Pediatric Airway Management
86
Pediatric Airway Management گ ن ت ر آد آ ر ر مه ر کت د س ن آ س آدآره آورر ی ی ر گاه ش ن ی دآ ن ا ن س مار$ ی& ت س ی’ ی1392/4/1
-
Upload
cedric-wilson -
Category
Documents
-
view
49 -
download
0
description
Pediatric Airway Management. دکتر مهرزاد آرتنگ رییس اداره اورژانس پیش بیمارستانی دانشگاه 1392/4/1. Pediatric Cardiopulmonary Arrests. In most infants and small children respiratory arrest precedes cardiac arrest. Characteristics of Newborn Respiratory System. - PowerPoint PPT Presentation
Transcript of Pediatric Airway Management

Pediatric Airway Management
دکتر مهرزاد آرتنگ
رییس اداره اورژانس پیش بیمارستانی
دانشگاه1392/4/1

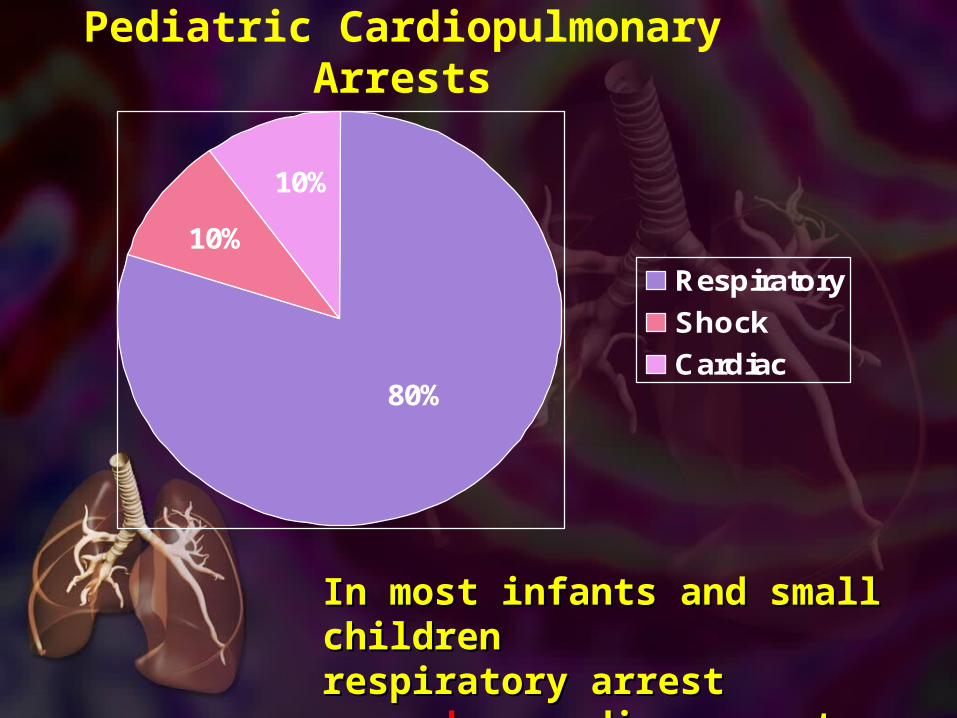
Pediatric Cardiopulmonary Arrests
10%
10%
80%
Respiratory
Shock
Cardiac
In most infants and small In most infants and small children respiratory children respiratory arrest arrest precedesprecedes cardiac cardiac arrest. arrest.
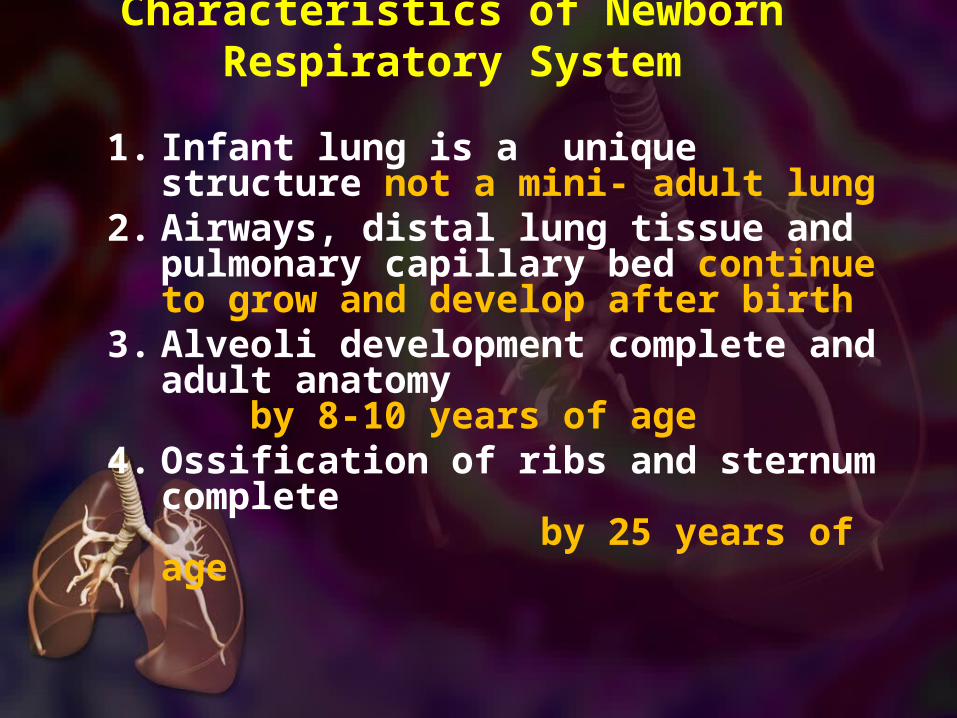
Characteristics of Newborn Respiratory System
1. Infant lung is a unique structure not a mini- adult lung
2. Airways, distal lung tissue and pulmonary capillary bed continue to grow and develop after birth
3. Alveoli development complete and adult anatomy by 8-10 years of age
4. Ossification of ribs and sternum complete by 25 years of age

Nose• Obligatory nasal breathing• Poor tolerance to
obstruction
• Relatively Large• Neck extension may not
relieve obstruction
Tongue
Head
• Relatively large• Anterior flexion may cause
airway obstruction
• Relatively large and U- shaped
• More susceptible to trauma• Forms more acute angle
with vocal cords
Epiglottis
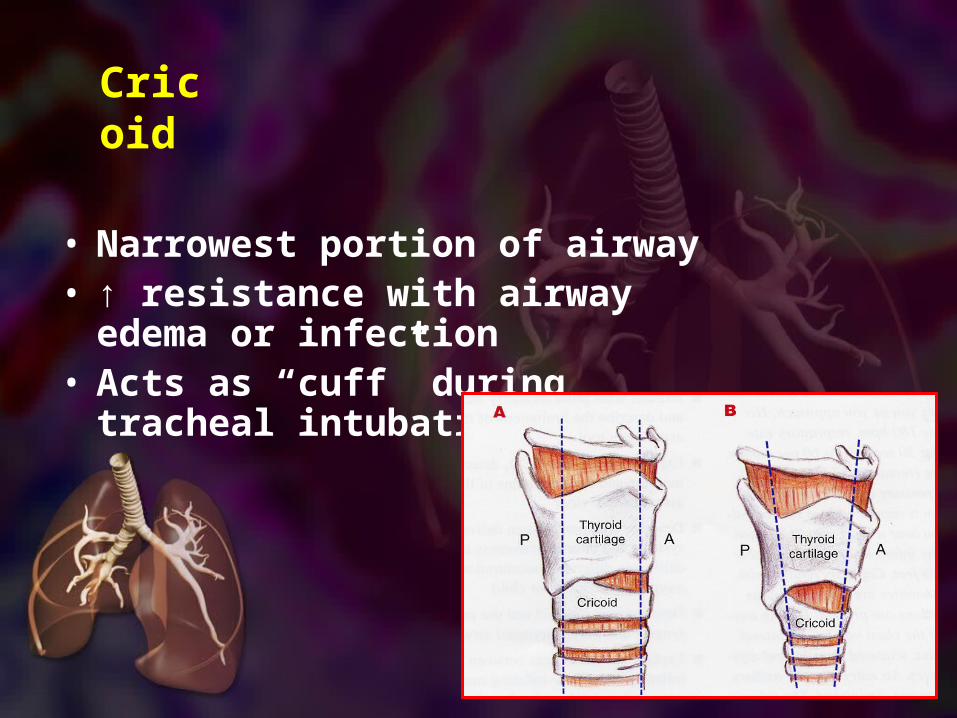
• Narrowest portion of airway• ↑ resistance with airway
edema or infection• Acts as “cuff” during
tracheal intubation
Cricoid
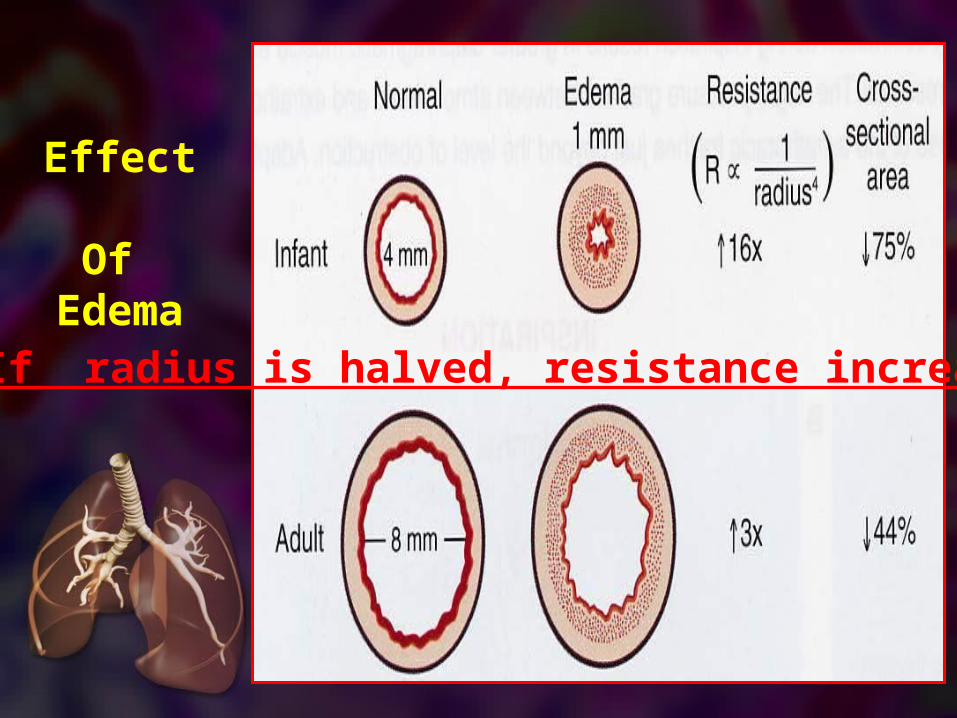
Effect Of
Edema
If radius is halved, resistance increases 16 x
Trachea• Small diameter (6mm), high
compliance• ↑ resistance with airway edema or
infection• Collapses easily with neck
hyperflexion or hyperextension
↑ pulmonary vascular resistance (PVR)Very sensitive to constriction by hypoxia, acidosis and hypercarbia
WOB
• Weak resp muscles
• Response to ↓ O2/ ↑ CO2 minimal
• Tolerates hypoxia poorly
Regulation of Breathing

Assessment
• 30 second rapid cardiopulmonary assessment is structured around ABC’s.
• Airway• Breathing• Circulation
Airway
• Airway must be clear and patent for successful ventilation.
• Position• Clear of foreign body• Free from injury
•Intubate if needed
“Patients do not die from lack of intubation
they die from lack of oxygenation”
Cricoid Pressure (Sellick's Maneuver)
• Cricoid pressure is indicated in the intubation of those who are deeply unconscious and in those who have been paralyzed for intubation.
Breathing
• Breathing is assessed to determine the child’s ability to oxygenate.
• Assessment:• Respiratory rate• Respiratory effort• Breath sounds• Skin color
Impending Respiratory Failure
• Respiratory rate less than 10 or greater than 60 is an ominous sign of impending respiratory failure.
Prearrest. sPrearrest. s
Airway assessment
• Best to 1st look from afar. Infants and small children don’t like strangers hard to assess baseline after they are upset.
• Is the chest moving?• Can you hear breath sounds?• Are there any abnormal airway
sounds ? (e.g.. Stridor, snoring)• Is there increased respiratory effort
with retractions or respiratory effort with no airway or breath sounds?
Breathing
• RR• Effort• Airway and lung sounds• SpO2
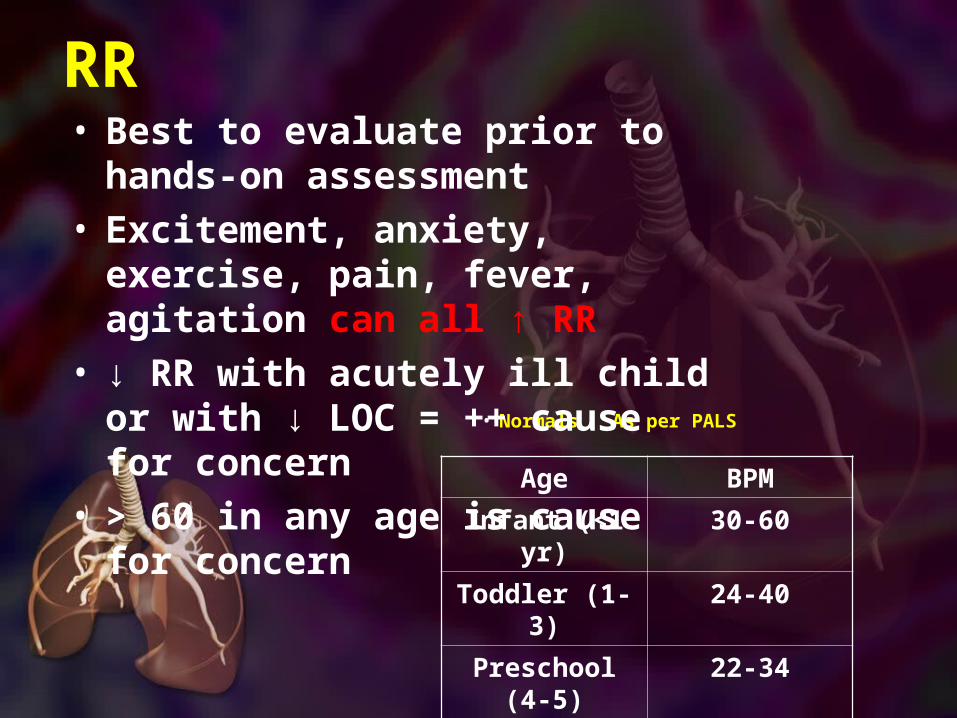
RR
• Normals As per PALS
Age BPM
Infant (<1 yr)
30-60
Toddler (1-3)
24-40
Preschool (4-5)
22-34
School age (6-12)
18-30
Adolescent(13-18)
12-16
• Best to evaluate prior to hands-on assessment
• Excitement, anxiety, exercise, pain, fever, agitation can all ↑ RR
• ↓ RR with acutely ill child or with ↓ LOC = ++ cause for concern
• > 60 in any age is cause for concern
Signs of Respiratory Distress
• Tachypnea• Tachycardia• Grunting • Stridor• Head bobbing• Flaring• Agitation
• Retractions• Access
muscles• Wheezing• Sweating• Prolonged
expiration• Apnea• Cyanosis

Lung Sounds
• Normal • Wheezes• Rales
(Crackles)• Stridor• Rhonchi• Pleural Rub
• Listen on every patient
• End of Expiration
• End of Inspiration
• During both phases
• Expiration• End of
Inspiration
Airway Management
• Simple things to improve airway Simple things to improve airway patencypatency• Suction nose and oropharynx• child/ allow child to assume
position of comfort• head-tilt-chin lift/ jaw thrust • Use airway adjuncts - NPA/ OPA
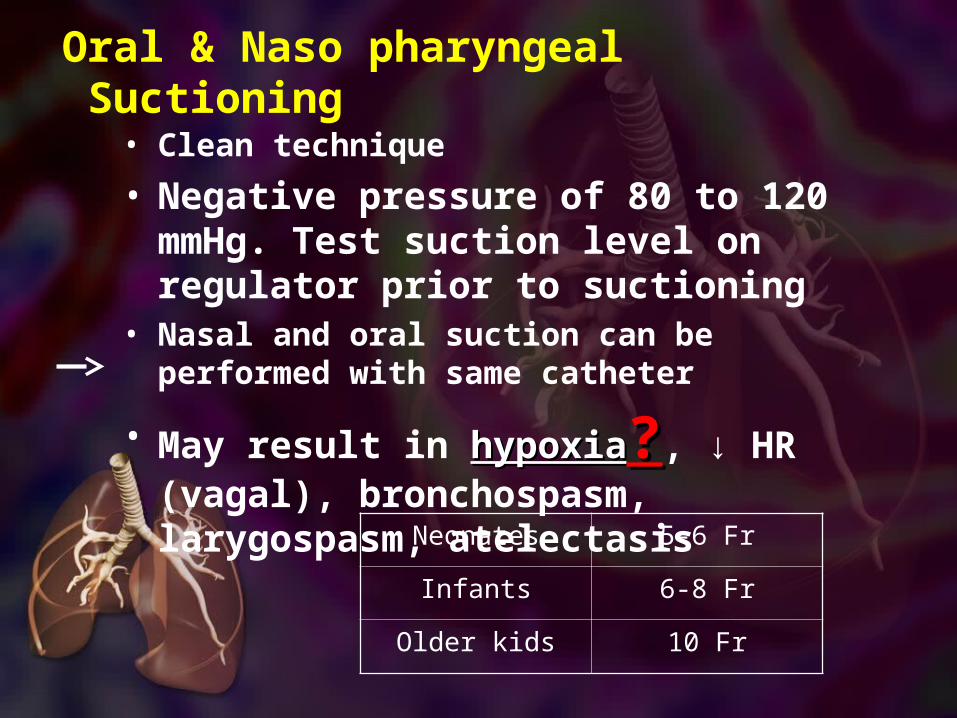
Oral & Naso pharyngeal Suctioning
• Clean technique
• Negative pressure of 80 to 120 mmHg. Test suction level on regulator prior to suctioning
• Nasal and oral suction can be performed with same catheter
• May result in hypoxiahypoxia??, ↓ HR (vagal), bronchospasm, larygospasm, atelectasisNeonates 5-6 Fr
Infants 6-8 Fr
Older kids 10 Fr
هیپوکسی و ساکشن
برای جلوگیری از این مشکل •، ساکشن کردن را به
ثانیه 5ثانیه در بالغین و 15در اطفال محدود کنید .
Oral Pharyngeal Airways (OPA)
• Only for use in UNCONSCIOUS pt with no intact cough/gag reflex
• Never tape in place
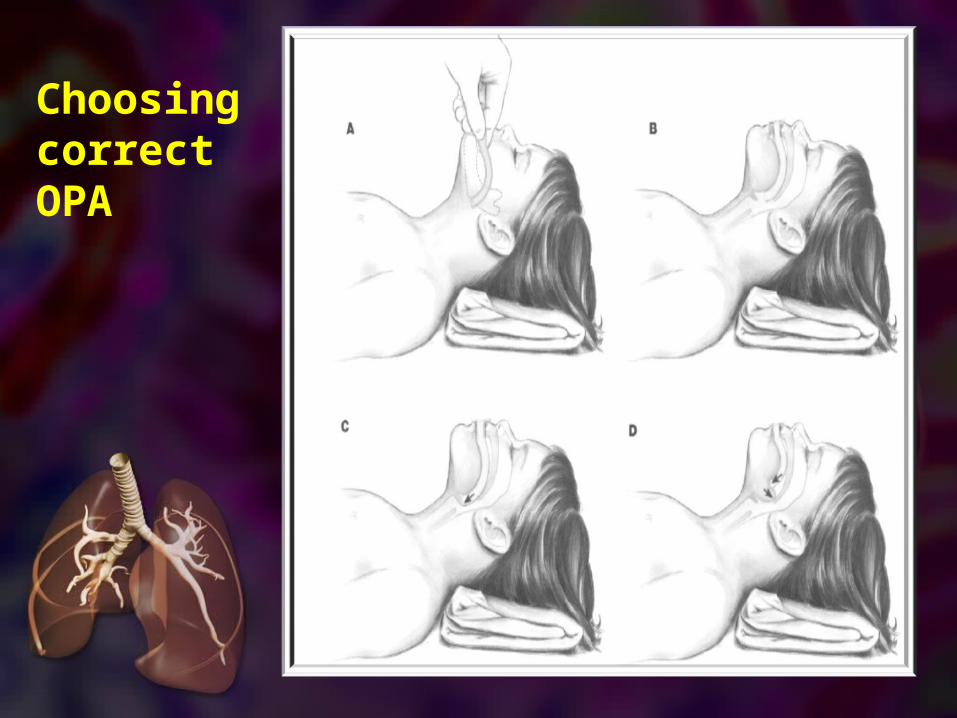
Choosing correct OPA
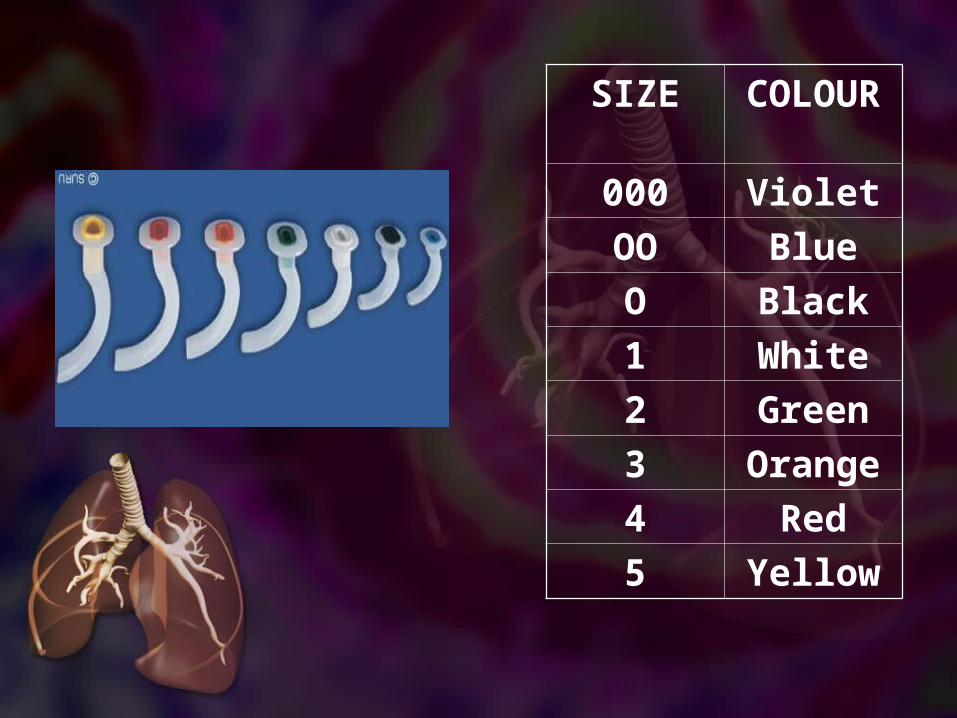
SIZE COLOUR
000 Violet
OO Blue
O Black
1 White
2 Green
3 Orange
4 Red
5 Yellow
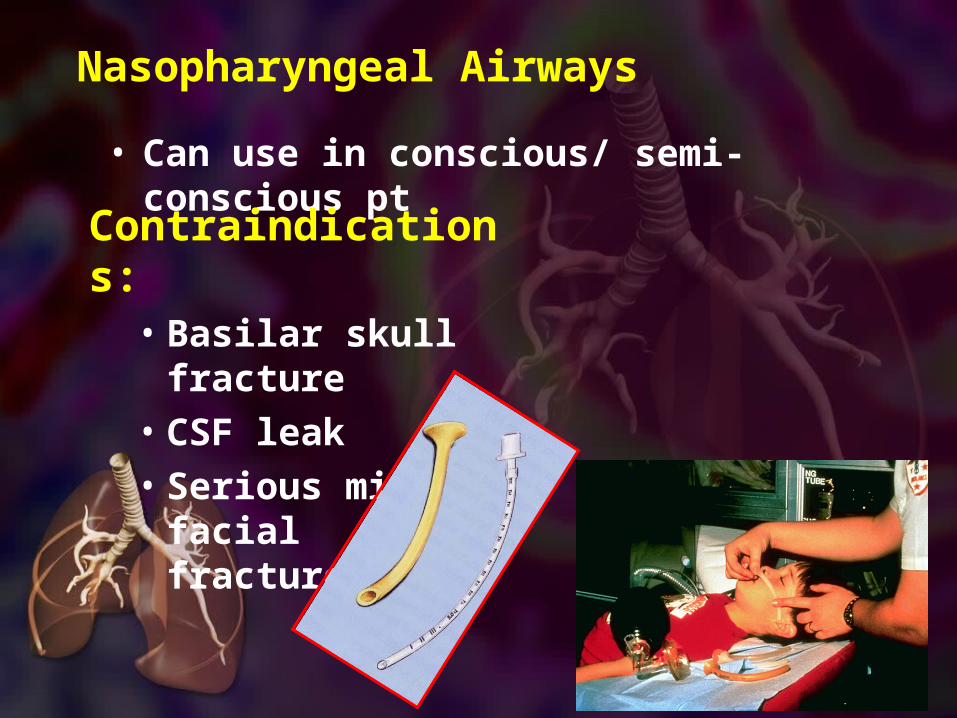
Nasopharyngeal Airways
• Can use in conscious/ semi-conscious pt
Contraindications:
• Basilar skull fracture
• CSF leak• Serious midline
facial fractures

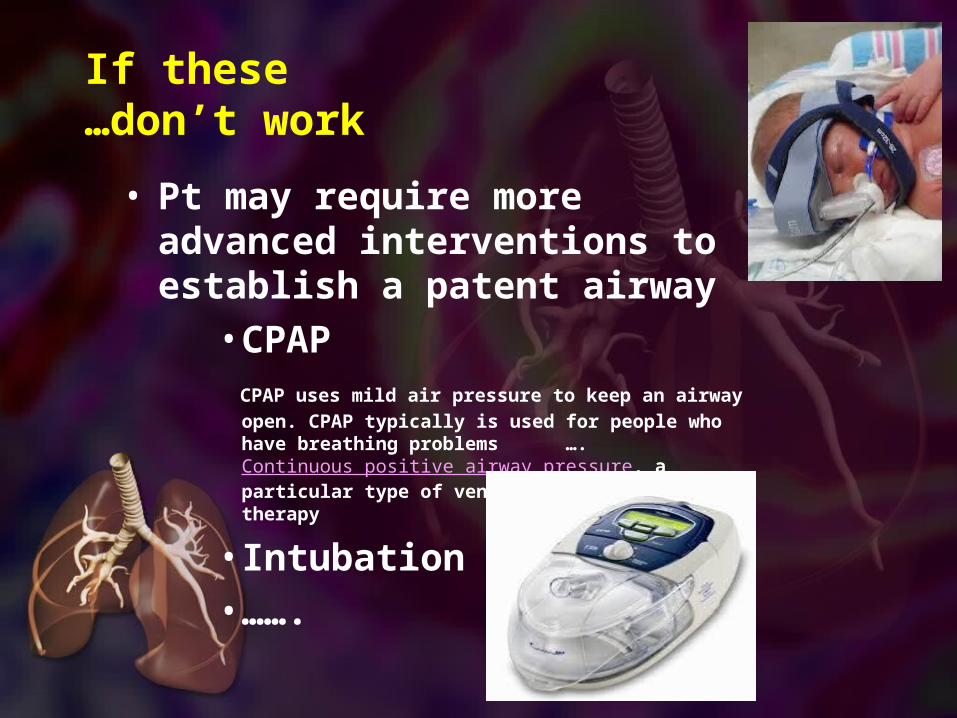
If these don’t work…
• Pt may require more advanced interventions to establish a patent airway
•CPAP CPAP uses mild air pressure to keep an airway
open. CPAP typically is used for people who have breathing problems …. Continuous positive airway pressure, a particular type of ventilation (breathing) therapy
•Intubation•…….
Positionning
• If pt has preferred position let them remain in that position e.g. tripod
• Repositioning can greatly improve airway patency
• Manual airway maneuvers can also help open the airway (head tilt-chin lift/ jaw thrust)
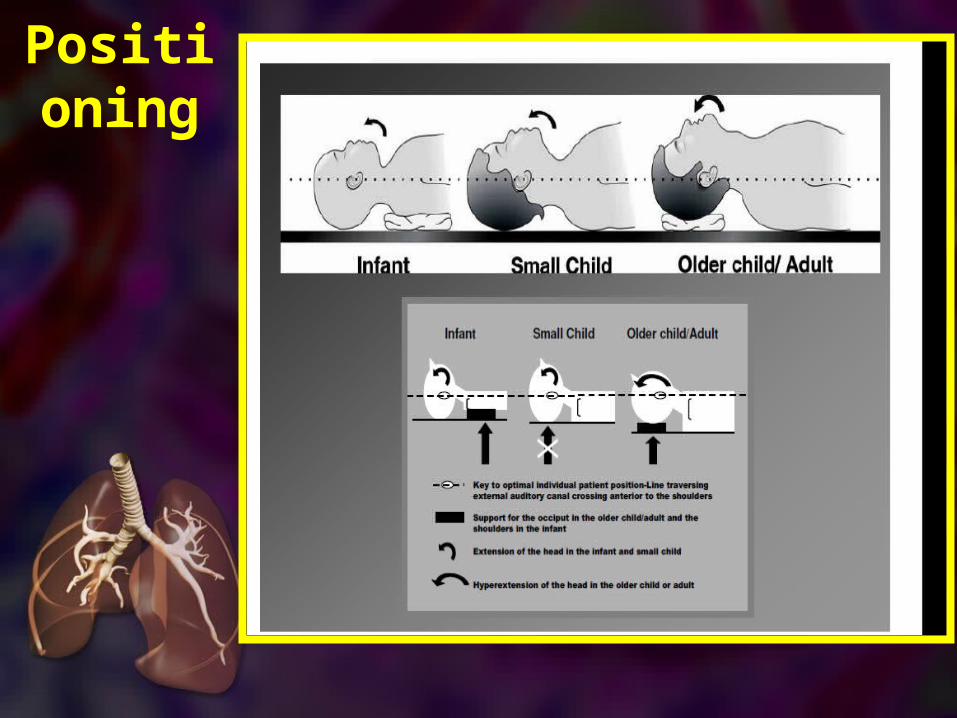
Positioning
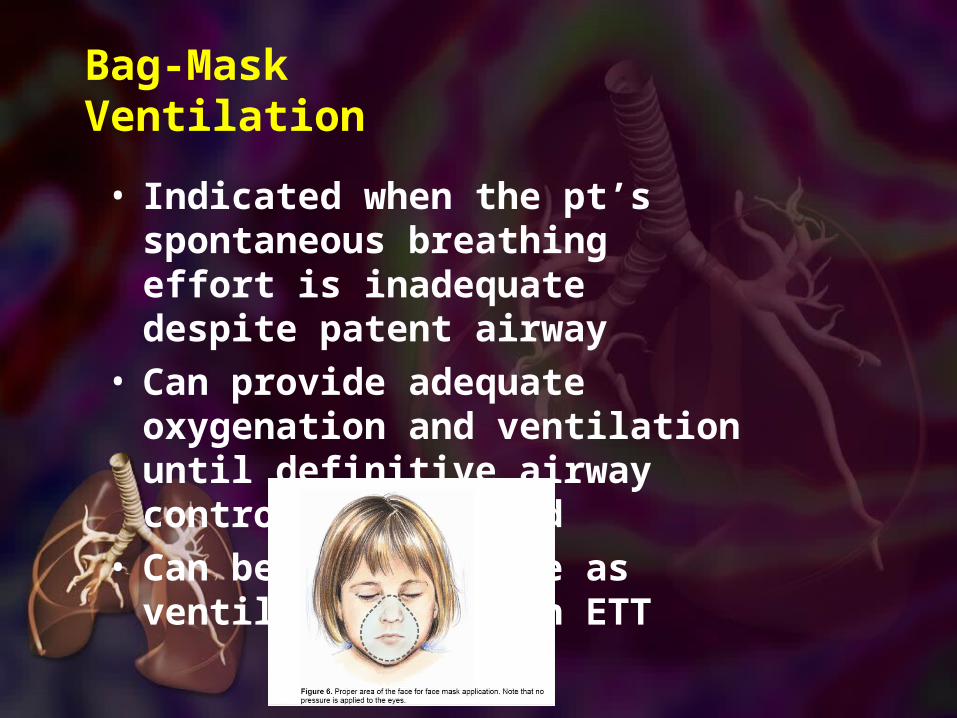
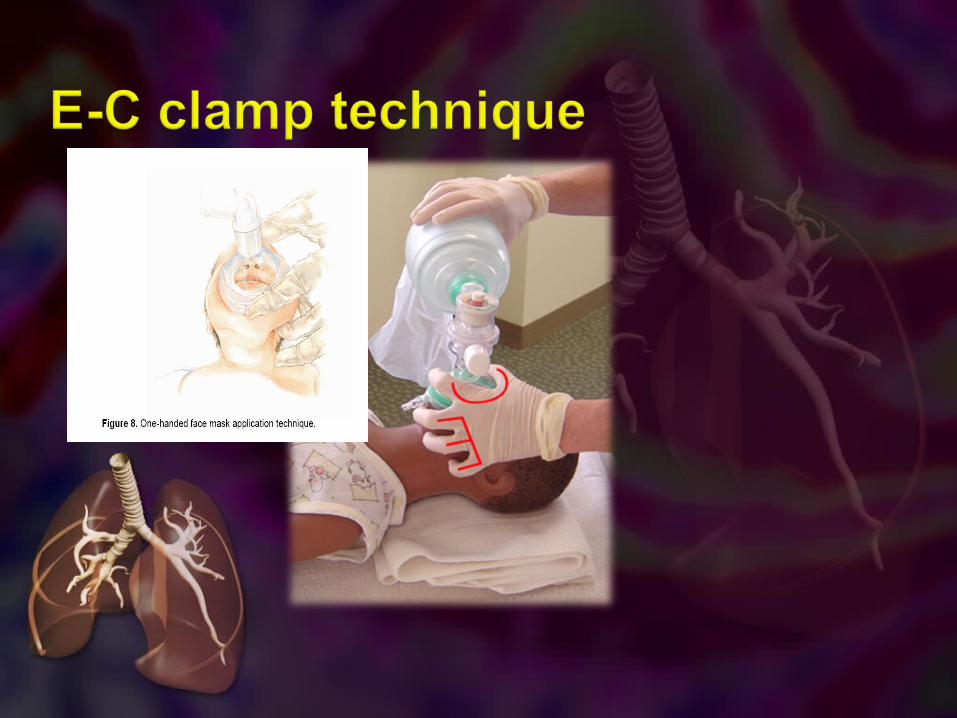
Bag-Mask Ventilation
• Indicated when the pt’s spontaneous breathing effort is inadequate despite patent airway
• Can provide adequate oxygenation and ventilation until definitive airway control is obtained
• Can be as effective as ventilation through ETT
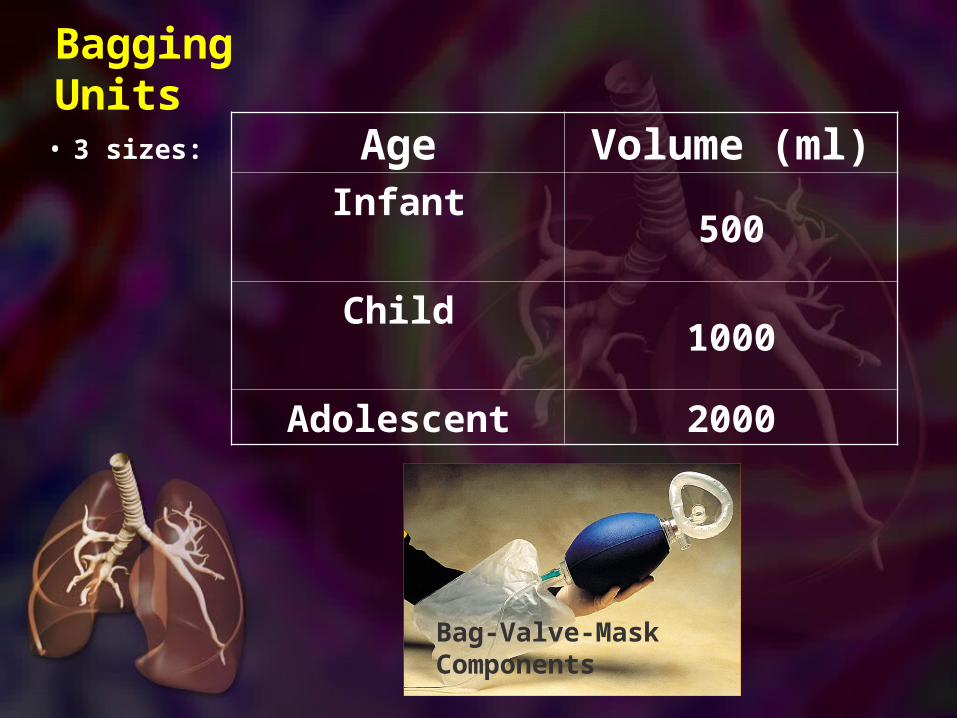
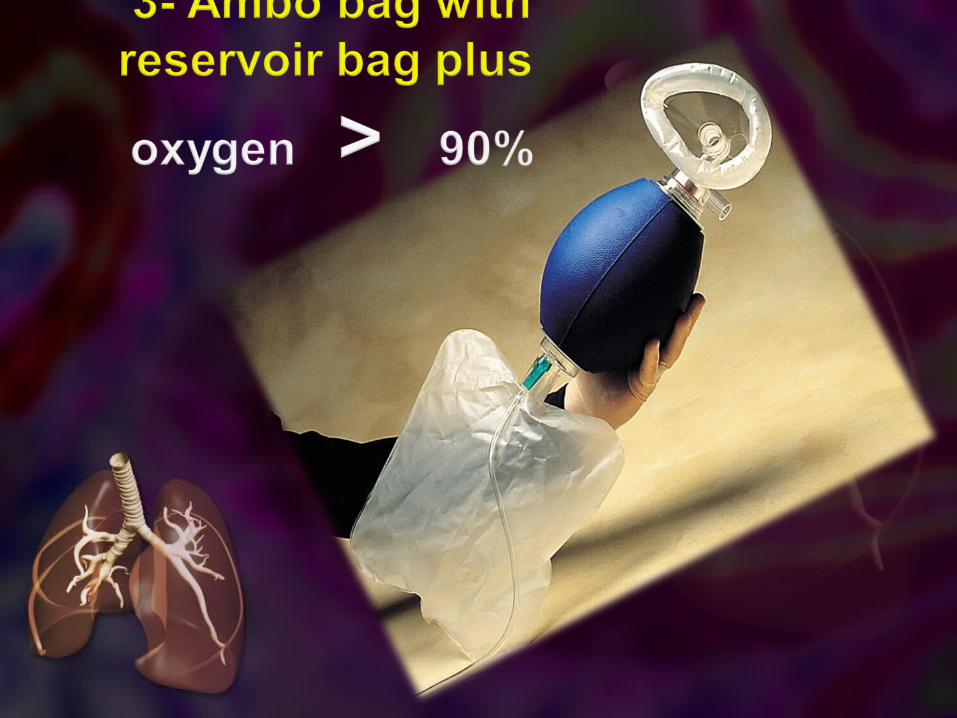
Bagging Units• 3
sizes:Age Volume (ml)
Infant500
Child1000
Adolescent 2000
Bag-Valve-Mask Components
Testing the bagging unit
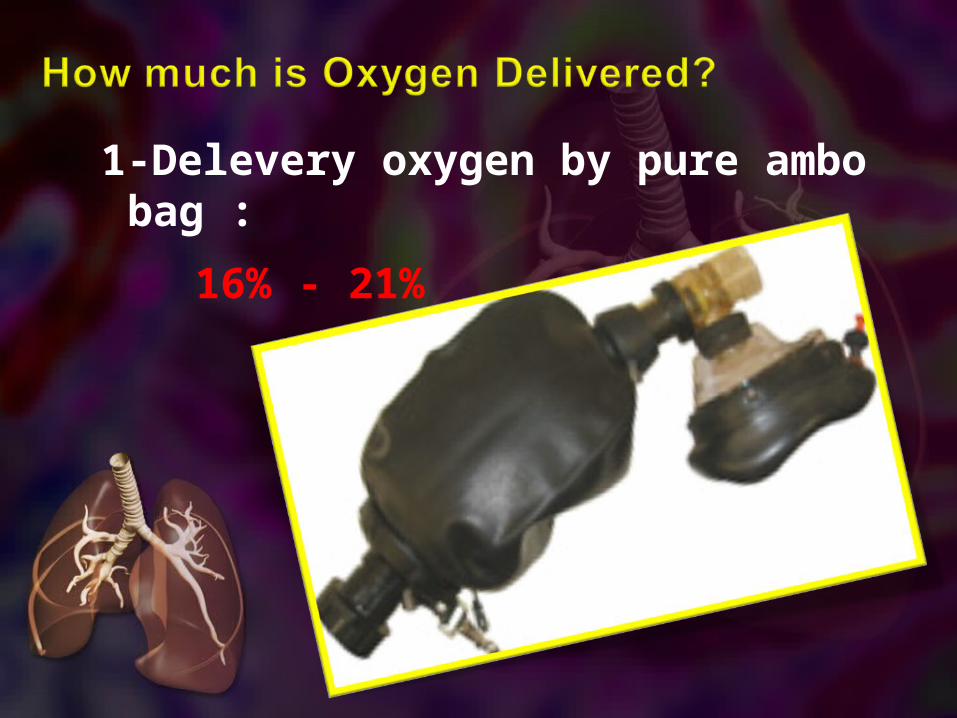
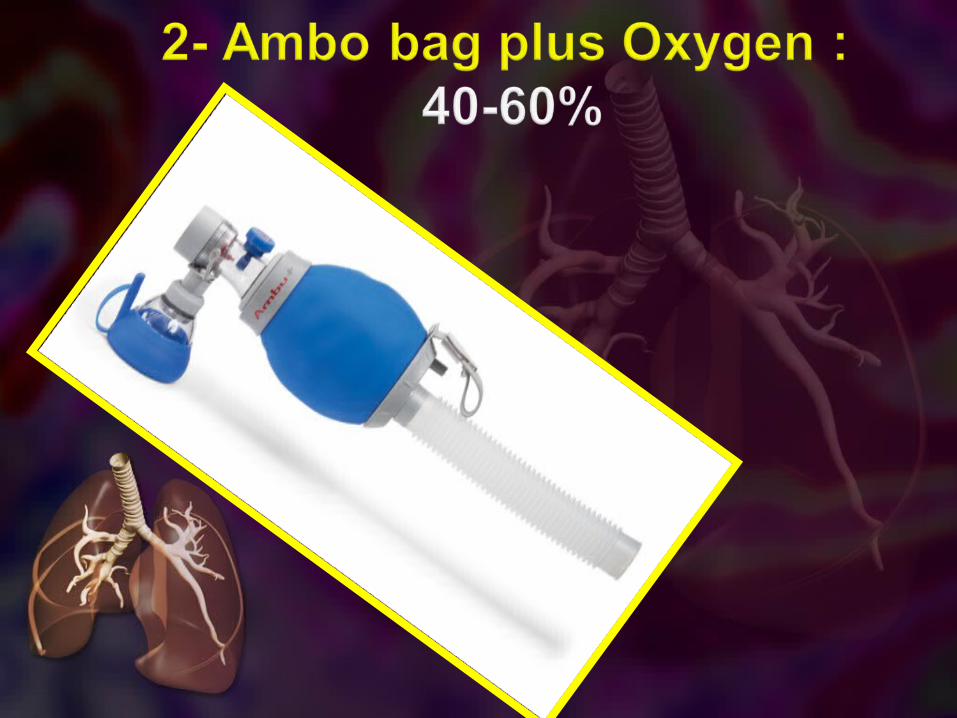
1-Delevery oxygen by pure ambo bag :
16% - 21%
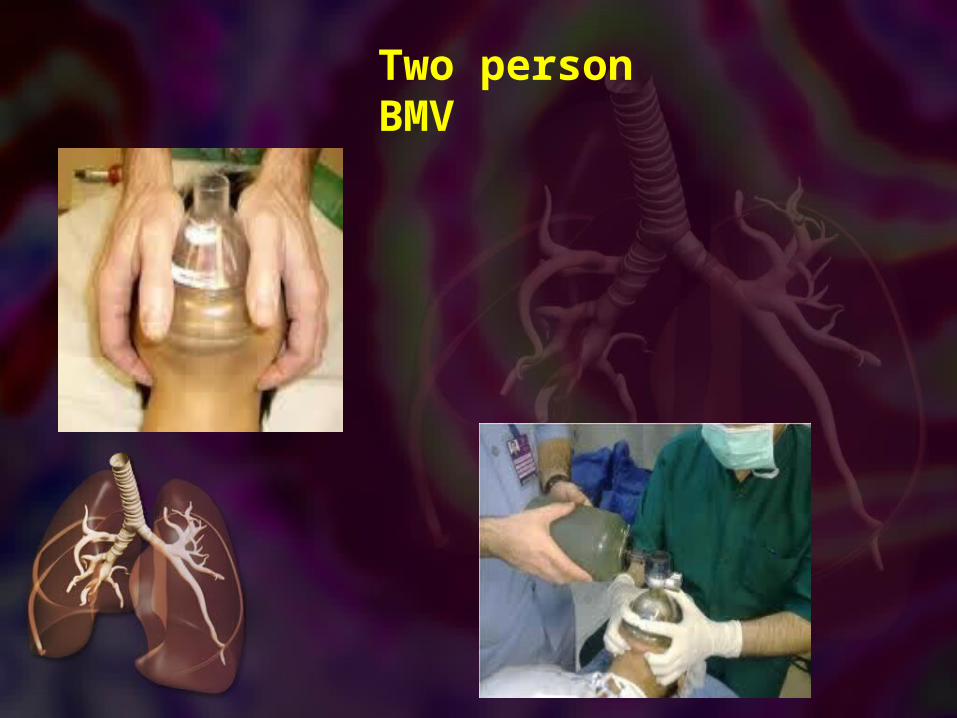
Two person BMV
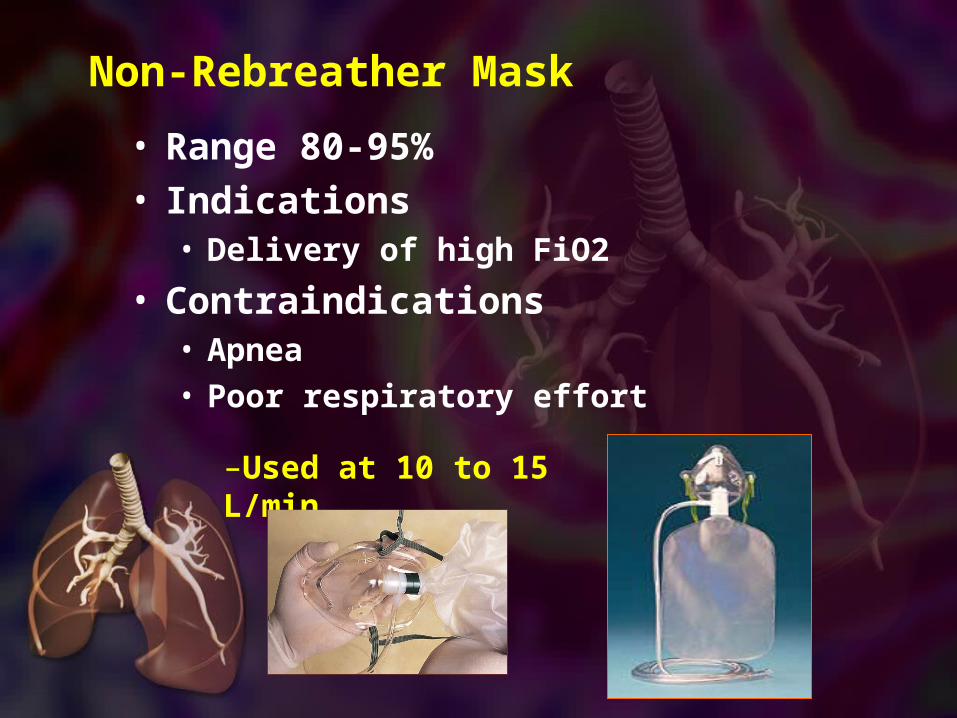
Non-Rebreather Mask
• Range 80-95% • Indications
• Delivery of high FiO2
• Contraindications• Apnea• Poor respiratory effort
–Used at 10 to 15 L/min
Monitor effectiveness of Ventilation
• Visible chest rise with each breath
• SpO2 • ETCO2 • HR• BP• Pt responsiveness• Air entry on auscultation
If ventilation is not effective…• Reposition pt. Reposition
airway. OPA.• Verify proper mask size and
placement• Suction airway• Check O2 source and flow• Check bag and mask for
function/leaks• Treat gastric inflation
Indications for intubation
• Respiratory distress• Apnea• Upper airway obstruction or
the potential to develop upper airway obstruction
• Actual or potential decrease in airway protection (compromised neurological function)
• Inadequate ventilation and/or oxygenation
Preparing for Intubation• Appropriate ETT for >1 yo: (age/4) + 4
Term infant: 3.0-3.5 ID6 mo: 3.5-4.0 ID1 yo: 4.0-4.5 ID
• Cuffed ETT’s for pt’s > 8 yo• If you anticipate need for high PEEP or
PIP (peak inspiratory pressure) may want to use cuffed ETT with <8 yo. Use ½ size smaller ETT.
• Remember SOAPME
Suction equipment
Oxygen: O2 flowmeter, preoxygenate 2-3 min, manual resuscitator bag with mask
Airway equipment: ETT, stylet, syringe (cuffed ETT), laryngoscope and blade, lubricating gel, OPA
Position, pharmacy, personnel: supine, rolls for positioning, bed height up
Monitors
ETCO2 detector
SOAPME
Complications
• Decrease in systemic venous return• Pulmonary barotrauma can be caused. Pulmonary barotrauma is lung injury that results from the hyperinflation of alveoli past the rupture point.• Increased intracranial pressure — In people with normal lung compliance, PEEP may increase the intracranial pressure (ICP) due to an impedance of venous return from the head.[7]• Renal functions and electrolyte imbalances, due to decreased venous return metabolism of certain drugs are altered and acid-base balance is impeded.[8]
Positive end-expiratory pressure (PEEP) is the pressure in the lungs (alveolar pressure) above atmospheric pressure (the pressure outside of the body) that exists at the end of expiration.[1] The two types of PEEP are extrinsic PEEP (PEEP applied by a ventilator) and intrinsic PEEP (PEEP caused by a non-complete exhalation). Pressure that is applied or increased during an inspiration is termed pressure support.
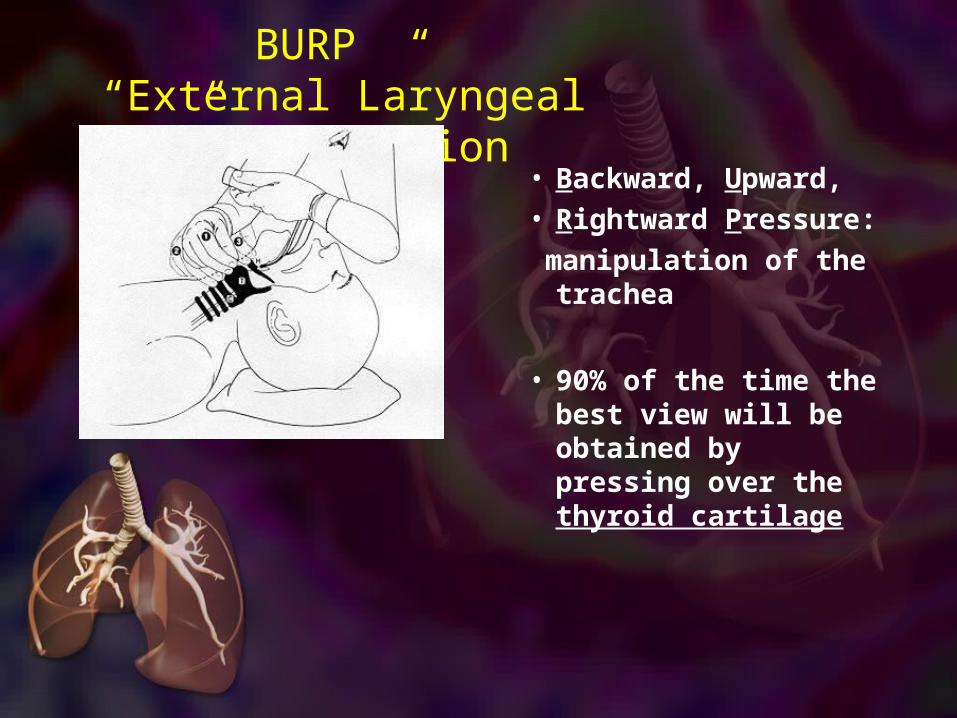
“BURP” “External Laryngeal
Manipulation”• Backward, Upward, • Rightward
Pressure: manipulation of the
trachea
• 90% of the time the best view will be obtained by pressing over the thyroid cartilage

Using The Miller Blade
Better in younger children with a floppy epiglottis
Straight Laryngoscope Blade – used to pick up the epiglottis
Post-Intubation• ETCO2 assessment for
confirmation of placement• Auscultation for bilateral air entry• Placement of ETT documented• ETT secured with tapes• CXR to confirm placement• Place pt on ventilator
Suctioning ETT
• Suction frequency depends on ETT size and pt needs:
•4.0 i.d. and smaller- a minimum of Q8H unless otherwise ordered
•4.5 i.d. and greater- prn or as ordered
• Suction depth should only be 0.5 cm past the end of ETT
•Determine suction depth by using suction guide or match number on catheter to number on ETT and advance 0.5 cm.
Selecting suction catheter
• Use largest size that can pass easily down the ETT
• Ideally not larger than half the diameter of ETT to avoid causing atelectasis
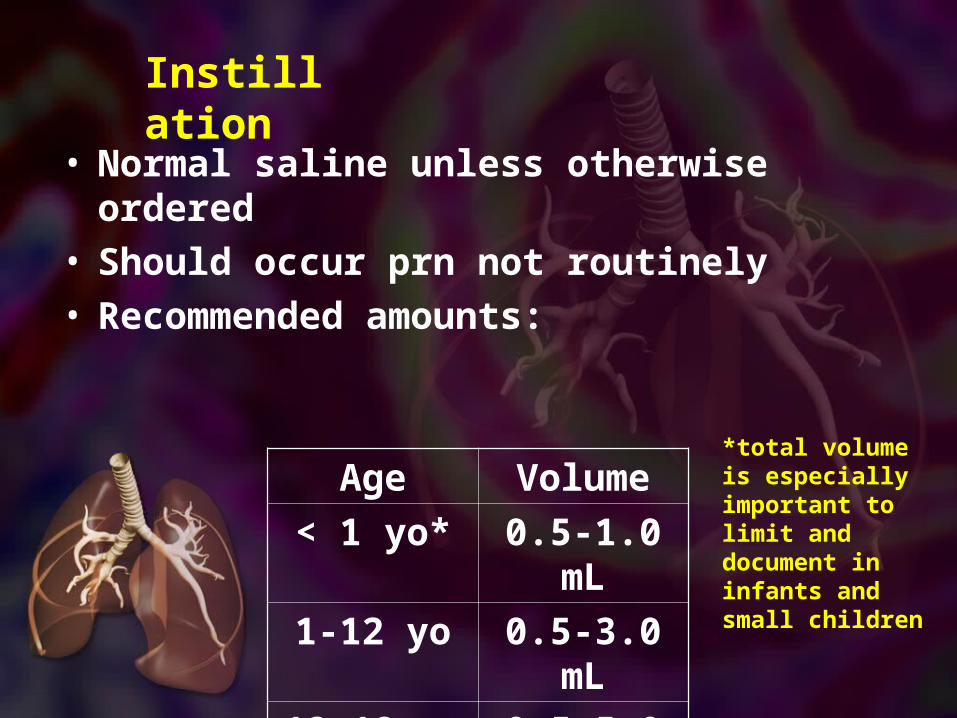
Instillation
• Normal saline unless otherwise ordered
• Should occur prn not routinely• Recommended amounts:
Age Volume
< 1 yo* 0.5-1.0 mL
1-12 yo 0.5-3.0 mL
13-18 yo 0.5-5.0 mL
*total volume is especially important to limit and document in infants and small children
Closed Suction
• Ensure suction is on and set appropriately• Ensure bagging unit attached to O2, adequate flow, and
intact• Attach sterile syringe with appropriate instillation
solution to instillation port• Securely hold ETT with one hand and insert catheter to
appropriate depth with the other• Apply continuous suction while slowly withdrawing the
catheter• Flush catheter by instilling into instillation port while
applying suction• Allow pt to re-oxygenate at least 30 sec between passes
Back-up Plan
• Can’t ventilate or basics not working• Consider adjuncts
(OPA/NPA/positioning)• Intubation?
• Can’t intubate• Rescue devices
• Can’t rescue• Surgical procedure

Basics
• Positioning• Adjuncts
• OPA - good choice if tolerated• NPA - easy to tear mucosa
• Effective BVM use is most important skill• Get a good seal (two person
better)• Don’t over ventilate
• Don’t forget the suction
Intubation -Preparation
• Preoxygenate• Monitors - ECG, pulse
ox• Sellick’s• Good basics
• Equipment selection• Miller vs. Mac• Cuffed vs. uncuffed• ETT size
• Positioning
Blind Techniques• Exist but need practice for proficiency• Digital intubation
• Small work area• Blind nasotracheal intubation
• Tough angles for tube placement• Remember anatomic differences• Contraindicated until >10 years old
In general, blind techniques not useful in children
Laryngospasm
common when extubation is done when the patient is in a semiconscious state
extubation should be done in a deep anesthesia or when the protective laryngeal reflex has returned
Extubation• ensure that the patient is recovering is breathing spontaneously with adequate volumes
• evaluate the patient's ability to protect his airway by observing whether the patient responds appropriately to verbal commands
• Oxygenate patient with 100 percent high flow O2 for 2 to 3 minutes
• if secretions are suspected in the tracheobronchial tree, remove them with a suction catheter through the lumen of the endotracheal tube
• ensure that the patient is not in a semiconscious state
• deflate the cuff and remove the endotracheal tube quickly and smoothly during inspiration
• continue to give the patient O2 as required
Rescue Devices
• LMAs (laryngeal mask airway)
• Combitube
LMA • Used in any age
• Easy to place • Few complications• Contraindications:
• Gag reflex• FBs• Airway obstruction• High ventilation
pressure• Does not secure airway
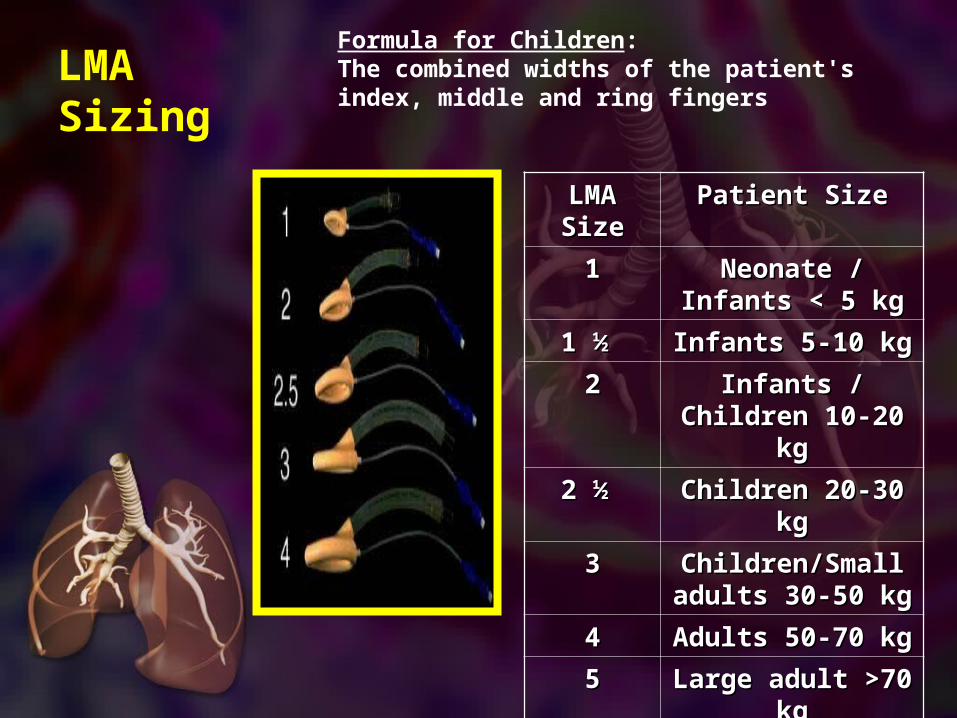
LMA Sizing
LMA LMA SizeSize
Patient SizePatient Size
11 Neonate / Neonate / Infants < 5 kgInfants < 5 kg
1 ½ 1 ½ Infants 5-10 kgInfants 5-10 kg
22 Infants / Infants / Children 10-20 Children 10-20
kgkg
2 ½ 2 ½ Children 20-30 Children 20-30 kgkg
33 Children/Small Children/Small adults 30-50 kgadults 30-50 kg
44 Adults 50-70 kgAdults 50-70 kg
55 Large adult >70 Large adult >70 kgkg
66
Formula for Children: The combined widths of the patient's index, middle and ring fingers
Combitube
• Two sizes• Small (4 to 5.5 feet
tall)• Regular (over 5.5 feet
tall)• Not useful in most kids
• Easy to place• Contraindications
• Gag reflex• Esophageal disease• Caustic ingestions• FBs/Airway
obstruction
Surgical Airways - Cricothyrotomy• Indications (only if >10 years old)
• Failed airway• Failed ventilation
• Predictors of difficulty• Previous neck surgery• Obesity• Hematoma or infection

automated external
defibrillatorAED
• Age > 8 years• use adult AED
• Age 1-8 years• use paediatric pads /
settings if available (otherwise use adult mode)
• Age < 1 year• use only if
manufacturer instructions indicate
it is safe

Title
•Text
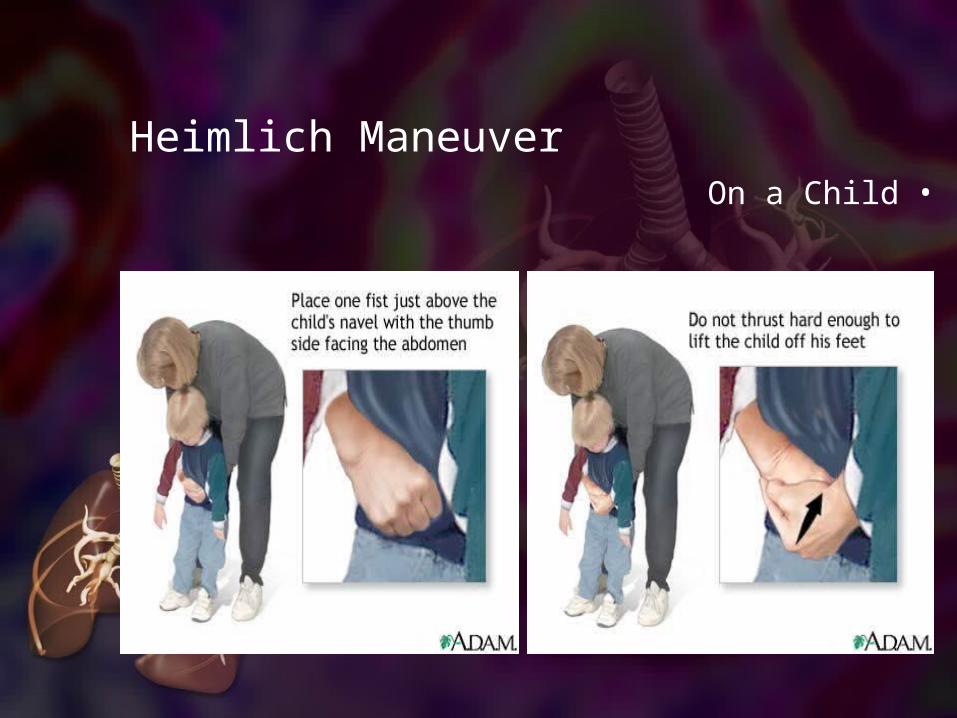
Heimlich Maneuver•On a Child
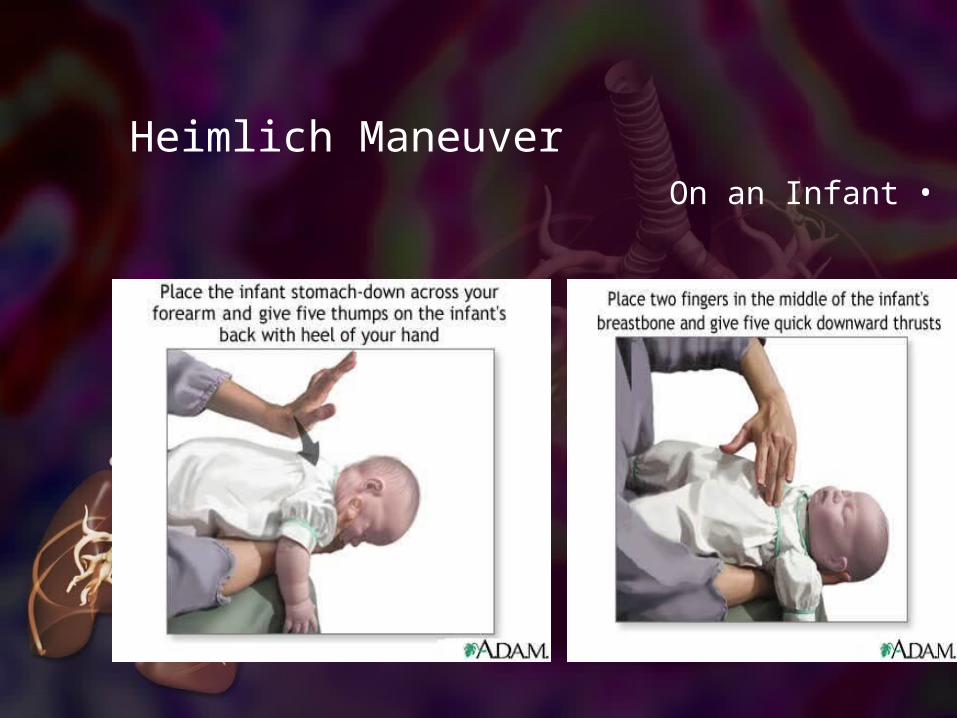
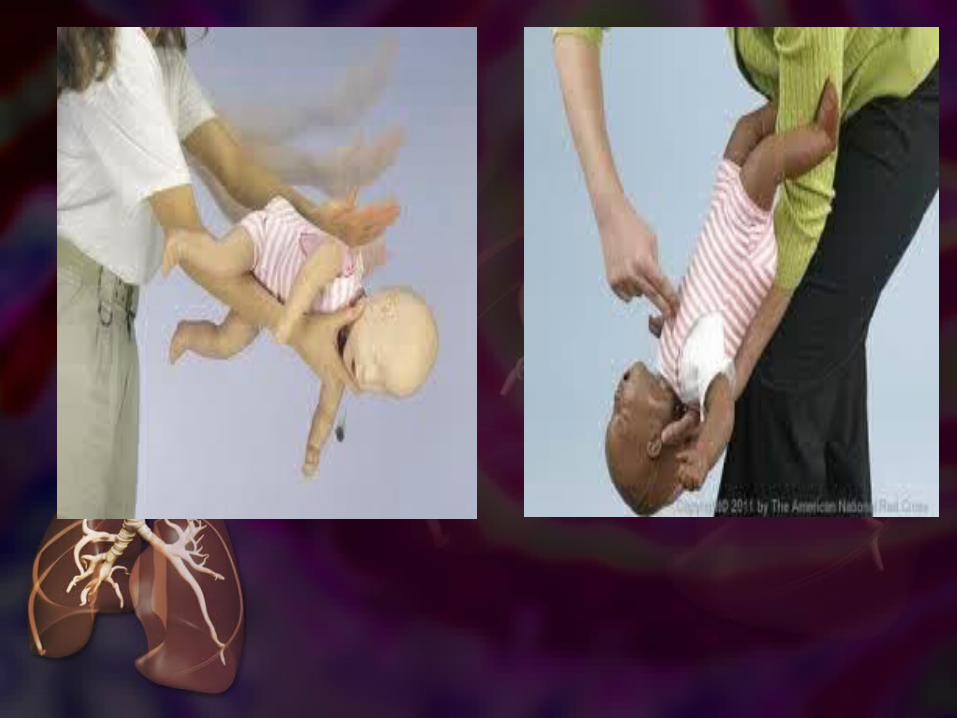
Heimlich Maneuver•On an Infant
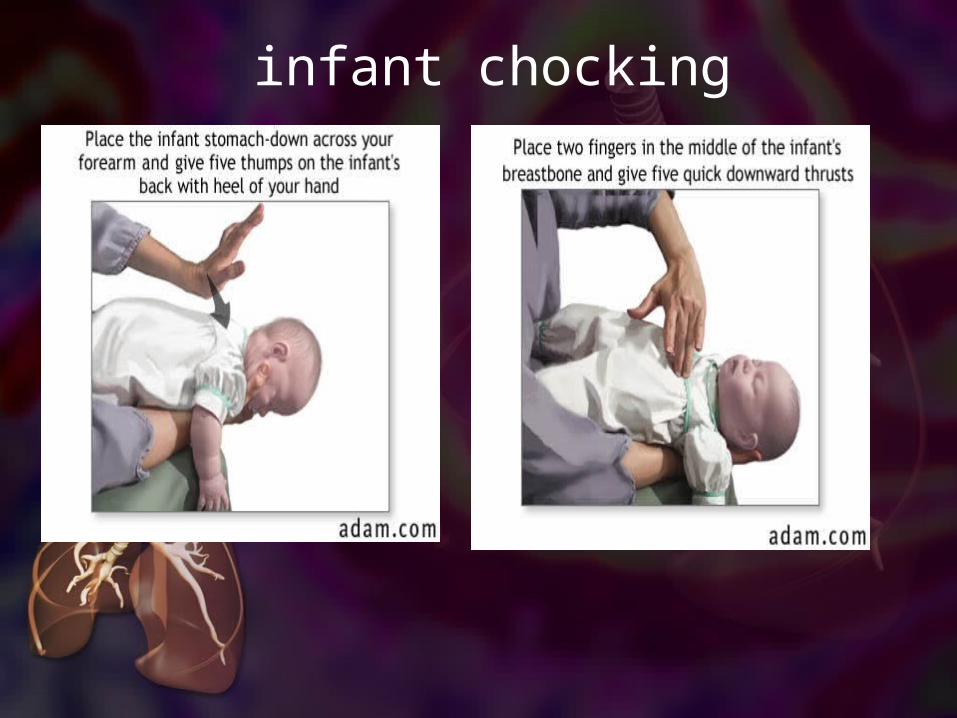
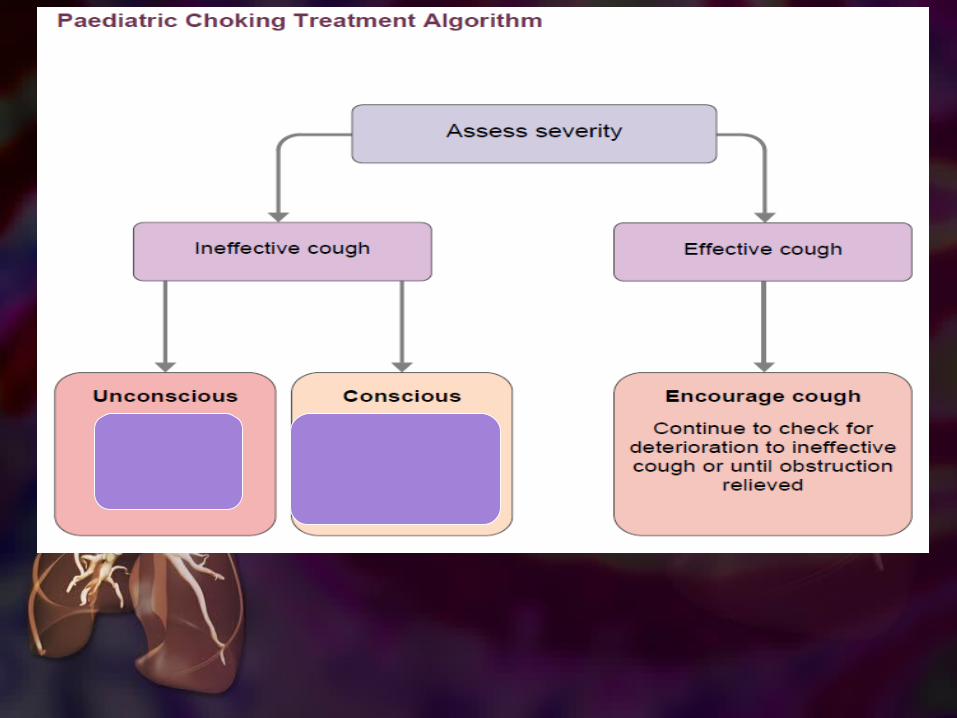
infant chocking
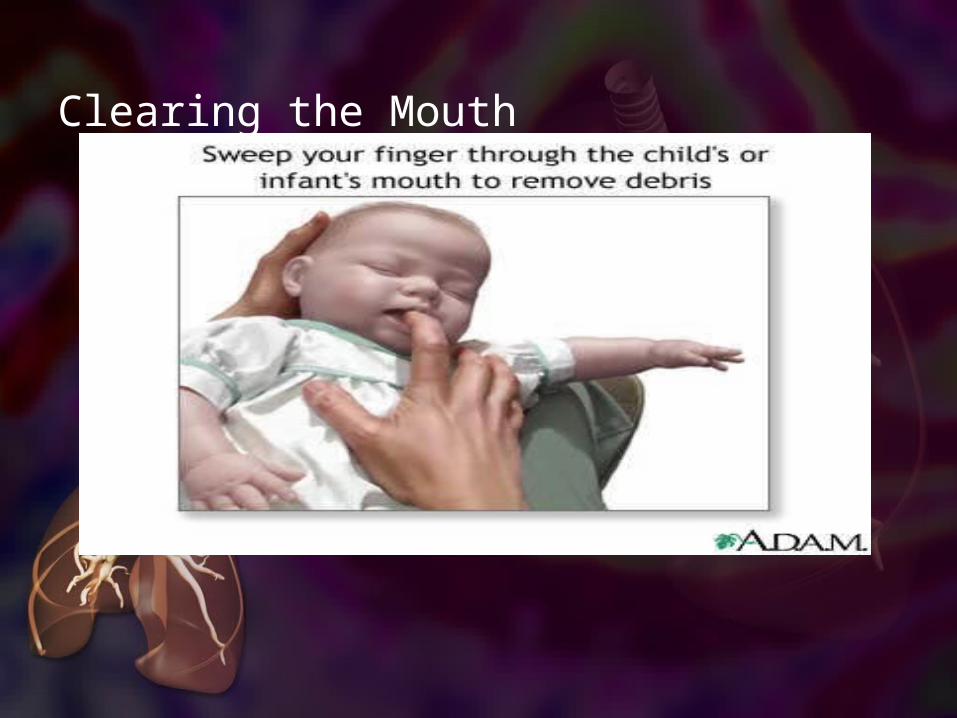
Clearing the Mouth
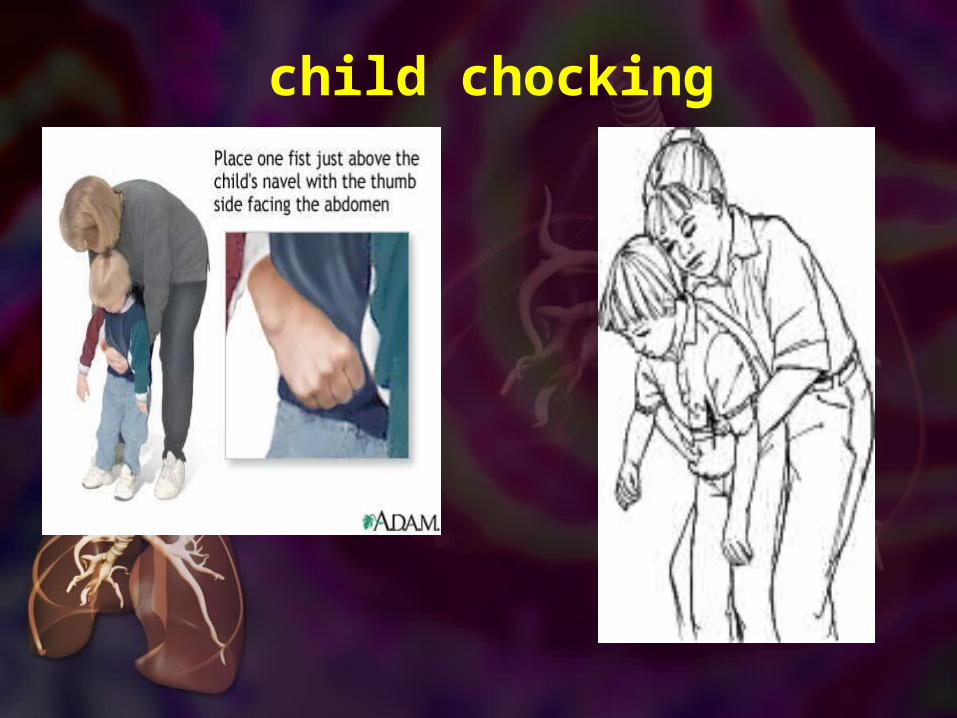
child chocking
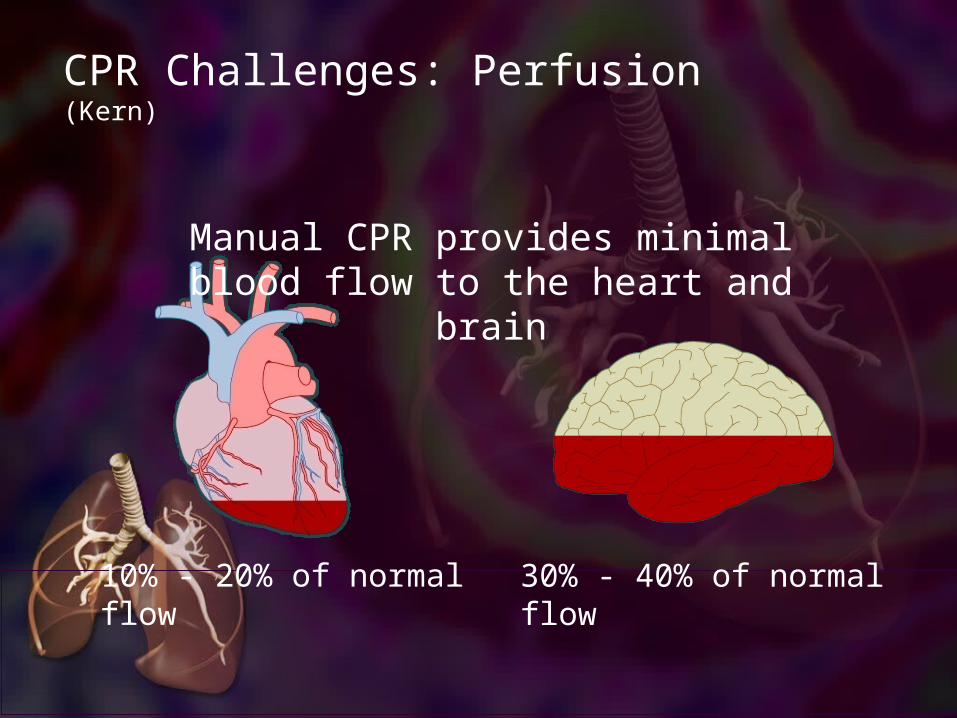
CPR Challenges: Perfusion (Kern)
Manual CPR provides minimal blood flow to the heart and brain
30% - 40% of normal flow10% - 20% of normal flow
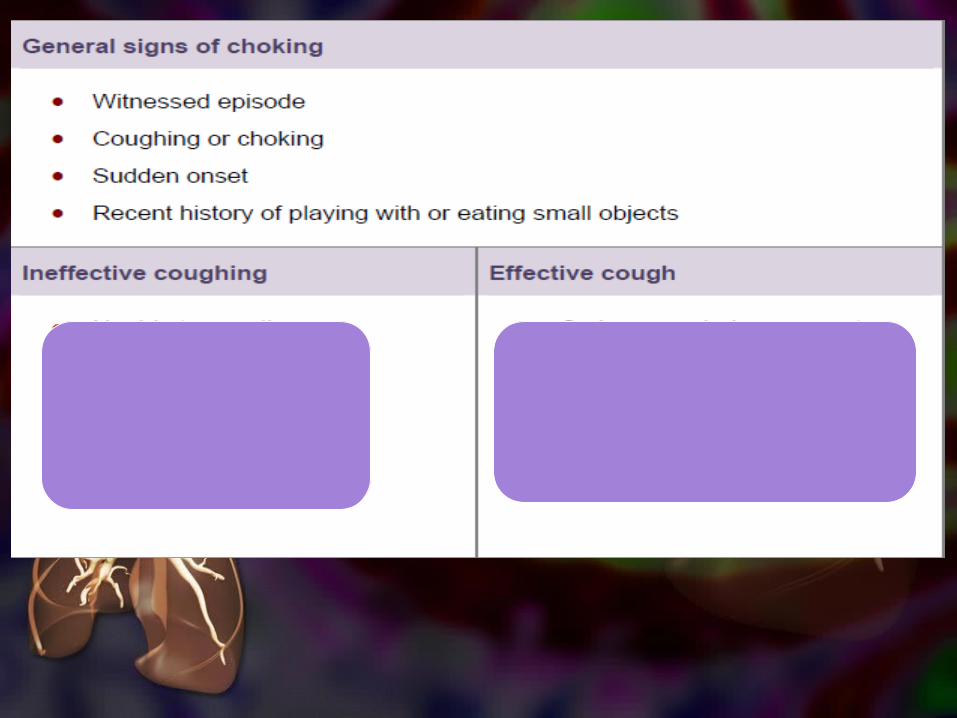
گرانتینگ: بازدم صداداری است که به دلیل بسته بودن اپی گلوت ایجاد میشود و در نوزادان مثل ناله کردن میمونهناله يا صداي خرخر
مانند بازدمي .
صدای غیر طبیعی دیگر استرایدور است. این صدا هنگام عبور هوا از مجاری بزرگ اکسترا توراسیک مثل نای که تنگ شده باشند ایجاد میشود
و مانند صدای سرفه های خشک صدادار همچون پارس سگ میماند. مثل موقعی که میگن طرف خروسک گرفته.
ویزینگ:اس}ت ک}ه در راهه}ای ه}وایی high pitchصدایی م}داوم و موزیک}ال و
کوچ}ک در ب}ازدم ش}نیده میش}ود.این ص}دا را در م}وارد تنگی راهه}ای هوایی مثل آسم میتوانیم بشنویم.