Pediatric Anesthesia Basics 2012 Laura Downey, MD Yun-Sheen Liu, MD Julie Williamson, DO.
24
Pediatric Pediatric Anesthesia Basics Anesthesia Basics 2012 2012 Laura Downey, MD Laura Downey, MD Yun-Sheen Liu, MD Yun-Sheen Liu, MD Julie Williamson, DO Julie Williamson, DO
-
Upload
meryl-sullivan -
Category
Documents
-
view
215 -
download
1
Transcript of Pediatric Anesthesia Basics 2012 Laura Downey, MD Yun-Sheen Liu, MD Julie Williamson, DO.

Pediatric Pediatric Anesthesia BasicsAnesthesia Basics
20122012
Laura Downey, MDLaura Downey, MD
Yun-Sheen Liu, MDYun-Sheen Liu, MD
Julie Williamson, DOJulie Williamson, DO

NPO guidelinesNPO guidelines
Solids/formula = 6hSolids/formula = 6h Breast milk = 4hBreast milk = 4h Clears = 2hClears = 2h
Older kids should be NPO after Older kids should be NPO after
midnightmidnight Chewing gum and candy are Chewing gum and candy are
considered clear liquids considered clear liquids

PremedicationPremedication
IV PremedIV Premed 0.5mg/kg Versed for toddlers, up to 2 mg of 0.5mg/kg Versed for toddlers, up to 2 mg of
IV Versed for children >5 yearsIV Versed for children >5 years Oral Medication – order 20-30min Oral Medication – order 20-30min
before case to be given by pre-op before case to be given by pre-op holding RNsholding RNs <6mo = usually no premed needed<6mo = usually no premed needed 6mo to 12y = oral premed (0.5 mg/kg up to 6mo to 12y = oral premed (0.5 mg/kg up to
20 mg)20 mg) Over 12y = IV in pre-op areaOver 12y = IV in pre-op area

Set Up: T-MSMAIDSet Up: T-MSMAID
TableTable MachineMachine SuctionSuction MonitorsMonitors AirwayAirway IV IV DrugsDrugs
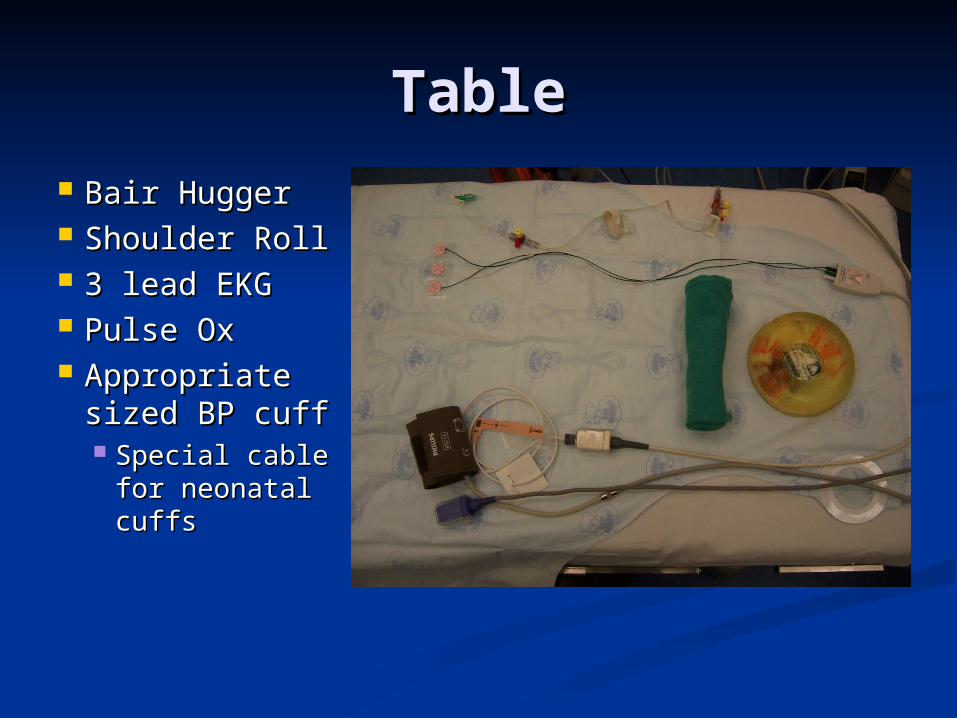
TableTable
Bair HuggerBair Hugger Shoulder RollShoulder Roll 3 lead EKG3 lead EKG Pulse OxPulse Ox Appropriate Appropriate
sized BP cuffsized BP cuff Special cable Special cable
for neonatal for neonatal cuffscuffs

Machine Machine
Standard Machine checkStandard Machine check Monitor set to Neonate or Pediatric Monitor set to Neonate or Pediatric
ModeMode Reset alarms for age appropriate Reset alarms for age appropriate
vitalsvitals

SuctionSuction
Red rubber Rob Nell for little kidsRed rubber Rob Nell for little kids
Yankauers may be in anesthesia Yankauers may be in anesthesia machine or on surgical shelves. machine or on surgical shelves. Have available before induction.Have available before induction.
Turn on suctionTurn on suction

MonitorsMonitors
BP cuff of appropriate sizeBP cuff of appropriate size Pulse oxPulse ox 3 lead EKG3 lead EKG
White lead on rightWhite lead on right Green lead is V5 and equivalent to red Green lead is V5 and equivalent to red
lead in adultslead in adults

AirwayAirway ETT (3)ETT (3)
One half size bigger and One half size bigger and one half size smallerone half size smaller Appropriate size styletAppropriate size stylet
Two laryngoscope bladesTwo laryngoscope blades Oral airwaysOral airways Flavored face maskFlavored face mask Cloth white tape to secure ETTCloth white tape to secure ETT
Two Y-stripsTwo Y-strips Red rubber for suctionRed rubber for suction Eye tape: Eye tape:
Paper tape > 1yearPaper tape > 1year Mepitec for <1 yearMepitec for <1 year or fragile skinor fragile skin
Mepitec
Cloth Tape

ETTETT
Size based on Size based on the child’s pinky the child’s pinky or (age/4) + 4or (age/4) + 4
Subtract 0.5 size Subtract 0.5 size for cuffed tubefor cuffed tube
Have one half-Have one half-size smaller and size smaller and larger availablelarger available

Laryngoscope bladesLaryngoscope blades
for babies up to 3 months: Miller 0for babies up to 3 months: Miller 0 for babies aged 3 months to 18 months: for babies aged 3 months to 18 months:
Miller 1Miller 1 for 18 month- 3 years: Miller 1.5, Mac 1, for 18 month- 3 years: Miller 1.5, Mac 1,
Wisc 1.5Wisc 1.5 for 3-5 years: Miller 1.5, Mac 2, Wisc 1.5for 3-5 years: Miller 1.5, Mac 2, Wisc 1.5 for >5 years: Miller 2, Mac 2-3for >5 years: Miller 2, Mac 2-3
Note: Mac 4 is not standard in room. You Note: Mac 4 is not standard in room. You will need to request one from techwill need to request one from tech

AirwayAGE For
mula
32 weeks
Term
3 mo
6mo 12 mo
18 mo
2 yr 3 yr 5 yr 10 yr
Kg 2.0 3.5 5.0 6.0 8 11 13 15 20 40
ETT size
(age/4) +4
2.5 3.0 3.5 3.5 4.0 4.5 4.5 4.5 5.0 5.5
ETT depth
ETT size*3
7.5 9.0 10.5 10.5 12.0 13.5 13.5 13.5 15.0
Blade
Mil 0 Mil 0 Mil 0 Mil 1 Mil 1 Mil 1 Wis 1.5Mac 1
Mil 1.5Mac 1
Mil 1.5Mac 2
Mil 2Mac 2-3
LMA
1 1 1 1.5 1.5 2 2 2 2.5-3

IVIV IV supplies – in kidney basinIV supplies – in kidney basin
mini tourniquet – cut tomini tourniquet – cut to half width for small babieshalf width for small babies Alcohol padsAlcohol pads 20, 22, 24g PIV catheters20, 22, 24g PIV catheters OpsitesOpsites 2x2 gauze2x2 gauze Paper tape for additionalPaper tape for additional reinforcementreinforcement ScissorsScissors Arm boardArm board Syringe with T-pieceSyringe with T-piece

IV continuedIV continued Debubble all buretrols and Debubble all buretrols and
IV sets. Green clip should IV sets. Green clip should be left in open positionbe left in open position A bubble is a bullet to A bubble is a bullet to
the brain – Boltzthe brain – Boltz Draw back on syringes Draw back on syringes
to de-air before injectingto de-air before injecting Children <6m should have Children <6m should have
dextrose infusiondextrose infusion Buretrol IV set for <2yoBuretrol IV set for <2yo
Microdripper for <12 yoMicrodripper for <12 yo Buretrols a
re currently
out of
stock. 2
50cc bags for p
atients
<5 yo or syrin
ge pump for IV
F
for
infants.

Drugs Pyxis machine in OR
Contains: Emergency drugs, opioids, induction agents Note that ketamine comes in 100mg/ml (for IM injection) and
10mg/ml Albumin, Crystalloid, Dextrose
Access: 6 digit dictation number + password or fingerprint
LPCH Pharmacy (near OR 7): Call to have drips made for big cases – 721-2731. Can
be ordered in advance under “Anesthesia OR drips” in Cerner.
10mcg/ml pre-made Epinephrine sticks available Stanford Main OR Pharmacy:
Sign out a green box for patients going for procedures in Stanford Hospital (AMC, interventional radiology)

DrugsDrugs Emergency DrugsEmergency Drugs
SuxSux 4-6 mg/kg on IM needle 4-6 mg/kg on IM needle AtropineAtropine 0.02 mg/kg on IM 0.02 mg/kg on IM
needleneedle EphedrineEphedrine 10cc of 5mg/cc 10cc of 5mg/cc PhenylephrinePhenylephrine
1 syringe of 100ug/cc1 syringe of 100ug/cc 1 syringe of 10ug/cc1 syringe of 10ug/cc
EpinephrineEpinephrine 10 mcg/cc 10 mcg/cc
Two syringes of saline flush Two syringes of saline flush
Have small syringes and needles available.
Do not draw up for EVERY case.

Other emergency drugsOther emergency drugs
Calcium Chloride Calcium Chloride 10cc of 100mg/cc10cc of 100mg/cc 10cc of 10mg/cc10cc of 10mg/cc
Sodium bicarbonateSodium bicarbonate 8.4% 1 mEq/cc for patients >1 year8.4% 1 mEq/cc for patients >1 year Note dilute solution for infantsNote dilute solution for infants
Syringes of 5% albuminSyringes of 5% albumin

Induction DrugsInduction Drugs
Ketamine – 0.5-5 mg/kg IV, 3-5 Ketamine – 0.5-5 mg/kg IV, 3-5 mg/kg IMmg/kg IM
Propofol – 2-3 mg/kg IVPropofol – 2-3 mg/kg IV Time and date all syringes. Discard Time and date all syringes. Discard
after 6 hours.after 6 hours. Rocuronium 0.6-1.2 mg/kg, dilute to Rocuronium 0.6-1.2 mg/kg, dilute to
1 mg/cc for children <1 years1 mg/cc for children <1 years

Pain medicationsPain medications PRPR acetaminophenacetaminophen 30-40 mg/kg (single 30-40 mg/kg (single
dose)dose) IVIV acetaminophenacetaminophen dose is age dependent: dose is age dependent:
10mg/kg <2 years. 15 mg/kg >2 years. Re-10mg/kg <2 years. 15 mg/kg >2 years. Re-dose Q 6 hours. Slow push/infusion over 15 dose Q 6 hours. Slow push/infusion over 15 minutes.minutes.
ToradolToradol 0.5 mg/kg IV or IM 0.5 mg/kg IV or IM FentanylFentanyl single dose 0.5 to 1 mcg/kg, single dose 0.5 to 1 mcg/kg,
dilute to 1 mcg/cc for babies, 10 mcg/cc for dilute to 1 mcg/cc for babies, 10 mcg/cc for children<10 yearschildren<10 years
MorphineMorphine single dose 0.1 mg/kg IV single dose 0.1 mg/kg IV HydromorphoneHydromorphone single dose 10 mcg/kg IV single dose 10 mcg/kg IV

Flow of the OR Pre-op: Ground floor of LPCH outside OR
Patient admitted to Pre-op where NPs see patients and often start care form
Holding: 8 bed area in OR suite Inpatients are brought to holding when <30 min until
case start Patients too big to carry out of pre-op are brought to
holding for premed Need GO sticker before you can leave holding OR
7 main ORs MRI/CT suites on ground floor APU – outpatient procedures on 1st floor LPCH
PACU: next to holding area ICUs are all on 2nd floor LPCH

May I have a GO?.....
GO stickers: H and P from surgeon (with 24 hour update) Preoperative note from anesthesia signed by
attending Patient marked Room is ready
First “time out” is done in pre-op at patient’s bedside. Check MRN, birth date, allergies.
GO!

Maneuvering the Paperwork
Cerner Powerchart is LPCH EMR User name and Password are the same as for OB
EMR access from home is on LPCH intranet: https://intranet.lpch.org Or access from ether.stanford.edu Intranet password is different password than
Cerner Choose LINKS from menu and Powerchart Sign into Cerner

How do I find my schedule?
In Cerner: Choose compass icon (Explorer
Menu) Open Main Menu Folder Open Perioperative
Services Folder Choose Perioperative
Schedule In Gray Box:
Surgery All Areas Bookshelf: Choose LPCH Perioperative All Areas Bookshelf
View Master View Execute This generates the daily
schedule with Anesthesia Attending, Resident, Patient name and number and site

Finding information Old Anesthesia
Records: Clinical Documents Tab:
(after 9/2009) OR and Procedure Notes
Anesthesia Records, Anesthesia Pre-Op
Scanned Documents Tab: (before 9/2009)
OR and Procedure Notes Under ClinDocs, Care
Forms, Pre Anesthesia NP note
ECHOS/EKG Clin Docs Tab
Ancillary Documents