Pediatric Upper Airway Emergencies

of 30
-
Upload
irma-amalia -
Category
Documents
-
view
234 -
download
0
Transcript of Pediatric Upper Airway Emergencies
-
8/9/2019 Pediatric Upper Airway Emergencies
1/30
Pediatric Upper Airway
Emergencies
Sangeeta Schroeder, MD
Resident Noon Conference
-
8/9/2019 Pediatric Upper Airway Emergencies
2/30
Infectious
Croup
Bacterial Tracheitis
Epiglottitis
Other Infectious
Infectious Mono
Neck Abscess
Retropharyngeal
Paratonsillar
2Pediatric Upper Airway Emergencies
Usual Suspects
-
8/9/2019 Pediatric Upper Airway Emergencies
3/30
-
8/9/2019 Pediatric Upper Airway Emergencies
4/30
Extrathoracic/SupraglotticLacks cartilaginous
support
Composed mostly of
soft tissue and muscle
Glottic/SubglotticSmallest part of the
pediatric airway
Some cartilaginous
support
Intrathoracic
Tracheo-Bronchial Tree
4Pediatric Upper Airway Emergencies
-
8/9/2019 Pediatric Upper Airway Emergencies
5/30
Epiglottitis
Laryngomalacia
Croup
Subglottic Stenosis
Subglottic HemangiomaLaryngeal Webs
Bacterial Tracheitis
Tracheomalacia
Vascular Rings/Slings
Bronchomalacia
5Pediatric Upper Airway Emergencies
-
8/9/2019 Pediatric Upper Airway Emergencies
6/30
History
Fever
High fevers with sudden onset: bacterial infections
URI symptoms
Acute onset of symptoms
Acute worsening of insidious symptoms
Incomplete Hib immunization: Epiglottitis
Associated Varicella infection: Epiglottitis
Pediatric Upper Airway Emergencies 6
Clinical Presentation:
Infectious
-
8/9/2019 Pediatric Upper Airway Emergencies
7/30
Exam
Anxious appearing child; tripod positioning:
epigottitis, bacterial tracheitis
Gurgling sounds without stridor: epiglottitis
Severe respiratory distress: bacterial tracheitis,
severe croup
Nasal congestion: croup
Pediatric Upper Airway Emergencies 7
Clinical Presentation
-
8/9/2019 Pediatric Upper Airway Emergencies
8/30
Epiglottitis
Acute process of edema andinflammation
Two age groups:
-
8/9/2019 Pediatric Upper Airway Emergencies
9/30
Inflammation and mucous production in the subglottis
Parainfluenza (1,2,3), Influenza (A,B), RSV, Adenovirus
Mild nasal congestion that progresses to a barking
cough and/or stridor Categorized into Mild, Moderate or Severe
Mild: no stridor at rest; can have stridor with activity
Moderate: stridor and retractions at rest
Severe: stridor and severe retractions at rest associatedwith behavioral changes (extreme agitation or lethargy)
Laryngotracheitis (Croup)
9Pediatric Upper Airway Emergencies
-
8/9/2019 Pediatric Upper Airway Emergencies
10/30
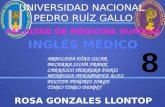
Croup: Steeple Sign on AP view
Epiglottitis: Thumb Sign on Lateral view
NOT WARRANTED
X-Ray only if you suspect a foreign body
Bacterial Tracheitis: Laryngoscopy
Pediatric Upper Airway Emergencies 10
Diagnostics
-
8/9/2019 Pediatric Upper Airway Emergencies
11/30
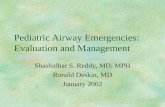
Epiglottitis Bacterial Tracheitis
Pediatric Upper Airway Emergencies 11
Endoscopic Visualization
-
8/9/2019 Pediatric Upper Airway Emergencies
12/30
Humidified Air and Cool Mist are not effective treatments
0.6mg/kg Decadron PO/IM for ALL croup Do not need to repeat dose
Racemic epi nebs for moderate and severe croup
If there is stridor at rest: use racemic epi Continuous to Q4 PRN
Observe for 2-3 hrs after treatment for epi to wear off
Rebound Effect: likely not real
Admission Criteria: 2 or more racemic epi treatments
Poor PO intake or inadequate follow-up
Admit to PICU if on continuous racemic nebs
Pediatric Upper Airway Emergencies 12
Treatment: Croup
-
8/9/2019 Pediatric Upper Airway Emergencies
13/30
Airway Management
Bronchoscopy to suction purulent and necrotic
debris
Continued suctioning while intubated
IV Antibiotics
Vancomycin + 3rd Generation Cephalosporin
PICU admission
Pediatric Upper Airway Emergencies 13
Treatment:
Bacterial Tracheitis
-
8/9/2019 Pediatric Upper Airway Emergencies
14/30
Do all kids with epiglottitis need intubation? Prospective study done in Germany in 1996
International Journal of Pediatric Otorhinolaryngology
Fiberoptic visualization of airway Assess degree of inflammation and airway involvement
Kids managed without intubation increased from 8% to 45% Mean age of child intubated: 3.4
Mean age of child not intubated: 6.1
Regardless, current practice is to still intubate all kids with
epiglottitis in a controlled environment IV Antibiotics and PICU Admission
Vancomycin + 3rd Generation Cephalosporin
Pediatric Upper Airway Emergencies 14
Treatment: Epiglottitis
-
8/9/2019 Pediatric Upper Airway Emergencies
15/30
History Overview
Insidious and/or intermittent symptoms
Past history of prolonged intubation or severe GERD:
subglottic stenosis Trisomy 21: congenital subglottic stenosis
DiGeorge Syndrome: laryngeal webs
Congenital Cardiac Lesions: laryngeal webs, vascular
rings Underlying neuromuscular disorder/hypotonia:
tracheo/bronchomalacia
Pediatric Upper Airway Emergencies 15
Clinical Presentation:
Anatomic/Congenital
-
8/9/2019 Pediatric Upper Airway Emergencies
16/30
Pediatric Upper Airway Emergencies 16
Exam Overview
Hypotonia: Malacia
Skin Hemangiomas: Subglottic hemangioma Biphasic Stridor: Subglottic hemangioma
Surgical Scars: Subglottic stenosis
Abnormal Facies: Laryngeal webs
Caf au lait spots: Neurofibromas of the airway
Clinical Presentation
-
8/9/2019 Pediatric Upper Airway Emergencies
17/30
Laryngomalacia
Intermittent episodes of stridor without fever
Usually Mild without evidence of respiratory
distress Worsens with activity/URIs
Worse in the supine position
Most self-resolve by 1 year
Male predilection
Associated GERD (more severe)
Pediatric Upper Airway Emergencies 17
Congenital Causes Clinical
Presentations
-
8/9/2019 Pediatric Upper Airway Emergencies
18/30
-
8/9/2019 Pediatric Upper Airway Emergencies
19/30
Tracheo/Bronchomalacia
Symptoms are more persistent and severe than
laryngomalacia
Significant distress with mild URIs and basic
activities (coughing/feeding/stooling)
Underlying hypotonia
Pediatric Upper Airway Emergencies 19
Congenital Causes Clinical
Presentations
-
8/9/2019 Pediatric Upper Airway Emergencies
20/30
Congenital Causes:
Subglottic Stenosis
Acquired V congenital If no hx of intubation, considered to be congenital
Males >> Females
Two forms Mucosal: Submucosal hypertrophy (more common)
Cartilaginous: Narrow cricoid cartilage (more severe)
Usually presents with biphasic stridor during
URIs Recurrent Croup
Acquired is usually more severe
Pediatric Upper Airway Emergencies 20
-
8/9/2019 Pediatric Upper Airway Emergencies
21/30
Congenital Causes:
Subglottic Hemangioma
Females >> Males
Insidious presentation of biphasic stridor without fever
Recurrent Croup
Rapidly enlarges from 2 months to 1 year of age
Resolve by 2-5 yrs of life
Most need surgical management prior to 2 years
50% will have a face/neck hemangioma
Enlarging hemangioma: sudden upper airway
obstruction and distress
Pediatric Upper Airway Emergencies 21
-
8/9/2019 Pediatric Upper Airway Emergencies
22/30
Congenital Causes:
Laryngeal Webs
Weak cry, horseness
Varying degress of resp distress
Type 1 (75% webbing)
Caused by failure of normal embryonic tissueregression
Type 4 usually diagnosed at birth with respiratoryfailure
1/3 associated with other anomalies of the airway Subglottic stenosis (most common)
Recurrent croup
Pediatric Upper Airway Emergencies 22
-
8/9/2019 Pediatric Upper Airway Emergencies
23/30
Congenital Causes:
Vascular Rings/Slings
Tracheo-esophageal compression
Caused by the abnormal persistence of embryonictissue that comprises the aortic arch
Double aortic arch (50-60%)
Right aortic arch with an aberrant left subclavian (12-25%)
Pulmonary artery sling
Wheezing (from the ring/sling) and stridor (from
ass. GERD) Often diagnosed as recurrent bronchiolitis
Can present with sudden apneic and cyanotic spells
Pediatric Upper Airway Emergencies 23
-
8/9/2019 Pediatric Upper Airway Emergencies
24/30
Laryngomalacia: Usually not warranted
Tracheo/bronchomalacia: Bronchoscopy
Subglottic Stenosis: Rigid Bronchoscopy
Subglottic Hemangioma: MRI Airway endoscopy to rule out other causes
Laryngeal Webs: Laryngoscopy, Lateral neck films
Sail sign: persistent tissue from the glottis to thesubglottis
Vascular Rings: Barium Swallow, MRI
Pediatric Upper Airway Emergencies 24
Diagnostics
-
8/9/2019 Pediatric Upper Airway Emergencies
25/30
Laryngomalacia Self-resolves by 1 year as the larynx travels into the
neck
Treat concurrent GERD
Surgical correction is rare: Supraglottoplasty
Tracheomalacia/Bronchomalacia Self resolve by 1-2 years
If pt has underlying hypotonia, can be persistent
Treatment focused on concurrent infections Often will need Positive Pressure ventilation until the
airways grow in size (CPAP, BiPAP)
Pediatric Upper Airway Emergencies 25
Treatment: Malacia
-
8/9/2019 Pediatric Upper Airway Emergencies
26/30
Subglottic Stenosis
More than self resolve by
2 years of age
Surgical Interventions: Stenting
Tracheostomy
Usually can de-cannulate by
3-4 yrs of age
Reconstruction(Laryngotracheoplasty)
Reserved for severe cases
Subglottic Hemangioma
Regress completely by 5
years of age
Most require intervention Small/Medium hemangiomas:
Steroid Injections, Endoscopic
Laser Ablation
If a circumferential area is
ablated at one treatment:subglottic stenosis
Large hemangiomas:
resection, tracheostomy
Pediatric Upper Airway Emergencies 26
Treatment
-
8/9/2019 Pediatric Upper Airway Emergencies
27/30
Laryngeal Webs
Child is observed until they are 3-4 yrs of age if able
Types I-II: knife or laser ablation
Types III-IV: early larygo-tracheal reconstruction
Complicated webs may require revision surgeries
Vascular Rings
Corrected early Decrease the risk of malacia
Allow for normal growth of the tracheo-bronchial tree
Pediatric Upper Airway Emergencies 27
Treatment:
Webs and Rings
-
8/9/2019 Pediatric Upper Airway Emergencies
28/30
Dexamethasone 0.6mg/kg IM or PO has become the mainstay
of treatment for croup, regardless of severity.
Bacterial Tracheitis is now the most common infectious cause
of pediatric upper respiratory emergencies, with the most
common bacterial agents being Staphylococcus aureus and
Streptococcus pyogenes.
Epiglottitis is no longer a disease of infants. Since
Haemophilus type B immunization, the most common causes
of epiglottitis are Streptococcus pneumonia and group Astrep. With this change in bacterial etiology, the average age
of children with epiglottitis is now 6-7 years.
Pediatric Upper Airway Emergencies 28
Key Points
-
8/9/2019 Pediatric Upper Airway Emergencies
29/30
-
8/9/2019 Pediatric Upper Airway Emergencies
30/30
1Hopkins A, Lahiri T, Salerno R, Heath B. Changing epidemiology of life-threatening upper
airway infections: the reemergence of bacterial tracheitis. Pediatrics 2006; 118:1418-1421
2Hartnick CJ, Cotton RT. Congenital laryngeal anomalies. Laryngeal atresia, stenosis, webs and
clefts. Otolaryngol Clin North Am 2000; 33(6):1293-1308
3Kussman BD, Geva R, McGowan F. Cardiovascular causes of airway compression. Pediatric
Anaesthesia 2004; 14:60-74
4Leung A, Cho J. Diagnosis of stridor in children.American Family Physician 1999; 60 (8)
5Long S, Pickering L, Prober C. Upper respiratory tract and oral infections. In: Principles andPractice of Pediatric Infectious Diseases, 2nded. 2003; Ch 26, 31.
6Grattan-Smith T, Forer M, Kilham H, Gillis J. Viral supraglottitis.J Pediatrics 1987; 110:434
7Bjornson C, Johnson D. Croup. The Lancet2008; 317:329-339
8Damm M, Eckel HE, Jungehulsing M, Roth B. Airway endoscopy in the interdisciplinary
management of acute epiglottitis. Int J Pediatric Otorhinolaryngology1996; 38:41-51
9Scolnik D, Coates A, Stephens D et al. Controlled delivery of high vs. low humidity vs. mist
therapy for croup in emergency departments: a randomized controlled trial.JAMA 2006;
295:1274-1280
10Cruz M, Stewart G, Rosenberg N. Use of dexamethasone in the outpatient management of
acute laryngotracheitis. Pediatrics 1995; 96:220-223
11Bjornson C, Klassen T, Williamson J et al. A randomized trial of single dose of oral
dexamethasone for mild croup. New England Journal of Medicine 2004; 351:1306-1313Pediatric Upper Airway Emergencies 30
References