
PEDIATRIC CARDIOLOGY - vfn.cz · atrial septal defect ... to maintain pda patency (tga)...
68
PEDIATRIC CARDIOLOGY Zuzana Urbanová
Transcript of PEDIATRIC CARDIOLOGY - vfn.cz · atrial septal defect ... to maintain pda patency (tga)...

PEDIATRIC CARDIOLOGY
Zuzana Urbanová
HISTORY
• Family history (sudden death, SIDS,
structural cardiac abnormality)
• Pregnancy (gestational diabetes
mellitus, chronic maternal illness,
congenital infections, drug use)
• Perinatal course
• Symptoms

SYMPTOMS AND SIGNS OF
HEART DISEASE
• rate of growth and development
• history of past illnesses
• feeding difficulties-congestive heart
failure (30% infants with CHD)
• tachypnea, dyspnea, grunting, flaring of
the alae nasi
• cyanosis (reduced hemoglobin >3-5gm%)

PHYSICAL EXAMINATION
• height, weight - growth chart
• heart and respiratory values
rate/min birth-6w 6w-2y 2-6y 6-10y over 10y
resp. 45-60 40 30 25 20
heart 125±30 115±25 100±20 90±15 85±15
• blood pressure measurement
appropriately sized cuffs, covers 2/3 of the full length of the arm

PHYSICAL EXAMINATION
• Arterial examination (radial and femoral
pulse - volume, character, delay) - CoA
• Venous examination - generally difficult or
impossible in infants and children
• Liver - position, size, consistency (1-2 cm
below the right costal margin by 1 year of
age)
• Precordial examination (bulge, thrills,
apical impulse)

DIAGNOSIS OF CHD
• PHYSICAL EXAMINATION
• BLOOD PRESSURE MEASUREMENT
• ECG , X-RAY
• ECHOCARDIOGRAPHY
• CARDIAC CATETRIZATION
• HOLTER MONITORING
• EXERCISE TESTING
AUSCULTATION
• under optimal condition
• supine, sitting and standing position
• first heart sound - atrioventricular valves closure
• second heart sound - aortic and pulmonary valve closure ( split during inspiration)
• cardiac murmurs

CARDIAC MURMURS
• systolic, diastolic, continuous
• intensity: graded as 1-6 / 6
1. heard with intense concentration
2. faint, but heard immediately
3. easily heard
4. associated with thrill
5. very loud
6. audible off the chest wall

INNOCENT MURMURS
OF CHILDHOOD
• Intensity grade 3 or less
• Never solely diastolic
• Never associated with thrill
• Diminishes and the pitch changes or
disappears with upright position
Vibratory Still´s, Pulmonary flow, Peripheral
pulmonary stenosis, Supraclavicular or
Brachiocephalic Systolic, Aortic systolic, Venousis hum,

ETIOLOGY OF CHD
• multifactorial
• 3% chromosomal aberrations
• 2% new mutations
• viremia during pregnancy, inflammation,
• treatment (hormones, insulin,
anticonvulsants, cytostatics)

RISK OF CHD IN FAMILY
one member two members
• VSD 3,0%
• PDA 3,0%
• ASD 2,5% 3 times higher
• TOF 2,5%
• PS 2,0%
• TGA 2,0%
• TA 1,0%
• PTA 1,0%

Fetální kardiologie

FETAL ECHOCARDIOGRAPHY

FETAL ECHOCARDIOGRAPHY HYPOPLASTIC LEFT HEART SYNDROMA

PREVALENCY OF CHD
7-8 / 1 000 newborns
40% of all congenital defects • 35% VSD
• 12% ASD
• 6% PDA, PS, AS, CoA
• 5% TGA
• 4% TOF
• 20% others
•

PREVALENCY OF CHD
ASDAS CoA
TOF
0
10
20
30
40
50
%
VSD PDA PS TGA others

CLASSIFICATION OF CHD
• ANATOMICAL
• FUNCTIONAL
LEFT-TO-RIGTT SHUNT
RIGHT-TO-LEFT SHUNT
WITHOUT SHUNT
• URGENT - NONURGENT

LEFT-TO-RIGHT SHUNT
LESIONS
• Atrial septal defect
ostium secundum, ostium primum, sinus venosus, inferior vena cava
• Ventricular septal defect
perimembranous, supracristal, atrioventricular, muscular
• Patent ductus arteriosus
• Atrioventricular septal defect
• Aorticopulmonary window

ATRIAL SEPTAL DEFECT
1. sinus venosus
2. ostium secundum
3. ostium primum
4. cleft in the MV
septal leaflet

ATRIAL SEPTAL DEFECT

ATRIAL SEPTAL DEFECT

ATRIAL SEPTAL DEFECT
• Symptoms usually after 1. year of life
• Systolic murmur –excess blood flow through
the pulmonary valve, fixed splitting of second
sound
• ECG: hypertrophy of the RV, IRBB
• X-ray: increase pulmonary vascularity
• Echocardiogram: 2D, Doppler, color mapping
• Treatment: cardiac failure, surgical, catheterization

ASD AMPLATZ

ASD – AMPLATZ

VENTRICULAR SEPTAL DEFECT
1. supracristal
2. perimembranous
3. muscular
4. apical

VENTRICULAR SEPTAL DEFECT

VENTRICULAR SEPTAL DEFECT
• Holosystolic murmur depends on the pressure (after the decrease of pulmonary vascular resistance, mostly in 2 month)
• ECG: normal or hypertrophy of LV, RV
• X-ray: increase pulmonary vascularity
• Echocardiogram: 2D, Doppler, color mapping
• Treatment: cardiac failure, surgical, catheterization

PERIMEMBRANOUS VSD

MUSCULAR VSD

VENTRICULAR SEPTAL DEFECT

SURGICAL REPAIR OF VSD

SURGICAL REPAIR OF VSD

ATRIOVENTRICULAR CANAL

PATENT DUCTUS ARTERIOSUS

PDA - ECHO

PATENT DUCTUS ARTERIOSUS

PATENT DUCTUS ARTERIOSUS
• Continuous murmur (in newborn infants systolic)
• ECG: normal or hypertrophy of LV, RV
• Chest X-ray: increase pulmonary vascularity
• Echocardiogram: 2D, Doppler, color mapping
• Treatment: surgical, catheterization, pharmacological in premature neonates
• In ductus dependent CHD prostaglandins
to maintain PDA patency (TGA)

RIGHT-TO-LEFT SHUNT
LESIONS (CYANOTIC)
MECHANISM
• 1. DECREASED PULMONARY
BLOOD FLOW ( TA, TS, PA, PS, TOF)
• 2. MALPOSITION OF GREAT
ARTERIES (TGA, DORV, DOLV,
Truncus arteriosus)
• 3. SINGLE VENTRICLE

TRICUSPID ATRESIA

TRANSPOSITION OF GREAT
ARTERIES

TRANSPOSITION OF GREAT
ARTERIES

TGA - echocardiography
PA
A
O
LV
RV

TGA-prenatal ECHO

TRANSPOSITION OF GREAT
ARTERIES
• Balloon atrial septostomy - Rashkind
• Surgical atrial switch- atrial baffle in the
atrium redirects deoxygenated blood
Mustard, Sennig procedure
ARTERIAL SWITCH
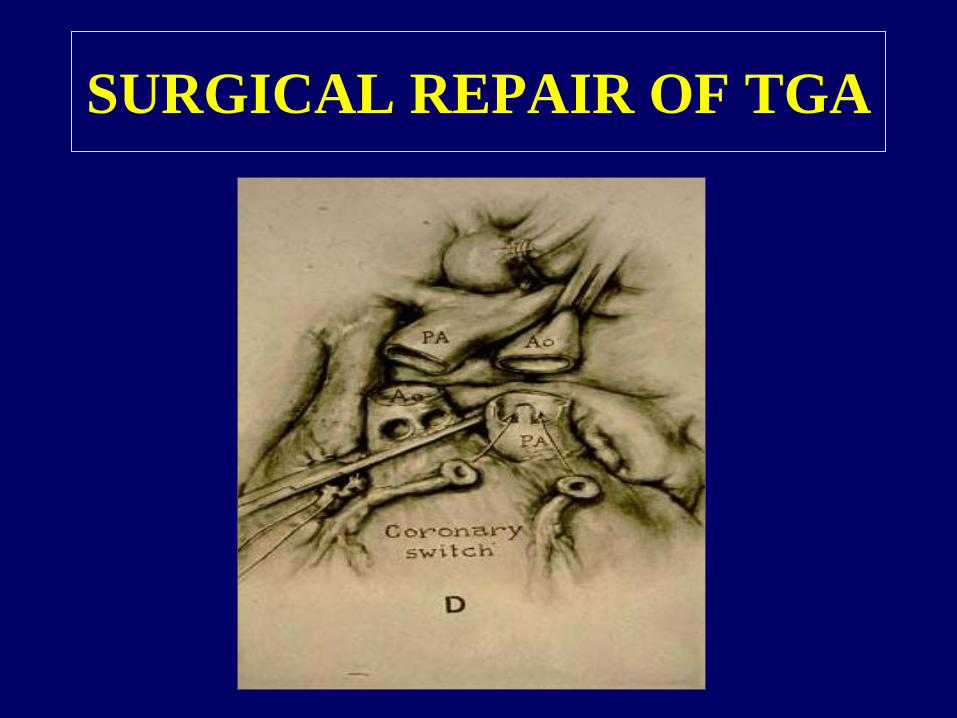
SURGICAL REPAIR OF TGA

TETRALOGY OF FALLOT
1. VSD
2. RV HYPERTROFY
3. OVERRIDING OF
AORTA
4. SUBPULMONARY
STENOSIS

TETRALOGY OF FALLOT

TOF - ECHO

TETRALOGY OF FALLOT
• Cyanosis
• Polyglobulia
• Hypoxic attacks
• Surgery: close the hole and open
obstruction

TOF repair
• Closure of VSD with pericardial
patch
• Shifting aorta to LV
• Reconstruction of right ventricle
outflow tract
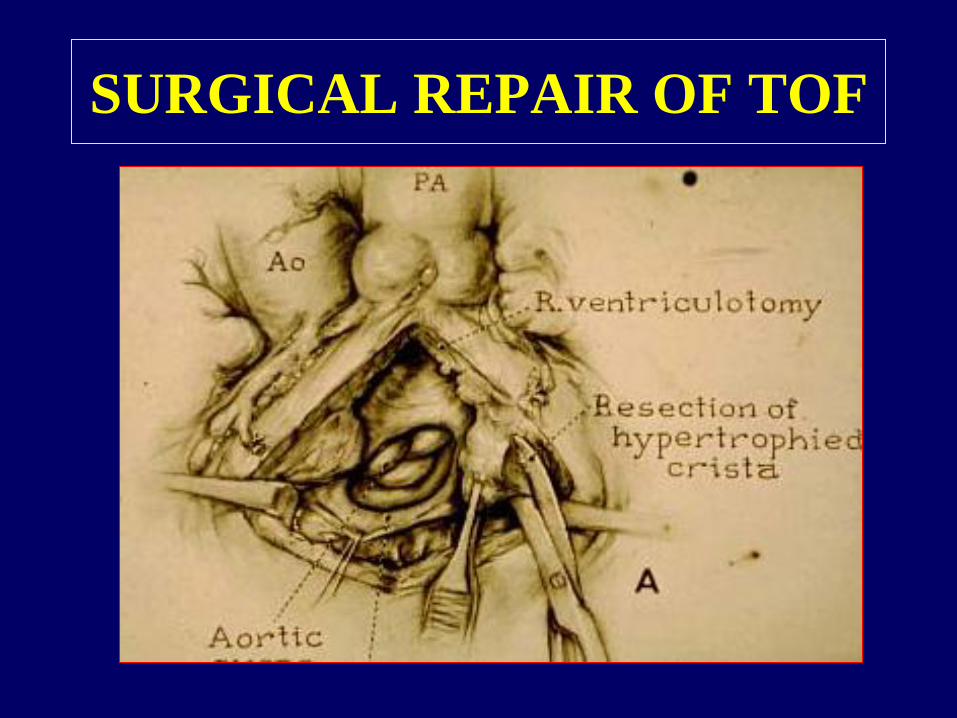
SURGICAL REPAIR OF TOF

LESIONS WITHOUT SHUNT
• PULMONARY STENOSIS
• AORTIC STENOSIS
subvalvular, valvular, supravalvular
• COARCTATION OF AORTA

PULMONARY STENOSIS
• Symptoms related to aortic or pulmonary
stenosis depend on the degree of valve
stenosis.
• Systolic ejection murmur
• ECG: normal or ventricular hypertrophy
• Echocardiography: pressure gradient
across the valve

PULMONARY STENOSIS

BALLOON DILATATION OF
CRITICAL PS

SURGICAL REPAIR OF PS

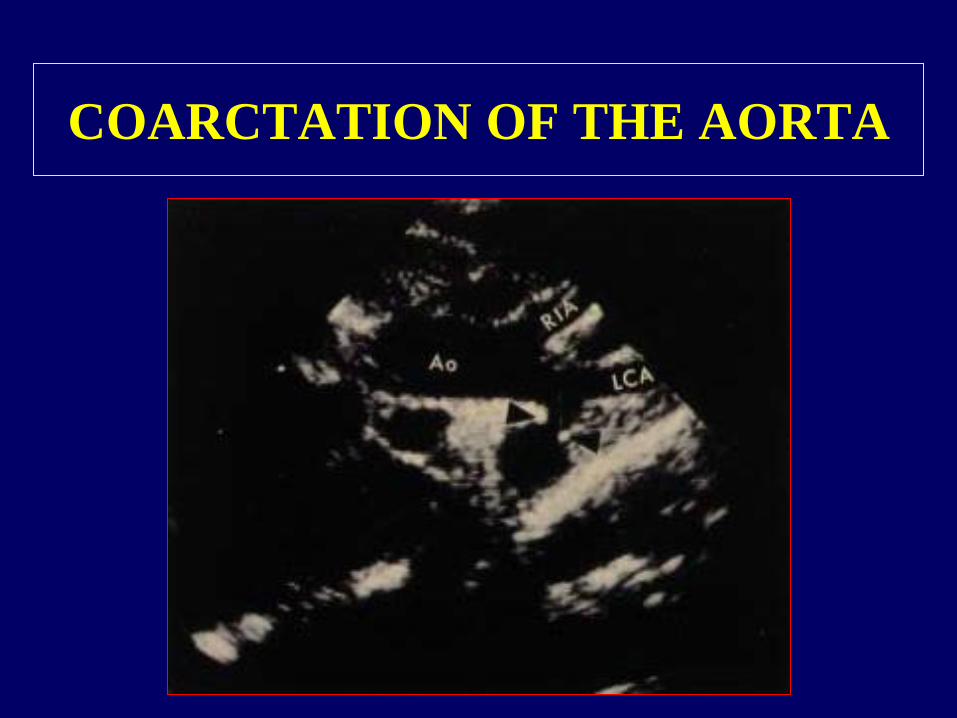
COARCTATION OF THE AORTA

COARCTATION OF THE AORTA
COARCTATION OF THE AORTA

COARCTATION OF THE AORTA

COARCTATION OF THE AORTA

INTERRUPTION OF THE
AORTIC ARCH

COARCTATION OF THE AORTA
• Clinical presentation depends on the age and
severity of the obstruction
• Preductal – critical CoA – cardiac failure in
neonates
• Postductal – elective repair between the ages 3
and 10 years
• Upper extremity hypertension, femoral pulse
• Systolic murmur medial to the left scapula

COARCTATION OF THE AORTA
surgical corrections
• Patch aortoplasty
• Subclavian flap repair
• Resection with end-to-end
anastomosis


Surgery - Kardiocentrum Prague
1977 – 2011
• 12 000 operated children
• 3096 operations before age 1
• Switch TGA 443
• TOF 199
• A-V canal 146
• TAPVD 148
• 97% survive 93% 10 years after surgery, 84% 15 years after surgery

Surgical mortality rate
Kardiocentrum Prague (1980-2010)


















