up Baseline, n (%) ORa (95% CI)
Less Than Daily Daily
Mother Intervention Less than daily 4 (3.2) 25 (20.0) 51 (3.08–860.92)b
Daily 0 (0) 96 (76.8)Control Less than daily 4 (3.2) 15 (12.2) 31 (1.83–519.26)b
Daily 0 (0) 104 (84.6)Smoker Intervention Less than daily 6 (5.1) 17 (14.5) 8.50 (2.02–75.85)
Daily 2 (1.7) 92 (78.6)Control Less than daily 8 (7.1) 12 (10.7) 6.0 (1.34–55.20)
Daily 2 (1.8) 90 (80.4)
CI, con!dence interval.a McNemar’s test for matched pairs.b Calculated by adding 0.5 to each cell.
TABLE 6 Unadjusted and Adjusted ORs for Comparing Intervention and Control Groups According to Household Smoking Restrictions and Children’sExposure to SHS
Variable Mother Smoker
ORa (95% CI) Adjusted ORb,c (95% CI)a ORa (95% CI) Adjusted ORb,c (95% CI)a
Household smoking restrictionsNo restriction 1.00 (Ref) 1.00 (Ref) 1.00 (Ref) 1.00 (Ref)Any restriction 1.06 (0.58–1.94) 1.10 (0.59–2.05) 1.13 (0.59–2.16) 1.29 (0.66–2.53)
Children’s exposure SHSDaily 1.00 (Ref) 1.00 (Ref) 1.00 (Ref) 1.00 (Ref)Less than daily 1.73 (0.88–3.42) 1.87 (0.93–3.74) 1.29 (0.61–2.73) 1.54 (0.70–3.39)
CI, con!dence interval.a Univariate logistic regression analysis.b Multiple logistic regression analysis.c Adjusted for child’s age, child’s gender, participant’s baseline knowledge and attitude scores, baseline household smoking restrictions, and children’s exposure to SHS.
8 HARUTYUNYAN et al at Philippines:AAP Sponsored on December 2, 2013pediatrics.aappublications.orgDownloaded from

would allow for developing and testinga pediatric practice-based modi!ca-tion of our model to reduce children’sexposure to SHS at homes.
CONCLUSIONS
This study demonstrated that in-personcounseling, along with provision of im-mediate personalized feedback and
follow-up counseling telephone calls, waseffective indecreasingchildren’spersonalexposure to SHS. In addition, it more ef-fectively educated nonsmoking mothersabout the health hazards of SHS andpromoted smoking restrictions at homethan providing an educational lea"etalone. The superiority of intensiveintervention over the minimal interventionwas not statistically signi!cant; there is
a need for a cost-effectiveness evaluationto justify implementation of the intensiveintervention or to test its effectiveness inother settings.
ACKNOWLEDGMENTSThe authors thank Marie Diener-Westfor her thorough review of the analysisandvaluablecomments; theyalso thankthe participants of the study.
REFERENCES
1. US Department of Health and HumanServices. The Health Consequences of In-voluntary Exposure to Tobacco Smoke: AReport of the Surgeon General. Atlanta, GA:US Department of Health and HumanServices, Centers for Disease Control andPrevention, Coordinating Center for HealthPromotion, National Center for ChronicDisease Prevention and Health Promotion,Of!ce on Smoking and Health; 2006
2. Jenkins RA, Guerin MR, Tompkins BA. Thechemistry of environmental tobacco smoke:composition and measurement. WashingtonDC; Lewis Publishers 2000
3. US Environmental Protection Agency. Re-spiratory Health Effects of Passive Smok-ing: Lung Cancers and Other Disorders.Washington, DC: Of!ce of Research andDevelopment, Of!ce of Health and Environ-mental Assessment; 1992
4. World Health Organization. Tobacco Free Ini-tiative. International Consultation on Envi-ronmental Tobacco Smoke (ETS) andChild Health. Consultation Report. Geneva,Switzerland: World Health Organization; 1999
5. US Department of Health and HumanServices. Children and Secondhand SmokeExposure. Excerpts from The Health Con-sequences of Involuntary Exposure to To-bacco Smoke: A Report of the SurgeonGeneral, Atlanta, GA: U.S. Department ofHealth and Human Services, Centers forDisease Control and Prevention, Co-ordinating Center for Health Promotion,National Center for Chronic Disease Pre-vention and Health Promotion, Of!ce onSmoking and Health, 2007
6. National Statistical Service [Armenia],Ministry of Health [Armenia], and ICF In-ternational. 2012. Armenia Demographicand Health Survey 2010. Calverton, Maryland:National Statistical Service, Ministry of Health,and ICF International
7. Gyurjyan G, Bazarchyan A. Report on theresults of the national survey on the drug,
alcohol and smoking prevalence amongthe general population of Armenia 2005.Available at: www.ichd.org/download.php?f=352&fc=Drug_Survey_eng.pdf. Accessed July2012
8. Movsisyan N, Sahakyan K, Petrosyan V.Household smoking rules in Armenia. In:Abstracts from 14 th World Conference onTobacco or Health (WCTOH), March 2009,Mumbai, India. Indian J Cancer. 2010;47:109–210
9. World Health Organization. Policies to re-duce exposure to environmental tobaccosmoke. Report on a WHO Working GroupMeeting. Lisbon, Portugal; May 29–30, 2000
10. Hovell MF, Meltzer SB, Wahlgren DR, et al.Asthma management and environmentaltobacco smoke exposure reduction inLatino children: a controlled trial. Pediat-rics. 2002;110(5):946–956
11. Marbury MC, Hammond SK, Haley NJ. Mea-suring exposure to environmental tobaccosmoke in studies of acute health effects. AmJ Epidemiol. 1993;137(10):1089–1097
12. Al-Delaimy WK. Hair as a biomarker forexposure to tobacco smoke. Tob Control.2002;11(3):176–182
13. Global Adult Tobacco Survey CollaborativeGroup. Global Adult Tobacco Survey (GATS):Core Questionnaire with Optional Ques-tions, Version 2.0. Atlanta, GA: Centers forDisease Control and Prevention, 2010
14. Curry SJ, Ludman EJ, Graham E, Stout J,Grothaus L, Lozano P. Pediatric-based smokingcessation intervention for low-income women:a randomized trial. Arch Pediatr Adolesc Med.2003;157(3):295–302
15. Emmons KM, Hammond SK, Fava JL, VelicerWF, Evans JL, Monroe AD. A randomized trialto reduce passive smoke exposure in low-income households with young children.Pediatrics. 2001;108(1):18–24
16. Rubak S, Sandbaek A, Lauritzen T, ChristensenB. Motivational interviewing: a systematic
review and meta-analysis. Br J Gen Pract.2005;55(513):305–312
17. US Environmental Protection Agency. Sec-ondhand tobacco smoke and the health ofyour family. Available at: http://wwwepa-gov/smokefree/pdfs/trifold_brochurepdf.Accessed July 1, 2012
18. Model AM510 SIDEPAKTM Personal AerosolMonitor. User guide. Available at: http://tobaccofreeair.org/downloads/1980456b%20SidePak%20manual.pdf. Accessed July1, 2012
19. DiClemente CC, Marinilli AS, Singh M,Bellino LE. The role of feedback in theprocess of health behavior change. Am JHealth Behav. 2001;25(3):217–227
20. Wip"i H, Avila-Tang E, Navas-Acien A, et al;Famri Homes Study Investigators. Second-hand smoke exposure among women andchildren: evidence from 31 countries. Am JPublic Health. 2008;98(4):672–679
21. Fleiss JL. Statistical Methods for Retes andProportions. 2nd ed. John Wiley; New York;1981
22. Heritier SR, Gebski VJ, Keech AC. Inclusionof patients in clinical trial analysis: theintention-to-treat principle. Med J Aust.2003;179(8):438–440
23. Gehrman CA, Hovell MF. Protecting childrenfrom environmental tobacco smoke (ETS)exposure: a critical review. Nicotine TobRes. 2003;5(3):289–301
24. Conway TL, Woodruff SI, Edwards CC, HovellMF, Klein J. Intervention to reduce envi-ronmental tobacco smoke exposure in La-tino children: null effects on hairbiomarkers and parent reports. Tob Con-trol. 2004;13(1):90–92
25. Klerman L. Protecting children: reducingtheir environmental tobacco smoke expo-sure. Nicotine Tob Res. 2004;6(suppl 2):S239–S253
26. Wilson I, Semple S, Mills LM, et al. REFRESH—reducing families’ exposure to secondhand
ARTICLE
PEDIATRICS Volume 132, Number 6, December 2013 9 at Philippines:AAP Sponsored on December 2, 2013pediatrics.aappublications.orgDownloaded from

smoke in the home: a feasibility study. TobControl. 2013;22(5):e8
27. Greenberg RA, Strecher VJ, Bauman KE,et al. Evaluation of a home-based in-tervention program to reduce infant pas-sive smoking and lower respiratory illness.J Behav Med. 1994;17(3):273–290
28. Hovell MF, Meltzer SB, Zakarian JM, et al.Reduction of environmental tobacco smokeexposure among asthmatic children: a con-trolled trial. Chest. 1994;106(2):440–446
29. Hovell MF, Zakarian JM, Matt GE, HofstetterCR, Bernert JT, Pirkle J. Effect of counsel-ling mothers on their children’s exposureto environmental tobacco smoke: rando-mised controlled trial. BMJ. 2000;321(7257):337–342
30. Wahlgren DR, Hovell MF, Meltzer SB,Hofstetter CR, Zakarian JM. Reduction of
environmental tobacco smoke exposurein asthmatic children. A 2-year follow-up.Chest. 1997;111(1):81–88
31. Chiu HT, Isaac Wu HD, Kuo HW. The re-lationship between self-reported tobaccoexposure and cotinines in urine and bloodfor pregnant women. Sci Total Environ.2008;406(1–2):331–336
32. Matt GE, Wahlgren DR, Hovell MF, et al.Measuring environmental tobacco smokeexposure in infants and young childrenthrough urine cotinine and memory-basedparental reports: empirical !ndings anddiscussion. Tob Control. 1999;8(3):282–289
33. Adams J, Parkinson L, Sanson-Fisher RW,Walsh RA. Enhancing self-report of adoles-cent smoking: the effects of bogus pipelineand anonymity. Addict Behav. 2008;33(10):1291–1296
34. Schulz KF, Grimes DA. Blinding in rando-mised trials: hiding who got what. Lancet.2002;359(9307):696–700
35. Friedberg JP, Lipsitz SR, Natarajan S. Chal-lenges and recommendations for blindingin behavioral interventions illustrated us-ing a case study of a behavioral in-tervention to lower blood pressure. PatientEduc Couns. 2010;78(1):5–11
36. McIntosh NA, Clark NM, Howatt WF. Re-ducing tobacco smoke in the environmentof the child with asthma: a cotinine-assisted, minimal-contact intervention. JAsthma. 1994;31(6):453–462
37. Rosen LJ, Noach MB, Winickoff JP, Hovell MF.Parental smoking cessation to protectyoung children: a systematic review andmeta-analysis. Pediatrics. 2012;129(1):141–152
10 HARUTYUNYAN et al at Philippines:AAP Sponsored on December 2, 2013pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2012-2351; originally published online November 4, 2013;Pediatrics
Frances StillmanArusyak Harutyunyan, Narine Movsisyan, Varduhi Petrosyan, Diana Petrosyan and
TrialReducing Children's Exposure to Secondhand Smoke at Home: A Randomized
ServicesUpdated Information &
/peds.2012-2351http://pediatrics.aappublications.org/content/early/2013/10/30including high resolution figures, can be found at:
Supplementary Material
0/peds.2012-2351.DCSupplemental.htmlhttp://pediatrics.aappublications.org/content/suppl/2013/10/3Supplementary material can be found at:
Rs)3Peer Reviews (PPost-Publication
51v1
http://pediatrics.aappublications.org/cgi/eletters/peds.2012-23R has been posted to this article: 3One P
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Philippines:AAP Sponsored on December 2, 2013pediatrics.aappublications.orgDownloaded from