Pediatric Endoscopic Airway Management With Posterior ...€¦ · Pediatric Endoscopic Airway...
5
The Laryngoscope V C 2011 The American Laryngological, Rhinological and Otological Society, Inc. Pediatric Endoscopic Airway Management With Posterior Cricoid Rib Grafting Matthew J. Provenzano, MD; Stephanie L. Hulstein, BA; Donald H. Solomon, MD; Nancy M. Bauman, MD; Jose M. Manaligod, MD; Deborah S. F. Kacmarynski, MD; Richard J. H. Smith, MD Objectives/Hypothesis: To confirm and extend reported successful treatment of posterior glottic stenosis in pediatric patients using endoscopic laser division of the posterior cricoid plate with augmentation using costal cartilage. Study Design: A retrospective chart review and case series. Methods: Medical records were examined to determine the surgical indications, outcomes, and postoperative complica- tions of this procedure. Results: Twelve patients underwent the procedure, six females and six males, with an average age of 7 years (range, 2–26 years). There were 8/12 (67%) patients successfully decannulated after being tracheostomy dependent. There were no consistent anatomic abnormalities or surgical findings predictive of failure to decannulate. Average hospital stay was 3.6 days (range, 2–9 days). There were no deaths or other major complications; one patient had extrusion. Conclusions: Endoscopic posterior cricoid grafting is a valuable surgical option for patients with posterior glottic steno- sis. The procedure is associated with low morbidity and permits decannulation in the majority of patients. Key Words: posterior glottic expansion, costal cartilage, posterior glottic stenosis. Level of Evidence: 4. Laryngoscope, 121:1062–1066, 2011 INTRODUCTION The primary goal of pediatric airway surgery is to pro- vide the young patient with an airway that allows for tracheotomy-free respiration, appropriate phonation, and normal swallowing. Treatment for glottic and subglottic ste- nosis has traditionally involved open procedures such as anterior or posterior cricoid expansion. Although these pro- cedures have high rates of decannulation, the patients often have significant postoperative morbidity. Postoperative vocal cord malposition resulting from the laryngofissure necessary to access the posterior cricoid can leave the patient with phonation difficulties. There is now emerging evidence demonstrating phonation changes in pediatric patients who have undergone open airway reconstruction. 1 Open procedures also leave external scaring and likely have longer hospitalizations compared to endoscopic alternatives. We have encountered a number of these postopera- tive difficulties in our experience with open airway procedures in children. Determining the correct vocal cord position after laryngofissure is often difficult and results in unpredictable voice outcomes. Some patients have significant hospital length of stays, including initial observation in the intensive care unit. 2 Given the postoperative morbidity of open proce- dures, innovative surgical procedures have been developed. In 2003, Inglis and colleagues introduced laser-assisted, endoscopic posterior cricoid expansion for patients with bilateral vocal cord paralysis and posterior glottic-subglottic stenosis. 3 Their work showed that the procedure carried minimum morbidity while allowing for decannulation and improved speech and swallowing. 3 The technique, which built on a procedure introduced by Gray et al. in 1994, 4 has now been cited in a case series including the treatment of a 3-week-old neonate. 5 In this study, we present the largest series of patients who have undergone laser-assisted, endoscopic posterior cricoid expansion with chondral cartilage. The decannulation rate was high, with minimal intensive care unit time. Postoperative phonation and deglutition were excellent. Results were consistent across all airway abnormalities, confirming the Inglis study and demon- strating the utility of this procedure in the treatment of pediatric airway abnormalities. MATERIALS AND METHODS After institutional review board approval, the medical charts of patients undergoing endoscopic posterior cricoid graft- ing from 2003 to 2010 were examined. Patient demographics, procedure information, and outcomes as presented in the Results section were collected and analyzed with Microsoft Excel (Microsoft Corp., Redmond, WA). From the Departmentof Otolaryngology–Head and Neck Surgery (M.J.P ., S.L.H., D.H.S., J.M.M., D.S.F .K., R.J.H.S.), University of Iowa, Hospital and Clinic, Iowa City, Iowa; and the Department of Otolaryngology (N.M.B.), Children’s National Medical Center, Washington, District of Columbia, U.S.A. Editor’s Note: This Manuscript was accepted for publication December 7, 2010. The authors have no funding, financial relationships, or conflicts of interest to disclose. Send correspondence to Richard J. H. Smith, MD, Department of Otolaryngology–Head and Neck Surgery, University of Iowa Hospitals and Clinics, 200 Hawkins Drive, Iowa City, IA 52242. E-mail: [email protected] DOI: 10.1002/lary.21579 Laryngoscope 121: May 2011 Provenzano et al.: Endoscopic Posterior Cricoid Grafting 1062
Transcript of Pediatric Endoscopic Airway Management With Posterior ...€¦ · Pediatric Endoscopic Airway...
The LaryngoscopeVC 2011 The American Laryngological,Rhinological and Otological Society, Inc.
Pediatric Endoscopic Airway Management With PosteriorCricoid Rib Grafting
Matthew J. Provenzano, MD; Stephanie L. Hulstein, BA; Donald H. Solomon, MD; Nancy M. Bauman, MD;
Jose M. Manaligod, MD; Deborah S. F. Kacmarynski, MD; Richard J. H. Smith, MD
Objectives/Hypothesis: To confirm and extend reported successful treatment of posterior glottic stenosis in pediatricpatients using endoscopic laser division of the posterior cricoid plate with augmentation using costal cartilage.
Study Design: A retrospective chart review and case series.Methods: Medical records were examined to determine the surgical indications, outcomes, and postoperative complica-
tions of this procedure.Results: Twelve patients underwent the procedure, six females and six males, with an average age of 7 years (range,
2–26 years). There were 8/12 (67%) patients successfully decannulated after being tracheostomy dependent. There were noconsistent anatomic abnormalities or surgical findings predictive of failure to decannulate. Average hospital stay was 3.6 days(range, 2–9 days). There were no deaths or other major complications; one patient had extrusion.
Conclusions: Endoscopic posterior cricoid grafting is a valuable surgical option for patients with posterior glottic steno-sis. The procedure is associated with low morbidity and permits decannulation in the majority of patients.
Key Words: posterior glottic expansion, costal cartilage, posterior glottic stenosis.Level of Evidence: 4.
Laryngoscope, 121:1062–1066, 2011
INTRODUCTIONThe primary goal of pediatric airway surgery is to pro-
vide the young patient with an airway that allows fortracheotomy-free respiration, appropriate phonation, andnormal swallowing. Treatment for glottic and subglottic ste-nosis has traditionally involved open procedures such asanterior or posterior cricoid expansion. Although these pro-cedures have high rates of decannulation, the patients oftenhave significant postoperative morbidity. Postoperativevocal cord malposition resulting from the laryngofissurenecessary to access the posterior cricoid can leave thepatient with phonation difficulties. There is now emergingevidence demonstrating phonation changes in pediatricpatients who have undergone open airway reconstruction.1
Open procedures also leave external scaring and likely havelonger hospitalizations compared to endoscopic alternatives.
We have encountered a number of these postopera-tive difficulties in our experience with open airwayprocedures in children. Determining the correct vocal
cord position after laryngofissure is often difficult andresults in unpredictable voice outcomes. Some patientshave significant hospital length of stays, including initialobservation in the intensive care unit.2
Given the postoperative morbidity of open proce-dures, innovative surgical procedures have beendeveloped. In 2003, Inglis and colleagues introducedlaser-assisted, endoscopic posterior cricoid expansion forpatients with bilateral vocal cord paralysis and posteriorglottic-subglottic stenosis.3 Their work showed that theprocedure carried minimum morbidity while allowing fordecannulation and improved speech and swallowing.3
The technique, which built on a procedure introduced byGray et al. in 1994,4 has now been cited in a case seriesincluding the treatment of a 3-week-old neonate.5
In this study, we present the largest series ofpatients who have undergone laser-assisted, endoscopicposterior cricoid expansion with chondral cartilage. Thedecannulation rate was high, with minimal intensivecare unit time. Postoperative phonation and deglutitionwere excellent. Results were consistent across all airwayabnormalities, confirming the Inglis study and demon-strating the utility of this procedure in the treatment ofpediatric airway abnormalities.
MATERIALS AND METHODSAfter institutional review board approval, the medical
charts of patients undergoing endoscopic posterior cricoid graft-ing from 2003 to 2010 were examined. Patient demographics,procedure information, and outcomes as presented in theResults section were collected and analyzed with MicrosoftExcel (Microsoft Corp., Redmond, WA).
From the Departmentof Otolaryngology–Head and Neck Surgery(M.J.P., S.L.H., D.H.S., J.M.M., D.S.F.K., R.J.H.S.), University of Iowa, Hospitaland Clinic, Iowa City, Iowa; and the Department of Otolaryngology(N.M.B.), Children’s National Medical Center, Washington, District ofColumbia, U.S.A.
Editor’s Note: This Manuscript was accepted for publicationDecember 7, 2010.
The authors have no funding, financial relationships, or conflictsof interest to disclose.
Send correspondence to Richard J. H. Smith, MD, Department ofOtolaryngology–Head and Neck Surgery, University of Iowa Hospitalsand Clinics, 200 Hawkins Drive, Iowa City, IA 52242.E-mail: [email protected]
DOI: 10.1002/lary.21579
Laryngoscope 121: May 2011 Provenzano et al.: Endoscopic Posterior Cricoid Grafting
1062

Our technique followed the procedure as described by Ingliset al.,3 with some modifications. In brief, the diagnosis of poste-rior glottic stenosis or vocal cord paralysis/fixation is confirmedby a functional evaluation of the larynx in the clinic and operat-ing room. On the day of endoscopic posterior cricoid expansion, atracheotomy is performed if not already present. Autologous ribharvest is the preferred grafting material, although on occasion,we use cadaveric cartilage. Both options work without difficultyand provide sufficient material for carving multiple grafts.
To harvest costal cartilage, a 3-cm incision is made medialto the synchondrosis approximately one finger breadth above andparallel to the inferior margin of the rib cage. The soft tissues areretracted to expose the underlying cartilage, which is markedand harvested with its external perichondrium. Elevating the in-ternal perichondrium from the cartilage as the graft is harvestedminimizes the possibility of a pneumothorax. After taking therequired amount of cartilage, the wound is irrigated under posi-tive pressure to confirm the absence of a pneumothorax and thenclosed, carefully approximating the muscle fascia to minimizepostoperative pain. At the conclusion of the entire procedure,local anesthetic is infiltrated around the incision.
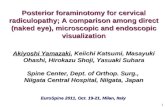
The patient is then placed in suspension using a Lindholmlaryngoscope. Draping with moistened towels and minimizingthe FiO2 are standard laser precautions used in all laser proce-dures at our institution. To optimize access to the pediatriclarynx, we have customized a number of instruments for use inthis procedure. We use a modified laryngeal spreader to visual-ize the entire depth of the cricoid (Fig. 1). The intra-arytenoidmusculature is pushed posteriorly with the modified spatula,thereby exposing the superior aspect of the cricoid. The CO2
laser is used to divide the overlying mucosa and the cricoid car-tilage, working slowly from superior to inferior to divide the
Fig. 1. A number of instruments were modified for use in pediatricendoscopic airway procedures. The smaller retractors allow forgreater access for the laser and other instruments. (A) Viewed fromabove, the adult and laryngeal spreaders have the same profile. Theadult spreaders are on the right. (B) The adult spreaders are on arebottom and the modified pediatric spreaders on top. The length ofthe spreader blades measures approximately 1 cm in both. (C) Thepediatric spreader is on top. The blade height measures approxi-mately 3 mm. The blade on the adult spreader (bottom) measuresapproximately 5 mm in height. [Color figure can be viewed in theonline issue, which is available at wileyonlinelibrary.com.]
Fig. 2. The modified pediatric spatula is smaller than its adult coun-terpart and aids in distraction of the cricoid and placement of thecartilage graft. (A) The two spatulas have the same length. (B) Thelength of the working end of the two spatulas is approximately thesame (3 cm). (C) The pediatric spatula (left) has a height of 3 mm,whereas the height of the adult spatula (right) is 5 mm. [Color figurecan be viewed in the online issue, which is available atwileyonlinelibrary.com.]
Laryngoscope 121: May 2011 Provenzano et al.: Endoscopic Posterior Cricoid Grafting
1063
cricoid plate. Progress is assessed by palpation using the modi-fied pediatric spatula. Once the superior/posterior aspect of thecartilage is divided, a laser platform can be used to protect theesophageal mucosa. We also use a right-angle hook on the supe-rior aspect of the cricoid to rotate the cricoid plate and providebetter exposure for the laser.
Once the cricoid plate is divided, the pediatric spatula isused to distract the halves (Fig. 2). The costal cartilage is thencarved. Prior to placement, a safety suture is placed throughthe graft to aid in its retrieval if repeated attempts at place-ment are required. Depending on the size of the harvestedcartilage, I-beam or keystone shapes can be fashioned, althoughwe prefer the I-beam shape because it firmly locks in position.The pediatric spatula is used to push the graft into place, a ma-
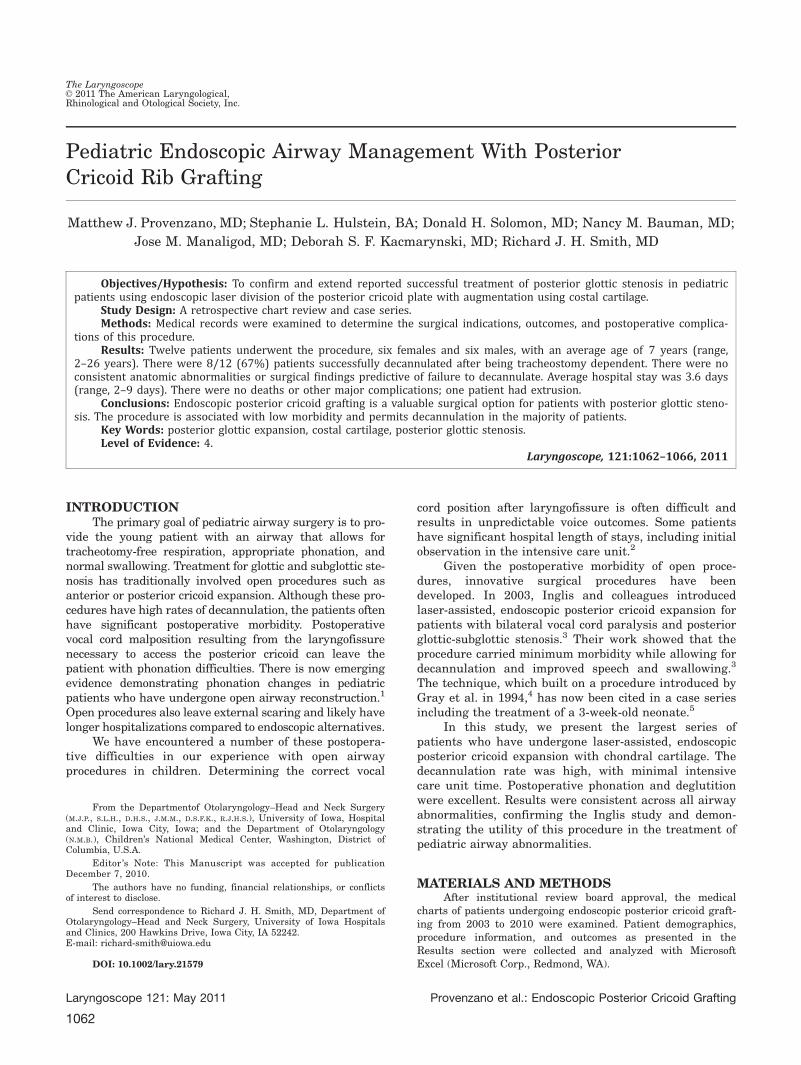
neuver that often takes considerable force. The safety suture isthen cut and photographs are taken (Fig. 3).
Postoperatively, the majority of patients are observed inthe pediatric intensive care unit. Decannulation is performed ata subsequent procedure after a corking trial with a fenestratedtracheostomy tube.
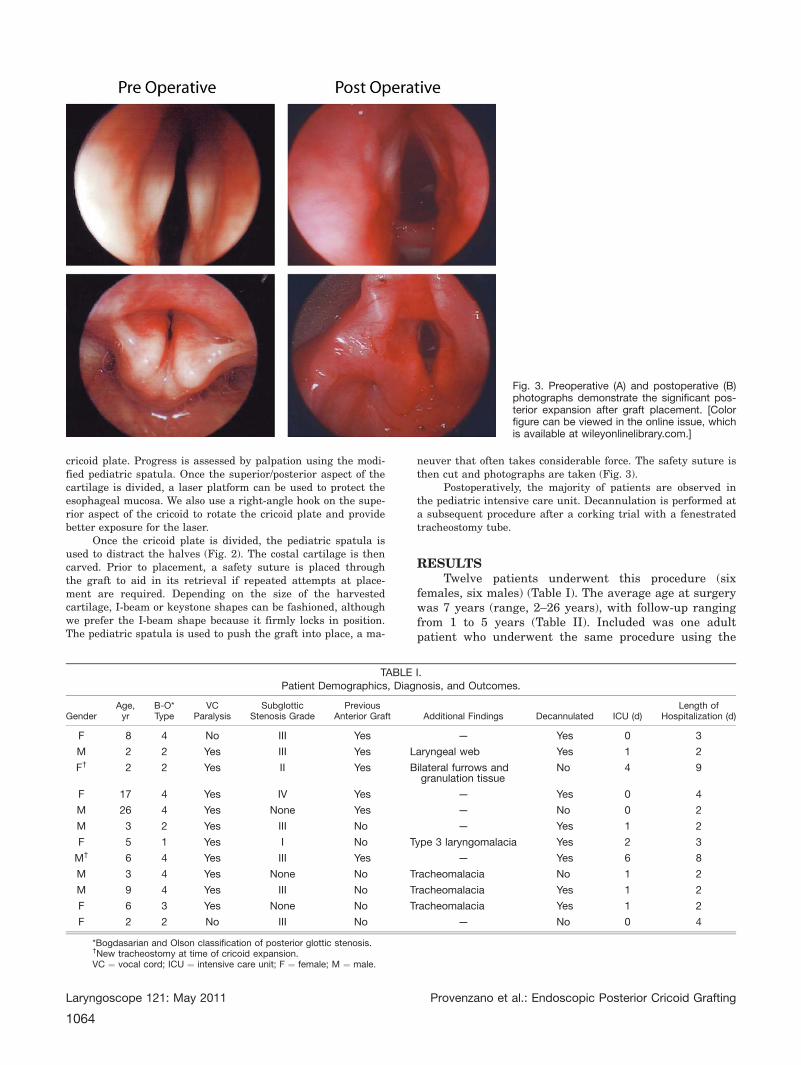
RESULTSTwelve patients underwent this procedure (six
females, six males) (Table I). The average age at surgerywas 7 years (range, 2–26 years), with follow-up rangingfrom 1 to 5 years (Table II). Included was one adultpatient who underwent the same procedure using the
Fig. 3. Preoperative (A) and postoperative (B)photographs demonstrate the significant pos-terior expansion after graft placement. [Colorfigure can be viewed in the online issue, whichis available at wileyonlinelibrary.com.]
TABLE I.Patient Demographics, Diagnosis, and Outcomes.
GenderAge,yr
B-O*Type
VCParalysis
SubglotticStenosis Grade
PreviousAnterior Graft Additional Findings Decannulated ICU (d)
Length ofHospitalization (d)
F 8 4 No III Yes — Yes 0 3
M 2 2 Yes III Yes Laryngeal web Yes 1 2
F† 2 2 Yes II Yes Bilateral furrows andgranulation tissue
No 4 9
F 17 4 Yes IV Yes — Yes 0 4
M 26 4 Yes None Yes — No 0 2
M 3 2 Yes III No — Yes 1 2
F 5 1 Yes I No Type 3 laryngomalacia Yes 2 3
M† 6 4 Yes III Yes — Yes 6 8
M 3 4 Yes None No Tracheomalacia No 1 2
M 9 4 Yes III No Tracheomalacia Yes 1 2
F 6 3 Yes None No Tracheomalacia Yes 1 2
F 2 2 No III No — No 0 4
*Bogdasarian and Olson classification of posterior glottic stenosis.†New tracheostomy at time of cricoid expansion.VC ¼ vocal cord; ICU ¼ intensive care unit; F ¼ female; M ¼ male.
Laryngoscope 121: May 2011 Provenzano et al.: Endoscopic Posterior Cricoid Grafting
1064

same technique as in the pediatric patients. Mostpatients had multiple upper airway abnormalities.
Ten patients had a pre-existing tracheostomy, andin the remaining two patients, a tracheostomy wasplaced in conjunction with the procedure. Eight patients(67%) were successfully decannulated. One half ofpatients had type 4 Bogdasarian-Olson posterior glotticstenosis.6 Three of the patients yet to be decannulatedhave bilateral vocal cord paralysis and varying degreesof posterior glottic stenosis. Repeat direct laryngoscopicevaluation of their airways has confirmed posterior cri-coid expansion, and decannulation is planned. Onepatient who has not undergone decannulation had arecent posterior graft. Decannulation is expected. Nonehas yet undergone a corking trial with a fenestrated tra-cheotomy tube, which is our practice prior todecannulation.7 One patient who was decannulated sub-sequently developed additional scar tissue distal to theposterior graft site and required a second tracheostomy.A number of patients also had open anterior laryngotra-cheal reconstruction prior to endoscopic cricoidexpansion. Six patients had balloon dilations prior toposterior cricoid expansion (average number, 6.2; range,1–19).
Hospitalization after graft placement averaged 3.6days (range, 2–9 days) including eight patients observedin the intensive care unit for an average of 2 days(range, 1–6 days). Excluding the two patients whounderwent tracheostomy in conjunction with grafting,the average hospitalization was 2.6 days (range, 2–4days), with 1 day in the intensive care unit (Table II).The first patient to undergo this procedure had extru-sion of the graft 7 days after the procedure andsubsequently underwent a repeat procedure. There wereno deaths or major complications from the procedure.
DISCUSSIONAs described by Inglis and colleagues, endoscopic
posterior cricoid expansion offers a number of advan-tages over an open procedure. Most importantly, itobviates the need for an anterior laryngofissure and theassociated potential morbidities of true vocal cord mal-
alignment, anterior glottic webbing, and an anteriorcervical scar. Our series of 12 patients is the largest yetpublished and confirms and extends previous findings.Included in our series are an adult (age 26 years) andan older pediatric patient. Inclusion of these twopatients demonstrates the applicability of this techniqueto a wide patient population. This series, together withthe reports of Inglis and Thakkar, provides data on 24patients.
Our experience has shown the procedure to be safeand associated with few complications. Although initiallyconcerned about potential donor site morbidity, esopha-geal injury, changes to speech and swallowing, orinfection, we encountered no major or minor complica-tions aside from graft extrusion after the first procedure.Postoperative flexible and direct laryngoscopy demon-strated rapid graft mucosalization. Our experiencecompares favorably to open procedures that havereported complications including dysphonia and aryte-noid prolapse.8
Initially, we used adult laryngeal instruments, butthe size of these instruments limited access, visualiza-tion, and manipulation of the cricoid cartilage. We nowuse modified instruments including a smaller laryngealspreader (Fig. 1A and 1B). The reduced profile of the pe-diatric laryngeal spreader increases visualization andminimizes trauma to surrounding tissue. Rotation of thecricoid cartilage is facilitated with a right angle hook.The pediatric spatula aids in distraction of the cricoidhalves, a step we found difficult with the adult-sizedinstruments. Our modified instruments have the requi-site strength to manipulate the cricoid cartilage and toplace the graft into position with greater ease.
Two patients received a posterior graft fashionedfrom cadaveric cartilage for confounding medical rea-sons. Although our experience is limited, carving,placement, and postoperative outcomes appear to be nodifferent when comparing patients with cadaveric andautologous grafts. Nevertheless, based on our long-termexperience with anterior costal grafting to expand thetrachea and subglottis, we believe that autologous carti-lage is preferable.
A tracheostomy was present in 10 of 12 patientsprior to the procedure, with the remaining two under-going tracheostomy during graft placement. Eight (67%)patients have been decannulated; the four remainingpatients are expected to be decannulated after a corkingtrial using a fenestrated tracheostomy tube. This resultis comparable to that reported by Inglis and colleagues,who decannulated five of seven patients (71%) in theirseries. Similar to our experience, the remaining patientsin their series demonstrate an improved airway. Takentogether, 13 of 19 (68%) patients have been decannulatedafter posterior cricoid expansion. This decannulationrate is lower than the 97% reported in some open proce-dure series; however, we anticipate that all of ourpatients will eventually be decannulated.8 A longer fol-low-up period will allow for accurate comparisonbetween open and endoscopic decannulation rates.
One patient in our series was successfully decannu-lated but later developed stenosis distal to the posterior
TABLE II.Outcomes Data.
Average 6 SD (Range)
Gender (M/F), % 50/50
Age, yr 7 6 7 (2–26)
Follow-up, mo 36 6 25 (2–80)
Decannulation rate (n¼8), % 67
Length of ICU stay, d
Including new tracheostomies 2.1 6 1.9 (1–6)
Excluding new tracheostomies 1.2 6 0.6 (1–2)
Length of hospitalization, d
Including new tracheostomies 3.6 6 2.4 (2–9)
Excluding new tracheostomies 2.6 6 0.8 (2–4)
SD ¼ standard deviation; M ¼ male; F ¼ female; ICU ¼ intensive care unit.
Laryngoscope 121: May 2011 Provenzano et al.: Endoscopic Posterior Cricoid Grafting
1065

cricoid graft site and required a second tracheotomy.This patient had a subsequent distal airway expansionprocedure and has now been decannulated for a secondtime. Our practice of requiring a tracheotomy for endo-scopic posterior cricoid grafting is in contrast to bothInglis and Thakkar, who have performed posterior cri-coid expansion in patients without a tracheostomy.Thakkar and Gerber report expansion in a 3-week-oldinfant who weighed 3.4 kg at birth. We believe that cri-coid expansion without tracheostomy should be reservedfor select patients without additional airway abnormal-ities and after gaining experience with this procedure.
Inglis and colleagues have commented on the diffi-culty of decannulating patients with high grade III andgrade IV subglottic stenosis. Only one of our patientshad a grade IV stenosis, whereas six had a grade III ste-nosis. We did not find that grade III or IV stenosisprecludes successful decannulation. Our single grade IVstenosis was in a 17-year-old female who required a pos-terior cricoid graft and additional anterior airwayprocedures prior to decannulation. This patient illus-trates the importance of using posterior cricoidexpansion as a technique to address a specific portion ofthe airway. It should be used in conjunction with addi-tional airway procedures focused on the other airwayabnormalities that are frequently present in thesepatients.
Neither the severity of the posterior glottic pathol-ogy as graded using the Bogdasarian-Olson classificationnor the dynamic status of the vocal folds (paralyzed ornot paralyzed) correlated with decannulation outcome,although the number of patients in all series is too smallfor statistical analysis. We documented no phonation orswallowing difficulties, with some parents reportingimproved phonation in their children. Inglis and col-
leagues also reported that many patients had improvedphonation, feeding, and exercise tolerance. Future stud-ies should examine quality-of-life measures, pre- andpostoperative voice quality, and feeding outcome.
CONCLUSIONAdvancements in pediatric airway management
have seen the development of a number of endoscopictechniques, one of which is laser-assisted posterior cri-coid expansion. Using modified pediatric laryngealinstruments, this technique is a reliable and safe methodto address posterior glottic pathology. Morbidity is mini-mal, and in conjunction with other airway procedures,decannulation is possible in the majority of tracheotomy-dependent children.
BIBLIOGRAPHY
1. Kelchner LN, Weinrich B, Brehm SB, Tabangin ME, de Alarcon A. Charac-terization of supraglottic phonation in children after airway reconstruc-tion. Ann Otol Rhinol Laryngol 2010;119:383–390.
2. Cable BB, Manaligod JM, Bauman NM, Smith RJ. Pediatric airway recon-struction: principles, decision-making, and outcomes at the Universityof Iowa hospitals and clinics. Ann Otol Rhinol Laryngol 2004;113:289–293.
3. Inglis AF Jr, Perkins JA, Manning SC, Mouzakes J. Endoscopic posteriorcricoid split and rib grafting in 10 children. Laryngoscope 2003;113:2004–2009.
4. Gray SD, Kelly SM, Dove H. Arytenoid separation for impaired pediatricvocal fold mobility. Ann Otol Rhinol Laryngol 1994;103:510–515.
5. Thakkar K, Gerber ME. Endoscopic posterior costal cartilage graft place-ment for acute management of pediatric bilateral vocal fold paralysiswithout tracheostomy. Int J Pediatr Otorhinolaryngol 2008;72:1555–1558.
6. Bogdasarian RS, Olson NR. Posterior glottic laryngeal stenosis. OtolaryngolHead Neck Surg 1980;88:765–772.
7. Merritt RM, Bent JP, Smith RJ. Suprastomal granulation tissue and pediat-ric tracheotomy decannulation. Laryngoscope 1997;107:868–871.
8. Rutter MJ, Cotton RT. The use of posterior cricoid grafting in managing iso-lated posterior glottic stenosis in children. Arch Otolaryngol Head NeckSurg 2004;130:737–739.
Laryngoscope 121: May 2011 Provenzano et al.: Endoscopic Posterior Cricoid Grafting
1066