
Pediatric Drug Formulations: A Review of Challenges...
14
Pediatric Drug Formulations: A Review of Challenges and Progress abstract Children differ from adults in many aspects of pharmacotherapy, in- cluding capabilities for drug administration, medicine-related toxicity, and taste preferences. It is essential that pediatric medicines are for- mulated to best suit a child’ s age, size, physiologic condition, and treatment requirements. To ensure adequate treatment of all chil- dren, different routes of administration, dosage forms, and strengths may be required. Many existing formulations are not suitable for children, which often leads to off-label and unlicensed use of adult medicines. New regulations, additional funding opportunities, and in- novative collaborative research initiatives have resulted in some re- cent progress in the development of pediatric formulations. These advances include a paradigm shift toward oral solid formulations and a focus on novel preparations, including flexible, dispersible, and multiparticulate oral solid dosage forms. Such developments have enabled greater dose flexibility, easier administration, and better ac- ceptance of drug formulations in children. However, new pediatric for- mulations address only a small part of all therapeutic needs in children; moreover, they are not always available. Five key issues need to be addressed to stimulate the further development of better medicines for children: (1) the continued prioritization of unmet formulation needs, particularly drug delivery in neonates and treatment gaps in pediatric cancers and childhood diseases in developing countries; (2) a better use of existing data to facilitate pediatric formulation de- velopment; (3) innovative technologies in adults that can be used to develop new pediatric formulations; (4) clinical feedback and practice-based evidence on the impact of novel formulations; and (5) improved access to new pediatric formulations. Pediatrics 2014;134:361–372 AUTHORS: Verica Ivanovska, PharmD, MPH, a,b Carin M.A. Rademaker, PharmD, PhD, c Liset van Dijk, PhD, d and Aukje K. Mantel-Teeuwisse, PharmD, PhD a a Utrecht Institute for Pharmaceutical Sciences, Utrecht University, Utrecht, Netherlands; b Faculty of Medical Sciences, University Goce Delcev, Republic of Macedonia; c Department of Clinical Pharmacy, University Medical Center Utrecht, Utrecht, Netherlands; and d NIVEL, Netherlands Institute for Health Services Research, Utrecht, Netherlands KEY WORDS administration, age groups, oral medications, pediatric, therapeutics ABBREVIATION WHO—World Health Organization Dr Ivanovska conceptualized and designed the study, and drafted the initial manuscript; Drs Rademaker, van Dijk, and Mantel-Teeuwisse contributed to the study concept and outline, and reviewed and revised the manuscript; and all authors approved the final manuscript as submitted. www.pediatrics.org/cgi/doi/10.1542/peds.2013-3225 doi:10.1542/peds.2013-3225 Accepted for publication Feb 27, 2014 Address correspondence to Verica Ivanovska, PharmD, MPH, Utrecht Institute for Pharmaceutical Sciences, Utrecht University, PO Box 80082, 3508 TB, Utrecht, Netherlands. E-mail: [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2014 by the American Academy of Pediatrics FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose. FUNDING: No external funding. POTENTIAL CONFLICT OF INTEREST: Dr van Dijk’ s institute (NIVEL) has received research funds from Astra Zeneca, Bristol-Myers Squibb, and Pfizer for studies not related to the present study. Dr Mantel-Teeuwisse receives no direct funding or donations from private parties, including the pharmaceutical industry. Research funding from public/private partnerships (ie, TI Pharma [www.tipharma.nl]) has been accepted under the conditions that no company-specific product or company-related study is conducted. She has received unrestricted research funding from public sources (ie, the Netherlands Organisation for Health Research and Development [ZonMW], the EU 7th Framework Program [FP7], the Dutch Medicines Evaluation Board [MEB], and the Dutch Ministry of Health). Dr Ivanovska and Dr Rademaker have indicated they have no potential conflicts of interest to disclose. PEDIATRICS Volume 134, Number 2, August 2014 361 STATE-OF-THE-ART REVIEW ARTICLE by guest on May 4, 2018 http://pediatrics.aappublications.org/ Downloaded from
Transcript of Pediatric Drug Formulations: A Review of Challenges...

Pediatric Drug Formulations: A Review of Challengesand Progress
abstractChildren differ from adults in many aspects of pharmacotherapy, in-cluding capabilities for drug administration, medicine-related toxicity,and taste preferences. It is essential that pediatric medicines are for-mulated to best suit a child’s age, size, physiologic condition, andtreatment requirements. To ensure adequate treatment of all chil-dren, different routes of administration, dosage forms, and strengthsmay be required. Many existing formulations are not suitable forchildren, which often leads to off-label and unlicensed use of adultmedicines. New regulations, additional funding opportunities, and in-novative collaborative research initiatives have resulted in some re-cent progress in the development of pediatric formulations. Theseadvances include a paradigm shift toward oral solid formulationsand a focus on novel preparations, including flexible, dispersible, andmultiparticulate oral solid dosage forms. Such developments haveenabled greater dose flexibility, easier administration, and better ac-ceptance of drug formulations in children. However, new pediatric for-mulations address only a small part of all therapeutic needs in children;moreover, they are not always available. Five key issues need to beaddressed to stimulate the further development of better medicinesfor children: (1) the continued prioritization of unmet formulationneeds, particularly drug delivery in neonates and treatment gaps inpediatric cancers and childhood diseases in developing countries; (2)a better use of existing data to facilitate pediatric formulation de-velopment; (3) innovative technologies in adults that can be used todevelop new pediatric formulations; (4) clinical feedback andpractice-based evidence on the impact of novel formulations; and(5) improved access to new pediatric formulations. Pediatrics2014;134:361–372
AUTHORS: Verica Ivanovska, PharmD, MPH,a,b Carin M.A.Rademaker, PharmD, PhD,c Liset van Dijk, PhD,d and AukjeK. Mantel-Teeuwisse, PharmD, PhDa
aUtrecht Institute for Pharmaceutical Sciences, UtrechtUniversity, Utrecht, Netherlands; bFaculty of Medical Sciences,University Goce Delcev, Republic of Macedonia; cDepartment ofClinical Pharmacy, University Medical Center Utrecht, Utrecht,Netherlands; and dNIVEL, Netherlands Institute for HealthServices Research, Utrecht, Netherlands
KEY WORDSadministration, age groups, oral medications, pediatric,therapeutics
ABBREVIATIONWHO—World Health Organization
Dr Ivanovska conceptualized and designed the study, anddrafted the initial manuscript; Drs Rademaker, van Dijk, andMantel-Teeuwisse contributed to the study concept and outline,and reviewed and revised the manuscript; and all authorsapproved the final manuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2013-3225
doi:10.1542/peds.2013-3225
Accepted for publication Feb 27, 2014
Address correspondence to Verica Ivanovska, PharmD, MPH,Utrecht Institute for Pharmaceutical Sciences, Utrecht University,PO Box 80082, 3508 TB, Utrecht, Netherlands. E-mail:[email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2014 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: Dr van Dijk’s institute (NIVEL)has received research funds from Astra Zeneca, Bristol-MyersSquibb, and Pfizer for studies not related to the present study.Dr Mantel-Teeuwisse receives no direct funding or donationsfrom private parties, including the pharmaceutical industry.Research funding from public/private partnerships (ie, TIPharma [www.tipharma.nl]) has been accepted under theconditions that no company-specific product or company-relatedstudy is conducted. She has received unrestricted researchfunding from public sources (ie, the Netherlands Organisationfor Health Research and Development [ZonMW], the EU 7thFramework Program [FP7], the Dutch Medicines EvaluationBoard [MEB], and the Dutch Ministry of Health). Dr Ivanovskaand Dr Rademaker have indicated they have no potentialconflicts of interest to disclose.
PEDIATRICS Volume 134, Number 2, August 2014 361
STATE-OF-THE-ART REVIEW ARTICLE
by guest on May 4, 2018http://pediatrics.aappublications.org/Downloaded from

Drug formulations used in pediatricpharmacotherapy should be adapted tochildren’s needs to suit their age, size,physiologic condition, and treatmentrequirements.1,2 Such pediatric medi-cines are key to achieving safe andaccurate dose administration, re-ducing the risk of medication errors,enhancing medication adherence, andimproving therapeutic outcomes inchildren.3,4
The use of inadequate drug formula-tions in children may pose problemsnot seen in adults, such as difficulty inswallowing conventionally sized tab-lets, safety issues with certain excip-ients that are acceptable in adultformulations, and adherence problemswith unpalatable medicines.1,5 Theseissues have led to tragedies in the past,and they exist partly because onlya small fraction of all marketed drugsare available in formulations that areage appropriate.6–12 As a result, manyadult medicines are used off-labelin children, a practice that carriesadditional health and environmentalrisks.13–15
To strengthen the development of pe-diatric drug formulations, new legis-lation was introduced in the UnitedStates and Europe, and efforts forglobal collaboration were made by theWorld Health Organization (WHO).16–20 Anumber of innovative pediatric for-mulations have followed, but their ac-tual effect on pediatric drug approvalsremains to be seen, as clinical trialsand marketing authorization takea substantial amount of time.21–24
To optimize pharmacotherapy in chil-dren, it is important for clinicians tounderstand the background of theaforementioned problems as well as togain insight into the challenges, devel-opments, and potential solutions. Theaim of the present review was to de-scribe why there is a specific need forpediatric drug formulations and to il-lustrate the clinical consequences of
the absence of suitable medicines forchildren. We will discuss the progressachieved so far and determine addi-tional steps required to improve thedevelopment and availability of pedi-atric drug formulations.
THE NECESSITY OF PEDIATRICDRUG FORMULATIONS
Diversity in Children
It has been well established that chil-dren are not small adults but rathera distinct and heterogeneous patientgroup with regard to pharmacother-apy.25 They often exhibit a different re-sponse to both active substance andexcipients.26 Children present a contin-uum of growth and developmentalphases as a result of their rapid growth,maturation of the body composition,and physiologic and cognitive changesduring childhood.
Children differ from adults in manyaspects of pharmacokinetics and phar-macodynamics, potential routes of ad-ministration, medicine-related toxicity,and taste preferences.3,25 Importantpharmacokinetic differences betweenchildren and adults include the rateof gastric emptying and pH, gastroin-testinal permeability, and the surfacearea available for drug absorption.Dissimilarities have also been reportedin drug metabolism, transporter ex-pression, biliary function, and renalclearance, resulting in differences indrug disposition and elimination.27,28
The largest deviation from adult phar-macokinetics is observed in the first12 to 18 months, when organ functionsare developing.29,30 In older childrenand adolescents, the pharmacokineticparameters approach adult valuesand are thus easier to predict.26,31–33
The effect of age on pharmacokineticsleads to different dosing require-ments for different age groups. Frombirth to adulthood, the body size andweight of an average child increasesup to 20-fold, and the magnitude of
dose variation administered throughoutchildhood may be 100-fold.5 More dra-matically, premature neonates admittedto the hospital can weigh as little as 500g, further highlighting the need for dosevariability.29,30 Maturation processes inchildren are not linear, and thereforedoses in certain age subsets may belower, identical to, or higher than inadults, depending on a drug’s metabolicpathway.32,34,35
Due to this extensive variability inchildren, there is an obvious need fordrug formulations tailored to childrenin all the target age groups. The Inter-national Conference of Harmonisationdivides childhood into 5 age groupsrelated to the developmental stages,derived from the physiologic and phar-macokinetic differences mentioned ear-lier.28 These groups (with age ranges)are: preterm newborn infants; termnewborn infants (0–27 days); infantsand toddlers (1–23 months); children(2–11 years); and adolescents (12–16years in the United States or 12–18 yearsin the European Union).5,36
The European Committee for MedicinalProducts for Human Use further sub-divides the age group “children” (2–11years) into “preschool children” (2–5years), and “school children” (6–11years) to more precisely reflect thechildren’s ability to accept and usedifferent dosage forms.5 However, theclassification of the pediatric pop-ulation into age categories is to someextent arbitrary because children ofthe same chronologic age may stilldevelop at different rates.28
Age-Related Adherence to PediatricDrug Formulations
Formulation acceptability and prefer-ences facilitate medication adherencein children, and they are importantfactors in achieving the intended treat-ment outcomes. Formulation acceptabil-ity differs across age groups as childrengradually develop their cognitive and
362 IVANOVSKA et al
by guest on May 4, 2018http://pediatrics.aappublications.org/Downloaded from

motor skills, and improve their ability toswallowmedications. At certainages, thedependence on caregivers also playsa role in the administration of pediatricdosage forms.1 Pain, discomfort, and anunnecessary burden on children and/orcaregivers during drug administrationshould be minimized to assure ade-quate medication adherence. In olderchildren and adolescents, lifestyle andpeer pressure may also influence med-ication adherence and possible prefer-ences for particular formulations.
Tasteattributesmaybecritical toensureacceptable adherence to pediatric oralformulations. Because children havea low tolerance for disagreeable taste,the use of tasteless or palatable medi-cines can minimize the loss of medica-tion from spillage and/or spitting.14,37,38
Taste preferences may differ betweenchildren and adults, as children prefersweet and salty flavors, and dislike bit-ter and peppermint taste. These find-ings suggest that taste assessmentshould involve children early in the drugformulation development.35,38,39 Chil-dren’s communication about taste per-ceptions can be facilitated by usingage-appropriate methods, scales, andmeasures.40 Alternative taste-screeningmethods may include adult taste panelswith validated design for data trans-ferability or predictive electrochemicalsensor systems (so called “electronictongues”).41,42
CLINICAL CONSEQUENCES OF THEABSENCE OF SUITABLE PEDIATRICDRUG FORMULATIONS
Potential Limitations of PediatricDrug Formulations
Historically, the failure to appreciate thedevelopmental changes in children hasled tomanyadverse outcomes in clinicalpractice. Examples include infant deathsfromchokingonalbendazole tablets, thelethal use of benzyl alcohol or diethyleneglycol in sulfanilamide elixirs, and elec-trolyteimbalancescausedbyhighcontents
of sodium or potassium in parenteralformulations.6–9
To prevent such tragedies and ensureadequate treatment of children of allages,different routesofadministration,dosage forms, and strengths are oftenneeded for the same active substance.1
Table1 illustrates the specific purposes,potential strengths, and weaknesses ofvarious routes of administration anddosage forms for pediatric use.1,2,5,43–47
As in adults, the oral route is the pre-dominant route of administration inchildren.1,2,43 Alternative nonoral routesof administration include rectal, dermal,nasal, pulmonary, and ocular routes.1,2
The selection for clinical use is influ-enced by the limitations of each dosageform. Oral solids are associated withthe risk of choking or chewing and withlimited dose flexibility, whereas palat-ability and dose uniformity may bechallengingfor liquidpreparations.1,2,43,44
In addition, liquid forms raise issuesregarding stability (chemical, physical,or microbiological) and the require-ment for clean water; moreover, theycan be bulky, impractical, and expen-sive to ship and store, particularly inlower income countries with hot andhumid climates.48,49
The use of nonoral routes of drug ad-ministration may be hampered by dif-ficult application, local irritation, fluidoverload, electrolyte imbalance, or poordrug acceptability (Table 1).1,2,5,43–47 Inneonates, intravenous administrationmay lead to volume overload. Moreover,measuring small dose volumes maycause large dosage variations anderrors.47 Similarly, age-appropriate dos-ing volumes are important to ensure fulldose ingestion for oral liquids.5
Another important concern in pediat-ric drug formulations are the excipi-ents, frequently used as preservatives,sweeteners, fillers, solvents, and coatingand coloring agents. Their selection forpediatric medicines is challenging be-cause neither the inactive ingredients
guide list of the US Food and Drug Ad-ministrationnor the “generally regardedas safe” status has been validated forpediatric use.3,29,30,50 Little is knownabout the safety of excipients in children,and accepted daily and cumulative in-takes of excipients have not been estab-lished. Anecdotal evidence suggests anassociation between some excipientscommonly used in adult medicines and el-evated toxicity andsafety issues inchildren,especially neonates (Table 2).3,6–9,26,50–60
A recent example is the administrationof lopinavir/ritonavir (Kaletra [AbbottLaboratories, Abbott Park, IL]) oral so-lution in premature newborns whowere exposed to the risk of ethanoland/or propylene glycol toxicity. Thissituation resulted in a Food and DrugAdministration drug safety communi-cation and a change in the drug label in2011.61 A number of recent studies inNICUs revealed systemic concentra-tions of excipients that were intol-erable even in older age groups.54,62,63
The urgent need to understand thesesafety concerns has led to a collabora-tive effort by the United States and theEuropeanUnion to create a STEP (Safetyand Toxicity of Excipients for Pediatrics)database. Its aim is to improve sys-tematic data collection on excipienttoxicity and tolerance in children.64–66
A similar initiative, ESNEE (EuropeanStudy of Neonatal Exposure to Excipients),has developed a platform for the sys-tematic assessment of excipients in neo-nates.67
Concerns Over Off-label andUnlicensed Use of Medicines inChildren
Pediatric drug development is associ-atedwithnumerouschallenges, includingmethodologic and ethical requirementsfor pediatric trials, high developmentalcosts, and a small and fragmentedmarket.3,4,50,68–71 As a result of thesechallenges, there have only been limitedresearch efforts to adapt medicinesaccording to pediatric needs. Thus, only
STATE-OF-THE-ART REVIEW ARTICLE
PEDIATRICS Volume 134, Number 2, August 2014 363
by guest on May 4, 2018http://pediatrics.aappublications.org/Downloaded from
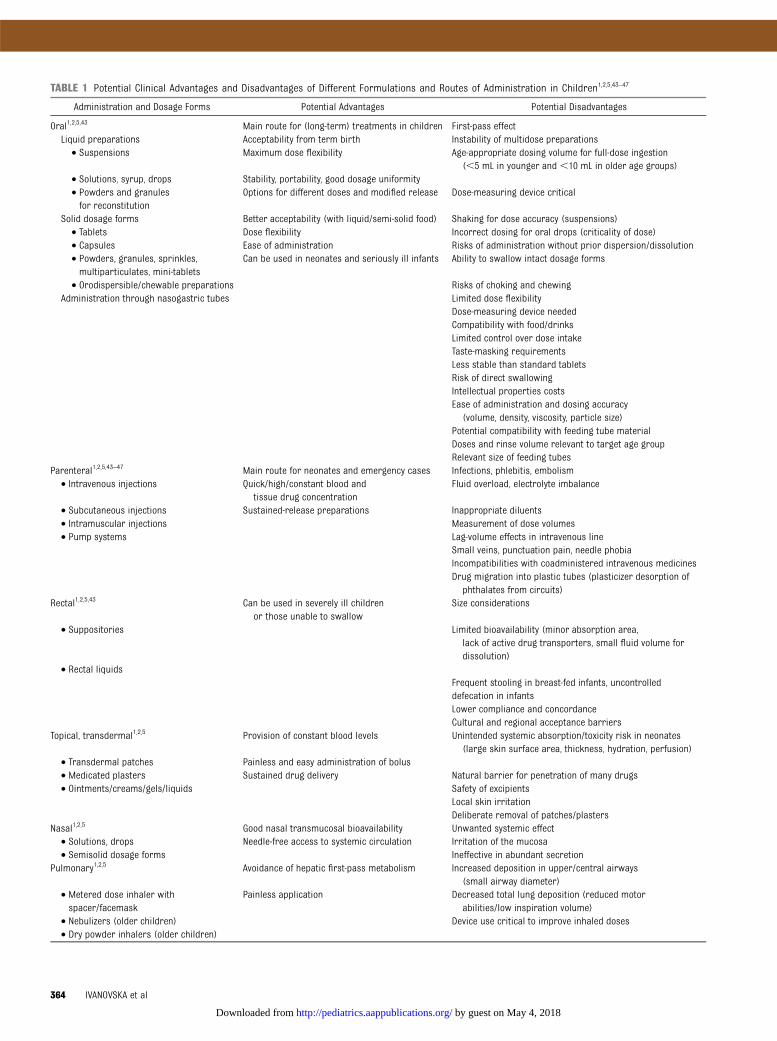
TABLE 1 Potential Clinical Advantages and Disadvantages of Different Formulations and Routes of Administration in Children1,2,5,43–47
Administration and Dosage Forms Potential Advantages Potential Disadvantages
Oral1,2,5,43 Main route for (long-term) treatments in children First-pass effectLiquid preparations Acceptability from term birth Instability of multidose preparations• Suspensions Maximum dose flexibility Age-appropriate dosing volume for full-dose ingestion
(,5 mL in younger and ,10 mL in older age groups)• Solutions, syrup, drops Stability, portability, good dosage uniformity• Powders and granulesfor reconstitution
Options for different doses and modified release Dose-measuring device critical
Solid dosage forms Better acceptability (with liquid/semi-solid food) Shaking for dose accuracy (suspensions)• Tablets Dose flexibility Incorrect dosing for oral drops (criticality of dose)• Capsules Ease of administration Risks of administration without prior dispersion/dissolution• Powders, granules, sprinkles,multiparticulates, mini-tablets
Can be used in neonates and seriously ill infants Ability to swallow intact dosage forms
• Orodispersible/chewable preparations Risks of choking and chewingAdministration through nasogastric tubes Limited dose flexibility
Dose-measuring device neededCompatibility with food/drinksLimited control over dose intakeTaste-masking requirementsLess stable than standard tabletsRisk of direct swallowingIntellectual properties costsEase of administration and dosing accuracy
(volume, density, viscosity, particle size)Potential compatibility with feeding tube materialDoses and rinse volume relevant to target age groupRelevant size of feeding tubes
Parenteral1,2,5,43–47 Main route for neonates and emergency cases Infections, phlebitis, embolism• Intravenous injections Quick/high/constant blood and
tissue drug concentrationFluid overload, electrolyte imbalance
• Subcutaneous injections Sustained-release preparations Inappropriate diluents• Intramuscular injections Measurement of dose volumes• Pump systems Lag-volume effects in intravenous line
Small veins, punctuation pain, needle phobiaIncompatibilities with coadministered intravenous medicinesDrug migration into plastic tubes (plasticizer desorption of
phthalates from circuits)Rectal1,2,5,43 Can be used in severely ill children
or those unable to swallowSize considerations
• Suppositories Limited bioavailability (minor absorption area,lack of active drug transporters, small fluid volume fordissolution)
• Rectal liquidsFrequent stooling in breast-fed infants, uncontrolleddefecation in infantsLower compliance and concordanceCultural and regional acceptance barriers
Topical, transdermal1,2,5 Provision of constant blood levels Unintended systemic absorption/toxicity risk in neonates(large skin surface area, thickness, hydration, perfusion)
• Transdermal patches Painless and easy administration of bolus• Medicated plasters Sustained drug delivery Natural barrier for penetration of many drugs• Ointments/creams/gels/liquids Safety of excipients
Local skin irritationDeliberate removal of patches/plasters
Nasal1,2,5 Good nasal transmucosal bioavailability Unwanted systemic effect• Solutions, drops Needle-free access to systemic circulation Irritation of the mucosa• Semisolid dosage forms Ineffective in abundant secretion
Pulmonary1,2,5 Avoidance of hepatic first-pass metabolism Increased deposition in upper/central airways(small airway diameter)
• Metered dose inhaler withspacer/facemask
Painless application Decreased total lung deposition (reduced motorabilities/low inspiration volume)
• Nebulizers (older children) Device use critical to improve inhaled doses• Dry powder inhalers (older children)
364 IVANOVSKA et al
by guest on May 4, 2018http://pediatrics.aappublications.org/Downloaded from

one-third of all medicines approved bythe European Medicines Agency overthe period of 1995 to 2005 were licensedfor use in children.11,23,72 Higher but stillunsatisfactory rates were reported inNew Zealand (35%), Australia (38%),and the United States (54%).23,73,74 Thepediatric market has focused mostlyon only a limited number of thera-peutic areas, such as antiinfectives,hormones, and medicines for the re-spiratory and central nervous system.75
Meanwhile, there are hardly any dermalpreparations and medicines specificallyaimed at younger age groups for thecardiovascular system, sensory organs,and cancers.23 Moreover, especially inyounger children and neonates, evenauthorized pediatric medicines may notalways be age appropriate with respectto dosing, suitability of dosage forms,and excipients.
This lackofpediatric formulationsoftenleaves health care professionals noalternativebut touseadultmedicines inan off-label or unlicensed manner. Thetrend is widespread: in the EuropeanUnion, 45% to 60% of all medicines aregiven to children off-label. This trend isalso true for 90% of medicines adminis-tered to neonates and infants, particu-larly in PICUs.76 Not surprisingly, off-labeluse is common for antiarrhythmics,antihypertensives, protonpump inhibitors,H2-receptor antagonists, antiasthmaticagents, and some antidepressants.76 Inthe United States, two-thirds of medicinesused in pediatrics are off-label; world-
wide, this proportion is up to three-quarters.77
Risk Management of Compoundingand Manipulation of Medicines forChildren
Alternative treatment options are oftenused to make unavailable drugs ac-cessible for children and/or to adjustdrug doses according to individualpatientneeds. Theseoptions include themodification of administration routes(eg, oral use of parenteral formulations);manipulation of adult dosage forms(eg, diluting liquid formulations); seg-menting tablets and suppositories,cutting patches, and dispersing opencapsules or crushed tablets in water,liquid, or food; or extemporaneousdispensing (ie, compounding medi-cines from ingredients within phar-macies).5,78
Administering medicines in this wayis difficult and unsafe because limiteddata are available to validate stability,bioavailability, pharmacokinetics, phar-macodynamics, dosing accuracy, tol-erability, and reproducibility.79–84 Adocumented example is the crushingof Kaletra tablets for pediatric admin-istration, which resulted in reducedbioavailability and drug exposure inchildren.85 All these manipulations maycompromise drug efficacy and/orsafety, as well as create risks for theenvironment and individuals handlingthe dosage forms, particularly in thecase of mutagen and cytotoxic com-pounds.79–84
Producing a medicine by extempora-neous dispensingmay be the only optionfor some children to receive a certainmedicine in a suitable dosage form. Insuchsituations, theriskscanbereducedby applying sound quality assurancesystems. Pharmacists should ensurethat good manufacturing principles areimplemented, adequate raw materialsand formulae are used, and stabilitystudies are validated and conductedby certified laboratories. Moreover, be-
cause practices and guidelines forextemporaneous formulations differgreatly among practitioners, there is anurgent need for a standardization ofcommonly applied compounding prac-tices.78,86 Existing networks, resources,and guidelines should be stimulated toprovide appropriate information on thestandards of practice for extempora-neous formulations.78,84 However, theavailable informationmay not always beeasily transferable to a local situation ormay not be exclusively focused on chil-dren.87
PROGRESS IN DEVELOPINGPEDIATRIC DRUG FORMULATIONS
New Frameworks for theDevelopment of Pediatric DrugFormulations
To overcome the aforementioned chal-lenges, a new pediatric regulatory en-vironment hasbeencreated tostimulatethe development and availability of age-appropriate medicines for children.16–19
The intended long-term aim is to in-tegrate pediatric needs into overalldrug development, so that each newcomponent is systematically evaluatedfor its potential use in children. Initialprogress has been made by combininglegal requirements with incentives forcompanies to test, authorize, and for-mulate medicines for use in children.Over the past decade, the Best Phar-maceuticals for Children Act and thePediatric Research Equity Act in theUnited States, and the Pediatric Regu-lation in the European Union, havefueled an increasing number of pediat-ric clinical trials and innovations in pe-diatric drug formulations.22,24
Nonetheless, therapeutic areas ad-dressed by the industry seem to bemore aligned with adult drug de-velopment than with unmet publichealth needs in children.22,68,88,89 Toguide the efforts toward significanttherapeutic benefits for children, theUS and European Union government
TABLE 2 Examples of Excipients WithElevated Toxicity and Safety Risksfor (Preterm and Term) Newbornsand Infants,6 Months of Age7,8,53–60
Excipient Adverse Reaction
Benzylalcohol7,8,53,54
Neurotoxicity, metabolicacidosis
Ethanol55 Neurotoxicity, cardiovascularproblems
Propyleneglycol54,56–59
Neurotoxicity, seizures,hyperosmolarity
Polysorbate20 and 8060
Liver and kidney failure
STATE-OF-THE-ART REVIEW ARTICLE
PEDIATRICS Volume 134, Number 2, August 2014 365
by guest on May 4, 2018http://pediatrics.aappublications.org/Downloaded from

agencies have produced priority med-icines lists, highlighting areas withsubstantial off-label use in childrenand gaps in pediatric data.90,91
Simultaneously, a WHO initiative (“MakeMedicines Child Size”) has drawn at-tention to the fact that the lack of med-icines most acutely affects childrenliving in developing countries.20,92 A fo-cus on the development of suitabledosage forms to treat diseases of highburden in childhood in low-resourcesettings could greatly reduce child-hood morbidity and mortality.92 Therehave been comprehensive WHO activi-ties to improve access to and use of safeand appropriate pediatric medicines.These activities include establishinga model list of essential medicines forchildren and a list of priority life-savingmedicines for women and children, de-veloping model formularies for chil-dren, updating childhood treatmentrecommendations, and including pedi-atric medicines in the prequalificationprocess.93–97
Furthermore, the present reward sys-tem has not proved to be an adequateincentive for investment in off-patentdrug research.69,89 This tendency maybe linked to prescription reimburse-ment rules that attach little value toold medicines, even if they includenew child-friendly formulations.69 Togenerate more interest in off-patentmedicines, new public funding oppor-tunities in academia and small- andmedium-sized enterprises have beenprovided by both the US Eunice KennedyShriver National Institute of Child Healthand Human Development Pediatrics For-mulation Initiative and the EU’s SeventhFramework Program for Research.98–100
However, new technologies developedfrom these initiativesmust be adopted bythe industry and marketed so they canrealize their full potential.
There is also increased recognition thatthe selection of appropriate pediatricformulations requires a risk/benefit
analysis on a case-by-case basis.1,2
Taking into consideration the het-erogeneity of children and specificcharacteristics of each dosage form(Table 1), the industry has recentlyproposed a composite assessment toolto guide optimal formulation choicesfor individual patients.44 This struc-tured framework is based on 3 pre-determined criteria for each drugformulation: product efficacy and easeof use (eg, dose flexibility, drug ac-ceptability, convenient handling, correctuse), patient safety (eg, bioavailability ofactive substances, safety of excipients,medication stability, risk of medicationerrors) and patient access (eg, prod-uct manufacturability, affordability, de-velopment, production speed).41 Thechoice between alternatives is based ona quantitative scoring system for eachpharmaceutical formulation option.44
This individualized approach to optimalformulations can also be replicated inclinical settings if the selection criteriainclude relevant aspects of patient care.
Novel Oral Pediatric Formulations
Recent progress in pediatric drug de-velopment mostly concerns oral for-mulations.22,101 Until recently, liquidformulations were preferred for youn-ger children because of their easy andsimple dosing across age subgroups.5,10,102 In 2008, a WHO expert forum pro-posed a paradigm shift toward pedi-atric oral solids in view of stabilityproblems and the high transportationand storage costs involved in liquidformulations.92 From then on, flexibleoral solid dosage forms, such as oro-dispersible tablets and/or tablets usedto prepare oral liquid preparationssuitable for younger children, havebecome the recommended pediatricdosage forms worldwide. In 2009,Coartem Dispersible (Novartis Inter-national AG, Basel, Switzerland, andMedicines for Malaria) was launchedto offer flexible artemisinin-basedcombination therapy for children (5–
35 kg) with a cure rate comparable tothat of the Coartem tablet.103,104
For oral medicines requiring precisedose measurement, a new flexibleplatform technology was proposed toproduce solid multiparticulate dosageforms (eg, mini-tablets, pellets) anddosage forms dispersible in liquids orsprinkled on food.92 This platformtechnology has the potential flexibilityto construct fixed-dose combinationproducts, especially for chronic dis-eases such as HIV or tuberculosis.105–107
Table 3 illustrates some of the quality-certified, innovative oral pediatric dos-age forms brought to market, includingmuch needed heat-stable formulationsand fixed-dose combination productsfor low-resource settings.97,104,108–116
Current surveys reveal that novel oralsolids may be used in children at anearlier age than previously antici-pated.5,117,118 Initially, in 2009, Thomsonet al119 demonstrated that 46% of 2-year-old children and 86% of 5-year-oldchildren could swallow innovative 3-mm mini-tablets without choking oraspiration. The age limit was furtherdecreased in an exploratory studywhich demonstrated that childrenaged 6 to 12 months were capable ofswallowing uncoated, drug-free, 2-mmmini-tablets and accepted them betterthan sweet liquid formulations.120,121
For infants aged ,2 years, a newpromising development is the orallydisintegrating mini-tablet, which com-bines mini-tablets and fast-dissolvingdosage forms.111
A complementary research area is thedevelopment of pediatric dosing de-vices, which facilitate the accurate andconsistent administration of oral pe-diatric formulations.1,122 New devicesgenerally assist the oral delivery ofliquids to small children by using mod-ified feeding bottles and pacifiers withmedicines placed in a reservoir, helpimprove the palatability of oral solutionsby using a dose-sipping technology, or
366 IVANOVSKA et al
by guest on May 4, 2018http://pediatrics.aappublications.org/Downloaded from

help increase product stability by usinga pulp-spoon with a single dry dose ofmedicine (see Table 4 for more detailedexamples).3,116,122
FUTURE STEPS
The ideal pediatric formulation shouldhave flexible dosage increments andminimal excipients, be palatable, safeand easy to administer, and be stablewith regard to light, humidity, and heat.
Nevertheless, a significant number ofdrug formulations are unsuitable forchildren,which leads to unsafe off-labeland unlicensed use of adult medicines.Recent initiatives promoting pediatricdrug development have made someinitial progress in the neglected area ofpediatric formulations. Most effortshave focused on age-appropriate oralsolid preparations, which enable doseflexibility, easier administration, and
better acceptance in children. Despitethese advances, the new pediatric for-mulations are still only a small part ofthe full therapeutic arsenal needed toserve all pediatric patients.
The following 5 priorities have beenidentified as critical for the furtherdevelopment of appropriate pediatricformulations. The first key issue is thecontinuous prioritization process thatfocuses on unmet public health issues
TABLE 3 Examples of Recently Marketed/Prequalified Novel Oral Drug Formulations for Children97,104,108–116
Dosage Form International Nonproprietary Name Regulatory Agency Authorization/WHO PQ Year
Multi-particulates97,108–110
Sprinkles, granules and pellets Para-aminosalicylate granules WHO PQ 2009TFV granules FDA 2012, EMA 2012Rabeprazole sprinkles FDA 2013
Flexible dispersible formulations97,104,111–114
Dispersible and orodispersible tablets Artemether/lumefantrine dispersible tablets Swissmedic 2008 /WHO PQ 2009
3TC/NVP/d4T WHO PQ 2008Isoniazid/pyrazinamide/rifampicin WHO PQ 2009Isoniazid/rifampicin WHO PQ 20093TC/NVP/AZT (Mylan Laboratories) WHO PQ 2009ABC WHO PQ 20103TC/d4T WHO PQ 20113TC/AZT WHO PQ 2011EFV WHO PQ 20123TC WHO PQ 2012Artemether/lumefantrine WHO PQ 2012Isoniazid/pyrazinamide/rifampicin WHO PQ 2012Isoniazid/rifampicin WHO PQ 2012Benznidazole WHO PQ 2012Lamotrigine orodispersible tablets FDA 2012AZT WHO PQ 2013
Orodispersible films (wafer) Ondasetron FDA 2010Chewable dispersible tablets Lamotrigine FDA 2012Orally disintegrating mini-tablets Hydrochlorothiazide Model drug under investigation
Other novel oral formulations115,116
Chewable tablets Atorvastatin EMA 2011Raltegravir FDA 2012
3TC, lamivudine; ABC, abacavir; AZT, zidovudine; d4T, stavudine; EFV, efavirenz; FDA, US Food and Drug Administration; ODT, orodispersible tablet; PQ, prequalification; NVP, nevirapine; TFV,tenofovir.
TABLE 4 Examples of Novel Drug Devices That Facilitate Oral Administration of Medicines in Children3,116,122
Novel Drug Devices Examples of Medicines Administered With DrugDevices (Brand Name, Manufacturer)
Purpose of Use
Modified teat/pacifier with drug-loaded reservoir Nystatin (Mykundex, Bioglan Giessen, Germany) Constant delivery of medicine (in oral cavity) inneonates/infants
Dosing spoon filled with liquid medicine Diphenhydramine (Benadryl, Pfizer ConsumerHealthcare, Madison, New Jersey)
Exact measurement of single doses, low risk of spillage
Coated particles on dosage spoon (pulp-spoon) Azythromycin powder for oral pulp (predosedazithromycin spoon; Sandoz Kundl, Austria)
Exact measurement of single doses, low risk of spillageimproves stability of medicines
Dropper tube Codeine drops (Paracodin, Abbott Laboratories,Abbott Park, IL)
Ensures dose uniformity
Dose-sipping technology (straw withmedicine and beverage)
Clarithromycin micropellets (Clarosip, GrünenthalGmbH, Aachen, Germany)
Improves palatability and adherence
Solid dosing pen Carvedilol/metoprolol tartrate (model drugs) Exact measurement of doses
STATE-OF-THE-ART REVIEW ARTICLE
PEDIATRICS Volume 134, Number 2, August 2014 367
by guest on May 4, 2018http://pediatrics.aappublications.org/Downloaded from

and ensures that drug developmentaligns with the true clinical needs inchildren. Special attention should bepaid to innovations that improve drugdelivery in neonates, fill treatment gapsin pediatric cancers, and treat diseasesof high burden in developing coun-tries.49,90,91,94,123
Second, better use of existing data arerequired to facilitate pediatric drugdevelopment. Some innovative scenar-ios under investigation include pre-liminary “enabling” formulations thatbridge existing adult formulations andpotential pediatric market formulations,adjustments of adult in vitro gastrointes-tinal models to study drug bioavailabilityin children, and refined criteria for theextrapolation of adult efficacy data to thepediatric population.124–126
Third, future research on pediatricformulations could potentially benefitfrom existing or innovative technolo-gies under development in adults.127
Novel experimental treatments of adultcancers, infections, and asthma haveused nanoparticle-targeted therapy,novel smart polymer-based drug de-
livery systems, new chemical entities(eg, dendrimers), and remote trigger-ing devices. These treatments mayhave significant applications in chil-dren, and the identification of appro-priate animal models for pediatricpreclinical studies should be a re-search priority.128–130
Fourth, ongoing technologic advancesneed to be accompanied by relevantpatient outcome studies and clinicalfeedback on efficacy, safety, patientacceptability, preferences, and adher-ence regarding new formulations;currently, such studies and feedbackare lacking.131 Practice-based evidenceon the impact of novel formulations,generated by health care professionalsand caregivers, could provide furthersupport for the development of pedi-atric medicines with clear clinicaladvantages.
The fifth priority concerns finance. Be-cause innovative technologies arecostly, the ultimate challenge is tomake these new pediatric formulationsavailable on the market and in dailypractice.22,89,132 Their commercial via-
bility might be improved by an in-creased market size (eg, global scale,inclusion of geriatric patients andadults with swallowing difficulties);new incentive schemes (particularlyfor off-patent drugs), such as limitedexclusivity and premiums, funding, andtax breaks; and public–private part-nerships that support the developmentof orphan drugs and other less profit-able niches.69,98–100
In sum, to reach these goals, it is es-sential that there is a committedcollaboration between stakeholdersthat extends across disciplines andgeographic regions. Moreover, thiscollaboration should have the in-novative potential to further shape thepediatric drug development agendaand thus to close the adult–childmedicine gap.
ACKNOWLEDGMENTWe acknowledge Dr Richard Laing(WHO) for his advice on the progressanalysis and recommendations forimproving pediatric drug formula-tions.
REFERENCES
1. European Medicines Agency. Guideline onpharmaceutical development of medi-cines for paediatric use. EMA/CHMP/QWP/805880/2012 Rev. 2
2. World Health Organization. Developmentof Paediatric Medicines: Points to Con-sider in Formulation. Geneva, Switzerland:World Health Organization; 2012. WHOTechnical Report Series, No. 970, Annex 5
3. Breitkreutz J, Boos J. Paediatric and ge-riatric drug delivery. Expert Opin DrugDeliv. 2007;4(1):37–45
4. Ernest TB, Elder DP, Martini LG, Roberts M,Ford JL. Developing paediatric medicines:identifying the needs and recognizing thechallenges. J Pharm Pharmacol. 2007;59(8):1043–1055
5. European Medicines Agency. Committeefor Medicinal products for Human use(CHMP) 2005: Reflection Paper: For-mulations of Choice for the PaediatricPopulation. EMEA/CHMP/PEG/194810/2005
6. Geiling EMK, Cannon PR. Pathologicaleffects of elixir of sulfanilamide poison-ing. JAMA. 1938;111(10):919–926
7. Hiller JL, Benda GI, Rahatzad M, et al.Benzyl alcohol toxicity: impact on mor-tality and intraventricular hemorrhageamong very low birth weight infants. Pe-diatrics. 1986;77(4):500–506
8. Brown WJ, Buist NR, Gipson HT, Huston RK,Kennaway NG. Fatal benzyl alcohol poi-soning in a neonatal intensive care unit.Lancet. 1982;1(8283):1250
9. World Health Organization. Promoting Safetyof Medicines for Children. Geneva, Switzer-landWorld Health Organization; 2007
10. Nahata MC. Lack of pediatric drug for-mulations. Pediatrics. 1999;104(3 pt 2,suppl 3):607–609
11. Ceci A, Felisi M, Baiardi P, et al. Medicines forchildren licensed by the European MedicinesAgency (EMEA): the balance after 10 years.Eur J Clin Pharmacol. 2006;62(11):947–952
12. Shirkey H. Therapeutic orphans. J Pediatr.1968;72(1):119–120
13. European Medicines Agency. Report onthe Survey of all Paediatric Uses of Me-dicinal Products in Europe. EMA/794083/2009
14. Bazzano AT, Mangione-Smith R, SchonlauM, Suttorp MJ, Brook RH. Off-label pre-scribing to children in the United Statesoutpatient setting. Acad Pediatr. 2009;9(2):81–88
15. Mason J, Pirmohamed M, Nunn T. Off-labeland unlicensed medicine use and adversedrug reactions in children: a narrativereview of the literature. Eur J Clin Phar-macol. 2012;68(1):21–28
16. Best Pharmaceuticals for Children Act. In:Proceedings of 107th Congress of theUnited States of America. Washington, DC;January 3, 2002
17. Pediatric Research Equity Act of 2003. In:proceedings of 108th Congress of the
368 IVANOVSKA et al
by guest on May 4, 2018http://pediatrics.aappublications.org/Downloaded from

United States of America. Washington, DC;January 7, 2003
18. US Food and Drug Administration Amend-ments Act of 2007. In: Proceedings of 110thCongress of the United States of America.Washington, DC; January 4, 2007
19. The European Parliament and the Councilof the European Union. Regulation EC No.1901/2006 Medicinal Products for Paedi-atric Use. Official Journal of the EuropeanUnion L. 378/2. 27.12.2006. Available at:http://ec.europa.eu/health/files/eudralex/vol-1/reg_2006_1901/reg_2006_1901_en.pdf. Accessed August 15, 2013
20. World Health Organization. Make medi-cines child size. Available at: www.who.int/childmedicines/en/. Accessed August 15,2013
21. BPCA Collaborative Efforts. Inter-agencyinitiatives. Pediatric formulations platform.Inter-Agency Agreement between theEunice Kennedy Shriver National Instituteof Child Health and Human Development(NICHD) and the US Food and Drug Ad-ministration (FDA). Available at: http://bpca.nichd.nih.gov/collaborativeefforts/initiatives/index.cfm. Accessed August 15. 2013
22. European Medicines Agency. Draft 5-yearreport to the European Commission:general report on the experience ac-quired as a result of the application of thePaediatric Regulation. July 8, 2012; EMA/428172/2012
23. van Riet-Nales DA, de Jager KE, SchobbenAF, Egberts TC, Rademaker CM. The avail-ability and age-appropriateness of medi-cines authorized for children in TheNetherlands. Br J Clin Pharmacol. 2011;72(3):465–473
24. Balakrishnan K, Grieve J, Tordoff J, NorrisP, Reith D. Pediatric licensing status andthe availability of suitable formulationsfor new medical entities approved inthe United States between 1998 and2002. J Clin Pharmacol. 2006;46(9):1038–1043
25. Moore P. Children are not small adults.Lancet. 1998;352(9128):630
26. Kearns GL, Abdel-Rahman SM, Alander SW,Blowey DL, Leeder JS, Kauffman RE. De-velopmental pharmacology—drug dispo-sition, action, and therapy in infants andchildren. N Engl J Med. 2003;349(12):1157–1167
27. Fernandez E, Perez R, Hernandez A, TejadaP, Arteta M, Ramos JT. Factors and mech-anisms for pharmacokinetic differencesbetween pediatric population and adults.Pharmaceutics. 2011;3(1):53–72
28. European Medicines Agency (EMEA) 2000:ICH Topic E 11. Clinical Investigations of
Medicinal Products in the PaediatricPopulation. EMEA/CHMP/ICH/2711/99
29. Allegaert K. Neonates need tailored drugformulations. World J Clin Pediatr. 2013;2(1):1–5
30. Noel GJ, Van Den Anker JN, Lombardi D,Ward R. Improving drug formulations forneonates: making a big difference in oursmallest patients. J Pediatr. 2012;161(5):947–949
31. Bartelink IH, Rademaker CM, Schobben AF,van den Anker JN. Guidelines on paediat-ric dosing on the basis of developmentalphysiology and pharmacokinetic consid-erations. Clin Pharmacokinet. 2006;45(11):1077–1097
32. Strolin Benedetti M, Whomsley R, BaltesEL. Differences in absorption, distribution,metabolism and excretion of xenobioticsbetween the paediatric and adult pop-ulations. Expert Opin Drug Metab Toxicol.2005;1(3):447–471
33. Strolin Benedetti M, Baltes EL. Drug me-tabolism and disposition in children.Fundam Clin Pharmacol. 2003;17(3):281–299
34. Meissner HC, Smith AL. The current statusof chloramphenicol. Pediatrics. 1979;64(3):348–356
35. Albani M, Wernicke I. Oral phenytoin ininfancy: dose requirement, absorption,and elimination. Pediatr Pharmacol (NewYork). 1983;3(3–4):229–236
36. Food and Drug Administration. Specificrequirements on content and format oflabeling for human prescription drugs:revision of “Pediatric Use” subsection inthe labeling; final rule. 21 CFR Part 201(Docket No 92N-0165). Federal Register:December 13, 1994. Available at: http://www.fda.gov/ohrms/dockets/ac/01/briefing/3778b1_Tab6_7-21CFR%20Part%20201.pdfAccessed August 15, 2013
37. Matsui D. Assessing the palatability ofmedications in children. Paediatr PerinatDrug Ther. 2007;8(2):55–60
38. Cram A, Breitkreutz J, Desset-Brèthes S,Nunn T, Tuleu C; European PaediatricFormulation Initiative (EuPFI). Challengesof developing palatable oral paediatricformulations. Int J Pharm. 2009;365(1–2):1–3
39. Mennella JA, Beauchamp GK. Optimizingoral medications for children. Clin Ther.2008;30(11):2120–2132
40. Davies EH, Tuleu C. Medicines for children:a matter of taste. J Pediatr. 2008;153(5):599–604, e1–e2
41. Tuleu C, Breitkreutz J. Educational paper:formulation-related issues in pediatric
clinical pharmacology. Eur J Pediatr. 2013;172(6):717–720
42. Clapham D, Kirsanov D, Legin A, Rudnitskaya A,Saunders K. Assessing taste without usinghumans: rat brief access aversion model andelectronic tongue. Int J Pharm. 2012;435(2):137–139
43. Breitkreutz J, Wessel T, Boos J. 13. Dosageforms for oral drug administration. In:Choonara I, Nunn T, Kearns G, eds. In-troduction to Paediatric and PerinatalDrug Therapy. Nottingham, UK: Notting-ham University Press;2003:189–205
44. Sam T, Ernest TB, Walsh J, Williams JL;European Paediatric Formulation Initia-tive. (EuPFI). A benefit/risk approach to-wards selecting appropriate pharmaceuticaldosage forms—an application for paediatricdosage form selection. Int J Pharm. 2012;435(2):115–123
45. Shea KM; American Academy of PediatricsCommittee on Environmental Health. Pe-diatric exposure and potential toxicity ofphthalate plasticizers. Pediatrics. 2003;111(6 pt 1):1467–1474
46. Haishima Y, Matsuda R, Hayashi Y, HasegawaC, Yagami T, Tsuchiya T. Risk assessmentof di(2-ethylhexyl)phthalate released fromPVC blood circuits during hemodialysisand pump-oxygenation therapy. Int J Pharm.2004;274(1–2):119–129
47. Allegaert K, Anderson BJ, Vrancken M,et al. Impact of a paediatric vial on themagnitude of systematic medication errorsin neonates. Paediatr Perinat Drug Ther.2006;7(2):59–63
48. Mulberg A, Silber S, van den Anker J, eds.Pediatric Drug Development. Conceptsand Applications. Hoboken, NJ: J. Wiley &Sons; 2009
49. UNICEF/WHO. Priority essential medicinesfor child survival report, Copenhagen,Denmark. Available at: www.who.int/child-medicines/progress/Unicef_prioriry_meds_child_survival.pdf. Accessed August 15, 2013
50. Fabiano V, Mameli C, Zuccotti GV. Paediatricpharmacology: remember the excipients.Pharmacol Res. 2011;63(5):362–365
51. Nahata MC. Safety of “inert” additives orexcipients in paediatric medicines. ArchDis Child Fetal Neonatal Ed. 2009;94(6):F392–F393
52. American Academy of Pediatrics Commit-tee on Drugs. “Inactive” ingredients inpharmaceutical products: update (subjectreview). Pediatrics. 1997;99(2):268–278
53. Hiller JL, Benda GI, Rahatzad M, et al.Benzyl alcohol toxicity: impact on mortal-ity and intraventricular hemorrhage amongvery low birth weight infants. Pediatrics.1986;77(4):500–506
STATE-OF-THE-ART REVIEW ARTICLE
PEDIATRICS Volume 134, Number 2, August 2014 369
by guest on May 4, 2018http://pediatrics.aappublications.org/Downloaded from
54. Shehab N, Lewis CL, Streetman DD, DonnSM. Exposure to the pharmaceuticalexcipients benzyl alcohol and propyleneglycol among critically ill neonates.Pediatr Crit Care Med. 2009;10(2):256–259
55. American Academy of Pediatrics. Ethanolin liquid preparations intended for chil-dren. Pediatrics. 1984;73(3):405–407
56. Arulanantham K, Genel M. Central nervoussystem toxicity associated with ingestionof propylene glycol. J Pediatr. 1978;93(3):515–516
57. Martin G, Finberg L. Propylene glycol:a potentially toxic vehicle in liquid dosageform. J Pediatr. 1970;77(5):877–878
58. MacDonald MG, Getson PR, Glasgow AM,Miller MK, Boeckx RL, Johnson EL. Pro-pylene glycol: increased incidence ofseizures in low birth weight infants. Pe-diatrics. 1987;79(4):622–625
59. Glasgow AM, Boeckx RL, Miller MK, Mac-Donald MG, August GP, Goodman SI.Hyperosmolality in small infants due topropylene glycol. Pediatrics. 1983;72(3):353–355
60. Balistreri WF, Farrell MK, Bove KE. Lessonsfrom the E-Ferol tragedy. Pediatrics. 1986;78(3):503–506
61. US Food and Drug Administration. DrugSafety Communication: Serious HealthProblems Seen in Premature Babies GivenKaletra (Lopinavir/Ritonavir) Oral Solution.Available at: www.fda.gov/Drugs/DrugSaf-ety/ucm246002.htm. Accessed August 15,2013
62. Whittaker A, Currie AE, Turner MA, FieldDJ, Mulla H, Pandya HC. Toxic additives inmedication for preterm infants. Arch DisChild Fetal Neonatal Ed. 2009;94(4):F236–F240
63. Lass J, Naelapää K, Shah U, et al. Hospi-talised neonates in Estonia commonly re-ceive potentially harmful excipients. BMCPediatr. 2012;12:136
64. Salunke S, Giacoia GP, Tuleu C. The STEP(safety and toxicity of excipients for paedi-atrics) database. Part 1-A need assessmentstudy. Int J Pharm. 2012;435(2):101–111
65. Salunke S, Brandys B, Giacoia GP, Tuleu C.The STEP (Safety and Toxicity of Excipientsfor Paediatrics) database: part 2—the pilotversion. Int J Pharm. 2013;457(1):310–322
66. Paediatric Formulation Initiative. STEPdatabase: database of safety and toxicityof excipients for paediatrics. Available at:www.eupfi.org/gpage11.html. Accessed Au-gust 15, 2013
67. Turner MA, Storme T. European Study forNeonatal Excipient Exposure (ESNEE). EurJ Hosp Pharm. 2012;19(2):67
68. Schirm E, Tobi H, de Vries TW, Choonara I,De Jong-van den Berg LT. Lack of appro-priate formulations of medicines forchildren in the community. Acta Paediatr.2003;92(12):1486–1489
69. Milne CP, Bruss JB. The economics of pe-diatric formulation development for off-patent drugs. Clin Ther. 2008;30(11):2133–2145
70. Institute of Medicine (US) Committee onClinical Research Involving Children. Thenecessity and challenges of clinical re-search involving children. In: Field M,Behrman R, eds. Ethical Conduct of Clini-cal Research Involving Children. Wash-ington, DC: National Academies Press;2004
71. Institute of Medicine (US). Addressing thebarriers to pediatric drug development:Workshop summary. Forum on Drug Dis-covery, Development, and Translation.Washington, DC: The National AcademiesPress; 2008
72. Balakrishnan K, Tordoff J, Norris P, ReithD. Establishing a baseline for the moni-toring of medicines availability for chil-dren in the UK: 1998-2002. Br J ClinPharmacol. 2007;63(1):85–91
73. Chui J, Tordoff J, Kennedy J, Reith D.Trends in accessibility to medicinesfor children in New Zealand: 1998–2002. Br J Clin Pharmacol. 2004;57(3):322–327
74. Chui J, Tordoff J, Reith D. Changes inavailability of paediatric medicines inAustralia between 1998 and 2002. Br JClin Pharmacol. 2005;59(6):736–742
75. Osterberg RE. 4. FDA Approach to Pediat-ric Testing. In: Hoberman AM, Lewis EM,eds. Pediatric Nonclinical Drug Testing:Principles, Requirements, and Practices.Hoboken, NJ: John Wiley & Sons, Inc; 2012:59–78
76. European Medicines Agency. Report onthe survey of all paediatric uses of me-dicinal products in Europe. December 10,2010, EMA/794083/2009
77. Tobias LD, Harkness J. IAPO Briefing Paperon Paediatric Medicines and Clinical Re-search (November 2006). InternationalAlliance of Patients’ Organizations (IAPO)Available at: www.patientsorganizations.org/paediatrics. Accessed May 23, 2014
78. Nahata MC, Allen LV Jr. Extemporaneousdrug formulations. Clin Ther. 2008;30(11):2112–2119
79. Choonara I, Conroy S. Unlicensed and off-label drug use in children: implicationsfor safety. Drug Saf. 2002;25(1):1–5
80. European Medicines Agency. Evidence ofHarm From Off-Label or Unlicensed Med-
icines in Children. EMEA/126327. EMEA;2004
81. Shah SS, Hall M, Goodman DM, et al. Off-label drug use in hospitalized children.Arch Pediatr Adolesc Med. 2007;161(3):282–290
82. Cuzzolin L, Atzei A, Fanos V. Off-label andunlicensed prescribing for newborns andchildren in different settings: a review ofthe literature and a consideration aboutdrug safety. Expert Opin Drug Saf. 2006;5(5):703–718
83. Pandolfini C, Bonati M. A literature reviewon off-label drug use in children. Eur JPediatr. 2005;164(9):552–558
84. Lowey A, Jackson M. Handbook of Ex-temporaneous Formulation—A Guide toPharmaceutical Compounding. London,UK: Pharmaceutical Press; 2010
85. Best BM, Capparelli EV, Diep H, et al.Pharmacokinetics of lopinavir/ritonavircrushed versus whole tablets in chil-dren. J Acquir Immune Defic Syndr. 2011;58(4):385–391
86. Kairuz TE, Gargiulo D, Bunt C, Garg S.Quality, safety and efficacy in the ‘off-label’use of medicines. Curr Drug Saf. 2007;2(1):89–95
87. PharmInfoTech. eMixt database: databaseof oral liquid formulations. Available at: www.pharminfotech.co.nz/manual/Formulation/mixtures/. Accessed August 15, 2013
88. Boots I, Sukhai RN, Klein RH, et al. Stim-ulation programs for pediatric drug re-search—do children really benefit? Eur JPediatr. 2007;166(8):849–855
89. European Medicines Agency. General re-port on the experience acquired as a re-sult of the application of the PaediatricRegulation. Summary of the replies tothe public consultation. SANCO/D5/FS/ci D(2013) 27105 Available at: http://ec.europa.eu/health/files/paediatrics/2013_pc_paedi-atrics/2013_paediatric_report_summary.pdf. Accessed August 15, 2013
90. Best Pharmaceuticals for Children Act(BPCA). Priority List of Needs in PediatricTherapeutics, 2012. Eunice KennedyShriver National Institute of Child Healthand Human Development (NICHD). BestPharmaceuticals for Children Act. Availableat: http://bpca.nichd.nih.gov/prioritization/upload/2012_Priority_List_FINAL.pdf. AccessedAugust 15, 2013
91. European Medicines Agency. Revised pri-ority list for studies into off-patent pae-diatric medicinal products. EMA/98717/2012, August 2013. Available at: www.ema.europa.eu/docs/en_GB/document_library/Other/2009/10/WC500004017.pdf. AccessedAugust 15, 2013
370 IVANOVSKA et al
by guest on May 4, 2018http://pediatrics.aappublications.org/Downloaded from

92. World Health Organization. Report of theinformal expert meeting on dosage formsof medicines for children. WHO Headquar-ters, Geneva, Switzerland, 2008. Available at:www.who.int/selection_medicines/committees/expert/17/application/paediatric/Dosage_form_reportDEC2008.pdf. Accessed August15, 2013
93. World Health Organization. WHO model listof essential medicines for children, 4thlist. WHO, Geneva, April 2013. www.who.int/medicines/publications/essentialmedicines/4th_EMLc_FINAL_web_8Jul13.pdf. AccessedAugust 15, 2013
94. World Health Organization. Priority life-saving medicines for women and children2012 Geneva, WHO/EMP/MAR/2012. Availableat: http://apps.who.int/iris/bitstream/10665/75154/1/WHO_EMP_MAR_2012.1_eng.pdf.Accessed August 15, 2013
95. World Health Organization. WHO ModelFormulary for Children. WHO, Geneva,Available at: www.who.int/selection_me-dicines/list/WMFc_2010.pdf. Accessed Au-gust 15, 2013
96. World Health Organization. Maternal,newborn, child and adolescent health.Documents on child health. Available at:www.who.int/maternal_child_adolescent/documents/child/en/. Accessed August 15,2013
97. World Health Organization. WHO List ofPrequalified Medicinal Products. Availableat: http://apps.who.int/prequal/97. AccessedAugust 15, 2013
98. National Institutes of Health (NICHD)Funding Opportunities. Development ofappropriate pediatric formulations andpediatric drug delivery systems (R01, R03,R21, R41/R43). Available at: http://grants.nih.gov/grants/guide. Accessed August 15,2013
99. Zajicek A. The National Institutes ofHealth and the Best Pharmaceuticals forChildren Act. Paediatr Drugs. 2009;11(1):45–47
100. European Commission. EU Research Proj-ects FP7 Health. CORDIS (Community Re-search and Development Information Centre).Available at: http://cordis.europa.eu/projects/home_en.html. Accessed August 15, 2013
101. Pediatric Formulations Platform. BPCA,National Institutes of Health. Inter-agencyagreement between the Eunice KennedyShriver National Institute of Child Healthand Human Development (NICHD) and theUS Food and Drug Administration (FDA). Oralformulations platform–report 1. Available at:http://bpca.nichd.nih.gov/collaborativeefforts/initiatives/upload/Formulations_Table_for_Web_11-02-11.pdf Accessed August 15, 2013
102. Nunn T, Williams J. Formulation of medi-cines for children. Br J Clin Pharmacol.2005;59(6):674–676
103. Stoltenberg I, Winzerburg G, Breitkreutz J.Solid oral forms for children—formulations,excipients and acceptance issues. J AppTher Res. 2010;7(4):141–146
104. Abdulla S, Sagara I, Borrmann S, et al.Efficacy and safety of artemether-lumefantrine dispersible tablets com-pared with crushed commercial tabletsin African infants and children with un-complicated malaria: a randomised, single-blind, multicentre trial. Lancet. 2008;372(9652):1819–1827
105. Kayitare E, Vervaet C, Ntawukulilyayo JD,Seminega B, Bortel V, Remon JP. De-velopment of fixed dose combination tab-lets containing zidovudine and lamivudinefor paediatric applications. Int J Pharm.2009;370(1–2):41–46
106. Vanprapar N, Cressey TR, ChokephaibulkitK, et al. IMPAACT P1056 Team. A chewablepediatric fixed-dose combination tablet ofstavudine, lamivudine, and nevirapine:pharmacokinetics and safety comparedwith the individual liquid formulations inhuman immunodeficiency virus-infectedchildren in Thailand. Pediatr Infect Dis J.2010;29(10):940–944
107. Chokephaibulkit K, Cressey TR, CapparelliE, et al; IMPAACT P1069 Team. Pharmaco-kinetics and safety of a new paediatricfixed-dose combination of zidovudine/lamivudine/nevirapine in HIV-infected chil-dren. Antivir Ther. 2011;16(8):1287–1295
108. Larka. Press release. Aptalis announcesEuropean Commission approval for newformulation of Viread. Available at: www.pharmaceutical-technology.com/contractors/drug_delivery/eurand/pressaptalis-ec-approval-new-formulation-of-viread.html. AccessedAugust 15, 2013
109. Eisai Inc. Press release. FDA approvesACIPHEX Sprinkle (Rabeprazole Sodium)for use in children ages 1 to 11. Availableat: http://us.eisai.com/wps/wcm/connect/Eisai/Home/Press+Room/Press+Releases/2013/FDAapprovesaciphexsprinkle.html.Accessed August 15, 2013
110. World Health Organization. Benznidazole:child-adapted dosage form approved. WHODrug Information. 2012;26(1):21–22
111. Food and Drug Administration. Lamictalmedication guide. Available at: www.fda.gov/downloads/Drugs/DrugSafety/UCM152835.pdf. Accessed August 15, 2013
112. Drug Information online. Press release 2012:FDA approves Zuplenz. Available at: www.drugs.com/newdrugs/fda-approves-strativa-pharmaceuticals-zuplenz-ondansetron-oral-
soluble-film-2208.html. Accessed August 15,2013
113. Stoltenberg I, Breitkreutz J. Orally dis-integrating mini-tablets (ODMTs)—anovel solid oral dosage form for paedi-atric use. Eur J Pharm Biopharm. 2011;78(3):462–469
114. Pfizer Medic and News 2009. Pfizer an-nounces European Union approval of anew form of Lipitor (atorvastatin) for usein children. Available at: http://press.pfizer.com/press-release/pfizer-announces-european-union-approval-new-form-lipitor-atorvastatin-use-children. Accessed August 15, 2013
115. Merck News Room. FDA approves Merck’sISENTRESS (raltegravir) for use in chil-dren ages two years and older as part ofHIV-1 combination therapy. Available at:www.mercknewsroom.com/press-release/prescription-medicine-news/fda-approves-mercks-isentress-raltegravir-use-children-ages. Accessed August 15, 2013
116. Breitkreutz J. Arzneiformen für Kinder.Nach der EU-Reform. Pharmazie in unsererZeit 2009;38(1):30–37.
117. Yeung VW, Wong IC. When do childrenconvert from liquid antiretroviral to solidformulations? Pharm World Sci. 2005;27(5):399–402
118. Garvie PA, Lensing S, Rai SN. Efficacy ofa pill-swallowing training intervention toimprove antiretroviral medication adher-ence in pediatric patients with HIV/AIDS.Pediatrics. 2007;119(4). Available at:www.pediatrics.org/cgi/content/full/119/4/e893
119. Thomson SA, Tuleu C, Wong IC, Keady S, PittKG, Sutcliffe AG. Minitablets: new modality todeliver medicines to preschool-aged children.Pediatrics. 2009;123(2): Available at www.pe-diatrics.org/cgi/content/full/123/2/e235
120. Spomer N, Klingmann V, Stoltenberg I,et al. Acceptance of uncoated mini-tabletsin young children: results from a pro-spective exploratory cross-over study. ArchDis Child. 2012;97(3):283–286
121. Klingmann V, Spomer N, Lerch C, et al.Favorable acceptance of mini-tabletscompared with syrup: a randomized con-trolled trial in infants and preschool chil-dren. J Pediatr. 2013;163(6):1728–1732.e1
122. Walsh J, Bickmann D, Breitkreutz J,Chariot-Goulet M; European PaediatricFormulation Initiative (EuPFI). Deliverydevices for the administration of paedi-atric formulations: overview of currentpractice, challenges and recent develop-ments. Int J Pharm. 2011;415(1–2):221–231
123. World Health Organization. Priority medi-cines for Europe and the World UpdateReport. WHO Geneva, 2013. Available at:
STATE-OF-THE-ART REVIEW ARTICLE
PEDIATRICS Volume 134, Number 2, August 2014 371
by guest on May 4, 2018http://pediatrics.aappublications.org/Downloaded from

www.who.int/medicines/areas/priority_medicines/en/. Accessed August 15, 2013
124. Ricci BM. Bridging studies in support oforal pediatric formulation development.Int J Pharm. 2013;457(1):323–326
125. Havenaar R, Anneveld B, Hanff LM, et al.In vitro gastrointestinal model (TIM) withpredictive power, even for infants andchildren? Int J Pharm. 2013;457(1):327–332
126. Dunne J, Rodriguez WJ, Murphy MD, et al.Extrapolation of adult data and other datain pediatric drug-development programs.Pediatrics. 2011;128(5). Available at: www.pediatrics.org/cgi/content/full/128/5/e1242
127. Giacoia GP, Taylor-Zapata P, Zajicek A.Eunice Kennedy Shriver National Institute
of Child Health and Human DevelopmentPediatrics Formulation Initiative: proceed-ings from the Second Workshop on Pedi-atric Formulations. Clin Ther. 2012;34(11):S1–S10
128. Menjoge AR, Kannan RM, Tomalia DA.Dendrimer-based drug and imaging con-jugates: design considerations for nano-medical applications. Drug Discov Today.2010;15(5–6):171–185
129. Timko BP, Kohane DS. Materials to clinicaldevices: technologies for remotely triggereddrug delivery. Clin Ther. 2012;34(11):S25–S35
130. Krishnan V, Xu X, Barwe SP, et al.Dexamethasone-loaded block copolymernanoparticles induce leukemia cell death
and enhance therapeutic efficacy: a novelapplication in pediatric nanomedicine.Mol Pharm. 2013;10(6):2199–2210
131. van Riet-Nales DA, Schobben AF, EgbertsTC, Rademaker CM. Effects of the phar-maceutical technologic aspects of oralpediatric drugs on patient-related out-comes: a systematic literature review. ClinTher. 2010;32(5):924–938
132. United States Government AccountabilityOffice. Pediatric medical devices. Provi-sions support development, but betterdata needed for required reporting. Re-port to Congressional Committees. Avail-able at: www.gao.gov/assets/590/587164.pdf. Accessed August 15, 2013
POUTINE: Church Street is a pedestrian street that runs through the heart ofdowntown Burlington, Vermont. During the summer and fall, the street iscrowded with food vendors selling all kinds of different foods. However, as re-quired by city ordinance, street vendors may only sell foods that do not directlycompete with restaurants on or immediately adjacent to Church Street. That isthe reason no food vendors sell pizza or hamburgers. Just recently, though, Inoticed a new vendor on the street selling poutine, a Canadian dish made ofFrench fries and nuggets of curd cheese smothered in gravy. As reported in TheWall Street Journal (In Search Of: May 2, 2014), poutine is not classically asso-ciated with fine dining. In fact, there is a debate as to whether something such as“great poutine” even exists. Still, the dish seems to exploding in popularity,moving from humble trucks stops and cafes in rural Quebec to fine diningestablishments in New York and Chicago. The roots of poutine are a bit myste-rious. Some say the dish was created in the mid-20th century after a cook inWarwick, Quebec, mixed the ingredients together with vinegar in a waxed paperbag and after the resultant explosion, labeled the concoction a “maudite poutine”— a blastedmess. Most aficionados report the “best” poutine includes very freshcheese curds, crisp French fries, and homemade brown gravy-preferably one thatwould do justice to a fine rib roast. Recently, restaurateurs have begun exper-imenting with all sorts of additional ingredients, but classic poutine has onlythree. Regardless of the quality of the ingredients, however, the dish is certainlynot light. Still, it is a wonderful guilty pleasure that I partake of at least oncea summer. Now I will not have to travel to a particular small town in upstate NewYork or Montreal, my traditional spots for poutine, but can savor the dish righthere in my own town.
Noted by WVR, MD
372 IVANOVSKA et al
by guest on May 4, 2018http://pediatrics.aappublications.org/Downloaded from

DOI: 10.1542/peds.2013-3225 originally published online July 14, 2014; 2014;134;361Pediatrics
Mantel-TeeuwisseVerica Ivanovska, Carin M.A. Rademaker, Liset van Dijk and Aukje K.Pediatric Drug Formulations: A Review of Challenges and Progress
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/134/2/361including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/134/2/361.full#ref-list-1This article cites 83 articles, 15 of which you can access for free at:
Subspecialty Collections
s_subhttp://classic.pediatrics.aappublications.org/cgi/collection/therapeuticTherapeuticsfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
https://shop.aap.org/licensing-permissions/in its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.pediatrics.aappublications.org/content/reprintsInformation about ordering reprints can be found online:
ISSN: . 60007. Copyright © 2014 by the American Academy of Pediatrics. All rights reserved. Print American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since . Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on May 4, 2018http://pediatrics.aappublications.org/Downloaded from
DOI: 10.1542/peds.2013-3225 originally published online July 14, 2014; 2014;134;361Pediatrics
Mantel-TeeuwisseVerica Ivanovska, Carin M.A. Rademaker, Liset van Dijk and Aukje K.Pediatric Drug Formulations: A Review of Challenges and Progress
http://pediatrics.aappublications.org/content/134/2/361located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: . 60007. Copyright © 2014 by the American Academy of Pediatrics. All rights reserved. Print American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since . Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on May 4, 2018http://pediatrics.aappublications.org/Downloaded from


















