PEDIATRIC ABDOMINAL CASE STUDIES - cdn.ymaws.com · APPENDICITIS Abdominal pain caused by distended...
24
9/26/2016 1 PEDIATRIC ABDOMINAL CASE STUDIES Julie McKee, RN, MN, CPNP DISCLOSURES: NONE OBJECTIVES 1. Identify patients that need referral to pediatric surgery and urgency of that referral. 2. Discuss clinical considerations in the use of diagnostic evaluation in pediatric patient with abdominal pain. 3. Identify abnormal stooling pattern in pediatric patients and discuss initial evaluation and management.
Transcript of PEDIATRIC ABDOMINAL CASE STUDIES - cdn.ymaws.com · APPENDICITIS Abdominal pain caused by distended...

9/26/2016
1
PEDIATRIC ABDOMINAL CASE STUDIES
Julie McKee, RN, MN, CPNP
DISCLOSURES: NONE
OBJECTIVES
1. Identify patients that need referral to pediatric surgery and urgency of that referral.
2. Discuss clinical considerations in the use of diagnostic evaluation in pediatric patient with abdominal pain.
3. Identify abnormal stooling pattern in pediatric patients and discuss initial evaluation and management.

9/26/2016
2
CASE STUDY #1
14 year old female with acute onset lower abdominal pain
No fevers, nausea, vomiting or diarrhea
No urinary symptoms
Normal stooling pattern
No ill contacts
HISTORY
PMH: ovarian teratoma
PSH: right oopherectomy
PHYSICAL EXAM
General: No acute distress
Abdomen: soft, nondistended, tender in bilateral lower quadrants, no palpable masses
9/26/2016
3
DIAGNOSTICS
DIAGNOSTICS
TUMOR MARKER LABS
AFP, HCG quantitative tumor antigen
LH, FSH
Inhibin A, Inhibin B
CEA, CA 19‐9, CA 125
Anti mullerian hormone

9/26/2016
4
OVARIAN TERATOMA, HEMORRHAGIC CYST, FOLLICULAR CYSTOVARIAN TORSION
Ultrasound used to determine size of mass, characteristics: solid vs cyst, blood flow to the ovaries
MRI used to evaluate this further in complex patient as ours
Tumor markers: normal results for our case study
Simple cysts less than 5 cm can be watched and surveilled with US. Most are follicular cysts. Cysts with few internal septationscan be observed with repeat imaging, most are hemorrhagic cysts.
Solid components need further evaluation with surgeon
Torsion is an emergent condition as the ovary can be salvaged
QUESTIONS
CASE STUDY #2
8 yr old female with 1 day abdominal pain
Started periumbilical area, worsened with time
Decreased appetite, no nausea or vomiting
One loose stool
No urinary symptoms
No ill contacts
In ER, pain now in RLQ, low grade fever
No PMH/PSH – otherwise healthy
9/26/2016
5
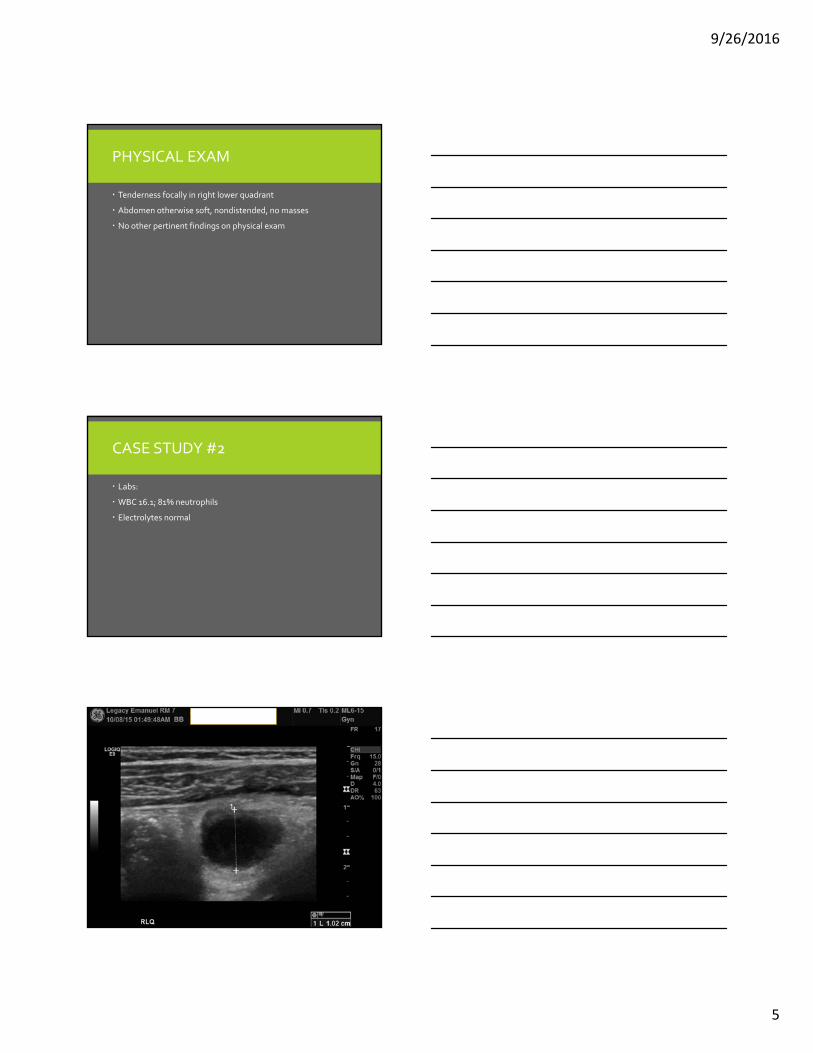
PHYSICAL EXAM
Tenderness focally in right lower quadrant
Abdomen otherwise soft, nondistended, no masses
No other pertinent findings on physical exam
CASE STUDY #2
Labs:
WBC 16.1; 81% neutrophils
Electrolytes normal

9/26/2016
6
PAIN VS TENDERNESS
DIFFERENTIAL
Female: ovarian pathology, endometriosis
Urinary tract
Gastrointestinal (IBD,constipation)
Pneumonia, strep throat
APPENDICITIS
Abdominal pain caused by distended appendix, pain usually comes first in history, followed by +/‐ nausea, vomiting, anorexia, fever, pain is constant

9/26/2016
7
PHYSICAL EXAM
Obturator sign‐ pain with internal rotation of leg
Rovsing sign – rebound tenderness at RLQ site after pushing and releasing LLQ
Psoas sign– pain with raising leg against resistance
Pain should be constant, worse with palpation/percussion to RLQ
Distraction good technique with pediatric patient
US FINDINGS
Noncompressible
Size
Surrounding tissue
Tenderness with exam
Fluid collection
Free fluid vs loculated fluid
DIAGNOSTIC ACCURACY
In study using maximal outer diameter of greater than or equal to 7 mm for the appendix, US compared favorably to CT
This saves patient radiation exposure, lower cost
If CT scan warranted, dose reduction of radiation strategies should be implemented.
If your local imaging is not regularly doing pediatric US, clinical suspicion is high, refer
If you are considering CT scan, refer
Children are more sensitive to the radiation, have longer life expectancy to manifest late effect cancer

9/26/2016
8
MANAGEMENT
OR for laparoscopic appendectomy
Preoperative considerations:
Hydration, antibiotics
ACUTE PERFORATED APPENDICITIS MANAGEMENT
Antibiotic treatment with inteval appendectomy 6‐8 weeks later vs operation
Limited CT scan to determine well formed abscess
If intraabdominal abscess, abdominal pain > 3 days duration, upfront antibiotics, IR drain if possible and interval appendectomy 8 weeks later
ACUTE PERFORATED APPENDICITIS TREATMENT PROTOCOL
Observational study of pediatric patients with suspected acute perforated appendicitis at Miami Children’s Hospital
Less than 96 hours of symptoms, WBC >12,000, diagnostic imaging findings
Exclusions: symptoms > 96 hours, palpable mass on exam, or well formed abscess seen on imaging
Zosyn, PICC, minimum 7 day course
Discontinuation of abx: afebrile > 48, normal WBC, absence of tenderness (fever = >100)
18 month study, 751 patients

9/26/2016
9
STUDY DISCUSSION
More likely to be ruptured: younger age, pain longer than 3 days, generalized tenderness, fever over 38 degrees celsius.
Lower complication rates, fewer abscesses, trend toward shorter LOS
Treatment failure predictors: WBC> 15,000, especially when accompanied by fecalith, symptoms > 48 hours
Other studies: prolonged fever, higher band count, imaging findings of disease spread beyond RLQ
OUR TREATMENT PROTOCOL PERFORATED APPENDICITIS
Ceftriaxone, flagyl once daily IV dose
Discharge criteria: home once afebrile (<38) for 48 consecutive hours, eating, pain controlled, ambulating, no diarrhea, normalized white blood cell count
NONVISUALIZEDAPPENDIX
This can present a diagnostic challenge. If you are clinically suspicious of appendicitis, refer.
Ensure close follow up if imaging/labs reassuring – can be done with PCP

9/26/2016
10
RED FLAGS
When evaluating children with vague abdominal pain, differential is broad, few things to consider:
Weight loss
Severe vomiting
Chronic severe diarrhea
GI bleeding
Hematemesis
Family history of inflammatory bowel disease
Appropriate referral may be to start with pediatric GI
QUESTIONS
CASE STUDY #3
8 week old female
Nonbilious vomiting after every feed for 2 weeks, increased fussiness
Passing flatus, no bowel movement x 2 days
Decreased urine output

9/26/2016
11
PHYSICAL EXAM
LABS
• NA 135
• K 3.7
• CL 91* (low)
• CO2 34* (high)
• BUN 13
• CREATININE 0.24*
• GLUCOSE 105*
• CALCIUM 10.8
9/26/2016
12
US FINDINGS
Size criteria – based on age, 4 mm x 14 mm (width x length)
GI tract content not moving through pylorus
UGI can suggest pyloric stenosis, but gold standard test is ultrasound with size criteria
DIFFERENTIAL
Bilious vomiting –must be evaluated for malrotationimmediately
Reflux
Classic lab findings: metabolic alkalosis
PYLORIC STENOSIS
Thickened and elongated pylorus that acts like an obstruction
Pylorus is smooth muscle at
end of stomach
Firstborn, more common in male

9/26/2016
13
MANAGEMENT
OR for pyloromyotomy
Preoperative considerations: fluid resuscitation, electrolyte correction will happen with fluid resuscitation, NPO
Study based fluid needs and LOS on chloride level at diagnosis. For chloride <97: 2 x 20m/kg NS bolus, recheck labs to expedite care, decrease cost
Early diagnosis= less electrolyte derangement and shorter LOS
QUESTIONS
CASE STUDY #4
9 mos old male with abdominal pain, emesis and bloody stool
One week prior had been to ER for poor feeding and emesis
No PMH/PSH

9/26/2016
14
LABS
• WBC 7
• HCT 31.5
• Plt 449
• Na 138
• K 4.2
• Cl 99
• Co2 22
• BUN .2
• Creat 0.2
• Glucose 90
ULTRASOUND
INTUSSUSCEPTION

9/26/2016
15
DECISION MAKING
Differential
ileocolic vs small bowel‐small bowel intussusception
Other historical information
Other diagnostics
Concern for intussusception : notification of pediatric surgery team, radiologic reduction can happen elsewhere, be prepared to transfer, require IV access at our institution. Risk of perforation during exam.
Small bowel‐small bowel often resolves, does not require urgent referral
9/26/2016
16
DIFFERENTIAL
Classic presentation: age range 6 months‐ 6 years, preceeded by viral illness symptoms, crampy abdominal pain – Ileocolic
Small bowel to small bowel can happen intermittently and usually does not require surgery
Older children, consider pathologic mass as a lead point –lymphoma
MANAGEMENT
Fluid resuscitation
Enema reduction – if successful, observation for recurrence
74‐79% success rate
If unsuccessful, delayed repeat enema vs operative reduction
Retrospective review over 5 year period: of the unsuccessful enema reduction group, ¾ went to surgery, ¼ had delayed repeat enema. 64% of delayed repeat enema did not need surgery
Bowel resection occurred more often with immediate surgery group
QUESTIONS
9/26/2016
17
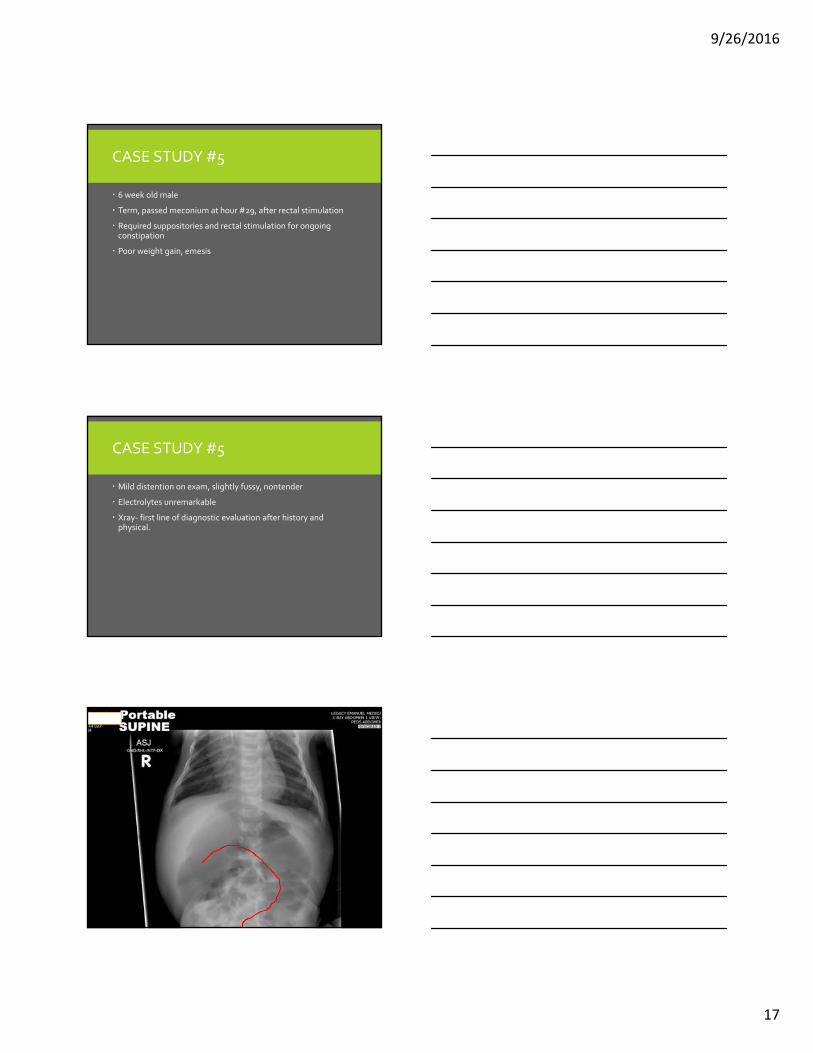
CASE STUDY #5
6 week old male
Term, passed meconium at hour #29, after rectal stimulation
Required suppositories and rectal stimulation for ongoing constipation
Poor weight gain, emesis
CASE STUDY #5
Mild distention on exam, slightly fussy, nontender
Electrolytes unremarkable
Xray‐ first line of diagnostic evaluation after history and physical.
CASE STUDY #5

9/26/2016
18
DIFFERENTIAL
Distal bowel obstruction
Rectal exam – patent anus?
Rush of air and stool on exam…
DECISION MAKING
Infants should pass first meconium in first 24 hours of life
Stooling patterns in infancy can vary widely
Refer to pediatric surgery, we often will order contrast enema
Keep child stooling until they can be seen – glycerin suppositories
CASE STUDY #5
Suction rectal biopsy
Path: Suction rectal biopsy:‐Ganglion cells (presence/absence): ABSENT; No ganglion cellspresent.‐Nerve Trunk Hypertrophy (presence/absence): PRESENT‐Calretinin Stain Result: NEGATIVE

9/26/2016
19
HIRSCHSPRUNGS
Aganglionic intestine can only contract
Peristalsis requires contraction and relaxation to have bowel movement
MANAGEMENT
Rectal irrigations with warm saline, 20 ml/kg with soft red rubber tube
Parents can be taught to do at home
Surgical intervention – colostomy – 2 stage procdure
Pull through as 1 stage to remove aganglionic bowel
LONG TERM CONSIDERATIONS
Enterocolitis
Bowel management

9/26/2016
20
QUESTIONS
CONSTIPATIONEvidence based guidelines from North American Society for Pediatric
Gastroenterology, Heptalogy, and Nutrition (NASPGHAN) and European Society for Pediatric Gastroenterology, Heptalogy and Nutrition(ESPGHAN)
QUESTION 1: WHAT IS THE DEFINITION OF FUNCTIONAL CONSTIPATION?
Rome III diagnostic criteria
In the absence of pathology, 2 or more of the following for child <4 years of developmental age for at least 1 month
less than or = 2 defecations a week
1 episode of incontinence per week
History of excessive stool retention
History of painful or hard BM
Presence of large fecal mass in rectum
History of large diameter stools
Accompanying symptoms may include irritability, decreased appetite, and or early satiety, which may disappear immediately following passage of a large stool
9/26/2016
21
ROME III DIAGNOSTIC CRITERIA FOR FUNCTIONAL CONSTIPATION
For children with developmental age >4 with insufficient criteria for IBS, have to have criteria fulfilled at least once per week for at least 2 months before diagnosis:
less than or = 2 defecations a week
1 episode of incontinence per week
History of retentive posturing or excessive volitional stool retention
History of painful or hard BM
Presence of large fecal mass in the rectum
History of large diameter stool
ALARM SIGNS AND SYMPTOMS
Constipation starting early < 1 month of age
Delayed passage of meconium > 48 hours of life
Family history of Hirschsprungs disease
Failure to thrive
Bilious vomiting
Severe abdominal distention
Abnormal position of anus/ perianal fistula
Decreased lower extremity strength/tone/reflex
REFERRAL
HISTORY
Key to guide your evaluation
Onset, precipitating factors, passage of meconium
Family history
Psychosocial history
Growth curve
Toilet training history
9/26/2016
22
PHYSICAL EXAM
General health
Abdominal exam
Perianal exam
DRE – if you suspect HD, not needed if you suspect functional constipation
Xray‐ not needed to diagnose functional constipation
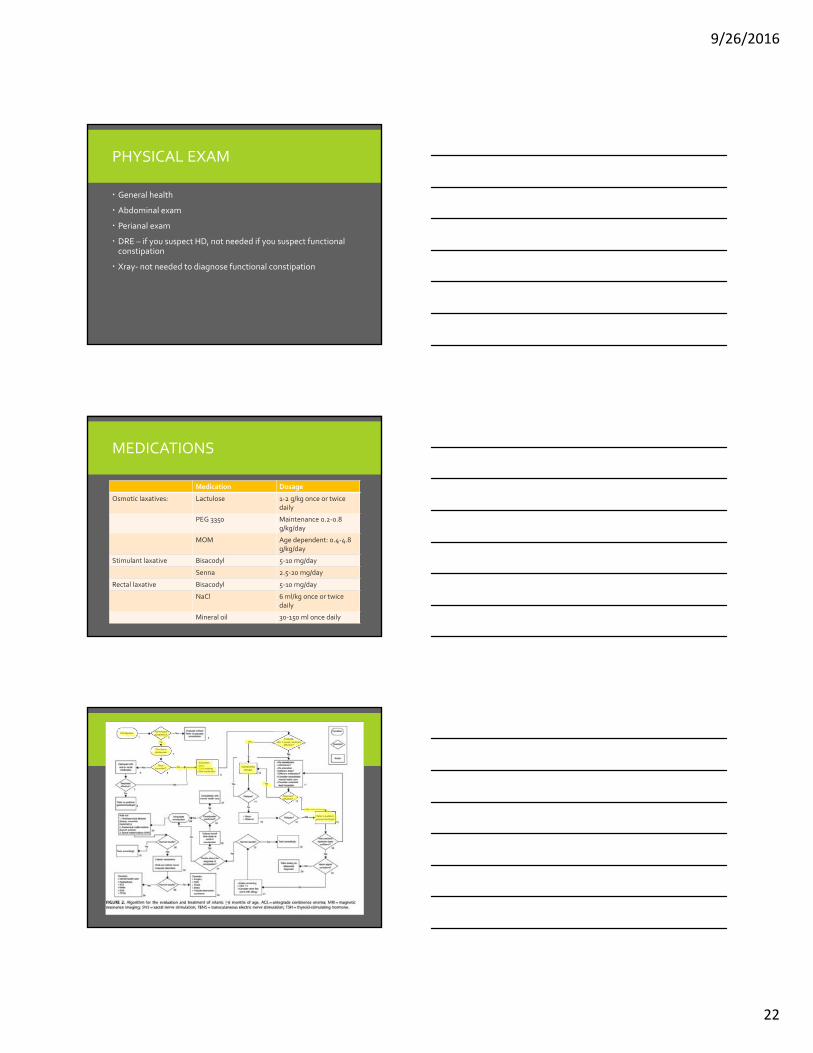
MEDICATIONS
Medication Dosage
Osmotic laxatives: Lactulose 1‐2 g/kg once or twicedaily
PEG 3350 Maintenance 0.2‐0.8 g/kg/day
MOM Age dependent: 0.4‐4.8 g/kg/day
Stimulant laxative Bisacodyl 5‐10 mg/day
Senna 2.5‐20 mg/day
Rectal laxative Bisacodyl 5‐10 mg/day
NaCl 6 ml/kg once or twice daily
Mineral oil 30‐150 ml once daily

9/26/2016
23
QUESTIONS
PEDIATRIC SURGERY RESOURCES
OHSU and Legacy
503.494.4799
503.413.4300
APSNA –American Pediatric Surgical Nurses Association, Inc.
Apsna.org – access to patient education handouts in English and Spanish
Email: [email protected]
REFERENCES
Ashcraft, K. W., Holcomb, G. W., Murphy, J. P., & Ostlie, D. J. (2010). Ashcraft's pediatric surgery (5th ed.). Philadelphia: Saunders/Elsevier.
Dalton, B. G., Gonzalez, K. W., Boda, S. R., Thomas, P. G., Sherman, A. K., & Peter, S. D. (2016). Optimizing fluid resuscitation in hypertrophic pyloric stenosis. Journal of Pediatric Surgery. doi:10.1016/j.jpedsurg.2016.01.013
Goldin, A.B., Khanna, P., Thapa, M., McBroom, J.A., Garrison, M.M., Parisi, M.T. (2011). Revised criteria for appendicitis in children improve diagnostic accuracy. Pediatric Radiology. 41:993‐999.
Green, M. (1998). Pediatric diagnosis: Interpretation of symptoms and signs in children and adolescents (6th ed.). Philadelphia: Saunders.
Lautz, T. B., Thurm, C. W., & Rothstein, D. H. (2015). Delayed repeat enemas are safe and cost‐effective in the management of pediatric intussusception. Journal of Pediatric Surgery, 50(3), 423‐427. doi:10.1016/j.jpedsurg.2014.09.002

9/26/2016
24
REFERENCES
Miglioretti, D. L., Johnson, E., Williams, A., Greenlee, R. T., Weinmann, S., Solberg, L. I., Smith‐Bindman, R. (2013). The Use of Computed Tomography in Pediatrics and the Associated Radiation Exposure and Estimated Cancer Risk. JAMA Pediatrics JAMA Pediatr, 167(8), 700. doi:10.1001/jamapediatrics.2013.311
Nazarey, P. P., Stylianos, S., Velis, E., Triana, J., Diana‐Zerpa, J., Pasaron, R., Burnweit, C. (2014). Treatment of suspected acute perforated appendicitis with antibiotics and interval appendectomy. Journal of Pediatric Surgery, 49(3), 447‐450. doi:10.1016/j.jpedsurg.2013.10.001
Olson, A. D., Hernandez, R., & Hirschl, R. B. (1998). The role of ultrasonography in the diagnosis of pyloric stenosis: A decision analysis. Journal of Pediatric Surgery, 33(5), 676‐681. doi:10.1016/s0022‐3468(98)90186‐5
Smith, J., & Fox, S. M. (2016). Pediatric Abdominal Pain. Emergency Medicine Clinics of North America, 34(2), 341‐361. doi:10.1016/j.emc.2015.12.010
REFERENCES
Tabbers, M., Dilorenzo, C., Berger, M., Faure, C., Langendam, M., Nurko, S., Benninga, M. (2014). Evaluation and Treatment of Functional Constipation in Infants and Children. Journal of Pediatric Gastroenterology and Nutrition, 58(2), 265‐281. doi:10.1097/mpg.0000000000000266