Pediatric Cardiac Emergencies. Infant Cardiac Disease Leading to ER Presentation ä Congenital ä...
139
Pediatric Cardiac Emergencies
-
Upload
leonardo-skidgel -
Category
Documents
-
view
223 -
download
1
Transcript of Pediatric Cardiac Emergencies. Infant Cardiac Disease Leading to ER Presentation ä Congenital ä...

Pediatric Cardiac EmergenciesPediatric Cardiac Emergencies
Infant Cardiac Disease Leading to ER PresentationInfant Cardiac Disease Leading to ER Presentation
CongenitalCongenital
AcquiredAcquired CardiomyopathyCardiomyopathy Myocarditis (usually with CHF)Myocarditis (usually with CHF) DysrhythmiasDysrhythmias
Heart Failure- Definition:Heart Failure- Definition:
A state in which the heart cannot provide A state in which the heart cannot provide sufficient cardiac output to satisfy the sufficient cardiac output to satisfy the metabolic needs of the bodymetabolic needs of the body
It is commonly termed congestive heart It is commonly termed congestive heart failure (CHF) since symptoms of increase failure (CHF) since symptoms of increase venous pressure are often prominent venous pressure are often prominent
CHF - PresentationCHF - Presentation
infants: irritable, poor feeding (early infants: irritable, poor feeding (early fatigue), failure to thrive, respiratory fatigue), failure to thrive, respiratory symptomssymptoms
always consider in patients with respiratory always consider in patients with respiratory symptoms symptoms often misdiagnosed as respiratory illness / often misdiagnosed as respiratory illness /
infectioninfection
CHF - EtiologyCHF - Etiology
Increased PreloadIncreased Preload L to R shunts (VSD, PDA, AV fistula)L to R shunts (VSD, PDA, AV fistula) severe anemiasevere anemia
Increased AfterloadIncreased Afterload HTNHTN Congenital (aortic stenosis, coarctation of aorta)Congenital (aortic stenosis, coarctation of aorta)
Decreased ContractilityDecreased Contractility myocarditis, pericarditis with tamponademyocarditis, pericarditis with tamponade cardiomyopathy (dilated or hypertrophic)cardiomyopathy (dilated or hypertrophic) Kawasaki syndrome (early phase)Kawasaki syndrome (early phase) metabolic: electrolyte, hypothyroidmetabolic: electrolyte, hypothyroid myocardial contusionmyocardial contusion toxins: dig, calcium channel blockers, beta blockerstoxins: dig, calcium channel blockers, beta blockers
Dysrhythmia Dysrhythmia
CHF - EtiologyCHF - Etiology
presents immediately at birthpresents immediately at birth anemia, acidosis, hypoxia, hypoglycemia, anemia, acidosis, hypoxia, hypoglycemia,
hypocalcemia, sepsishypocalcemia, sepsis presents at 1 day (congenital)presents at 1 day (congenital)
PDA in premature infantsPDA in premature infants presents in first month (congenital) presents in first month (congenital)
HPLV, aortic stenosis, coarctation, VSD presents later HPLV, aortic stenosis, coarctation, VSD presents later presents later (acquired)presents later (acquired)
myocarditis, cardiomyopathy (dilated or hypertrophic), myocarditis, cardiomyopathy (dilated or hypertrophic), SVT, severe anemia, rheumatic feverSVT, severe anemia, rheumatic fever
Etiology Etiology
It is a common end point for many It is a common end point for many diseases of cardiovascular systemdiseases of cardiovascular system
It can be caused by :It can be caused by : --Inappropriate work load Inappropriate work load ((volume or pressure volume or pressure
overload)overload)
--Restricted fillingRestricted filling --Myocyte lossMyocyte loss
by S. Solimanby S. Soliman
Causes of left ventricular failureCauses of left ventricular failure
• • Volume over loadVolume over load: : Regurgitate valveRegurgitate valve
High output statusHigh output status
•• Pressure overload:Pressure overload: Systemic hypertensionSystemic hypertension
Outflow obstructionOutflow obstruction
•• Loss of muscles:Loss of muscles: Post MI, Chronic ischemiaPost MI, Chronic ischemia
Connective tissue diseasesConnective tissue diseases
Infection, Poisons Infection, Poisons (alcohol,cobalt,Doxorubicin)(alcohol,cobalt,Doxorubicin)
• • Restricted Filling:Restricted Filling: Pericardial diseases, Restrictive Pericardial diseases, Restrictive
cardiomyopathy, tachyarrhythmiacardiomyopathy, tachyarrhythmia
by S. Solimanby S. Soliman
PathophysiologyPathophysiology
1.1. Hemodynamic changesHemodynamic changes
2.2. Neurohormonal changesNeurohormonal changes
3.3. Cellular changesCellular changes
by S. Solimanby S. Soliman
Hemodynamic changes Hemodynamic changes
From hemodynamic stand point HF can be From hemodynamic stand point HF can be secondary to systolic dysfunction or secondary to systolic dysfunction or
diastolic dysfunctiondiastolic dysfunction
by S. Solimanby S. Soliman
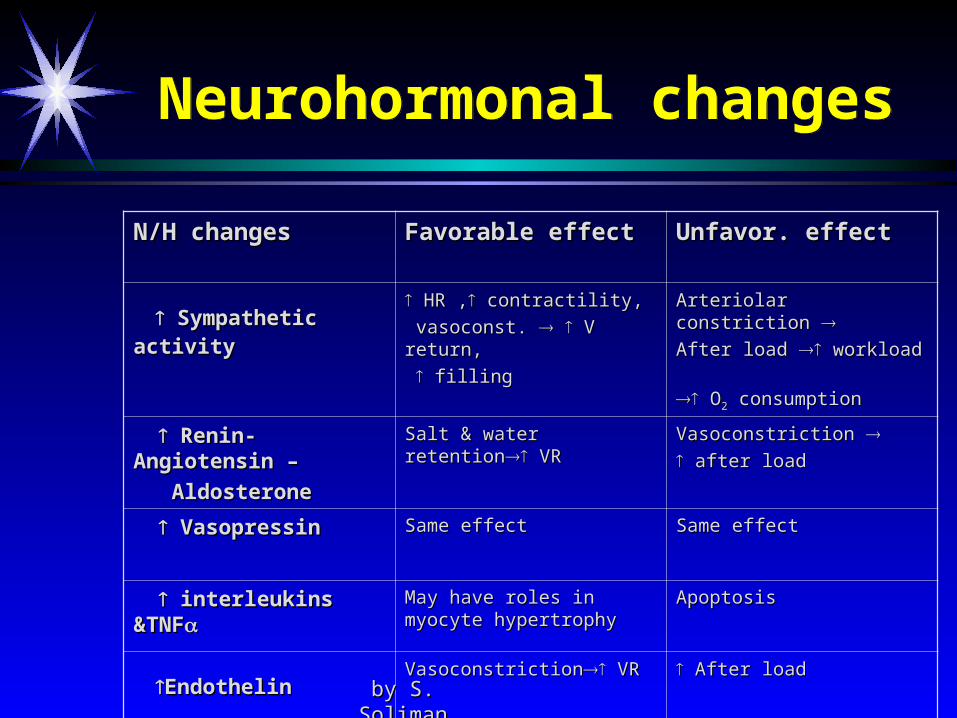
Neurohormonal changesNeurohormonal changes
N/H changesN/H changes Favorable effectFavorable effect Unfavor. effectUnfavor. effect
Sympathetic activitySympathetic activity HR ,HR , contractility, contractility,
vasoconst. vasoconst. V return, V return,
fillingfilling
Arteriolar constriction Arteriolar constriction After load After load workload workload
OO22 consumption consumption
Renin-Angiotensin – Renin-Angiotensin –
Aldosterone Aldosterone
Salt & water retentionSalt & water retention VR VR Vasoconstriction Vasoconstriction after loadafter load
VasopressinVasopressin Same effectSame effect Same effectSame effect
interleukins &TNFinterleukins &TNF May have roles in myocyte May have roles in myocyte hypertrophy hypertrophy
ApoptosisApoptosis
EndothelinEndothelinVasoconstrictionVasoconstriction VR VR After loadAfter load
by S. Solimanby S. Soliman
Cellular changesCellular changes
Changes in CaChanges in Ca+2+2 handling. handling.
Changes in adrenergic receptors:Changes in adrenergic receptors:
•• Slight Slight in in αα11 receptors receptors
• • ββ11 receptors desensitization receptors desensitization followed by down regulation followed by down regulation
Changes in contractile proteinsChanges in contractile proteins
Program cell death (Program cell death (ApoptosisApoptosis))
Increase amount of fibrous tissueIncrease amount of fibrous tissue
by S. Solimanby S. Soliman
SymptomsSymptoms
• • Shortness of breathShortness of breath, Orthopnea, , Orthopnea, paroxysmal nocturnal dyspneaparoxysmal nocturnal dyspnea
• • Low cardiac output symptomsLow cardiac output symptoms
• • Abdominal symptoms:Abdominal symptoms: Anorexia,nausea,Anorexia,nausea,
abdominal fullness,abdominal fullness, painpain
by S. Solimanby S. Soliman
Physical SignsPhysical Signs
1.1. High diastolic BP & occasional decrease High diastolic BP & occasional decrease in systolic BP (decapitated BP)in systolic BP (decapitated BP)
2.2. JVDJVD
3.3. RalesRales (Inspiratory)(Inspiratory)
4.4. Displaced and sustained apical impulsesDisplaced and sustained apical impulses
5.5. Third heart sound – Third heart sound – low pitched sound that is low pitched sound that is heard during rapid filling of ventricleheard during rapid filling of ventricle
by S. Solimanby S. Soliman
Physical signs (cont.)Physical signs (cont.)
Mechanism of SMechanism of S3 3 sudden deceleration of blood sudden deceleration of blood
as elastic limits of the ventricles are as elastic limits of the ventricles are
reachedreached
Vibration of the ventricular wall by blood Vibration of the ventricular wall by blood
fillingfilling
Common in childrenCommon in children
by S. Solimanby S. Soliman
Physical signs (cont.)Physical signs (cont.)
Fourth heart Sound (S4)
- Usually at the end of diastole
- Exact mechanism is not known
Could be due to contraction of
atrium against stiff ventricle
Pale, cold sweaty skin
by S. Solimanby S. Soliman
Framingham Criteria for Dx of Heart FailureFramingham Criteria for Dx of Heart Failure
Major Criteria:Major Criteria: PNDPND- paroxysmal nocturnal dyspnea- paroxysmal nocturnal dyspnea JVDJVD- jugular venous distention- jugular venous distention RalesRales CardiomegalyCardiomegaly Acute Pulmonary EdemaAcute Pulmonary Edema SS3 3 GallopGallop
Positive hepatic Jugular reflexPositive hepatic Jugular reflex ↑ ↑ venous pressure > 16 cm Hvenous pressure > 16 cm H22OO
by S. Solimanby S. Soliman
Dx of Heart Failure (cont.)Dx of Heart Failure (cont.)
Minor CriteriaMinor Criteria
LL edema,LL edema,
Night cough Night cough
Dyspnea on exertionDyspnea on exertion
HepatomegalyHepatomegaly
Pleural effusionPleural effusion ↓ ↓ vital capacity by 1/3 of normalvital capacity by 1/3 of normal
Tachycardia 120 bpmTachycardia 120 bpm
Weight loss 4.5 kg over 5 days managementWeight loss 4.5 kg over 5 days management
by S. Solimanby S. Soliman
Forms of Heart FailureForms of Heart Failure
Systolic & DiastolicSystolic & Diastolic High Output Failure High Output Failure
Pregnancy, anemia, thyrotoxisis, A/V fistula, Beriberi, Pregnancy, anemia, thyrotoxisis, A/V fistula, Beriberi,
Low Output FailureLow Output Failure AcuteAcute
large MI, aortic valve dysfunctionlarge MI, aortic valve dysfunction ChronicChronic
by S. Solimanby S. Soliman
Forms of heart failure ( cont.)
Forms of heart failure ( cont.)
Right vs Left sided heart failure:Right vs Left sided heart failure:
Right sided heart failure :Right sided heart failure : Most common cause is left sided failureMost common cause is left sided failure
Other causes included : Pulmonary embolismsOther causes included : Pulmonary embolisms
Other causes of pulmonary htn.Other causes of pulmonary htn.
RV infarctionRV infarction
MSMS
Usually presents with: LL edema, ascitesUsually presents with: LL edema, ascites
hepatic congestionhepatic congestion
cardiac cirrhosis (on the long run) cardiac cirrhosis (on the long run)
by S. Solimanby S. Soliman
Left ventricular failureLeft ventricular failure
- respiratory discomfort, vary with respiratory discomfort, vary with position,stress and activity, associated with position,stress and activity, associated with physical signs of disturbances in the lungsphysical signs of disturbances in the lungs
- Dyspnea during modest exertion- usually Dyspnea during modest exertion- usually the first symptoms of left heart failure, the first symptoms of left heart failure, associated with increased rate of breathingassociated with increased rate of breathing
- OrtopneaOrtopnea- CoughCough
Left ventricular failureLeft ventricular failure
On examination:On examination:
-patient: pale and sweaty, cold hands because of -patient: pale and sweaty, cold hands because of periferal vasoconstrictionperiferal vasoconstriction
- rapid heart raterapid heart rate- Gallop rhythmGallop rhythm- Murmur of mitral insufficiencyMurmur of mitral insufficiency- Rales on auscultation of the lungsRales on auscultation of the lungs
( interstitial edema and fluid)( interstitial edema and fluid)
Right Ventricular FailureRight Ventricular Failure
-neck veins distention-neck veins distention-hepatomegaly, splenomegaly-hepatomegaly, splenomegaly-congestion and edema of the gastrointestinal tract, -congestion and edema of the gastrointestinal tract,
anorexia,nausea, vomitinganorexia,nausea, vomiting- weight loss, failure to gain weight,malnutritionweight loss, failure to gain weight,malnutrition- Murmur or tricuspid insufficiencyMurmur or tricuspid insufficiency- HydrothoraxHydrothorax- Pericardial effusionPericardial effusion- Irritability,restlessnessIrritability,restlessness- oliguriaoliguria
Differential diagnosis Differential diagnosis
Pericardial diseasesPericardial diseases Liver diseasesLiver diseases Nephrotic syndromeNephrotic syndrome Protein losing enteropathyProtein losing enteropathy
by S. Solimanby S. Soliman
Laboratory Findings Laboratory Findings
AnemiaAnemia Hyperthyroid Hyperthyroid Chronic renal insuffiency, electrolytes Chronic renal insuffiency, electrolytes
abnormalityabnormality Pre-renal azotemiaPre-renal azotemia HemochromatosisHemochromatosis
by S. Solimanby S. Soliman
ElectrocardiogramElectrocardiogram
Old MI or recent MIOld MI or recent MI ArrhythmiaArrhythmia Some forms of Cardiomyopathy are tachycardia Some forms of Cardiomyopathy are tachycardia
related related LBBBLBBB→→may help in managementmay help in management
by S. Solimanby S. Soliman
Chest X-rayChest X-ray
Size and shape of heartSize and shape of heart Evidence of pulmonary venous congestion Evidence of pulmonary venous congestion
(dilated or upper lobe veins (dilated or upper lobe veins → perivascular → perivascular edema)edema)
Pleural effusionPleural effusion
by S. Solimanby S. Soliman
EchocardiogramEchocardiogram
Function of both ventriclesFunction of both ventricles Wall motion abnormality that may signify CADWall motion abnormality that may signify CAD Valvular abnormalityValvular abnormality Intra-cardiac shuntsIntra-cardiac shunts
by S. Solimanby S. Soliman

Cardiac CatheterizationCardiac Catheterization
When CAD or valvular is suspectedWhen CAD or valvular is suspected
If heart transplant is indicatedIf heart transplant is indicated
by S. Solimanby S. Soliman
TREATMENTTREATMENT
Correction of reversible causesCorrection of reversible causes IschemiaIschemia Valvular heart diseaseValvular heart disease Thyrotoxicosis and other high output statusThyrotoxicosis and other high output status ShuntsShunts ArrhythmiaArrhythmia
A fib, flutter, A fib, flutter, permanent junctional reciprocating tachycardiapermanent junctional reciprocating tachycardia
Medications Medications Ca channel blockers, some antiarrhythmics Ca channel blockers, some antiarrhythmics
by S. Solimanby S. Soliman

Diet and ActivityDiet and Activity
Salt restrictionSalt restriction Fluid restrictionFluid restriction Daily weight (tailor therapy)Daily weight (tailor therapy) Gradual exertion programsGradual exertion programs
by S. Solimanby S. Soliman
Diuretic TherapyDiuretic Therapy
The most effective symptomatic reliefThe most effective symptomatic relief Mild symptomsMild symptoms
HCTZHCTZ ChlorthalidoneChlorthalidone MetolazoneMetolazone Block Na reabsorbtion in loop of henle and Block Na reabsorbtion in loop of henle and
distal convoluted tubulesdistal convoluted tubules Thiazides are ineffective with GFR < 30 --/minThiazides are ineffective with GFR < 30 --/min
by S. Solimanby S. Soliman
Diuretics (cont.)Diuretics (cont.)
Side EffectsSide Effects Pre-renal azotemia Pre-renal azotemia Skin rashesSkin rashes NeutropeniaNeutropenia ThrombocytopeniaThrombocytopenia HyperglycemiaHyperglycemia ↑ ↑ Uric AcidUric Acid Hepatic dysfunctionHepatic dysfunction
by S. Solimanby S. Soliman
Diuretics (cont.)Diuretics (cont.)
More severe heart failure More severe heart failure → loop → loop diureticsdiuretics FurosemideFurosemide 1-3 mg/kg m.c. 1-3 mg/kg m.c.Mechanism ofMechanism of actionaction: : Inhibit chloride reabsortion in ascending limb of Inhibit chloride reabsortion in ascending limb of
loop of Henle results in natriuresis, kaliuresis and metabolic alkalosisloop of Henle results in natriuresis, kaliuresis and metabolic alkalosis
Adverse reaction:Adverse reaction:
pre-renal azotemiapre-renal azotemia
HypokalemiaHypokalemia
Skin rashSkin rash
ototoxicityototoxicityby S. Solimanby S. Soliman
K+ Sparing AgentsK+ Sparing Agents
Triamterene & amilorideTriamterene & amiloride – – acts on distal tubules to acts on distal tubules to ↓ K ↓ K secretionsecretion
SpironolactoneSpironolactone (Aldosterone inhibitor) (Aldosterone inhibitor)
recent evidence suggests that it may improve survival in recent evidence suggests that it may improve survival in CHF patients due to the effect on renin-angiotensin-CHF patients due to the effect on renin-angiotensin-aldosterone system with subsequent effect on myocardial aldosterone system with subsequent effect on myocardial remodeling and fibrosisremodeling and fibrosis
by S. Solimanby S. Soliman
Inhibitors of renin-angiotensin- aldosterone system
Inhibitors of renin-angiotensin- aldosterone system
Renin-angiotensin-aldosterone systemRenin-angiotensin-aldosterone system is activation is activation early in the course of heart failure and plays an early in the course of heart failure and plays an
important roleimportant role in the progression of the syndromein the progression of the syndrome
Angiotensin converting enzyme inhibitorsAngiotensin converting enzyme inhibitors Angiotensin receptors blockersAngiotensin receptors blockers SpironolactoneSpironolactone
by S. Solimanby S. Soliman
Angiotensin Converting Enzyme Inhibitors
Angiotensin Converting Enzyme Inhibitors
They block the R-A-A system by inhibiting the They block the R-A-A system by inhibiting the conversion of angiotensin I to angiotensin II conversion of angiotensin I to angiotensin II → → vasodilation and ↓ Na retentionvasodilation and ↓ Na retention
↓ ↓ Bradykinin degradation ↑ its Bradykinin degradation ↑ its levellevel → ↑ PG → ↑ PG secretion & nitric oxidesecretion & nitric oxide
Ace Inhibitors were found to improve survival in Ace Inhibitors were found to improve survival in CHF patientsCHF patients Delay onset & progression of HF in pts with Delay onset & progression of HF in pts with
asymptomatic LV dysfunctionasymptomatic LV dysfunction ↓ ↓ cardiac remodelingcardiac remodeling
by S. Solimanby S. Soliman
Side effects of ACE inhibitorsSide effects of ACE inhibitors
AngioedemaAngioedema HypotensionHypotension Renal insuffiencyRenal insuffiency RashRash coughcough
by S. Solimanby S. Soliman
Angiotensin II receptor blockers
Angiotensin II receptor blockers
Has comparable effect to ACE IHas comparable effect to ACE I
Can be used in certain conditions when ACE I are Can be used in certain conditions when ACE I are contraindicated (angioneurotic edema, cough)contraindicated (angioneurotic edema, cough)
by S. Solimanby S. Soliman
Digitalis Glycosides (Digoxin, Digitoxin)Digitalis Glycosides (Digoxin, Digitoxin)
The role of digitalis has declined somewhat The role of digitalis has declined somewhat because of safety concernbecause of safety concern
Recent studies have shown that digitals does not Recent studies have shown that digitals does not affect mortality in CHF patients but causes affect mortality in CHF patients but causes significant significant Reduction in hospitalizationReduction in hospitalization Reduction in symptoms of HFReduction in symptoms of HF
by S. Solimanby S. Soliman
Digitalis (cont.)Mechanism of ActionDigitalis (cont.)Mechanism of Action
+ve inotropic effect by +ve inotropic effect by ↑ intracellular Ca & ↑ intracellular Ca & enhancing actin-myosin cross bride formation enhancing actin-myosin cross bride formation (binds to the Na-K ATPase → inhibits Na pump (binds to the Na-K ATPase → inhibits Na pump → ↑ intracellular Na → ↑ Na-Ca exchange→ ↑ intracellular Na → ↑ Na-Ca exchange
Vagotonic effectVagotonic effect Arrhythmogenic effectArrhythmogenic effect
by S. Solimanby S. Soliman
Digitalis ToxicityDigitalis Toxicity
Narrow therapeutic to toxic ratioNarrow therapeutic to toxic ratio
Non cardiac manifestationsNon cardiac manifestations
Anorexia,Anorexia,
Nausea, vomiting,Nausea, vomiting,
Headache, Headache,
Xanthopsia sotoma, Xanthopsia sotoma,
DisorientationDisorientation
by S. Solimanby S. Soliman
Digitalis ToxicityDigitalis Toxicity
Cardiac manifestationsCardiac manifestations Sinus bradycardia and arrestSinus bradycardia and arrest A/V block (usually 2A/V block (usually 2ndnd degree) degree) Atrial tachycardia with A/V BlockAtrial tachycardia with A/V Block Development of junctional rhythm in patients with a fibDevelopment of junctional rhythm in patients with a fib PVC’s, VT/ V fib (bi-directional VT)PVC’s, VT/ V fib (bi-directional VT)
by S. Solimanby S. Soliman
Digitalis ToxicityTreatment
Digitalis ToxicityTreatment
Hold the medicationsHold the medications ObservationObservation In case of A/V block or severe bradycardia In case of A/V block or severe bradycardia → →
atropine followed by temporary PM if neededatropine followed by temporary PM if needed In life threatening arrhythmia → digoxin-specific In life threatening arrhythmia → digoxin-specific
fab antibodiesfab antibodies Lidocaine and phenytoin could be used – try to Lidocaine and phenytoin could be used – try to
avoid D/C cardioversion in non life threatening avoid D/C cardioversion in non life threatening arrhythmiaarrhythmia
by S. Solimanby S. Soliman
β Blockersβ Blockers
Has been traditionally contraindicated in pts with CHF
Now they are the main stay in treatment on CHF & may be the only medication that shows substantial improvement in LV function
In addition to improved LV function multiple studies show improved survival
The only contraindication is severe decompensated CHF
by S. Solimanby S. Soliman
VasodilatorsVasodilators
Reduction of afterload by arteriolar vasodilatation (hydralazin) reduce LVEDP, O2
consumption,improve myocardial perfusion, stroke volume and COP
Reduction of preload By venous dilation
( Nitrate) ↓ the venous return ↓ the load on both ventricles.
Usually the maximum benefit is achieved by using agents with both action.
by S. Solimanby S. Soliman
Positive inotropic agentsPositive inotropic agents
These are the drugs that improve myocardial These are the drugs that improve myocardial contractility (contractility (β adrenergic agonists, dopaminergic β adrenergic agonists, dopaminergic
agents, phosphodiesterase inhibitors),agents, phosphodiesterase inhibitors),
dopamine, dobutamine, milrinone, amrinonedopamine, dobutamine, milrinone, amrinone Several studies showed ↑ mortality with oral Several studies showed ↑ mortality with oral
inotropic agentsinotropic agents So the only use for them now is in acute sittings as So the only use for them now is in acute sittings as
cardiogenic shockcardiogenic shock
by S. Solimanby S. Soliman
Anticoagulation (coumadine)Anticoagulation (coumadine)
Atrial fibrillationAtrial fibrillation
H/o embolic episodesH/o embolic episodes
Left ventricular apical thrombusLeft ventricular apical thrombus
by S. Solimanby S. Soliman
AntiarrhythmicsAntiarrhythmics
Most common cause of SCD in these patients is Most common cause of SCD in these patients is ventricular tachyarrhythmiaventricular tachyarrhythmia
Patients with h/o sustained VT or SCD Patients with h/o sustained VT or SCD → ICD → ICD implantimplant
by S. Solimanby S. Soliman
Antiarrhythmics (cont.)Antiarrhythmics (cont.)
Patients with non sustained ventricular tachycardiaPatients with non sustained ventricular tachycardia Correction of electrolytes and acid base imbalanceCorrection of electrolytes and acid base imbalance In patients with ischemic cardiomyopathy → ICD In patients with ischemic cardiomyopathy → ICD
implant is the option after r/o acute ischemia as the implant is the option after r/o acute ischemia as the causecause
In patients wit non ischemic cardiomyopathy In patients wit non ischemic cardiomyopathy management is not clearmanagement is not clear
Amiodarone may have a role in this group of patientsAmiodarone may have a role in this group of patients
by S. Solimanby S. Soliman
New MethodsNew Methods
Implantable ventricular assist devicesImplantable ventricular assist devices
Biventricular pacingBiventricular pacing (only in patient (only in patient with LBBB & CHF)with LBBB & CHF)
Artificial HeartArtificial Heartby S. Solimanby S. Soliman
Nursing Interventions - CHFNursing Interventions - CHF
Decrease energy expenditure Frequent rest periods Small, frequent feedings Minimize crying Prevent cold stress
Provide nutrition Use soft nipple Gavage feeding if needed
Nursing Interventions - CHFNursing Interventions - CHF
Monitor fluid status I & O, specific gravity Daily weight
Provide adequate rest, position for comfort Prevent infections Promote growth & development Reduce respiratory distress
DigoxinDigoxin
Check dosage with another RN Give 1 hour before feeding or 2 hours after
feeding Give at 12 hour intervals Take apical pulse for 1 minute
Hold if HR <90 in infants or<70 in children Monitor serum potassium levels Monitor for toxicity: vomiting, nausea,
bradycardia, lethargy
MyocarditisMyocarditis
leading cause of dilated cardiomyopathy and one leading cause of dilated cardiomyopathy and one of the most common causes of CHF in childrenof the most common causes of CHF in children
etiology: idiopathic, viral, bacterial, parasiticetiology: idiopathic, viral, bacterial, parasitic hallmark is CHFhallmark is CHF failure to respond to bronchodilators in wheezing failure to respond to bronchodilators in wheezing
childchild treatment includes inotropes, afterload reduction, treatment includes inotropes, afterload reduction,
diuretics, antibiotics, antiviralsdiuretics, antibiotics, antivirals
PericarditisPericarditis
sharp stabbing precordial painsharp stabbing precordial pain worse with supine and better leaning worse with supine and better leaning
forwardforward no sensory innervation of the pericardiumno sensory innervation of the pericardium
pain referred from diaphragmatic and pleural pain referred from diaphragmatic and pleural irritationirritation
EtiologyEtiology
infectiousinfectious viralviral bacterialbacterial TBTB fungal fungal parasiticparasitic
Connective tissueConnective tissue RARA Rheumatic feverRheumatic fever SLESLE
Metabolic / EndocrineMetabolic / Endocrine uremiauremia hypothyroidhypothyroid
Hematology / OncologyHematology / Oncology bleeding diathesisbleeding diathesis malignancymalignancy
TraumaTrauma IatrogenicIatrogenic
PericarditisPericarditis
usually a benign courseusually a benign course virulent bacteria (H. flu, E. coli) can cause virulent bacteria (H. flu, E. coli) can cause
constrictive pericarditis and subsequent constrictive pericarditis and subsequent tamponade – may need urgent tamponade – may need urgent pericardiocentesispericardiocentesis
uncomplicated pericarditis usually responds uncomplicated pericarditis usually responds to rest and anti-inflammatoriesto rest and anti-inflammatories
Chest PainChest Pain
4% of children will have a cardiac origin4% of children will have a cardiac origin remainder: MSK, pulmonic (asthma, remainder: MSK, pulmonic (asthma,
bronchitis, pneumonia), GIbronchitis, pneumonia), GI Cardiac causes: myocarditis, pericarditis, Cardiac causes: myocarditis, pericarditis,
structural abnormalities such as congenital structural abnormalities such as congenital heart disease or hypertrophic heart disease or hypertrophic cardiomyopathycardiomyopathy
SyncopeSyncope
20-50% of adolescents experience at least one 20-50% of adolescents experience at least one episode of syncopeepisode of syncope most cases benignmost cases benign
PathophysiologyPathophysiology vascularvascular orthostatic, hypovolemiaorthostatic, hypovolemia neurally mediatedneurally mediated hypoxia: PE, CNS depression from OD, COhypoxia: PE, CNS depression from OD, CO cardiaccardiac
Cardiac SyncopeCardiac Syncope
DysrhythmiasDysrhythmias tachytachy bradybrady
Outflow obstructionOutflow obstruction Myocardial DysfunctionMyocardial Dysfunction
cardiac syncope often precedes future cardiac syncope often precedes future sudden cardiac deathsudden cardiac death
Sudden Cardiac DeathSudden Cardiac Death
EtiologyEtiology myocarditismyocarditis cardiomyopathy (hypertrophic)cardiomyopathy (hypertrophic) cyanotic and noncyanotic congenital heart diseasecyanotic and noncyanotic congenital heart disease valvular heart diseasevalvular heart disease congenital complete heart blockcongenital complete heart block WPWWPW long QT syndromelong QT syndrome Marfan syndromeMarfan syndrome coronary artery diseasecoronary artery disease anomalous coronary arteriesanomalous coronary arteries

Risk Factors for Serious Cause of SyncopeRisk Factors for Serious Cause of Syncope
history of cardiac disease in patienthistory of cardiac disease in patient FH of sudden death, cardiac disease, or deafnessFH of sudden death, cardiac disease, or deafness recurrent episodesrecurrent episodes recumbent episoderecumbent episode exertionalexertional prolonged loss of consciousnessprolonged loss of consciousness associated chest pain or palpitationsassociated chest pain or palpitations medications that can alter cardiac conductionmedications that can alter cardiac conduction
What to look for in the Department: EKG
What to look for in the Department: EKG
Long QT syndromeLong QT syndrome congenital or acquiredcongenital or acquired get paroxysmal v tach with torsades de pointesget paroxysmal v tach with torsades de pointes congenital long QT associated with hypertrophic congenital long QT associated with hypertrophic
cardiomyopathycardiomyopathy long QT defined as corrected QT longer than 0.44 slong QT defined as corrected QT longer than 0.44 s T wave alternans sometimes presentT wave alternans sometimes present can have normal ECG in the departmentcan have normal ECG in the department two clinical syndromes not associated with structural two clinical syndromes not associated with structural
heart disease: Romano-Ward and Jervell-Lange-Nielsenheart disease: Romano-Ward and Jervell-Lange-Nielsen
Other dysrhythmiasOther dysrhythmias
WPW and other SVT’sWPW and other SVT’s AV block AV block
usually acquired, rarely congenitalusually acquired, rarely congenital Sick sinus syndromeSick sinus syndrome
Other structural cardiac diseasesOther structural cardiac diseases
dilated cardiomyopathydilated cardiomyopathy usually secondary to myocarditisusually secondary to myocarditis syncope and death secondary to ventricular dysrhythmias or severe syncope and death secondary to ventricular dysrhythmias or severe
myocardial dysfunctionmyocardial dysfunction arrhythmogenic RV dysplasiaarrhythmogenic RV dysplasia congenital cyanotic and non-cyanotic heart diseasecongenital cyanotic and non-cyanotic heart disease valvular diseasesvalvular diseases
aortic stenosisaortic stenosis coronary artery anomaliescoronary artery anomalies
exertional syncope or sudden deathexertional syncope or sudden death aberrant artery passes between aorta and pulmonary arteryaberrant artery passes between aorta and pulmonary artery
Definition- cardiomyopathyDefinition- cardiomyopathy
““A primary disorder of the heart muscle that A primary disorder of the heart muscle that causes abnormal myocardial performance causes abnormal myocardial performance and is not the result of disease or and is not the result of disease or dysfunction of other cardiac structures … dysfunction of other cardiac structures … myocardial infarction, systemic myocardial infarction, systemic hypertension, valvular stenosis or hypertension, valvular stenosis or regurgitation”regurgitation”
Cardiomyopathy-definitionCardiomyopathy-definition
According to World Health Organisation According to World Health Organisation and International Society and Cardiology and International Society and Cardiology Federation (WHO/ISFC) from 1996, Federation (WHO/ISFC) from 1996, cardiomyopathy is definied as any disease cardiomyopathy is definied as any disease of heartmuscle which is connected with its of heartmuscle which is connected with its disfunctiondisfunction
WHO ClassificationWHO Classification
Unknown causeUnknown cause(primary)(primary) Dilated Dilated HypertrophicHypertrophic RestrictiveRestrictive unclassifiedunclassified
Specific heart muscle Specific heart muscle disease (secondary)disease (secondary) InfectiveInfective MetabolicMetabolic Systemic diseaseSystemic disease HeredofamilialHeredofamilial SensitivitySensitivity ToxicToxic
Br Heart J 1980; 44:672-673
Functional ClassificationFunctional Classification
DilatatedDilatated (DCM) (DCM) ventricular enlargement and syst dysfunctionventricular enlargement and syst dysfunction
HypertrophicHypertrophic ( HCM) ( HCM) inappropriate myocardial hypertrophyinappropriate myocardial hypertrophy
in the absence of HTN or aortic stenosisin the absence of HTN or aortic stenosis RestrictiveRestrictive (infiltrative) (infiltrative)
abnormal filling and diastolic functionabnormal filling and diastolic function
Idiopathic Dilated CardiomyopathyIdiopathic Dilated Cardiomyopathy
IDC - DefinitionIDC - Definition
a disease of unknown etiology that a disease of unknown etiology that principally affects the myocardiumprincipally affects the myocardium
LV dilatation and systolic dysfunctionLV dilatation and systolic dysfunction pathologypathology
increased heart size and weightincreased heart size and weight ventricular dilatation, normal wall thicknessventricular dilatation, normal wall thickness heart dysfunction out of portion to fibrosisheart dysfunction out of portion to fibrosis
Incidence and PrognosisIncidence and Prognosis
3-10 cases per 100,0003-10 cases per 100,000 20,000 new cases per year in the U.S.A.20,000 new cases per year in the U.S.A. death from progressive pump failuredeath from progressive pump failure
1-year1-year 25%25%2-year2-year 35-40%35-40%5-year5-year 40-80%40-80%
stabilization observed in 20-50% of patientstabilization observed in 20-50% of patient complete recovery is rarecomplete recovery is rare
Clinical ManifestationsClinical Manifestations
Highest incidence in middle ageHighest incidence in middle age blacks 2x more frequent than whitesblacks 2x more frequent than whites men 3x more frequent than womenmen 3x more frequent than women
symptoms may be gradual in onsetsymptoms may be gradual in onset acute presentation acute presentation
misdiagnosed as viral URI in young adultsmisdiagnosed as viral URI in young adults uncommon to find specific myocardial disease uncommon to find specific myocardial disease
on endomyocardial biopsyon endomyocardial biopsy
History and Physical Examination
History and Physical Examination
Symptoms of heart failureSymptoms of heart failure pulmonary congestion (left HF)pulmonary congestion (left HF)
dyspnea (rest, exertional, nocturnal), dyspnea (rest, exertional, nocturnal), orthpneaorthpnea
systemic congestion (right HF)systemic congestion (right HF)edema, nausea, abdominal pain, nocturiaedema, nausea, abdominal pain, nocturia
low cardiac outputlow cardiac outputfatigue and weaknessfatigue and weakness
hypotension, tachycardia, tachypnea, JVDhypotension, tachycardia, tachypnea, JVD
Cardiac ImagingCardiac Imaging
Chest radiogramChest radiogram ElectrocardiogramElectrocardiogram 24-hour ambulatory ECG (Holter)24-hour ambulatory ECG (Holter)
lightheadedness, palpitation, syncopelightheadedness, palpitation, syncope Two-dimensional echocardiogramTwo-dimensional echocardiogram Radionuclide ventriculographyRadionuclide ventriculography Cardiac catheterizationCardiac catheterization
age >40, ischemic history, high risk profile, abnormal age >40, ischemic history, high risk profile, abnormal ECGECG
Clinical Indications for Endomyocardial BiopsyClinical Indications for Endomyocardial Biopsy
DefiniteDefinite monitoring of cardiac allograft rejectionmonitoring of cardiac allograft rejection monitoring of anthracycline cardiotoxicitymonitoring of anthracycline cardiotoxicity
PossiblePossible detection and monitoring of myocarditisdetection and monitoring of myocarditis diagnosis of secondary cardiomyopathiesdiagnosis of secondary cardiomyopathies differentiation between restrictive and differentiation between restrictive and
constrictive heart diseaseconstrictive heart disease
Management of DCMManagement of DCM
Limit activity based on functional statusLimit activity based on functional status salt restriction of a 2-g Nasalt restriction of a 2-g Na++ (5g NaCl) diet (5g NaCl) diet fluid restriction for significant low Na+fluid restriction for significant low Na+ initiate medical therapyinitiate medical therapy
ACE inhibitors, diureticsACE inhibitors, diuretics digoxin, carvediloldigoxin, carvedilol hydralazine / nitrate combinationhydralazine / nitrate combination
Management of DCMManagement of DCM
consider adding ß-blocking agents if consider adding ß-blocking agents if symptoms persistssymptoms persists
anticoagulation for EF <30%, history of anticoagulation for EF <30%, history of thromboemoli, presence of mural thrombithromboemoli, presence of mural thrombi
intravenous dopamine, dobutamine and/or intravenous dopamine, dobutamine and/or phosphodiesterase inhibitorsphosphodiesterase inhibitors
cardiac transplantationcardiac transplantation
Hypertrophic CardiomyopathyHypertrophic Cardiomyopathy
Hypertrophic CardiomyopathyHypertrophic Cardiomyopathy
First described by the French and Germans around First described by the French and Germans around 19001900
uncommon with occurrence of 0.02 to 0.2%uncommon with occurrence of 0.02 to 0.2% a hypertrophied and non-dilated left ventricle in a hypertrophied and non-dilated left ventricle in
the absence of another disease the absence of another disease small LV cavity, asymmetrical septal small LV cavity, asymmetrical septal
hypertrophy (ASH), systolic anterior hypertrophy (ASH), systolic anterior motion of the mitral valve leaflet (SAM)motion of the mitral valve leaflet (SAM)
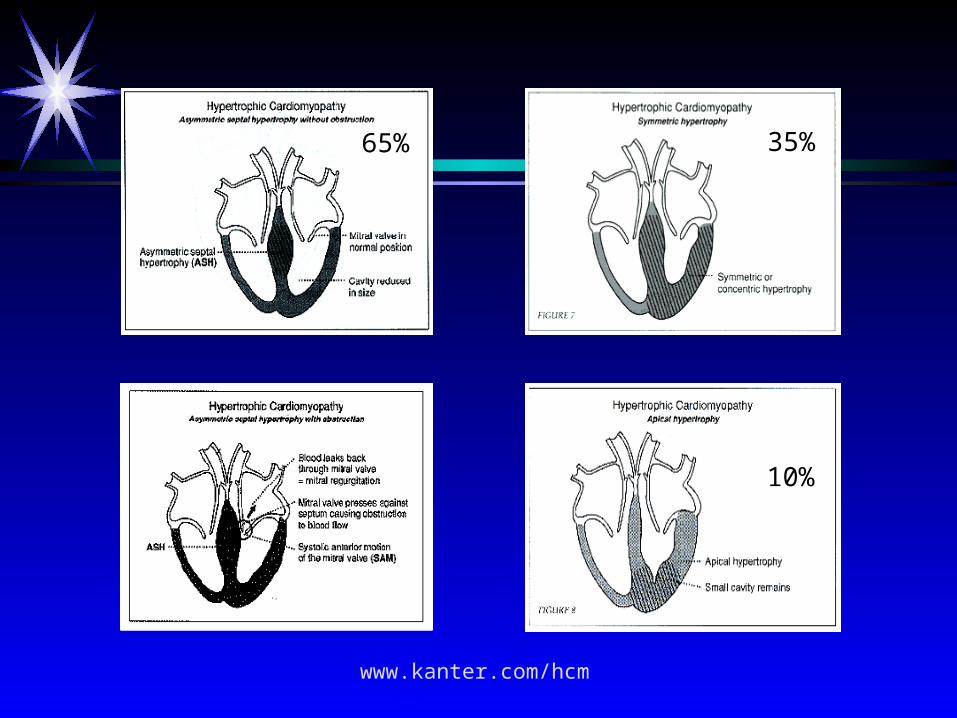
65% 35%
10%
www.kanter.com/hcm
Clinical ManifestationClinical Manifestation
Asymptomatic, echocardiographic findingAsymptomatic, echocardiographic finding SymptomaticSymptomatic
dyspnea in 90%dyspnea in 90% angina pectoris in 75%angina pectoris in 75% fatigue, pre-syncope, syncopefatigue, pre-syncope, syncope
risk of SCD in children and adolescents risk of SCD in children and adolescents palpitation, PND, CHF, dizziness less frequentpalpitation, PND, CHF, dizziness less frequent
Natural HistoryNatural History
annual mortality 3% in referral centersannual mortality 3% in referral centersprobably closer to 1% for all patientsprobably closer to 1% for all patients
risk of SCD higher in children risk of SCD higher in children may be as high as 6% per yearmay be as high as 6% per yearmajority have progressive hypertrophymajority have progressive hypertrophy
clinical deterioration usually is slowclinical deterioration usually is slow progression to DCM occurs in 10-15%progression to DCM occurs in 10-15%
Risk Factors for SCDRisk Factors for SCD
Young age (<30 years)Young age (<30 years) ““Malignant” family history of sudden deathMalignant” family history of sudden death Gene mutations prone to SCD (ex. Arg403Gln)Gene mutations prone to SCD (ex. Arg403Gln) Aborted sudden cardiac deathAborted sudden cardiac death Sustained VT or SVTSustained VT or SVT Recurrent syncope in the youngRecurrent syncope in the young Nonsustained VT (Holter Monitoring)Nonsustained VT (Holter Monitoring) Brady arrhythmias (occult conduction disease)Brady arrhythmias (occult conduction disease)
Br Heart J 1994; 72:S13
ManagementManagement
beta-adrenergic blockersbeta-adrenergic blockers calcium antagonistcalcium antagonist disopyramidedisopyramide amiodarone, sotololamiodarone, sotolol DDD pacingDDD pacing myotomy-myectomymyotomy-myectomy plication of the anterior mitral leafletplication of the anterior mitral leaflet

Restrictive CardiomyopathyRestrictive Cardiomyopathy
Restrictive CardiomyopathiesRestrictive Cardiomyopathies
Hallmark: abnormal diastolic functionHallmark: abnormal diastolic function rigid ventricular wall with impaired rigid ventricular wall with impaired
ventricular fillingventricular filling bear some functional resemblance to bear some functional resemblance to
constrictive pericarditisconstrictive pericarditis importance lies in its differentiation from importance lies in its differentiation from
operable constrictive pericarditisoperable constrictive pericarditis
Exclusion “Guidelines”Exclusion “Guidelines”
LV end-diastolic dimensions LV end-diastolic dimensions 7 cm 7 cm Myocardial wall thickness Myocardial wall thickness 1.7 cm 1.7 cm LV end-diastolic volume LV end-diastolic volume 150 mL/m2 150 mL/m2 LV ejection fraction < 20%LV ejection fraction < 20%
ClassificationClassification
IdiopathicIdiopathic MyocardialMyocardial
1. Noninfiltrative1. Noninfiltrative IdiopathicIdiopathic SclerodermaScleroderma
2. Infiltrative2. Infiltrative AmyloidAmyloid SarcoidSarcoid Gaucher diseaseGaucher disease Hurler diseaseHurler disease
3. Storage Disease3. Storage Disease HemochromatosisHemochromatosis Fabry diseaseFabry disease Glycogen storageGlycogen storage
EndomyocardialEndomyocardial endomyocardial fibrosisendomyocardial fibrosis Hyperesinophilic syndHyperesinophilic synd CarcinoidCarcinoid metastatic malignanciesmetastatic malignancies radiation, anthracyclineradiation, anthracycline
Clinical ManifestationsClinical Manifestations
Symptoms of right and left heart failureSymptoms of right and left heart failure Jugular Venous Pulse Jugular Venous Pulse
prominent prominent xx and and yy descents descents Echo-DopplerEcho-Doppler
abnormal mitral inflow patternabnormal mitral inflow pattern prominent E wave (rapid diastolic filling)prominent E wave (rapid diastolic filling) reduced deceleration time (reduced deceleration time ( LA pressure) LA pressure)

Basic Life SupportBasic Life SupportBasic Life SupportBasic Life Support
Cardiopulmonary ArrestCardiopulmonary Arrest
Cardiac arrestCardiac arrest is the sudden loss of cardiac output, is the sudden loss of cardiac output, which is potentially reversible with prompt which is potentially reversible with prompt restoration of circulation and oxygen delivery. restoration of circulation and oxygen delivery.
Sudden cardiac deathSudden cardiac death and and cardiac arrestcardiac arrest are not are not synonymous. Sudden cardiac death is unexpected synonymous. Sudden cardiac death is unexpected death within 1 hour of symptom onset because of a death within 1 hour of symptom onset because of a primarily cardiac cause in a victim with or without primarily cardiac cause in a victim with or without previously diagnosed heart disease. previously diagnosed heart disease.
Pathophysiology of CPAPathophysiology of CPA
CPA causes hypoxia, respiratory and metabolic acidosisCPA causes hypoxia, respiratory and metabolic acidosis
cell death appears to be mediated by substances cell death appears to be mediated by substances
released from anoxic cell membranes released from anoxic cell membranes
agents associated with brain and heart injury are free agents associated with brain and heart injury are free
iron, hydroxyl radicals, calciumiron, hydroxyl radicals, calcium
CPA for as little as 5 minutes may cause permanent CPA for as little as 5 minutes may cause permanent
brain injury or deathbrain injury or death
The Most Common Causes of Pediatric The Most Common Causes of Pediatric CPACPAThe Most Common Causes of Pediatric The Most Common Causes of Pediatric CPACPA
infantsinfants SIDS (40%)SIDS (40%) respiratory diseasesrespiratory diseases airway obstructionairway obstruction sepsissepsis neurological diseasesneurological diseases metabolic abnormalitiesmetabolic abnormalities
chidren chidren injuryinjury
Pediatric CPAPediatric CPA
the epidemiology of pediatric CPA is different from that the epidemiology of pediatric CPA is different from that
of adultsof adults
sudden, primary cardiac arrest is raresudden, primary cardiac arrest is rare
ventricular fibrillation has been reported in less than 10% ventricular fibrillation has been reported in less than 10%
(more likely in children with complex congenital heart (more likely in children with complex congenital heart
disease)disease)
respiratory insufficiency is the more common causerespiratory insufficiency is the more common cause
50% of all children who require CPR are infants50% of all children who require CPR are infants
Out-of-Hospital CPAOut-of-Hospital CPAOut-of-Hospital CPAOut-of-Hospital CPA
Out-of-hospital primary cardiac failure with Out-of-hospital primary cardiac failure with cardiopulmonary arrest (CPA) is unusual in cardiopulmonary arrest (CPA) is unusual in children. children.
It may occur in children with chronic diseases It may occur in children with chronic diseases cardiomyopathycardiomyopathy myocarditis myocarditis congenital heart diseases.congenital heart diseases.It occur around the home, where children are under It occur around the home, where children are under
the supervision of parents. the supervision of parents. Parents of children at high risk should be educated in Parents of children at high risk should be educated in
BLS.BLS.
In-Hospital CPAIn-Hospital CPAIn-Hospital CPAIn-Hospital CPA
Primary cardiopulmonary arrest is often in Primary cardiopulmonary arrest is often in hospitalised children hospitalised children
after cardiac surgery after cardiac surgery with rare arrhythmia caused by with rare arrhythmia caused by
cardiac catheterization or angiographycardiac catheterization or angiography general anesthesiageneral anesthesia antiarrhythmic drug administrationantiarrhythmic drug administration
Respiratory Causes of Pediatric Cardiopulmonary ArrestRespiratory Causes of Pediatric Cardiopulmonary Arrest
Upper airway obstructionUpper airway obstruction Lower airway Lower airway obstructionobstruction
- croup- croup - asthma- asthma- foreign body- foreign body - bronchiolitis- bronchiolitis- strangulation- strangulation - foreign body- foreign body- inhalation injury- inhalation injury - inhalation - inhalation
injuryinjury
Intrinsic lung conditionsIntrinsic lung conditions- pneumonia- pneumonia- drowning- drowning- chest trauma- chest trauma
Cardiovascular Causes of Pediatric Cardiopulmonary ArrestCardiovascular Causes of Pediatric Cardiopulmonary ArrestHypovolemiaHypovolemia DysrrhythmiasDysrrhythmias
- trauma- trauma - open heart surgery- open heart surgery
- burns- burns - cardiac catheterization- cardiac catheterization- gastroenteritis- gastroenteritis - coronary angiography- coronary angiography
SepsisSepsis - - general anesthesiageneral anesthesia
Cardiogenic shockCardiogenic shock - prolonged QT syndrom- prolonged QT syndrom
- congenital heart diseases- congenital heart diseases IntoxicationIntoxication- cardiomyopathy- cardiomyopathy- myocarditis- myocarditis- post-open heart surgery- post-open heart surgery
Basic Life SupportBasic Life Support
Strictly defined, Strictly defined, basic life supportbasic life support (BLS) is the initial (BLS) is the initial
phase of emergency cardiac care, encompassing phase of emergency cardiac care, encompassing
recognition of recognition of cardiac arrestcardiac arrest and delivery of rescue and delivery of rescue
breathing (ventilation) and chest compressions breathing (ventilation) and chest compressions
(circulation). (circulation).
Advanced Life SupportAdvanced Life Support
Advanced life supportAdvanced life support (ACLS) includes BLS, ECG (ACLS) includes BLS, ECG
monitoring, rhythm identification, and restoration monitoring, rhythm identification, and restoration
of hemodynamic stability through intubation, of hemodynamic stability through intubation,
defibrillation, and pharmacologic therapy. defibrillation, and pharmacologic therapy.
Cardiopulmonary resuscitation effectively restores Cardiopulmonary resuscitation effectively restores
hemodynamic stability, return of spontaneous hemodynamic stability, return of spontaneous
circulation (ROSC), in 40% to 60% of arrests.circulation (ROSC), in 40% to 60% of arrests.
Modern CRPModern CRP
Modern CPR began in 1960 with the landmark study by Modern CPR began in 1960 with the landmark study by
Kouwenhoven which reported combining closed chest Kouwenhoven which reported combining closed chest
compression, mouth-to-mouth breathing, and external compression, mouth-to-mouth breathing, and external
defibrillation. As they explained it, their algorithm was defibrillation. As they explained it, their algorithm was
remarkably easy to perform: remarkably easy to perform:
""Anyone, anywhere, can now initiate cardiac resuscitative Anyone, anywhere, can now initiate cardiac resuscitative
procedures. All that is needed are two handsprocedures. All that is needed are two hands." ."
Modern CPRModern CPR
Cardiac arrest outcomes will be most improved with public Cardiac arrest outcomes will be most improved with public
education and earlier initiation of CPR, both Basic Life Support education and earlier initiation of CPR, both Basic Life Support
and Advanced Life Support, notably defibrillation.and Advanced Life Support, notably defibrillation.
After unresponsiveness, lack of pulse, and apnea are confirmed in After unresponsiveness, lack of pulse, and apnea are confirmed in
unmonitored cardiac arrests, the initial management consists ofunmonitored cardiac arrests, the initial management consists of
BLSBLS
closed-chest compressionsclosed-chest compressions
artificial ventilation. artificial ventilation.
Circulation: The Cardiac Pump The Cardiac Pump
TheoryTheory Circulation: The Cardiac Pump The Cardiac Pump
TheoryTheory
The mechanism by which closed-chest compressions The mechanism by which closed-chest compressions
increase forward cardiac output remains increase forward cardiac output remains
controversial. controversial.
The traditional cardiac pump theory states the heart is The traditional cardiac pump theory states the heart is
massaged and blood forced out by massaged and blood forced out by direct direct
compressioncompression between the sternum and spine. between the sternum and spine.
Circulation: The Thoracic Pump The Thoracic Pump TheoryTheory Circulation: The Thoracic Pump The Thoracic Pump TheoryTheory The thoracic pump theory suggests that forward blood The thoracic pump theory suggests that forward blood
flow increases through a passive cardiac conduit by a flow increases through a passive cardiac conduit by a
general general increase in intrathoracic pressureincrease in intrathoracic pressure transmitted transmitted
to the cardiac chambers and the intrathoracic to the cardiac chambers and the intrathoracic
portion of the great vessels. Because of intact venous portion of the great vessels. Because of intact venous
valves, the pressure generated during compression is valves, the pressure generated during compression is
not transmitted to the periphery, forcing blood to not transmitted to the periphery, forcing blood to
flow from the arteries to the veins.flow from the arteries to the veins.
The ABCs of Cardiopulmonary ResuscitationThe ABCs of Cardiopulmonary Resuscitation
AAirwayirway BBreathingreathing CCirculationirculation
The ABCs of CPR - ResponsivenessThe ABCs of CPR - Responsiveness
Quickly assess the presence or extent of injury and Quickly assess the presence or extent of injury and determine whether the child is conscious. determine whether the child is conscious.
The level of responsiveness is determined by tapping The level of responsiveness is determined by tapping the child and speaking loudly to elicit a response. the child and speaking loudly to elicit a response.
Carefully look, listen, and feel the pulse to determine Carefully look, listen, and feel the pulse to determine that a cardiopulmonary arrest has occurred.that a cardiopulmonary arrest has occurred.
Call for help once CPA is diagnosed.Call for help once CPA is diagnosed.
The ABCs of CPR - AirwayThe ABCs of CPR - Airway
Open the airway. Use the Open the airway. Use the head-tilt/chin-lift head-tilt/chin-lift
maneuvermaneuver, avoiding hyperextension of the neck. , avoiding hyperextension of the neck.
Too vigorous head-tilt may occlude the trachea or Too vigorous head-tilt may occlude the trachea or
injure the cervical spine. In infants, large head may injure the cervical spine. In infants, large head may
flex the neck and compromise air exchange.flex the neck and compromise air exchange.
If spinal injury is suspected, use a If spinal injury is suspected, use a jaw-thrustjaw-thrust
instead of head-tilt.instead of head-tilt.
Suction may be needed to clear secretions, blood, Suction may be needed to clear secretions, blood,
or foreign bodies from the airway.or foreign bodies from the airway.
Foreign-Body Airway ObstructionForeign-Body Airway Obstruction
the infant: the infant: back blows back blows chest thrustschest thrusts
the child: the Heimlich maneuverthe child: the Heimlich maneuver abdominal thrusts with victim standing or sitting abdominal thrusts with victim standing or sitting
(conscious)(conscious) abdominal thrusts with victim laying or sitting abdominal thrusts with victim laying or sitting
(conscious (conscious or unconscious)or unconscious)
Foreign-Body Airway ObstructionForeign-Body Airway Obstruction
If the airway remains obstructed attempt to evacuate a If the airway remains obstructed attempt to evacuate a possible aspirated foreign body.possible aspirated foreign body.
For infants give 5 sharp For infants give 5 sharp blows to the backblows to the back with the heel with the heel of the hand between securely held shoulder blades. of the hand between securely held shoulder blades. Then, deliver 5 Then, deliver 5 chest thrustschest thrusts to the mid-sternum. to the mid-sternum.
For children deliver 5 rapid subdiaphragmatic For children deliver 5 rapid subdiaphragmatic abdominal thrustabdominal thrusts using the heel of the hand (modifed s using the heel of the hand (modifed Heimlich maneuverHeimlich maneuver) with the patient supine.) with the patient supine.
If airway patency isn’t established, repeat the sequence. If airway patency isn’t established, repeat the sequence. If 2 rapid series of maneuvers fail, perform immediate If 2 rapid series of maneuvers fail, perform immediate direct laryngoscopy to inspect the obstructed area.direct laryngoscopy to inspect the obstructed area.
The ABCs of CPR - Breathing1The ABCs of CPR - Breathing1
Assessment of breathing Assessment of breathing look for a rise and fall of the chest and abdomen, look for a rise and fall of the chest and abdomen,
listen for exhaled air, and feel for exhaled air flow at listen for exhaled air, and feel for exhaled air flow at the mouth or the palmthe mouth or the palm
Rescue breathing Rescue breathing if no spontaneous breathing is detected, begin if no spontaneous breathing is detected, begin mouth-mouth-
to-mouthto-mouth or or mouth-to-nose-and-mouth mouth-to-nose-and-mouth oror bag-valve- bag-valve-maskmask ventilation ventilation
provide 2 slow breaths, pausing after the first one to provide 2 slow breaths, pausing after the first one to take a breath to maximize oxygen content and take a breath to maximize oxygen content and minimize COminimize CO2 2 concentration in the delivered breathsconcentration in the delivered breaths
The ABCs of CPR - Breathing2The ABCs of CPR - Breathing2
rescue breaths are the most important support for rescue breaths are the most important support for
a nonbreathing infant or childa nonbreathing infant or child
the pressure and volume of ventilation should be the pressure and volume of ventilation should be
sufficient to cause the chest to risesufficient to cause the chest to rise
rapidly performed rescue breathing may cause rapidly performed rescue breathing may cause
gastric distention, which elevating the diaphragm gastric distention, which elevating the diaphragm
and decreasing lung volumeand decreasing lung volume
The ABCs of CPR - Circulation1The ABCs of CPR - Circulation1
Assessment of circulationAssessment of circulation
ineffective cardiac contraction will result in the absence of ineffective cardiac contraction will result in the absence of
a palpable pulse in a large central arterya palpable pulse in a large central artery
in children older than 1 yr, the in children older than 1 yr, the carotid arterycarotid artery , on the side , on the side
of the neck, is the most accessible central artery to palpateof the neck, is the most accessible central artery to palpate
in infants palpation of the in infants palpation of the brachial arterybrachial artery is recommended, is recommended,
due to the short, chubby neckdue to the short, chubby neck
the the femoral arteryfemoral artery is often used by health care is often used by health care
professionalsprofessionals
The ABCs of CPR - Circulation2The ABCs of CPR - Circulation2
Chest compressionsChest compressions
serial rhythmic compressions of the chest circulate serial rhythmic compressions of the chest circulate
blood to the vital organs to keep them viable until blood to the vital organs to keep them viable until
advanced life support (ALS) care can be providedadvanced life support (ALS) care can be provided
chest compressions must always be accompanied by chest compressions must always be accompanied by
ventilation ventilation
the child should be supine on a hard, flat surfacethe child should be supine on a hard, flat surface
for an infant the hard surface can be rescuer’s hand or for an infant the hard surface can be rescuer’s hand or
forearmforearm
The ABCs of CPR - Coordination of Compressions and Rescue BreathingThe ABCs of CPR - Coordination of Compressions and Rescue Breathing external chest compression must always be external chest compression must always be
accompanied by rescue breathingaccompanied by rescue breathing at the end of every fifth compression, a pause of 1 to 1.5 at the end of every fifth compression, a pause of 1 to 1.5
sec should be allowed for a ventilationsec should be allowed for a ventilation in infant and child the 5:1 compression-ventilation in infant and child the 5:1 compression-ventilation
ratio is maintained for both one and two rescuers ratio is maintained for both one and two rescuers the infant and child should be reassessed after 20 cycles the infant and child should be reassessed after 20 cycles
of compression and ventilation (apr. 1 min) and every of compression and ventilation (apr. 1 min) and every few minutes thereafterfew minutes thereafter
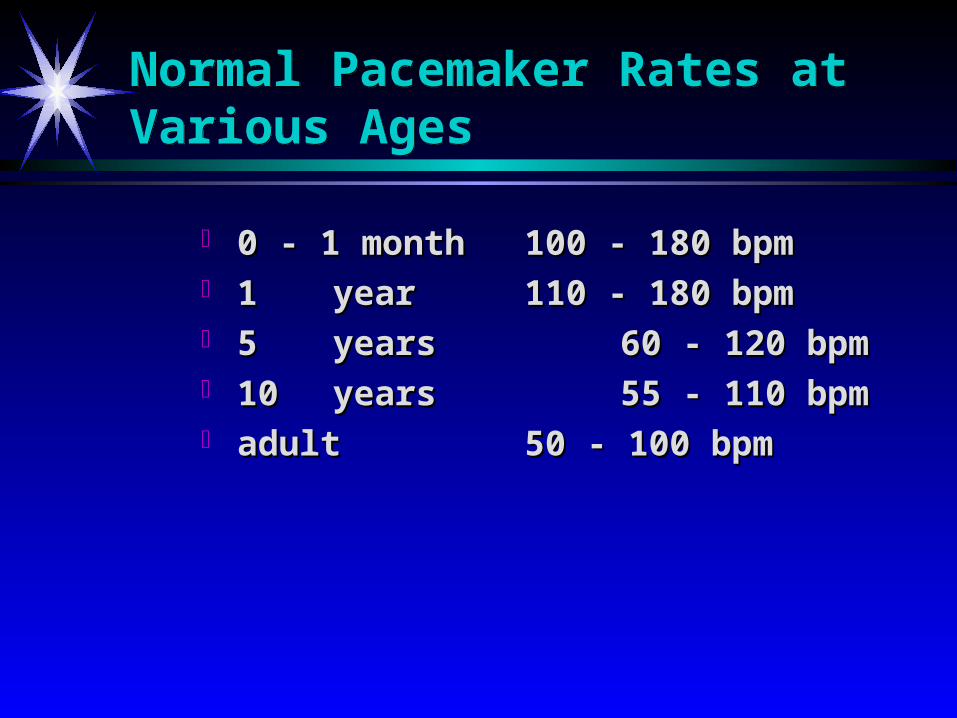
Normal Pacemaker Rates at Various AgesNormal Pacemaker Rates at Various Ages
0 - 1 month 0 - 1 month 100 - 180 bpm100 - 180 bpm 1 1 yearyear 110 - 180 bpm110 - 180 bpm 5 5 yearsyears 60 - 120 bpm60 - 120 bpm 10 10 yearsyears 55 - 110 bpm55 - 110 bpm adultadult 50 - 100 bpm50 - 100 bpm
Advanced Life SupportAdvanced Life SupportAdvanced Life SupportAdvanced Life Support
Medication Administration1 Medication Administration1
venous administration (IV) is the preferred route for drug venous administration (IV) is the preferred route for drug
delivery during advanced life support delivery during advanced life support
in neonatal resuscitation the umbilical vein is more easily in neonatal resuscitation the umbilical vein is more easily
cannulated than scalp or peripheral veinscannulated than scalp or peripheral veins
in older infants and children, peripheral access is usually in older infants and children, peripheral access is usually
more easily established than central accessmore easily established than central access
all doses should be followed by a 5 ml normal saline flush all doses should be followed by a 5 ml normal saline flush
to help move the drug more rapidly into the central to help move the drug more rapidly into the central
circulationcirculation
Medication Administration2Medication Administration2
in patients less than 6 yrs of age, an intraosseous (IO) needle in patients less than 6 yrs of age, an intraosseous (IO) needle
may be usedmay be used
all resuscitation medications, including catecholamines, may all resuscitation medications, including catecholamines, may
be administered into the bone marrowbe administered into the bone marrow
intramuscular (IM) and sublingual (SL) routes are not intramuscular (IM) and sublingual (SL) routes are not
recommended due to delayed drug deliveryrecommended due to delayed drug delivery
intracardiac injection is not recommended due to the risks of intracardiac injection is not recommended due to the risks of
hemopericardium and vessel injury; questionable drug hemopericardium and vessel injury; questionable drug
absorptionabsorption
Medication Administration3Medication Administration3
some medications may be given endotracheally (ET) during some medications may be given endotracheally (ET) during
advanced life support if IV or IO access is unavailableadvanced life support if IV or IO access is unavailable
the dose should be diluted in 3 to 5 ml of normal saline the dose should be diluted in 3 to 5 ml of normal saline
(1 to 2 ml for neonatal resuscitation)(1 to 2 ml for neonatal resuscitation)
catheter inserted below the end of the endotracheal tube catheter inserted below the end of the endotracheal tube
each dose should be followed by several positive-pressure each dose should be followed by several positive-pressure
ventilations using a hand resuscitation bag to ensure drug ventilations using a hand resuscitation bag to ensure drug
deposition into the lungsdeposition into the lungs
Epinephrine1Epinephrine1
epinephrine is the most frequently used resuscitation epinephrine is the most frequently used resuscitation medication in infants and childrenmedication in infants and children
alpha-adrenergic effectsalpha-adrenergic effects cause an intense vasoconstriction, cause an intense vasoconstriction, increases systemic vascular resistance, improves coronary increases systemic vascular resistance, improves coronary blood flowblood flow
reduction in blood flow to renal, mucosal, and dermal reduction in blood flow to renal, mucosal, and dermal vascular beds, preserving blood flow to more critical vascular beds, preserving blood flow to more critical organsorgans
beta-adrenergic effectsbeta-adrenergic effects cause an increase in cardiac cause an increase in cardiac contractility and heart rate, while relaxing smooth musclecontractility and heart rate, while relaxing smooth muscle
Epinephrine2Epinephrine2
epinephrine is used for cardiac arrest, asystole, symptomatic epinephrine is used for cardiac arrest, asystole, symptomatic
bradycardia, and hypotension unrelated to volume depletionbradycardia, and hypotension unrelated to volume depletion
it can be administered every 3 to 5 minutes as neededit can be administered every 3 to 5 minutes as needed
in neonatal resuscitation - 0.01 to 0.03 mg/kg in neonatal resuscitation - 0.01 to 0.03 mg/kg
(0.1 to 0.3 ml/kg of the 1:10,000 solution) IV or ET(0.1 to 0.3 ml/kg of the 1:10,000 solution) IV or ET
in the newborn higher doses are not recommended due to in the newborn higher doses are not recommended due to
risk of intracranial hemorrhage and hypertensionrisk of intracranial hemorrhage and hypertension
in pediatric resuscitation, the recommended initial dose of in pediatric resuscitation, the recommended initial dose of
epinephrine is 0.01 mg/kg (0.1 ml/kg of the 1:10,000 solution) epinephrine is 0.01 mg/kg (0.1 ml/kg of the 1:10,000 solution)
IV for bradycardia and cardiac arrestIV for bradycardia and cardiac arrest
Epinephrine3Epinephrine3
if pulseless arrest persists, the dose may be increased to 0.1 if pulseless arrest persists, the dose may be increased to 0.1 mg/kg (0.1 ml/kg of the 1:1000 solutionmg/kg (0.1 ml/kg of the 1:1000 solution
this is the same dose used for endotracheal administration (ET)this is the same dose used for endotracheal administration (ET) patients with continued hypotension, epinephrine may be given patients with continued hypotension, epinephrine may be given
as a continuous infusion (drip)as a continuous infusion (drip) starting dose is 2 mcg/kg/min, with the infusion rate then starting dose is 2 mcg/kg/min, with the infusion rate then
reduced to maintain the desired response, usually to 0.1 to 1 reduced to maintain the desired response, usually to 0.1 to 1 mcg/kg/min. mcg/kg/min.
infusion of doses greater than 5 mcg/kg/min may produce infusion of doses greater than 5 mcg/kg/min may produce profound vasoconstriction at the site of administrationprofound vasoconstriction at the site of administration
AcidosisAcidosis mixed metabolic and respiratory acidosis is common during mixed metabolic and respiratory acidosis is common during
cardiopulmonary arrest as a result of anaerobic metabolism cardiopulmonary arrest as a result of anaerobic metabolism
and carbon dioxide retentionand carbon dioxide retention
acidosis may cause a decrease in myocardial contractility, acidosis may cause a decrease in myocardial contractility,
lowering of blood pressure, and a blunting of the response to lowering of blood pressure, and a blunting of the response to
catecholamines catecholamines
optimal method to reverse this situation is to provide optimal method to reverse this situation is to provide
adequate ventilation (excretion of COadequate ventilation (excretion of CO22) and systemic ) and systemic
perfusionperfusion
sodium bicarbonate is reserved for sodium bicarbonate is reserved for severe metabolic acidosissevere metabolic acidosis
and only when ventilatory support can be assuredand only when ventilatory support can be assured

Sodium Bicarbonate1 - Paradoxical AcidosisSodium Bicarbonate1 - Paradoxical Acidosis bicarbonate infusion has the potential to induce bicarbonate infusion has the potential to induce
paradoxical intracellular and central nervous system paradoxical intracellular and central nervous system
acidosisacidosis
it combines with protons (Hit combines with protons (H++) to produce CO) to produce CO22 and water and water
COCO2 2 is freely diffusable into myocytes and the is freely diffusable into myocytes and the
subarachnoid space where it combines with water to subarachnoid space where it combines with water to
produce free hydrogen ions (COproduce free hydrogen ions (CO22 + H + H22O = HO = H+ + + HCO+ HCO33--))
Sodium Bicarbonate2Sodium Bicarbonate2
standard dose is 1 to 2 mEq/kg IV or IOstandard dose is 1 to 2 mEq/kg IV or IO additional doses (0.5 mEq/kg) should be guided by additional doses (0.5 mEq/kg) should be guided by
assessment of laboratory valuesassessment of laboratory values standard solutions of 8.4% (1 mEq/ml) sodium bicarbonate standard solutions of 8.4% (1 mEq/ml) sodium bicarbonate
are very hyperosmolar (2,000 mOsm/L) and should be used are very hyperosmolar (2,000 mOsm/L) and should be used with cautionwith caution
in neonates, only the 4.2% (0.5 mEq/ml) solution should be in neonates, only the 4.2% (0.5 mEq/ml) solution should be used to avoid increasing the risk of intraventricular used to avoid increasing the risk of intraventricular hemorrhagehemorrhage
rate of administration should be no greater than 1 rate of administration should be no greater than 1 mEq/kg/minmEq/kg/min
Sodium Bicarbonate3Sodium Bicarbonate3
sodium bicarbonate should not be given sodium bicarbonate should not be given
endotracheallyendotracheally
- - it can cause substantial tissue injury it can cause substantial tissue injury
it should not be mixed with other medications it should not be mixed with other medications
-- precipitation of calcium and inactivation of precipitation of calcium and inactivation of
catecholamines may occur if they are mixed with catecholamines may occur if they are mixed with
sodium bicarbonatesodium bicarbonate
Atropine - indicationsAtropine - indications
treatment of symptomatic bradycardia, as a treatment of symptomatic bradycardia, as a second-line therapy after epinephrinesecond-line therapy after epinephrine
bradycardia as the result of increased vagal tone bradycardia as the result of increased vagal tone (such as during intubation) (such as during intubation)
bradycardia as the result of documented bradycardia as the result of documented atrioventricular blockatrioventricular block
AtropineAtropine
in children, the dose of atropine is 0.02 mg/kg in children, the dose of atropine is 0.02 mg/kg
IV,ET or IO, with a minimum dose of 0.1 mg to IV,ET or IO, with a minimum dose of 0.1 mg to
avoid paradoxical bradycardiaavoid paradoxical bradycardia
the recommended maximum single dose is 0.5 mg the recommended maximum single dose is 0.5 mg
for a child and 1 mg for an adolescent or adultfor a child and 1 mg for an adolescent or adult
this dose may be repeated once, if no response is this dose may be repeated once, if no response is
seen within 5 minutesseen within 5 minutes
Naloxone - indicationsNaloxone - indications
pure antagonist which reverses the effects of opioids pure antagonist which reverses the effects of opioids
such as morphine and fentanylsuch as morphine and fentanyl
in resuscitations, it is used to reverse the respiratory in resuscitations, it is used to reverse the respiratory
and central nervous system depression and and central nervous system depression and
hypertension caused by administration of opioids hypertension caused by administration of opioids
naloxone is also indicated for severe respiratory naloxone is also indicated for severe respiratory
depression in neonates whose mothers received opioids depression in neonates whose mothers received opioids
within four hours of deliverywithin four hours of delivery
NaloxoneNaloxone naloxone acts within 2 to 3 minutes and has a duration of naloxone acts within 2 to 3 minutes and has a duration of
30 to 60 minutes30 to 60 minutes dose for total reversal is 0.1 mg/kg for infants and children dose for total reversal is 0.1 mg/kg for infants and children
up to 5 years of age or 20 kg body weightup to 5 years of age or 20 kg body weight children over 5 years or 20 kg should receive a standard 2 children over 5 years or 20 kg should receive a standard 2
mg dosemg dose smaller doses may be used if only partial opioid reversal is smaller doses may be used if only partial opioid reversal is
desireddesired naloxone may be administered by rapid IV push, IO, or ETnaloxone may be administered by rapid IV push, IO, or ET intramuscular or subcutaneous administration may result intramuscular or subcutaneous administration may result
in erratic absorption and reduced efficacyin erratic absorption and reduced efficacy
Calcium chlorideCalcium chloride
calcium enhance cardiac contractility and increase calcium enhance cardiac contractility and increase systemic vascular resistancesystemic vascular resistance
calcium administration is recommended calcium administration is recommended only in cases ofonly in cases of hypocalcemia, hyperkalemia, hypermagnesemia, and hypocalcemia, hyperkalemia, hypermagnesemia, and calcium channel blocker overdosecalcium channel blocker overdose
dose of calcium chloride is 0.2 to 0.25 ml/kg of a 10% dose of calcium chloride is 0.2 to 0.25 ml/kg of a 10% solution, to provide 5 to 7 mg/kg elemental calcium (20 solution, to provide 5 to 7 mg/kg elemental calcium (20 to 25 mg/kg calcium salt)to 25 mg/kg calcium salt)
this dose should be infused at a rate this dose should be infused at a rate no fasterno faster than 100 than 100 mg/min and may be repeated one time - rapid infusion mg/min and may be repeated one time - rapid infusion may result in bradycardia or asystolemay result in bradycardia or asystole
Dopamine - indicationsDopamine - indications
patients who remain hypotensive or poorly perfused patients who remain hypotensive or poorly perfused
after initial resuscitationafter initial resuscitation
dopamine acts at a variety of receptorsdopamine acts at a variety of receptors
dopaminergicdopaminergic 2 to 5 mcg/kg/min2 to 5 mcg/kg/min
beta-adrenergicbeta-adrenergic above 5 mcg/kg/minabove 5 mcg/kg/min
alpha-adrenergicalpha-adrenergic 10 to 20 mcg/kg/min10 to 20 mcg/kg/min
DopamineDopamine
low doses, 2 to 5 mcg/kg/min, dopamine causing increased low doses, 2 to 5 mcg/kg/min, dopamine causing increased renal, coronary, splanchnic, and cerebral blood flowrenal, coronary, splanchnic, and cerebral blood flow
above 5 mcg/kg/min, dopamine stimulates beta-adrenergic above 5 mcg/kg/min, dopamine stimulates beta-adrenergic receptors and increases release of norepinephrine, receptors and increases release of norepinephrine, producing an increase in cardiac contractilityproducing an increase in cardiac contractility
in the range of 10 to 20 mcg/kg/min, dopamine begins to in the range of 10 to 20 mcg/kg/min, dopamine begins to act at alpha-adrenergic receptors, producing act at alpha-adrenergic receptors, producing vasoconstriction and significant tachycardiavasoconstriction and significant tachycardia
because of its rapid elimination, dopamine can only be because of its rapid elimination, dopamine can only be administered as a administered as a continuous infusioncontinuous infusion
DobutamineDobutamine
dobutamine stimulates beta-adrenergic receptors and dobutamine stimulates beta-adrenergic receptors and
produces a positive inotropic responseproduces a positive inotropic response
it does not act on dopaminergic or alpha-adrenergic it does not act on dopaminergic or alpha-adrenergic
receptorsreceptors
dobutamine produces a mild vasodilatationdobutamine produces a mild vasodilatation
it is recommended in cases of cardiogenic or septic shock it is recommended in cases of cardiogenic or septic shock
when the patient is not already hypotensivewhen the patient is not already hypotensive
dobutamine is typically started at a dose of 5 mcg/kg/min and dobutamine is typically started at a dose of 5 mcg/kg/min and
titrated to achieve the desired blood pressure responsetitrated to achieve the desired blood pressure response
AdenosineAdenosine
adenosine is a pharmacologic alternative to defibrillation adenosine is a pharmacologic alternative to defibrillation
in patients with supraventricular tachycardiain patients with supraventricular tachycardia
produces a transient block of the atrioventricular nodeproduces a transient block of the atrioventricular node
its short elimination half-life (approximately 9 seconds) its short elimination half-life (approximately 9 seconds)
makes it a safe medication, but also makes it difficult to makes it a safe medication, but also makes it difficult to
get adequate drug concentrations at the site of actionget adequate drug concentrations at the site of action
dose for infants and children is 0.1 to 0.2 mg/kg dose for infants and children is 0.1 to 0.2 mg/kg
administered by rapid IV push, followed immediately by a administered by rapid IV push, followed immediately by a
2 to 3 ml normal saline flush (maximum dose is 12 mg)2 to 3 ml normal saline flush (maximum dose is 12 mg)
LidocaineLidocaine
lidocaine is used to control ventricular tachycardia or lidocaine is used to control ventricular tachycardia or
fibrillationfibrillation
recommended method of administration is a 1 mg/kg recommended method of administration is a 1 mg/kg
bolus loading dose, followed by a continuous infusion of bolus loading dose, followed by a continuous infusion of
20 to 50 mcg/kg/min20 to 50 mcg/kg/min the dosage should be reduced in children with low the dosage should be reduced in children with low
cardiac output or reduced hepatic blood flow or cardiac output or reduced hepatic blood flow or function to avoid lidocaine accumulationfunction to avoid lidocaine accumulation
signs of toxicity include drowsiness, confusion, tremors, signs of toxicity include drowsiness, confusion, tremors, and seizures.and seizures.