
Pediatric Tracheotomy: An Update Shraddha Mukerji, MD University of Texas Medical Branch Department...
36
Pediatric Pediatric Tracheotomy: An Tracheotomy: An Update Update Shraddha Mukerji, MD Shraddha Mukerji, MD University of Texas Medical University of Texas Medical Branch Branch Department of Otolaryngology Department of Otolaryngology Didactics Didactics September 24, 2009 September 24, 2009
-
Upload
edward-pearson -
Category
Documents
-
view
214 -
download
0
Transcript of Pediatric Tracheotomy: An Update Shraddha Mukerji, MD University of Texas Medical Branch Department...

Pediatric Tracheotomy: Pediatric Tracheotomy: An UpdateAn Update
Shraddha Mukerji, MDShraddha Mukerji, MDUniversity of Texas Medical BranchUniversity of Texas Medical Branch
Department of OtolaryngologyDepartment of OtolaryngologyDidactics Didactics
September 24, 2009September 24, 2009
OverviewOverview
HistoryHistory Changing IndicationsChanging Indications Surgical ConsiderationsSurgical Considerations ComplicationsComplications Long term effects of trach in children Long term effects of trach in children DecannulationDecannulation
History of tracheotomyHistory of tracheotomy
Period of legend 1500BC-1500AD Homer, Galen
Period of fear 460BC-1500AD Hippocrates
Period of drama 1500-1900 First modern tracheotomy, Pediatric tracheotomy for foreign body, tracheotomy for diphtheria
Period of rationalization 1900- Jackson: better instruments, post-operative care, safer anesthetics
PioneersPioneers
Antonio M. Brasavola
First successful tracheotomy
Chevalier Jackson
Good postoperative care
Pierre Bretonneau
Tracheotomy for diphtheria
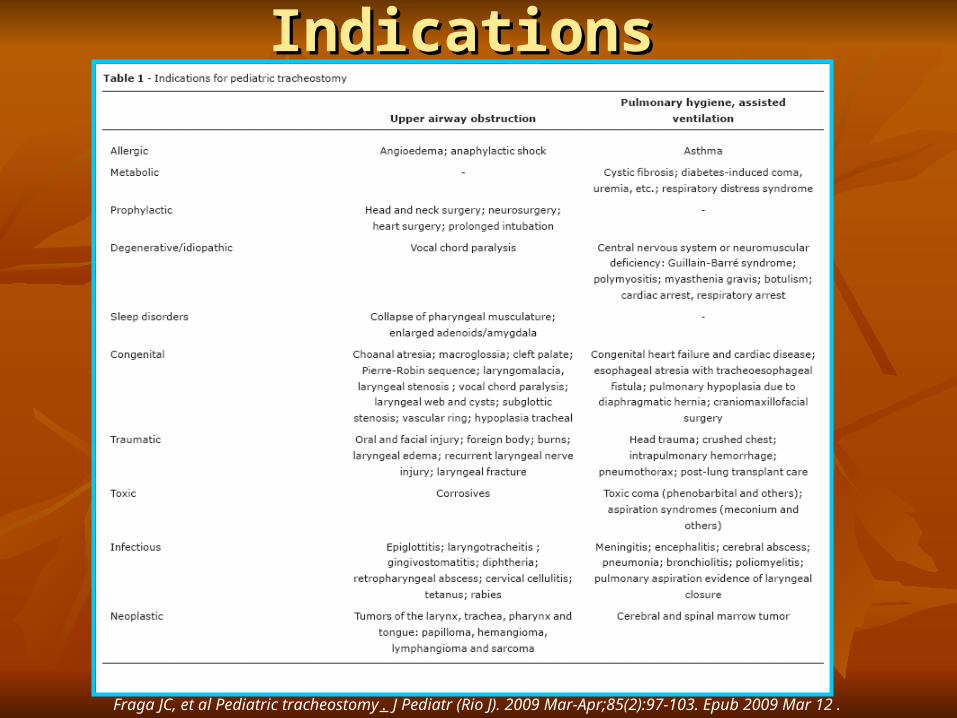
Indications Indications
Fraga JC, et al Pediatric tracheostomy. J Pediatr (Rio J). 2009 Mar-Apr;85(2):97-103. Epub 2009 Mar 12.

How have they changed?How have they changed?
1980
Inflammatory diseases of the upper airway
50% - 3%
Prematurity, prolonged intubation
28% - 58%
Congenital anomalies
6% - 23%
Arcand and Granger, J Otol 1988, Line et al Laryngoscope 1986, Fraga et al, J Pediatr 2009
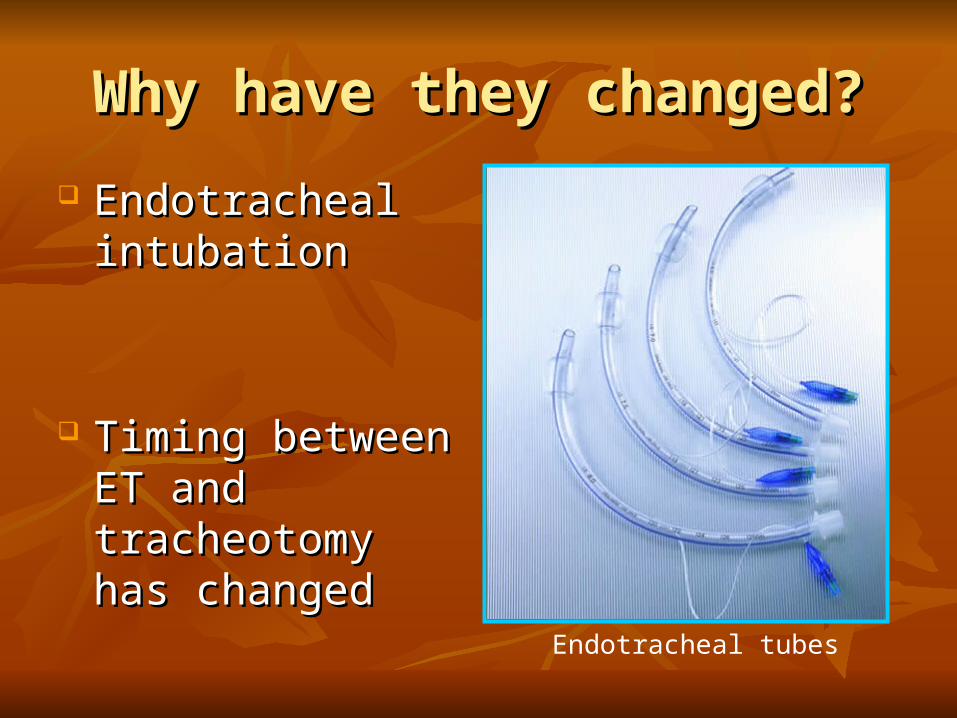
Why have they changed?Why have they changed?
Endotracheal Endotracheal intubationintubation
Timing between ET Timing between ET and tracheotomy has and tracheotomy has changedchanged
Endotracheal tubes

Most common indicationsMost common indications Prematurity, chronic ventilatory supportPrematurity, chronic ventilatory support
Craniofacial anomalies: Pierre Robin, Craniofacial anomalies: Pierre Robin, CHARGECHARGE
Congenital anomalies: Subglottic stenosisCongenital anomalies: Subglottic stenosis
Tracheotomy for tracheobronchial hygieneTracheotomy for tracheobronchial hygiene
Carron JD, et al Pediatric tracheotomies: changing indications and outcomes. Laryngoscope. 2000 Jul;110(7):1099-10
Fraga JC, et al Pediatric tracheostomy. J Pediatr (Rio J). 2009 Mar-
Apr;85(2):97-103. Epub 2009 Mar 12.

Tracheotomy tubesTracheotomy tubes
Shiley tracheostomy tubes
Bivona tracheostomy tubes
Metal tracheostomy tubes
Pre-op Parental counselingPre-op Parental counseling
Multidisciplinary meetingMultidisciplinary meeting Reassurance about voice issues, swallowing Reassurance about voice issues, swallowing
and feedingand feeding Educational material/videos/meeting other Educational material/videos/meeting other
parents of children with tracheotomyparents of children with tracheotomy How soon can we go home?How soon can we go home?

Surgical stepsSurgical steps
Patient positionPatient position
Landmarks: hyoid and cricoid, thyroid Landmarks: hyoid and cricoid, thyroid obscuredobscured

Anatomical differences between Anatomical differences between pediatric and adult larynxpediatric and adult larynx

Surgical steps contd…Surgical steps contd…
IncisionIncision
Removal of Removal of subcutaneous fatsubcutaneous fat
Exposure of the thyroid Exposure of the thyroid isthmusisthmus

Surgical steps contd…Surgical steps contd…
Always divide the thyroid isthmusAlways divide the thyroid isthmus Palpate cricoid and identify tracheal rings, Palpate cricoid and identify tracheal rings,
usually skin hook is used to hitch up the usually skin hook is used to hitch up the cricoidcricoid
Stay SuturesStay Sutures
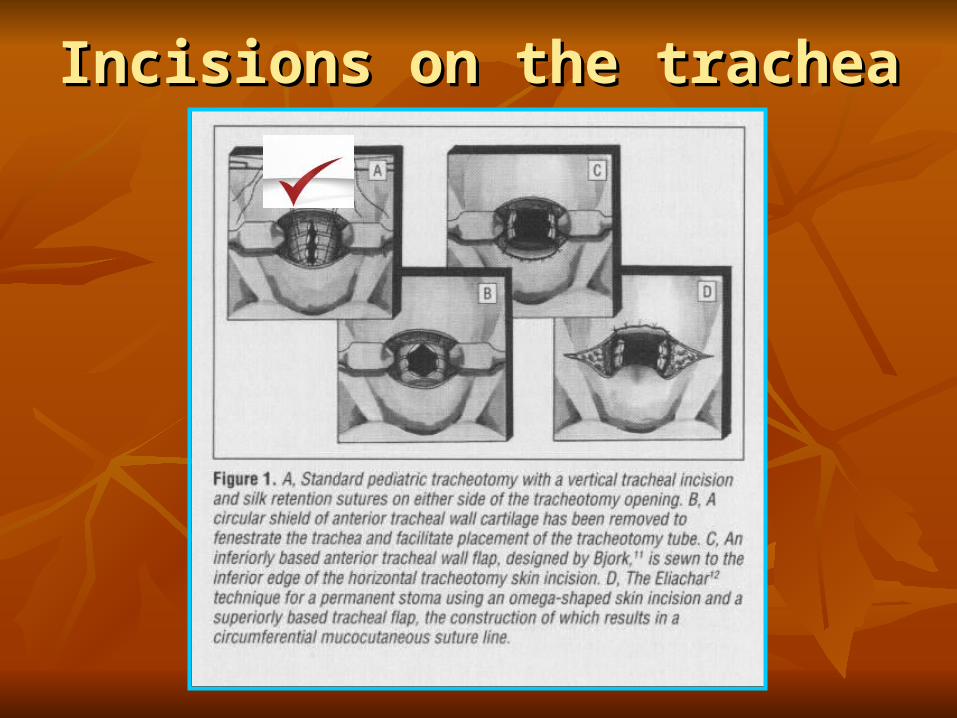
Incisions on the tracheaIncisions on the trachea
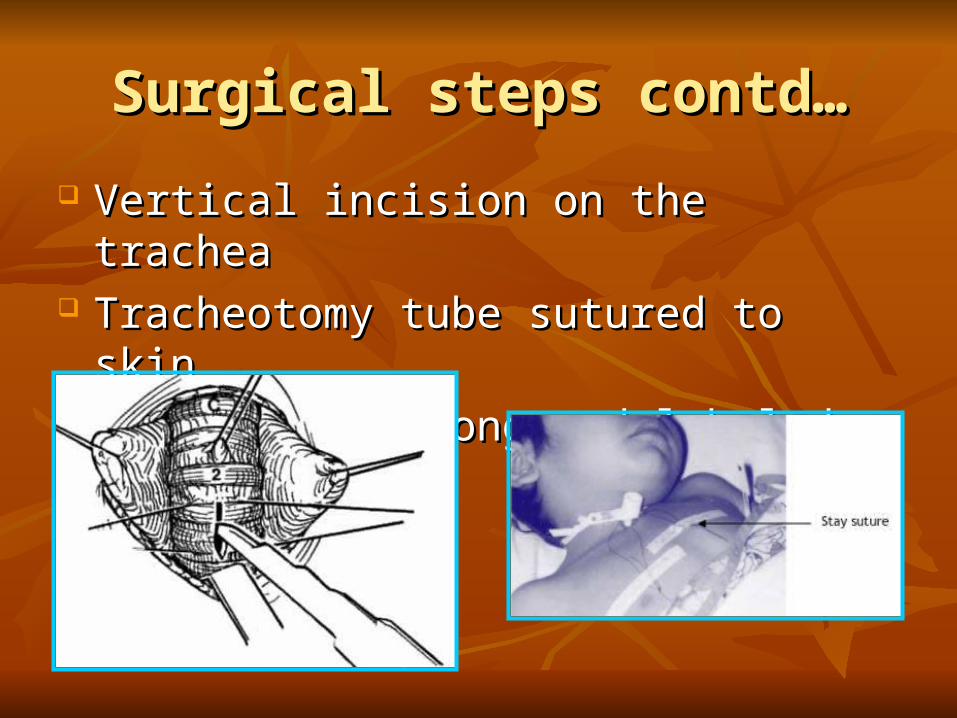
Surgical steps contd…Surgical steps contd…
Vertical incision on the tracheaVertical incision on the trachea Tracheotomy tube sutured to skinTracheotomy tube sutured to skin Stay sutures long and labeled left and rightStay sutures long and labeled left and right
Post-op carePost-op care
Chest XrayChest Xray ICU stay till first trach change, then ICU stay till first trach change, then
intermediate levelintermediate level Sedated and paralyzed for 48 hoursSedated and paralyzed for 48 hours Suture tray at bedsideSuture tray at bedside Tracheotomy tube Tracheotomy tube ≤≤ Endotracheal tube ≤Endotracheal tube ≤ Trach change on day 5 (2 persons)Trach change on day 5 (2 persons)

ComplicationsComplications
Children: Adults---2,3:1Children: Adults---2,3:1-Premature>>Term-Premature>>Term
Complications are reduced if operation is Complications are reduced if operation is carried out by trained physicians in a tertiary carried out by trained physicians in a tertiary care settingcare setting
Mortality related directly to tracheotomy Mortality related directly to tracheotomy varies between 0-6%varies between 0-6%
Pereira et al. Complications of neonatal tracheostomy: a 5 year review. Otolaryngol Head Neck Surg.2004;131:810-13

Complications cont’d…Complications cont’d…
Early (5-49%)Early (5-49%) BleedingBleeding PneumomediastinumPneumomediastinum Subcut emphysemaSubcut emphysema Accidental decannulationAccidental decannulation Wound breakdownWound breakdown
Late (24-100%)Late (24-100%) Granuloma formationGranuloma formation TracheomalaciaTracheomalacia Tracheal stenosisTracheal stenosis Tracheoesophageal Tracheoesophageal
fistulafistula

Pneumomediastinum/PneumothoraxPneumomediastinum/Pneumothorax
One of the commonest One of the commonest early Cxearly Cx
28% of premature 28% of premature babies affectedbabies affected
Damage to Damage to pleura,forceful pleura,forceful coughing coughing
Subcutaneous emphysemaSubcutaneous emphysema
Increase ventilatory Increase ventilatory pressurespressures
Overzealous ventilationOverzealous ventilation
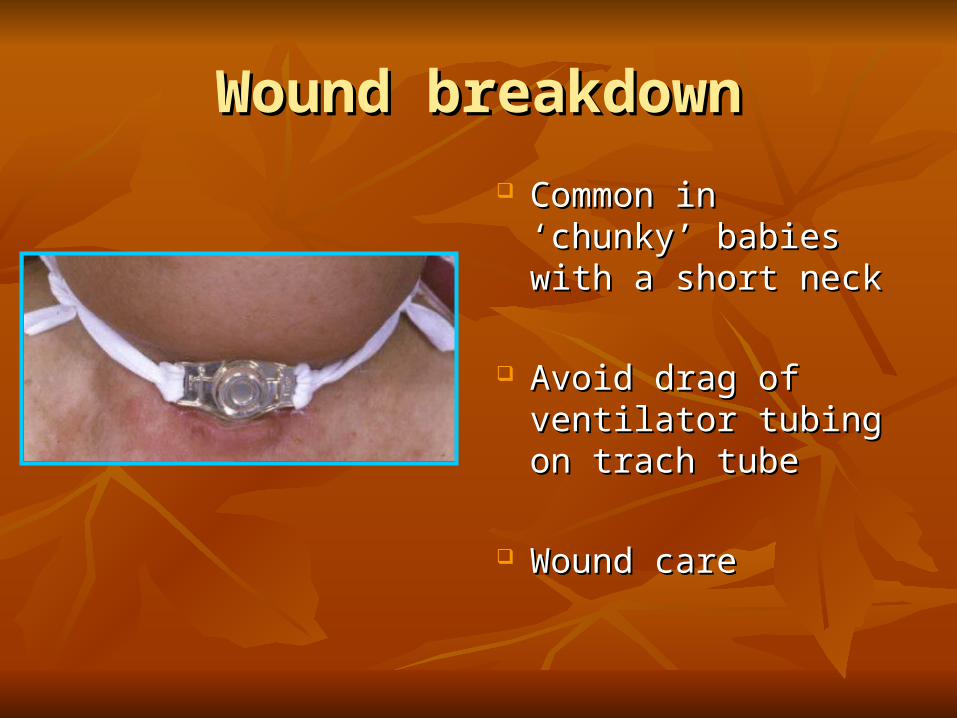
Wound breakdownWound breakdown
Common in ‘chunky’ Common in ‘chunky’ babies with a short neckbabies with a short neck
Avoid drag of ventilator Avoid drag of ventilator tubing on trach tubetubing on trach tube
Wound careWound care
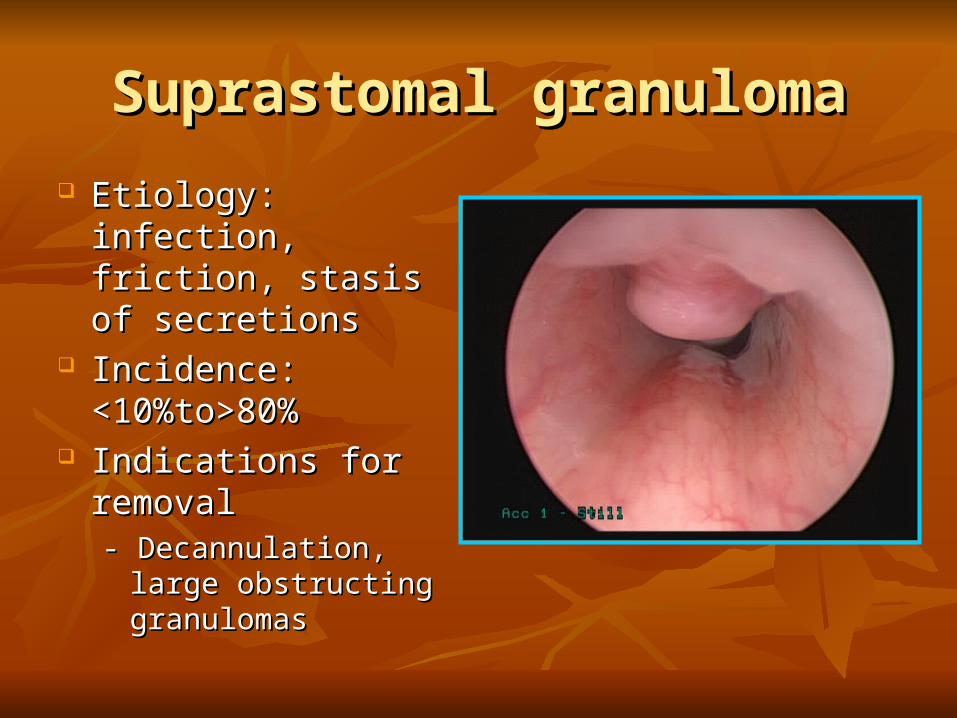
Suprastomal granulomaSuprastomal granuloma
Etiology: infection, Etiology: infection, friction, stasis of friction, stasis of secretionssecretions
Incidence: Incidence: <10%to>80%<10%to>80%
Indications for removalIndications for removal- Decannulation, large - Decannulation, large
obstructing granulomasobstructing granulomas

Suprastomal/Tracheal granulomaSuprastomal/Tracheal granuloma
Complications cont’d…Complications cont’d…
TracheitisTracheitis Usually colonization, viral infectionUsually colonization, viral infection Determine: change in color of secretions, O2 Determine: change in color of secretions, O2
saturations, vent settingssaturations, vent settings Tracheoscopy to differentiate colonization from Tracheoscopy to differentiate colonization from
true bacterial tracheitistrue bacterial tracheitis Gram stain and parenteral antimicrobialsGram stain and parenteral antimicrobials
PneumoniaPneumonia

Accidental decannulationAccidental decannulation
Commonest cause of tracheotomy related Commonest cause of tracheotomy related deathdeath
Premature babies: 7% and older children 16%Premature babies: 7% and older children 16%
Vigilant post-operative monitoringVigilant post-operative monitoring
Long Term Effects of Tracheotomy Long Term Effects of Tracheotomy in Childrenin Children
Study by Freeland et al – Delayed physical Study by Freeland et al – Delayed physical development and increase likelihood of development and increase likelihood of complications if tracheostomy > 1 weekcomplications if tracheostomy > 1 week
Hill and Singer – delayed speech acquisition Hill and Singer – delayed speech acquisition and delayed communicationand delayed communication
Freeland AP Developmental influences of infant tracheostomy. J Laryngol Otol. 1974 Oct;88(10):927-36
Hill BP, Singer LT Speech and language development after infant tracheostomy. J Speech Hear Disord. 1990 Feb;55(1):15-20
Care of the tracheotomyCare of the tracheotomy
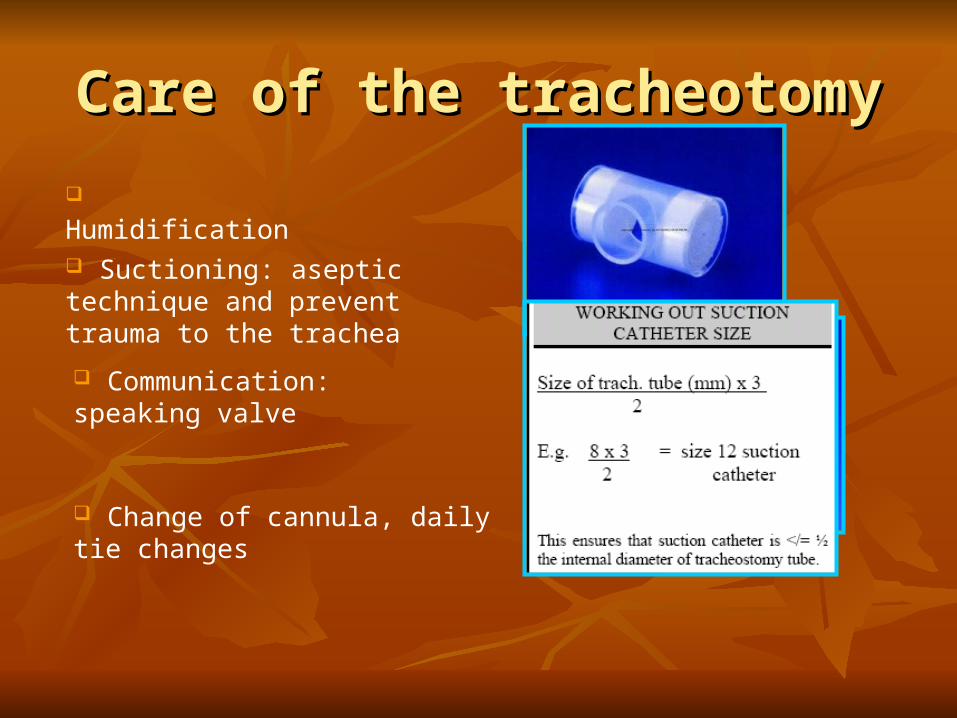
Humidification
Suctioning: aseptic technique and prevent trauma to the trachea
Communication: speaking valve
Change of cannula, daily tie changes
Passy Muir valvePassy Muir valve
Principle ‘No leak’, closed Principle ‘No leak’, closed respiratory system with one respiratory system with one way valveway valve
Various types available for Various types available for different tracheostomy tubesdifferent tracheostomy tubes
Benefits: Speech, better Benefits: Speech, better cough, aids swallow, cough, aids swallow, expedites decannulation expedites decannulation

DecannulationDecannulation
Indication for decannulationIndication for decannulation
Clinical: resolution of the primary disease, no Clinical: resolution of the primary disease, no active infection, tolerance of speaking valveactive infection, tolerance of speaking valve
Endoscopic: a clear tracheobronchial treeEndoscopic: a clear tracheobronchial tree
Functional: Adequate pulmonary reserveFunctional: Adequate pulmonary reserve
Process of decannulationProcess of decannulation
Timing of decannulation-Spring,Summer vs Timing of decannulation-Spring,Summer vs Fall/WinterFall/Winter
Role of capped sleep studyRole of capped sleep study
Observation for 24 hours after decannulation Observation for 24 hours after decannulation in a monitored setttingin a monitored settting

Decannulation contd…Decannulation contd… Rate of decannulation:34%-75%Rate of decannulation:34%-75%
Children with craniofacial anomalies have the highest Children with craniofacial anomalies have the highest decannulation ratedecannulation rate
Neurologically impaired children and children with prolonged Neurologically impaired children and children with prolonged ventilation-lower decannulation rateventilation-lower decannulation rate
Children decannulated < 2years have a lower incidence of Children decannulated < 2years have a lower incidence of TCFTCF
Carron et al. Pediatric Tracheostomies: Changing Indications and Outcomes. Laryngoscope 2000;110 (7):1099-1104
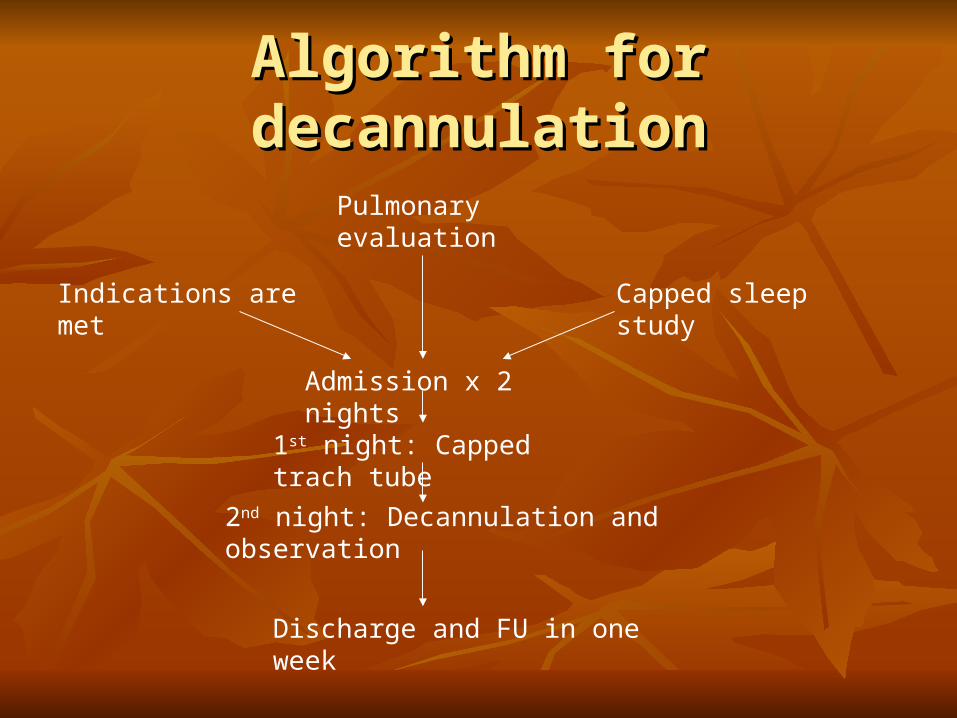
Algorithm for decannulationAlgorithm for decannulation
Indications are met
Pulmonary evaluation
Capped sleep study
Admission x 2 nights
1st night: Capped trach tube
2nd night: Decannulation and observation
Discharge and FU in one week

SummarySummary
Endotracheal intubation has virtually replaced Endotracheal intubation has virtually replaced tracheotomy for inflammatory lesions of the pediatric tracheotomy for inflammatory lesions of the pediatric larynxlarynx
Commonest indications include chronic ventilatory Commonest indications include chronic ventilatory dependency, craniofacial and congenital anomalies of dependency, craniofacial and congenital anomalies of the larynxthe larynx
Removal of subcutaneous fat, vertical tracheal Removal of subcutaneous fat, vertical tracheal incision and stay suturesincision and stay sutures
Summary contd…Summary contd…
Common complications include bleeding, wound Common complications include bleeding, wound infection, pneumomediastinum and granuloma infection, pneumomediastinum and granuloma formationformation
Accidental decannulation remains the most important Accidental decannulation remains the most important cause of tracheotomy related deathcause of tracheotomy related death
Rates of decannulation are the highest in children Rates of decannulation are the highest in children with craniofacial anomalieswith craniofacial anomalies
Christmas in the bronchoscopic clinic ward. Children with tracheostomies usually lived in the hospital. Photo from The Life of Chevalier Jackson, An Autobiography


















