Pediatric asthma diagnosis
25
ن م ح ر ل ها ل ل ما س ب م ي ح ر ل ا
-
Upload
hisham-alrabty -
Category
Health & Medicine
-
view
103 -
download
1
Transcript of Pediatric asthma diagnosis

الرحمن الله بسمالرحيم

Pediatric asthma diagnosis
By Dr Hisham AlrabtyPediatric consultant and pulmonologist
Tripoli teaching children hospital

There is no global consensus concerned asthma diagnosis in children.There is no a single test diagnostic to asthma in children whatever was blood ,skin or imaging(radiological).Asthma can be diagnosed in children aged less than 2 years with exclusion of other causes of recurrent wheeze like GERD.
Facts:

To diagnose asthma in children you should pass by
next steps:
Good history.Clinical examination.Some investigational
procedures(peak flow metry).

Personal history of asthma or allergy.Recurrent wheeze and shortness of breath.Bronchodilator use as nebulizer or syrup.History of previous admission because of wheeze.History of chronic cough certainly at night.History of breathlessness on exercise.Patient has eczema or AR.Symptoms relieved by bronchodilators.Symptoms exacerbated by cold last more than 10 days.Symptoms got worse by either animal dander,emotion,dust,smoke,drugs,dust mite. from gina asthma
booklet
History:

Signs of respiratory distress:tachypnea.Wheeze.Flaring alae nasii.Cyanosis.Chest indrawings.Decreased air entry.Rhonchi +/- rales.Silent chest.Hypoxia.
Clinical examination:

**By detailed history and clinical evaluation we could diagnose asthma in children in more than 95% of cases, the remaining 5% of cases we could seek help of some
investigation/s .
It should not be done on routine basis for each asthma episode only when we suspect patient could have complication like pneumothorax.
Chest x ray:
CBC:High IgE and eosinophilia indicate the child is allergic.

Hyper inflated chest

Results of pulmonary function testing are not reliable in patients younger than 5 years. In young children (3-6 y) and older children who are unable to perform the conventional spirometry maneuver, newer techniques, such as measurement of airway resistance using impulse oscillometry system, are used. By which measurement of airway resistance before and after a dose of inhaled bronchodilator may help to diagnose bronchodilator-responsive airway obstruction.
Pulmonary Function Tests:

impulse oscillometry system

In a typical case, an obstructive defect is present in the form of normal forced vital capacity (FVC), reduced forced expiratory volume in 1 second (FEV1), and reduced forced expiratory flow more than 25-75% of the FVC (FEF 25-75). Documentation of reversibility of airway obstruction after bronchodilator therapy is central to the definition of asthma. FEF 25-75 is a sensitive indicator of obstruction and may be the only abnormality in a child with mild disease.
Spirometry:

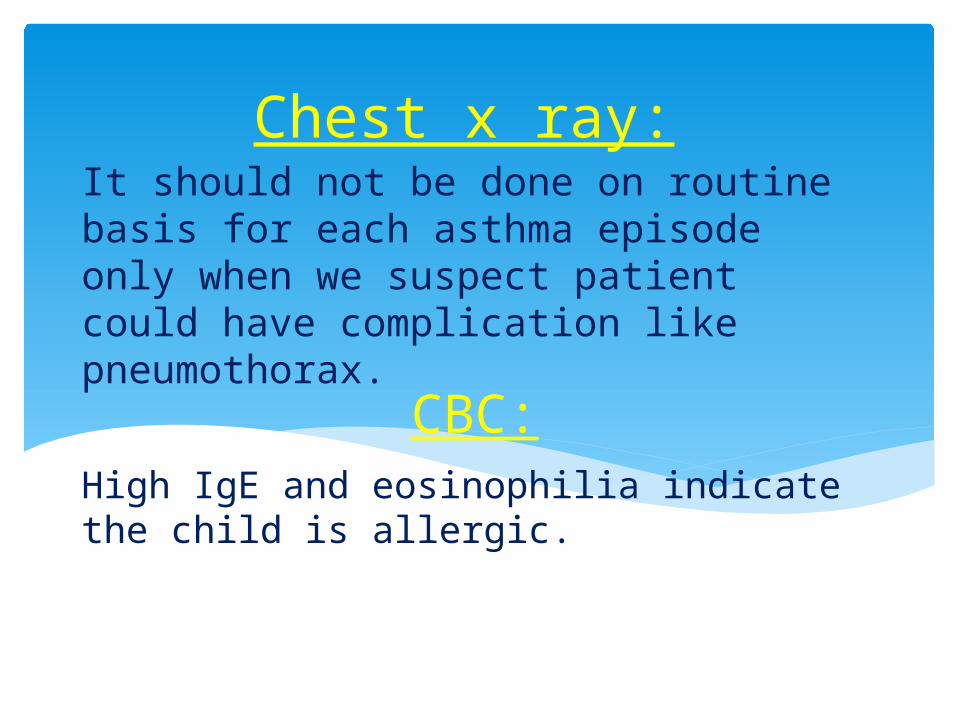
Patients with chronic persistent asthma may have hyperinflation, as evidenced by an increased total lung capacity (TLC) at Plethysmography. Increased residual volume (RV) and functional residual capacity (FRC) with normal TLC suggests air trapping. Airway resistance is increased when significant obstruction is present.
Plethysmography:
Plethysmography

It could be measured before and after dose of inhaled bronchodilator and if there were improvement by 15% , it is asthma.It can be used as monitor for asthma control.
Peak expiratory flow merty:

In patient has history of exercise induced symptoms this test could be done to establish diagnosis of asthma.Done in kids age more than 6 yrs.Baseline spirometry followed by exercise on treadmill or bicycle till heart rate reaches 60% of predicted maximum under monitor of ECG and pulse oxymeter.Then spirometry done at 3.5,10,15 and 20 min interval.Then assess reversibility of airway obstruction by neb.bronchodilator.
Exercise challenge:

Either by use of inhaled methacholine or histamine to induce wheeze in suspected patient and they should be done by experienced personnel in specialized labs.It is neither applicable nor practical certainly in children.Positive response is 20% fall in FEV1.
Asthma provocative tests:
Either specific igE level in blood or skin brick test both are done to recognize the allergen/s patient is sensitized to, in patients do not respond to maximum treatment of chromic asthma, both are not diagnostic.
Allergen detecting tests:
Measuring the fraction of exhaled nitric oxide (FeNO) has proved useful as a noninvasive marker of airway inflammation, in order to guide adjustment of the dose of inhaled corticosteroids. in some patients, the FeNO rose before significant exacerbations of the asthma.Due to the high cost of equipment, FeNO measurement is used primarily as a research tool at present.
Fraction of Exhaled Nitric Oxide Testing:

Measuring the level of interleukin-5 in exhaled breath condensate is a possible way of titrating asthma progress, according to one study. In a longitudinal study of 40 asthmatic children aged 6-16 years, asthma control score and level of interleukin-5 were significant predictors of an asthma exacerbation..
Measuring the level of interleukin-5:

It will reveal infiltration with inflammatory cells, narrowing of airway Lumina, bronchial and bronchiolar epithelial denudation and mucus plugs.Thickened basement membrane and airway remodeling in form of severe subepithelial fibrosis and smooth muscle hypertrophy or hyperplasia in severe cases of chronic asthma.
Histological findings:

Like chest CT,MRI, bronchoscopy, gatrograffin study, sweat test, 24 ph monitoring… all done to exclude other causes of recurrent wheeze.
Other investigations:

Major criteria:Parent with asthma.Physician diagnosed atopic dermatitis.Minor criteria:Physician diagnosed allergic rhinitis.Eosinophilia (>4%).Wheezing apart from colds.If the child has more than 4 episodes of wheezing per year lasting more than 1 day affecting sleep with one MAJOR or two MINOR criteria.It is asthma upto this index…
Asthma Predictive Index:

Conclusively asthma is still clinical based
diagnosis.

Thanks for attention and
attendance