Pediatric News - Global Academy for Medical Education · Pediatric News ® The articles in ......
16
Pediatric News ® A SUPPLEMENT TO Introduction Tor A. Shwayder, MD • Henry Ford Hospital • Detroit Clinical Presentation of Atopic Dermatitis and Its Differential Diagnosis Seth J. Orlow, MD, PhD • New York University School of Medicine The Pathophysiology of Atopic Dermatitis and Standard Therapies Ronald C. Hansen, MD • University of Arizona College of Medicine • Tucson New Therapies for Atopic Dermatitis Moise L. Levy, MD • Baylor College of Medicine • Houston A TOPIC DERMATITIS IN THE PEDIATRIC P ATIENT : P ATHOPHYSIOLOGY , PRESENTATION, AND AN UPDATE ON NOVEL THERAPIES Jointly sponsored by Medical Education Collaborative, a nonprofit education company, and PEDIATRIC NEWS
Transcript of Pediatric News - Global Academy for Medical Education · Pediatric News ® The articles in ......

it.
9.
.
i-
e
til
-
Pediatric News®
A S U P P L E M E N T T O
IntroductionTor A. Shwayder, MD • Henry Ford Hospital • Detroit
Clinical Presentation of Atopic Dermatitis and Its Differential DiagnosisSeth J. Orlow, MD, PhD • New York University School of Medicine
The Pathophysiology of Atopic Dermatitis and Standard TherapiesRonald C. Hansen, MD • University of Arizona College of Medicine • Tucson
New Therapies for Atopic DermatitisMoise L. Levy, MD • Baylor College of Medicine • Houston
ATOPIC DERMATITIS INTHE PEDIATRIC PATIENT:PATHOPHYSIOLOGY, PRESENTATION, AND AN UPDATE ON NOVEL THERAPIES
Jointly sponsored by Medical EducationCollaborative, a nonprofit education company, and PEDIATRIC NEWS
Novartis/PED/Derm2 1/17/03 7:13 PM Page 2

Group Publisher/
General Manager
Alan J. Imhoff
Vice President,
Medical Education
& Business Development
Sylvia H. Reitman
Manager, Medical Education
Jenny R. McMahon
Clinical Editor
Geneva Collins
National Account Manager
Rory Flanagan
Graphic Design
Lehner & Whyte, Inc.
Production Manager
Judi Sheffer
Pediatric News®
The articles in this supplement are
based on presentations made at a
continuing medical education sym-
posium held on October 21, 2002,
in Boston, Mass.
This supplement was supported by
an unrestricted educational
grant from
It was produced by the medical
education and business develop-
ment department of International
Medical News Group. Neither the
Editor of PEDIATRIC NEWS nor the
reporting staff contributed to its
content.
ATOPIC DERMATITIS IN THE PEDIATRIC PAPATHOPHYSIOLOGY, PRESENTATION, AND AN UP
4
4
Copyright 2003 International Medical NewsGroup, an Elsevier Science company. All rightsreserved. No part of this publication may bereproduced or transmitted in any form, by anymeans, without prior written permission of thePublisher. The opinions expressed in thissupplement are those of the presenters and do notnecessarily reflect the views of the supporter or thePublisher. International Medical News Groupwill not assume responsibility for damages, loss, orclaims of any kind arising from or related to theinformation contained in this publication,including any claims related to the products,drugs, or services mentioned herein.
Tor A. Shwayder, MDDirector of Pediatric
Dermatology
Henry Ford Hospital
Detroit
Seth J. Orlow, MD, PhDProfessor of Dermatology,
Cell Biology, and Pediatrics
Director of Pediatric
Dermatology
New York University School
of Medicine
Ronald C. Hansen, MDProfessor of Medicine
(Dermatology) and Pediatrics
Director, Pediatric Dermatology
University of Arizona College
of Medicine
Tucson
Moise L. Levy, MDProfessor of Dermatology
and Pediatrics
Baylor College of Medicine
Chief, Dermatology Service
Texas Children’s Hospital
Houston
Faculty
Introduction
Clinical Presentation of Atopic Dermatitis and Its Differential Diagnosis
7 The Pathophysiology of Atopic Dermatitis and Standard Therapies
11 New Therapies for Atopic Dermatitis
16 CME Post-Test and Evaluation
Novartis/PED/Derm2 1/28/03 12:10 PM Page 3

Target AudienceThis activity has been developed for pediatricians and other
health care professionals involved in the treatment of pediatric
atopic dermatitis.
Educational NeedsAtopic dermatitis has become an increasingly prevalent skin con-
dition in infants and children. Pediatricians need to be able to
accurately diagnose the disease and distinguish it from many
other cutaneous dermatoses common to childhood. They also
need to have access to the most current research into the patho-
physiology and epidemiology of atopic dermatitis in order to bet-
ter understand the nature of this chronically relapsing condition.
Pediatricians need to keep abreast of the latest advances in atopic
dermatitis therapy, which allow safe and effective management of
the underlying disease and symptoms, even in infants and young
children.
AccreditationThis activity has been planned and implemented in accor-
dance with the Essential Areas and Policies of the
Accreditation Council for Continuing Medical Education
(ACCME) through the joint sponsorship of Medical Education
Collaborative (MEC) and PEDIATRIC NEWS. Medical Education
Collaborative, a nonprofit education organization, is accredited
by the ACCME to provide continuing medical education for
physicians.
Medical Education Collaborative designates this educational
activity for a maximum of 2 hours of category 1 credit toward the
AMA Physician’s Recognition Award. Each physician should
claim only those hours of credit that he/she actually spent in the
educational activity.
Release date: February 2003
Expiration date: January 2004
RIC PATIENT:AN UPDATE ON NOVEL THERAPIES
D
s
gy
Faculty DisclosuresFaculty/authors must disclose any significant financial interest or
relationship with proprietary entities that may have a direct
relationship to the subject matter. They must also disclose any
discussion of investigational or unlabeled uses of products.
Dr. Hansen is a consultant to, is on the advisory board of, and
has received honoraria from Novartis Pharmaceuticals
Corporation. Dr. Orlow is a consultant to and has received
honoraria from Novartis. Dr. Levy has received clinical research
support from and is a consultant to Fujisawa Healthcare and
Novartis and he has received honoraria from Fujisawa, Galderma
Laboratories, L.P. and Novartis. He discusses the unlabeled use of
pimecrolimus in children under the age of 2. Dr. Shwayder has
nothing to disclose.
Learning ObjectivesBy reading and studying this supplement, participants should be
able to:
• Identify the major diagnostic criteria for atopic dermatitis
and describe the age-determined patterns seen in infants and
children.
• Distinguish atopic dermatitis from other cutaneous diseases
common to the pediatric patient who presents with erythe-
ma, papulation, and/or scale.
• Describe the pathophysiology of atopic dermatitis and list
immunoregulatory abnormalities commonly associated with
the condition.
• Name the most common exacerbants and triggers of atopic
dermatitis.
• Summarize conventional treatment options, their benefits,
and their limitations.
• Describe the mechanism of action of steroid-free topical
immunomodulators.
• Summarize the findings of clinical trials that have examined
the efficacy and safety of the new steroid-free agents.
Novartis/PED/Derm2 1/28/03 12:10 PM Page 4

4 Atopic Dermatitis in the Pediatric Patient
o definitive laboratory tests currently exist to diagnose
atopic dermatitis, nor are the lesions themselves pathog-
nomonic. Diagnosis of atopic dermatitis is based solely
on clinical criteria, which include factors such as lesion
appearance, distribution, and duration; history of the illness;
symptoms; and family medical history.
Atopic dermatitis is distinguished by erythema, papulation,
excoriation, and lichenification. Pruritus is the first symptom,
followed by erythema and papulation. External factors such as
scratching, rubbing, and irritation cause the excoriation and
lichenification of the skin that are often seen.
N
CLINICAL PRESENTATION OF ATOPIC DERMATITISAND ITS DIFFERENTIAL DIAGNOSIS
Seth J. Orlow, MD, PhD
Atopic dermatitis can be characterized by age-determined pat-
terns. The disease can be thought of as having infantile, child-
hood, and adolescent/adult stages. In young infants, erythema
and raised papules are the chief characteristics seen, and involve-
ment typically occurs on the cheeks, forehead, and scalp. The
extensor surfaces of the arms and legs often are affected. The
infant may be quite itchy and miserable but too young to possess
the ability to scratch the affected areas. Parents are often surprised
to learn that their child is itchy since they do not see the infant
scratching. Atopic infants too young to scratch will typically rub
the area bothering them. When the infant becomes able to
scratch or rub persistently, the affected area may evolve into ery-
thematous, scaling, oozing, crusty patches, and plaques.
The diaper area of an infant with atopic dermatitis is typically
spared. If atopic dermatitis is evident in the diaper area, this may
suggest that food allergies are responsible. According to Sicherer
and Sampson,1 approximately 40% of children with moderate to
severe atopic dermatitis have food allergies. However, it is unclear
what role the allergy plays in provoking a flare of atopic dermati-
tis in the majority of children.
In the childhood stage, atopic dermatitis is most likely to
appear on the flexor surfaces—antecubital and popliteal fossae,
wrists, ankles, and neck.2 If the disease is not controlled, scratch-
ing causes the skin to thicken, lichenification begins to occur, and
pigmentary changes may become evident (Figure 1).
Many pediatric patients do “outgrow” the disease. Even in
those who do not, the condition typically ameliorates over time.
INTRODUCTION
ne of the more common sights to be found at a pedia-
trician’s office is a parent accompanied by a child who is
described as “red and itchy.” Is it atopic dermatitis or a
host of other cutaneous conditions that present with
similar symptoms? Atopic dermatitis is a disease estimated to
affect 10% to 20% of children.1 It has a characteristic presenta-
tion but no definitive laboratory tests.
In these pages, Seth J. Orlow, MD, PhD, reviews the major
and minor clinical criteria needed to make a diagnosis of atopic
dermatitis, with special emphasis on infantile and childhood pre-
sentations of the disease. He provides insight on how to make the
differential diagnoses between atopic dermatitis and conditions
with which it might be confused, such as seborrheic dermatitis,
allergic contact dermatitis, scabies, and psoriasis. Ronald C.
Hansen, MD, reviews the prevalence and pathophysiology of
O
Tor A. Shwayder, MD
atopic dermatitis and factors thought to exacerbate the condition
and summarizes the benefits and limitations of conventional
treatment, which currently comprises a constellation of cortico-
steroid, emollient, antibiotic, and allergen-avoidance therapies.
In his presentation, Moise L. Levy, MD, focuses on the novel
calcineurin inhibitors that offer a corticosteroid-free option for
those concerned about skin atrophy and other side effects of top-
ical corticosteroid use. He reviews the many recent short-term
and long-term safety and efficacy trials of the topical
immunomodulators tacrolimus and pimecrolimus in infants,
children, adolescents, and adults.
Reference1. Schultz-Larsen F, Hanifin JM. Epidemiology of atopic dermatitis.
Immunol Allergy Clin North Am. 2002:22:1-24.
Lichenification in atopic dermatitis is characterized by skin thickeningand the exaggeration of normal skin markings. Pigmentary changesare particularly evident in patients with darker skin.Courtesy of Seth J. Orlow, MD, PhD
Figure 1. Lichenified Atopic Dermatitis
Novartis/PED/Derm2 1/23/03 3:28 PM Page 5

Atopic Dermatitis in the Pediatric Patient 5
It is recommended that physicians not tell parents that their
child’s atopic dermatitis will disappear by a certain age, because it
is impossible to predict which patient will have persistent disease.
A useful analogy pediatricians can use for parents is that atopic
dermatitis prevalence is shaped like a pyramid, with infants at the
bottom and adults at the top.
Atopic dermatitis after puberty implies a higher risk of lifelong
involvement. In adults, atopic dermatitis most commonly occurs
on the face, hand, or antecubital regions. This discussion, how-
ever, will focus primarily on atopic dermatitis in the pediatric
patient.
Diagnostic Criteria for Atopic DermatitisFormal diagnostic criteria have been
established for the diagnosis of atopic der-
matitis. They are typically used in a
research setting. Many of them are varia-
tions of the Hanifin-Rajka criteria, estab-
lished during the First International
Symposium on Atopic Dermatitis, in
1979.3 According to these criteria, three of
the following four major features must
be present for a diagnosis of atopic
dermatitis:
• Pruritus, often severe
• Morphology and distribution that includes facial and/or
extensor involvement in infants and flexor and/or neck
involvement in children
• Chronically relapsing course
• Personal or family history of atopy (eg, allergic rhinitis,
allergic conjunctivitis, asthma)
Pruritus is the hallmark of the disease, whether or not the
patient is old enough to scratch the affected area or voice the
complaint. Parents are often disappointed to learn that atopic
dermatitis is chronically relapsing and that there is no magic cure
that will permanently eradicate their child’s condition.
In addition to having at least three major features, the patient
should exhibit at least three of these minor features, which have
been grouped into three broad categories:
Common/General
• Xerosis
• Ichthyosis vulgaris/keratosis pilaris/palmar hyperlinearity
• Early age of onset
• Tendency toward cutaneous infections/impaired cell-
mediated immunity
• Tendency toward nonspecific hand or foot dermatitis
• Nipple eczema
• Erythroderma
Facial/Ocular
• Cheilitis of upper lip
• Recurrent conjunctivitis
• Infraorbital (Dennie-Morgan) fold/orbital darkening
• Keratoconus
• Posterior/anterior subscapular cataracts
Hyperreactivity
• Increased levels of serum immunoglobulin E (IgE)
• Positive (type 1) hypersensitivity on skin tests
• Peripheral blood eosinophilia
It should be noted that although elevated serum IgE is a com-
mon finding in atopy, approximately 20% of patients with atopic
dermatitis have normal levels.4 A patient’s parents may be
confused by the classification of atopic dermatitis as an “allergic”
disorder, since it may lead to the erroneous conclusion that iden-
tification of a single or multiple allergic agents can “cure” their
child’s disease. A better way to describe the child’s condition is to
explain that atopic dermatitis is not an allergy to any one thing
but a “supersensitivity” to myriad provocational factors, many of
them irritant in nature.
Nummular dermatitis lesions are some-
times seen in pediatric patients with atopic
dermatitis. The lesions appear as round,
fixed, very itchy plaques that are thicker than
the sites of atopic dermatitis elsewhere on
the child’s body. They sometimes can be mis-
taken for psoriasis because they are thick and
scaly like psoriatic lesions, but there is usual-
ly other evidence of atopic dermatitis
present. Nummular dermatitis also can be
distinguished from tinea corporis by the fact
that unlike those characteristic of tinea corporis, nummular lesions
are multiple, symmetric, and lacking in pustules and evidence of
central healing. The condition can be distinguished from impetigo
lesions in that nummular dermatitis lesions, although sometimes
crusted, are clearly thick inflammatory plaques.
Infectious Complications of Atopic DermatitisSome lesions that appear on the skin of children with atopic der-
matitis are the result of infections of the disease. The major infec-
tious complications of atopic dermatitis are eczema herpeticum,
molluscum contagiosum, and impetigo.
Eczema herpeticum is caused by the spread of herpes simplex
virus into atopic dermatitis lesions. Eczema herpeticum, also
known as Kaposi’s varicelliform eruptions, appears as 2- to 3-mm,
punched-out, hemorrhagic erosions that skip from one area of der-
matitis to another. A primary herpetic infection may be accompa-
nied by fever, malaise, and lymphadenopathy. The most serious
complication in a normal host is risk of keratitis. Because it also
predisposes to the spread of smallpox, atopic dermatitis is a con-
traindication to smallpox vaccination.
Molluscum contagiosum is the most common viral complication
of atopic dermatitis. These dome-shaped papules have a caseous
core. The papules, which can appear in large numbers in atopic
patients, are typically flesh-colored but can be inflamed and erythe-
matous. Sometimes they are surrounded by eczematous patches. In
pediatric patients with atopic dermatitis, outbreaks typically occur
along the flanks and the antecubital and popliteal fossae.
Impetigo is a common bacterial complication of atopic dermati-
tis (Figure 2, page 6). It has been known for 40 years that atopic
“...atopic dermatitisis not an allergy toany one thing but a‘supersensitivity’ to
myriad provocationalfactors, many of them
irritant in nature.”
y
y
Novartis/PED/Derm2 1/9/03 5:55 PM Page 6

6 Atopic Dermatitis in the Pediatric Patient
patients have substantial quantities of Staphylococcus aureus in their
skin, particularly in the regions where they experience flares, so it
is not surprising that they are more prone to bacterial skin infec-
tion. Impetigo is characterized by vesicles or bullae with straw-col-
ored discharge that dries to form a thick crust.
Distinguishing Atopic Dermatitis From Four Common Conditions
Many dermatoses resemble atopic dermatitis, at least superfi-
cially. Some conditions with which it can be confused include
seborrheic dermatitis, allergic contact dermatitis, scabies, and
psoriasis. However, there are frequently clues, such as disease his-
tory or lesion distribution, that can aid the physician in distin-
guishing them from atopic dermatitis.
Infantile seborrheic dermatitis, commonly known as cradle
cap, has an earlier onset than atopic dermatitis. Pruritus is usual-
ly lacking. It may be present on the face, ears, scalp, and trunk,
where one often sees atopic dermatitis, but it may also appear in
skinfolds, axillae, and groin—sites where atopic dermatitis usual-
ly is not found. It is typified by the presence of a greasy yellow
scale. If the pediatrician is unable to distinguish it from atopic
dermatitis during the first office visit, having the child return for
a second visit to see how the condition has responded to treat-
ment is usually sufficient to make the correct diagnosis.
Allergic contact dermatitis is an eczematous dermatitis, but it
is not atopic dermatitis. Common causes are exposure to poison
ivy or nickel (contained in items such as jewelry or belt buckles).
It may have a sudden onset or appear insidiously, and it may
exhibit an unusual distribution. For example, a patient may have
a square patch of dermatitis on one arm from exposure to tape
used to secure an intravenous line, or inflammation on an earlobe
where a nickel-containing gold earring stud was inserted.
Key features that distinguish scabies from atopic dermatitis are
that, in addition to papules, small linear burrows and sometimes
nodules are present. Scabies is caused by skin infestation by a
mite and spreads easily in infants and immunocompromised
patients, so there can be large-scale involvement along the flanks,
wrists, ankles, palms, soles, and scalp. Older children and adults
may have scabies on their finger webs, wrists, axillae, and groin.
Another clue to the diagnosis of scabies may be that pruritus is
not limited to the patient but may include other family members
or those who have come in close contact. Microscopic examina-
tion of skin scrapings can reveal the presence of the mite, her eggs,
or feces.
The morphology of psoriasis is also different from that of
atopic dermatitis. In psoriasis, well-circumscribed lesions consist
of pink plaques topped with silvery white scale. Tearing the scale
off a psoriatic plaque will reveal the Auspitz sign—multiple fine
bleeding points caused by thinning of the epidermis over the der-
mal papillae. There is typically less pruritus with psoriasis than
with atopic dermatitis. Distribution is symmetric, with lesions
found on extensor extremities, behind the ears, on palmar/plantar
skin, and on the scalp. One would not expect to find atopic der-
matitis or seborrheic dermatitis on the palms and soles. Younger
children can have facial involvement. Psoriasis can also be found
in the diaper area, where atopic dermatitis is uncommon.
Less Common Differential DiagnosesLess common dermatoses that may occasionally need to be dis-
tinguished from atopic dermatitis include dermatophytosis (tinea
corporis), drug eruptions, dermatomyositis, and cutaneous T-cell
lymphoma.
It is important to recognize tinea corporis because the topical
corticosteroids used to treat atopic dermatitis will worsen a fungal
infection. Tinea lesions typically have an asymmetric, scaly border
with central clearing. Sometimes there are pustules. Diagnosis can
be confirmed by performing a culture.
Certain medications can trigger erythema and pruritus in some
patients. A full review of drug reactions in children has recently
been published.5 Dermatomyositis may at first be mistaken for
atopic dermatitis because there is typically some facial involve-
ment, including the eyelids. However, violaceous papules on the
knuckles are pathognomonic for dermatomyositis. Edema in the
periorbital tissue and sun provocation are also characteristic of
that disease. In pediatric patients, muscle weakness and calcinosis
of subcutaneous tissue are common.
Cutaneous T-cell lymphoma is extremely rare in children and
encompasses several non-Hodgkin’s lymphomas that present
initially in the skin, including mycosis fungoides and its
leukemic phase, Sézary syndrome. Mycosis fungoides first appears
as erythematous scaly patches that are few in number and typi-
cally distributed on the trunk or limb girdle area. These persis-
tent, pruritic patches may be mistaken for atopic dermatitis at
first. Skin biopsy of suspicious lesions can confirm diagnosis of
mycosis fungoides.
ConclusionAlthough atopic dermatitis cannot be diagnosed definitively
by laboratory tests or pathognomonic lesions, the disease is
Continued on page 15.
Staphylococcus aureus is the pathogen most likely to cause impetigo in patients with atopic dermatitis. The cutaneous lesions are character-ized by pus-filled vesicles that rupture. The thick, pale-yellow dischargedries and crusts.Courtesy of Seth J. Orlow, MD, PhD
Figure 2. Infectious Complications of Atopic Dermatitis: Impetigo
Novartis/PED/Derm2 1/9/03 5:56 PM Page 7

Atopic Dermatitis in the Pediatric Patient 7
THE PATHOPHYSIOLOGY OF ATOPIC DERMATITISAND STANDARD THERAPIES
Ronald C. Hansen, MD
topic dermatitis (AD) is a chronic inflammatory skin
disease that has experienced increasing prevalence over the
past 40 years in industrialized countries. Recent studies of
atopic dermatitis in pediatric populations have found rates
of 17.2% in the United States (among children 5 to 9 years of age),
15.6% in northern Europe (children 7 years of age), and 19% in
Japan (children 7 to 9 years of age).1,2,3 A study of childhood preva-
lence of atopic dermatitis in 56 countries found wide variations
within and between countries, affecting approximately 5% to 20%
of children at 6 to 7 years and 13 to 14 years of age.4 The authors
concluded that the disease is a major public health problem
worldwide.
Approximately half of all cases of atopic
dermatitis are diagnosed before 1 year of age,
and 80% are diagnosed by 5 years of age.5
Although atopic dermatitis will remit in a
majority of children by the time they reach
puberty, this is small comfort to the parents
of an infant or toddler whose skin is ravaged
by severe disease. In its severest manifesta-
tions, atopic dermatitis can cause failure to
thrive.6 Children besieged by pruritus have
little interest in eating, and their appetite is
further suppressed by the release of
cytokines, including tumor necrosis factor, that have a cachectic
effect. They also lose substantial amounts of albumin from exfoli-
ated skin. According to one study, school-aged children with
moderate to severe atopic dermatitis are at high risk of developing
psychological difficulties.7 Although there is no cure for atopic der-
matitis, there are, fortunately, many more tools available today to
help control and manage its flares.
Pathogenesis and Immunology of Atopic Dermatitis
The precise pathogenesis of atopic dermatitis is unclear;
however, genetics and environmental factors are both thought to
play a role. There is also evidence to suggest that atopic individu-
als exhibit altered local immune responses to many different stim-
ulants, including antigens.
Approximately 60% to 70% of children with atopic dermatitis
have a family history of atopy (eg, asthma, allergic rhinitis, atopic
dermatitis).8 A substantial number of children have no obvious
family history of atopic disease, however. One way to explain the
condition to parents, whether there is a family history or not, is
that the child has genetically determined itchy skin.
According to Leung,9 the following immunoregulatory abnor-
malities are characteristic of patients with atopic dermatitis
(Table 1):
• Increased levels of serum
immunoglobulin E (IgE)
• Eosinophilia
• Increased spontaneous histamine
release from basophils
• Chronic macrophage activation
• Increase in interleukin (IL)-4– and
IL-5–secreting T-helper type 2 (TH2)
cells
• Decrease in interferon (IFN)-�–
secreting TH1 cells
The increased IgE response and eosinophilia seen in atopic
dermatitis reflect the increased expression of TH2 cytokines, and
these factors plus the histamine release from basophils increase
the pruritus and inflammation experienced by the patient.
The central mechanisms by which atopic dermatitis initiates
are believed to be as follows: Langerhans’ cells, which are den-
dritic antigen-presenting cells in the epidermis, hyperstimulate T
cells, perhaps in response to specific antigens.10 As indicated in
the list of immunologic findings above, the two subtypes of T
cells primarily affected are TH2 cells, associated with acute atopic
dermatitis, and TH1 cells, associated with chronic disease.
After the activated Langerhans’ cell, which has IgE bound to
it, presents the antigen to the T cells, a number of processes
begin to occur, including calcineurin phosphatase, which Dr.
Levy discusses in more detail elsewhere in this supplement, that
activates T cells. In acute atopic dermatitis, TH2 cells infiltrate
the dermis. The TH2 response is accompanied by increased IgE
levels and expression of IL-4 and IL-5 and manifests clinically
and histologically with papulation and spongiosis. Histamine
release plays only a small role in this T-cell activation process,
which is why antihistamines are relatively ineffective in treating
atopic dermatitis.
As the disease progresses from an acute to a chronic phase,
there is a biphasic switch from TH2 to TH1 cellular response,
A
“Approximately halfof all cases of atopic
dermatitis are diagnosed before 1 year of age, and80% are diagnosedby 5 years of age.”
Table 1. Systemic Immune Findings in Atopic Dermatitis
• Increased serum IgE• Eosinophilia• Increased spontaneous histamine release
from basophils• Chronic macrophage activation• More IL-4/IL-5–secreting TH2 cells• Fewer IFN�-secreting TH1 cells
(but greater role in chronic stages)Adapted from: Leung DYM. J Allergy Clin Immunol. 2000;105:860-876
Novartis/PED/Derm2 1/9/03 5:56 PM Page 8

8 Atopic Dermatitis in the Pediatric Patient
accompanied by the clinical/histologic evidence of lichenifica-
tion, epidermal hypertrophy, and dermal fibrosis.
Exacerbants and Triggers of Atopic DermatitisA person with atopic dermatitis has skin that is hyperirritable.
A number of factors can cause the disease to relapse or worsen.
Known exacerbants and triggers include anxiety and stress, cli-
matic factors, irritants, allergens, and infection (Table 2).
Psychosocial factors such as anxiety and stress influence the
disease process of atopic dermatitis. The relentless pruritus of
active disease can create a vicious cycle by evoking irritability and
sleep disturbance that further erode a patient’s emotional state.
Changes in both temperature and humidity can affect the dis-
ease. Patients’ atopic dermatitis may worsen in winter, when the
air is cold and dry. The warm, arid air of desert climes (and
indoor heating) similarly may heighten pruritus by causing xero-
sis. Excessively warm, moist air can be equally irritating to atopic
patients because it triggers perspiration that leaves skin desiccat-
ed and/or pruritic.
Patients with atopic dermatitis have reduced tolerability to
irritants, which can be either chemical or physical. The most
common irritant is water. Any water exposure—swimming,
showering, repeated hand washing—is ultimately drying to the
skin, unless an emollient is applied immediately afterward to trap
moisture in the stratum corneum. As already noted, water in the
form of perspiration is drying to the skin. Soaps, detergents, per-
fumes, and solvents are examples of chemical irritants. Wool and
other rough material, including synthetics, fall into the category
of cutaneous contact irritants.
Contact allergic reactions to certain substances (eg, cosmetics
and topical medications) can provoke recurrence of atopic der-
matitis. The degree to which aeroallergens (particularly pollen
and house dust mites) and food allergens are atopic dermatitis
cofactors is the subject of an ongoing debate. Although a large
number of patients with atopic dermatitis also have respiratory
and food allergies, the role such allergies play in the actual
pathogenesis of atopic dermatitis is unclear. There is certainly no
harm in experimenting with elimination diets for foods most
likely to cause allergic reactions (eg, eggs, milk, peanuts, soy, and
wheat), as such reactions may complicate allergic dermatitis in a
subset of sensitized patients. However, it is recommended that
elimination diets be done in conjunction with, not in lieu of,
other therapies for atopic dermatitis.
The primary microbial allergen is Staphylococcus aureus. It is
found in more than 90% of patients with atopic dermatitis lesions;
in contrast, only 5% of healthy subjects harbor the organism on
their skin.9 Because of the pervasiveness of S. aureus in atopic
patients, a positive culture does not necessarily indicate a clinically
relevant infection. However, it appears that the organism may
worsen atopic dermatitis even when it does not cause obvious
infection. Lever et al11 found that topical antibiotic treatment
reduced clinical severity in patients with atopic dermatitis even in
the absence of overt infection. Fungal infection from Malassezia
furfur (also called Pityrosporum ovale) also has been implicated as a
pathogen in atopic dermatitis. These ubiquitous lipophilic yeasts
are associated with immune response in atopic dermatitis, especial-
ly head and neck dermatitis.12 However, the role of these yeasts in
causation and exacerbation of atopic dermatitis is much more con-
troversial than the role of S. aureus.
Pruritus Control Is KeyIt is often said of atopic dermatitis that it is not the rash that
itches, but the itch that rashes. Patients with atopic dermatitis
have a lower itch threshold. In addition to the environmental,
allergenic, and infectious exacerbants discussed, the itch-scratch
cycle is intrinsic to the perpetuation of atopic dermatitis. In the
itch-scratch cycle, pruritus invokes scratching, scratching causes
skin trauma and excoriation, which then lead to inflammation
and more pruritus. Chronic inflammation and scratching lead to
lichenification of the skin.
Controlling the patient’s pruritus, therefore, is paramount to
disease management. The itch-scratch cycle must be interrupted.
Because pruritus precedes the visible eruption, therapy should be
initiated then.
Xerosis, or abnormally dry skin, is a common complaint of
atopic dermatitis and a source of pruritus on its own. Xerosis occurs
in 48% to 98% of patients with atopic dermatitis.13 Atopic skin has
Table 3. Therapies for Atopic Dermatitis
• Combination therapy for effective control– Emollients– Irritant and allergen avoidance– Antihistamines– Topical corticosteroids (first-line therapy)– Antibiotics– Phototherapy (eg, PUVA)– Immunosuppressive/immunomodulatory therapy– Corticosteroid-free agents
PUVA= psoralen plus ultraviolet AAdapted from: Beers MH, Berkow R, eds. Dermatitis. In: The Merck Manual of Diagnosis andTherapy. 17th ed. Rahway, N.J.: Merck Research Laboratories; 1999:816-818.
Table 2. Exacerbants and Triggers
• Anxiety/stress
• Climate factors– Temperature– Humidity
• Irritants– Detergents, solvents– Wool or other rough material– Perspiration
• Allergens (contact, inhaled, and possibly food)
• Infection (staph)
Adapted from: Glickman FS. In: Clinics in Dermatology. Greenwich, Conn.: Conn.
Postgraduate Healthcare. Berkow R, Fletcher AJ, eds. Dermatitis. In: The Merck Manual of
Diagnosis and Therapy. 16th ed. Rahway, N.J.: Merck Research Labs, 1992:2407-2415.
Novartis/PED/Derm2 1/17/03 5:34 PM Page 9

Atopic Dermatitis in the Pediatric Patient 9
been found to have reduced water-binding capacity. When water
content of the stratum corneum is decreased, skin barrier function
is impaired and the skin is more easily irritated and pruritic.
As noted previously, atopic skin is hyperirritable, and certain
conditions may trigger pruritus in the atopic patient that would
not affect others, such as perspiring after exertion or exposure to
perfumes, cosmetics, soaps, or other prod-
ucts.
Standard Therapies for AtopicDermatitis
Combination therapy appears to be the
most effective control for atopic dermati-
tis, and the physician’s treatment arsenal
includes emollients, avoidance of triggers,
antihistamines, topical corticosteroids,
antibiotics, phototherapy, and immuno-
suppressive therapy, as well as the new
corticosteroid-free topical agents Dr. Levy discusses in detail
elsewhere in this supplement (Table 3).
Emollients
Emollients are a mainstay of atopic dermatitis therapy. They
restore moisture to the epidermis and help relieve pruritus. Lucky
et al14 found emollients to be corticosteroid-sparing in the
treatment of mild to moderate atopic dermatitis in a pediatric
population. Emollients should be applied routinely and after
every skin-drying experience such as showering, swimming, or
physical activity that generates heavy perspiration. Even when
topical corticosteroids are used on lesions, emollients should be
applied to uninvolved skin.
Corticosteroids
Topical corticosteroids have represented the traditional first-
line therapy for many years. Used correctly, these antiinflamma-
tory agents are effective, inexpensive, and relatively safe.
Corticosteroids are ranked by potency into seven classes. To avoid
potential side effects, it is recommended that one use the least
potent corticosteroid that will interrupt the itch-scratch cycle;
only low-potency formulations should be used on the face, groin,
skinfolds, and axillae.
Topical corticosteroids have many limitations, however
(Table 4). One is tachyphylaxis. After extended use, these agents
lose some of their effectiveness. Problems associated with long-
term use of corticosteroids, although rare, include serious skin
side effects such as atrophy, telangiectasia, and striae. If cortico-
steroids are applied to the eyelid or periorbital area, there is a risk
of cataract and glaucoma. Systemic side effects such as hypothal-
amic-pituitary-adrenal (HPA)–axis suppression represent a special
risk in pediatric populations, because children have a higher body
surface area-to-weight ratio than adults.
Steroid phobia is another limitation of corticosteroid therapy.
Although corticosteroids are relatively safe when used correctly,
parental, patient, and, to some extent, physician concern over
their toxicity affects compliance. Charman et al15 found that 73%
of patients worried about using topical corticosteroids on them-
selves or on their children, and 24% admitted to noncompliance
due to these concerns. The concern over side effects also causes
physicians to convey an inconsistent message. Parents are told to
use the corticosteroids on their children to stop the rash, but to
stop before side effects occur. They find these instructions con-
fusing and halt therapy prematurely, resulting in undertreatment
and a child with poorly controlled disease.
One way to combat steroid phobia, if the
parents cannot be convinced that these
products can be used safely, is to switch to
one of the corticosteroid-free agents now
available.
Oral corticosteroids have proven to be
effective and fast-acting in treating atopic
dermatitis, but there are toxicity issues with
repeated use. Another limitation is that
their effectiveness tends to derail the topical
program that needs to accompany the oral
therapy. The children get better right away, so the parents do not
see the need to embark on the labor-intensive process of applying
emollients and topical corticosteroids, administering hydrother-
apy, and taking the other steps involved to prevent flare
recurrence. In this pediatric dermatologist’s experience, oral corti-
costeroids are reserved for emergency therapy.
Other therapies
Avoidance of food and inhalant allergens, chemical and
mechanical irritants, and other triggers, such as stress or tempera-
ture extremes, can be beneficial but is not always possible. Oral
antihistamines are often used to treat pediatric patients and are
thought to work primarily through sedating the patient, providing
relief from nocturnal scratching. (For this reason, it is unclear
whether the newer nonsedating antihistamines are effective in treat-
ing atopic dermatitis.) Topical antihistamines have not demonstrat-
ed much benefit and pose the risk of cutaneous sensitization.
Antibiotics are likely underused in the treatment of atopic
dermatitis. As noted previously, these agents can be effective in
treating the disease even in patients with no obvious bacterial
Table 4. Limitations of Topical Corticosteroid Therapy
• Efficacy (tachyphylaxis)
• Skin side effects– Atrophy– Telangiectasia– Striae
• Risk of cataract and glaucoma (eyelid application)
• HPA-axis suppression– Since children have higher body surface area
(BSA)-to-weight ratio than adults, they are moreprone to systemic steroid effects
Adapted from: Leung DY, et al. Ann Allergy Asthma Immunol. 1997;79:197-211. Hepburn D,et al. Adv Dermatol. 1994;9:225-254.
“Combination therapy appears to be the most
effective control for atopic
dermatitis...”
Novartis/PED/Derm2 1/9/03 5:57 PM Page 10

10 Atopic Dermatitis in the Pediatric Patient
infection. Viral pathogens, addressed elsewhere in this supple-
ment by Dr. Orlow, also need to be treated when present, as do
fungal pathogens, which increase the risk of dermatophyte
infections in atopic dermatitis.16
Phototherapy using ultraviolet light is sometimes prescribed
for patients with recalcitrant disease.17 Studies investigating
immunosuppressive therapy (eg, cyclosporine) for treatment of
atopic dermatitis have shown mixed results. The therapy may
be better suited for adults than for pediatric patients.
Mentholated lotions, which counterstimulate and distract the
patient, may provide temporary relief but do not provide real
therapeutic benefit. Topical cromolyn has been investigated for
its antipruritic benefit for atopic patients, but it cannot
penetrate the epidermis sufficiently to inhibit mast cell
degranulation.
ConclusionAtopic dermatitis is a disease with a poorly understood patho-
genesis and is best treated with a combination of therapies.
Conventional treatment therapies all have limitations, and most
patients with moderate to severe disease are inadequately treated.
Atopic dermatitis has a significant impact on the quality of life
and psychosocial health of the pediatric patient and on the
patient’s family as well.
References1. Laughter D, Istvan JA, Tofte SJ, Hanifin JM. The prevalence of
atopic dermatitis in Oregon schoolchildren. J Am Acad Dermatol.
2000;43:649-655.
2. Schultz-Larsen F, Diepgen T, Svensson A. The occurrence
of atopic dermatitis in North Europe: An international question-
naire study. J Am Acad Dermatol. 1996;34:760-764.
3. Sugiura H, Umemoto N, Deguchi H, et al. Prevalence of child-
hood and adolescent atopic dermatitis in a Japanese population:
Comparison with the disease frequency examined 20 years ago.
Acta Derm Venereol. 1998;78:293-294.
4. Williams H, Robertson C, Stewart A, et al. Worldwide variations
in the prevalence of symptoms of atopic eczema in the interna-
tional study of asthma and allergies in childhood. J Allergy Clin
Immunol. 1999;103:125-138.
5. Leung DYM. Atopic dermatitis: Immunobiology and treatment
with immune modulators. Clin Exp Immunol. 1997;107(suppl
1):25-30.
6. Abrahamov A, Schifmann R, Goldstein R, et al. Growth failure
due to protein loss in dermatitis. Eur J Pediatr. 1986;145:223-
226.
7. Absolon CM, Cottrell D, Eldridge SM, Glover MT. Psychological
disturbance in atopic eczema: The extent of the problem in
school-aged children. Br J Dermatol. 1997;137:241-245.
8. Svensson A. Diagnosis of atopic skin disease based on clinical cri-
teria. Thesis. Kristionsted: Bohlins Grafiska, 1989.
9. Leung DYM. Atopic dermatitis: New insights and opportunities
for therapeutic intervention. J Allergy Clin Immunol. 2000;105:
860-876.
10. Hanifin JM, Chan S. Biochemical and immunologic mechanisms
in atopic dermatitis: New targets for emerging therapies. J Am
Acad Dermatol. 1999;41:72-77.
11. Lever R, Hadley K, Downey D, Mackie R. Staphylococcal colo-
nization in atopic dermatitis and the effect of topical mupirocin
therapy. Br J Dermatol. 1988;119:189-198.
12. Jensen-Jarolim E, Poulsen L, With H, et al. Atopic dermatitis of
the face, scalp, and neck: Type 1 reaction to the yeast
Pityrosporum ovale? J Allergy Clin Immunol. 1992;89:44-51.
13. Linde YW. Dry skin in atopic dermatitis. Acta Derm Venereol.
Suppl (Stockh). 1992;177:9-13.
14. Lucky AW, Leach AD, Laskarzewski P, Wenck H. Use of an emol-
lient as a steroid-sparing agent in the treatment of mild to mod-
erate atopic dermatitis in children. Pediatr Dermatol. 1997;14:
321-324.
15. Charman CR, Morris AD, Williams, HC. Topical corticosteroid
phobia in patients with atopic eczema. Br J Dermatol. 2000;
142:931-936.
16. Rudikoff D, Lebwohl M. Atopic dermatitis. Lancet. 1998;
351:1715-1721.
17. Leung DY, Hanifin JM, Charlesworth EN. Disease management
of atopic dermatitis: A practice parameter. Ann Allergy Asthma
Immunol. 1997;79:197-211.
Novartis/PED/Derm2 1/17/03 5:35 PM Page 11

Atopic Dermatitis in the Pediatric Patient 11
opical corticosteroids are the cornerstone of conventional
treatment for atopic dermatitis at present, as Dr. Hansen
has described elsewhere in this supplement, but new treat-
ment therapies have recently been introduced that show
promising results in some short-term and long-term pediatric
studies.
This discussion focuses on two topical corticosteroid-free
immunomodulatory agents, tacrolimus and pimecrolimus.
Tacrolimus, formerly known as FK506, is the older of the two
drugs. It was approved for atopic dermatitis treatment by the U.S.
Food and Drug Administration in late 2000. Tacrolimus was first
developed to prevent allograft rejection in liver and kidney trans-
plant recipients and is still used for that purpose. Pimecrolimus, an
ascomycin derivative formerly known as SDZ ASM 981, was
approved approximately 1 year later. It was the first immunomod-
ulatory therapy to be developed specifically to treat inflammatory
skin diseases.
Calcineurin Inhibitors: Similarities and Differences
Both tacrolimus and pimecrolimus are commonly referred to
as immunomodulatory drugs or antiinflammatory agents. The
term that best describes their mechanism of action might be
topical calcineurin inhibitors. As Dr. Hansen notes in his dis-
NEW THERAPIES FOR ATOPIC DERMATITIS
Moise L. Levy, MD
cussion, atopic dermatitis originates from an inflammatory
cascade resulting from T-cell hyperstimulation from antigen-
presenting cells. Both tacrolimus and pimecrolimus have the
ability to bind with a specific immunophilin or macrophilin
and then to calcineurin. This effectively blocks the dephospho-
rylation of the nuclear factor of activated T cells (NF-AT),
which is a necessary step in activating the T cells that generate
the proinflammatory cytokines.
Tacrolimus and pimecrolimus have very similar chemical
structures. However, the small structural differences that distin-
guish them from one another can lead to a host of important
differences in pharmacologic activity.
Meingassner et al1 compared pimecrolimus with tacrolimus in
murine and rat models of T-cell–mediated skin inflammation
(allergic contact dermatitis). The same study also compared the
two agents in systemic immunosuppression (graft-vs-host and
kidney transplant rat models) (Figure 1). Pimecrolimus was
found to be as effective as tacrolimus in skin inflammation mod-
els. In the immunosuppression models, however, pimecrolimus
was found to have a low potential for affecting systemic immune
responses, in contrast to tacrolimus. These findings indicate that
pimecrolimus, unlike tacrolimus, has a skin-selective pharmaco-
logic profile. Research by Bilich et al2 showed pimecrolimus to be
more lipophilic and permeate less through rat, pig, and human
Figure 1. Pimecrolimus vs Tacrolimus in Systemic Immunosuppression
T
0
1
2
3
4
5
ACD rat ACD mouse Graft vs host Kidney transplant
>2
1/66 1/15
Skin inflammation models
Potency Relative to Tacrolimus in Animal Models
Equivalence
Systemic immunosuppression models
oral oral sc oral
ACD = allergic contact dermatitis;sc = subcutaneous.
1
Pim
ecro
limus
: ta
crol
imus
Adapted from Meingassner JG et al. (inflammation/immunosuppression models),Presented at AAD 60th Annual Meeting, February 2002, New Orleans, La.
Novartis/PED/Derm2 1/17/03 5:36 PM Page 12

12 Atopic Dermatitis in the Pediatric Patient
Figure 2. Infantile Atopic Dermatitis
skin than tacrolimus, suggesting that pimecrolimus offers a lower
risk of systemic exposure.
In open-label pharmacokinetic studies of pediatric patients
(3 months to 14 years of age) with moderate to severe atopic
dermatitis treated with pimecrolimus 1% cream, blood concen-
trations of pimecrolimus were found to be consistently low
(99.2% <2 ng/mL) regardless of age, extent of skin area treated
(19% to 92% of body surface area), and duration of therapy (up
to 1 year).3 Even after oral administration of pimecrolimus, a reg-
imen under examination as a treatment for psoriasis in adults,
blood concentrations were found not to exceed 55 ng/mL.4 No
systemic accumulation was seen over a 12-month duration in
any of these studies.
Short-Term Studies Show Calcineurin Inhibitors Provide Fast Results
The effectiveness of both tacrolimus and pimecrolimus, com-
pared to vehicle, has been investigated in short-term studies of
adult and pediatric patients.
Tacrolimus
Paller et al5 evaluated topical tacrolimus at two different
concentrations (0.03% and 0.1%) vs vehicle in a randomized,
double-blind, 12-week study of 351 children 2 to 15 years of age
who had moderate to severe atopic dermatitis. The primary effi-
cacy end point was physician global assessment. Patients were
evaluated at baseline and at weeks 1, 2, 3, 6, 9, and 12.
Significantly more patients (P<0.001) achieved clinical improve-
ment of 90% or greater (ie, excellent improvement or cleared)
with either strength of the active medication, compared with
vehicle. Improvements were achieved early in treatment and
maintained throughout the study.
In a pooled analysis of two 12-week, randomized, double-
blind studies of adult patients with moderate to severe atopic
dermatitis, Hanifin et al6 found that tacrolimus performed sig-
nificantly better (P<0.001) than vehicle, as measured by several
efficacy indicators. The adult studies, which had a total of 632
patients, used the same two concentrations of tacrolimus as the
aforementioned children’s study. In adults, the 0.1% concentra-
tion was found to be more effective in patients with severe
disease or more extensive body surface involvement.
A pediatric safety study of 180 children 7 to 16 years of age
by Boguniewicz et al7 tested three concentrations of tacrolimus
(0.03%, 0.1%, and 0.3%) for 22 days with a 2-week follow-up.
The study found no serious systemic adverse events; the most
common application-site events were pruritus and skin burning.
Pimecrolimus
Efficacy and safety of pimecrolimus were examined in three
6-week, randomized, double-blind trials of pediatric patients with
mild to moderate atopic dermatitis.8,9 The results of two of the
studies of children 1 to 17 years of age were combined. The pooled
results of those two trials, in which a total of 403 patients partici-
pated, will be referred to in this discussion as the children’s study.
The third study, in 186 infants 3 to 23 months of age, was similar
in design. It will be called the infants’ study.
In both the children’s and the infants’ studies, once the 6-week
phase ended, patients who had been on vehicle were allowed to
receive active medication in a 20-week, open-label extension.
The primary efficacy end point in both studies was Investigator
Global Assessment (IGA). The IGA ranks disease severity on a scale
of 0 (clear, defined as no inflammatory signs of atopic dermatitis)
to 5 (very severe, defined as erythema and papulation/infiltration
with oozing and crusting). Treatment success was defined as an IGA
score of 0 (clear) or 1 (almost clear) at day 43.
Secondary efficacy parameters for both studies included
Eczema Area and Severity Index (EASI) score and severity of pru-
ritus score. With the EASI, proportionate values are assigned to
four body regions, and each region is assessed separately for ery-
thema, infiltration/papulation, excoriation, and lichenification.
The severity of each region is assigned a score of 0 to 3, or from
none to severe. Possible total scores range from 0 (no disease any-
where on the body) to 72 (severest disease over total body surface
area). The pruritus score was assigned by the caregiver after
patient interview; numerical values ranged from 0 (no
itching/scratching) to 3 (bothersome itching/scratching that dis-
turbs sleep). Patients were evaluated at baseline and on days 8, 15,
22, 29, and 43.
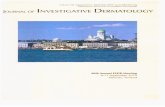
The infant is shown before and after 6 weeks' therapy using pimecrolimus 0.1% for moderate atopic dermatitis.Courtesy of Prof. Dr. Roland Kaufmann, JW Goethe University Medical School,
Frankfurt, Germany.
Novartis/PED/Derm2 1/17/03 5:36 PM Page 13
Atopic Dermatitis in the Pediatric Patient 13
The results seen in Figure 2 are typical of those seen in the
short-term pimecrolimus studies. This 7-month-old female had a
history of erythema and papulation on the face and neck and was
diagnosed with moderate atopic dermatitis. Her parents had been
applying emollients but were reluctant to use topical cortico-
steroids. The atopic dermatitis flares were causing sleep distur-
bance and distress to not only the infant but also the parents.
Twice-daily therapy with pimecrolimus was initiated to control
the atopic dermatitis and prevent exacerbations. Six weeks later,
the infant's skin was essentially cleared.
In the children’s study, a significantly higher proportion of
patients treated with pimecrolimus than those treated with vehi-
cle were clear or almost clear by IGA at every postbaseline visit
(P ≤0.05 for day 8 and 29 visits; P ≤0.001 for day 15, 22, and 43
visits). For the infants’ study, this was true beginning with the day
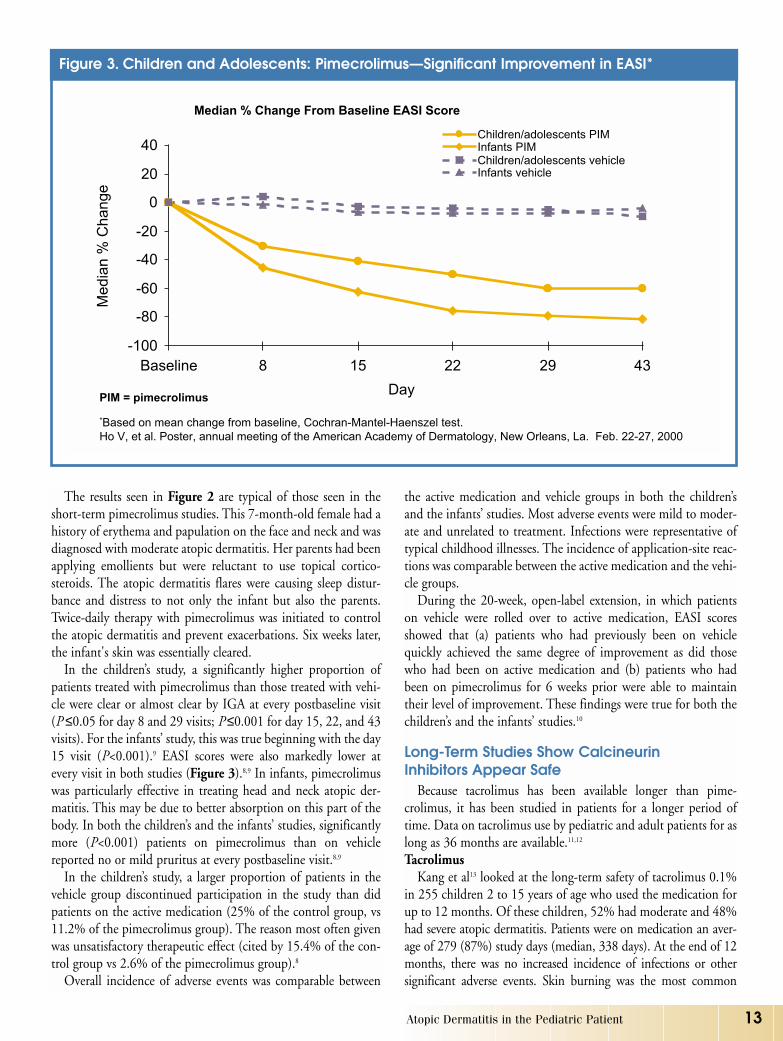
15 visit (P<0.001).9 EASI scores were also markedly lower at
every visit in both studies (Figure 3).8,9 In infants, pimecrolimus
was particularly effective in treating head and neck atopic der-
matitis. This may be due to better absorption on this part of the
body. In both the children’s and the infants’ studies, significantly
more (P<0.001) patients on pimecrolimus than on vehicle
reported no or mild pruritus at every postbaseline visit.8,9
In the children’s study, a larger proportion of patients in the
vehicle group discontinued participation in the study than did
patients on the active medication (25% of the control group, vs
11.2% of the pimecrolimus group). The reason most often given
was unsatisfactory therapeutic effect (cited by 15.4% of the con-
trol group vs 2.6% of the pimecrolimus group).8
Overall incidence of adverse events was comparable between
the active medication and vehicle groups in both the children’s
and the infants’ studies. Most adverse events were mild to moder-
ate and unrelated to treatment. Infections were representative of
typical childhood illnesses. The incidence of application-site reac-
tions was comparable between the active medication and the vehi-
cle groups.
During the 20-week, open-label extension, in which patients
on vehicle were rolled over to active medication, EASI scores
showed that (a) patients who had previously been on vehicle
quickly achieved the same degree of improvement as did those
who had been on active medication and (b) patients who had
been on pimecrolimus for 6 weeks prior were able to maintain
their level of improvement. These findings were true for both the
children’s and the infants’ studies.10
Long-Term Studies Show Calcineurin Inhibitors Appear Safe
Because tacrolimus has been available longer than pime-
crolimus, it has been studied in patients for a longer period of
time. Data on tacrolimus use by pediatric and adult patients for as
long as 36 months are available.11,12
Tacrolimus
Kang et al13 looked at the long-term safety of tacrolimus 0.1%
in 255 children 2 to 15 years of age who used the medication for
up to 12 months. Of these children, 52% had moderate and 48%
had severe atopic dermatitis. Patients were on medication an aver-
age of 279 (87%) study days (median, 338 days). At the end of 12
months, there was no increased incidence of infections or other
significant adverse events. Skin burning was the most common
Figure 3. Children and Adolescents: Pimecrolimus—Significant Improvement in EASI*
-100
-80
-60
-40
-20
0
20
40
Baseline 8 15 22 29 43
Children/adolescents PIMInfants PIMChildren/adolescents vehicleInfants vehicle
Median % Change From Baseline EASI Score
*Based on mean change from baseline, Cochran-Mantel-Haenszel test.Ho V, et al. Poster, annual meeting of the American Academy of Dermatology, New Orleans, La. Feb. 22-27, 2000
PIM = pimecrolimusDay
Med
ian
% C
hang
e
Novartis/PED/Derm2 1/9/03 5:59 PM Page 14

14 Atopic Dermatitis in the Pediatric Patient
application-site reaction (25.9%), followed by pruritus (23.1%).
These adverse events were highest on the first few days of treatment
and typically declined after days 5 to 8 in most patients. (It has
been this author’s experience that risk of skin burning can be less-
ened by instructing the family not to apply tacrolimus to the child
immediately after bathing.)
The Kang study also looked at several efficacy measures: EASI
score decreased from 19.7 at baseline to 5.7 at month 12, percent
of body surface area affected improved, and pruritus also
decreased.
Paller et al11 evaluated long-term safety of
tacrolimus in 389 pediatric patients in a
noncomparative, open-label extension
study of patients 2 to 15 years of age. Most
patients had moderate to severe atopic der-
matitis at baseline. Mean body surface area
affected was 33%. Patients applied the
0.1% tacrolimus ointment twice daily until
1 week after clearing, with instructions to
resume treatment if atopic dermatitis
recurred. After month 3, patients were eval-
uated at 3-month intervals. Of the 389
patients, 234 had been followed for 2 years and 56 patients for 3
years.
As with the Kang study, the most common drug-related
adverse event was skin burning (18%), followed by pruritus
(15%) and erythema (5%). These events typically were of short
duration and subsided after a few days’ treatment. Incidence of
infections from herpes simplex virus (HSV) was 1.8% in the first
6 months of the study; no cases of HSV infection were reported
in months 25 to 30 (representing 131 patients). The authors
indicated that this rate was comparable to that seen in pediatric
patients with atopic dermatitis.
In a similarly designed safety study of 407 patients 16 years of
age or older, tacrolimus was found to be safe after up to 3 years
of use.12 Most patients had moderate to severe atopic dermatitis
at baseline. Nearly half of the patients were followed for at least
2 years. Skin burning, pruritus, and erythema were the most
common application-site events. The authors concluded that
long-term tacrolimus use did not increase risk of any adverse
event, including the risk associated with concurrent illnesses.
Pimecrolimus
Three long-term studies of pimecrolimus have compared the
agent’s efficacy and safety to that of conventional therapy.14,15,16
Two were 1-year studies of pediatric patients and one was a
6-month study of adults.
All three studies were similar in design: Patients were random-
ized into two groups. Both groups were instructed to apply
emollients to dry skin. At the first sign of early atopic dermatitis
symptoms, patients applied either pimecrolimus or, if they were
in the conventional therapy group, vehicle to the affected areas.
If flares occurred, patients in both groups were given moderately
potent corticosteroids to apply. All severities of atopic dermatitis,
from mild to very severe, were allowed.
In a study of 251 infants 3 to 23 months of age, pimecrolimus
significantly reduced (P<0.001) the incidence of flares compared
with the conventional therapy regimen.14 Overall corticosteroid
use was substantially lower in the pimecrolimus group; 64% used
no corticosteroids during the 12-month period, vs only 35% of
the control group. Results of a study of 713 patients 2 to 17 years
of age were similar; 57% of the pimecrolimus group did not use
any topical corticosteroid therapy, vs only 32% of the conven-
tional therapy group after 12 months.15 EASI scores in both
pediatric studies demonstrate that pime-
crolimus could maintain disease control for
1 year.15
The adult study of 192 patients 18 to 68
years of age lasted only 6 months, but
results mirrored those of the pediatric stud-
ies; pimecrolimus was found to be topical
corticosteroid–sparing. The adult study
also looked at quality of life as a secondary
efficacy indicator. Pimecrolimus was found
to significantly improve (P<0.05) quality of
life, compared with conventional therapy.16
Overall incidence of adverse effects was
comparable between the pimecrolimus and conventional therapy
groups in all three long-term studies. In the pediatric studies,
most adverse events were mild or moderate and representative of
typical childhood illnesses or atopic diseases. Application-site
reactions were low in both those who received active medication
and those who used the vehicle. There were no significant differ-
ences between the two groups.
In the children’s study by Wahn et al15, a skin-recall antigen test
was performed at the end of 12 months to see if pimecrolimus
impaired immune response to common antigens. There were no
significant differences between the two treatment groups, however.
In summary, safety and efficacy conclusions that can be
reached from clinical trials are that pimecrolimus:
• Significantly reduced signs and symptoms of eczema.
• Significantly reduced pruritus, perhaps the most vexing
symptom for patients.
• Reduced the number of flares and the need for cortico-
steroids, when used at the earliest onset of signs and
symptoms of atopic dermatitis.
• Was effective in a broad population of patients by age and
disease severity.
• Was safe for at least 1 year.
• Was safe for use over a large percentage of body surface area.
• Was safe for use on face, neck, and skinfolds, where potent
corticosteroids are contraindicated.
• Exhibited no contact sensitization, phototoxicity, photo-
allergy, or cumulative irritation.
• Showed low systemic absorption regardless of patient age,
disease extent or severity, or treatment duration.
ConclusionHave topical immunomodulators changed pediatricians’ abili-
“Overall incidence of adverse effectswas comparable
between the pimecrolimus and
conventional therapygroups in all threelong-term studies.”
Novartis/PED/Derm2 1/17/03 5:38 PM Page 15

Atopic Dermatitis in the Pediatric Patient 15
ty to treat atopic dermatitis? It is the opinion of this author that
they have. These agents have been shown to be selective for the
aberrant immunologic activities that initiate and sustain atopic
dermatitis. Early treatment at the initial signs and symptoms of
atopic dermatitis improves disease control. The pimecrolimus
research, in particular, which pitted an immunomodulator
against conventional therapy, suggests that treatment should per-
haps evolve in the way management of asthma has—by starting
antiinflammatory treatment early, rather than as reactive, crisis-
based therapy, and by developing disease severity-based algo-
rithms with an emphasis on asymptomatic/disease-free periods.
References1. Meingassner JG, Di Padova F, Hiestand P, et al. Pimecrolimus (SDZ
ASM 981): Highly effective in models of skin inflammation but low
activity in models of immunosuppression. Poster presented at the
60th Annual Meeting of the American Academy of Dermatology;
February 22-27, 2002; New Orleans, La.
2. Bilich A, Aschauer H, Stuetz A. Pimecrolimus (SDZ ASM 981) is
more lipophilic and permeates less through skin than tacrolimus (FK
506). Poster presented at the 20th World Congress of Dermatology;
July 1-5, 2002; Paris, France.
3. Data on file, Novartis Pharmaceuticals Corp., East Hanover, N.J.
4. Data on file, Novartis Pharmaceuticals Corp., East Hanover, N.J.
5. Paller A, Eichenfield LF, Leung DYM, Stewart D, Appell M. A 12-
week study of tacrolimus ointment for the treatment of atopic der-
matitis in pediatric patients. J Am Acad Dermatol. 2001;44:S47-S57.
6. Hanifin JM, Ling MR, Langley R, Breneman, Rafal E. Tacrolimus
ointment for the treatment of atopic dermatitis in adult patients: Part
I, efficacy. J Am Acad Dermatol. 2001;44:S28-S38.
7. Boguniewicz M, Fiedler VC, Ramer S, et al. A randomized, vehicle-
controlled trial of tacrolimus ointment for treatment of atopic der-
matitis in children. J Allergy Clin Immunol. 1998;102:637-644.
8. Eichenfield LF, Lucky AW, Boguniewicz M, et al. Safety and effica-
cy of pimecrolimus (ASM 981) cream 1% in the treatment of mild
and moderate atopic dermatitis in children and adolescents. J Am
Acad Dermatol. 2002;46:495-504.
9. Ho V, Papp K, Halbert A, et al. Pimecrolimus (ASM 981) cream is
effective and safe in infants aged 3-23 months with atopic dermati-
tis. Poster presented at the 60th Annual Meeting of the American
Academy of Dermatology; February 22-27, 2002; New Orleans,
La.
10. Ling M, Boguniewicz M, Eichenfield LF, et al. Pimecrolimus (ASM
981) cream is safe in the long-term control of atopic dermatitis.
Poster presented at the 60th Annual Meeting of the American
Academy of Dermatology; February 22-27, 2002; New Orleans, La.
11. Paller AS, Hanifin J, Eichenfield L, Rico MJ, Ayers M. Long-term
safety of topically applied tacrolimus ointment in pediatric patients
2-15 years of age with atopic dermatitis. Poster presented at the
60th Annual Meeting of the American Academy of Dermatology;
February 22-27, 2002; New Orleans, La.
12. Caro I, Gordon KB, West DP, et al. Long-term safety of topically
applied tacrolimus ointment in adult patients with atopic dermati-
tis. Poster presented at the 60th Annual Meeting of the American
Academy of Dermatology; February 22-27, 2002; New Orleans,
La.
13. Kang S, Lucky AW, Pariser D, Lawrence I, Hanifin JM. Long-term
safety and efficacy of tacrolimus ointment for the treatment of
atopic dermatitis in children. J Am Acad Dermatol. 2001;44:S58-
S64.
14. Kapp A, Papp K, Bingham A, et al. Long-term management of atopic
dermatitis in infants with topical pimecrolimus, a nonsteroid anti-
inflammatory drug. J Allergy Clin Immunol. 2002;110:277-284.
15. Wahn U, Bos JD, Goodfield M, et al. Efficacy and safety of pime-
crolimus cream in the long-term management of atopic dermatitis
in children. Pediatrics. 2002;110(1 pt 1):e2.
16. Meurer M, Fölster-Holst R, Bräutigam M. Pimecrolimus (ASM
981) cream improves disease control and quality of life in the long-
term management of atopic dermatitis in adults. Poster presented at
the 20th World Congress of Dermatology; July 1-5, 2002; Paris,
France.
characterized by severe pruritus and morphologic features (ery-
thema, papulation, excoriation, and lichenification) that make
clinical diagnosis possible. Formal diagnostic criteria exist to
aid the clinician, but generally the diagnosis is made readily
by simple examination and history. The physician should
recognize that the disease presents differently in an infant
or child than it does in an adolescent or adult. Morphologic
features, disease duration and distribution, family history,
and other factors can be used to distinguish atopic dermatitis
from other dermatoses, including seborrheic dermatitis,
allergic contact dermatitis, scabies, and psoriasis.
CLINICAL PRESENTATIONContinued from page 6.
References1. Sicherer SH, Sampson HA. Food hypersensitivity and atopic der-
matitis: Pathophysiology, epidemiology, diagnosis, and management.J Allergy Clin Immunol. 1991;104:S114-S122.
2. Hurwitz S. Clinical Pediatric Dermatology. Philadelpha, Pa: WBSaunders Co; 1981:44-45.
3. Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. ActaDerm Venereol (Stockh). 1980;92(suppl):44-47.
4. Hanifin JM. Immunologic aspects of atopic dermatitis. DermatolClin. 1990;8:747-750.
5. Shin HT, Chang MW. Drug eruptions in children. Curr Probl Pediatr.2001;31:207-234.
Novartis/PED/Derm2 1/9/03 6:00 PM Page 16
Instructions for CME credit.This self-assessment examination gives you the opportunity to assess your understanding and retention of information presented in this publication. To earn 2 hours of
American Medical Association category 1 credit, complete the application for CME credit, the post-test, and the evaluation. You must score at least 70% to receive credit.
Mail or fax a photocopy of the completed form to: Medical Education Collaborative • 651 Corporate Circle, Suite 104 • Golden • CO 80401 • Fax: 303-420-3259.
A certificate of course completion will be mailed to you. There is no fee to participate in this activity.
Pediatric News®
ATOPIC DERMATITIS IN THE PEDIATRIC PATIENT: PATHOPHYSIOLOGY, PRESENTATION, AND AN UPDATE ON NOVEL THERAPIES
CME Post-Test and Evaluation
Copyright 2003 International Medical News Group, an Elsevier Science company
INSTRUCTIONS: For each question or incomplete statement, one answer is correct. Check the most appropriate response. Seven out of ten correct responses are required for credit.
Name Degree
Address Email
City State ZIP
Phone Fax
PROGRAM EVALUATION1. How many hours did you actually spend completing this activity?
0.5 to 1 hour 1 to 1.5 hours 1.5 to 2 hours 2 to 2.5 hours
2. Rate how well the activity achieved the learning objectives listed on page 3.
Poor Good Excellent
3. Rate the relevance of the activity’s content to its objectives.
Poor Good Excellent
4. Rate the faculty’s effectiveness in communicating the material.
Poor Good Excellent
5. Rate the information about diagnosis and treatment of atopic dermatitis in pediatric
patients.
Poor Good Excellent
6. This supplement was commercially supported. Did you perceive any bias?
Yes No
If yes, please explain.
7. How would you rate the content? (Circle the letter of the most appropriate answer.)
a. Will definitely change the way I practice
b. Challenged me to think about the topics
c. Applicable to my practice—a good review
d. Of limited use in my practice
e. Not applicable to my practice
8. What other CME topics would be of value to you? Please offer additional comments.
1. Approximately ____ of all cases of atopic dermatitis are diagnosed by 5years of age.a. 60% c. 80%b. 70% d. 90%
2. Which of the following statements about atopic dermatitis is true?a. Atopic dermatitis can cause failure to thrive.b. Atopic dermatitis remits in a minority of children by the time they
reach puberty.c. T-helper type 2 cells are associated with chronic atopic dermatitis.d. Because Staphylococcus aureus is so prevalent in atopic dermatitis lesions,
antibiotics should be used only in cases of overt infection.
3. Which of the following side effects is not associated with corticosteroid use?a. Telangiectasiab. Glaucomac. Skin atrophyd. Rapidly increasing response to the medication after several weeks’ use
4. Which of the following is not an effective treatment for atopic dermatitis?a. Oral antihistamines c. Topical immunomodulatorsb. Topical antihistamines d. Avoidance of known triggers
5. Which of the following morphologic features is not commonly associated with atopic dermatitis?a. Erythema c. Excoriationb. Hemorrhagic erosions d. Lichenification
6. Pruritus and papulation accompanied by small linear burrows and noduleson the wrists, ankles, and finger webs in an older child are likely signs of:a. Nummular dermatitis. c. Eczema herpeticum.b. Molluscum contagiosum. d. Scabies.
7. Young infants are more likely than older children to have atopic dermati-tis:a. On the hands. b. In the diaper region.c. On the cheeks.d. None of the above.
8. Which of the following statements comparing tacrolimus and pimecrolimus is true?a. In immunosuppression models, pimecrolimus has been found to have
a higher potential for affecting systemic immune responses.b. Tacrolimus is more lipophilic than pimecrolimus.c. Pimecrolimus was equal or superior to tacrolimus in skin
inflammation models.d. All of the above statements are true.
9. Which statement is accurate regarding the findings of the two short-term pimecrolimus efficacy trials in infants and children?a. A significantly higher proportion of patients treated with
pimecrolimus than vehicle were rated clear or almost clear byInvestigator Global Assessment at the day 15 visit.
b. Pruritus relief was not seen in most patients on active medication untilthe day 29 visit.
c. Patients on pimecrolimus had significantly more application-site reac-tions than did patients on vehicle.
d. The 20-week extension phase of the trials showed that tachyphylaxis may be an issue with pimecrolimus after week 14.
10. Long-term safety trials that measured the effectiveness of pimecrolimus vs that of conventional therapy found pimecrolimus: a. To be topical corticosteroid-sparing.b. Could maintain disease control for up to 1 year.c. Did not impair immune response to common antigens.d. All of the above are true.
A
Novartis/PED/Derm2 1/17/03 5:31 PM Page 1