Pediatric Cardiology for the School Nurse - NEUSHA · Pediatric Cardiology for the School Nurse...
36
5/17/17 1 Pediatric Cardiology for the School Nurse Stewart Mackie, MD Pediatric Cardiologist Assistant Professor of Pediatrics Associate Residency Program Director UMass - Baystate Medical Center Disclosures: I have no financial disclosures.
-
Upload
dangkhuong -
Category
Documents
-
view
225 -
download
0
Transcript of Pediatric Cardiology for the School Nurse - NEUSHA · Pediatric Cardiology for the School Nurse...
5/17/17
1
Pediatric Cardiology for the School Nurse
Stewart Mackie, MD Pediatric Cardiologist
Assistant Professor of Pediatrics Associate Residency Program Director
UMass - Baystate Medical Center
Disclosures: I have no financial disclosures.
5/17/17
2
Further “Disclosures”
• The approach and management styles of many pediatric conditions are not evidence based, therefore different institutions/schools may have different protocols to evaluate and work up patients with possible cardiac complaints.
• This is how I would triage/evaluate these type of issues as a pediatric cardiologist, your school may or may not agree…..
Objectives
• Provide outline for routine and emergency cardiac care for school nurses to manage and treat common cardiac complaints
• Review pathophysiology and concerning clinical findings for hypertrophic cardiomyopathy and other conditions associated with sudden cardiac death
• Understand the diagnosis and implications of a diagnosis of long QT syndrome and Wolf-Parkinson-White (WPW) syndrome

5/17/17
3
Evaluation of Possible Cardiac Issues
• Starts with a good history: SAMPLE t Symptoms t Allergies t Medications t Past Medical History t Last Oral Intake t Events leading to issue
Symptoms in evaluating Chest Pain
• Character – How would you describe the pain?
• Location • Exacerbating – Is it worse with inspiration or
palpation? • Alleviating • Radiation • Severity/Other Symptoms – Have you had
recent fever/illness? Doe you have other symptoms?
• Timing – When did it start? When does it occur? How long does it last?
5/17/17
4
History
• Past Medical History t Asthma t Cardiac Disease t Kawasaki Disease t Sickle Cell Disease t Marfan t Turner Syndrome t Ehlers-Danlos t Cardiac Surgery t Thoracic Surgery
Family History • ESSENTIAL in cardiac evaluation as often family
history is positive with inherited cardiac disease • May need to call parent to get details QUESTIONS TO ASK: • Unexplained fainting, seizure or near drowning in a
family member • Premature death <50 years old due to heart disease • Anyone in family with a heart problem, pacemaker or
implanted defibrillator • Specific knowledge of certain cardiac conditions (long-
QT, other channelopathies like ARVC, CPVT or Brugada Syndrome, HOCM)
Modified from American Academy of Pediatrics Prepartication Physical Evaluation Form - http://www.aap.org/en-us/professional-resources/practice-support/pages/Preparticipation-Physical-Evaluation-Forms.aspx
5/17/17
5
Exam • Vitals signs are vital.
t Weight, Heart Rate, Blood pressure, Oxygen saturation
• Exam t General t Neck: Jugular Venous Distension t Resp t Cardiovascular
v Evaluate S1 and S2 v Assess for murmurs in multiple positions – squatting,
standing, lying, and sitting t Abdomen
v Evaluate if soft, tender, distended
Exam (cont.) t Neuro
v Alert to time, place and person – if not are they responsive to pain
v Focal deficits v PERRL (especially if with syncope/head trauma) v Gait, coordination, speech
t Skin v Bruising, rashes, abnormal chest wall shape (i.e.
pectus) t Ext
v Perfusion, cap refill v Evaluate for Cyanosis, clubbing, edema v Distal pulses
5/17/17
6
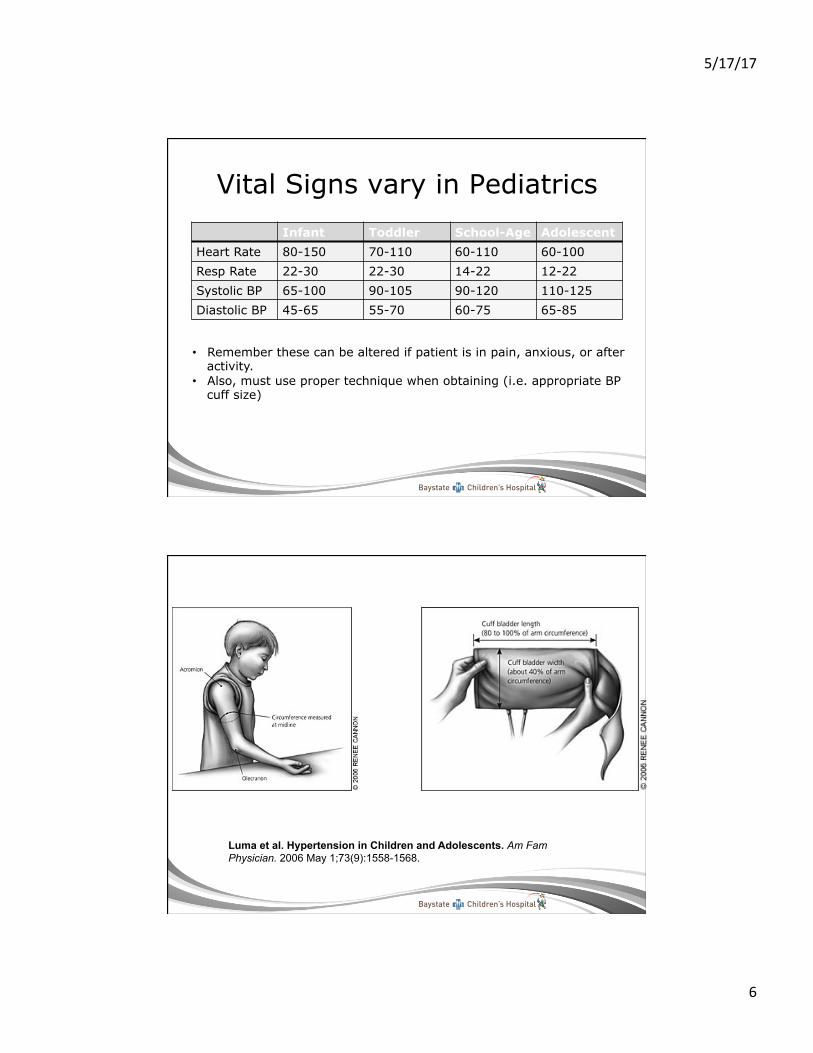
Vital Signs vary in Pediatrics Infant Toddler School-Age Adolescent
Heart Rate 80-150 70-110 60-110 60-100 Resp Rate 22-30 22-30 14-22 12-22 Systolic BP 65-100 90-105 90-120 110-125 Diastolic BP 45-65 55-70 60-75 65-85
• Remember these can be altered if patient is in pain, anxious, or after activity.
• Also, must use proper technique when obtaining (i.e. appropriate BP cuff size)
Luma et al. Hypertension in Children and Adolescents. Am Fam Physician. 2006 May 1;73(9):1558-1568.
5/17/17
7
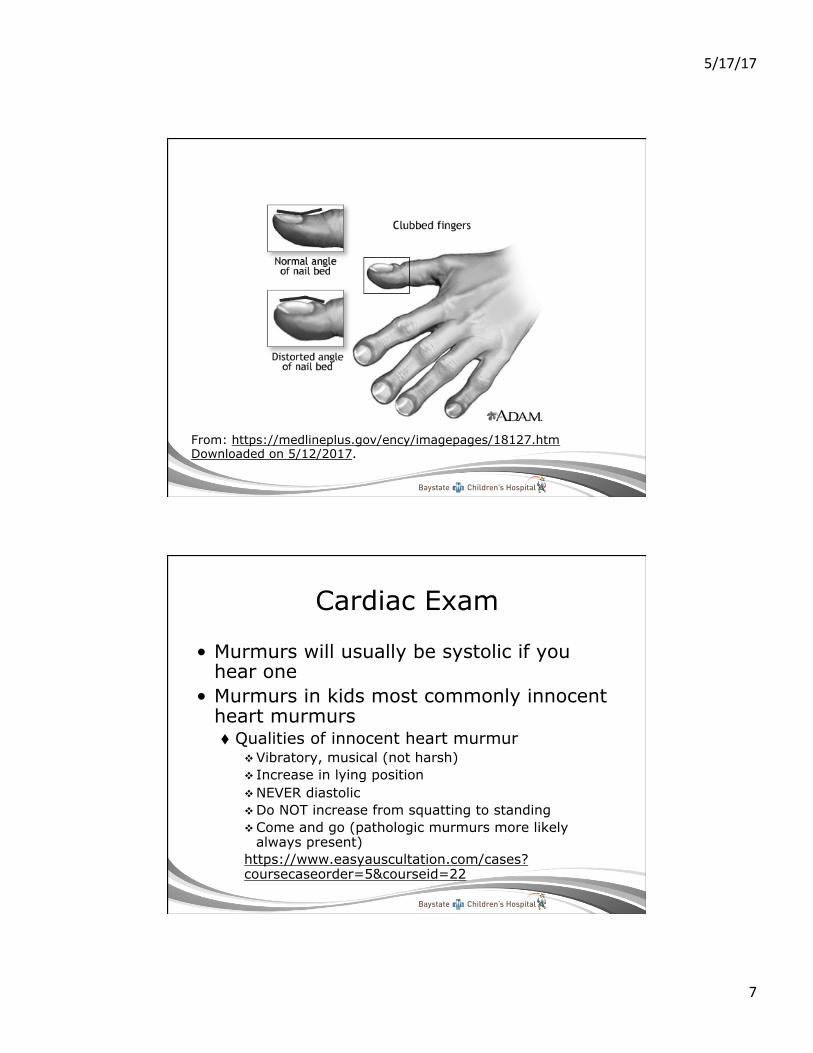
From: https://medlineplus.gov/ency/imagepages/18127.htm Downloaded on 5/12/2017.
Cardiac Exam
• Murmurs will usually be systolic if you hear one
• Murmurs in kids most commonly innocent heart murmurs t Qualities of innocent heart murmur
v Vibratory, musical (not harsh) v Increase in lying position v NEVER diastolic v Do NOT increase from squatting to standing v Come and go (pathologic murmurs more likely
always present) https://www.easyauscultation.com/cases?coursecaseorder=5&courseid=22
5/17/17
8
Pathologic Murmurs
• Typically more harsh in sound • Increase from squatting to standing • Do not get louder from sitting to laying • Diastolic murmurs https://www.easyauscultation.com/cases-listing-details?caseid=7
Some Emergent Cardiac Issues • Severe chest pain • Recurrent syncope, not c/
w vasovagal syncope • Syncope without
prodromal symptoms • Change in level of
consciousness • Bradycardia/tachycardia
• Cyanosis (sats <94% on RA)
• Persistent palpitations • or if HR persistently >180
bpm • Shortness of Breath • Poor peripheral pulses • Diaphoretic • Hypotensive • Poor perfusion (Cap refill
>2 seconds)
5/17/17
9
What to do…..
• Support airway, breathing, circulation • Activate EMS and ask for help if available • Have AED available • Continue to assess student closely with
repeat vital signs at least every 5 minutes • Contact parent/guardian • Notify school administration
Urgent Cardiac Issues
• Moderate chest pain • Vasovagal/situational syncope • Non-exertional cardiac issues • Anxiety • Patient should have stable vital signs • Family history should be reassuring • There should not be red flags
5/17/17
10
What to do…..
• Support airway, breathing, circulation • Determine need for EMS • Ensure availability of AED • Observe student closely with reassessment
of vital signs • Contact parent/guardian consider transport
student to home or medical care • Follow-up
Less Concerning Cardiac Issues
• Reproducible chest pain on palpation • Dizziness improved with hydration • Palpitations with noted normal heart rate
and regularity on your exam • Fast heart rate in anxious/agitated patient
that improves with calming down • No red flags on history/physical exam

5/17/17
11
What to do…..
• Support airway, breathing, circulation – likely fine
• Unlikely need for EMS or AED • Reassess vital signs • Contact parent/guardian to ensure no red
flags not previously disclosed • Determine need for going home with
parent/guardian and seeking medical care
Why do we care so much?
5/17/17
12
The Common Cardiac Causes of Sudden Death
• Structural/Functional t Hypertrophic Cardiomyopathy t Coronary artery anomalies t Myocarditis t ARVC (Arrhythmogenic Right Ventricular
Cardiomyopathy) t Aortic aneurysm/rupture (i.e. Marfan’s) t Mitral Valve Prolapse

5/17/17
13
Cardiac Causes of Cardiac Death
Electrical • Long QT syndrome • Wolff-Parkinson White Syndrome • Brugada Syndrome • CPVT (Catecholaminergic Polymorphic
Ventricular Tachycardia)
Distribution of cardiovascular causes of sudden death in 1435 young competitive athletes.
Maron B et al. Circulation 2007;115:1643-1655

5/17/17
14
Hypertrophic Cardiomyopathy • Thickening of the left
ventricle • Most commonly, asymmetric
septal hypertrophy but may be concentric or localized to a small segment of the septum
• Microscopically, disarray of hypertrophied myocardial cells and myocardial scarring
• Approximately 50% are Autosomal Dominant t Other 50% are sporadic
Nishimura R A et al. Circulation. 2003;108:e133-e135
Red Flags concerning for HCM
• Chest pain with exertion, worsening fatigue, exercise tolerance, syncope with exertion, palpitations, dyspnea
• Family history of HCM, SUED (+ in 30-60% of px)
5/17/17
15
Physical Examination
• Left ventricular lift and systolic thrill on palpation of the apex of the heart
• Grade 1-3/6 systolic murmur which is crescendo-decrescendo usually best appreciated at MLSB or LLSB
• +/- systolic regurgitant murmur of mitral insufficiency
PRELOAD EFFECTS DEGREE OF MURMUR
• Increase preload, decrease murmur t Squatting or hand-grip (more systemic venous return)
• Decrease preload, increase murmur t Standing or Valsalva (decreased systemic venous
return)
http://www.easyauscultation.com/cases.aspx?coursecaseorder=7&courseid=26
5/17/17
16
Treatment
• Beta-blocker/ACE Inhibitor • Myectomy • ICD • No competitive/strenous sports
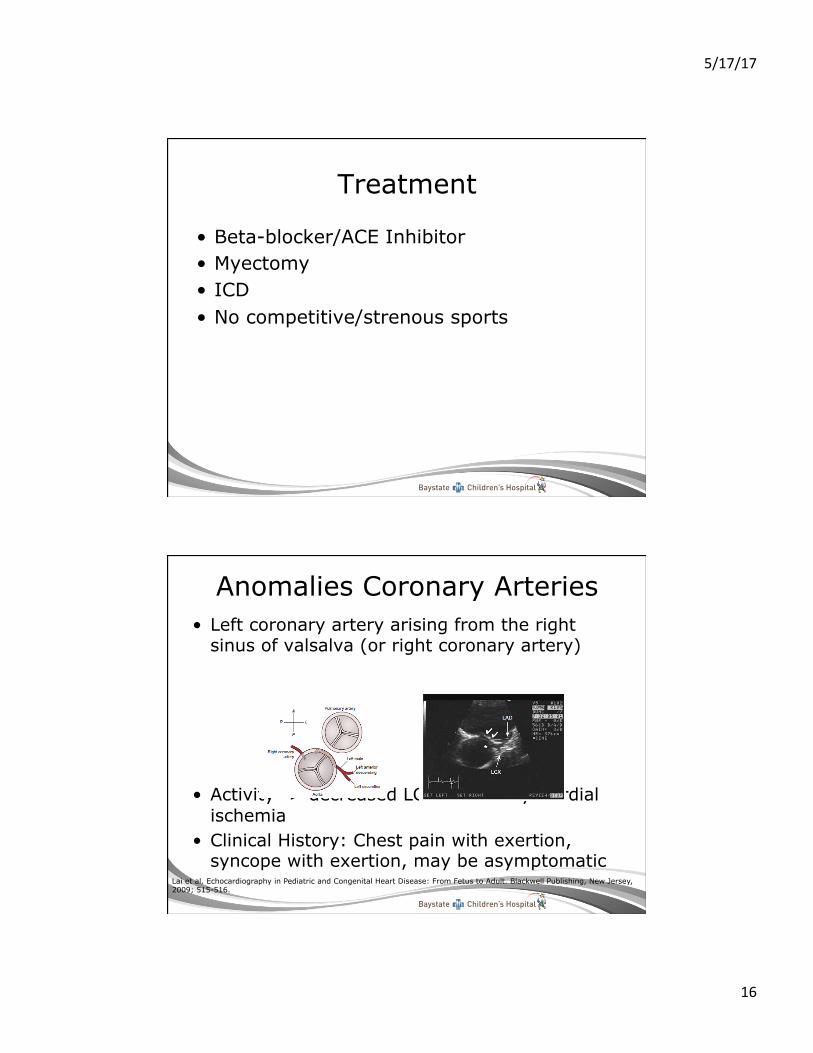
Anomalies Coronary Arteries • Left coronary artery arising from the right
sinus of valsalva (or right coronary artery)
• Activity -> decreased LCA flow-> Myocardial ischemia
• Clinical History: Chest pain with exertion, syncope with exertion, may be asymptomatic
Lai et al. Echocardiography in Pediatric and Congenital Heart Disease: From Fetus to Adult. Blackwell Publishing, New Jersey, 2009; 515-516.
5/17/17
17
Diagnoses/Treatment
• ECG may show signs of ischemia but often normal
• Echocardiography to delineate the anatomy
• Surgical correction depending on LCA course, or if symptomatic
Myocarditis
• Typically a viral infection of the heart believed to be due to a cell-mediated immunologic reaction
• History usually significant for previous URI and may have significant fatigue, poor weight gain, activity intolerance/dyspnea, and if severe cardiogenic shock
• Diagnosis mainstay is echocardiography +/- cath for biopsy
• Treatment is supportive care, ? steroids, and if severe without improvement over time possible transplant

5/17/17
18
Pericarditis
• Typically a viral infection • History usually significant for previous URI
and may have significant fatigue
• Chest pain often position – worse laying down
• PE: Friction rub • Diagnosis: CXR, echocardiography • Treatment is NSAID, ?colchicine, ?
drainage

5/17/17
19
Long QTc Syndrome • Channelopathy that can cause lethal
ventricular arrhythmia • Autosomal dominant (50% inheritance)
t ~60% of families have a positive family history
• Presentation often syncope or seizure most commonly with activity or emotion t Could present with palpitations.
• Treatment – beta-blockade, ICD • If patient with known long QTc, very low
threshold for EMS, must have AED available
5/17/17
20
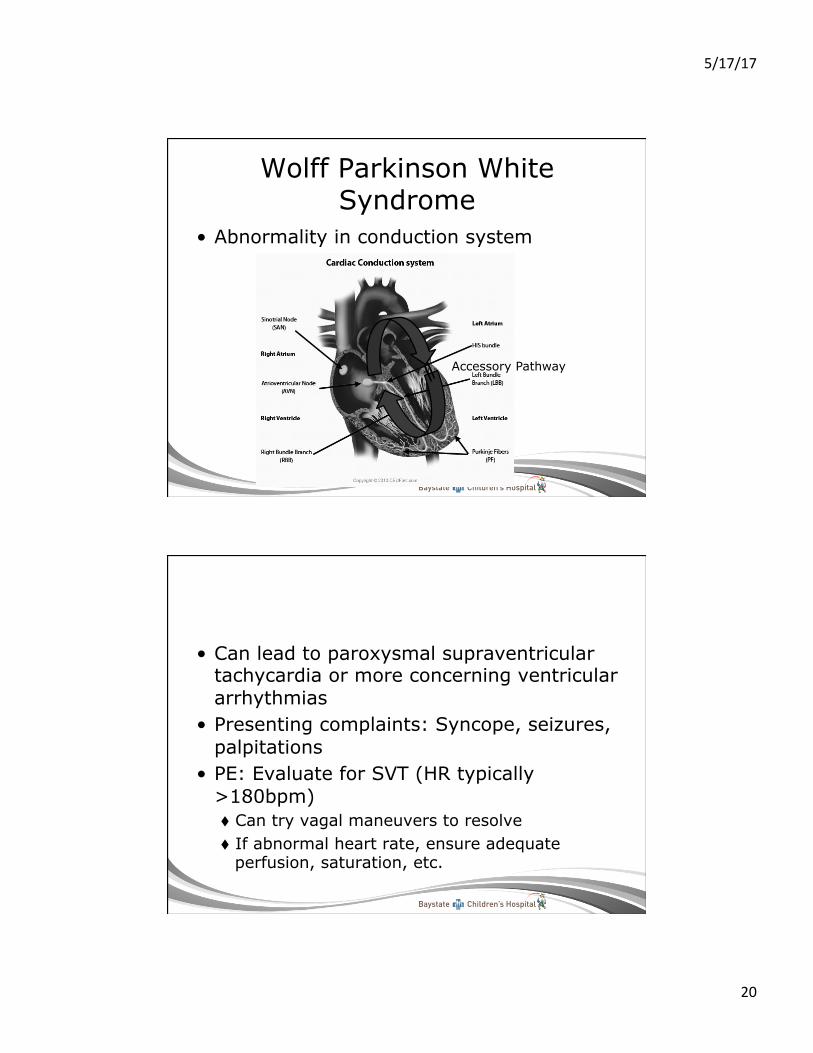
Wolff Parkinson White Syndrome
• Abnormality in conduction system
Accessory Pathway
• Can lead to paroxysmal supraventricular tachycardia or more concerning ventricular arrhythmias
• Presenting complaints: Syncope, seizures, palpitations
• PE: Evaluate for SVT (HR typically >180bpm) t Can try vagal maneuvers to resolve t If abnormal heart rate, ensure adequate
perfusion, saturation, etc.
5/17/17
21
School Resources for Long QT and other lethal arrhythmias
http://www.sads.org/
A Case
A 13 year old girl presents to the school nurse’s office with chest pain. The chest pain is mid-sternal, non-radiating, and rated as 5/10. It is described as a sharp, stabbing pain. Pain is worse with inspiration. She has not had chest pain with activity. She has had previous similar episodes of chest pain. No other symptoms with episode. No recent fever or viral URI symptoms. Mother states family history negative for sudden unexplained death, congenital heart defect, or arrhythmias.
5/17/17
22
You classify this as……
a. Emergent Chest Pain and call EMS b. Urgent Chest Pain and call parents to
immediately pick up patient and bring to medical care
c. Non-urgent chest pain most likely musculoskeletal in etiology
Chest Pain
• Most chest pain in children and adolescents is NOT caused by cardiac disease
• Figuring out a way to differentiate cardiac vs non-cardiac chest pain can be difficult
• History including family history and physical exam can give you a lot of helpful information
5/17/17
23
Non-Cardiac Chest Pain
• Musculoskeletal t Costochondritis
• Pulmonary t Asthma (most common) t Infectious (PNA, empyema) t Pleurisy t Acute Chest – Sickle Cell Disease: An emergency
• Gastrointestinal t Acid Reflux t Esophageal Spasm
• Other stuff t Panic Disorder – Anxiety Attack t Conversion Disorder
Cardiac Chest Pain Causes
• Structural t Cardiomyopathy t LVOT obstruction
v Aortic Stenosis v Subaortic Stenosis v Supravalvular
stenosis t Mitral Valve Prolapse
• Dysrhythmias • Inflammatory
t Pericarditis t Myocarditis
• Drugs
• Coronary Arteries t ALCAPA t ALCARCS t Kawasaki t Transplant related t CAD
• Other t Aortic aneurysm or
dissection t Pulm HTN t Intracardiac Mass
5/17/17
24
Structural Causes of Cardiac Chest Pain
• LVOT obstruction t Exertional chest
pain, dizziness, and/or syncope
t Fatigue t Harsh ejection
murmur with radiation to carotids in AS
• Cardiomyopathy t Chest pain with
exercise intolerance and fatigue
• Mitral Valve Prolapse t Barlow Syndrome
v Pain v Palpitations v Dizziness v Panic Attacks
Other Cardiac Related Causes • Aortic Dissection
t Tearing pain t Radiation to back t Risk Factors?
v Marfan v Turner Syndrome v Ehlers-Danlos (IV) v Homocystinuria
• Dysrhythmia
t Re-entry dysrhythmias in Fontan patients
• Pulmonary HTN
t Chest pain with exertion t Syncope
• Drugs
t Cocaine, Meth
5/17/17
25
A 14-year-old girl with type 1 diabetes drops suddenly when walking to the door. She had LoC for seconds and was alert upon waking. She had no palpitations, chest pain, or tonic-clonic movements. She had a blood sugar of 35mg/dL when seen in the ED. Is this syncope?
Semantics of Syncope
• Transient loss of consciousness t Transient with rapid onset, short duration, and
spontaneous recovery • Syncope
t T-LOC secondary to GLOBAL CEREBRAL HYPOPERFUSION
5/17/17
26
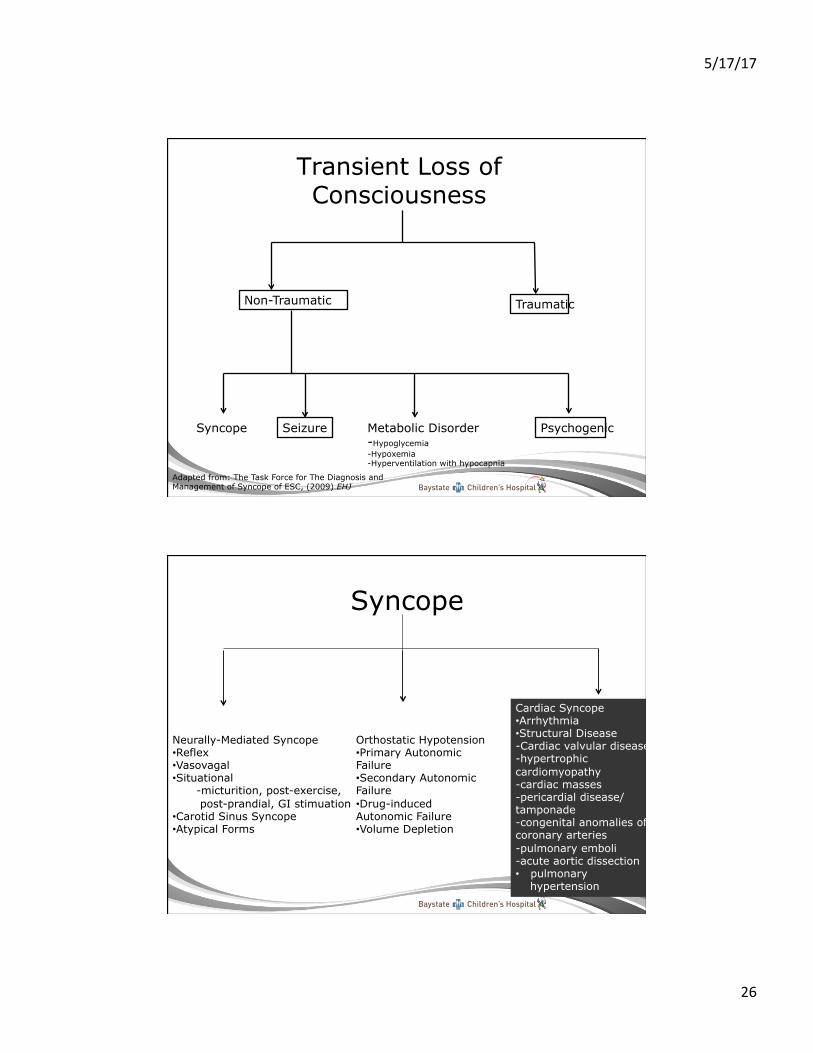
Transient Loss of Consciousness
Non-Traumatic Traumatic
Syncope Seizure Psychogenic Metabolic Disorder -Hypoglycemia -Hypoxemia -Hyperventilation with hypocapnia
Adapted from: The Task Force for The Diagnosis and Management of Syncope of ESC, (2009) EHJ
Syncope
Neurally-Mediated Syncope • Reflex • Vasovagal • Situational
- micturition, post-exercise, post-prandial, GI stimuation
• Carotid Sinus Syncope • Atypical Forms
Orthostatic Hypotension • Primary Autonomic Failure • Secondary Autonomic Failure • Drug-induced Autonomic Failure • Volume Depletion
Cardiac Syncope • Arrhythmia • Structural Disease -Cardiac valvular disease -hypertrophic cardiomyopathy -cardiac masses -pericardial disease/tamponade -congenital anomalies of coronary arteries -pulmonary emboli -acute aortic dissection • pulmonary
hypertension

5/17/17
27
A 16 year old girl is running a cross-country race. She finishes the run and is standing when she becomes dizzy and has LoC for approximately 5 seconds. No other prodromal symptoms and no convulsive activity.
Her symptoms are most likely secondary to….
a. Hypertrophic cardiomyopathy b. Anomalous left coronary artery from the
right sinus of valsalva c. Neural Mediated Syncope d. Prolonged QTc leading to Torsades
5/17/17
28
Most commonly it is…. Neural Mediated Syncope
• Alterations in Autonomic function by changes in the sympathetic/parasympathetic pathways
NMS (cont.)
t Can be due to low heart rate (increased parasympathetic activity) – Cardioinhibitory: 12-35%
t Can be due to decreased blood pressure (decreased sympathetic response) - Vasodepressor 5-15%
t Can be both - Mixed response - 50-80% v NMS Variants – Postural Orthostatic Tachycardia
Syndrome

5/17/17
29
Diagnosing Neural Mediated Syncope
• Vasovagal Syncope
t Mediated by emotion or by orthostatic stress t Preceded by prodromal symptoms (sweating,
pallor, nausea) • Situational Syncope
t Reflex syncope which occurs in certain circumstances
t i.e. post exercise syncope in young • Carotid Sinus Syncope
t Caused by mechanical manipulation of carotid sinus
Postural Orthostatic Tachycardia Syndrome (POTS)
• Orthostatic intolerance associated with an increase in HR of 30 bpm or more
• Non-specific complaints common of fatigue, light-headedness, palpitations, nausea, decreased concentration
• May or may not have syncope • Symptoms have been present for >3
months
Grubb, B.P. (2008) Circ. 117, 2814-2817.
5/17/17
30
Cardiac Causes of Syncope
• Arrhythmia • Structural Disease -Cardiac valvular disease -Hypertrophic cardiomyopathy -Cardiac masses -Pericardial disease/tamponade -Congenital anomalies of coronary arteries • Acute Aortic Dissection (not common in
pediatrics) • Pulmonary Hypertension
Syncope Red Flags
• Syncope with exertion • No prodromal symptoms prior to syncope • Poor perfusion upon nurse evaluation • Abnormal vital signs • Altered mental status and/or focal deficits
on neurologic exam • Palpitations with syncope or irregular
heart rate noted on nurse evaluation • Past Medical History of previous cardiac
issues
5/17/17
31
What to do…..
• Support airway, breathing, circulation • Activate EMS and ask for help if available • Have AED available • Continue to assess student closely with
repeat vital signs at least every 5 minutes • Contact parent/guardian • Notify school administration
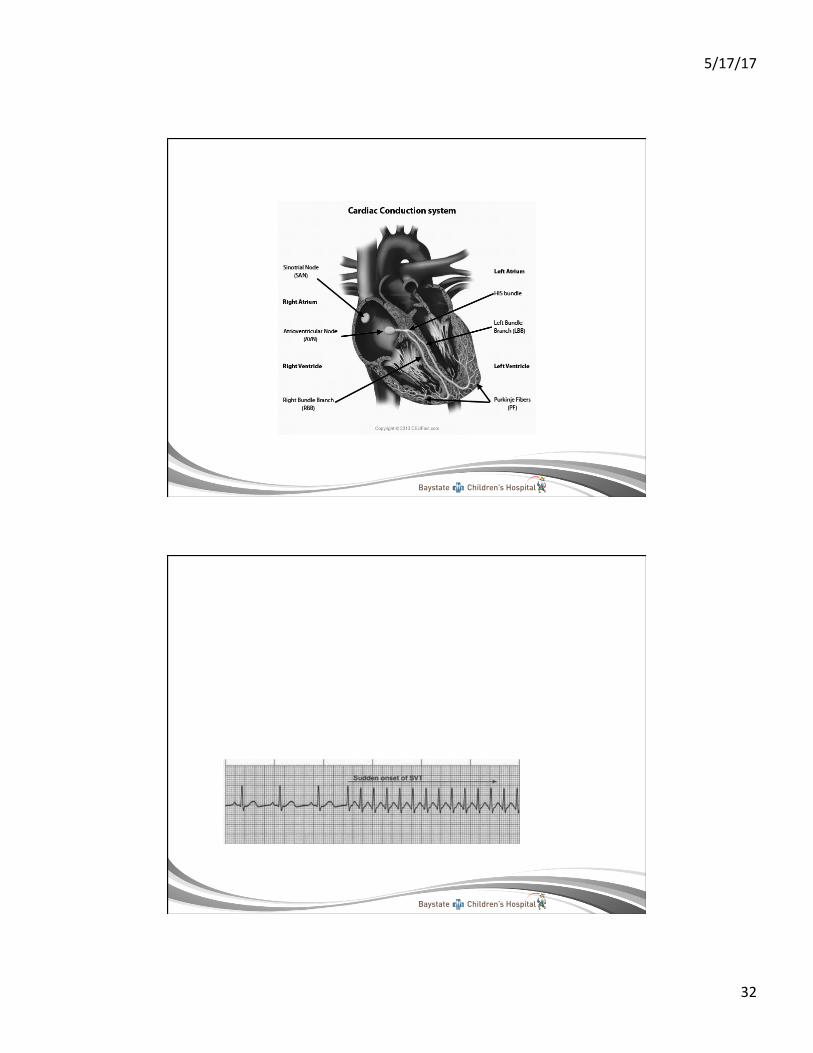
Supraventricular Tachycardia
• Fast heart rate secondary to “an origin above the ventricle” that is not the normal pacemaker
• Heart rate usually >180 bpm
5/17/17
32

5/17/17
33
• History: Quick onset, offset. Heart rate persistently the same. May have chest discomfort, dizziness. Syncope unusual.
• PE: Vitals. Check perfusion, mental status, etc.
• Management: t Try vagal maneuvers these reset pacemaker.
v Bearing down, blowing through a straw, cold water/ice on face
t If persistent, poor perfusion, or with other symptoms - call EMS.
• Long-term Management t May be controlled on oral medication (beta-
blocker such as propranolol) or ablated t Medication decreases rate and ideally will stop
episodes of SVT t If SVT infrequent, may not be on medication
and not have ablation.
5/17/17
34
SVT – “Pill in pocket method”
t These patient may have “pill in pocket method” v Try vagal maneuvers, not successful take
propranolol, retry vagal maneuvers 15 minutes later v If with continued SVT for >20 minutes or if with any
concerns of hemodynamic compromise call EMS ->ED
Summary
• History is very important t Including details of event, family history, and
past medical history • Vital signs are “Vital”
t These vary by age • Chest pain and syncope aren’t usually
going to be cardiac t But need to think about them
5/17/17
35
Summary (cont)
• If concerned ensure you get help, assess ABCs (CPR if necessary), and have AED
• If with underlying cardiac issues, low threshold for EMS
• Come up with protocols for these issues at your institution ahead of time
We made it!

5/17/17
36
References 1. American Academy of Pediatrics. Prepartication Physical Evaluation
Form. Obtained from: http://www.aap.org/en-us/professional-resources/practice-support/pages/Preparticipation-Physical-Evaluation-Forms.aspx
2. Lai et al. Echocardiography in Pediatric and Congenital Heart Disease: From Fetus to Adult. Blackwell Publishing, New Jersey, 2009; 630.
3. Luma et al. Hypertension in Children and Adolescents. Am Fam Physician. 2006 May 1;73(9):1558-1568 2 Maron et al. Profile and frequency of sudden death in 1463 young competitive athletes:analysis of 1866 deaths in the United States. Circulation. 2009;119(8)1085-2006.
4. Maron B, Thompson P, Ackerman M et al. Recommendations and Considerations Related to Preparticipation Screening for Cardiovascular Abnormalities in Competitive Athletes:2007 Update. A Scientific Statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism. Circulation. 2007; 115:1643-1655.
5. Park, Myung. The Pediatric Cardiology Handbook, 3rd Ed. Elsevier Publishing, Pennsylvania; 2003.